Back to Journals » International Journal of Women's Health » Volume 12
Evaluation of Pulmonary Function Tests Among Pregnant Women of Different Trimesters in Debre Berhan Referral Hospital, Shoa, Ethiopia
Received 6 August 2020
Accepted for publication 25 November 2020
Published 7 December 2020 Volume 2020:12 Pages 1135—1143
DOI https://doi.org/10.2147/IJWH.S275742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Yosef Eshetie Amare,1 Diresibachew Haile2
1Department of Biomedical Sciences, Institute of Medicine and Health Sciences, Debre Berhan University, Debre Berhan, Ethiopia; 2Department of Physiology, College of Medicine and Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Yosef Eshetie Amare
Department of Biomedical Sciences, Institute of Medicine and Health Sciences, Debre Berhan University, Ethiopia
Tel +251910966364
Email [email protected]
Introduction: Pregnancy is characterized by a sequence of dynamic physiological changes that impact multiple organ system functions and is associated with various changes in pulmonary anatomy and physiology. Precise knowledge of the pulmonary function test parameters helps to understand and manage the course and outcome of pregnancy leading to safe delivery. It also helps to avoid misdiagnosis and unnecessary interventions. The aim of this study was to evaluate the effect of normal pregnancy on pulmonary function tests among pregnant women in Debre Berhan Referral Hospital, Ethiopia.
Methods: A total of 176 study participants (first, second, and third trimester; and control) were involved under a comparative cross-sectional study design and convenience sampling technique. Anthropometric data, oxygen saturation of arterial blood, and pulmonary function tests were measured. Data were tabulated and statistically analyzed using SPSS version 20.0 statistical software. Means of all parameters were compared using one-way ANOVA followed by Tukey’s post hoc multiple comparison test. Statistical significance was preset at a p-value of less than 0.05.
Results: Mean of FVC for the controls, first, second, and third trimesters was 2.59 ± 0.26, 2.13 ± 0.15, 1.93 ± 0.27, and 1.90 ± 0.11 liters, respectively. Except for FEV1%, the mean values of FVC, FEV1, PEFR, and FEF 25– 75% in the pregnant group (all the three trimesters) were significantly decreased from the controls (P< 0.05). Strong negative correlation was seen between SaO2 and RR (r= − 0.865; P < 0.01). As the pregnancy progressed from first to the third trimester, dynamic pulmonary function tests (FVC, FEV1, FEF25-75%, and PEFR) were dropped and the respiratory rate increased.
Conclusion: The results had shown the tendency of obstructive pattern while pregnancy becoming advanced. We have observed also a remarkable decline of SaO2 in pregnant women that might be counterbalanced by raised respiratory rate.
Keywords: pregnancy, high altitude, FVC, trimester, oxygen saturation
Background
Pregnancy causes physiological and anatomical changes in different body systems.1–3 The physiological changes occurring in a pregnant woman are vast and widespread. These include changes in genital organs, an increase in breast size, weight gain, and other systemic alterations including respiratory, cardiovascular, body water metabolism, hematological, and metabolic changes.4 These adaptations are necessary to meet the increased metabolic demands of the mother and the fetus.
The combination of hormonal changes and mechanical effects of the enlarging uterus leads to a change in the pulmonary physiology of a mother.1,5 Progressively enlarging uterus causes a diaphragm position to rise approximately 4 cm above its usual resting position that favors the lung to hold less air.6 As a result, lung volumes are compromised including functional residual capacity (FRC), total lung capacity (TLC), and vital capacity (VC).7,8 Dynamic pulmonary function tests like FVC, FEV1, FEV1%, and FEF25-75% also decrease due to the gravid state of advanced pregnancy.1,2
Besides the size of the gravid uterus, many of the physiological changes in the respiratory system are mediated by increased progesterone levels.9 Progesterone is a known stimulant of breathing, and its level in the blood gradually rises approximately from 25 ng/mL at six weeks of gestation to 150 ng/mL at term.10,11 This progressive increment is responsible for the raised respiratory depth and rate.12,13 Progesterone increases tidal volume by 200mL (from 500mL to 700mL) and minute-ventilation approximately by 40%. This is by increasing the sensitivity of the respiratory center to carbon dioxide. Progesterone-mediated hypersensitivity to CO2 increases the respiratory rate by 10% which attributes to the raised oxygen consumption during pregnancy.13 It also causes a fall in the functional residual capacity that comprises residual and expiratory reserve volume. As a consequence, alveolar ventilation increases.3 Total lung capacity is minimally decreased because of the reduction in residual volume.13 Moreover, pregnancy-induced elevated progesterone causes bronchial and tracheal smooth muscle relaxation. Therefore, the upward displacement of the diaphragm along with reduced strength of expiratory muscles may hamper forceful expiration.5 Progesterone increases respiratory rate and tidal volume which in turn drives an increment of both alveolar and minute ventilation and hence a fall in PaCO2.7,9,14 PaCO2 might reach to a mean of 20–30 mmHg in the last 12 weeks of pregnancy,6 resulting in constriction of bronchial smooth muscle.5 Even, progesterone accompanies reduced chest wall compliance through structural changes in the ribcage and abdominal compartments.15
At high altitude, PaO2 in the atmosphere falls thereby the number of molecules of O2 present per breath decreases that leads to hypobaric hypoxia and this would be more pronounced during pregnancy.16,17 Moreover, ventilation has a positive correlation with the consumed energy cost and also, the power and endurance of respiratory muscles which have basic roles for ventilation activity.16 This has been shown by the fatigue of diaphragmatic muscle that may affect breathing at high altitude. Ventilatory studies at high altitudes have shown decreased forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), and maximal mid expiratory flow rate (FEF25-75%).16,18
Over breathing is one of the many physiological adaptations of pregnancy which is made considerably in the progress of maternal and fetal possible needs. The increase in minute ventilation that accompanies pregnancy is often perceived as shortness of breath. About 75% of pregnant women have exertional dyspnea by 30 weeks of gestation. Shortness of breath at rest or with mild exertion is so common that it is often referred to as physiologic dyspnea and is completely reversible once pregnancy is over.4,15 Understanding of the changes is critical in distinguishing the common dyspnea that occurs during normal pregnancy from pathophysiologic states associated with cardiopulmonary diseases seen in pregnancy and anticipating disease worsening conditions during pregnancy in those women with cardiopulmonary diseases.1
Therefore, accurate knowledge of the physiological changes in pulmonary functions during normal pregnancy is necessary. In Ethiopia, there are few published findings on pulmonary function tests among pregnant women at altitude. Knowledge of predicted changes in the respiratory system associated with pregnancy helps clinicians to prevent misdiagnosis of physiological changes as pathological. Thus, the present study focused on the evaluation of pulmonary function tests among pregnant women of the different trimesters in Debre Berhan Referral Hospital, Shoa, Ethiopia.
Materials and Methods
Study Area
This study was carried out at Debre Berhan Referral Hospital. Debre Berhan is located in the North Shoa Zone of the Amhara Region, about 130 kilometers North East of Addis Ababa at an average altitude of 2840 meters above sea level.
Study Design and Period
The comparative cross-sectional study design was employed to assess the effect of normal pregnancy on pulmonary function outcomes among pregnant women who visited the ANC clinic of Debre Berhan Referral Hospital from January to March 2019. Non-pregnant women who came for family planning services were taken as controls. One hundred and seventy-six study participants were recruited and divided equally into four groups, each comprising 44 women. The groups include those in their first, second, and third trimesters, and also the non-pregnant women as controls.
Source Population
All pregnant and non-pregnant women in Debre Berhan town, North Shoa Zone, Amara region, Ethiopia.
Study Population
All pregnant women who visited the ANC clinic, and non-pregnant women who visited the family planning clinic of Debre Berhan referral Hospital.
Inclusion Criteria
Healthy pregnant women who were volunteered to participate in the study. And, those clients came to use either of any family planning method.
Exclusion Criteria
Those participants who had a history of (smoking, general debility, recurrent or persistent expectoration, asthma or recurrent bronchitis, occupational exposure to lung toxins, having diabetes mellitus, any current or past cardiovascular or respiratory disorder) and with the sign of any bone deformity of the thoracic cage were excluded from the study.
Operational Definition
First Trimester
Designates gestational age from 1–12 weeks; Second Trimester: Designates gestational age from 13–26 weeks; Third Trimester: Designates gestational age from 27–40+ weeks; Control: Non-pregnant women they came for utilization of family planning service.
High Altitude
It is an elevation of between 1500m to 3500m above sea level.19
FVC: The volume of air that can forcibly be blown out after maximum inspiration; FEV1: This is the speed of air forcibly expelled from the lungs in the first one second from maximal inspiration; FEV1%: The percentage of the FVC expired in the first one second of maximal forced expiration following full inspiration; FEF25-75%: Indicates expiratory flow in the middle portion of the FVC; PEFR: The highest flow achieved from maximal lung inflation and forced expiration.20
Sample Size Determination
The sample size was determined by considering the following assumptions: α (two-sided) = 0.05; power = 0.80; effect size = 2.6; SD = 8.7, and the total sample size was becoming 176 mothers. These 176 mothers were purposely allocated into four groups each containing 44 mothers (first trimester, second trimester, third trimester, and controls).
Sampling Procedure and Technique
All the women who visit the ANC and family planning clinic of Debre Berhan referral Hospital were considered. Those pregnant and non-pregnant women that fulfilling inclusion criteria were included through convince sampling.
Data Collection Tools and Process
Height and weight measuring scale, Spiropro handheld spirometer with extra pneumotachometer with mouthpiece (Jaeger, digital Spiropro, 150×9×40 mm, 0.2kg, rechargeable, and touch sensitive display), and pulse oximetry (Oxi-Max N-65) were used. The height was taken in centimeters (nearest to 0.1 cm) without shoes, feet together, standing as tall as possible with the eye level and looking straight ahead, and using an accurate measuring device. Weight was also measured in kilograms (nearest to 0.1 kg) of the subject wearing light clothing and barefooted on the weighing scale. The PFTs were measured with a spirometer under recommendations of the American Thoracic Society (ATS) at room temperature by the same investigator to ensure its validity. Before each measurement, the spirometer was calibrated by a volume of 1 liter syringe. Following receipt of consent, the study participants rested for 15 minutes before measurements and the investigator informed study participants about the whole procedure and allowed to do multiple trials before the start of the experiment to familiarize the subjects with the test procedures. The study participants were asked to sit comfortably in a chair. After appropriate placement of the nose clip, they were instructed to seal the lips around the sterile mouthpiece. The study participant was asked to breathe in maximally and then forcefully expire the air, as fast and as far as possible. Each participant performed the test at least three times, as per the requirement of ATS so that at least two of the maneuvers were reproducible. In some cases, the tests were made more than three times, when the participant failed to produce reliable value. Maternal SaO2 is also measured in the sitting position at the dominant index finger. Respiratory rate was recorded by inspection and palpation on the chest and abdomen.
Data Quality Control
To assure the quality of the data, the following measures were undertaken. Training has been given to data collectors about the objective of the study, data collection procedures, and relevance of the study before actual data collection. The principal investigator was actively involved in supervising data collection and checking the completeness of the sheet daily. The collected data were reviewed before entry. The spirometer was regularly checked for ambient conditions (temperature of 17–20°C, 65–74% humidity, and a barometric pressure of 1018–1025 hPa).
Data Processing and Analysis
Data were coded, entered, and cleaned after checking for completeness and consistencies. SPSS version 20.0 statistical software package was used for analysis. Mean ± SD of all study groups were compared for statistical significance by independent “t” test and one-way ANOVA. Statistical significance was preset at P< 0.05.
Ethical Considerations
Ethical approval was obtained from the Ethical Review Committee of the Department of Physiology, Addis Ababa University. Full information was given to participants on the purpose and significance of the study. The informed and written consent was then obtained from all participants and it was conducted in accordance with the declaration of Helsinki.32
Result
Characteristics of Study Participants
A total of 176 study participants were involved in this study. Out of these, 132 were pregnant women correspondingly allocated to each trimester and the rest were 44 controls. Anthropometric measurements, respiratory rate, oxygen saturation of arterial blood, and dynamic pulmonary function tests were measured for all 176 individuals.
The mean age of first, second, third trimesters; and control were (24.41 ± 2.34, 25.02 ± 2.31, 25.07 ± 3.17, and 24.36 ± 1.57 years) respectively (Figure 1). An insignificant difference of age was seen in all groups.
 |
Figure 1 Mean age of study participants in Debre Berhan Referral Hospital, January to March 2019. |
When comparing the anthropometric measurements of each group; the height of third-trimester women was significantly (P < 0.01) higher than the control group. The weight of all trimesters increased significantly (P < 0.01) when compared to the control group. The BMI of the first-trimester group did not show significant variation when compared to the control group. But, it was increased substantially in the second and third trimesters (P < 0.01). BMI across all study groups lied within a normal range.
Assessing Arterial Blood Oxygen Saturation and Respiratory Rate of Study Participants
The mean respiratory rate was significantly increased in all trimesters as compared to the control group. Likewise, arterial blood oxygen saturation of pregnant women was significantly decreased when compared to the control group (Table 2). The respiratory rate of pregnant women was showing increasing pattern as gestational age rises. However, arterial blood oxygen saturation was significantly dropping as gestational age upsurges. The arterial blood oxygen saturation and respiratory rate of study participants have revealed a strong negative correlation (p<0.01, r = - 0.865) (Figure 2).
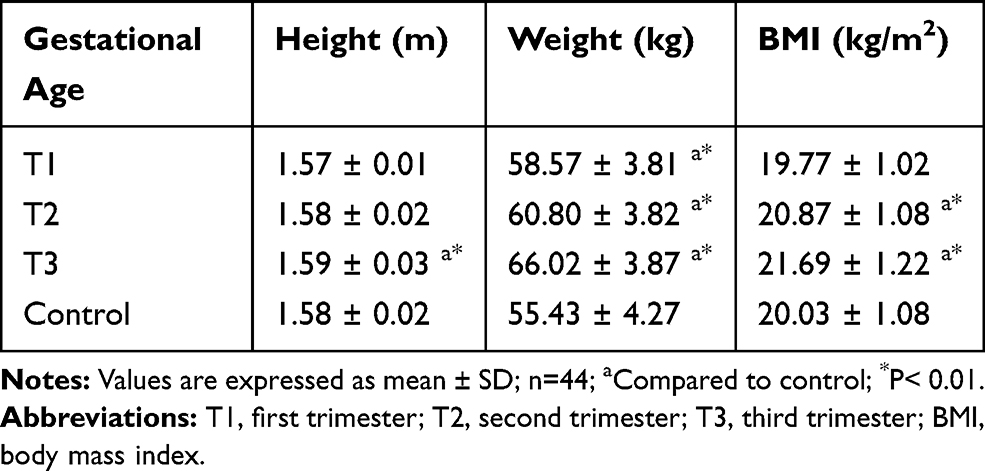 |
Table 1 Comparison of Anthropometric Measurements of Study Participants in Debre Berhan Referral Hospital, January to March 2019 |
 |
Table 2 Mean of Arterial Blood Oxygen Saturation and Respiratory Rate of Study Participants in Debre Berhan Referral Hospital, January to March 2019 |
 |
Figure 2 Correlation between mean arterial blood oxygen saturation and respiratory rate of study participants in Debre Berhan Referral Hospital, January to March 2019. |
Assessing Dynamic Pulmonary Function Testes
As presented in Table 3, the parameters of PFTs were compared across each group. Comparing first trimester and second-trimester pregnant women, the mean of FEV1%, FEF25-75%, and PEFR did not show a significant difference. Meanwhile, the mean FVC (P <0.05) and FEV1 (P < 0.01) of first trimester women have shown significant increment when compared to second-trimester women. Except for unchanged FEV1% mean value, other PFTs parameters were significantly (P < 0.01) decreased in third-trimester women when compared to first trimester women. Mean values of PFTs parameters of the control group were significantly (P < 0.01) increased when compared to all the groups of pregnant women; except, FEV1% remained insignificant.
 |
Table 3 Comparison of Mean PFTs Across Pregnant Women of Each Trimester and Control in Debre Berhan Referral Hospital, January to March 2019 |
Discussion
In this study, the mean difference in age and height of pregnant women were statistically insignificant as compared to the control group. This is in agreement with previous finding.1,5,7,21,22 Hence, possible variation in indices of PFTs due to age and height would not be a factor for this study. The difference in mean weight and BMI was statistically significant amongst pregnant and control groups. The present study showed that both weight and BMI were increased significantly per the rising of gestational age (Table 1). Other studies revealed the same result.1 This might be because of the normal weight gain, and uterine enlargement which occurs in pregnancy.
Our study showed that the mean RR was significantly increased from the first trimester to the third trimester which is in agreement with several studies.11,21,23 Likewise, the mean RR of the control group was markedly decreased when compared to all the three trimesters (Table 1). Other studies also reported a 10%,9 and borderline increment of RR during pregnancy.4 This might be due to the increasing pattern of progesterone; from 25 ng/mL at 6 weeks of gestation to 150 ng/mL at term thereby triggering the primary respiratory center by increasing the sensitivity of the respiratory center to carbon dioxide.10,11 Furthermore, gestational hyperventilation is attributed to upward displacement of the diaphragm, hypervolemia, increased cardiac output, and increased demand a growing fetus.21 However, another study reported no change in respiratory rate during pregnancy.24 This is probably, because, sometimes increase in ventilation occurs without an increase in respiratory rate; and accomplished mainly by a rise in tidal volume only.
This study found a strong negative correlation between RR and SaO2 (P< 0.01; r = - 0.865). This can be due to the considerable reduction in the partial pressure of oxygen in Debre Berhan as compared to sea level which can trigger a compensatory rise in respiratory rate.
In the present study, the mean arterial blood oxygen saturation was significantly dropped as gestational age increased while the mean SaO2 of the control group became higher (Table 2). Previous studies have shown similar findings.25 However, increased SaO2 with advanced gestation,23 and unchanged mean SaO2 (~97%),7,26 were reported. The reduced SaO2 for Debre Berhan pregnant women might be due to diminished partial pressure of oxygen which reduces alveolar oxygen tension. Other possible reasons could also due to the increment of maternal plasma volume by 45%, and red blood cell mass by 20–30% during pregnancy. In the meantime, this disproportionate increment of plasma volume with red blood cell mass might cause arterial oxygen to be dissolved more and then unable to be detected by pulse oximetry easily.27
The Mean FEV1 of all the three trimesters was found to be significantly decreased as compared to the control group. Previous studies support our findings.1,2,5,7,11 In other studies, however, FEV1 was significantly reduced only in the third trimester while it was showing an insignificant difference between the first and second trimester when compared to the control group.28
Our study found an insignificant difference in mean FEV1% between pregnant and non-pregnant control groups which is consistent with other similar studies.29 Unlike our results, a substantial decline of FEV1% was reported by numerous studies.2,11,28 Other findings also stated that raised FEV1% in all trimesters as compared to non-pregnant counterparts.7 The mean FEV1% of second and third-trimester pregnant women was slightly decreased as compared to non-pregnant women.1 The present study revealed that mean FVC in the third trimester significantly reduced when compared to the control group; which was in agreement with others.5,7,22 The decrease in FVC is attributable to the mechanical pressure of enlarging gravid uterus, elevating the diaphragm, and restricting the movements of lungs that hamper the forceful expiration. The current study implied a significant decrease in mean FEF25-75% in all the trimesters of pregnancy as compared to the control group, and a similar result was reported.2 The reductions in FEF25-75% might be due to reduced lung volumes as the pregnancy is getting advanced.9
In our study, the mean FVC, FEV1, and FEF25%-75% of the third-trimester pregnant women significantly decreased as compared to the control group. This finding was comparable with other studies.1,21,22 The present study revealed that persistent mean FEV1% throughout pregnancy. This might be due to a proportional decrement of FEV1 and FVC thereby the ratio of FEV1/FVC has appeared like unity. In contrast, the sustained mean values of FVC, FEV1, and FEV1% were presented from first to the third trimester.7 However, another study described a definite increase of FEV1% due to less drop in FEV1 as compared to FVC.22
In line with ours, studies reported a significant fall in FEV1 of the third trimester as compared to the first trimester.5,28 However, other studies found a highly significant decrease in FEV1 and FEF25-75% in the first trimester than the third trimester.2,11
We found that significantly lower mean PEFR values in pregnant women as compared to the non-pregnant control which is in agreement with several studies.1,5,7,11 Other findings, however, accounted for no substantial change in PEFR in the first and second trimester except that a significant decrease in the third trimester.4 Other complementary studies found a significant decrease in PEFR only in the third trimester.21,22 Our findings showed an extensive drop in PEFR for each trimester as compared to the control group. The decrease in mean PEFR may be attributed to the lesser force of contraction of main expiratory muscles or could be due to the mechanical effect of enlarging gravid uterus affecting the vertical dimension by restricting the diaphragmatic movement. In line with the current study, several researchers reported a progressive decline in PEFR as gestation advanced from the first to third trimester.4,5,7,30 A maximum decrease of PEFR was documented in the first trimester which may be attributable to hormonal changes.11 However, in this study, PEFR was highly dropped in the third trimester. This is probably because the PEFR maneuver involves a muscular element that is negatively affected due to the downward displacement of the diaphragm around full-term pregnancy.31
Conclusion
During pregnancy, the mean of respiratory parameters declines as gestational age progresses from first to the third trimester. Moreover, mean PFTs of each trimester of pregnancy significantly reduced when compared to non-pregnant controls. Except for FEV1% other pulmonary function tests including FVC, FEV1, PEFR, and FEF25-75% decreased significantly. Thus the present study concluded PFTs of pregnant women would show a tendency of restrictive pattern. These outcomes might arise from a combination of hormonal changes and mechanical adjustments of the enlarging uterus that has a significant effect on the pulmonary physiology of the pregnant mother. It was also concluded that the raised respiratory rate would happen when gestational age increased. On the other hand, oxygen saturation of arterial blood declined as pregnancy advances. These alterations are compulsory to meet the increased metabolic demands of the mother and fetus. Therefore, the present study concluded that pregnancy at altitude can bring about compensatory changes to balance with the changes occurring in dynamic pulmonary function tests. However, longitudinal studies may reveal better results with larger sample sizes; therefore, future studies need to be done with large sample size and longitudinal studies taking parity, chest size, type of pregnancy, and other socioeconomic factors into consideration.
Abbreviations
AAU, Addis Ababa University; ANC, Antenatal Care; ANOVA, Analysis of Variance; ATS, American Thoracic Society; BMI, Body Mass Index; CI, Confidence Interval; cm, Centimeter; CO2, Carbon Dioxide; COPD, Chronic Obstructive Pulmonary Disease; FEF25-75%, Forced Expiratory Flow Rate at the Middle Part of FVC; FEV1, Forced Expiratory Volume in one Second; FEV1%, FEV1 to FVC ratio x 100; FVC, Forced Vital Capacity; L/s, Liter per Second; PaCO2, Partial Pressure of Carbon Dioxide; PaO2, Partial Pressure of Oxygen; PEFR, Peak Expiratory Flow Rate; PFTs, Pulmonary Function Tests; RR, Respiratory Rate; SaO2, Oxygen Saturation of Arterial Blood; SD, Standard Deviation.
Data Sharing Statement
All used raw data are available and can be accessed when reasonably requested.
Ethical Approval
The proposal was approved by the Ethical Review Committee of the Department of Physiology, Addis Ababa University before the beginning of the study.
Acknowledgment
The authors express thanks to all participants who willingly helped us. We would also like to thank the College of Medicine and Health Sciences, Addis Ababa University for financial support.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Addis Ababa University, Addis Ababa, Ethiopia.
Disclosure
The authors report no conflicts of interest for this work, the authorship, and publication of this article.
References
1. Biswas D, Kulsange S. Effect of normal pregnancy on pulmonary function tests in a rural setting. Int J Physiol. 2013;1(2):27–32. doi:10.5958/j.2320-608X.1.2.006
2. Teli A, Doddamani P, Ghatnatti R, et al. Physiological alternation in small airway parameters during pregnancy: its application in clinical scenario. Int J Biomed Res. 2013;4(4):173–178. doi:10.7439/ijbr.v4i4.239
3. Carlin A, Alfirevic Z. Physiological changes of pregnancy and monitoring. Best Pract Res Clin Obstet Gynaecol. 2008;22(5):801–823. doi:10.1016/j.bpobgyn.2008.06.005
4. Omorogiuwa A, Iyawe V. Effect of parity on FVC and FEV1 during pregnancy. J Adv Med Med Res. 2015;1–9.
5. Jadhav S, et al. Comparative study of pulmonary function tests on different trimesters of pregnancy. Int J Current Res Rev. 2013;5(2):118.
6. Ratigan T. Anatomic and physiologic changes of pregnancy: anesthetic considerations. AANA J. 1983;51(1):38–42.
7. Richlin S, Cusick W, Sullivan C, et al. Normative oxygen saturation values for pregnant women at sea level. Prim Care Update Ob Gyns. 1998;5(4):154–155. doi:10.1016/S1068-607X(98)00042-0
8. Pandey D, Garg D, Tripathi B, et al. Case report: dyspnea in pregnancy: an unusual cause. J Basic Clin Reproductive Sci. 2014;3(1):68–70. doi:10.4103/2278-960X.129290
9. Heidemann BH, McClure JH. Changes in maternal physiology during pregnancy. BJA CEPD Rev. 2003;3(3):65–68. doi:10.1093/bjacepd/mkg065
10. LoMauro A, Aliverti A. Respiratory physiology of pregnancy: physiology masterclass. Breathe. 2015;11(4):297–301. doi:10.1183/20734735.008615
11. Teli A, Dharwadkar A, Aithala M. A study of pulmonary functions of women at different trimesters of pregnancy in Bldeu’s Shri Bm Patil Medical College Hospital. Analytica Medica. 2010;13:28.
12. Cebakulu S. From Dyspnoea to Respiratory Failure in Pregnancy. In Obstetrics and Gynaecology Forum. House Publications; 2014.
13. Yeomans ER, Gilstrap LC. Physiologic changes in pregnancy and their impact on critical care. Crit Care Med. 2005;33(10):S256–S258. doi:10.1097/01.CCM.0000183540.69405.90
14. Bhatia P, Bhatia K. Pregnancy and the lungs. Postgrad Med J. 2000;76(901):683–689. doi:10.1136/pmj.76.901.683
15. Hegewald MJ, Crapo RO. Respiratory physiology in pregnancy. Clin Chest Med. 2011;32(1):1–13. doi:10.1016/j.ccm.2010.11.001
16. Chawla S, Saxena S. Physiology of high-altitude acclimatization. Resonance. 2014;19(6):538–548. doi:10.1007/s12045-014-0057-3
17. San T, Polat S, Cingi C, et al. Effects of high altitude on sleep and respiratory system and theirs adaptations. Scientific World J. 2013;2013. doi:10.1155/2013/241569
18. Zada W, Aydin, Framushi. Comparison of pulmonary function parameters changes at different altitudes in female athletes. Available from: https://repository.uma.ac.ir/id/eprint/7943. 2009.
19. Taylor AT. High-altitude illnesses: physiology, risk factors, prevention, and treatment. Rambam Maimonides Med j. 2011;2:1. doi:10.5041/RMMJ.10022
20. West JB. Respiratory Physiology: The Essentials. Lippincott Williams & Wilkins; 2012.
21. Panchal V, Dodiya D. Comparative study of dynamic lung function tests between third trimester of pregnancy and non-pregnant women. Int J Res Med. 2014;3(2):158–169.
22. Kaur V. Effect of advanced uncomplicated pregnancy on pulmonary function parameters of North Indian subjects. Indian J Physiol Pharmacol. 2010;54(1):69–72.
23. Haile D, Abebe Y. Trends of lung function indices, arterial blood oxygen saturation and pulse rate among the first and third trimester pregnant women in Addis Ababa, Ethiopia. Ethiopian JReproductive Health. 2016;8:1.
24. Shailaja D, Srikanth D. Lung function tests in different trimesters of pregnancy. Indian J Basic Appl Med Res. 2013;3(1):285–292.
25. Yanamandra N, Chandraharan E. Anatomical and physiological changes in pregnancy and their implications. Obstetric Intrapartum Emergencies. 2012;1.
26. Van Hook J, Harvey CJ, Anderson GD. Effect of pregnancy on maternal oxygen saturation values: use of reflectance pulse oximetry during pregnancy. South Med J. 1996;89(12):1188–1192. doi:10.1097/00007611-199612000-00011
27. Branch DW, Wong LF. Normal Pregnancy, Pregnancy Complications, and Obstetric Management, in Contraception and Pregnancy in Patients with Rheumatic Disease. Springer; 2014:31–62.
28. Sunyal DK, et al. Study of forced expiratory volume in first second (FEV1) and ratio of forced expiratory volume in first second and forced vital capacity in percentage (FEV1/FVC%) in pregnant women. J Enam Med College. 2012;2(1):29–32. doi:10.3329/jemc.v2i1.11926
29. Phatak MS, Kurhade G. Short communication a longitudinal study of antenatal changes in lung function tests and importance of postpartum exercises in their recovery. Indian J Physiol Pharmacol. 2003;47(3):352–356.
30. Bansal M, et al. Longitudinal study of peak expiratory flow rate in pregnant women. NJIRM. 2012;3(1):34–38.
31. Pradhan G, et al. Evaluation and comparison of lung function parameters during pregnancy. Int J Current Res Rev. 2014;6(7):35.
32. World Medical Association. World Medical Association declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull World Health Organ. 2001;79(4):373–374. World Health Organization.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.