Back to Journals » Journal of Blood Medicine » Volume 15
Evaluation of IgG and Complement Component C4 Levels in Low-Income Countries, Yemen Republic in Light of Their Proposed Role in the Hemolysis of Stored CPDA-1 Whole Blood
Authors Obaid JM ![]() , Sakran KA, Mohammed SA, Al-Salahi SL, Mahdi NA, AL-Sharabi MA, AL-Gaadi AS, AL-Fatahi MN
, Sakran KA, Mohammed SA, Al-Salahi SL, Mahdi NA, AL-Sharabi MA, AL-Gaadi AS, AL-Fatahi MN
Received 21 June 2024
Accepted for publication 21 October 2024
Published 27 October 2024 Volume 2024:15 Pages 459—469
DOI https://doi.org/10.2147/JBM.S472605
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Jamil MAS Obaid,1,2 Khawla AAS Sakran,2 Shaima AH Mohammed,1 Shifa`a LA Al-Salahi,1 Nawal AN Mahdi,1 Mohammed AM AL-Sharabi,1 Asadaddin SM AL-Gaadi,2 Mohammed NM AL-Fatahi2
1Department of Medical Laboratory Sciences, Faculty of Medicine and Health Sciences, Ibb University, Ibb, Yemen; 2Department of Medical Microbiology, Faculty of Science, Ibb University, Ibb, Yemen
Correspondence: Jamil MAS Obaid, Ibb University, Assalaba, Ibb, Yemen, Email [email protected]; [email protected]
Objective: Hemolysis is the most severe change that occurs in stored blood and can cause severe consequences in patients after transfusion. This study examines the potential role of IgG and complement, exampled by C4, in the hemolysis of stored CPDA-1 blood under poor storage conditions in low-income countries.
Methods: The study was performed on 30 whole blood units (250 mL) drawn from convenience healthy volunteer donors with CPDA-1 anticoagulant and stored at 2– 6 °C for 35 days. Each well-mixed blood bag was sampled at 0, 7, 21 and 35 days and examined for CBC, plasma hemoglobin, hemolysis percent and determination of IgG and C4.
Results: The plasma hemoglobin level and hemolysis percent increased continuously to reach 1.56 g/dl and 7.05% at the end of storage time. Hemolysis increased alongside the mean IgG concentration that was increased significantly from day 0 of storage (7.68± 1.75 g/L) and peaked on day 7 (11.55± 1.57 g/L), then declined to reach 8.33± 2.09 g/L on day 35. Also, the mean concentration of C4 increased from day 0 of storage (0.15± 0.06 g/L) to a peaked on day 21 (0.18± 0.04) then declined on day 35 (0.17± 0.06 g/L). The coordinated action of IgG and C4 is reflected by the positive correlation of their delta changes (r=0.616, p< 0.0001).
Conclusion: Elevated hemolysis percent in whole CPDA-1 stored blood in Yemen was accompanied by initial increase of IgG and C4 followed by final decline, which indicate their activation and consumption during hemolysis. Further studies for other hemolysis markers and analyses will give a full idea about that.
Keywords: IgG, complements, hemolysis, CPDA-1 blood, transfusion
Introduction
Transfusion represents a suitable therapy for the treatment of critically ill anemic patients. Whole blood transfusion for anemic patients is still the first type of blood product used in most developing countries, including Yemen, which has been in war for 9 years.1 Despite its essential use in the treatment of some situations, such as acute blood loss in accidents and shots, the use of whole blood in other cases contributes to meeting the need for blood. Some data suggest that the gap between need and supply in low-income and middle-income countries is large, and the WHO also targets 10–20 donations per 1000 people for many countries.2 A study of blood transfusion among pediatric patients in Aden city, Yemen, reported a frequency of 26.4% for whole blood transfusions.3 Blood transfusion in Yemen is carried out with a little improvement, most clinical transfusion therapy uses whole blood, and little components are produced (only packed RBCs and platelet-rich plasma) at a narrow range.
During storage, many changes affect many components and aspects of blood. Preservatives such as citrate phosphate dextrose adenine (CPDA-1) were used to ameliorate these changes and extend the lifespan of red blood cells (RBCs).4 Changes in RBCs may be attributed to the storage conditions (mainly a storage temperature that must be ranging from 2–6 °C) and donor attributes, which are reflected in donated blood.5,6 The previously reported causes of changes in stored blood are metabolite accumulation or depletion and oxidative damage that eventually leads to increased red cell hemolysis.7 Most biochemical and cellular changes include increased intracellular potassium, increased cytoplasmic sodium, decreased glucose, decreased pH, changes in RBC morphology and membrane protein composition, and the production of harmful membrane fragments, microparticles, and free hemoglobin.8,9 However, the effects of blood storage time and the extent to which stored blood is safe and potent remain the main issues of debate. Prolonged blood storage increases mortality, serious infections, and multiorgan failure after transfusion.10
RBC hemolysis in stored blood bags occurs during blood collection, processing, handling and storage. RBC hemolysis above the accepted level (1% according to international guidelines) is a marker of RBC storage failure.11 RBCs are very fragile as they age, and consequently, cell-free hemoglobin and microparticles are released. Cell-free hemoglobin and microparticles lead to further hemolysis and breakdown of RBCs.12 Leukocytes contribute to hemolysis through the release of various chemicals and enzymes, especially proteases. Therefore, the use of leukocyte reduction filters decreases the hemolysis rate in stored blood.13
The induction of immunological mechanisms may be indicated by many marker changes in stored blood that can be initiated by antibody sensitization of red blood cells followed by complement activation via the classical pathway. For instance, it was reported that leukocyte-reduction filtration decreases the hemolysis rate.14 Thielen et al, in their in vitro study, showed that RBCs in stored blood were sensitized by antibodies and complement independent of storage time.15 In vivo, leukocytes can increase humoral responses activated by T-helper-2.16 This study examines the potential role of IgG and complement components (C4, a prototype component of the classical activation pathway) in the hemolysis of stored CPDA-1 blood under poor storage conditions in low-income countries.
Methods
Overview of the Study
This prospective experimental study was conducted at the Faculty of Medicine and Health Sciences-Ibb University, Yemen, for the period from May 31, 2023, to July 5, 2023. The study was performed on whole blood units (250 mL) that were drawn from suitable healthy volunteer donors into a CPDA-1 anticoagulant-containing single blood bag and stored to the expired date after 35 days.
A convenience sample was used to select participants. After checking the donor eligibility requirements, 30 donors were selected; 7 of them were females, and 23 were males with all ABO phenotypes. The donors were aged between 18 and 33 years. Informed consent was obtained from each healthy volunteer verbally. This study was conducted according to the international ethical guidelines of medical research, mainly the Declaration of Helsinki–ethical principles for medical research involving human subjects, in 2013.
The inclusion criteria included healthy donors who met the whole blood donation eligibility requirements, who were aged at least 18 years, who had a normal hemoglobin level, and who were free from disease for at least 6 months. The exclusion criterion for all donors was that they did not meet the eligibility requirements of the American Association of Blood Banks (AABB).
Experimental Design
A total of thirty healthy volunteer donors had the following ABO phenotypes: 9 with the A blood phenotype, 3 with the B phenotype, 7 with the AB phenotype, and 11 with the O phenotype. Eligible donors underwent venous blood collection for donation, with appropriate care and adequate safety precautions to prevent donor and worker infections and to avoid contamination of blood units. A total of 250 mL of blood was drawn from each volunteer donor in a single blood bag with approximately 35 mL of CPDA-1 as an anticoagulant. The blood was gently mixed during collection, immediately placed in a disinfected blood bank refrigerator and kept at 2–6 °C for 5 weeks (35 days).
During storage, approximately 10 mL of each well-mixed blood bag was collected aseptically at 0, 7, 21 and 35 days of storage. Each sample was analyzed for complete blood count (CBC) and then centrifuged for 10 min at 4000 rpm to obtain plasma. The plasma was used for the measurement of free plasma hemoglobin spectrophotometrically and, consequently, for the calculation of hemolysis percent. Part of the separated plasma was kept in an Eppendorf tube and immediately frozen at –20 °C for the analysis of IgG and complement C4.
ABO and Rh Blood Grouping
The ABO blood group of the donors was determined by direct agglutination testing using the anti-sera, anti-A, and anti-B reagents (Agappe, India).
Complete Blood Count
CBCs were analyzed for each sample on an automatic hematology analyzer (Sysmex XS-500i, Japan). A Sysmex XS-500i hematology analyzer was used for flow cytometry to analyze the physiological and chemical properties of the cells. All parameters of red blood cells, white blood cells and thrombocytes were obtained and reported properly on each examination day.
Plasma Hemoglobin Determination
The plasma Hb concentration was measured using the cyanmethemoglobin method by mixing 20 μL of plasma with 5 mL of Drabkin’s reagent (Hemoglobin Monlab test, Spain), and the absorbance was measured after 5 minutes spectrophotometrically at 540 nm (BTS–350, Biosystems, Spain).
Calculation of Hemolysis Percent
The percentage of hemolysis in the stored whole blood unit was calculated according to the following formula:

Immunoglobulin G and C4 Determination
The plasma samples were analyzed for IgG and C4 with an immunoturbidimetric assay technique using the IGG-2 CAN 674 and C4-2 Tina-quant kits (Roche Diagnostics, Germany) and an immunological analyzer Cobas c311 (Roche/Hitachi, Japan) at a wavelength of 340 nm.
Statistical Analysis
The data were analyzed using the IBM Statistical Package for Social Sciences (SPSS) version 19. The data were analyzed with descriptive statistics to determine the means, SDs, frequencies, and percentages, as appropriate. A t test or Mann‒Whitney rank sum test was used to analyze the difference between two groups, or ANOVA was used for more groups. Spearman correlation tests were used for correlation analyses. A p value ≤0.05 indicated statistical significance.
Results
The most important change in RBC parameters was an increase in the mean cell volume (MCV) from day 0 to the end of storage (from 81.52±5.29 fl to 87.70±6.08 fl, p=0.001). The red cell distribution width (RDW) also increased (from 12.66±1.13 to 14.97±1.18, p<0.0001). Moreover, the mean cell hemoglobin concentration (MCHC) decreased from 36.72±0.88 g/dl to 33.76±0.97 g/dl. (Table 1). WBCs showed a significant reduction in total count or as an individual absolute leukocyte type, except for lymphocytes, which increased in number with increasing incubation time. The mean thrombocyte count generally increased significantly from 177±39.65*109 PLTs/L to 290±113.87*109 PLTs/L during storage. Other parameters, such as the mean platelet volume (MPV), platelet distribution width (PDW) and platelet large cell ratio (P-LCR), also showed gradual increases compared with the baseline values on day 0. All these data are listed in Table 1.
 |
Table 1 Changes in the Mean CBC Parameters of the Stored CPDA-1 Whole Blood Samples During Storage |
The changes in the mean plasma hemoglobin level and the mean hemolysis percent of the stored blood are depicted in Figure 1. Both showed continuous elevation, with a statistically significant difference between measurements (p<0.0001). The continuous increase in these parameters was also significantly different among the different ABO phenotypes, except for B blood group patients, as listed in Table 2.
 |
Table 2 Changes in the Mean Plasma Hemoglobin Concentration and Hemolysis Percent of Donated Blood from Different ABO Blood Group Phenotypes During Storage |
 |
Figure 1 Changes in the mean plasma hemoglobin level and the mean hemolysis percent of the stored blood during storage. |
The mean immunoglobulin G level increased significantly from day 0 of storage (7.68±1.75 g/L) to day 7 (11.55±1.57 g/L) and then declined to 8.33±2.09 g/L on day 35, as illustrated in Figure 2. However, the mean complement C4 level increased insignificantly from day 0 of storage (0.15±0.06 g/L) to peak on day 21 (0.18±0.04) and declined on day 35 (0.17±0.06 g/L), as depicted in Figure 3. The delta changes in IgG levels moderately correlated with the delta changes in C4 levels (r=0.616, p<0.0001), as shown in Figure 4.
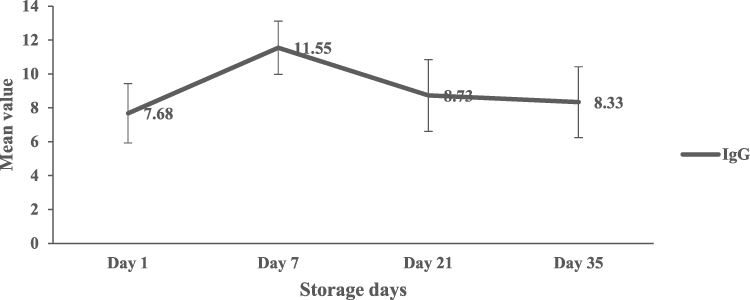 |
Figure 2 Changes in the mean IgG level in the stored blood during storage. |
 |
Figure 3 Mean C4 level change in the stored blood during the storage time. |
 |
Figure 4 Correlation analysis between delta change in IgG level and delta change in complement component C4 of CPDA-1 stored blood. |
The plasma hemoglobin and hemolysis percent which are strongly correlated (r= 0.954, p<0.0001), were positively correlated with the traditional affected variable MCV and platelet count and negatively correlated with the MCHC and absolute monocyte count (Figure 5). The IgG level was negatively correlated with MCH, MCHC and eosinophils but positively correlated with platelet count. Similarly, C4 was negatively correlated with MCH, MCHC and the absolute neutrophil count but positively correlated with the absolute lymphocyte count (Figure 6).
 |
Figure 5 Correlation analysis between plasma hemoglobin, hemolysis percent with MCV, platelet count, MCHC and absolute monocyte count of CPDA-1-stored blood. |
 |
Figure 6 Correlation analysis between the IgG and complement component C4 levels and the MCH, MCHC, absolute monocyte, eosinophil and lymphocyte counts in CPDA-1-stored blood. |
Discussion
Blood for transfusion must be kept at optimum storage conditions to achieve good posttransfusion survival of cells to fulfill their desired functions. The cellular and chemical changes that occur in stored blood have been studied and have yielded some recommendations for improving storage conditions. This study is a contribution in this field and assumes a potential role for IgG and complement proteins in the hemolysis of stored blood, taking into consideration the situation in low-income countries with limited resources, such as the Yemen Republic. One of these considerations is the transfusion of whole blood for most patients who must receive one blood component rather than whole blood because of the poor service of blood banks and the lack of double, triple and quadruple blood bags. Therefore, the preparation of blood components is unattainable. Similarly, whole blood transfusions are also performed in many centers in another low-income country, Nigeria.17
Blood storage in vitro causes cellular changes resulting in reduced red blood cell survival that may culminate in hemolysis. The accumulation of changes with increasing storage time was studied for the extent to which red blood cells lost their safety and efficacy and for the increased risk of transfusion complications when transfused blood was stored for long periods even before the expiry date.18,19 Stored red blood cells undergo hemolysis and microparticle formation, which is an ever-dangerous change. Moreover, hemolysis increased significantly over time in the stored blood,20 which is in accordance with our results showing that hemolysis changes progresses during storage. Hemoglobin in microparticles that is released from hemolysis may represent a common factor driving multiple pathways leading to negative consequences; these pathways include oxidative stress, nitric oxide depletion and platelet activation.21
An increase in the MCV and RDW and a logic decrease in the MCHC are the traditional significant changes in RBC parameters reported here as well as in both previous and recent studies.22–24 The total WBC count, absolute monocyte and eosinophil counts were decreased, in agreement with the findings of a previous study that attributed this decrease to the degeneration of leukocytes.25 An increase in the mean absolute lymphocyte count may be due to an artifactual cause, where the leukocytes prepared for apoptosis condense their nucleus and decrease in size, which may give these cells a small lymphocyte appearance; hence, they may be counted as lymphocytes. Surprising changes were observed in the platelet count and indices. An increase in the PLT is artifactual and is attributed to an increase in the number of microvesicles or microparticles released from RBCs and WBC fragmentation during storage. Because of their similar sizes, fragments may be counted as platelets by a hematology analyzer. Another possibility is the reversal of the aggregation process that may occur for platelets under warming conditions during sampling.26
As mentioned previously, hemolysis is the worst manifestation of red cell lesions during storage, and the most important marker determines the suitability of blood for transfusion. The parallel increase in plasma hemoglobin and hemolysis percent with advance storage time was predicted to occur as a result of red cell storage damage. This was also reported in this study, as well as in previous studies. It is the greatest change occurred during the last week of storage.26–28 Hemolysis was not associated with a certain ABO phenotype despite the lack of a statistically significant difference in the changes in plasma hemoglobin and hemolysis percent among B blood group donors, which may be attributed to the small sample size. Both markers were positively correlated with the conventional marker MCV and platelet count and inversely correlated with the MCHC. Plasma hemoglobin and hemolysis percent were associated by a moderate negative correlation with the absolute monocyte count, this may refer to monocyte consumption in phagocytosis activity.
The high hemolysis rate in this study—above the internationally accepted limits, FDA accepted level is 1% —is related to poor storage conditions, including an unstable electrical power supply for refrigerators and deterioration of the collection bags quality due to difficulties of their importing and transporting processes in low-income countries. In terms of the biological mechanisms responsible for hemolysis, leukocytes contribute significantly to hemolysis via several pathways. Leukocyte release of various chemicals and enzymes, especially proteases that cause red cell lysis, using leukocyte reduction filters decreases the rate of this hemolysis in stored blood units.27 Unfortunately, leukoreduction is rarely performed during blood transfusion in Yemen.
This study showed a gradual increased IgG level and complement C4 components during storage. Increased IgG level with storage in non-leukoreduced blood was also proved in agreement with our result by Antonelou et al,29 Therefore, these findings lead our hypothesis that suggest IgG and complement contribution in hemolysis of the stored blood by an immune mechanism start by IgG binding to RBCs and consequent complement activation via classical pathway. This mechanism culminates in red cell lysis. Storage causes continuous decrease of red cell hemoglobin content (decrease MCHC) and its precipitation on red cell that may alter the membrane leading to red cell sensitization by IgG and complement activation. Thus, this study showed a negative correlation between IgG and C4 levels and MCHC. The deposition of IgG and complement component C3 on stored RBCs has been proven previously, despite the limited uptake and phagocytosis by macrophages in vitro, according to Thielen et al.15 Meanwhile, Hult et al proved that in vitro phagocytosis of red blood cells can occur in the presence of serum.30 Therefore, the presence of serum will activate macrophage as the situation in this study. IgG binding and complement activation on RBCs develop because of membrane alterations of the stored red cells was proved previously.31 An important supportive results are the manner by which IgG and complement changed. The reasonable and coordinated suggested scenario is the gradual increase of IgG firstly peaked on day 7 to sensitize red cells, this is followed also by a gradual increase in C4 component peaked on day 21, both of which were declined later. The final decline in these markers denotes their consumption after activation. The coordinated increase in both markers was evidenced by the direct correlation between the delta change in the IgG level and the delta change in complement component C4 (r=0.661, p<0.0001).
Antibody-dependent cell-mediated cytotoxicity and opsonization mechanisms can also be suggested. The supportive results were the negative correlations between C4 and neutrophil count, between IgG and eosinophil count, and between plasma hemoglobin and hemolysis percent with monocyte count. Phagocytosis of sensitized cells by antibodies and complement may also lead to phagocyte cell exhaustion and apoptosis, as proposed by Frankenberg et al.32
The limitation of this study lies in the lack of financial support to explore additional markers of hemolysis in relation to the supposed immune mechanisms studied in this paper. Additional analyses are needed to explore certain immune mechanisms in the hemolysis of stored blood using more markers and advanced techniques. Furthermore, the findings of this in vitro study cannot be exactly translated to what we would expect in vivo without performing clinical trial studies. It is recommended to generalize leukoreduction strategy in all transfusion centers, also transfuse blood units as early as possible before the expiry date to avoid the bad effects of storage.
In conclusion, the higher hemolysis percent in whole CPDA-1 stored blood in Yemen, a low-income country, warrants further investigations for implicated mechanisms and prevention strategies. The immunological mechanism of hemolysis mediated by IgG and the ensued complement activation via the classical pathway in the whole CPDA-1 stored blood is strongly suggestive in this study and pronounced by their final decrease (due to consumption) after initial increase (due to activation). Plasma presence and non-leukodepletion in this blood units also enhance the phagocytic activity of macrophages in blood units. Further studies for other hemolysis indicators and analyses will provide us with a full idea about that.
Abbreviations
CBC, complete blood count; IgG, immunoglobulin; CPDA-1, citrate phosphate dextrose adenine; AABB, American Association of Blood Banks; SPSS, Statistical Package for Social Sciences; ANOVA, analysis of variance; MCV, mean cell volume; RDW, red cell distribution width; MCHC, mean cell hemoglobin concentration; MPV, mean platelet volume; PDW, platelet distribution width; P-LCR, platelet large cell ratio, PLTs; platelets.
Data Sharing Statement
All data are available in this manuscript.
Ethical issue
This study was conducted under the approval of ethical committee at the Medical Laboratory Sciences Department at the Faculty of Medicine and Health Sciences, Ibb University (Ethical approval No. 13-MLS-Feb. 2023). An informed consent for all donors was taken verbally with authorization from Ethical Committee because all donors were students at our faculty and belong to our scientific community, verbal consent in this community is sufficient. They are in daily contact with the ethical committee. A third-party witness, the faculty’s general manager, was present during the donation procedure and told the committee. All research processes also committed to the international ethical guidelines of medical research, mainly the Declaration of Helsinki–ethical principles for medical research involving human subjects, in 2013.
Acknowledgments
The authors would like to acknowledge the contributions of the investigators: Eissa A. Al- Mousami, Deia’a M.A. Al-Bukhaiti, Najeeb A. Al-Hayani, Azzam S. Al- Jaberi, Dalal M. Noman, Suhaira D. Al-Salami, Ebtehal A. Al-Sabahi, Rayan S. Shamakh, Abdulkhalik A. Almaddah, Abdulmalik M. Almusali, Mujeeb M. Dawi, Ibraheem A. Alkhulaidy, Radwan M. Alshahry, Mohammed H. Dawi, Rabie M. Alharemi, Osama M. Alnajm.
Funding
The authors did not receive any funding.
Disclosure
The authors have disclosed no conflicts of interest.
References
1. Erhabor O, Adias TC. From whole blood to component therapy: the economic, supply/demand need for implementation of component therapy in sub-Saharan Africa. Transfus Clin Biol. 2011;18(5–6):516–526. doi:10.1016/j.tracli.2011.06.001
2. Roberts N, James S, Delaney M, et al. The global need and availability of blood products: a modelling study. Lancet Haematol. 2019;6(12):e606–e615. doi:10.1016/S2352-3026(19)30200-5
3. Al-Saqladi AM. Albanna TA. A study of blood transfusion in pediatric patients at a teaching hospital, Aden. Yemen Interl J Clinic Transf Med. 2021(9):1–9.
4. Hess JR. An update on solutions for red cell storage. Vox Sang. 2006;91(1):13–19. doi:10.1111/j.1423-0410.2006.00778.x
5. Yoshida T, Prudent M, A D. Red blood cell storage lesion: causes and potential clinical consequences. Blood Transfus. 2019;17(1):27–52. doi:10.2450/2019.0217-18
6. Tzounakas VL, Georgatzakou HT, Kriebardis AG, et al. Donor variation effect on red blood cell storage lesion: a multivariable, yet consistent, story. Transfusion. 2016;56(6):1274–1286. doi:10.1111/trf.13582
7. McAteer MJ, Dumont LJ, Cancelas J, et al. Multi-institutional randomized control study of haemolysis in stored red cell units prepared manually or by an automated system. Vox Sang. 2010;99:34–43. doi:10.1111/j.1423-0410.2010.01313.x
8. Oyet C, Okongo B, Apecu-Onyuthi R, et al. Biochemical changes in stored donor units: implications on the efficacy of blood transfusion. J. Blood Med. 2018;9:111–115. doi:10.2147/JBM.S163651
9. W‒W T, Wang D, Liang W-J, et al. How Cell Number and Cellular Properties of Blood-Banked Red Blood Cells of Different Cell Ages Decline during Storage. PLoS One. 2014;9(8):e105692. doi:10.1371/journal.pone.0105692
10. Sheppard CA, Josephson CD, Hillyer CD. Bacterial Contamination of Platelets for Transfusion: recent Advances and Issues. Labmedicine. 2005;36(12):767–770.
11. Janatpour KA, Paglieroni TG, Crocker VL, et al. Visual assessment of hemolysis in red cell units and segments can be deceptive. Transfusion. 2004;44:984–989. doi:10.1111/j.1537-2995.2004.03315.x
12. Kim-Shapiro DB, Lee J, Gladwin MT. Storage lesion: role of red blood cell breakdown. Transfusion. 2011;51(4):844–851. doi:10.1111/j.1537-2995.2011.03100.x
13. Mustafa I, Al Marwani A, Mamdouh Nasr K, et al. Time Dependent Assessment of Morphological Changes: leukodepleted Packed Red Blood Cells Stored in SAGM. Biomed Res Int. 2016;2016:4529434. doi:10.1155/2016/4529434
14. Gammon RR, Strayer SA, Avery NL, et al. Hemolysis during leukocyte-reduction filtration of stored red blood cells. Ann Clin Lab Sci. 2000;30(2):195–199.
15. Thielen AJF, Meulenbroek EM, Baas I, et al. Complement Deposition and IgG Binding on Stored Red Blood Cells Are Independent of Storage Time. Transfus Med Hemother. 2018;45(6):378–384. doi:10.1159/000486759
16. Aguilar-Nascimento JE, Zampieri-Filho JP, Bordin JO. Implications of perioperative allogeneic red blood cell transfusion on the immune-inflammatory response. Hematol Transfus Cell Ther. 2021;43:58–64. doi:10.1016/j.htct.2020.03.003
17. Oluyombo A, Oluyombo O, Uchegbu OO, et al. Quantitative assessment of erythrocytes and leukocytes in CPD-A stored blood. Biomed Res. 2014;24(4):503–508.
18. Weinberg JA, Mc Gwin JG, Griffin RL, et al. Age of transfused blood: an independent predictor of mortality despite universal leukoreduction. J Trauma Acute Care Surg. 2008;65(2):279–284. doi:10.1097/TA.0b013e31817c9687
19. Koch CG, Li L, Sessler DI, et al. Duration of red-cell storage and complications after cardiac surgery. N Engl J Med. 2008;358(12):1229–1239. doi:10.1056/NEJMoa070403
20. Ozment CP, Mamo LB, Campbell ML, et al. Transfusion-related biologic effects and free hemoglobin, heme, and iron. Transfusion. 2013;53(4):732–740. doi:10.1111/j.1537-2995.2012.03837.x
21. Lee J, Gladwin M. Bad Blood: the risks of red cell storage. Nat Med. 2010;16:381–382. doi:10.1038/nm0410-381
22. Ghezelbash B, Azarkeivan A, Pourfathollah AA, et al. Comparative evaluation of biochemical and hematological parameters of pre-storage leukoreduction during RBC storage. Intl J HemaOnc Stem Cell Res. 2018;12(1):35.
23. Noguira D, Rocha S, Abreu E, et al. Biochemical and cellular changes in leukocyte depleted red blood cells stored for Transfusion. Transfu Med Hemotherapy. 2015;42(1):46–51. doi:10.1159/000370140
24. Salzer U, Zhu R, Luten M, et al. Vesicles generated during storage of red cells are rich in the lipid raft marker stomatin. Transfusion. 2008;48(3):451–462. doi:10.1111/j.1537-2995.2007.01549.x
25. Al Nuaimy MIK. Haematological Changes in Stored Blood. Journal of Education and Science. 2008;21(4):49–56. doi:10.33899/edusj.2008.56106
26. Sivertsen J, Hervig T, Strandenes G, et al. In vitro quality and hemostatic function of cold-stored CPDA −1 whole blood after repeated transient exposure to 28°C storage temperature. Transfusion. 2022;62(Suppl 1):S105–S113. doi:10.1111/trf.16970
27. Arif SH, Yadav N, Rehman S, et al. Study of Hemolysis During Storage of Blood in the Blood Bank of a Tertiary Health Care Centre. Indian J Hematol Blood Transfus. 2017;33(4):598–602. doi:10.1007/s12288-016-0769-5
28. Tzounakas VL, Anastasiadi AT, Karadimas DG, et al. Temperature-dependent haemolytic propensity of CPDA-1 stored red blood cells vs whole blood - Red cell fragility as donor signature on blood units. Blood Transfus. 2017;15(5):447–455. doi:10.2450/2017.0332-16
29. Antonelou MH, Tzounakas VL, Velentzas AD, Stamoulis KE, Kriebardis AG, Papassideri IS. Effects of pre-storage leukoreduction on stored red blood cells signaling: a time-course evaluation from shape to proteome. J Proteomics. 2012;76:220–238. doi:10.1016/j.jprot.2012.06.032
30. Hult A, Toss F, Malm C, Oldenborg PA. In vitro phagocytosis of liquid-stored red blood cells requires serum and can be inhibited with fucoidan and dextran sulphate. Vox Sang. 2020;115(8):647–654. doi:10.1111/vox.12922
31. Kamhieh-Milz J, Bartl B, Sterzer V, et al. Storage of RBCs results in an increased susceptibility for complement-mediated degradation. Transfus Med. 2014;24:392–399. doi:10.1111/tme.12166
32. Frankenberg T, Kirschnek S, Häcker H, et al. Phagocytosis-induced apoptosis of macrophages is linked to uptake, killing and degradation of bacteria. Eur J Immunol. 2008;38(1):204–215. doi:10.1002/eji.200737379
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.