Back to Journals » Clinical Interventions in Aging » Volume 20
Evaluation of Potential Drug–Drug Interactions, Polypharmacy, and Prescribing Patterns of NSAIDs Among the Older Adults in a Secondary Care Setting
Authors Shareef J ![]() , Sridhar SB, Saeed ZM, Alsereidi AMR
, Sridhar SB, Saeed ZM, Alsereidi AMR
Received 18 June 2025
Accepted for publication 10 October 2025
Published 5 November 2025 Volume 2025:20 Pages 1875—1894
DOI https://doi.org/10.2147/CIA.S545906
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Javedh Shareef,1 Sathvik Belagodu Sridhar,1 Zainab Mohammed Saeed,1 Amal Mohammed Rashed Alsereidi1,2
1Department of Clinical Pharmacy & Pharmacology, Ras Al Khaimah College of Pharmacy, Ras Al Khaimah Medical & Health Sciences University, Ras Al Khaimah, United Arab Emirates; 2Clinical Pharmacy Department, Dibba Hospital, Emirates Health Services, Al Fujairah, United Arab Emirates
Correspondence: Javedh Shareef; Sathvik Belagodu Sridhar, Department of Clinical Pharmacy & Pharmacology, Ras Al Khaimah College of Pharmacy, Ras Al Khaimah Medical & Health Sciences University, Ras Al Khaimah, United Arab Emirates, Tel +971565915310, Email [email protected]; [email protected]
Purpose: In clinical practice, non-steroidal anti-inflammatory drugs (NSAIDs) are widely prescribed to older adults patients for pain and inflammation. However, drug therapy in this population carries risks of polypharmacy and potential drug–drug interactions (pDDIs). This study aimed to evaluate prescribing trends of NSAIDs and examine the incidence of polypharmacy and pDDIs among older adults patients in the Outpatient Pharmacy Department of a secondary care hospital.
Patients and Methods: A prospective observational study was conducted using electronic health records of older adults patients prescribed NSAIDs from January to June 2023. Data were screened for NSAID prescription patterns, polypharmacy, and pDDIs using the Micromedex database. Descriptive statistics and logistic regression assessed relationships between treatment-related factors and pDDIs, while Chi-square tested associations between NSAID prescriptions and gastro-protective drugs. A p-value < 0.05 was considered statistically significant.
Results: The study was conducted in 174 older adults patients. Celecoxib (28.2%) and ketoprofen (27.6%) were the most often given oral and topical NSAIDs among the study populations, respectively. Aspirin and celecoxib were the most commonly involved NSAIDs causing pDDIs. A total of 340 potential pDDIs were found, with a mean of 1.95 ± 3.66 interactions for each prescription. The analysis of polypharmacy in relation to treatment factors revealed a significant correlation with comorbidities (p < 0.001). A robust positive association exists between the quantity of pDDIs and continuous treatment-related factors, including the Charlson comorbidity index (p = 0.004), the comorbidity burden (p < 0.001), and the overall number of medications being taken (p < 0.001).
Conclusion: The research elucidates the prescribing trends of NSAIDs and uncovers the occurrence of polypharmacy and pDDIs within the older adults population. Giving the right screening and intervention resources to maximize their medication regimen may ensure safer and more effective management of older adults patients.
Plain Language Summary: Doctors often give older people NSAIDs (non-steroidal anti-inflammatory meds) to help with pain and swelling. But as people get older, they are more likely to be given more than one medicine at a time, which is called polypharmacy. Taking many drugs raises the chance of bad side effects, especially when several drugs interact in harmful ways. These are known as possible drug-drug interactions (pDDIs).
This study looked at how NSAIDs are given to older people who go to a secondary care hospital’s outpatient pharmacy. Researchers got information from people 60 and older who were given NSAIDs between January and June 2023. The study examined which NSAIDs were most commonly used, how many patients were taking more than one medication, and how often pDDIs happened. We used a medical database called Micromedex to identify the interactions.
There were 174 senior patients in the study. Celecoxib (oral) and ketoprofen (topical gel) were the NSAIDs doctors prescribed most. Aspirin and celecoxib were the NSAIDs that most often interacted with other drugs. There were 340 pDDIs in all, averaging over two per prescription. The results showed that patients who used more medications and had greater health problems were more likely to have pDDIs.
The study shows that older persons need to be watched closely and that doctors should be more careful when giving drugs. Better screening and advice for doctors and pharmacists could help lower risks and make patients safer.
Keywords: older adults, prescription pattern, poly pharmacy, drug-drug interactions, non-steroidal anti-inflammatory drugs
Introduction
The field of medicine known as geriatrics focuses on the healthcare of older adults individuals, defined as those aged 65 years and older.1 This demographic constitutes an increasingly significant segment of the global population. Projections indicate that by 2050, the proportion of older individuals worldwide is expected to reach 22%.2 In the Arab region specifically, experts predict that the older adults population will reach 49.6 million by 2030, representing 9.5% of the total population. Furthermore, this figure is expected to surpass 102 million by 2050, with older adults comprising 15.1% of the population.3 As life expectancy increases and healthcare advances extend longevity, understanding and addressing the unique healthcare needs of older adults becomes paramount.2,4
Among the various challenges encountered by this demographic, the judicious use of pharmacological agents, especially non-steroidal anti-inflammatory drugs (NSAIDs), plays a crucial role in managing common conditions, ranging from mild pain to chronic inflammatory conditions such as arthritis and musculoskeletal disorders.5 They account for almost 20% of all prescription drug usage and are the most widely utilized class of pharmaceuticals globally. Due to their easy availability as over-the-counter drugs, studies have shown that approximately 30 million people worldwide consume NSAIDs daily, of whom 40% are older than 60 years.6 Previous studies also report the inappropriate prescribing or irrational use of NSAIDs, thereby having the potential to cause serious adverse effects, including elevated blood pressure, heart disease, kidney damage, and gastrointestinal (GI) problems.7,8 The widespread prescription of these medications can be attributed to their effectiveness in managing symptoms. Nonetheless, their application among older adults requires meticulous evaluation, given the common occurrence of comorbidities and age-related physiological alterations. These factors often necessitate the simultaneous administration of multiple medications, a phenomenon known as polypharmacy.5,9
“Polypharmacy (PP) is defined by the World Health Organization (WHO) as the simultaneous use of many medications or as the routine use of five or more medications”. Despite the WHO endorsing a criterion of ≤5 per day, the assessment of PP remains a contentious issue.10,11 Numerous older adults with chronic illnesses frequently have multiple concurrent medical problems. Prescribing several drugs enables healthcare providers to thoroughly address each ailment, enhancing overall illness management and quality of life.12 Nonetheless, numerous drugs exacerbate the risk of polypharmacy in the older adults, correlating with incorrect prescribing, heightened risks of drug-related complications, and increased hospitalizations. [10] Furthermore, the intricacy of polypharmacy heightens the probability of drug-drug interactions (DDIs), wherein the synergistic effects of drugs may lead to undesired outcomes, including therapeutic failure and toxicity.13
DDIs are more common in older adults people because of age-related physiological changes and concurrent usage of various drugs. These interactions may result in altered medication efficacy, increased toxicity, and compromised therapeutic outcomes.14 According to epidemiological research, the prevalence rates of clinically relevant DDIs vary greatly throughout healthcare settings, and older patients with multimorbidity are particularly prone to them. Age, comorbidities, dietary condition, genetic predispositions, and the sheer volume of prescribed medications are some of the factors that lead to DDIs.15,16 Understanding and mitigating drug-drug interactions (DDIs) is crucial to optimizing pharmacotherapy and enhancing patient safety in geriatric populations.
Despite these risks, there is a paucity of comprehensive studies examining NSAID prescribing practices, the incidence of polypharmacy, and pDDIs, particularly within the demographic of older adults receiving care in secondary hospital settings. Addressing these deficiencies is crucial for improving patient outcomes and optimizing healthcare resource utilization among older adults populations, as well as for enhancing pharmacological safety and efficacy. In light of these findings, the present study aimed to evaluate the prescribing practices of NSAIDs and to investigate the prevalence of polypharmacy and pDDIs among older adults patients who are prescribed NSAIDs within the outpatient pharmacy department of a secondary care hospital.
Materials and Methods
Study Design and Study Setting
A prospective observational study was conducted in the outpatient pharmacy department at Dibba Hospital in Al Fujairah, United Arab Emirates, from January 2023 to June 2023.
Ethical Consideration
The research proposal has received approval from the Institutional Review Board – Ras Al Khaimah Medical and Health Sciences University, designated as [RAKMHSU-REC-031-2022/23-PG-P], as well as from the Regional Research and Ethics Committee of Ras Al Khaimah, Ministry of Health and Prevention, UAE, identified by the reference number [MOHAP/REC/2022/36-2022-PG-P]. This study was conducted by relevant regulations and legal frameworks, including adherence to the principles outlined in the Declaration of Helsinki. All participants were recruited after providing written informed consent using a standardized form that explained the study objectives, data confidentiality, and the voluntary nature of participation.
Sample Size and Sampling Technique
The sample size was calculated a prioriusing Epi Info™ version 7.2 software (CDC, Atlanta, USA). The standard formula for single population proportion was applied:

Where:
- n = required sample size
- Z = Z-value at 95% confidence level (1.96)
- P = expected proportion of polypharmacy/pDDIs (set at 0.5 for maximum sample size since no prior local data were available)
- d = margin of error (0.05)
This yielded a sample size of 170 participants, which was used as the study target. To select the study participants, a systematic random sampling method was implemented.
Inclusion and Exclusion Criteria
All patients, regardless of gender, who are 65 years of age or older and prescribed at least one systemic NSAID in conjunction with other drugs, registered in the outpatient departments of the study setting, and who consent to participate in the trial. Hospitalized older adults patients, critical care unit, and emergency department, as well as those prescribed predominantly lotions, ointments, and compounded products, and whose data are insufficient or inadequately documented in their case records, were eliminated from the study.
Study Procedure
The study included prescription records for all patients who fulfilled the specified inclusion criteria. Patient parameters, including name, age, gender, diagnosis (International Classification of Diseases, Tenth Revision, ICD-10), co-morbid conditions, medication history, and duration of hospitalization, along with prescribed medications, were extracted from the electronic health records (Wareed system) at the outpatient pharmacy department of the study setting using a data collection form. All prescriptions were gathered prospectively and analyzed to evaluate the prescribing patterns of NSAIDs. Prescriptions comprising NSAIDs were assessed based on the designated study parameters (type, brand name, dosage, mode of administration, duration of therapy, monotherapy, fixed drug combination, etc).
World Health Organization Core Prescribing Indicators
Each prescription was evaluated based on the World Health Organization (WHO) drug use indicators to determine the logic of the prescribing pattern. This contains the average number of medications in each interaction. The proportions of encounters involving prescribed NSAIDs, NSAID injections, non-selective NSAIDs, COX-2 selective NSAIDs, NSAIDs prescribed by generic name, NSAIDs from the Essential Medicines list, fixed-dose combinations (FDCs) of NSAIDs, and NSAIDs prescribed with gastroprotective agents were calculated to evaluate prescribing patterns.
Assessment of Polypharmacy
We examined the quantity of drugs prescribed in individual prescriptions within the study populations at the outpatient pharmacy department. Due to the absence of an internationally recognized definition of polypharmacy, the prevalent definition refers to the simultaneous administration of five or more drugs for research purposes.7,9,10 We evaluated the prevalence of polypharmacy based on prescription data, categorizing it into three distinct classifications: non-polypharmacy (fewer than five medications), polypharmacy (5 to 9 medications), and hyper-polypharmacy (10 or more medications).
Assessment of Drug-Drug Interactions
To ascertain the possible drug-drug interactions (DDIs) associated with NSAIDs prescriptions, all medications prescribed, excluding those designated as “stat” or “as needed”, were included in the “drugs to check” list and evaluated using the Thomson Reuters Micromedex® DrugReax® system. The incidence rates and clinical consequences of these drug-drug interactions (DDIs) were subsequently assessed. They were classified based on various factors, including “severity” (minor, moderate, major), “onset” (quick, delayed, not specified), classification, and “degrees of documentation” (excellent, good, fair, and unknown). Clinical monitoring was performed by reviewing patient electronic health records (laboratory parameters, comorbidities, and treatment notes) to assess the clinical relevance of identified interactions. The definitions of onset, severity, significance rating, and documentation used in the study, as provided by the Micromedex DrugReax system, are detailed below.
Criteria for Onset
The gravity of an interaction’s consequences depends on the rapidity with which its clinical effects manifest and the urgency required for preventive measures to mitigate them. It is categorized as “Rapid -the effect will manifest within 24 hours of administering the interacting medicines; Delayed -the effect will not be apparent within 24 hours of simultaneous administration, and Not specified - Effects may require several days or weeks of simultaneous dosing to manifest.
Criteria for Severity
When weighing the risks and benefits of a treatment, as well as those of alternative therapies, it is crucial to consider the potential severity of any possible interactions that may occur. The adverse effects of many interactions can be prevented by adjusting the administration schedule or dosage appropriately. Five levels of severity are delineated as follows: “The medications are contraindicated for simultaneous use. Major - The interaction may pose a life-threatening risk and/or necessitate medical intervention to mitigate or avert severe adverse effects. Moderate - The interaction may lead to a worsening of the patient’s condition and/or necessitate a modification in treatment. Minor - The interaction would provide minimal clinical consequences. Manifestations may involve an escalation in the frequency or intensity of adverse effects, but often do not necessitate a significant modification in treatment. Unknown – No identified medication interactions”.
Criteria for Documentation
The extent of confidence regarding the potential for an interaction to result in a modified therapeutic response is dependent on the available documentation. This assessment reflects the editorial team’s evaluation of both the quality and clinical significance of the primary research that establishes the presence of such an interaction. Nonetheless, several variables may influence whether a patient experiences even a well-recorded interaction. The documentation is unaffected by the interaction’s possible intensity of effect and makes no mention of the interaction’s incidence or frequency. It is classified as “Excellent - Controlled research has definitively demonstrated the presence of the interaction. Good - Documentation strongly suggests the existence of interactions; however, well-controlled studies are lacking. Fair - The available evidence is inadequate. However, pharmacological considerations prompt doctors to suspect the existence of the interaction; alternatively, documentation is robust for a pharmacologically analogous substance. Unidentified – Unidentified”.
Charlson Comorbidity Index
The Charlson Comorbidity Index (CCI) score, established in 1987, is a validated and straightforward tool for assessing the mortality risk associated with comorbid conditions. It is often utilized as a predictor of death and prognosis.17 The Charlson Comorbidity Index (CCI) categorizes comorbidities, including cardiovascular, metabolic, renal, hepatic, pulmonary, and oncological illnesses, making it the most prevalent and reliable method for estimating mortality. The age-adjusted Charlson Comorbidity Index (CCI) is derived from age and 17 medical comorbidities that may influence the CCI score, resulting in a number ranging from 1 to 6, depending on the condition. The cumulative score for the CCI is only the aggregation of the weights, with elevated scores indicating greater severity of comorbidity or multimorbidity.
Data Analysis
The compiled data were entered into a Microsoft Excel spreadsheet for further analysis. The analysis was performed utilizing the Statistical Package for the Social Sciences (SPSS) version 29.0 for Windows (IBM, Armonk, New York). The findings were evaluated by the World Health Organization’s (WHO) standard key indicators for prescription. Descriptive statistics, encompassing means, percentages, frequencies, and standard deviation (SD), were employed to characterize patient demographics and to evaluate the prevalence of NSAIDs prescriptions, as well as their concomitant prescriptions with other specific medications. Multivariable logistic regression analyses were executed to identify potential predictive factors associated with NSAID usage. The association between dependent and independent categorical variables was analyzed using the Chi-square test and Relative Risk. Furthermore, the determinants influencing the incidence of DDIs were evaluated through both univariate and multivariate regression analyses. A Pearson correlation analysis was performed to investigate the relationship between continuous variables and their correlation with the number of pDDIs. A p-value of less than 0.05 was considered statistically significant.
Results
Sociodemographic Characteristics of the Study Populations
In total, 174 case records of the older adults population receiving NSAIDs prescriptions were reviewed during the study period. The predominant demographic among the study participants consisted of females (59.77%) with an age category between 65–74 years (75.86%), and the average age was found to be 71.9 ± 7.89 (Mean ± SD) years (range: 65 to 103 years). Three-quarters of the study samples consisted of UAE nationals, and nearly 90% of them were currently retired. Comorbidities were identified in more than 90% of the study samples, with over half of them having 3–4 comorbidities. Cardiovascular illnesses (33.74%) were the predominant comorbidity, followed by diabetes mellitus (17.59%). The mean quantity of medications administered to each patient was 6.74 ± 3.67 (Mean ± SD), with about half of the research group receiving 1–5 medications each prescription (Table 1).
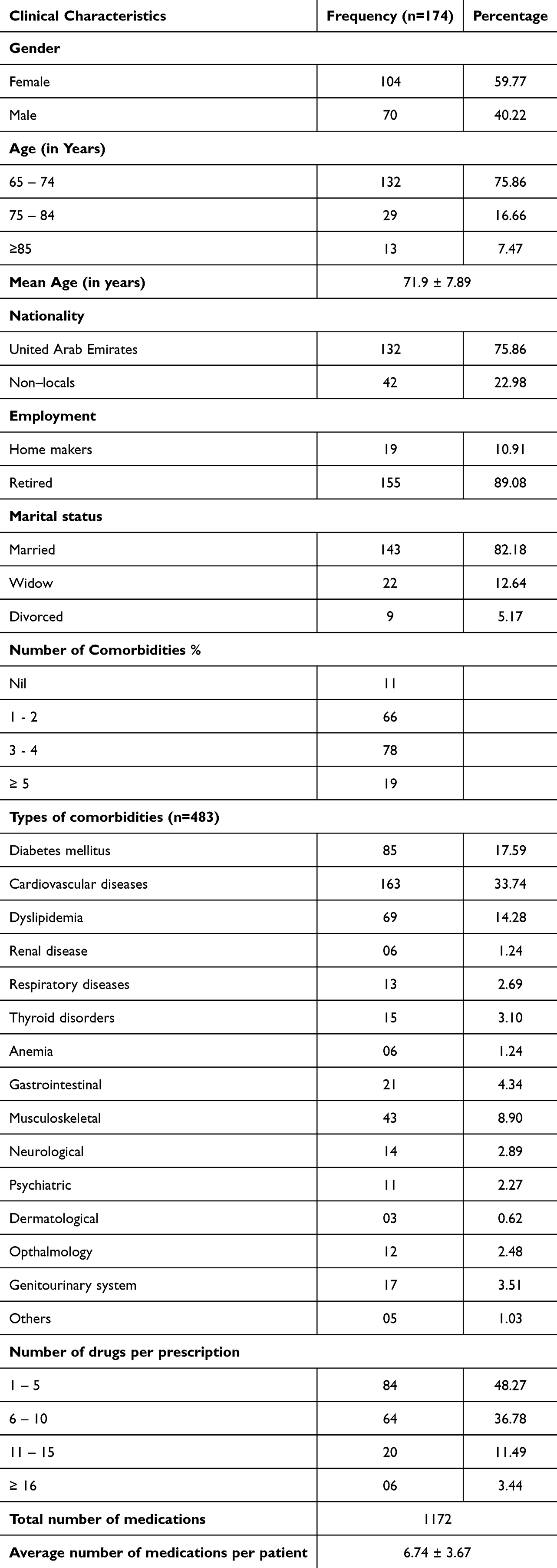 |
Table 1 Sociodemographic Characteristics of the Study Populations (n=174) |
Therapeutic Class of Medications
In the study populations, the most frequently prescribed therapeutic class of medications was those about the musculoskeletal system, accounting for 31.29% of prescriptions. This was followed by medications for the cardiovascular system, which constituted 22.15%, and those for the alimentary tract and metabolism, representing 21.06%. (Table 2).
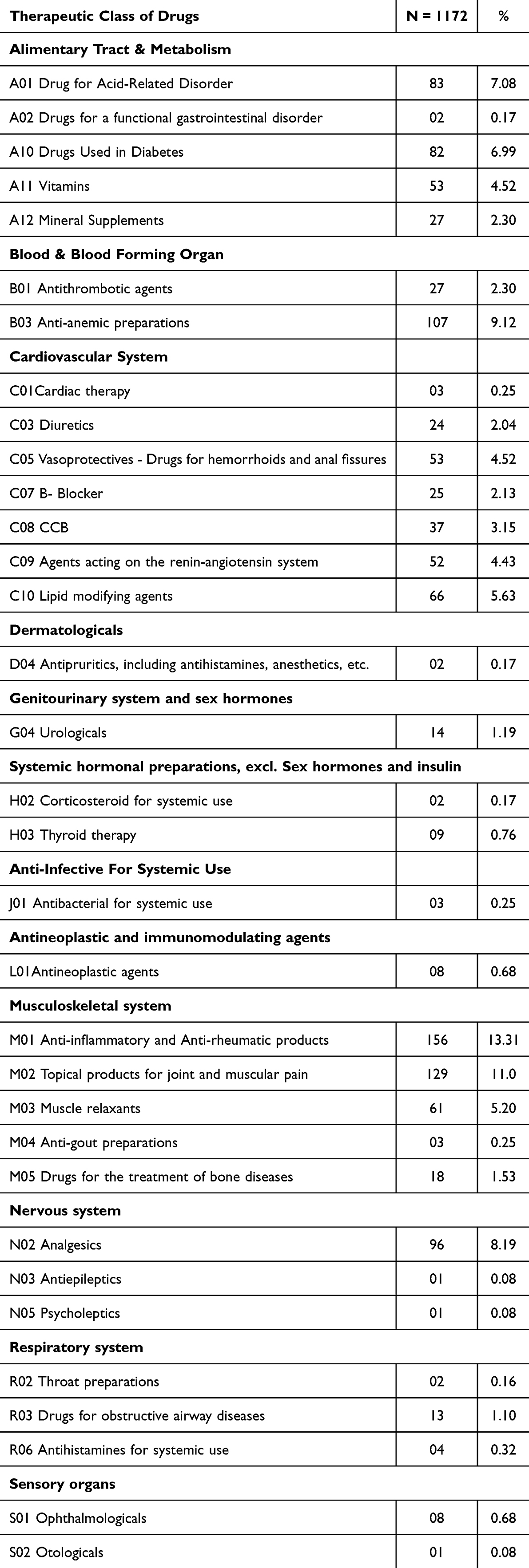 |
Table 2 Therapeutic Class of Prescriptions Medications Received by the Study Population (n=1172) |
Evaluation by the WHO Core Prescribing Indicators for NSAIDs
The examination of NSAIDs prescription data, utilizing the WHO core prescribing indicators, yielded several significant findings. Among the 174 prescriptions analyzed, the mean quantity of NSAID medications per prescription was 1.74 ± 0.58. Notably, selective COX-2 inhibitors constituted 49.42% of the NSAID prescriptions. It is important to highlight that no prescriptions included parenteral formulations of NSAIDs. Furthermore, all prescriptions were issued using generic nomenclature and sourced from the national essential drug list, achieving a 100% compliance rate. Additionally, approximately 97.12% of NSAID prescriptions were accompanied by co-prescribed medications, including acid-suppressive agents, vitamins, and antimicrobials, with acid-suppressive agents being the most frequently co-prescribed at a rate of 48.8%. (Table 3).
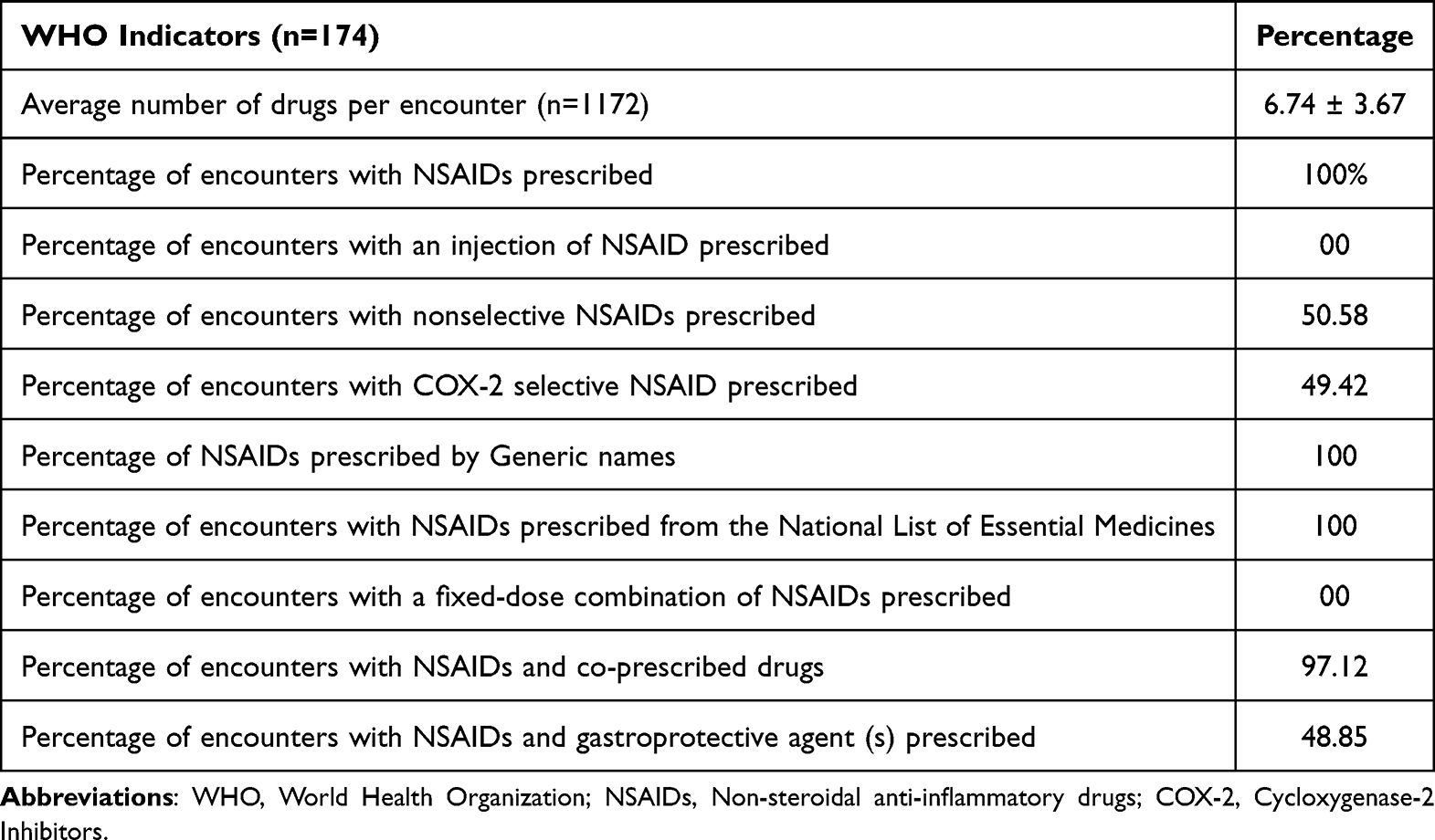 |
Table 3 WHO Core Prescribing Indicators for NSAIDs |
Prescribing Pattern of NSAID Drugs
A total of 304 NSAID medications were prescribed for the 174 study populations, with an average of 1.74 ± 0.58 pills per prescription. The minimum number of NSAID medicines prescribed /patient was one, and the maximum was three. It was observed that 111 (63.79%) of the patients were receiving both topical and oral NSAID medications per prescription. However, 45 (25.86%) patients received only oral NSAIDs, and 10.34% of patients were prescribed topical NSAIDs alone. (Table 4).
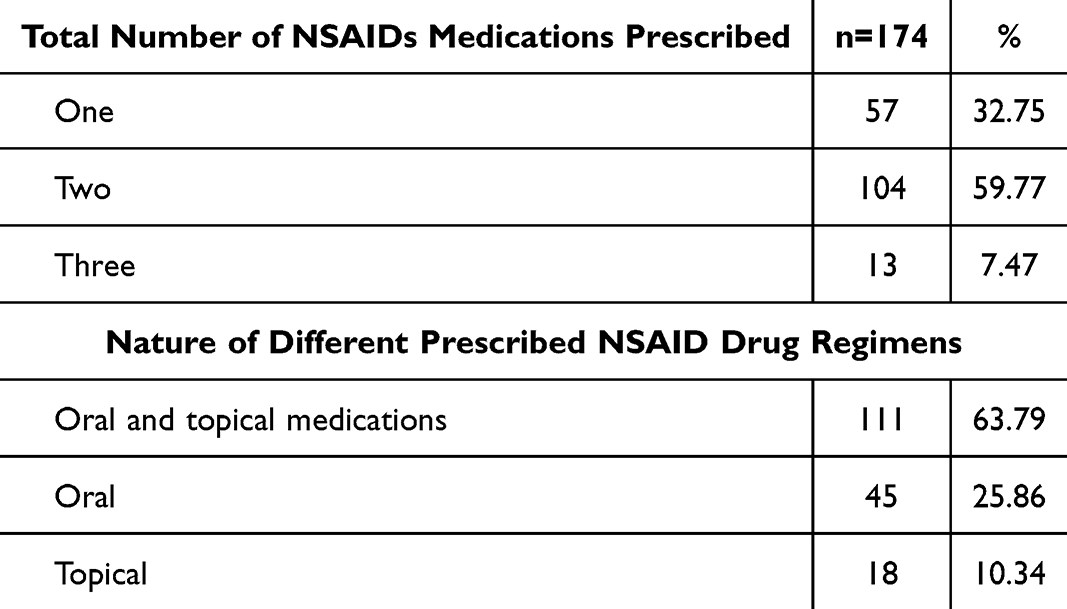 |
Table 4 Nature and Number of NSAIDs Prescribed per Prescription in Study Populations |
Diagnosis Versus Prescription of NSAIDs
Out of the 174 study populations, 213 diagnoses were found to have involved the prescription of NSAIDs. The most frequent reason for prescribing NSAIDs in the study groups was pain linked to arthritis (39.9%). Spondylosis/radiculopathy (20.6%), pain without a known cause or disorder (14.55%), and pain in the shoulder, joint, elbow, or low back (7.98%) are the other main clinical indications (Figure 1).
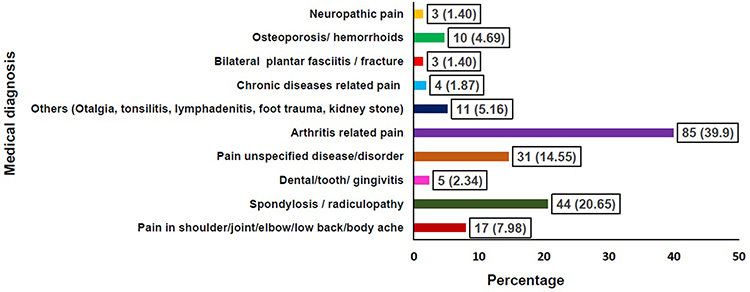 |
Figure 1 Most common diagnosis for prescribing NSAIDs. |
Prescribing Pattern of NSAID Medications According to Therapeutic Class of Medications
Among the therapeutic class of NSAIDs medications, non-selective COX inhibitors were the most frequently prescribed class of drugs [141(46.38%)], followed by Selective COX Inhibitors [49.7%]. The Preferential COX-2 inhibitors were prescribed in 25.32% of the study population. Considering the individual NSAIDs, celecoxib (28.2%) and ketoprofen (27.6%) were the most commonly prescribed oral and topical NSAIDs among the study populations (Table 5).
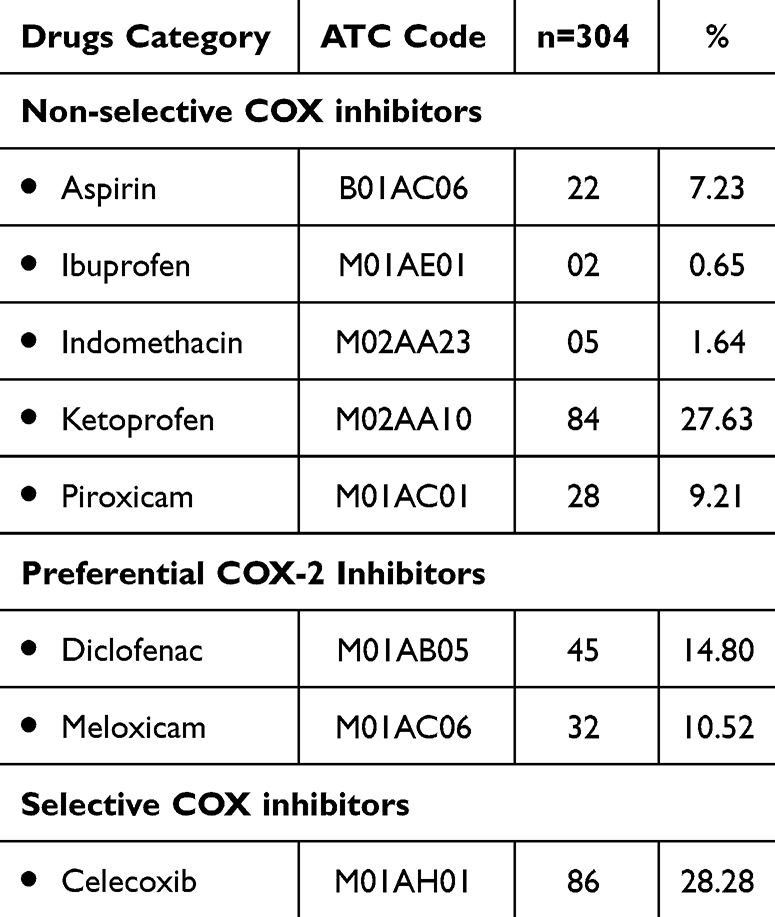 |
Table 5 Therapeutic Class of NSAID Medications with Individual Drugs |
Association Between the Type of NSAID and Co-Prescription with a Gastroprotective Agent
In the study sample, a mere 47.7% of patients received prescriptions for proton pump inhibitors (PPIs)—specifically, omeprazole at 44.5%, dexlansoprazole at 28.91%, esomeprazole at 22.8%, and pantoprazole at 6.02%—in conjunction with NSAIDs. In contrast, 52.29% of patients did not receive any gastroprotective agents. The analysis of the relationship between the prescribed NSAID type and its co-prescription with gastroprotective agents revealed significant associations for Diclofenac (P = 0.004), Aspirin (P = 0.017), and Meloxicam (P = 0.049), as shown in Table 6.
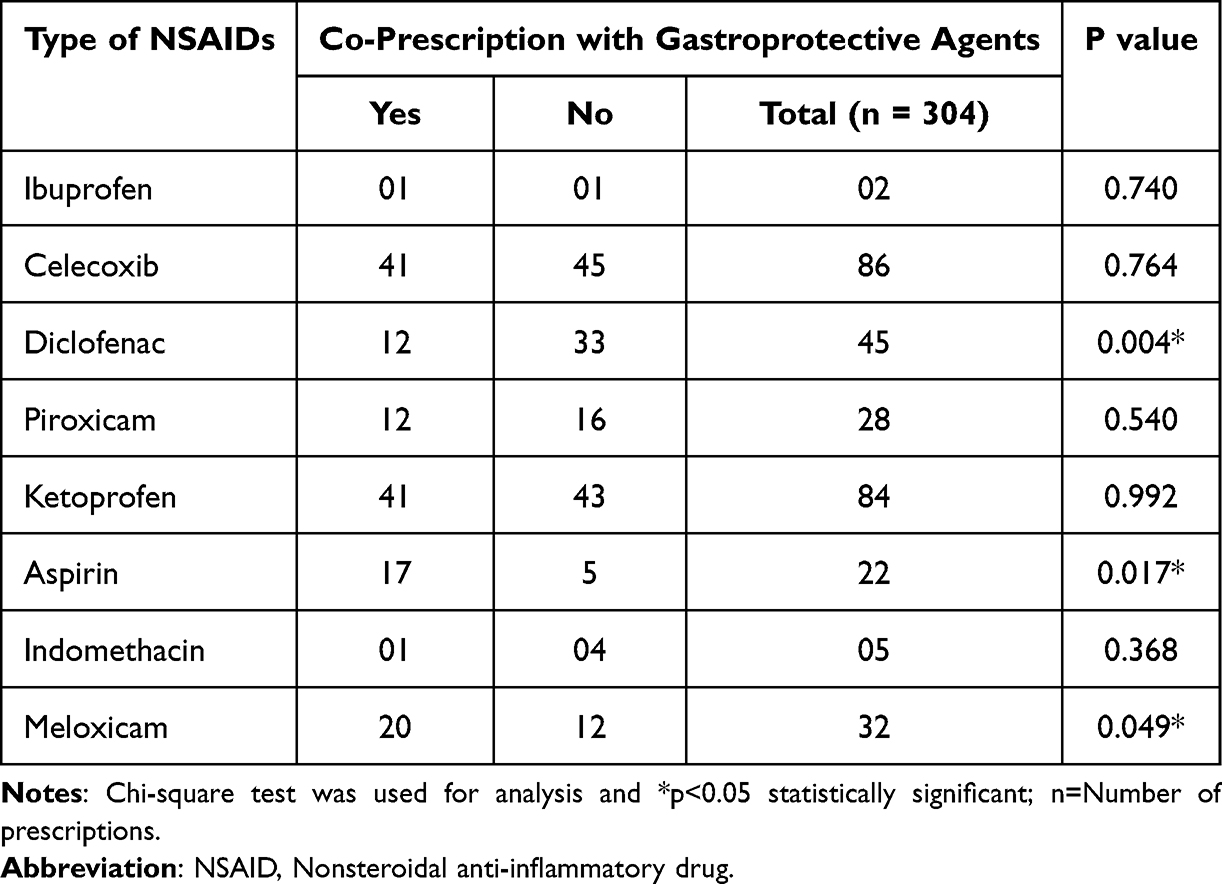 |
Table 6 Association Between Types of NSAID Prescribed and Whether It Is Co-Prescribed with Gastroprotective Agent (s) |
Polypharmacy
The median number of medications was 6, with a range from 2 to 20, and polypharmacy was identified in more than half of the study group, namely 51.72%. Hyper polypharmacy, defined as 10 more drugs per prescription, was observed in 18.96% of the prescriptions evaluated. Analysis of polypharmacy about treatment-related variables has shown that the presence of comorbidities (p < 0.001) is positively associated with polypharmacy. In contrast, gender, age, and Charlson Comorbidity Index (CCI) did not show any significance with polypharmacy (Table 7).
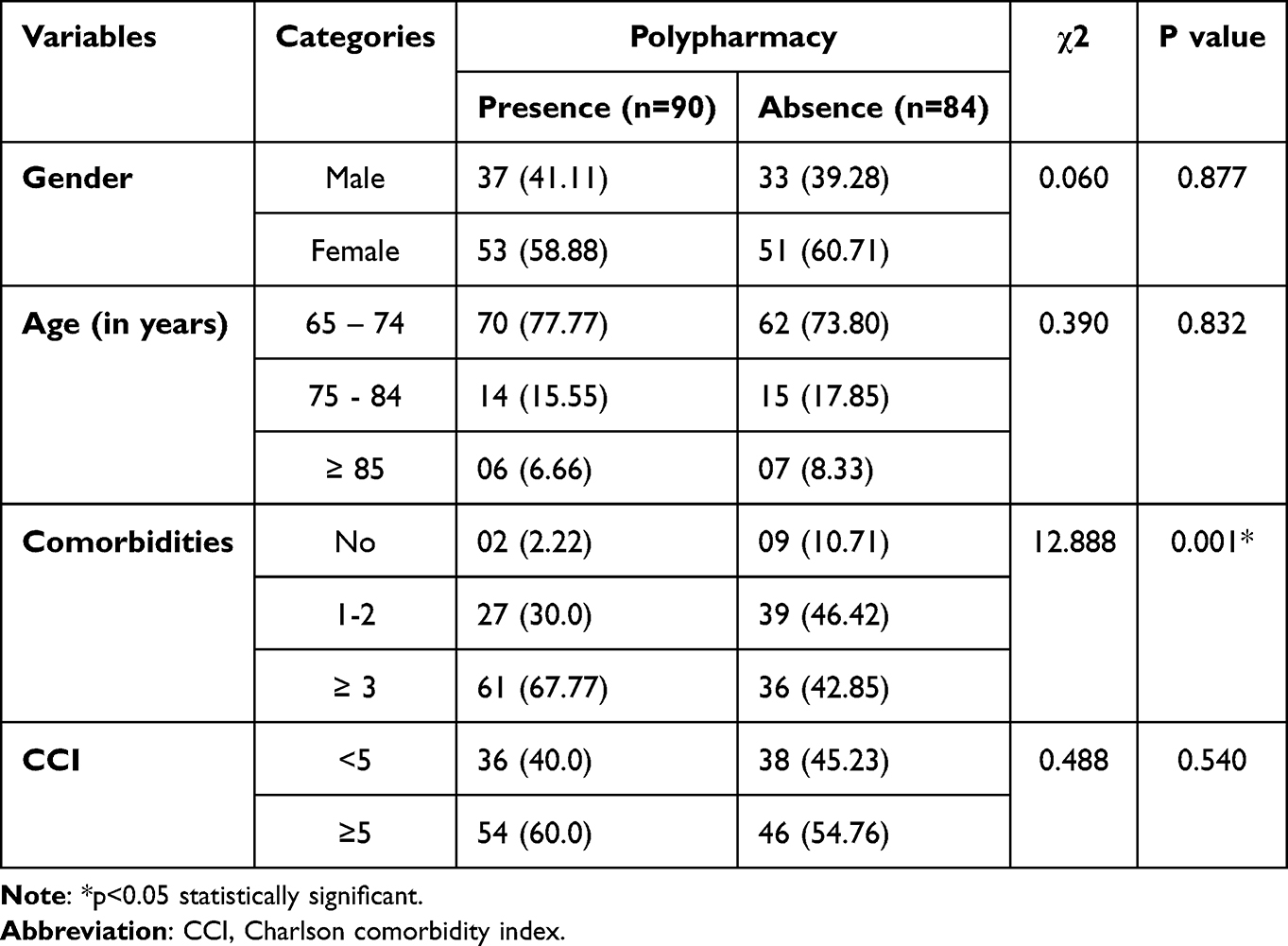 |
Table 7 Bivariate Analysis of Factors Associated with Polypharmacy Among the Study Populations |
Logistic regression analysis revealed that among the comorbidities, hypertension (CI: 1.340–6.546; p = 0.007) and musculoskeletal disorders (CI: 1.510–7.645; p = 0.003) were significantly associated with the occurrence of polypharmacy.
Potential Drug-Drug Interactions
Among the total 174 prescriptions analyzed, 340 pDDIs were identified affecting 76 (43.67%) of the individuals with a mean of 1.95 ± 3.66 interactions per prescription. Of all the pDDIs identified in the study populations, categorized by their level of severity, 198 (58.23%) were moderate, 136 (40.0%) were major, and 6 (1.76%) were minor interactions, respectively. There were no interactions classified as “contraindicated” or “unknown” observed in the study populations. Based on the documentation rating, 158 (46.47%) were rated as “fair”, 118 (34.7%) were rated as “good”, and 64 (18.82%) were rated as “excellent”. Considering the onset of the drug interactions, most of the interactions [203 (59.70%)] were classified as “not specified”, followed by “delayed” [108 (31.76%)] and “rapid” [29 (8.52%)] (Figure 2).
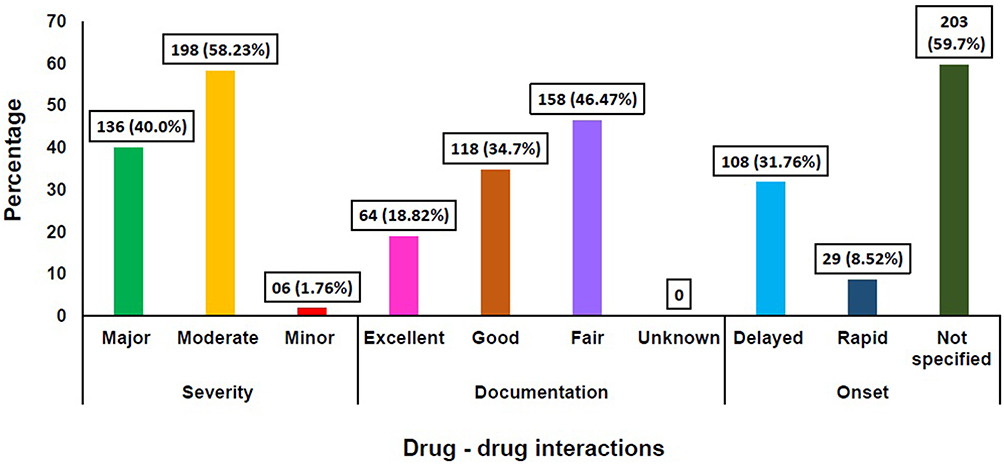 |
Figure 2 Classification of drug -drug interactions based on the severity, documentation and onset. |
In this study, it was observed that aspirin and celecoxib were the most common NSAIDs, along with the co-prescribed medications involved in causing pDDIs. Among the major DDIs, the most common drug pairs involved in DDIs were Aspirin + Metformin (2.94%) and Aspirin + Celecoxib (2.05%). Drug combinations such as omeprazole + vitamin B complex (3.52%), Amlodipine + Metformin (2.35%), celecoxib + valsartan (2.05%), and bisoprolol + celecoxib (1.76%) were found to have a moderate level of severity (Table 8).
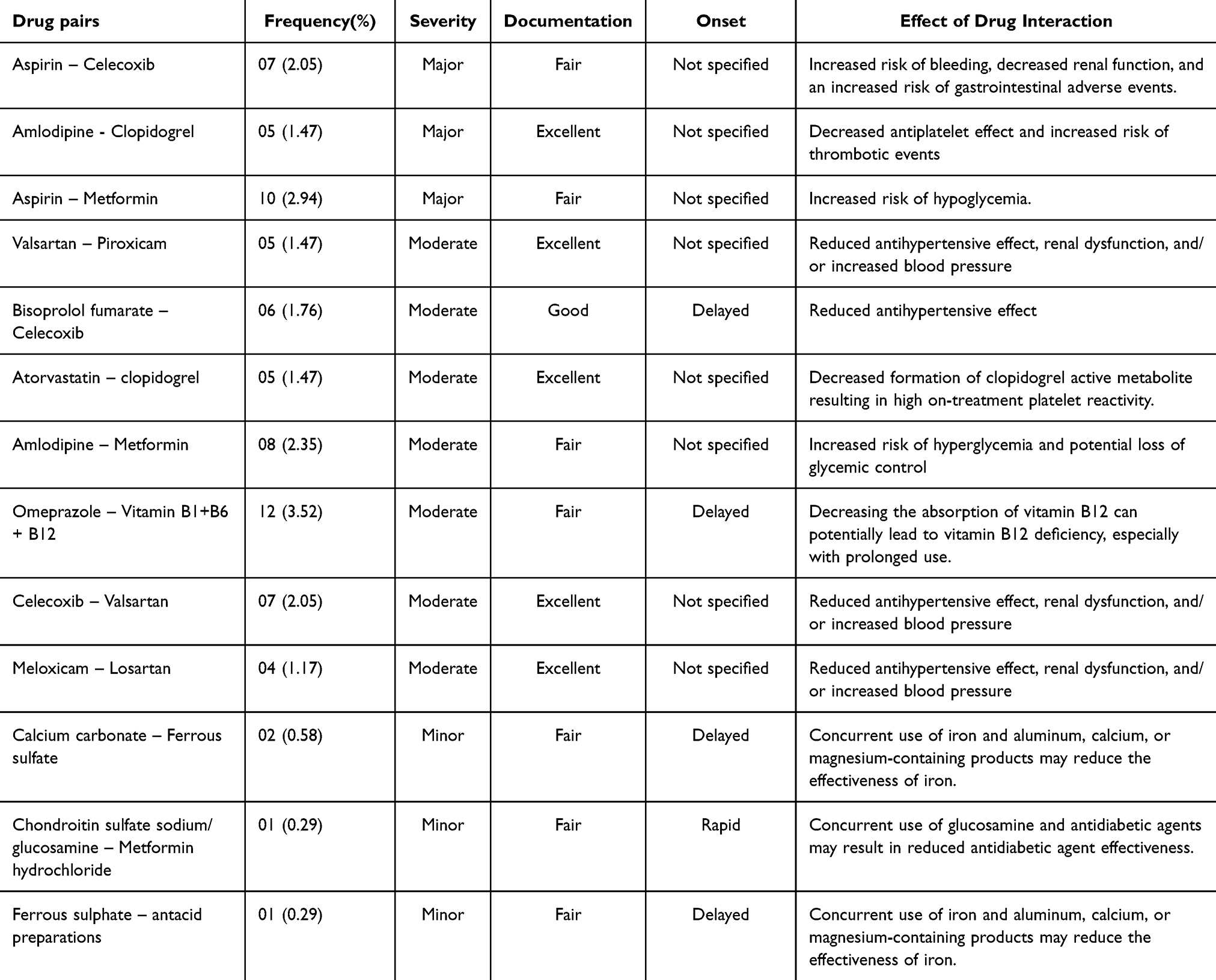 |
Table 8 The Most Common Drug Pairs Involved in Drug-Drug Interactions |
The probability of drug interactions escalates in proportion to the quantity of prescribed medications. Our research findings demonstrate a statistically significant association between the total number of prescribed medications and the frequency of drug interactions (P<0.0001) (Table 9).
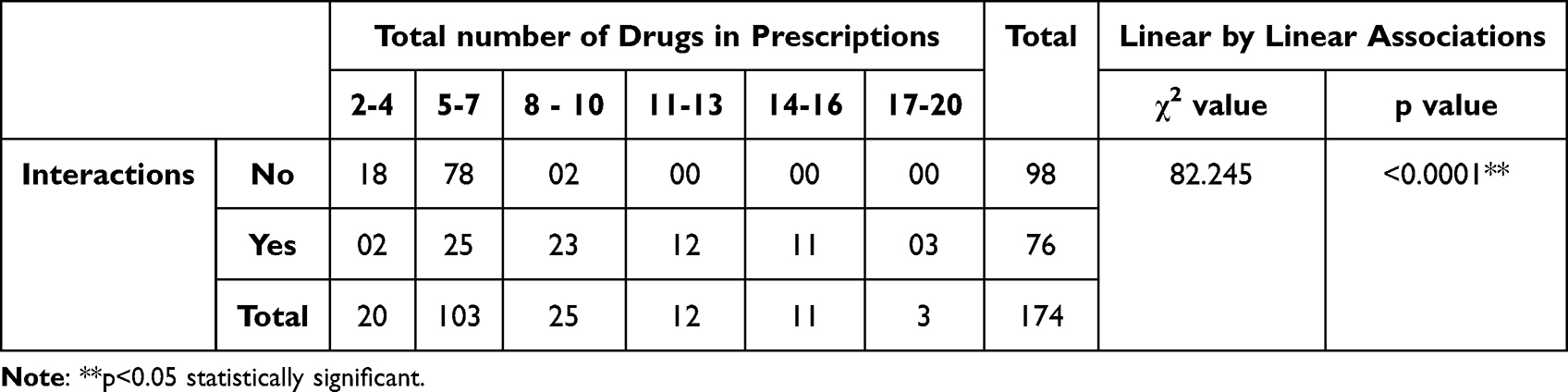 |
Table 9 Number of Drugs Prescribed, the Frequency of pDDIs, and Their Linear-by-Linear Associations |
The bivariate analysis conducted on the characteristics associated with drug interactions within the study population revealed a statistically significant relationship with both the cumulative comorbidities (p = 0.008) and the quantity of prescribed medications (p < 0.001) with the incidence of drug interactions. Variables yielding a p-value of less than 0.05 in the bivariate analysis were subsequently subjected to multivariate logistic regression analysis to ascertain predictors of potential drug-drug interactions (pDDIs). Notably, a significant association was identified between an increased number of medications (Confidence Interval: 9.367–51.269; p < 0.001) and the Charlson comorbidity index (Confidence Interval: 1.048–5.685; p = 0.039) with the prevalence of drug interactions. (Table 10).
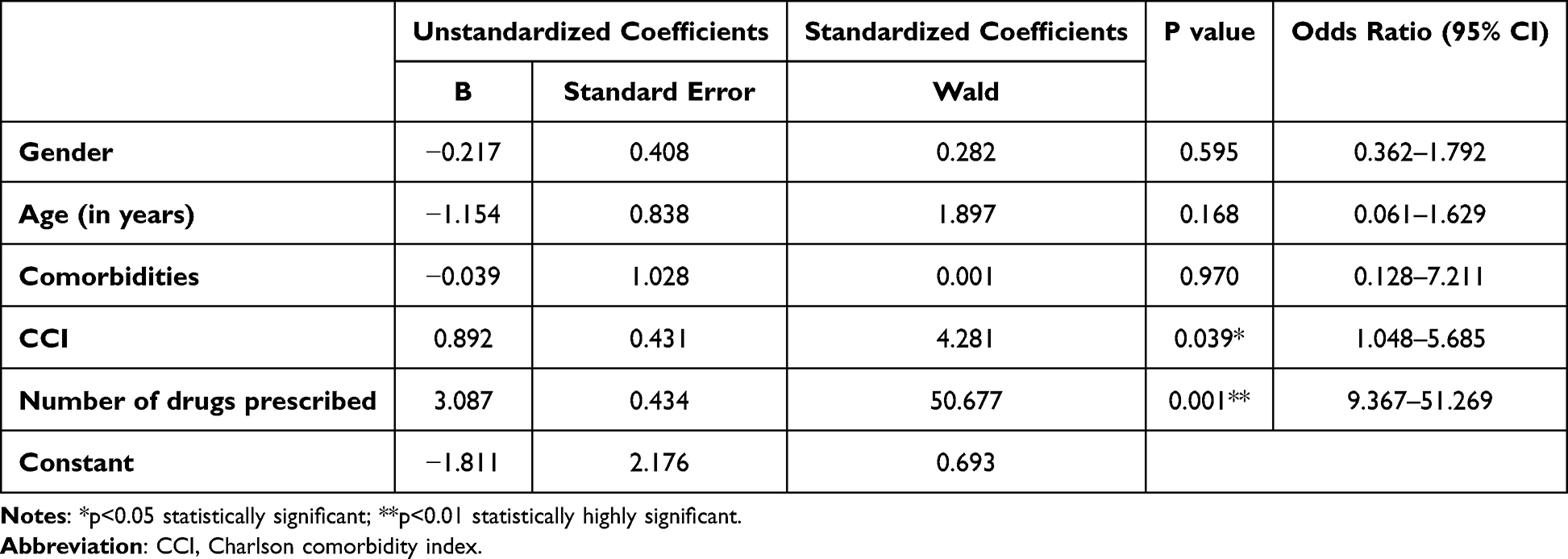 |
Table 10 Multiple Binary Logistic Regression Analyses for Factors Associated with Drug-Drug Interactions Among the Study Populations |
The Pearson correlation analysis indicates a statistically significant positive correlation between the number of pDDIs and various continuous treatment-related variables. Specifically, the correlation coefficients are as follows: Charlson comorbidity index (r = 0.218, p = 0.004), cumulative comorbidities (r = 0.366, p < 0.001), and the total number of medications administered (r = 0.790, p < 0.001) (Table 11).
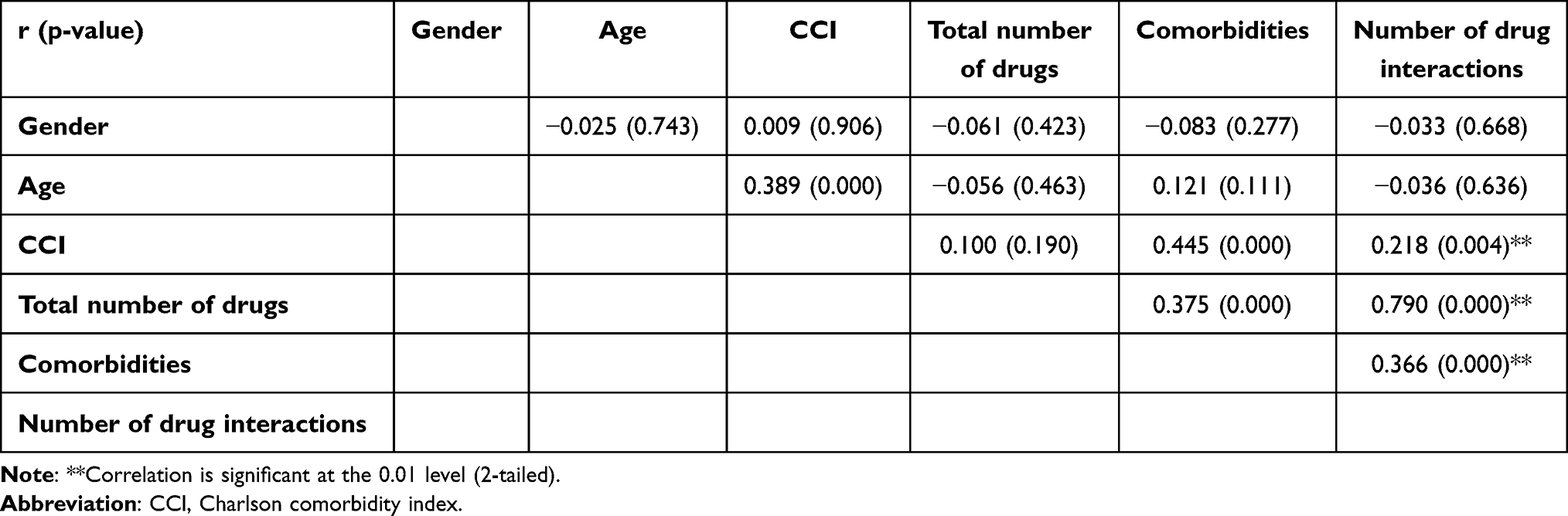 |
Table 11 Correlation Between DDIs and Treatment-Related Variables |
Discussion
Drug therapy is essential for older adults patients, but assessing prescribing patterns is vital to ensure clinical, economic, and educational efficacy.5 Research focused on drug utilization aims to provide insights for prescribers, enhancing their understanding of the rational use of medications.
In our study, female patients showed a preponderance, with the majority belonging to the age category 65–74 years with multiple comorbidities, particularly cardiovascular diseases and diabetes, aligning with patterns seen in similar studies.13,14,18 The decline in functional reserve due to age renders geriatric patients susceptible to the onset of various disorders impacting bodily systems.19 This highlights the importance of cautious medication management to address complicated health demands and reduce drug-related complications. Over 50% of the study population was prescribed five or more medications. The increased quantity of drugs per prescription may be associated with various comorbidities in our older adults populations. Studies conducted with comparable research populations and settings also found similar observations, aligning with our findings.2,9,14,18
The ATC classification indicates that the most often prescribed drugs were those for musculoskeletal disorders, encompassing pain and inflammation management. This differs from other research, which has shown a higher prescription rate for medications used to treat metabolic and cardiovascular conditions.3,20,21 The current investigation revealed an average of 6.74 ± 3.67 medications per prescription, exceeding the normal range of 1.6 to 1.8. Consistent results were also noted in investigations conducted by researchers worldwide.19,20,22 The discrepancies observed in the conventional value may be ascribed to the research being carried out within senior communities, where a substantial proportion of patients presented with one or more comorbid conditions. In our study, all NSAID prescriptions were issued under generic names and sourced from the national essential medication list formulary, aligning with the World Health Organization’s (WHO) recommendations (100%). The percentages reported in other research were unsatisfactory, varying from 17.8% to 98.5%.17,22,23 The prescription of medications by their generic names is a prevalent practice in public hospitals and primary health centers in the UAE, crucial for enhancing the rational utilization of pharmaceuticals. Additionally, it also works out to be more cost-effective for the patient, reducing the likelihood of dispensing errors and the cost per prescription.
The present investigation revealed that the mean quantity of NSAIDs prescribed per encounter was 1.74 ± 0.58 per prescription, with nearly two-thirds of the study population receiving two or more NSAIDs, consisting of both oral and topical preparations. Previous studies also reported similar results in all parts of the world.24,25 The route of administration is recognized to influence the therapeutic outcome, the onset of action, and the adverse effects that may arise. Nevertheless, the predominant use of oral NSAIDs elevates the likelihood of gastrointestinal adverse outcomes by 2–4 times in a dose-related manner, especially among older adults populations with co-morbidities. Therefore, topical preparations of NSAIDs is considered safe and offers the advantage of relieving symptoms of pain and inflammation with lower incidence of systemic adverse effects in such group of populations.26 Insufficient analgesia with a single agent specially in chronic and advanced stage of the disease, considering brief use of multiple NSAIDs to manage severe pain or may be some NSAIDs have slightly different mechanisms of action or targets, which might be used together to achieve a more comprehensive analgesic or anti-inflammatory effect are the possible reasons that could explain the reasons for multiple use of NSAIDs in our study populations.
Our data revealed that celecoxib was the most commonly given NSAID, which is in line with previous research.25,27,28 Celecoxib and other selective COX-2 inhibitors are preferred because they effectively reduce arthritis pain and inflammation and have less adverse effects on the kidneys and gastrointestinal tract than conventional NSAIDs. Their superiority in pain relief is ascribed to their extended duration of action and efficaciousness.29 The elevated risk of cardiovascular side effects associated with celecoxib, however, warrants serious caution. A significant fraction of the participants in our study had cardiovascular illnesses, and many of them were administered NSAIDs, such as celecoxib. This gives rise to concerns about the possibility of underestimating the cardiovascular risks connected to these medications. It is essential to thoroughly evaluate patients and conduct routine monitoring in order to weigh the advantages of COX-2 inhibitors against their potential cardiovascular concerns. Additionally, because of their longer shelf life and lower cost, non-selective NSAIDs, which accounted for almost 70% of prescriptions in our sample, are often utilized. Their broad use is probably motivated by perceived efficacy and customary habits. However, to optimize benefits and reduce risks in older patients, careful consideration of their potential side effects, such as gastrointestinal bleeding and renal impairment, is necessary.30
Researches showed that, in order to reduce gastrointestinal hazards, gastro protective medicines and NSAIDs are frequently administered together.24,25 Aspirin, diclofenac, and meloxicam are examples of NSAIDs that have a strong correlation with the usage of gastro protective drugs, according to our research. According to the guidelines of the American College of Gastroenterology, patients who are considered high-risk, meaning they have a history of gastrointestinal ulcers, are older than 65, or are on drugs such as low-dose aspirin or corticosteroids, should take gastro protective agents. But prolonged use of proton pump inhibitors (PPIs), which are frequently prescribed for gastro protection, has been associated with harmful side effects.31 Prescriptions for PPIs must adhere to evidence-based medicine principles, ensuring that their use is confined to the lowest effective dose for the minimal duration necessary.
Polypharmacy
Polypharmacy represents a significant global health concern within older adults populations, particularly as multiple comorbidities increase the necessity for various medications to attain therapeutic outcomes. The effects are extensive and may influence overall health outcomes, treatment effectiveness, and patient safety.32 The prevalence of polypharmacy in older adults populations, as indicated by various research studies, varies significantly across healthcare settings worldwide, with reported rates ranging from 18.5% to 94.3%.33–35 Studies also pointed out that polypharmacy and hyperpolypharmacy are significantly linked to aging populations, the definition used, comorbidities, and the geographical setting of the study, which could explain more than half the numbers seen in our research.1,14,17 Furthermore, cardiovascular, cerebrovascular, and arthritis related diseases were commonly linked with the practice of polypharmacy and pDDIs.34,36 In our study, comorbidities such as hypertension and musculoskeletal disorders were significantly associated with polypharmacy.
Evidence-based guidelines recommend the use of multiple pharmacological classes in treatment, as this approach has been shown to improve patient outcomes and alleviate symptoms. These guidelines address polypharmacy, the associated vulnerability to falls and fractures, and the economic burden in older adults populations with these comorbidities.37 Therefore, the study recommends that healthcare professionals prioritize medication optimization, de-prescribing, regular monitoring of laboratory parameters, and adjusting therapy doses based on clinical conditions to mitigate future complications related to polypharmacy. To enhance overall health outcomes and quality of life, addressing polypharmacy in the older adults requires careful supervision and a tailored approach that balances the benefits of medications against potential risks, ensuring that treatments have a positive impact on patient health.
Drug Interactions
The possibility of taking several medications for multiple comorbidities, age-related physiological changes, and greater susceptibility to side effects makes drug interactions in older adults people a serious concern.32 The present investigation revealed that 43.67% of the participants in the study exhibited at least one instance of drug-drug interaction, ranging from minor to major severity. Previous studies on DDIs in older adults patients in different healthcare settings showed widely heterogeneous results, ranging from 20% to 100%.36,38–40 Although study populations and regional variations contributed to these discrepancies, the definitions of the drug-drug interactions (potential or clinically significant, especially for clinically significant drug-drug interactions) and the standards employed to assess these interactions (including various databases, consensus guidelines, and reference materials) were the main factors leading to these differences. The medicines most commonly involved in DDIs in our study populations were cardiovascular drugs, oral hypoglycemic agents, analgesics and anti-inflammatory drugs, minerals and vitamin supplements, and gastro-protective agents. This may be explained by the fact that the most common chronic problems in this study were musculoskeletal disorders and metabolic diseases, including diabetes and cardiovascular disease.
The prevalent drug combinations that exhibit notable interactions include furosemide combined with piroxicam, metformin with aspirin, amlodipine alongside clopidogrel, and celecoxib paired with aspirin. Additionally, combinations with a modest level of relevance have been identified, including meloxicam and losartan, atorvastatin and clopidogrel, celecoxib and valsartan, omeprazole/esomeprazole and multivitamins, and bisoprolol and celecoxib. The pharmacological basis of these major pDDIs can be explained by additive or synergistic effects on similar pathways. For instance, NSAIDs combined with anticoagulants or antiplatelets increase bleeding risk by impairing platelet aggregation and damaging gastric mucosa, while NSAIDs with ACE inhibitors or diuretics reduce renal prostaglandin activity, leading to decreased renal perfusion and higher risk of nephrotoxicity. Similarly, combining metformin with aspirin may potentiate hypoglycemia due to overlapping effects on glucose metabolism. These mechanisms emphasize the importance of cautious co-prescribing and monitoring in older adults patients.41,42 On occasion, though, certain combinations cannot be avoided and may even be recommended. For such interactions, careful observation, a risk assessment of potential drug interactions, and an evaluation of the benefits of continuing both medications are necessary. Laboratory results, including blood sugar levels, renal function tests, serum electrolyte levels, and symptoms and signs of bleeding, should be regularly monitored while these medications are taken together. Earlier investigations have identified these combinations in older adults populations as clinically relevant drug-drug interactions (DDIs).35,37,38 Fewer percentages of mild interactions involving vitamin and mineral supplements were noted in the current investigation, which may have the impact of reducing the efficacy of medication therapy. Nevertheless, there are few clinical impacts of these interactions; therefore, changing medication therapy significantly is usually not necessary.
Another notable observation in this study was the highest prevalence of interactions involving cardiovascular medications and concomitant NSAIDs. In older adults individuals and those with chronic conditions, hypertension and chronic pain frequently occur together; consequently, the simultaneous use of NSAIDs and antihypertensive medications is common. The concurrent use of NSAIDs may diminish the efficacy of pharmacological agents that act on renal prostaglandins, exemplified by furosemide, or alter the pharmacodynamic effects of other diuretics, as well as drugs acting on the renin-angiotensin pathway. This contributes to higher blood pressure by suppressing renal prostaglandins and increasing fluid retention. As each of these drug groups affects kidney function through different pathways, there is a concern that a combination of NSAIDs and antihypertensive medicines may raise the risk of acute renal injury in addition to effects on blood pressure. Comprehending possible dangers and interactions is crucial when administering these drugs concurrently to older adults populations. To reduce side effects and ensure safe and effective treatment, careful evaluation, the selection of suitable NSAIDs, the use of gastroprotective measures, routine monitoring, patient education, and collaborative care are crucial.
While consistent with other research, most pDDIs found in this investigation exhibited intermediate severity levels.43,44 Nonetheless, further focus is necessary on the two DDI classifications with the highest severity: serious and contraindicated. In contrast to these findings, few investigations have identified a pattern of mild and major DDIs according to their severity.45,46 This entire body of data suggests that patient-specific factors influence the prevalence of DDIs.
Regarding documentation grades, approximately fifty percent of the PDDIs were assessed as fair, with good and exceptional ratings following. These findings align with those of various previous studies.33,40 A small number of researchers stated that the majority of drug interactions had good, reasonable, or excellent documentation, which runs counter to these findings.39,43 The variation in the drugs prescribed for patients in various study settings, the accessibility and cost of medications, national and international treatment guidelines, and the preference of prescribers based on their own experiences could all be contributing factors to the discrepancy in the documentation grade reporting.
The presence of specific risk factors, including comorbidities, polypharmacy, age, length of stay, and various patient characteristics, is recognized as a potential predictor of drug-drug interactions (DDIs).15,36,47 Research has established a significant correlation between polypharmacy and DDIs.44,48 Medications are often combined to manage chronic conditions, and these combinations carry a considerable risk of drug interactions. The study revealed no substantial relationship between the prevalence of DDIs and demographic factors such as age or gender. Nevertheless, a positive correlation was identified between the quantity of medications administered, the presence of comorbidities, and an elevated CCI, and the incidence of DDIs, corroborating the findings of prior research.34,35,49,50 It is commonly known that as a patient’s number of comorbidities rises, so does the number of drugs they take, making them more susceptible to DDIs; older individuals are more vulnerable to this phenomenon. It has been reported that patients who used 2–3, 4–5, and 6–7 drugs, respectively, had a 39%, 88.8%, and 100% chance of developing DDIs, aligning with our study investigations.14
The influence of drug interactions and polypharmacy on the effectiveness and safety of therapeutic interventions in the older adults population holds significant clinical relevance. The likelihood of negative drug interactions, which can result in less effective therapy, more side effects, and a lower quality of life, is greatly enhanced by polypharmacy. Age-related physiological changes, such as reduced drug metabolism and renal function, make older adults people especially vulnerable. Proper prescribing procedures and close observation are necessary when managing polypharmacy because interactions can occur over time and not always show symptoms right away, making early discovery and treatment more difficult. Adjusting dosages according to specific patient characteristics and weighing the advantages of polypharmacy against the potential drawbacks of adverse interactions are two major problems. Regular medication evaluations, a clinical pharmacist-assisted computer decision support system, and open communication between healthcare providers are all necessary for effective management. Optimizing therapeutic outcomes and minimizing risks requires educating patients and caregivers about potential dangers and the importance of adhering to treatment plans.
Limitations
Our research has certain shortcomings. Firstly, Reliance on a single database may not encompass all pDDIs and would limit the number of pDDIs that can be identified. It may be possible to increase the accuracy of DDI detection by utilizing comparisons and various database tools. Second, the Wareed system provided the data for this study, which mostly concentrated on the theoretical pDDIs. The absence of subsequent evaluations hindered our ability to analyze the actual drug interactions and their clinical outcomes effectively. Thirdly, because the study was cross-sectional and the data were only gathered once, we were unable to evaluate how the drug regimens of our study populations changed during their treatments. Fourth, the study was limited to analyzing prescription medicine names, dosage amounts, and disease diagnoses given to the older adults; hence, the inappropriateness of the prescription was outside the scope of the investigation. Lastly, information about self-medication and dietary and herbal supplements was not collected because the data were gathered from an electronic healthcare system without direct patient access.
Conclusion
This research emphasizes critical concerns regarding the prescribing practices of NSAIDs and the prevalence of polypharmacy among the older adults demographic. The notable incidence of polypharmacy, along with the potential for DDIs—particularly those classified as moderate to severe—underscores the imperative for meticulous prescribing protocols and continuous assessment of medication regimens. Applying evidence-based medicine, utilizing information technology, and addressing the critical needs of the patient are essential for rational prescribing and enhancing medication safety in high-risk populations, such as older adults patients. The findings reveal that comorbidities and the number of medications are critical factors influencing drug interactions. The adoption of enhanced monitoring protocols, thorough patient education, and targeted interventions is essential for maximizing therapeutic efficacy and minimizing the occurrence of adverse effects. This approach ultimately promotes safer and more effective management of older adults patients.
Acknowledgments
The author acknowledges the administration of the RAK Medical & Health Sciences University for the inspiration and drive toward medical research. Special gratitude to the Dean, College of Pharmacy, RAK Medical & Health Sciences University, and also to the Hospital Director and the In-charge of the pharmacy department at Dibba Hospital in Al Fujairah, United Arab Emirates, for their encouragement and directions in completing this study.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Golla P, Bheemathati RR, Ramesh ASP, et al. prescribing pattern of medications in geriatric patients in a South Indian Tertiary Care Teaching Hospital. Indian J Pharm Pract. 2020;13(1):68–72. doi:10.5530/ijopp.13.1.11
2. Lemma W, Islam M, Loha E, et al. Drug prescribing patterns in geriatric patients in selected health facilities of Addis Ababa, Ethiopia. J Appl Pharm Sci. 2020;10(11):103–109. doi:10.7324/JAPS.2020.101114
3. United Nations. Economic and Social Commission for Western Asia (ESCWA). Prospects of ageing with dignity in the Arab Region. [cited on March 06, 2024]. Available from: https://www.unescwa.org/sites/default/files/pubs/pdf/population-development-report-8-english_0.pdf.
4. Mangi AA, Hammad MA, Khan H, et al. Evaluation of the geriatric patient’s prescription for inappropriate medications frequency at Larkana Sindh Hospital in Pakistan. Clin Epidemiol Global Health. 2020;8(4):1390–1394. doi:10.1016/j.cegh.2020.06.001
5. Bindu S, Mazumder S, Bandyopadhyay U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: a current perspective. Biochem Pharmacol. 2020;180:114147. doi:10.1016/j.bcp.2020.114147
6. Regi JK, Lalwani K, Pawar S. Comparative trends in the usage of nonsteroidal anti-inflammatory drugs: self-administration versus prescription. MGM J Med Sci. 2024;11:139–145. doi:10.4103/mgmj.mgmj_145_22
7. Drożdżal S, Lechowicz K, Szostak B, et al. Kidney damage from nonsteroidal anti-inflammatory drugs-Myth or truth? Review of selected literature. Pharmacol Res Perspect. 2021;9(4):e00817. doi:10.1002/prp2.817
8. Bahreini A, Koneri R. Prescription pattern analysis of nonsteroidal anti‑ inflammatory drugs in the Southeastern Karnataka Population, India. Arch Pharma Pract. 2020;11(S1):116–119.
9. Keche Y, Gaikwad NR, Wasnik PN, et al. Analysis of drugs prescribed to older adults patients in a Tertiary Health Care Center in Raipur, Central India: an observational study. Cureus. 2024;16(1):e52770. doi:10.7759/cureus.52770
10. Sidamo T, Deboch A, Abdi M, et al. Assessment of polypharmacy, drug use patterns, and associated factors at the Edna Adan university hospital, Hargeisa, Somaliland. J Trop Med. 2022;2022:2858987. doi:10.1155/2022/2858987
11. Arshiya S, Noronha V, Ramaswamy A, et al. Pattern of analgesic prescriptions and pain-related outcomes in older patients with cancer: a retrospective observational study. Cancer Res Stat Treat. 2023;6(4):541–548. doi:10.4103/crst.crst_326_23
12. Guillot J, Maumus-Robert S, Bezin J. Polypharmacy: a general review of definitions, descriptions and determinants. Therapie. 2020;75(5):407–416. doi:10.1016/j.therap.2019.10.001
13. John N, VJ A, James A, et al. Prescribing patterns of drugs in geriatric patient. J Drug Delivery Ther. 2021;11(2):168–170. doi:10.22270/jddt.v11i2.4783
14. Dagnew SB, Tadesse TY, Zeleke MM, et al. Drug-drug interactions among hospitalized older adults in patients at medical wards of Northwest Ethiopia’s comprehensive specialized hospitals: a multicenter observational study. SAGE Open Med. 2022;10:20503121221135874. doi:10.1177/20503121221135874
15. Guisado-Clavero M, Violán C, López-Jimenez T, et al. Medication patterns in older adults with multimorbidity: a cluster analysis of primary care patients. BMC Fam Pract. 2019;20(1):82. doi:10.1186/s12875-019-0969-9
16. Aggarwal P, Woolford SJ, Patel HP. Multi-morbidity and polypharmacy in older people: challenges and opportunities for clinical practice. Geriatrics. 2020;5(4):85. doi:10.3390/geriatrics5040085
17. Zhang N, Lin Q, Jiang H, et al. Age-adjusted Charlson comorbidity index as effective predictor for in-hospital mortality of patients with cardiac arrest: a retrospective study. BMC Emerg Med. 2023;23(1):7. doi:10.1186/s12873-022-00769-4
18. Abdulah R, Insani WN, Putri NE, et al. Pattern of medication use in geriatric patients at primary health care facilities in Karawang, Indonesia. Drug Healthc Patient Saf. 2019;11:1–5. doi:10.2147/DHPS.S187829
19. Manirajan P, Sivanandy P. Drug utilisation review among geriatric patients with noncommunicable diseases in a primary care setting in Malaysia. Healthcare. 2023;11(12):1665. doi:10.3390/healthcare11121665
20. Guo J, Huang X, Dou L, et al. Aging and aging-related diseases: from molecular mechanisms to interventions and treatments. Sig Transduct Target Ther. 2022;7:391. doi:10.1038/s41392-022-01251-0
21. Akkawi ME, Mohd Taufek NH, Abdul Hadi AD, et al. The prevalence of prescribing medications associated with geriatric syndromes among discharged older adults patients. J Pharm Bio Allied Sci. 2020;12(Suppl 2):S747–S751. doi:10.4103/jpbs.JPBS_305_19
22. Ali T, Haq NU, Razaque G, et al. Drug utilization pattern in older adults hospitalized patients in tertiary care hospitals of Quetta, Pakistan. J Pharm Pract Community Med. 2022;8(2):26–33. doi:10.5530/jppcm.2022.2.7
23. Jyothsna CS, Nagarajaiah BH, Shivakumar KM. Drug utilization pattern in geriatric inpatients of medicine wards at a government tertiary care hospital. Natl J Physiol Pharm Pharmacol. 2019;9(4):320–327. doi:10.5455/njppp.2019.9.0102607022019
24. Alshakka MA, Badullah WF, Sultan OA, et al. Prescribing patterns of non-steroidal anti-inflammatory drugs (NSAIDs) at outpatient departments of four hospitals. Biomed Res. 2018;29(19):3643–3647. doi:10.4066/biomedicalresearch.29-18-1072
25. Anandan I, Selvaraj N, Anandabaskar N, et al. Assessment of drug use pattern of nonsteroidal anti-inflammatory drugs using the World Health Organization core indicators in a tertiary care teaching hospital: a cross-sectional study. Natl J Physiol Pharm Pharmacol. 2019;9(10):1021–1026. doi:10.5455/njppp.2019.9.0726201082019
26. Kandasamy G, Almaghaslah D, Almanasef M, et al. A study of prescribing patterns for non-steroidal anti-inflammatory drugs in a tertiary care teaching hospital. Indian J Pharm Sci. 2021;83(2):287–292. doi:10.36468/pharmaceutical-sciences.774
27. Al-Taie A, Hussein AN, Albasry Z. Prescription pattern of non-steroidal anti-inflammatory drugs (NSAIDs) among community patients with musculoskeletal and co-morbid conditions: a cross-sectional study from an Iraqi province. Trop J Pharm Res. 2021;20(1):203–210. doi:10.4314/tjpr.v20i1.29
28. Khalil V, Wang W, Charlson L, et al. Evaluation of prescribing patterns of nonsteroidal anti-inflammatory agents in a tertiary setting. Int J Evid Based Healthc. 2019;17(3):164–172. doi:10.1097/XEB.0000000000000173
29. Bakrin FS, Makmor-Bakry M, Che Hon WH, et al. Defined daily dose and appropriateness of clinical application: the coxibs and traditional nonsteroidal anti-inflammatory drugs for postoperative orthopaedics pain control in a private hospital in Malaysia. Pharmacy. 2020;8(4):235. doi:10.3390/pharmacy8040235
30. Sohail R, Mathew M, Patel KK, et al. Effects of Non-steroidal Anti-inflammatory Drugs (NSAIDs) and gastroprotective NSAIDs on the gastrointestinal tract: a narrative review. Cureus. 2023;15(4):e37080. doi:10.7759/cureus.37080
31. Tai FWD, McAlindon ME. Non-steroidal anti-inflammatory drugs and the gastrointestinal tract. Clin Med Lond. 2021;21(2):131–134. doi:10.7861/clinmed.2021-0039
32. Narayanan M, Reddy KM, Marsicano E. Peptic ulcer disease and helicobacter pylori infection. Mo Med. 2018;115(3):219–224.
33. Mohamed MR, Mohile SG, Juba KM, et al. Association of polypharmacy and potential drug-drug interactions with adverse treatment outcomes in older adults with advanced cancer. Cancer. 2023;129(7):1096–1104. doi:10.1002/cncr.34642
34. Sheikh-Taha M, Asmar M. Polypharmacy and severe potential drug-drug interactions among older adults with cardiovascular disease in the United States. BMC Geriatr. 2021;21(1):233. doi:10.1186/s12877-021-02183-0
35. Alhumaidi RM, Bamagous GA, Alsanosi SM, et al. Risk of polypharmacy and its outcome in terms of drug interaction in an older adults population: a retrospective cross-sectional study. J Clin Med. 2023;12(12):3960. doi:10.3390/jcm12123960
36. Hermann M, Carstens N, Kvinge L, et al. Polypharmacy and potential drug-drug interactions in home-dwelling older people - a cross-sectional study. J Multidiscip Healthc. 2021;14:589–597. doi:10.2147/JMDH.S297423
37. Surya Prabha KJ, Vijaya K, Sai SP, et al. Pattern of poly pharmacy among geriatric patients in a tertiary care teaching hospital: a cross-sectional study. J NTR Univ Health Sci. 2022;11:1–5. doi:10.4103/jdrntruhs.jdrntruhs_133_20
38. Yogavigneshwaran CP, Maheshwari UR, Biju GB, et al. An Interpretation of Polypharmacy and Prescription Pattern in geriatric patients: a prospective observational study. Eur Chem Bull. 2023;12(SP1):4565–4578. doi:10.31838/ecb/2023.12.s1-B.451
39. Wannawichate T, Limpawattana P. Potential drug-drug interactions and related factors among geriatric outpatients of a tertiary care hospital. Geriatrics. 2023;8(6):111. doi:10.3390/geriatrics8060111
40. Liu Y, Wang J, Gong H, et al. Prevalence and associated factors of drug-drug interactions in older adults outpatients in a tertiary care hospital: a cross-sectional study based on three databases. Ann Transl Med. 2023;11(1):17. doi:10.21037/atm-22-5463
41. Engin S, Barut E, Sezen F, Yarış E. Evaluation of potential drug-drug interactions in the prescriptions in outpatient settings. TJFMPC. 2020;14(4):564–571. doi:10.21763/tjfmpc.713208
42. Hines LE, Murphy JE. Potentially harmful drug-drug interactions in the older adults: a review. Am J Geriatr Pharmacother. 2011;9(6):364–377. PMID: 22078863. doi:10.1016/j.amjopharm.2011.10.004
43. Zerah L, Henrard S, Wilting I, et al. Prevalence of drug-drug interactions in older people before and after hospital admission: analysis from the OPERAM trial. BMC Geriatr. 2021;21(1):571. doi:10.1186/s12877-021-02532-z
44. Shetty V, Chowta MN, Chowta KN, et al. Evaluation of potential drug-drug interactions with medications prescribed to geriatric patients in a tertiary care hospital. J Aging Res. 2018;2018:5728957. doi:10.1155/2018/5728957
45. Chaudhari D, Chaudhary H. Usage of Non-Steroidal Anti-Inflammatory Drugs (NSAIDS) and their interaction with other concurrently used drugs in older adults patients. J Sur Fish Sci. 2023;10(4S):946–953. doi:10.17762/sfs.v10i4S.1086
46. Adem L, Tegegne GT. Medication appropriateness, polypharmacy, and drug-drug interactions in ambulatory older adults patients with cardiovascular diseases at Tikur Anbessa Specialized Hospital, Ethiopia. Clin Interv Aging. 2022;17:509–517. doi:10.2147/CIA.S358633
47. Mehuys E, De Backer T, De Keyser F, et al. Prevalence and management of drug interactions between nonsteroidal anti-inflammatory drugs and antithrombotics in ambulatory care. Br J Clin Pharmacol. 2022;88(8):3896–3902. doi:10.1111/bcp.15288
48. Rabba AK, Abu Hussein AM, Abu Sbeih BK, et al. Assessing drug-drug interaction potential among patients admitted to surgery departments in three Palestinian Hospitals. Biomed Res Int. 2020;2020:9634934. doi:10.1155/2020/9634934
49. Vegada BN, Shah AM, Shah D, et al. Polypharmacy and potential drug-drug interactions among geriatric patients. Natl J Physiol Pharm Pharmacol. 2020;10(5):393–399.
50. Rasool MF, Rehman A, Khan I, et al. Assessment of risk factors associated with potential drug-drug interactions among patients suffering from chronic disorders. PLoS One. 2023;18(1):e0276277. doi:10.1371/journal.pone.0276277
51. Epi Info™ calculator. Available from: https://www.cdc.gov/epiinfo/support/downloads.html.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.