Back to Journals » Open Access Emergency Medicine » Volume 14
Evaluation of Essential and Emergency Surgery Provide in Primary Hospitals of Gedeo Zone and Sidama Region, South, Ethiopia, 2020
Authors Regasa T ![]() , Zemedkun A, Neme D
, Zemedkun A, Neme D
Received 8 June 2022
Accepted for publication 13 September 2022
Published 19 September 2022 Volume 2022:14 Pages 507—514
DOI https://doi.org/10.2147/OAEM.S371509
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Teshome Regasa, Abebayehu Zemedkun, Derartu Neme
Anesthesiology Department, Dilla University, Dilla, Ethiopia
Correspondence: Teshome Regasa, Tel +251 910563710, Email [email protected]
Background: Surgical services at level referral hospitals were an essential part of overall health care. The surgical uhservice was approximated to account for 11% of the worldwide load of disease, with a large percentage of that burden being uncovered in resource-constraint settings. Even though the surgery service is significant and growing across all economic sectors, the majority of resource-limited countries have been unable to provide essential surgical services.
Objective: To investigate the capacity of essential and emergency surgical services in primary hospital facilities in the Gedeo zone and Sidama region.
Methodology: In the Gedeo zone and Sidama region, a cross-sectional study was undertaken in eight district hospitals. By looking at four areas of data: infrastructure, human resources, interventions available, and equipment, a World Health Organization tool for conditional analysis was used to assess a health set-up competence to perform essential surgical and anesthetic procedures. The tool looked for eight different categories of healthcare giving 35 surgical procedures, and 67 different pieces of instruments.
Results: This research found that 48.57% of the 35 essential interventions counted in the test, including cesarean section, were available at all hospitals. Prior to admission, each hospital reported a total of 53 beds, with an average travel distance of 28 kilometers. There were 189 healthcare providers in the eight facilities. According to the research, basic instruments were not always present at all of the sites.
Conclusion: Infrastructure, health profession, service supply, and key instruments and supplies deficiencies reveal major inadequacies in hospitals’ capacity to perform EESC and efficiently treat the growing surgical load of disease and damage in primary care.
Keywords: burden of emergency surgery, emergency and essential surgery, emergency and urgent surgical treatment
Background Information
Argent and emergency surgical services belong to procedures that are essential in averting premature morbidity and disability in a positive situation. Surgery management at primary hospitals was an essential portion of thorough health care. The worldwide load of surgical services is constantly increasing, with third-world countries bearing an equal share of the load.1
According to the report, 321 million surgeries will be necessary for 2010 to alleviate the sickness load of 69% global population. The minimal surgical demand varies by region, rating between 3383 procedures per 100,000 in South America to 6495 in western Sub-Saharan Africa. There were 131,412 surgeries for food-related shortages and 458 million treatments for unexpected accidents in the global surgical demand. Worldwide, an estimated five billion individuals lack immediate, conserve, and low-cost surgery and anesthesia procedures. This condition is magnified in third-world countries, where only 6.5% of surgical activities were undergone in low-income nations. To improve activities for surgical treatments in the poorest nations, a systematic technique is required.2,3
Death and disability rates from curable surgical illnesses remain unacceptably high in the poorest nations. Young adults were disproportionately affected by injuries (vehicle accidents, burns, and falls), infections (osteomyelitis and septic arthritis), and a variety of gastrointestinal problems, which inflict a considerable financial burden on society. Surgical situations hold up to 11% of all damage-related life years in the world. Providing safe, timely, and effective surgical care is hampered by a lack of infrastructure, as well as a scarcity of physical and human resources.4
Ethiopia’s maternal mortality ratio (MMR) remains high, according to a recent study. Ethiopia falls short of the millennium development goals (MDGs) objective for maternal mortality ratio, according to the findings. Anesthetic difficulties, postpartum cardiac problems, preterm delivery, maternal hemorrhage, pregnancy-induced hypertension, and maternal septic shock were all among the highest cause of parturients mortality. Argent maternal service, which frequently necessitates conserved and operatable surgical and/or anesthetic management, can address these issues.5
For decades, Ethiopia has been suffering from a severe scarcity of gynecologists and surgeons. In 2011, 606 total experts were working in the public health sector, with one specialist for every 54,000 people. The majority’s lack of access to these specialists is likely to have played a role in the high maternal and neonatal death and morbidity rates.6–8 Assessing the capacity of Gedeo zone and Sidama region hospitals for essential and emergency surgical care is the research question.
Materials and Methodology
Study Area, Design, and Period
The study was carried out in the Gedeo zone and Sidama region. Gedeo zone is found in Southern Nation Nationalities and Peoples Regional (SNNPR) states of Ethiopia at 359 km Southern of Addis Ababa (the capital city of Ethiopia). It has five woredas and two city administrations. There are 3 primary hospitals. Sidama region is found in Southern states of Ethiopia at 269 km Southern of Addis Ababa. There are 13 primary hospitals. The distribution of resources to the primary hospitals from the government was almost similar throughout the country. From May to July 2020, a cross-sectional investigation was undertaken. The Dilla University institutional review board provided ethical clearance. Every hospital that was involved in the project gave their informed consent. All active operating rooms in Gedeo and Sidama hospitals were involved in the study, while hospitals categorized for the corona treatment were excluded from the study. In the Gedeo zone and Sidama region, there were 16 primary hospitals. Eight hospitals were chosen by lottery from a pool of 16, giving all primary hospitals a 50% chance of being included in the trials. Argent and essential surgical service (AESS) capacity were assessed from hospitals in the Gedeo zone and Sidama area using the WHO integrated management for argent and critical surgical care (IMEESC) toolbox. Infrastructure, health professionals, and EESC instruments and supplies were investigated to evaluate the hospitals’ efficiency. The tool checks for eight8 different kinds of service providers, 35 surgical management, and 67 different pieces of instruments. The tool was provided to eight government hospitals in the Gedeo zone and Sidama region, and trained data collectors finished it at whole health services.10 After the data was collected, it was manually checked for mistakes before being imported into the software for evaluation. The indices were calculated using descriptive statistics.
Result
Wando primary hospital had the highest population service of over 200,000 people, followed by Cheffe primary hospital with around 170,000 people (Table 1).
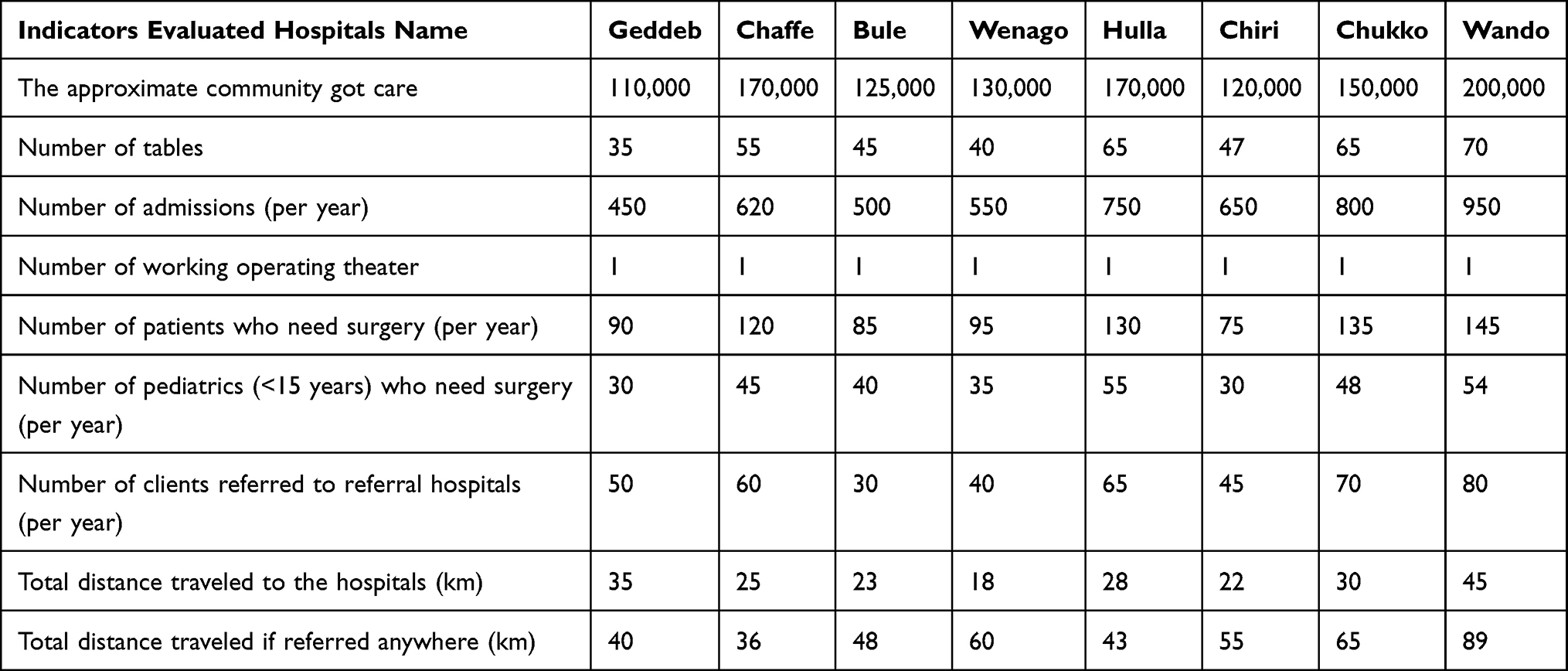 |
Table 1 Profile of Surveyed Hospitals. (n=8) |
The majority of the district hospitals in the Gedeo zone and Sidama region were served by clinical officers who provided surgery (Table 2).
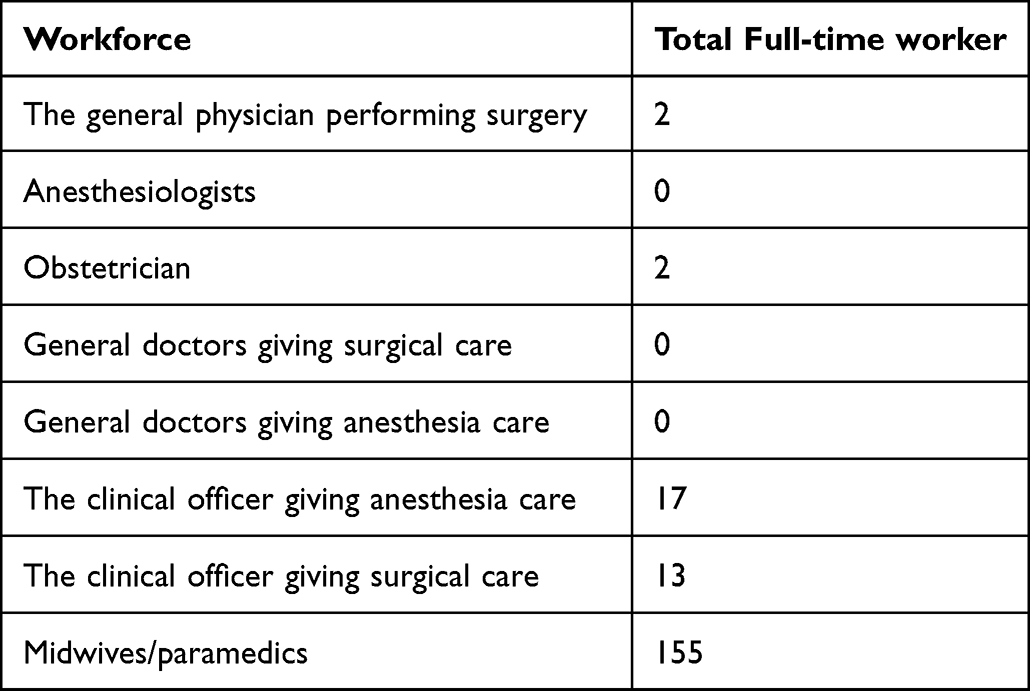 |
Table 2 Health Care Profession Profile in Gedeo Zone and Sidama Region Hospital 2020 |
Regarding the availability of infrastructure and health resources, there was a shortage of Functional x-ray machines and anesthesia machines (Table 3).
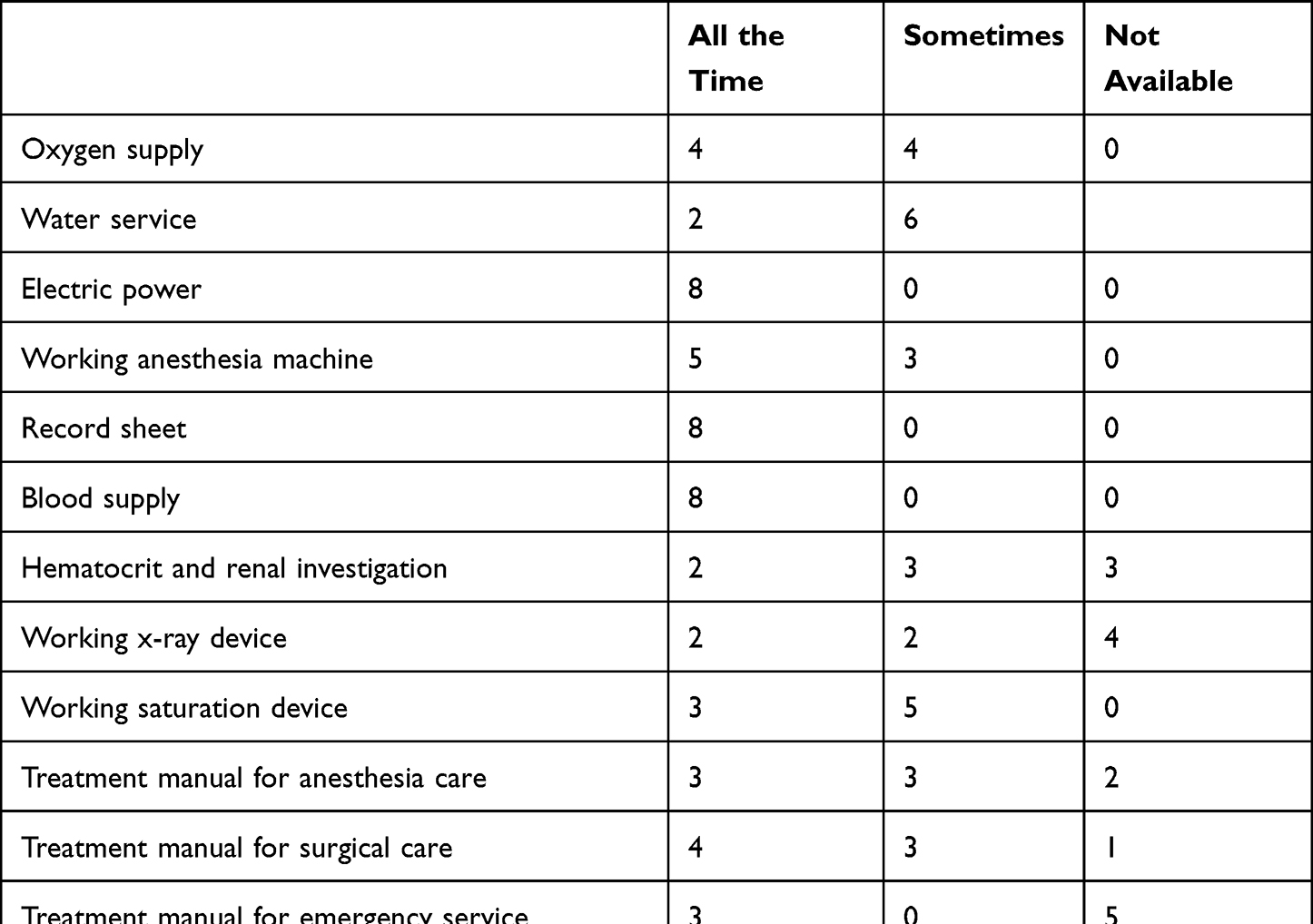 |
Table 3 Availability of Infrastructures and Health Resources in Gedeo Zone and Sidama Region Hospital. (N = 8) |
Only 48.57% of the 35 critical interventions indicated in the checklist were available at all facilities, including cesarean section. Not all hospitals, give services for fistula treatment, stricture dilatation, and club foot correction (Table 4).
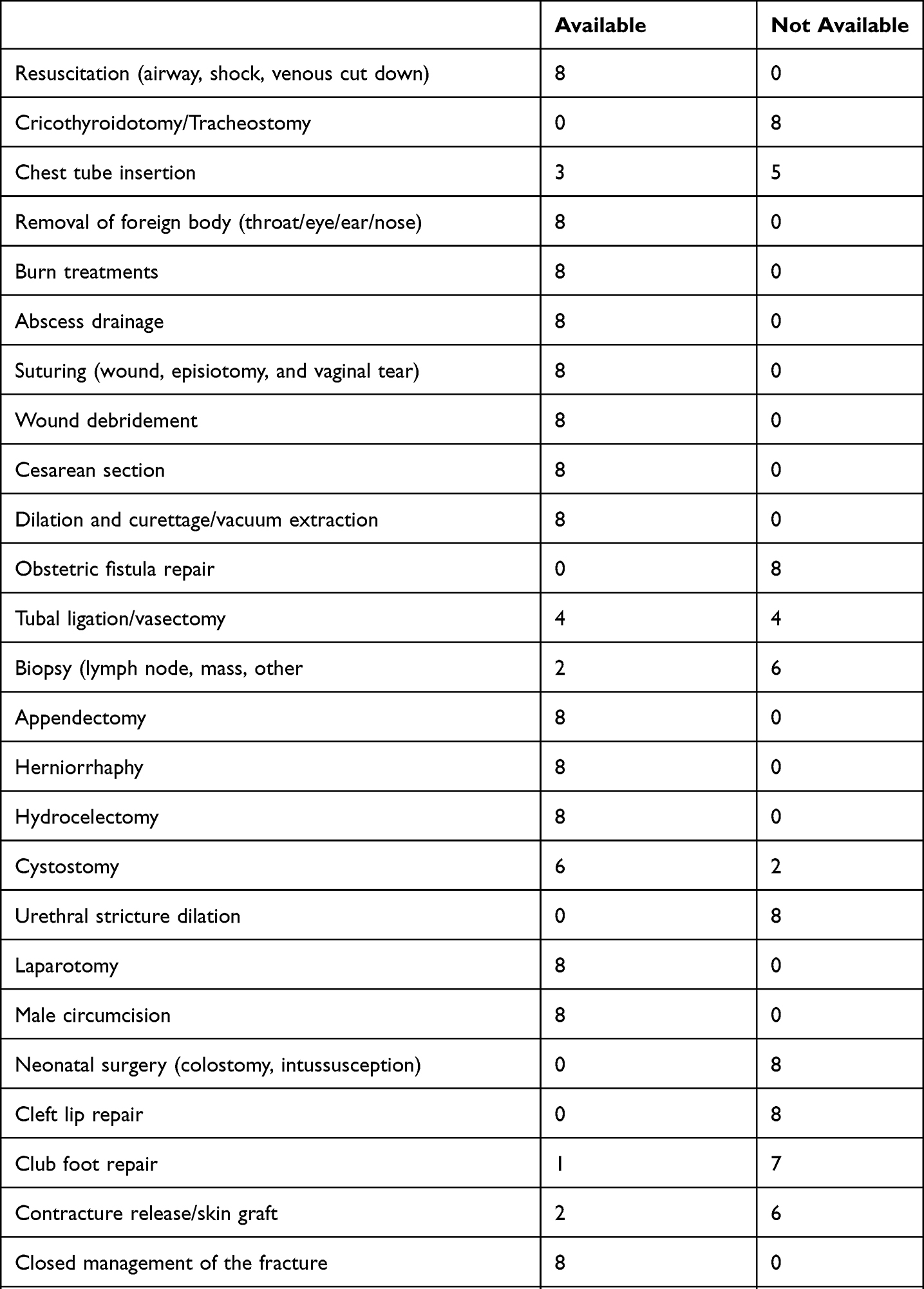 |
Table 4 Availability of Surgical Management in the Gedeo Zone and Sidama Region (N = 8) |
There was frequently a shortage of capital outlays for resuscitation in Gedeo & Sidama zone hospitals. Sterile gloves, airway and disposable gloves are frequently in shortage (Table 5).
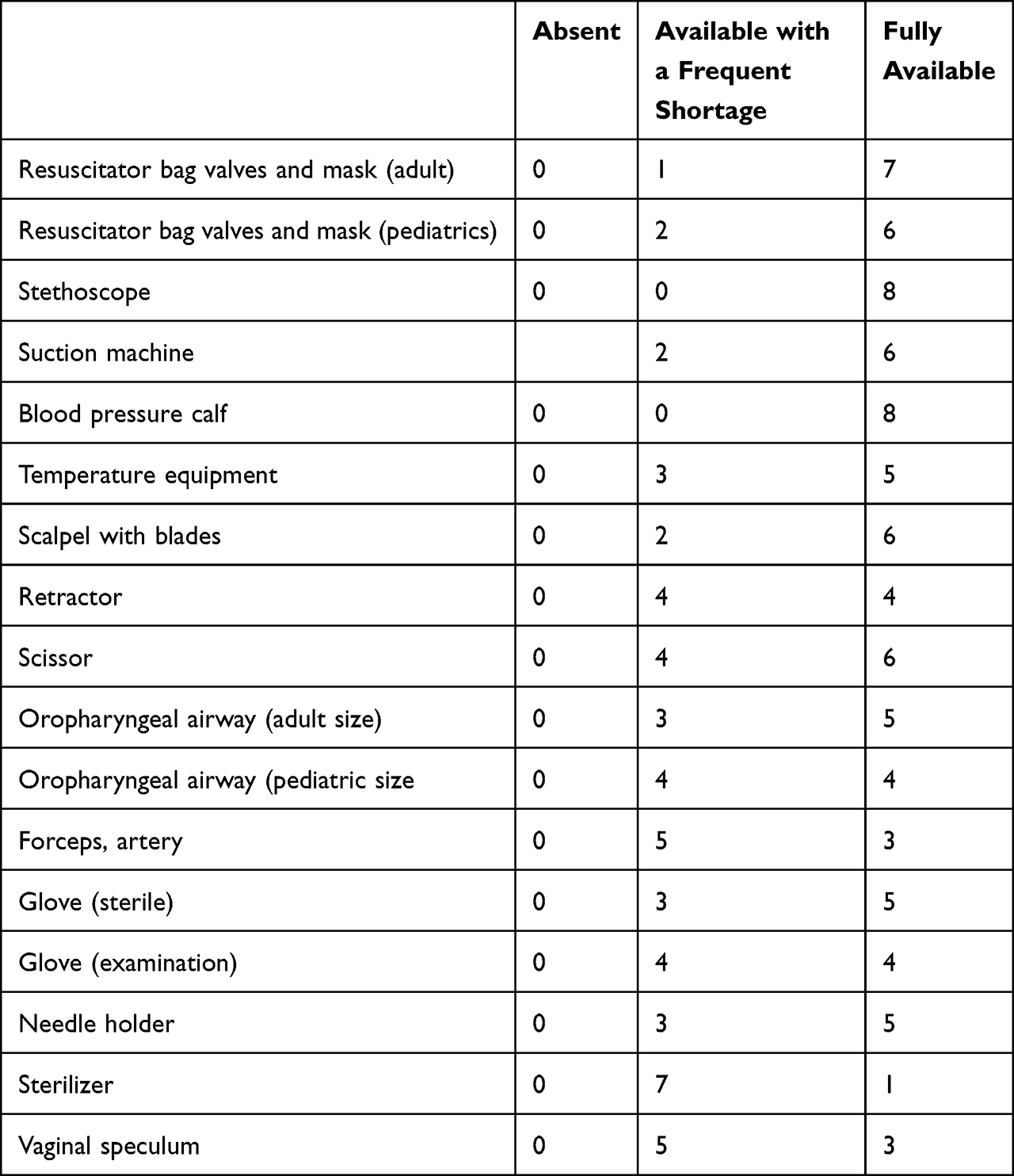 |
Table 5 Availability of Capital Outlays for Resuscitation in Gedeo Zone and Sidama Region Hospitals (N = 8) |
Splints for arms, and legs, Waste disposal containers, and Eye prevention were frequently in shortage in primary hospitals (Table 6).
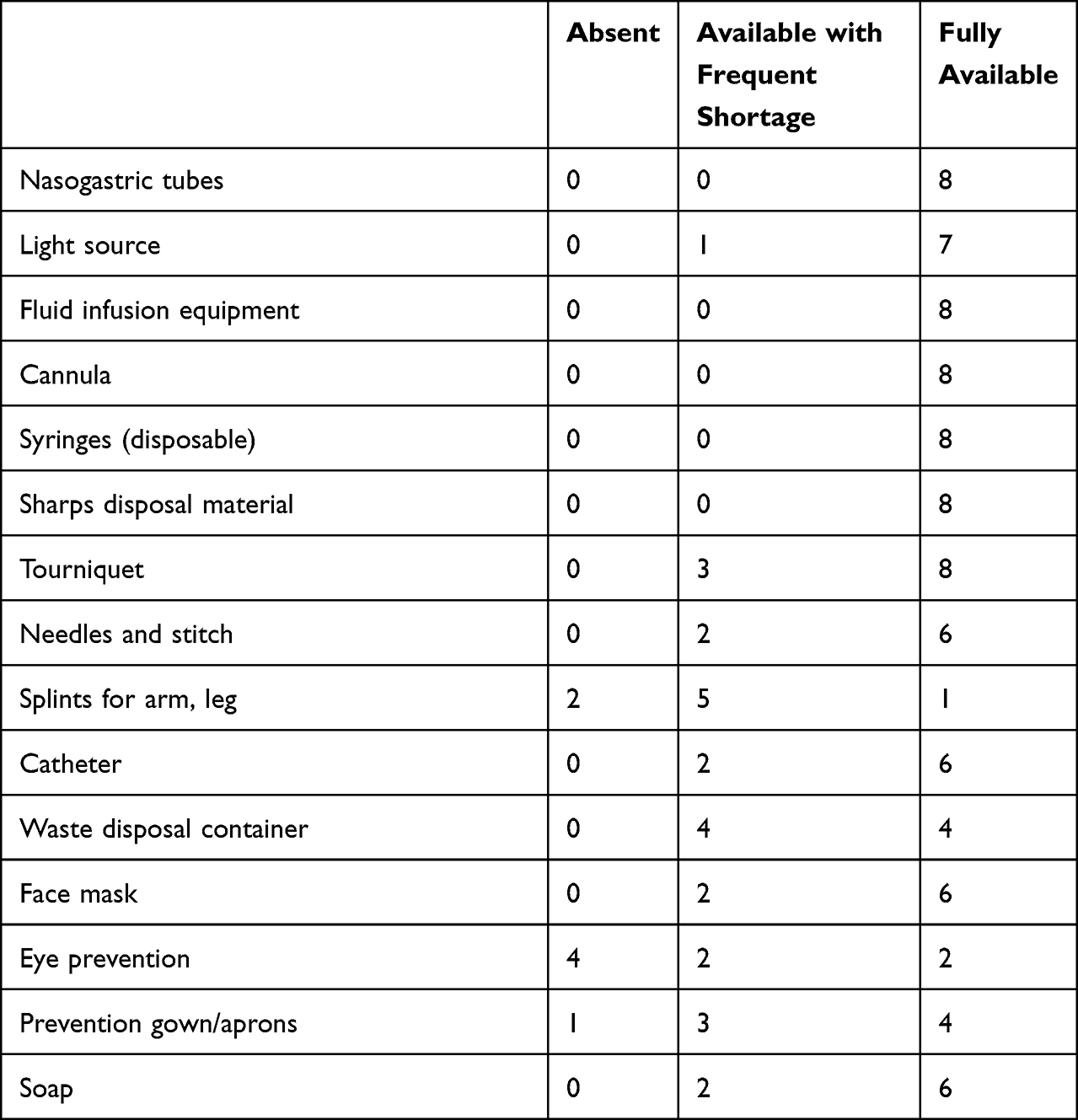 |
Table 6 Availability of Renewable Supplies for Resuscitation in Gedeo Zone and Sidama Region Hospitals (N = 8) |
Cricothyroidotomy set, Magill forceps, endotracheal tube, laryngoscopy, and IV infuser bag were frequent shortages in hospitals (Table 7).
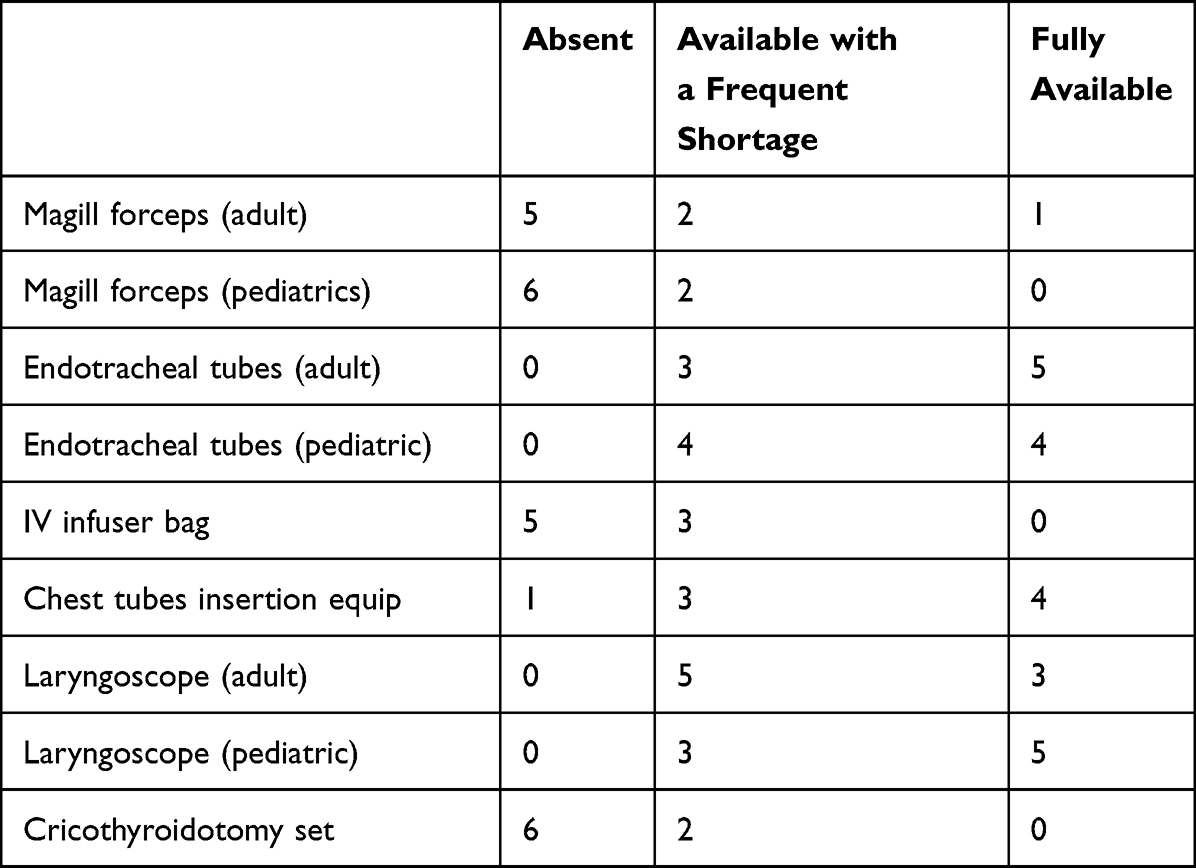 |
Table 7 Availability of Supplementary Equipment for Resuscitation in Gedeo Zone and Sidama Region Hospital, 2020 (N = 8) |
Discussion
Only 48.57% of the 35 emergency and necessary surgical operations mentioned in the WHO tool, such as cesarean section, were available at all facilities, according to our findings. Not all hospitals, on the other hand, provided fistula treatment, stricture dilatation, and clubfoot correction. When compared to a previous study done in the Amhara region, which found that 51.4% of basic surgical services in primary hospitals were covered, our findings show that a low percentage of basic emergency and essential surgical services were covered by primary hospitals.9
A well-functioning surgical system could assist to reduce the global disease burden significantly. Injury claims the lives of almost 5 million people each year, and many more are permanently crippled. For patients with surgically curable illnesses, there are significant differences in service between developed- and developing nations. Even though third world nations account for 70% of the worldwide people, a study of the global load of surgical procedures found that only 26% of expected surgical services were done in these nations.10,11
This study discovered a serious scarcity of basic infrastructure and qualified human resources needed to provide surgical care, which is consistent with previous studies in Sub-Saharan Africa. There was a severe lack of flowing water, hematocrit and urine testing, a functioning x-ray device, and a functioning saturation measure device. According to the research, vital instruments were not always present in the whole area. Systemic adjustments in the health profession, supplies/equipment, and infrastructure were necessary to reduce mortality from surgically curable conditions.12,13
To ensure the availability of critical equipment and materials, a functioning healthcare system requires proper planning and a procurement structure. Saturation measuring devices and anesthetic devices were not always operational or available in several of the institutions. According to a recent survey, approximately 58.47% of surgical rooms in Sub-Saharan Africa (SSA) shortage of saturation measuring devices.14 These findings show that a scarcity of critical equipment could threaten the safety of patients having surgery. Recognizing Ethiopia’s unmet surgical care needs, Ethiopia has devised special surgical care preparation approaches, which emphasize lifesaving surgery (SaLTS). In different hospitals in Ethiopia, these guidelines increase the safety of essential and argent surgery and anesthesia care. There has been no systematic evaluation of surgical service competence in our country regarding equipment and care service at a different portion of the healthcare facilities to date.11
This finding indicates that primary hospitals lacked EES services, implying that the ministry of health should establish guidelines for dealing with lacked service. Of course, the ministry of health developed unique surgical system development methodologies that focus on saving lives through safe surgery (SaLTS). At all levels of the healthcare system, this national initiative aims to improve access to safe, required, and emergency surgical and anesthetic services. So far, no comprehensive assessment of surgical care capability in Ethiopia has been conducted in terms of physical resources and service supply at various levels of the health care system, especially in primary hospitals which were found in rural areas.6 Therefore, this finding gives a clue for the development of new guidelines or improving this SaLTS system for the early management of such conditions.
Conclusion
Shortages in infrastructure, health professionals, care provision, and key instruments and supplies reveal major disparities in hospitals’ capabilities to deliver EESC and effectively treat the growing surgical load of disease and injury in primary hospitals in the south part of Ethiopia. The necessity for continuing investment in EESC infrastructure, instruments, and supplies, as enough qualified surgeons, anesthesiologists, and obstetricians/gynecologists, is highly important in this survey.
Abbreviations
EESC, essential emergency surgical care; IMEESC, integrated management for emergency & essential surgical care; MSc, Master of Science; WHO, World Health Organization.
Funding
There was no funding from the organization for this project.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Sherman L, Clement PT, Cherian MN, et al. Implementing Liberia’s poverty reduction strategy: an assessment of emergency and essential surgical care. Arch Surg. 2011;146(1):35–39. doi:10.1001/archsurg.2010.285
2. Alkire BC, Raykar NP, Shrime MG, et al. Global access to surgical care: a modelling study. Lancet Global Health. 2015;3(6):e316–e23. doi:10.1016/S2214-109X(15)70115-4
3. Labricciosa FM, Sartelli M, Correia S, et al. Emergency surgeons’ perceptions and attitudes towards antibiotic prescribing and resistance: a worldwide cross-sectional survey. World J Emerg Surg. 2018;13(1):1–9. doi:10.1186/s13017-018-0190-5
4. Alleyne G, Breman J, Claeson M, et al. Disease control priorities in developing countries. World Bank/OUP; 2006.
5. Tessema GA, Laurence CO, Melaku YA, et al. Trends and causes of maternal mortality in Ethiopia during 1990–2013: findings from the Global Burden of Diseases study 2013. BMC Public Health. 2017;17(1):1–8. doi:10.1186/s12889-017-4071-8
6. MOH E. Federal democratic republic of Ethiopia ministry of health health sector development program IV October 2010 contents; 2014.
7. CSA I. Ethiopia Demographic and Health Survey 2011. Addis Ababa, Ethiopia and Calverton. Maryland, USA: Central Statistical Agency and ICF International; 2012:430.
8. Demographic C. Health Survey 2011 Addis Ababa, Ethiopia and Calverton. Central Statistical Agency and ICF International: Maryland; 2011.
9. Alemayehu TY, Boled AT, Taye MG, Kibret S, Habtie MF. Assessment of emergency and essential surgical service in primary hospitals of South Gondar zone, Amhara region, Ethiopia, 2019. Int J Surg Open. 2020;23:35–38. doi:10.1016/j.ijso.2020.02.003
10. Albutt K, Yorlets RR, Punchak M, et al. You pray to your God: a qualitative analysis of challenges in the provision of safe, timely, and affordable surgical care in Uganda. PLoS One. 2018;13(4):e0195986. doi:10.1371/journal.pone.0195986
11. Burssa D, Teshome A, Iverson K, et al. Safe surgery for all: early lessons from implementing a national government-driven surgical plan in Ethiopia. World J Surg. 2017;41(12):3038–3045. doi:10.1007/s00268-017-4271-5
12. Choo S, Perry H, Hesse AA, et al. Assessment of capacity for surgery, obstetrics and anaesthesia in 17 Ghanaian hospitals using a WHO assessment tool. Trop Med Int Health. 2010;15(9):1109–1115.
13. Elkheir N, Sharma A, Cherian M, et al. A cross-sectional survey of essential surgical capacity in Somalia. BMJ open. 2014;4(5):e004360. doi:10.1136/bmjopen-2013-004360
14. Hsia RY, Mbembati NA, Macfarlane S, Kruk ME. Access to emergency and surgical care in sub-Saharan Africa: the infrastructure gap. Health Policy Plan. 2012;27(3):234–244. doi:10.1093/heapol/czr023
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.