Back to Journals » Clinical Ophthalmology » Volume 20
Evaluation of Risk Factors for Unilateral Aponeurotic Ptosis Using the Fellow Eye as Control: A Retrospective Study
Authors Katsuo A, Iwasaki K, Takayanagi R, Tanaka N, Suzuki M, Arimura S, Takamura Y, Inatani M
Received 11 December 2025
Accepted for publication 27 January 2026
Published 2 February 2026 Volume 2026:20 585186
DOI https://doi.org/10.2147/OPTH.S585186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ayami Katsuo,1 Kentaro Iwasaki,1 Ryoko Takayanagi,2 Nami Tanaka,1 Marie Suzuki,1 Shogo Arimura,1 Yoshihiro Takamura,1 Masaru Inatani1
1Department of Ophthalmology, Faculty of Medical Sciences, University of Fukui, Yoshida, Fukui, Japan; 2Faculty of Medicine, Hyogo Medical University, Nishinomiya, Hyogo, Japan
Correspondence: Kentaro Iwasaki, Department of Ophthalmology, Faculty of Medical Sciences, University of Fukui, 23-3 Shimoaizuki, Matsuoka, Eiheiji, Yoshida, Fukui, 910-1193, Japan, Tel +81-776-61-8400, Fax +81-776-61-8131, Email [email protected]
Purpose: Although aponeurotic ptosis is typically bilateral, the specific risk factors for unilateral cases remain unclear. Thus, we aimed to identify factors associated with unilateral aponeurotic ptosis by comparing eyes that underwent surgery with their non-ptotic contralateral counterparts.
Patients and Methods: This retrospective observational clinical study included patients who underwent levator resection for aponeurotic ptosis at the Fukui University Hospital, between April 1, 2014, and March 31, 2024, were included. The contralateral non-ptotic eye served as the internal control. The presence of risk factors, such as a history of filtering surgery, prostaglandin analog use, cataract surgery, and vitrectomy, was compared between the operated and fellow eyes using McNemar’s test. Firth’s penalized logistic regression analysis was performed to identify independent risk factors for unilateral aponeurotic ptosis.
Results: Sixty-eight patients were included in the analysis, with both eyes (136 eyes in total) evaluated. Glaucoma filtering surgery, prostaglandin analog use, and cataract surgery were significantly more frequent in operated eyes (P = 0.004, P = 0.045, and P = 0.002, respectively). Multivariate analysis showed that filtering surgery [odds ratio (OR) = 17.6, P = 0.009] and cataract surgery (OR = 2.07, P = 0.046) were independently associated with unilateral ptosis.
Conclusion: Prior glaucoma filtering and cataract surgeries are significant risk factors for the development of unilateral aponeurotic ptosis.
Keywords: unilateral aponeurotic ptosis, glaucoma filtering surgery, cataract surgery, prostaglandin analog, risk factors
Introduction
Aponeurotic ptosis is the most common form of acquired ptosis in older adults and is typically attributed to age-related dehiscence or disinsertion of the levator aponeurosis.1,2 It usually presents bilaterally; however, some patients may present with unilateral ptosis despite the absence of any apparent congenital, neurogenic, or myogenic cause. Although aponeurotic ptosis is prevalent in the aging population, the frequency and mechanisms underlying unilateral presentation remain insufficiently characterized.
Several ocular conditions and treatments, including glaucoma filtering surgery,3–11 long-term use of prostaglandin analogs,12–14 and cataract surgery,15–17 can induce mechanical or inflammatory changes that may contribute to degeneration of the levator aponeurosis. Moreover, habitual rigid gas permeable contact lens wear is a well-recognized iatrogenic factor associated with ptosis due to repeated manipulation of the eyelid.18–20 Furthermore, several systemic conditions, including dyslipidemia, obesity, impaired glucose metabolism, and diabetes mellitus, have been reported as potential risk factors for ptosis.21–25 These conditions may contribute to ptosis through metabolic and microvascular dysfunction, chronic low-grade inflammation, and age-related connective tissue degeneration affecting the levator aponeurosis. However, most previous studies have compared ptotic eyes with unrelated control groups, which may be confounded by interindividual differences in age, anatomy, and systemic factors. Only a limited number of studies have employed within-patient inter-eye comparisons to evaluate local ocular risk factors that may contribute to asymmetric disease manifestation.
Clinically, unilateral aponeurotic ptosis is of particular importance because it often results in noticeable cosmetic asymmetry, patient dissatisfaction, and challenges in surgical planning, including the selection of surgical technique and prediction of postoperative symmetry. Therefore, a better understanding of factors associated with unilateral involvement is essential for both etiological insight and clinical management.
Accordingly, this study aimed to identify risk factors associated with unilateral aponeurotic ptosis by using the fellow non-ptotic eye of the same individual as an internal control, thereby minimizing interindividual confounding and enabling a more precise assessment of local ocular contributors to asymmetric ptosis.
Material and Methods
Patient Selection
This retrospective clinical cohort study was approved by the Institutional Review Board of Fukui University Hospital in Japan and conducted in accordance with the Declaration of Helsinki. The requirement for informed consent was waived given the retrospective nature of the study. All patient data were anonymized prior to analysis, and confidentiality of patient information was strictly maintained in accordance with institutional and ethical guidelines.
We included patients who underwent surgery between April 1, 2014, and March 31, 2024, at Fukui University Hospital. All included patients underwent levator resection for unilateral aponeurotic ptosis, with the fellow eye without ptosis used as the control. Patients aged ≤20 years, as well as those with congenital, neurogenic, or myogenic ptosis, were excluded from the study.
Outcome Measures and Data Collection
We collected data on age, sex, history of rigid gas permeable contact lens wear, prior use of topical prostaglandin analogs, history of eyelid trauma, and history of intraocular surgery, including glaucoma filtering surgery, cataract surgery, and vitrectomy. Preoperative data were obtained from the patient’s medical records. The main outcome was the identification of risk factors for unilateral ptosis.
Statistical Analysis
All statistical analyses were performed using R software (version 4.5.1; R Foundation for Statistical Computing, Vienna, Austria). To compare the presence of each potential risk factor (history of filtering surgery, prostaglandin analog use, cataract surgery, and vitrectomy) between the operated and fellow eyes, McNemar’s test was applied to paired binary data. The exact McNemar’s test was used when the number of discordant pairs was ≤25. To identify independent factors associated with unilateral aponeurotic ptosis, logistic regression analysis was conducted. Because some explanatory variables were observed only in the operated eyes, leading to quasi-complete or complete separation, Firth’s penalized logistic regression was applied to obtain bias-reduced and stable estimates. The significance level was set at p < 0.05 for all tests.
Results
Preoperative Characteristics
A total of 68 patients (136 eyes) with unilateral aponeurotic ptosis who underwent levator resection were included in the study. The mean age was 72.7 ± 11.4 years, with 26 males and 42 females. Ten patients (14.7%) had a history of rigid gas permeable contact lens use, all of whom used lenses in both eyes. No patients had a history of eyelid trauma. Table 1 summarizes the preoperative characteristics compared with the contralateral control eyes. The number of patients with previous glaucoma filtering surgery was significantly higher in the operated group (13.2%) than in the control group (0.0%) (P = 0.004). Among the operated eyes, nine had a history of glaucoma filtering surgery: eight underwent trabeculectomy and one underwent Baerveldt glaucoma implant surgery. The number of patients with previous topical prostaglandin analog use was significantly higher in the operated group (19.1%) than in the control group (10.3%) (P = 0.045). In the operated group, prostaglandin-related eye drops were used in 13 eyes: five with latanoprost, five with bimatoprost, and one each with travoprost, tafluprost, and omidenepag isopropyl. In the control group, prostaglandin-related eye drops were used in seven eyes: four with latanoprost, three with bimatoprost, and one with travoprost. Additionally, the number of patients with previous cataract surgery was significantly higher in the operated group (69.1%) than in the control group (47.1%) (P = 0.002). No significant difference was observed in vitrectomy.
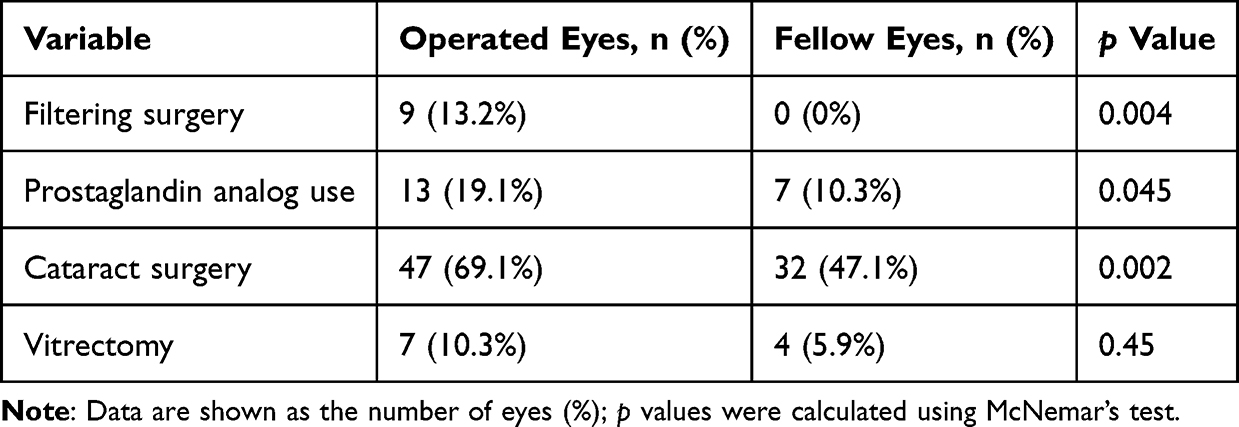 |
Table 1 Comparison of Preoperative Characteristics Between Operated and Fellow Eyes |
Multivariate Analysis of Risk Factors
Previous topical prostaglandin analog use, previous glaucoma filtering surgery, previous cataract surgery, and previous vitrectomy were evaluated as possible determinants of unilateral ptosis. Multivariate analyses using Firth’s penalized likelihood logistic regression in all eyes demonstrated that previous glaucoma filtering surgery and previous cataract surgery were significantly associated with the development of unilateral aponeurotic ptosis (Table 2). Among these two factors, previous glaucoma filtering surgery had the highest odds ratio (17.6). Prostaglandin analog use and vitrectomy were not statistically significant predictors.
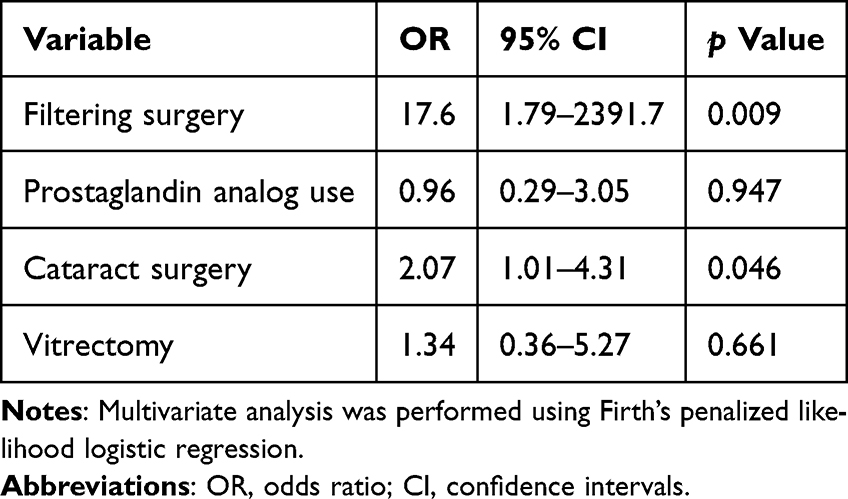 |
Table 2 Multivariate Analysis of Risk Factors for Unilateral Ptosis |
Discussion
In this study, we investigated risk factors associated with unilateral aponeurotic ptosis by comparing each operated eye with the contralateral non-ptotic eye of the same individual. This within-subject design minimized interindividual confounding factors and allowed for a more precise evaluation of local ocular conditions contributing to the asymmetric onset of ptosis. Our results demonstrate that a history of previous glaucoma filtering and cataract surgeries is independently associated with unilateral aponeurotic ptosis, while a history of prostaglandin analog use and vitrectomy is not.
The present findings are consistent with previous reports indicating that postoperative ptosis can occur after intraocular surgery.3–17,26,27 Proposed mechanisms include direct mechanical trauma to the levator aponeurosis from the eyelid speculum, postoperative inflammation, and prolonged eyelid edema, all of which may weaken the levator complex. Filtering surgery, in particular, often involves extensive conjunctival manipulation and prolonged eyelid traction, potentially resulting in levator dehiscence on the operated side. Cataract surgery has also been implicated as a cause of postoperative ptosis, especially when performed under prolonged local anesthesia or using a larger lid speculum.
Although prostaglandin-associated periorbitopathy (PAP) is a well-documented condition characterized by deepening of the upper eyelid sulcus and levator dehiscence,12–14,28 our study did not reveal a significant association between prostaglandin analog use and unilateral ptosis. Although a significant difference was observed in the simple paired comparison between operated and fellow eyes, this association did not remain significant when assessed using the multivariate analysis. This discrepancy may partly reflect the limited number of discordant pairs and the fact that most patients used the medication bilaterally, which could attenuate the detectable effect in the conditional model. Previous studies have suggested that a longer duration of prostaglandin analog therapy may exacerbate PAP-related eyelid changes, including ptosis;28,29 however, the duration of use could not be assessed in the present study, which may have limited our ability to detect an association between prostaglandin analog use and unilateral ptosis.
The role of vitrectomy in the development of ptosis remains controversial. While some reports have suggested postoperative eyelid drooping due to prolonged eyelid traction during pars plana vitrectomy,30,31 our results did not demonstrate a significant difference between operated and control eyes. This may be primarily attributed to the small number of vitrectomy cases, as well as variability in surgical techniques and operative duration.
The unique strength of this study lies in its within-subject design, directly comparing each patient’s operated eye with their contralateral, non-ptotic eye. This approach minimizes interindividual confounders such as age, sex, and systemic conditions, enabling a more precise assessment of local ocular factors. Moreover, multiple potential risk factors, including previous intraocular surgeries and prostaglandin analog use, were analyzed within a unified framework.
This study has certain limitations owing to its retrospective nature. First, data on the duration of prostaglandin analog use were unavailable. Because prolonged use of prostaglandin analogs may increase the risk of levator muscle or aponeurotic changes, the cumulative exposure period could influence ptosis development.28,29 Second, detailed perioperative information was not consistently available, including surgical time, lid speculum size, type of anesthesia, and intraoperative eyelid manipulation. Prolonged operative duration, excessive traction, or perioperative edema related to these factors may contribute to postoperative eyelid drooping.32 Third, detailed information on filtering surgery, such as surgical technique, use of traction sutures, needling procedures, and bleb morphology, was lacking. These factors may affect eyelid position and could contribute to the onset of aponeurotic ptosis.6,8,9,17 Fourth, wearing rigid gas permeable contact lens has been reported to induce aponeurotic ptosis in one eye.18 However, given that all rigid gas permeable contact lens users in this study wore lenses bilaterally, performing a direct inter-eye comparison was difficult. Moreover, the sample size for certain subgroups, such as vitrectomy cases, was relatively small, which may have limited statistical power to detect moderate associations. Therefore, a prospective study with standardized data collection is warranted to address these limitations and further elucidate the causal factors of aponeurotic ptosis.
Conclusion
In conclusion, previous intraocular surgeries, particularly filtering and cataract procedures, may contribute to the asymmetric onset of aponeurotic ptosis. Therefore, informing patients preoperatively about the potential risk of postoperative ptosis is important.27 When performing such procedures unilaterally, surgeons should also explain the possibility of postoperative cosmetic asymmetry between the two eyes.
Abbreviation
PAP, prostaglandin-associated periorbitopathy.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study design was approved by the Institutional Review Board of Fukui University Hospital in Japan (approval number: 20250170) and was conducted in accordance with the Declaration of Helsinki. The requirement for informed consent was waived due to its retrospective nature. All patient data were anonymized prior to analysis, and confidentiality of patient information was strictly maintained in accordance with institutional and ethical guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Frueh BR. The mechanistic classification of ptosis. Ophthalmology. 1980;87(10):1019–6. doi:10.1016/S0161-6420(80)35135-X
2. Sanke RF. Relationship of senile ptosis to age. Ann Ophthalmol. 1984;16(10):928–931.
3. Naruo-Tsuchisaka A, Maruyama K, Arimoto G, Goto H. Incidence of postoperative ptosis following trabeculectomy with mitomycin C. J Glaucoma. 2015;24(6):417–420. doi:10.1097/IJG.0000000000000174
4. Akai R, Yunoki T, Otsuka M, Hayashi A. Incidence of blepharoptosis after pars plana Baerveldt 350 glaucoma implant surgery by a single surgeon. Ophthalmic Plast Reconstr Surg. 2023;39(4):357–360. doi:10.1097/IOP.0000000000002319
5. Fukushima M, Yunoki T, Otsuka M, Hayashi A. Association of deepening of the upper eyelid sulcus with the incidence of blepharoptosis after glaucoma filtration surgery. Semin Ophthalmol. 2020;35(7–8):348–351. doi:10.1080/08820538.2020.1863435
6. Şen EM, Ceylanoğlu KS. Factors affecting the incidence of ptosis after trabeculectomy. Turk J Ophthalmol. 2023;53(2):85–90. doi:10.4274/tjo.galenos.2022.58812
7. Song MS, Shin DH, Spoor TC. Incidence of ptosis following trabeculectomy: a comparative study. Korean J Ophthalmol. 1996;10(2):97–103. doi:10.3341/kjo.1996.10.2.97
8. Koh V, Tatsios J, Chew PK, Amrith S. Comparison of incidence of ptosis after combined phacotrabeculectomy with mitomycin C and phacoemulsification. Indian J Ophthalmol. 2015;63(12):895–898. doi:10.4103/0301-4738.176032
9. Salvá-Palomeque T, Muñoz-Ramón P, Rebolleda G, Aguado-Casanova V, Ye-Zhu C, Muñoz-Negrete FJ. Changes in eyelid position after glaucoma filtering surgery. Eur J Ophthalmol. 2022;32(5):2886–2892. doi:10.1177/11206721211063723
10. Nilforushan N, Es’haghi A, Jafari S, et al. Postoperative blepharoptosis after trabeculectomy versus Ahmed glaucoma valve implantation. J Curr Ophthalmol. 2022;33(4):388–393. doi:10.4103/joco.joco_120_21
11. Roddy GW, Zhao B, Wang F, et al. Increased rate of ptosis following glaucoma drainage device placement and other anterior segment surgery: a prospective analysis. Graefes Arch Clin Exp Ophthalmol. 2020;258(7):1533–1541. doi:10.1007/s00417-020-04630-x
12. Shah M, Lee G, Lefebvre DR, et al. A cross-sectional survey of the association between bilateral topical prostaglandin analogue use and ocular adnexal features. PLoS One. 2013;8(5):e61638. doi:10.1371/journal.pone.0061638
13. Wang PX, Koh VT, Cheng JF. Periorbital muscle atrophy associated with topical bimatoprost therapy. Clin Ophthalmol. 2014;8:311–314. doi:10.2147/OPTH.S55754
14. Nakakura S, Yamamoto M, Terao E, et al. Prostaglandin-associated periorbitopathy in latanoprost users. Clin Ophthalmol. 2014;9:51–56. doi:10.2147/OPTH.S75651
15. Singh SK, Sekhar GC, Gupta S. Etiology of ptosis after cataract surgery. J Cataract Refract Surg. 1997;23(9):1409–1413. doi:10.1016/S0886-3350(97)80124-1
16. Bernardino CR, Rubin PA. Ptosis after cataract surgery. Semin Ophthalmol. 2002;17(3–4):144–148. doi:10.1076/soph.17.3.144.14782
17. Ropo A, Ruusuvaara P, Nikki P. Ptosis following periocular or general anaesthesia in cataract surgery. Acta Ophthalmol (Copenh). 1992;70(2):262–265. doi:10.1111/j.1755-3768.1992.tb04134.x
18. Kersten RC, de Conciliis C, Kulwin DR. Acquired ptosis in the young and middle-aged adult population. Ophthalmology. 1995;102(6):924–928. doi:10.1016/S0161-6420(95)30933-5
19. Epstein G, Putterman AM. Acquired blepharoptosis secondary to contact-lens wear. Am J Ophthalmol. 1981;91(5):634–639. doi:10.1016/0002-9394(81)90065-9
20. van den Bosch WA, Lemij HG. Blepharoptosis induced by prolonged hard contact lens wear. Ophthalmology. 1992;99(12):1759–1765. doi:10.1016/S0161-6420(92)31725-7
21. Cohen LM, Campbell BC, Esfandiari M, Goldberg RA, Rootman DB. Ophthalmic surgeries and systemic medical conditions associated with the development of involutional ptosis. Ophthalmic Plast Reconstr Surg. 2021;37(2):133–137. doi:10.1097/IOP.0000000000001707
22. Shirado M. Dyslipidaemia and age-related involutional blepharoptosis. J Plast Reconstr Aesthet Surg. 2012;65(6):e146–e150. doi:10.1016/j.bjps.2012.01.009
23. Kim MH, Cho J, Zhao D, et al. Prevalence and associated factors of blepharoptosis in Korean adult population: the Korea National Health and Nutrition Examination Survey 2008–2011. Eye. 2017;31(6):940–946. doi:10.1038/eye.2017.43
24. Paik JS, Jung SK, Han KD, Kim SD, Park YM, Yang SW. Obesity as a potential risk factor for blepharoptosis: the Korea National Health and Nutrition Examination Survey 2008–2010. PLoS One. 2015;10:e0131427.
25. Bosco D, Costa R, Plastino M, et al. Glucose metabolism in the idiopathic blepharoptosis: utility of the Oral Glucose Tolerance Test (OGTT) and of the Insulin Resistance Index. J Neurol Sci. 2009;284(1–2):24–28. doi:10.1016/j.jns.2009.03.017
26. Wang Y, Lou L, Liu Z, Ye J. Incidence and risk of ptosis following ocular surgery: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2019;257(2):397–404. doi:10.1007/s00417-018-4130-6
27. Godfrey KJ, Korn BS, Kikkawa DO. Blepharoptosis following ocular surgery: identifying risk factors. Curr Opin Ophthalmol. 2016;27(1):31–37. doi:10.1097/ICU.0000000000000218
28. Kim HW, Choi YJ, Lee KW, Lee MJ. Periorbital changes associated with prostaglandin analogs in Korean patients. BMC Ophthalmol. 2017;17(1):126. doi:10.1186/s12886-017-0521-4
29. Yoshino T, Fukuchi T, Togano T, Seki M, Ikegaki H, Abe H. Eyelid and eyelash changes due to prostaglandin analog therapy in unilateral treatment cases. Jpn J Ophthalmol. 2013;57(2):172–178. doi:10.1007/s10384-012-0199-3
30. Abdolalizadeh P, Kashkouli MB, Falavarjani KG, Karimi N, Khademi B, Sedaghat A. Postoperative Blepharoptosis After Pars Plana Vitrectomy Procedure. Ophthalmic Plast Reconstr Surg. 2021;37(5):431–434. doi:10.1097/IOP.0000000000001890
31. Pongsachareonnont P, Hemarat K, Panjaphongse R, Liu W, Vagefi MR, Stewart JM. Factors associated with the development of blepharoptosis after pars plana vitrectomy surgery. Semin Ophthalmol. 2022;37(4):509–514. doi:10.1080/08820538.2021.2006240
32. Crum AV, Bernardino CR. Preventing & managing post-surgical ptosis. 2010. Available from: https://www.reviewofophthalmology.com/article/preventing-managing-post-surgical-ptosis.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.