Back to Journals » Medical Devices: Evidence and Research » Volume 15
Evaluation of Common Nasal Cannulas in Neonatal Noninvasive Ventilation (NIV) Using a Novel Neonatal Nasal Model
Authors Borg U ![]() , Aviano J
, Aviano J ![]() , Ginani M, Li K
, Ginani M, Li K
Received 12 May 2022
Accepted for publication 11 August 2022
Published 1 September 2022 Volume 2022:15 Pages 307—315
DOI https://doi.org/10.2147/MDER.S374418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ulf Borg,1 Jeffrey Aviano,2 Milan Ginani,2 Kun Li2
1Department of Medical Science, Respiratory Interventions, Medtronic, Boulder, CO, USA; 2Department of Research and Development, Respiratory Interventions, Medtronic, Carlsbad, CA, USA
Correspondence: Ulf Borg, Department of Medical Science, Respiratory Interventions, Medtronic, 6135 Gunbarrel Avenue, Boulder, CO, 80301, USA, Tel +1 303 305 2544, Email [email protected]
Purpose: Non-invasive ventilation (NIV) may reduce intubation rates and be especially beneficial in the care of preterm infants, in addition to other care modalities. Currently, ventilators do not display the pressure at the nares but the pressure in the ventilator tubing system. There are several nasal cannulas available for use to deliver NIV. The purpose of this study was to compare the inspiratory pressure on the ventilator to the measured pressure delivered at the nares using three cannula brands (Manufacturer A, Fisher & Paykel; Manufacturer B, Neotech RAM; and Manufacturer C, Hudson RCI).
Patients and Methods: This bench study utilized a 3D printed nasal model, including nares in multiple sizes to accommodate all nasal prongs studied. The nasal adaptors were connected to neonatal test lungs, to simulate patient breathing. Multiple sizes of nasal cannulas from the three manufacturers were tested for inspiratory vs delivered pressure at the patient side of the cannula, using eight combinations of ventilator settings. Each nasal cannula was tested on six Puritan Bennett™ 980 ventilators.
Results: The measured delivered pressure at the nares was consistently lower than the clinician-set inspiratory pressure. Across all ventilator settings, 7 of the 11 cannulas delivered significantly less pressure at the nares compared to the inspiratory ventilator pressure (p < 0.01). For each cannula, as inspiratory pressure increased, the difference between delivered and inspiratory pressures also increased. The cannula from Manufacturer B consistently demonstrated the greatest differences between set inspiratory and delivered pressures for each ventilator setting.
Conclusion: This study demonstrated substantial differences between ventilator inspiratory pressure and measured delivered pressure, which may have clinical significance. Being unaware of the actual airway pressure delivered to the patient may lead to erroneous adjustments to the level of ventilator pressure, which may be especially consequential to those with delicate and developing respiratory systems.
Keywords: non-invasive ventilation, nasal cannula, airway pressure, ventilator, model, 3D print
Introduction
The use of invasive mechanical ventilation (IMV) via an endotracheal tube, in addition to other interventions such as the use of exogenous surfactant1 and antenatal steroids,2 has contributed to improvement in neonatal survival.3 However, the prolonged use of IMV may predispose infants to the development of various complications, including bronchopulmonary dysplasia.4,5 Avoiding IMV is a goal in clinical care,3 and different modes of non-invasive ventilation (NIV), such as high flow nasal cannula (HFNC),6 nasal continuous positive airway pressure (NCPAP),6 nasal intermittent positive pressure ventilation (NIPPV),7 and its more advantageous form, synchronized nasal intermittent positive pressure ventilation (SNIPPV),8 have been shown to decrease the rate of IMV. For example, though not a feature explored in the current study, the use of SNIPPV has been demonstrated to have several benefits in preterm infants, including decreased work of breathing,9 reduction in incidence of apnea of prematurity,8 shorter duration of ventilation,10 and reduction in death for very low birth weight infants.11
Currently, there are several nasal cannulas (prongs) available for use to deliver HFNC, NCPAP, and NIPPV. These cannulas come in different sizes and lengths, which combined with the ratio of nasal prong to nare diameter, can affect the air pressure delivered to the patient.12 Without proper knowledge of the specific impact of these factors on delivered pressure, clinicians are left guessing what pressure should be set on the ventilation system to deliver adequate support to the patient.12 Airway pressure set on a ventilator and the actual delivered pressure may vary significantly depending on variables including correct sizing, internal diameter of the delivery system, inspiratory time, and cannula length. When oxygen saturation falls as a sign of inadequate support, the clinician may question how much pressure is being delivered to the patient and whether the inspiratory pressure needs to be increased. Being unaware of the actual airway pressure delivered to the patient may lead to erroneous adjustments in the levels of airway support and, in some cases, influence the decision to intubate.
Previous bench studies have utilized an artificial nose-throat-lung model to investigate the accuracy of neonatal ventilation approaches. For example, one study measured the delivery of inhaled nitric oxide (NO) in an infant lung model during nasal CPAP, NIV, and HFNC, and found that with HFNC, NO delivery was not accurate, and warned that the set inhaled NO level may not reflect the concentration of NO delivered to the patient.13 Similarly, a separate bench study used a breathing simulator with multiple 3D printed pediatric upper airway sizes to examine the percent of leak using RAM cannula for CPAP delivery. While the amount of leak varied by ventilator settings, approximately 25% of the CPAP was lost due to leaks.14 In another study, Rigotti et al examined pressure transmission with NIPPV using five mechanical ventilators and three nasal interfaces, and found that while the difference between inspiratory and delivered pressure at the airway opening was ±1 cm H2O, there was a significant difference between pressure at the airway and pressure at the glottis.15 The authors concluded that the nasal interface has a more significant impact on delivered pressure than the ventilator type.15
The purpose of this neonatal nasopharyngeal bench study was to measure the delivered pressure from three popular cannulas: Manufacturer A, Fisher & Paykel (Auckland, New Zealand); Manufacturer B, Neotech RAM (Valencia, CA, USA); and Manufacturer C, Hudson RCI (Morrisville, NC, US) using a single ventilator type, across a variety of ventilator settings.
Materials and Methods
Nasal Model
A nasal model was 3D printed and made to fit different size nares. The nasal adaptors were printed in several sizes to accommodate all nasal prongs (Figure 1). The diameter of the nares and the nasal prongs were matched to standardize the fit, such that the prong occupied 85% of nares diameter (Table 1). A pressure transducer (accuracy: ±0.1%, range: ±150 cmH2O) was connected to the nasal model for measurement of pressure at the patient side of the cannula (Figure 2A). A set of IngMar Neolung test lungs (Pittsburgh, PA, USA) was connected to the nares model to simulate patient compliance and resistance (Figure 2B).
 |
Table 1 Characteristics of Nasal Cannulas Used in Testing |
 |
Figure 1 Nasal adaptors with varied nasal diameters to accommodate different sizes of nasal prongs. |
 |
Figure 2 (A) Schematic for nasal cannula testing (B) Photo of nasal cannula testing setup with 3D printed nares on the lower right side. |
Prior to the test, each cannula was calibrated by allowing a set gas flow through the cannula, while the internal ventilator pressure was measured for calculation of cannula resistance. Ventilator settings were pressure-controlled ventilation, respiration rate 30 breaths/min and average inspiratory time 375 ms. Ventilator pressures as well as nares pressures were automatically recorded. The smallest cannula from each manufacturer was also tested at inspiratory times 300 ms, 350 ms, 400 ms, 450 ms, and 500 ms.
Nasal Cannula Testing Protocol
The nasal cannulas tested are summarized in Table 1. To control for variation between ventilators, each cannula was tested using six different Puritan Bennett™ 980 ventilators (Medtronic, Carlsbad, CA). To test the range of ventilator settings and potential setting combinations, ventilator settings were manipulated in a non-uniform manner. This allowed for testing of potentially extreme or uncommon ventilator settings that, although perhaps of limited clinical significance, provided insight into the technical aspects of ventilator performance. This may have led to test conditions that were not reflective of the clinical setting. The testing consisted of a sample of six ventilators tested with eight cases in different settings for each selected cannula size. The eight test cases included: (1) 400 msec inspiration time, 15 cm H2O PEEP, and 10 cm H2O inspiratory pressure; (2) 500 msec inspiration time, 15 cm H2O PEEP, and 25 cm H2O inspiratory pressure; (3) 350 msec inspiration time, 10 cm H2O PEEP, and 10 cm H2O inspiratory pressure; (4) 450 msec inspiration time, 10 cm H2O PEEP, and 30 cm H2O inspiratory pressure; (5) 300 msec inspiration time, 5 cm H2O PEEP, and 10 cm H2O inspiratory pressure; (6) 400 msec inspiration time, 5 cm H2O PEEP, and 20 cm H2O inspiratory pressure; (7) 300 msec inspiration time, 3 cm H2O PEEP, and 12 cm H2O inspiratory pressure; and (8) 300 msec inspiration time, 3 cm H2O PEEP, and 17 cm H2O inspiratory pressure. For each of the eight test cases, 15 breaths were allowed to pass before the final delivered pressure measurements were taken. The resulting sample size for each cannula manufacturer was n = 6 ventilators × 8 test settings × the number of interfaces of different sizes under testing (4, 4, and 3 sizes for Manufacturers A, B, and C, respectively), for a total of n = 192 inspiratory and delivered pressures for Manufacturers A and B, and n = 144 inspiratory and delivered pressures for Manufacturer C.
Statistics
Analyses were performed using MedCalc Version 11.6.1.0 (MedCalc Software Ltd, Ostend, Belgium), and data were summarized by descriptive statistics for continuous variables or frequencies and percentages for categorical variables. Means and standard deviations were calculated using the number of observations for each cannula over the range of settings and collected readings. Two-sided t-tests were used to compare inspiratory vs delivered pressure for each cannula in each of the 8 test cases, with statistical significance accepted at P<0.05.
Results
Ventilator pressures from 15 cm H2O to 40 cm H2O were tested. Table 2 shows the low and high values for all tests. As expected, in many, though not all cases, the inspiratory pressure was higher compared to the delivered (measured) pressure at the nares, however, the delivered pressures varied by cannula type and size. At the low-pressure setting of 15 cm H2O, Manufacturers A and C delivered pressure that was not significantly different from the inspiratory pressure, and Manufacturer B had three cannulas that delivered significantly lower pressure than the inspiratory pressure. At the highest pressure setting (40 cm H2O) the difference between delivered and inspiratory pressures was significantly different for one cannula from Manufacturer A and two cannulas from Manufacturer B. The delivered and inspiratory pressures were not significantly different for Manufacturer C at high pressure (Table 2). Across all eight ventilator settings and all manufacturers, 7 out of 11 cannulas tested delivered significantly lower pressure at the nares than the ventilator setting (Table 3).
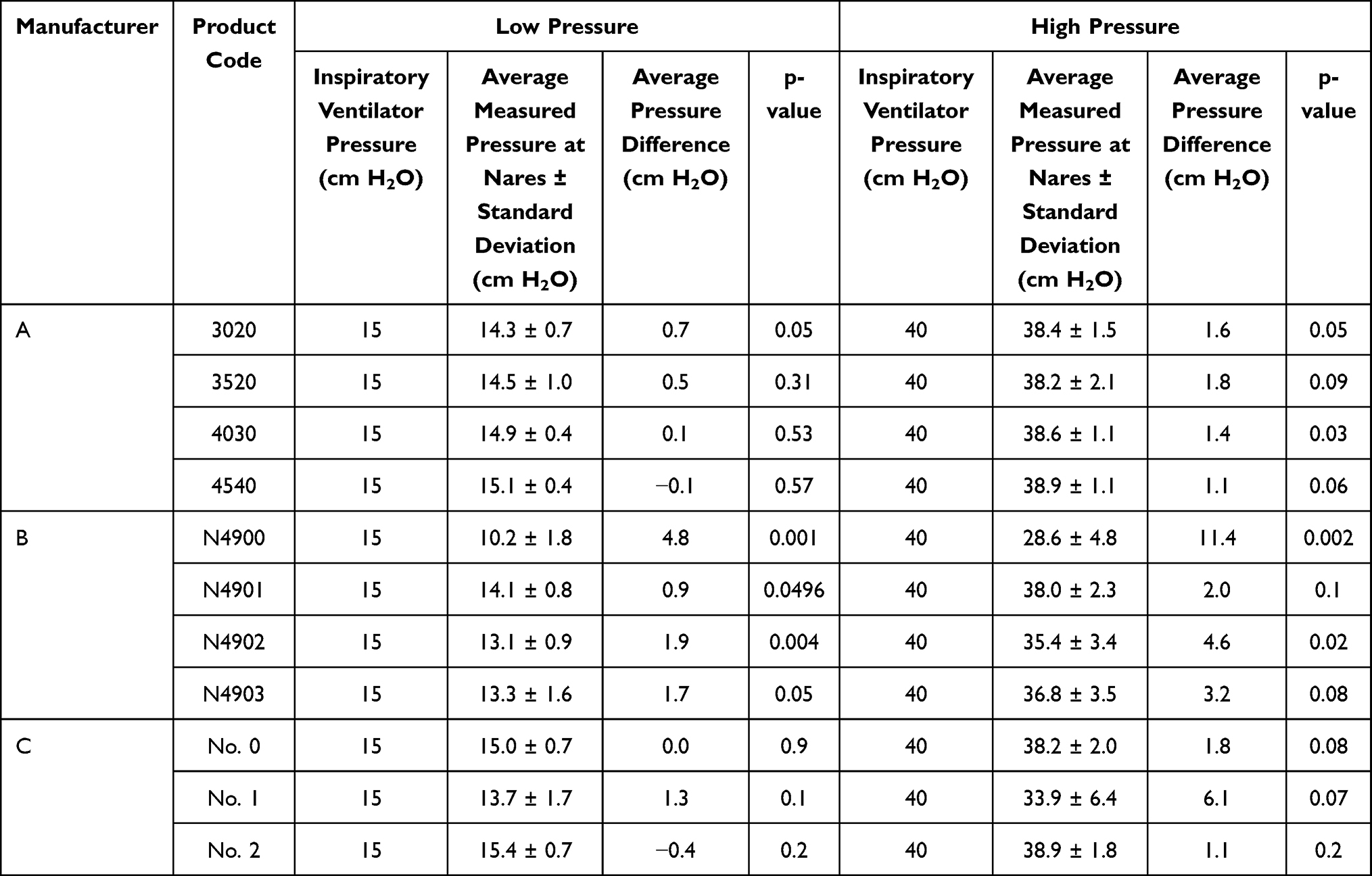 |
Table 2 Low and High Ventilator Pressure and Measured Pressures at Nares |
 |
Table 3 Average Ventilator Pressure and Measured Pressures for Cannulas When Used Across Eight Ventilator Settings |
With respect to the smallest cannula size for each manufacturer, the relative difference between inspiratory pressure and delivered pressure was consistent as inspiratory time increased (Figure 3). Multiple 300ms and 400ms measures are included, as different PEEP levels and inspiratory pressures were used, even though the total inspiratory pressure remained constant. Overall, the longer inspiration time in pressure control ventilation resulted in larger volume being delivered. The cannula from Manufacturer B consistently demonstrated the greatest pressure difference at each inspiratory time point compared to the other cannulas (p < 0.01). Of the three cannulas, the cannula from Manufacturer C showed the smallest differences in inspiratory pressure at all inspiratory times (p >0.05), and the cannula from Manufacturer A demonstrated significantly different pressure differences at 300ms and 400 ms (p < 0.05).
 |
Figure 3 Effect of inspiratory time on the delivered pressure for the smallest cannula size for each manufacturer. Multiple inspiratory times, along with different PEEP and inspiratory pressure ventilator settings were utilized, ranging from 5–15 cm H2O PEEP and 10–25 cm H2O inspiratory pressure. Green bars denote the total inspiratory pressure on the ventilator, for comparison to the delivered pressure. Significant differences between the inspiratory and delivered pressure for each cannula and ventilator setting are denoted as: * p<0.05; ** p<0.01; *** p<0.001. |
Discussion
Our study found that across 11 cannula types and 8 ventilator settings, the delivered pressure at the nares is often, though not always, statistically lower than the inspiratory pressure set on the ventilator. In general, smaller diameter cannulas demonstrated the largest difference between inspiratory and delivered pressure, and Manufacturer B consistently exhibited the largest difference between inspiratory and delivered pressure. Since premature infants utilize the smallest diameter cannulas, these results suggest that differences between inspiratory pressure and delivered pressure may be greatest in the smallest patients, with delivered pressure varying between cannula manufacturers and sizes.
Our results are supported by other bench studies examining delivered pressure during NIV. DiBlasi et al reported that using HFNC resulted in low accuracy between the set delivery of inhaled NO vs the actual NO delivered in a lung model,13 and Rigotti et al concluded that during NIPPV, the PEEP transmission and inspiratory pressures at the glottis are significantly reduced compared to the inspiratory values, with high variability.15 Similar findings have been reported in studies focusing on set vs delivered CPAP across a variety of CPAP levels, as well as during NIV using HFNC, where it was concluded that even with an integrated pressure relief valve, it is important for the clinician to select the appropriate nasal prong size to match the patient nares.12,16
Both the pressure level and choice of inspiration time affect the pressure differences due to change in flow rate. The paradoxical result with the cannula from Manufacturer B was a result of the constant pressure setting in ventilator pressure trying to deliver a larger tidal volume with longer inspiration time. In a similar study, Iyer et al looked at the delivered pressure of the cannula from Manufacturer B and found that it delivered clinically acceptable pressures when leaks were less than 30%, as measured by the Puritan Bennett™ 840 Ventilator; however, with leaks >50%, a negligible amount of pressure was being delivered.17
The use of NIV in preventing intubation and progressing respiratory failure in the neonate continues to grow.4,5 Currently, ventilators do not display the pressure at the nares but the pressure in the ventilator tubing system. Though the authors are unaware of published evidence suggesting negative outcomes or adverse events as a result of using these cannulas, being unaware of the actual airway pressure delivered to the patient may lead to erroneous adjustments to the level of ventilator pressure. This study demonstrated differences between the inspiratory pressure on the ventilator and the actual pressure delivered to the patient, which may impact clinical decisions, such as whether to adjust the pressure or transition to IMV. Transition to IMV requires orotracheal intubation, which adds risk of tracheal damage.18,19 It is also known that the positive pressures and tidal volumes delivered by the ventilator may result in ventilator-induced lung injuries,20 so care should be taken to ensure that before transition to IMV, the delivered pressure by NIV is adequate for the patient.
It is of clinical importance that clinicians are aware of the differences between inspiratory pressures on the ventilator and what is actually delivered to the patient. The use of NIV to establish and maintain lung volume is dependent on the correct display and interpretation of the delivered airway pressure. Additionally, avoidance of tracheal intubation may reduce the incidence of chronic pulmonary complications in preterm infants.21 While our results are corroborated by multiple other bench studies, only clinical studies can determine the clinical relevance of the findings in this bench study.13–17
One weakness of this bench study is that although leaks did occur around the nasal interface, the study did not measure the amount of leak at the nares. However, it is important to note that several previous bench studies have examined the impact of leaks on delivered pressure during NIV, and we expect that the leaks at the nares in our study are comparable to previous findings.14,15,17 Importantly, in our study, the nasal prongs occupied approximately 85% of the nares diameter, which may be a closer fit compared to use in the clinical setting. Thus, our bench study may have encountered less percentage leak than what may occur in a clinical setting where the nasal prong may not be fitted as closely to the patient nare diameter. In such a scenario, we would expect increased leaks at the nares to further exacerbate our results, leading to even lower delivered pressure compared to what we observed in this bench study.
Conclusion
Using 3D printed nare models of different sizes and prongs from three leading cannula manufacturers, this bench study observed some notable reductions in actual delivered pressure, compared to the inspiratory pressure on the ventilator. Differences between inspiratory and delivered pressure may have clinical consequences that impact decision-making, which may be especially profound in neonatal patients with delicate and developing respiratory systems. Clinicians should take into account the difference between inspiratory and delivered pressure when intervening in patient care.
Abbreviations
HFNC, High flow nasal cannula; IMV, Invasive mechanical ventilation; NCPAP, Nasal continuous positive airway pressure; NIPPV, Nasal intermittent positive pressure ventilation; NIV, Non-invasive ventilation; SNIPPV, Synchronized nasal intermittent positive pressure ventilation.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
Medical writing support was provided by Hanan Zavala, PhD, and Katherine Liu, PhD, both of Medtronic (Minneapolis, MN) in accordance with Good Publication Practice (GPP3) guidelines.22
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was sponsored by Medtronic, which contributed to the study design, data collection and analysis, and manuscript writing. The final decision to submit for publication was the responsibility of the authors.
Disclosure
All authors report Medtronic employment. Mr Milan Ginani reports a patent US Pub. No. 2021/0097891 assigned to Covidien LP, a Medtronic company. Mr Kun Li reports a patent 20210052839 pending to Covidien LP.
References
1. Härtel C, Glaser K, Speer CP. The miracles of surfactant: less invasive surfactant administration, nebulization, and carrier of topical drugs. Neonatology. 2021;118(2):225–234. doi:10.1159/000516106
2. McGoldrick E, Stewart F, Parker R, Dalziel SR. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Sys Rev. 2020;1:12.
3. Wheeler CR, Smallwood CD. 2019 year in review: neonatal respiratory support. Respir Care. 2020;65(5):693–704. doi:10.4187/respcare.07720
4. Permall DL, Pasha AB, Chen X. Current insights in non-invasive ventilation for the treatment of neonatal respiratory disease. Ital J Pediatr. 2019;45(1):1–7.
5. Nasef N, Rashed HM, Aly H. Practical aspects on the use of non-invasive respiratory support in preterm infants. Int J Pediatrics Adolescent Med. 2020;7(1):21–27.
6. Shi Y, Muniraman H, Biniwale M, Ramanathan R. A review on non-invasive respiratory support for management of respiratory distress in extremely preterm infants. Front Pediatr. 2020;8:270. doi:10.3389/fped.2020.00270
7. Oncel MY, Arayici S, Uras N, et al. Nasal continuous positive airway pressure versus nasal intermittent positive-pressure ventilation within the minimally invasive surfactant therapy approach in preterm infants: a randomised controlled trial. Arch Dis Childhood Fetal Neonatal Edition. 2016;101(4):F323–F328.
8. Gizzi C, Montecchia F, Panetta V, et al. Is synchronised NIPPV more effective than NIPPV and NCPAP in treating apnoea of prematurity (AOP)? A randomised cross-over trial. Arch Dis Childhood Fetal Neonatal Edition. 2015;100(1):F17–F23.
9. Aghai ZH, Saslow JG, Nakhla T, et al. Synchronized nasal intermittent positive pressure ventilation (SNIPPV) decreases work of breathing (WOB) in premature infants with respiratory distress syndrome (RDS) compared to nasal continuous positive airway pressure (NCPAP). Pediatr Pulmonol. 2006;41(9):875–881.
10. Santin R, Brodsky N, Bhandari V. A prospective observational pilot study of synchronized nasal intermittent positive pressure ventilation (SNIPPV) as a primary mode of ventilation in infants ≥ 28 weeks with respiratory distress syndrome (RDS). J Perinatol. 2004;24(8):487–493. doi:10.1038/sj.jp.7211131
11. Bhandari V, Finer NN, Ehrenkranz RA, et al. Synchronized nasal intermittent positive-pressure ventilation and neonatal outcomes. Pediatrics. 2009;124(2):517–526. doi:10.1542/peds.2008-1302
12. Sivieri EM, Gerdes JS, Abbasi S. Effect of HFNC flow rate, cannula size, and nares diameter on generated airway pressures: an in vitro study. Pediatr Pulmonol. 2013;48(5):506–514.
13. DiBlasi RM, Dupras D, Kearney C, Costa E, Griebel JL. Nitric oxide delivery by neonatal noninvasive respiratory support devices. Respir Care. 2015;60(2):219–230. doi:10.4187/respcare.03278
14. Fernandes ND, Chung E, Salt MD, Ejiofor B, Carroll RW, Kacmarek RM. Measured CPAP in a noninvasive pediatric airway and lung model. Respir Care. 2021;66(1):87–94. doi:10.4187/respcare.07864
15. Rigotti C, Zannin E, Dognini G, Dellacà R, Ventura ML. Role of ventilator and nasal interface in pressure transmission during neonatal intermittent positive pressure ventilation: a bench study. Pediatr Pulmonol. 2021;56(8):2561–2569. doi:10.1002/ppul.25449
16. Bailes SA, Firestone KS, Dunn DK, McNinch NL, Brown MF, Volsko TA. Evaluating the effect of flow and interface type on pressures delivered with bubble CPAP in a simulated model. Respir Care. 2016;61(3):333–339. doi:10.4187/respcare.04251
17. Iyer NP, Chatburn R. Evaluation of a nasal cannula in noninvasive ventilation using a lung simulator. Respir Care. 2015;60(4):508–512.
18. Holzki J, Laschat M, Puder C. Iatrogenic damage to the pediatric airway. Mechanisms and scar development. Paediatr Anaesth. 2009;19(Suppl 1):131–146. doi:10.1111/j.1460-9592.2009.03003.x
19. Hatch LD, Grubb PH, Lea AS, et al. Endotracheal intubation in neonates: a prospective study of adverse safety events in 162 infants. J Pediatr. 2016;168:62–66.e6. doi:10.1016/j.jpeds.2015.09.077
20. Kalikkot Thekkeveedu R, Guaman MC, Shivanna B. Bronchopulmonary dysplasia: a review of pathogenesis and pathophysiology. Respir Med. 2017;132:170–177. doi:10.1016/j.rmed.2017.10.014
21. Alexiou S, Panitch HB. Physiology of Non-Invasive Respiratory Support. Elsevier; 2016:174–180.
22. Battisti WP, Wager E, Baltzer L, et al. Good publication practice for communicating company-sponsored medical research: GPP3. Ann Intern Med. 2015;163(6):461–464.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.