Back to Journals » Vascular Health and Risk Management » Volume 21
Evaluation of a Brief Educational Intervention in Enhancing Venous Thromboembolism Knowledge Among Surgical Patients and Health-Care Providers: A Prospective Study
Authors Tan G ![]() , Yip HC, Siu HY, Yao AY, Yan BPY
, Yip HC, Siu HY, Yao AY, Yan BPY
Received 24 May 2025
Accepted for publication 8 September 2025
Published 23 October 2025 Volume 2025:21 Pages 879—887
DOI https://doi.org/10.2147/VHRM.S542572
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mirna N Chahine
Supplementary video of “Educational intervention in enhancing venous thromboembolism knowledge” [542572].
Views: 46
GuangMing Tan,1,2 Hon Chi Yip,3 Ho Yin Siu,4 Alan Yong Yao,4 Bryan Ping Yen Yan1,2
1Department of Medicine & Therapeutics, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China; 2Li Ka Shing Institutes of Health Science, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China; 3Department of Surgery, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China; 4Faculty of Medicine, the Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China
Correspondence: GuangMing Tan, Department of Medicine & Therapeutics, Faculty of Medicine, the Chinese University of Hong Kong, Hong Kong SAR, People’s Republic of China, Tel +852 55699658, Email [email protected]
Purpose: No study has systematically evaluated the impact of education on improving venous thromboembolism (VTE) knowledge in surgical patients despite its significance. This study a assessed the baseline VTE knowledge among patients undergoing major surgery and their healthcare providers (HCPs), and evaluated the impact of educational materials on knowledge and acceptance of VTE prophylaxis.
Patients and Methods: In this prospective, single-center, non-randomized controlled trial, VTE knowledge in surgical patients was measured using a validated questionnaire. Two sets of materials including questionnaire and educational videos were developed: Set A for patients and Set B for HCPs. The intervention was a 2‑minute educational video. VTE knowledge was initially assessed in the control group. Four weeks later, a separate group of patients (intervention group) and HCPs completed the questionnaire, before and immediately after the intervention. The primary outcome was post‑intervention knowledge difference between control and intervention patients. Secondary outcomes included pre‑/post‑intervention knowledge change in HCPs, VTE prophylaxis use, patient satisfaction, and VTE occurrence.
Results: 200 patients (100 in the control group and 100 in the intervention group) and 17 HCPs participated in the study. Patients had limited knowledge of VTE at baseline (29.4% and 29.6% in the respective groups), whereas HCPs had scores of 73.5%. After the intervention, the patients’ knowledge significantly improved to 46.1%, while HCPs scores showed no notable increase. VTE prophylaxis compliance was 42.5% and was similar in both groups, with no VTE occurrence reported. Patient satisfaction with prophylaxis improved significantly in the intervention group from 67% to 93%.
Conclusion: Patients undergoing major surgery exhibited a low baseline knowledge of VTE, highlighting the need for targeted education. A brief, structured educational intervention effectively improved awareness and patient satisfaction, supporting the integration of targeted education into perioperative care.
Plain Language Summary: Venous thromboembolism (VTE) is a serious condition; however, many surgical patients lack knowledge regarding its risks and prevention. A prospective single-centre trial involving 200 surgical patients (100 in the control group and 100 in the intervention group) and 17 healthcare providers (HCPs) was conducted. Patients completed a validated questionnaire to assess their VTE knowledge. The intervention group watched a brief, 2-minute educational video before completing the questionnaire. HCPs also participated in the study to evaluate the changes in their understanding of VTE. Before the intervention, the patients demonstrated limited awareness of VTE, scoring approximately 29.5% on the questionnaire. After receiving the educational materials, their knowledge improved significantly to 46.1%. The HCPs, who initially scored 73.5%, showed no significant post-intervention changes. Despite increased awareness, compliance with VTE preventive measures remained similar between patient groups, and no VTE cases were reported during the study period. Patient satisfaction with VTE prevention strategies was significantly increased in the intervention group, rising to 93%. These findings highlight the importance of structured education for surgical patients, showing that simple educational tools such as videos can improve understanding and satisfaction. However, further efforts are needed to ensure that increased knowledge translates into higher compliance with preventive measures, ultimately reducing the risk of VTE.
Keywords: post-operative thromboprophylaxis, patient knowledge, VTE education
Introduction
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common complication among post-operative patients, and is associated with significant morbidity and mortality.1 VTE is highly preventable through various prophylactic measures, ranging from conservative measures such as early mobilisation, to mechanical prophylaxis such as intermittent pneumatic compression (ICP), and pharmacological prophylaxis such as peri-operative anticoagulation. Despite well-established guidelines from professional societies,1–3 VTE prophylaxis practices vary widely across institutions. Evidence suggests a considerable gap between optimal thromboprophylaxis as suggested by experts and real-world implementation.4 Many healthcare-providers (HCPs) and at-risk patients either lack awareness of VTE risks or are uncertain about applying prophylactic measures effectively.4 Knowledge of VTE plays a pivotal role in adherence to the optimal thromboprophylaxis, and studies have suggested that a multifaceted educational approach could significantly improve VTE prophylaxis utilization.5,6 Various methods, including educational videos, administrative interventions, and continuing medical education programs, can be used to improve the knowledge of patients and HCPs.7–9 However, no prospective study has systematically evaluated the impact of an educational program on VTE knowledge among post-operative patients and their HCPs, nor examined whether knowledge improvement translates into better adherence to prophylaxis guidelines. To address this gap, we conducted a prospective, non-randomised controlled study to evaluate the impact of a brief education material on VTE knowledge among post-operative patients and their HCPs. This study will assess knowledge levels before and after exposure to educational materials and examine whether increased awareness leads to improved utilisation of and adherence to VTE prophylaxis. The findings of this study could help inform strategies for enhancing compliance and reducing the burden of VTE in patients undergoing surgery.
Materials and Methods
This prospective, single-centre, non-randomised, controlled trial was conducted at a 1,700 beds university-affiliated hospital. The study duration was 12 months, and it involved of patients aged ≥18 years scheduled for elective major surgical operations (group A) and their HCPs (group B, including ward nurses and nursing assistants). The major exclusion criteria were: 1. Inability to provide informed consent, and 2. Inability to comprehend the study protocol, 3. Visually or auditorily impairment affecting participation, or 4. History of VTE.
VTE knowledge was assessed using validated questionnaires, adapted and modified from previous studies.10–13 Separate sets of questionnaires were used for patients (Set A, total score 45, Supplementary Appendix 1A) and their HCPs (Set B, Supplementary Appendix 1B), with scores expressed as the percentage of correct response. The overall knowledge was categorized, using Bloom’s cut-off point, as good if the score was between 80 and 100%, moderate if the score was between 60 and 79%, and poor if the score was less than 60%.14 The questionnaires were initially developed in English, translated into Chinese, and back-translated to ensure accuracy. A panel of experts—including surgeons, vascular specialists, internal medicine physicians, and nurse consultants —reviewed the study instruments for face and content validity. The questionnaires were tested on 15 volunteers, and internal reliability was evaluated using Cronbach’s alpha coefficient, which demonstrated strong consistency, yielding a Cronbach’s alpha coefficient of 0.86. Patient’s satisfaction with VTE thromboprophylaxis was assessed using existing hospital patient survey form which assesses patients’ experiences on a 5-point Likert scale.
The intervention consisted of 2-minute educational videos, developed using PowerPoint® slides with audio narration. The educational material for patients was adapted from publicly available patient education resources (Video S1), whereas the educational material for the HCPs was sourced from Continuous Medical Education (CME) platforms (https://www.smartpatient.ha.org.hk/en/smart-patient-web/disease-management/disease-information/disease/DeepVeinThrombosis). Both videos were administered using a mobile device, with optional headphone use.
Questionnaire Set A was first administered to a group of patients after admission, serving as the control group. After a four-week interval, a separate group of patients and their HCPs completed Set A (patients) and Set B (HCPs), both before and immediately after the intervention. The four-week interval between the control and intervention groups was chosen arbitrarily to minimize behavioural influence on the patients and HCPs. The flow of this study is summarized in Figure 1.
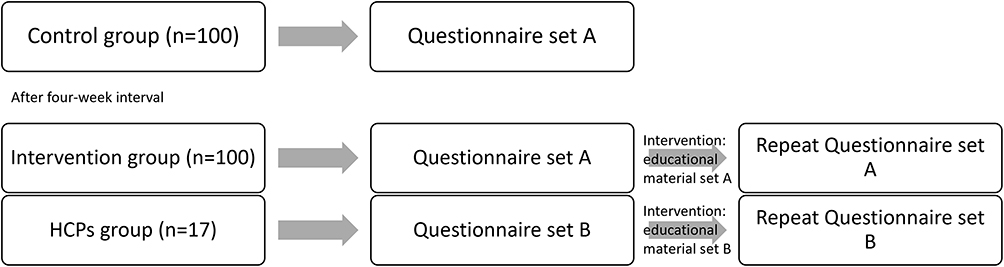 |
Figure 1 Study flow diagram. |
Data Collectable and Outcomes
Baseline patient demographics, medical and surgical backgrounds, laboratory results, clinical presentations, and operative records were collected. The VTE risk was calculated using the Caprini risk score.15 The prescription of VTE prophylactic measures such as early mobilisation, intermittent pneumatic compression, gradual compression stockings, and pharmacological thromboprophylaxis, were recorded. The occurrence of VTE such as DVT or PE within 30 days of hospital admission as confirmed by imaging studies was documented.
The primary outcome measured in this study was the difference in VTE knowledge between the control group, and intervention group following the intervention. The secondary outcomes measured in this study were changes in HCP knowledge before and after the intervention, differences in VTE thromboprophylaxis utilisation, patient satisfaction and VTE occurrence rate between the two patient groups.
Statistical Methods
Data analysis was performed using the STATA version 15 software (College Station, TX, USA). Data are reported as mean ± standard deviation (SD) or frequency (%). Comparisons between groups were made using the unpaired Student’s t-test for continuous variables, Fisher’s exact test for categorical variables, or Mann–Whitney U-test for ordinal variables. Based on previous research, the estimated difference in VTE knowledge score was 0.25–0.57.5,8,10,12 Therefore, an estimated sample size of 200 patients (100 patients in each group) was required to detect a difference at a 5% significance level and 80% power.
Ethics
Written informed consent was collected from individuals when they were enrolled. This study was conducted in accordance with the Declaration of Helsinki. The application for research ethics was granted by the Joint CUHK-NTEC Clinical Research Ethics Committee (HA-RE001F3) and was registered at Clinicaltrials.gov (NCT05548010).
Results
A total of 200 patients (mean age 59.1, 46.5% female) and 17 HCPs (mean age 34.5, 64% female) participated in this study, and their characteristics are shown in Tables 1 and 2. Baseline demographics, including the Caprini score, were comparable between the two patient groups. The Majority (95.0%) of the participants underwent major surgery, defined by the Caprini score, as procedures requiring general or regional anaesthesia for >45 min, including open, laparoscopic, or arthroscopic procedures.15 42% had a current or history of malignancy, whereas 48% had chronic cardiopulmonary disease. The mean Caprini score was 6.2, with 24.5% scoring 7 or higher, indicating a high (>1.8%) risk of postoperative VTE.16
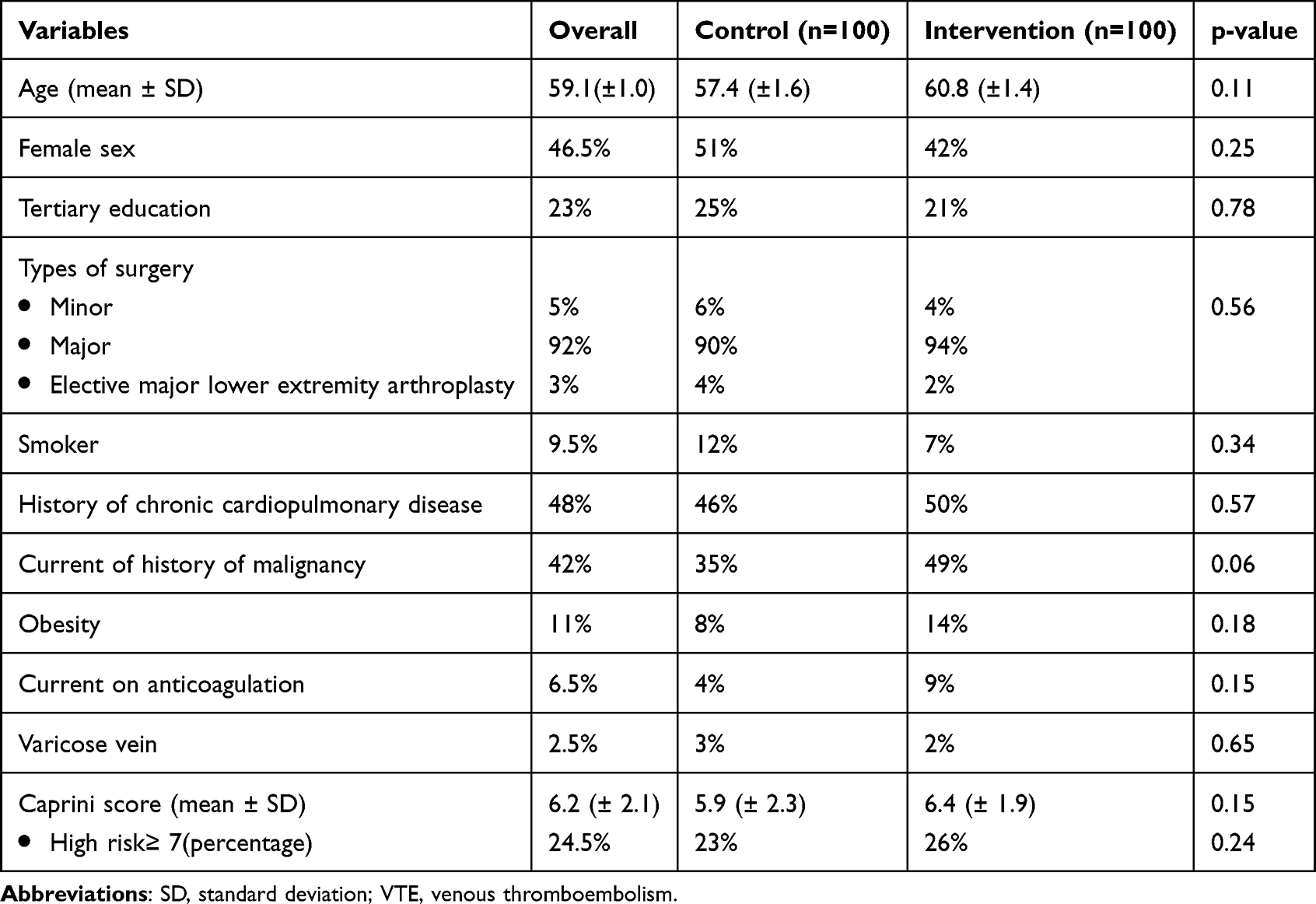 |
Table 1 Characteristics of the Study Participants |
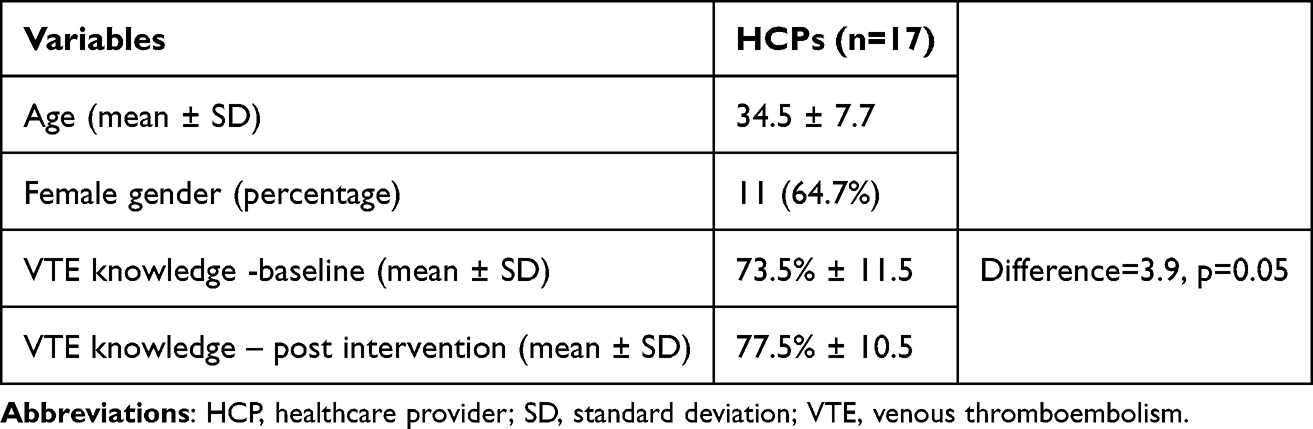 |
Table 2 VTE Knowledge of the HCPs |
Baseline VTE knowledge was similarly low between the two groups, with scores of 29.4% and 29.6%, respectively. Majority (92% and 91%) of subjects exhibited poor knowledge. A higher education level was significantly associated with higher scores (coefficient of interaction=5.49, p=0.026), whereas age and gender showed no such association. After the educational material, the VTE knowledge in the intervention group significantly improved by 16.4 points (55% increase), reaching 46.1% (Table 3 and Figure 2). The portion of subjects with moderate knowledge increased significantly from 9% to 18% (Figure 3). The breakdown of the different aspects of the VTE knowledge component is presented in Table 4. At baseline, most participants were unable to identify the risk factors, signs and symptoms, complications, and measures of thromboprophylaxis for VTE, although the majority recognised that VTE is a preventable disease. After the intervention, significant improvements were observed across various knowledge domains. Despite an enhanced understanding of VTE thromboprophylaxis, the proportion of patients willing to receive pharmacological thromboprophylaxis remained low (20%). Among the overall cohort, 42.5% received VTE thromboprophylaxis and only 4.5% received pharmacological thromboprophylaxis. The utilisation rates of VTE thromboprophylaxis were similar across groups (Table 3) and no VTE events were recorded during the study period. Overall, 66% of patients expressed satisfaction (score of ≥ 3 on the Likert scale) with their thromboprophylaxis at baseline, which was similar between the groups. After the intervention, satisfaction increased significantly by 26% to 93% in the intervention group. The HCPs demonstrated satisfactory knowledge level at baseline (73.5%), with a statistically insignificant improvement to 77.5% following the intervention (Table 2).
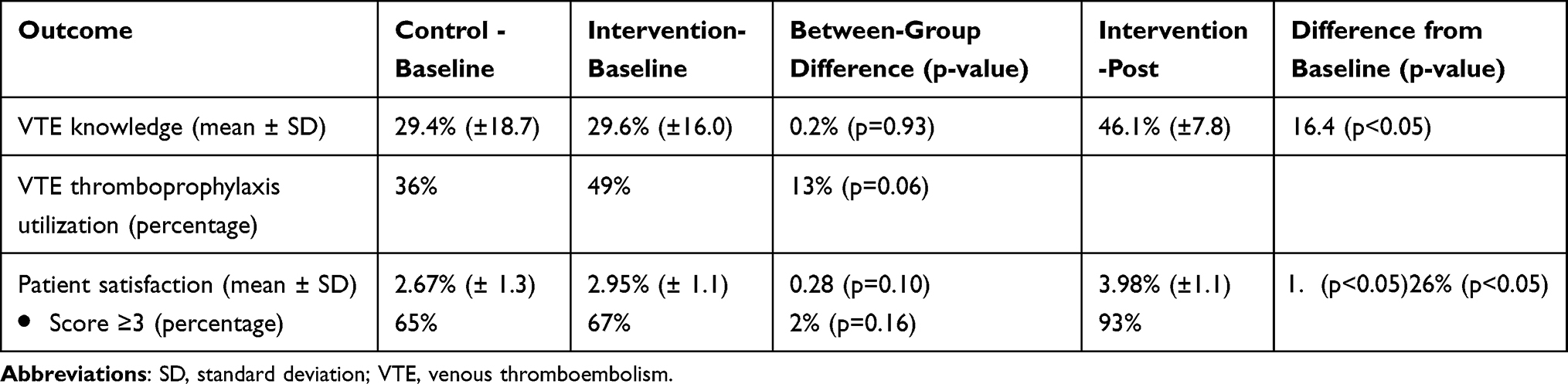 |
Table 3 Difference in VTE Knowledge, Thromboprophylaxis Utilization and Patient Satisfaction |
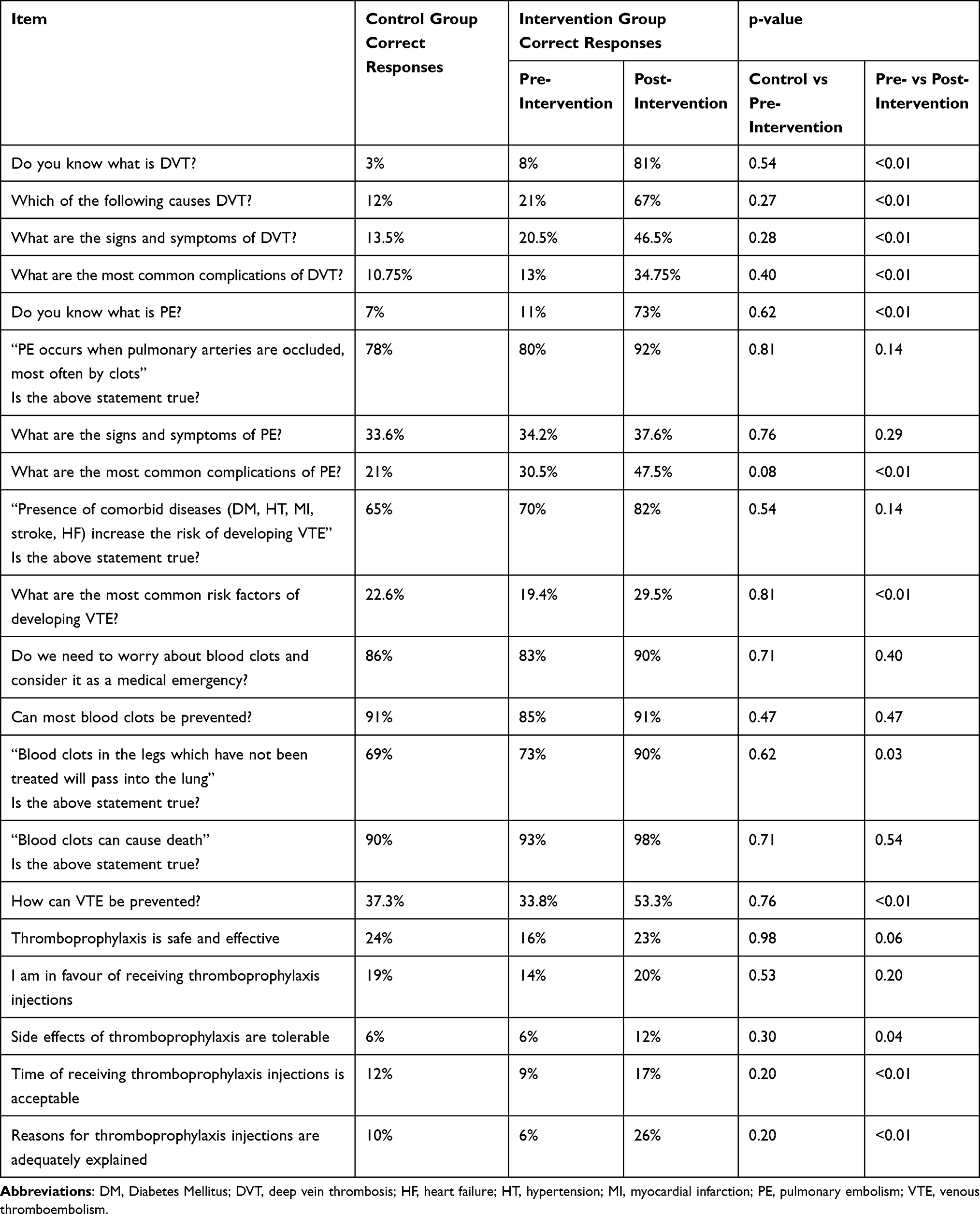 |
Table 4 Breakdown of Items of VTE Knowledge Questionnaire |
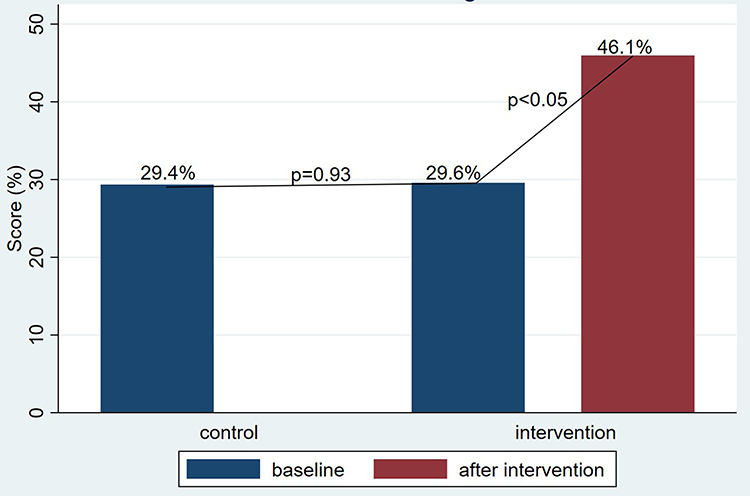 |
Figure 2 Differences in VTE knowledge between groups. |
 |
Figure 3 Bloom’s categories of patients’ VTE knowledge level. |
Discussion
This prospective study revealed a low level of knowledge regarding VTE among patients undergoing surgery, which is consistent with previously published studies.5–7,10,12,17 Participants demonstrated insufficient awareness of DVT causes, symptoms, and complications, yet showed greater familiarity with PE, particularly its symptoms, likely due to educated guesses given the context of the question. For example, participants might be able to guess that respiratory symptoms such as difficulty breathing and fast breathing are symptoms of PE, simply because PE is a condition that affects the respiratory system. However, the association between DVT and PE was poorly understood by the participants. The participants also lacked awareness of the key VTE risk factors. The most recognised risk factor was prolonged immobility, which is consistent with the results of previous studies. However, other key risk factors, such as hospitalisation, surgery, and cancer, were less well-recognised by the participants. These findings underscore the need to improve education regarding VTE prevention in high-risk patients.
Despite the gap in specific knowledge, most participants correctly recognised VTE as a serious, potentially fatal, but preventable condition, in contrast to international studies, where only 45% of patients believed that blood clots could be prevented.11 Regarding VTE thromboprophylaxis, only 24% of the participants believed that pharmacological thromboprophylaxis was safe and effective and only 20% were willing to receive it. This contrasts with findings from Jordan, where 89.8% perceived VTE thromboprophylaxis as safe, and 60.4% were willing to receive it.17 This reluctance may reflect cultural preferences, particularly among older Chinese patients who favour noninvasive treatments over Western medications.18
The 2-minutes education materials significantly enhanced patient knowledge, particularly in awareness of VTE causes and symptoms, underscoring the effectiveness of structured educational tools.8,9 Increased patient satisfaction with VTE thromboprophylaxis post intervention suggests better acceptance and the potential for improved adherence in high-risk populations, although this was not significant in our cohort. Despite the significant improvement in score after the intervention, the knowledge level remained suboptimal, with notable deficient persisting in patients understanding of VTE risk factors, complications, and thromboprophylaxis measures. These gaps highlight the need for enhanced educational strategies. Incorporating additional emphasis on these areas, supplemented by interactive question-and-answer sessions after the intervention may further improve patient comprehension and engagement.
HCPs exhibited adequate baseline knowledge of VTE prophylaxis, surpassing the levels reported in previous studies from other regions.13 The intervention did not significantly improve HCP knowledge, likely because of the high baseline scores. However, despite the incentives, the low participation rate among HCPs may introduce potential bias and limit the generalisability of the study results. Future studies should explore alternative strategies for improving HCP engagement.
Limitations
This study has several limitations. First, although we used a validated set of questions, closed-ended questions may have enabled participants to guess the answers rather than responding within the limits of their knowledge. Second, despite reaching the sample size estimation, the cohort remained small, restricting the strength of the conclusions and generalisability. Another factor limiting the generalisation is the single-centre setting, which further hinders the applicability of our findings beyond the study setting.
Conclusion
This study highlights a low baseline level of VTE knowledge among surgical patients and demonstrates that educational materials could effectively improve the knowledge level and patient satisfaction with thromboprophylaxis. Given the high risk of VTE in surgical populations, routine patient education regarding VTE should be integrated into the perioperative care protocols.
Acknowledgments
We acknowledge Mr. Adrian Jackson and his team from the Medical Protection Society Foundation for their invaluable guidance and support throughout this study. This study was supported by the Medical Protection Society Foundation.
Disclosure
This study was supported by the Medical Protection Society Foundation (MPF 8210006620). The authors report no conflicts of interest in this work.
References
1. Anderson DR, Morgano GP, Bennett C, et al. American society of hematology 2019 guidelines for management of venous thromboembolism: prevention of venous thromboembolism in surgical hospitalized patients. Blood Adv. 2019;3(23):3898–3944. doi:10.1182/bloodadvances.2019000975
2. Bates SM, Greer IA, Middeldorp S, Veenstra DL, Prabulos AM, Vandvik PO. VTE, thrombophilia, antithrombotic therapy, and pregnancy: antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e691S–e736S. doi:10.1378/chest.11-2300
3. Liew NC, Alemany GV, Angchaisuksiri P, et al. Asian venous thromboembolism guidelines: updated recommendations for the prevention of venous thromboembolism. Int Angiol. 2017;36(1):1–20. doi:10.23736/S0392-9590.16.03765-2
4. Henke PK, Kahn SR, Pannucci CJ, et al. Call to action to prevent venous thromboembolism in hospitalized patients: a policy statement from the American heart association. Circulation. 2020;141(24):e914–e931. doi:10.1161/CIR.0000000000000769
5. Apenteng PN, Fitzmaurice D, Litchfield I, et al. Patients’ perceptions and experiences of the prevention of hospital-acquired thrombosis: a qualitative study. BMJ Open. 2016;6(12):e013839. doi:10.1136/bmjopen-2016-013839
6. Nana M, Shute C, Williams R, Kokwaro F, Riddick K, Lane H. Multidisciplinary, patient-centred approach to improving compliance with venous thromboembolism (VTE) prophylaxis in a district general hospital. BMJ Open Qual. 2020;9(3):e000680. doi:10.1136/bmjoq-2019-000680
7. Nahar D, Nizam A, Farrow M, Restifo A, Nimaroff M. Improving patient compliance with mechanical venous thromboembolism prophylaxis. J Healthc Qual. 2018;40(3):163–171. doi:10.1097/JHQ.0000000000000137
8. Marini BL, Funk K, Kraft MD, et al. The effects of an informational video on patient knowledge, satisfaction and compliance with venous thromboembolism prophylaxis: a pilot study. Patient Educ Couns. 2014;96(2):264–267. doi:10.1016/j.pec.2014.05.008
9. Chehab R, Abboud R, Bou Zeidan M, et al. The impact of a randomized community-based intervention on the awareness of women residing in lebanon toward breast cancer, cervical cancer, and intimate hygiene. Healthcare. 2024;12(23):2422. doi:10.3390/healthcare12232422
10. Le Sage S, McGee M, Emed JD. Knowledge of venous thromboembolism (VTE) prevention among hospitalized patients. J Vasc Nurs. 2008;26(4):109–117. doi:10.1016/j.jvn.2008.09.005
11. Wendelboe AM, McCumber M, Hylek EM, et al. Global public awareness of venous thromboembolism. J Thromb Haemost. 2015;13(8):1365–1371. doi:10.1111/jth.13031
12. Almodaimegh H, Alfehaid L, Alsuhebany N, et al. Awareness of venous thromboembolism and thromboprophylaxis among hospitalized patients: a cross-sectional study. Thromb J. 2017;15(1):19. doi:10.1186/s12959-017-0144-2
13. Lloyd NS, Douketis JD, Cheng J, et al. Barriers and potential solutions toward optimal prophylaxis against deep vein thrombosis for hospitalized medical patients: a survey of healthcare professionals. J Hosp Med. 2012;7(1):28–34. doi:10.1002/jhm.929
14. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13:1949–1960. doi:10.2147/IDR.S258736
15. Lobastov K, Barinov V, Schastlivtsev I, Laberko L, Rodoman G, Boyarintsev V. Validation of the Caprini risk assessment model for venous thromboembolism in high-risk surgical patients in the background of standard prophylaxis. J Vasc Surg Venous Lymphat Disord. 2016;4(2):153–160. doi:10.1016/j.jvsv.2015.09.004
16. Pannucci CJ, Swistun L, MacDonald JK, Henke PK, Brooke BS. Individualized venous thromboembolism risk stratification using the 2005 caprini score to identify the benefits and harms of chemoprophylaxis in surgical patients: a meta-analysis. Ann Surg. 2017;265(6):1094–1103. doi:10.1097/SLA.0000000000002126
17. Jarab AS, Al-Azzam S, Badaineh R, Mukattash TL, Bsoul R. Awareness and perception of thromboembolism and thromboprophylaxis among hospitalized patients in Jordan. Curr Clin Pharmacol. 2020;15(1):72–80. doi:10.2174/1574884714666190823162055
18. Sun KS, Cheng YH, Wun YT, Lam TP. Choices between Chinese and Western medicine in Hong Kong - interactions of institutional environment, health beliefs and treatment outcomes. Complement Ther Clin Pract. 2017;28:70–74. doi:10.1016/j.ctcp.2017.05.012
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.