Back to Journals » Medical Devices: Evidence and Research » Volume 18
Evaluating the Impact of Smart Infusion Pump Interoperability on Reducing Medication Administration Errors: A Systematic Literature Review
Authors Borrelli EP ![]() , Lucaci JD
, Lucaci JD ![]() , Wilson NS, Taneja A
, Wilson NS, Taneja A ![]() , Weiss M, Beer I
, Weiss M, Beer I ![]()
Received 13 February 2025
Accepted for publication 7 April 2025
Published 15 April 2025 Volume 2025:18 Pages 247—260
DOI https://doi.org/10.2147/MDER.S522534
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Eric P Borrelli,1 Julia D Lucaci,2 Nicole S Wilson,3 Ashley Taneja,2 Mia Weiss,2 Idal Beer3
1Health Economics and Outcomes Research, MMS, Becton, Dickinson and Company, San Diego, CA, USA; 2HEOR Strategic Planning; Becton, Dickinson and Company, Franklin Lakes, NJ, USA; 3Medical Affairs, MMS, Becton, Dickinson and Company, San Diego, CA, USA
Correspondence: Eric P Borrelli, Health Economics and Outcomes Research (HEOR), Becton, Dickinson and Company, 3750 Torrey View Ct, San Diego, CA, 92130, USA, Email [email protected]
Purpose: Medication administration errors remain a persistent issue in the US healthcare system, impacting patient safety and leading to worsened outcomes, including increased mortality. Smart infusion pump interoperability with electronic health records (EHRs) has the potential to reduce intravenous (IV) medication administration errors. Smart Infusion pumps safely deliver IV medications using drug libraries that set standard dosing limits. Interoperability is their ability to wirelessly connect to EHRs to receive medications orders directly minimizing error-prone manual programming steps. However, despite being implemented over a decade ago, its real-world impact remains largely underexplored.
Methods and Materials: A systematic literature review (SLR) of PubMed/Medline and Embase in November 2024 identified peer-reviewed studies assessing medication administration errors pre- and post- interoperability implementation in the inpatient hospital setting. The primary outcome measured error types directly impacted by interoperability. The secondary outcome assessed the cumulative reduction in medication administration errors.
Results: Three studies met the inclusion criteria, spanning general community hospitals, pediatric facilities, and intensive care units (ICUs). For the primary outcome of assessing medication administration errors impactable by interoperability, interoperability implementation resulted in a 15.4% to 54.8% reduction in specific medication administration errors. For the secondary outcome of all medication administration errors, the cumulative reductions in medication administration errors post-implementation ranged from 21.2% to 90.5%, with variability influenced by baseline compliance, study setting, and patient populations.
Conclusion: Smart infusion pump interoperability demonstrated consistent potential to enhance medication safety by addressing key error types and reducing cumulative errors in real-world settings. However, future research is needed to assess its impact on adverse drug events, clinician workflows, and patient outcomes. These findings underscore the importance of tailored implementation strategies to maximize interoperability’s effectiveness in improving patient safety.
Plain Language Summary: Medication administration errors are a common issue in hospitals in the United States, with the potential to impact patient safety and lead to worsened outcomes. Smart infusion pump interoperability with electronic health records has the potential to reduce intravenous (IV) medication administration errors. Smart infusion pumps are infusion pumps that have drug libraries with standardized dosing. Interoperability is the technological advancement that wirelessly connects smart infusion pumps with EHRs, allowing medication orders to transfer directly instead of being entered manually. However, despite being implemented over a decade ago, its real-world impact remains largely underexplored in clinical practice. Therefore, we conducted a systematic literature review to identify studies assessing the impact of implementing smart infusion pump interoperability on medication administration errors in the inpatient hospital setting. Our review identified three studies assessing this impact. Two of the studies assessed our primary outcome of assessing medication administration errors impactable by interoperability and saw a post-implementation reduction ranging from 15.4% to 54.8%. All three of the studies assessed our secondary outcome of all medication administration errors and saw post-implementation reductions range from 21.2% to 90.5% post-implementation. Smart infusion pump interoperability demonstrated consistent potential to enhance medication safety by addressing key error types and reducing cumulative errors in real-world settings.
Keywords: smart infusion pump, interoperability, auto programming, medication administration errors, infusion errors, preventable adverse events
Introduction
Medical errors in the United States (US) first received major attention after the publication of To Err is Human: Building a Safer Health System by the Institute of Medicine in 1999, which brought to light how prevalent medical errors are, and that 44,000–98,000 deaths occur annually due to preventable medical errors.1 In response, policy and facility best practices have been implemented at local, state, and federal levels to improve patient safety.2 However, despite these efforts, medical errors remain a persistent issue in the US healthcare system.2 Approximately 5% of US adults experience a diagnostic error in outpatient settings,3 while 2.15% of inpatient stays involve an adverse drug event,4 and 0.59% of inpatient stays result in a preventable adverse drug event (pADE).5
In the hospital setting, intravenous (IV) infusions are a major contributor to medications errors,6,7 as they represent the most common route of administration.8 It is estimated that 85–90% of hospitalized patients receive IV infusions,9 and more than 50% of adverse drug events in hospitals are attributed to IV medications.10 A systematic review and Bayesian analysis of nine studies found that 21.7% (95% confidence interval (CI) 6.51–48.8) of medication errors for IV therapy occur during the administration phase.11
Medication administration errors, particularly those involving high-risk medications, are also a pervasive challenge in healthcare.2 Of particular concern, 3.9% of adverse drug events originating during hospital admissions led to mortality in 2014, resulting in over 18,000 deaths.4 These errors, such as incorrect drug selection, undocumented orders, and bypassing of safety systems, underscore the need for robust interventions like interoperability. Recent evidence suggests that interoperability not only reduces errors but also minimizes the cascading effects of such errors, which often lead to severe adverse events in vulnerable populations, particularly in high-risk settings such as neonates and intensive care unit (ICU) patients.12,13
Technological advancements, such as smart infusion pumps and interoperability with electronic health records (EHRs), have emerged as tools to reduce the risk of medication errors and improve patient safety.14 Smart infusion pumps are medical devices that safely deliver IV medications using built-in drug libraries to standardize dosing. Interoperability is their ability to connect with EHRs to wirelessly receive and program medication orders, rather than a user manually programming. Smart pump libraries are designed to catch programming errors, while interoperability automates the transfer of infusion parameters from the EHR to the smart pump, reducing manual entry (Figure 1).15 Smart pump interoperability is recommended as a potential prevention strategy to help mitigate manual medication administration errors.16 In 2018, the Institute for Safe Medication Practices (ISMP) published Guidelines for Optimizing Safe Implementation and Use of Smart Infusion Pumps, emphasizing the importance of interoperability in error prevention.15 Approximately 87.9% of US hospitals have adopted smart pumps as of 2020 according to a survey conducted by the American Society of Health-System Pharmacists.17 However, only about 9–15% have implemented interoperability between these pumps and their EHR.17–20 This gap highlights the underutilization of available technology to improve medication safety.
 |
Figure 1 Infusion-Related Medication Administration Errors Impacted by Interoperability*. Abbreviations: DERS, Dose Error Reduction Software; ID, Identification. Notes: *While some infusion-related medication administration errors may overlap across categories, this figure focuses on their primary impact to highlight interoperability’s role. Context and use cases should be given consideration when interpreting categorization |
An analysis by the ECRI Institute found that 28% of infusion-related events could potentially have been prevented with smart pump drug libraries, and an additional 47% of events could have been averted through smart pump-EHR interoperability.21 However, achieving these reductions is inherently more challenging, as interoperability builds upon smart pump systems already equipped with robust error prevention mechanisms. As a result, interoperability targets a narrower scope of remaining errors – yet these tend to be the most high-risk and clinically significant errors, with the potential to cause serious adverse events. A pre-/-post implementation study demonstrated the use of auto-programming reduced high-risk medication errors, with programming errors involving high-alert drugs dropping from 84% to 16%.22 Moreover, manual programming errors, which account for a substantial portion of administration and documentation errors, were also dramatically reduced. This highlights the importance of evaluating whether interoperability effectively reduces errors in real-world settings, particularly as improvements become increasingly incremental.
Although interoperability is inherently intended to reduce medication administration errors, its real-world impact has remained underexplored for over a decade since this advancement in healthcare technology was implemented. It is essential to assess whether its adoption has effectively reduced medication errors and improved patient safety in clinical settings. To address this gap, we conducted a systematic literature review (SLR) to evaluate the peer-reviewed literature and determine whether the implementation of smart infusion pump interoperability has successfully reduced medication errors and/or adverse drug events in healthcare settings.
Methods
Search Strategy
A SLR was conducted of PubMed/Medline and Embase in November 2024, attempting to identify published peer-reviewed literature that quantitatively measured the impact that smart infusion pump interoperability has on medication administration errors in the hospital setting. The search strategy is detailed in Appendix Tables 1 and 2. A review of citations of the studies undergoing full-text review was also conducted to identify studies that potentially met our inclusion criteria but were not indexed in the search databases or included different key terms.23–26 This review was conducted according to best practices25–28 and was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Appendix Table 3).29,30 A meta-analysis was not performed due to the limited number of studies and heterogeneity in study designs, methodologies, and outcomes. Given these differences, a systematic literature review was the most appropriate approach to evaluate and synthesize the available evidence on smart pump interoperability and medication administration errors. Defining the Population, Intervention, Comparator, and Outcomes (PICO) of the SLR, the population of interest was patients receiving infusions in the inpatient setting, the intervention of smart infusion pumps with interoperability, the comparator was smart infusion pumps without interoperability, and the outcomes were medication administration errors.
Selection Process
Articles were included if they quantitatively measured the impact of interoperability on medication administration errors in the inpatient setting and were published in English. Published conference abstracts could be included if they provided enough information regarding the study methodology, intervention of interest, and outcomes in the study and was consistent with our inclusion/exclusion criteria or if there was a conference poster that went along with the published abstract that provided this information. Studies were excluded if they only measured the impact that interoperability could have had on reducing errors, errors that were caught prior to administration, or compliance outcomes. Additional exclusion criteria consisted of studies assessing only insulin infusion pumps, qualitative studies, narrative reviews, editorials, SLRs, studies conducted in the outpatient setting only, and non-comparative studies. After removing duplicates, two reviewers independently screened abstracts, followed by a full-text review that passed the abstract screening phase. Conflicting decisions of study inclusion/exclusion were to be rectified by a third author reviewing the article of interest and making the final determination. However, conflicting decisions did not occur in this review.
Outcomes of Interest
The primary outcome was assessing the impact of infusion smart pump interoperability on medication administration errors. We categorized these errors as administration errors directly impacted by interoperability (Table 1), which included:
- Wrong drug library16
- Unauthorized/undocumented orders (medications)16
- Omitted medications16
- Improper dose16,21
- Wrong rate16,21
- Wrong duration16,21
- Wrong concentration16,21
- Wrong patient/patient ID error16
- Wrong medication16,21
- Wrong route16,21
- Wrong time16,21
- Dose error reduction software (DERS) limits16
- Wrong weight programmed16,21
- Bypassing drug library16
- Errors in the primary/secondary setting22
For inclusion in the primary outcome, studies had to stratify medication administration errors by type of error across the pre-implementation and post-implementation phases or explicitly report the medication administration errors that were impacted by interoperability.
The secondary outcome assessed the cumulative reduction in medication administration errors before and after implementing interoperability. This outcome was assessed so that we could include studies that did not stratify errors by error type but still measured the overall impact on medication administration errors post interoperability implementation.
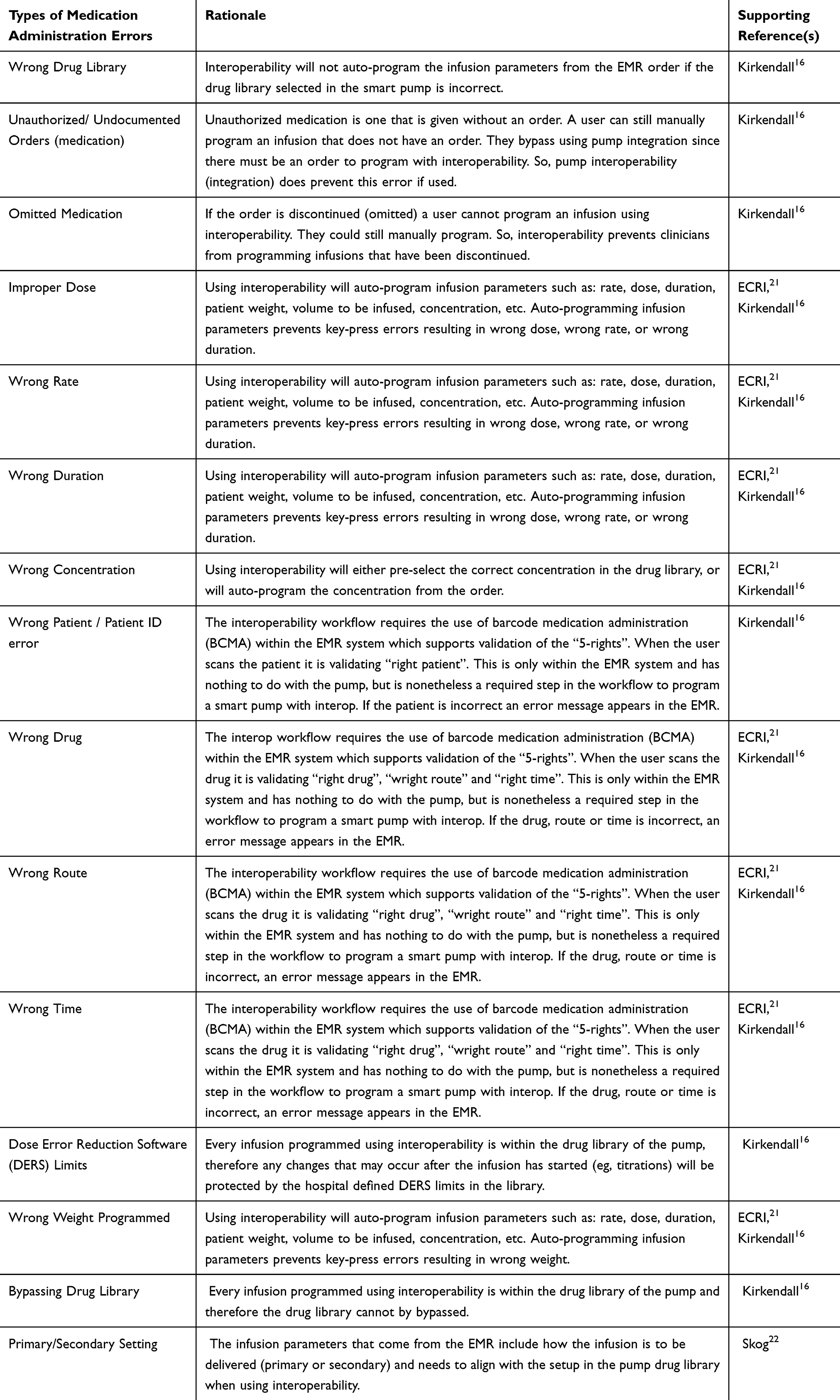 |
Table 1 Types of Infusion Errors That Interoperability Could Prevent |
Data Abstraction
Data was abstracted from included studies by a single reviewer, with validation performed by a separate reviewer. Extracted data consisted of title, first author, year of publication, study objective, study design, setting, time period, types of medication administration errors, results, and key limitations. Quality assessments of included studies were conducted by two authors utilizing the National Institutes of Health’s Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies.31
Results
The SLR returned 146 unique studies, with 32 undergoing full-text review and 3 meeting our inclusion criteria (Figure 2).13,22,32 Reasons for exclusion of articles that were not included in our review include outcomes assessed not being relevant to our inclusion criteria, the intervention of interest not being interoperability, and the analysis not being quantitative. The quality for the included studies was rated as fair for all three studies (Appendix Table 4). Two of the studies met the criteria for the primary outcome,22,32 while one additional study met the inclusion criteria for the secondary outcome (Table 2).13 For the primary outcome, the reduction in medication administration errors that could be impacted by interoperability post-implementation ranged from 15.4% to 54.8% (Figure 3).22,32 For the secondary outcome, the reduction in medication administration errors post-implementation ranged from 21.2% to 90.5%.13,22,32 None of the included studies included the specific medications that were related to the specific medication administration errors observed,13,22,32 while one of the studies included specific medications related to errors caught before administration.32
 |
Table 2 Included Study Demographic Information and Results |
 |
Figure 2 Flowchart of Studies Identified During the Systematic Literature Review. |
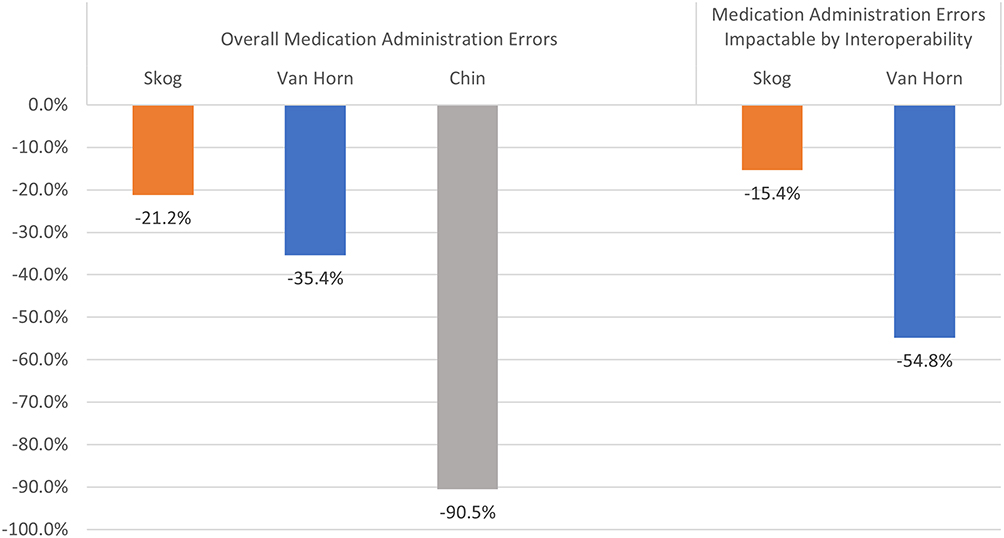 |
Figure 3 Impact of Smart Pump Interoperability on Medication Administration Errors. |
Study 1: Multi-Hospital Setting
Skog et al conducted a pre-post study at a health system consisting of 3 hospitals in San Diego, California with bed size ranging from 181 to 524 beds.22 The study assessed the impact of smart pump interoperability on medication errors during a pre-period (June to August 2017) and a post-period (August to September 2018).22 Among 350 infusions in the pre-period, 144 administration errors (41.1%) were recorded, compared to 110 errors (32.4%) across 367 infusions in the post-period, showing a 21.2% reduction in the overall errors.22 When focusing on administration errors directly impacted by interoperability, 132 errors (37.7%) were observed in the pre-period and 117 errors (31.9%) in the post-period, reflecting a reduction of 15.4%.22 High-risk medication errors were also significantly reduced, decreasing by 46.9% (12.8% in the pre-period vs 6.8% in the post-period, p=0.01).22
Study 2: Pediatric Setting
VanHorn et al conducted a retrospective pre-post study across two pediatric facilities within the same health system in Louisville, Kentucky.32 The analysis spanned a pre-period (January to June 2020) and a post-period (January to June 2022), covering 143,997 and 165,342 infusions, respectively.32 In the pre-period, 39 errors (0.027%) were observed, compared to 29 errors (0.018%) in the post-period, resulting in 35.4% reduction in overall errors.32 Errors specifically impacted by interoperability showed a greater reduction, with 27 (0.019%) errors in the pre-period and 14 errors (0.008%) in the post period, showing a 54.8% reduction in these specific errors.32 Before interoperability, 38% of severe harms averted were attributed to critical medication errors but this decreased to 24% post-interoperability. (p< 0.001).32
Study 3: Intensive Care Unit
Chin et al conducted a pre-post observational study in the ICU of a tertiary hospital in Australia.13 The pre-period (February to March 2022) included 1727 infusions, while the post-period (May to June 2022) included 1505 infusions with interoperability.13 The impact of interoperability was assessed by variances deemed “unintended variance/error” by a clinical pharmacist.13 These errors included incorrect drug library settings, discrepancies in volume/rate programing, incorrect start/end time, and others.13 During the pre-period, 360 infusions (20.85%) had an unintended variance/error, which decreased to 30 (1.99%) in the post-period, showing a 90.5% reduction in time-sensitive errors.13
Discussion
Key Findings and Implementation Challenges
This SLR identified three published studies that attempted to assess the impact of implementing smart infusion pump interoperability on medication administration errors, all of which demonstrated reductions in errors. The three studies spanned 6 institutions, across different hospital settings including general community hospitals, pediatric hospitals, and an ICU of a hospital, providing consistent results that highlight interoperability’s potential to reduce medication administration errors in diverse settings.13,22,32 However, none of the studies evaluated the impact of interoperability on adverse drug events, which underscores the need for further research to explore this aspect.
Despite these potential improvements, challenges remain in maximizing the benefits of smart infusion pump interoperability. Schnock et al emphasized that bypassing embedded safety systems and drug libraries undermines the full potential of these technologies.12 Their analysis revealed that 50% of errors in their study could have been prevented if interoperability and safety systems had been used appropriately. This highlights a critical gap in compliance and workflow adherence, which may limit the overall effectiveness of interoperability in real-world settings. Addressing these gaps requires focused efforts on training, workflow integration, and policy reinforcement to ensure that automated infusion programming is utilized as intended, reducing reliance on manual programming and mitigating preventable errors.
Variability in Error Reduction Across Studies
The studies included in this review highlight variability in reductions of medication administration errors associated with interoperability, driven by baseline factors and study-specific contexts. Skog et al reported a 15.4% reduction in errors, likely influenced by the inclusion of workflow-related issues not directly impacted by interoperability and high baseline compliance rates, emphasizing the role of existing prevention mechanisms.22 VanHorn et al, in a pediatric setting, demonstrated a 54.8% reduction, reflecting interoperability’s effectiveness in high-risk populations but with limited generalizability due to unique pediatric care factors.32 The complexity of pediatric settings introduces additional challenges, as errors in this population are often associated with weight-based dosing, frequent changes in infusion parameters, and heightened vulnerability to adverse outcomes. These factors can amplify the risk of programming inaccuracies and require tailored solutions to maximize interoperability’s effectiveness.
Chin et al observed a 90.5% reduction in unintended errors in an ICU, showcasing interoperability’s benefits in high-acuity environments under clinical oversight, though generalizability may be limited to hospitals with differing workflows.13 This reduction may have stemmed from high-risk overrides of drug library settings, a critical issue in ICU environments where timely administration of medications is essential for patient safety. By mitigating these overrides, interoperability further enhances the ability to reduce time-sensitive errors, which are particularly common with complex medication regimens. These findings underscore the need to consider baseline compliance, setting-specific challenges, and pre-existing prevention mechanisms when evaluating interoperability’s impact.
Comparison to Previous Literature
This SLR advances the findings of previous reviews, such as those conducted by Li et al,33 Chaudhry et al,34 and Jones et al,35 by offering a more targeted and rigorous evaluation of medication administration errors specifically impacted by smart infusion pump interoperability. Unlike earlier reviews, which broadly assessed health information technologies and EHR adoption on quality and safety outcomes, this review focuses on quantifying specific error types, including incorrect infusion rates, undocumented orders, and bypassed safety checks. Additionally, this review incorporates newer studies published in recent years, reflecting the most up-to-date evidence on interoperability’s role in medication safety. By analyzing data from diverse clinical settings, including pediatric, general hospital, and ICU, it provides a comprehensive and globally relevant perspective. This focused approach fills critical gaps in the literature by demonstrating the measurable impact of interoperability on medication errors while emphasizing its applicability across high-risk and varied healthcare settings.
Interoperability’s Impact on Medication Errors
Medication administration errors for infused medications are highly prevalent in hospitals, with reported errors ranging from 5% to 70%.11,12,22,36,37 A multisite study by Schnock et al at 10 hospitals found that even with dose error reduction software (DERS), 60% of the 1164 infusions analyzed still contained errors (n=699).12 Notably, 50% of these errors could have been prevented with interoperability as previously mentioned.12 None of the hospitals included in this study had smart pump interoperability, further highlighting gaps in implementation and use of available safety technologies. Despite ECRI’s report over a decade ago showing interoperability’s potential to reduce medication administration errors,21 our review identified only three eligible studies, underscoring a critical research gap. Some factors for this may include hospitals conducting this research for internal information only. Additionally, hospitals or health-systems may be concerned about publishing research showing their medication error rates from a liability or reputational perspective. One additional potential reason may be that hospitals and health-systems intrinsically know that interoperability reduces medication administration errors, and therefore it is not something that needs to be studied from a research and/or budget perspective.
While the impact of smart pump interoperability on medication errors remains underexplored, studies have consistently showed its ability to enhance drug library compliance, indirectly contributing to preventing errors. For example, Skog et al observed compliance rates increasing from 92% pre-interoperability to 94% post-interoperability (no p-value was provided).22 Similarly, VanHorn et al reported compliance increased from 94% to 96.7% due to interoperability (no p-value was provided).32 A community hospital in Texas saw a significant increase in compliance from 73.8% to 82.9% (p<0.001) post-interoperability.38 Smart-pump interoperability across a large health-system saw significant increases in compliances in half of the regions (4 of 8), and nonsignificant increases in 3 of the additional regions.39 It is important to note that while compliance rates seen in the Skog and VanHorn studies at baseline were much higher than typical real-world settings (eg 74%-80%),40 facilities with lower baseline compliance may experience even greater improvements post-implementation of interoperability. Increases in compliance are thought to lead to safer medication practices, ultimately reducing the risk of errors.
Although this review focused only on studies that assessed the impact on the occurrence of medication administration errors, related literature has shown that interoperability avoided potential medication errors. VanHorn et al showed a significant decrease in errors caught before administration from 197 to 20 (p<0.001).32 An analysis of the implementation of interoperability at a hospital in New York showed a reduction in significant near-miss medication errors from 1307 in the 12-month period pre-implementation to 400 in the 12-month period post-implementation.41 A general hospital in Pennsylvania found that after implementation of interoperability, the number of edits to infusion variables per month significantly reduced for the telemetry clinical care area from 56.9 to 14.2 (p<0.001) and from 61.2 to 14.7 (p<0.001) for the medical-surgical clinical care area.42 The previously mentioned community hospital in Texas that implemented interoperability saw a reduction in infusions generating alerts from 3.5% to 2.6% post-interoperability (p<0.001).38 Further evidence of interoperability’s impact comes from a Biltoft et al study, which noted a 19% monthly decrease in reprogrammed infusions in a 286-bed hospital due to a DERS alert,43 and a case study which found that infusion errors related to not following protocol by using pump auto-programming decreased by 50% from 20 errors per year to 10 errors per year post-interoperability.44
Broader Context and Existent Gaps
The variation in error reductions across studies highlights the influence of baseline error types, study designs, and contextual factors. VanHorn et al’s study demonstrated a larger reduction in errors directly impacted by interoperability compared to total errors, likely due to a higher baseline proportion of preventable errors in the pediatric setting, such as infusion programming issues.32 Conversely, Skog et al’s study showed a smaller relative reduction in interoperability-specific errors, possibly reflecting a broader inclusion of workflow-related errors not directly tied to interoperability mechanisms.22 Differences in baseline compliance with drug libraries, staff training, and existing technology may also account for the variability. These findings emphasize the importance of context in assessing interoperability’s impact and highlight the need to consider setting-specific factors when implementing and evaluating such interventions.
While not assessed directly in this review, medication errors can lead to adverse events for patients with the best available literature estimating that 1% of medication errors result in adverse drug events.45 Adverse drug events can be expensive and even fatal. An analysis of the Healthcare Cost and Utilization Project (HCUP) conducted by the Agency for Healthcare Research and Quality (AHRQ) of inpatient hospitalizations in the United States in 2014 estimated that the rate of adverse drug events originating during hospitalizations being 214.9 per 10,000 stays (2.15%), with a mean cost of $28,089 (in 2014 US$), a mean length of stay of 10.2 days, and an in-hospital mortality rate of 3.9%.4 However, not all adverse events are preventable, and a pooled analysis from a SLR of SLR’s found the pooled incidence of preventable adverse drug reactions to be 0.59 per 100 patients (0.59%).5 The reduction in medication errors seen from implementation of interoperability has the potential to lead to a reduction in adverse drug events and improved outcomes for patients, although further research is needed to assess this. In the study by VanHorn et al, the implementation of smart pump interoperability in pediatric settings was associated with a significant reduction in severe harm averted events, decreasing from 38% to 24% of total harm events.32 Additionally, Skog et al saw high-risk medication errors significantly decrease by 46.9%.22 This highlights the critical role of this technology in preventing life-threatening errors and reducing high-risk medication overrides.
Limitations
This review has several limitations. While this was a targeted SLR of peer-reviewed studies, there is a possibility that we may have inadvertently missed a study that utilized different key terms or was not indexed in the databases that we assessed. However, since two databases were utilized for the search and a review of citations was also conducted, the likelihood of missing a study is minimal. There is a chance that some research conducted on this topic may be published as white papers, or as non-peer-reviewed research that may have been omitted. Another potential limitation is publication bias. If researchers conducted a study or analysis and found negligible or even negative findings, they may be less likely to seek publication. Furthermore, the small number of included studies (n=3), although diverse, limits the generalizability of the findings. However, as stated above, one potential reason for the small number of studies on this topic may be due to hospitals or health-systems not wanting to publish research showing rates of medication errors in their facilities.
Conclusion
Implementation of infusion smart pump interoperability demonstrated significant reductions in medication administration errors across the three studies identified in this systematic review. These findings underscore the potential of interoperability to enhance patient safety in real-world clinical settings, by addressing key sources of errors, such as omitted errors, incorrect infusion rates, undocumented orders and others, and incorrect infusion rates, particularly in high-risk environments like neonatal ICUs (NICUs), ICUs, and pediatric care. While interoperability offers measurable safety benefits, its success depends on tailored workflows and consistent oversight to mitigate residual risks. Further exploration is needed to evaluate its broader impact on adverse drug events, cost-effectiveness, and long-term implications on clinician workload and patient outcomes. Expanding the evidence base will provide greater clarity on the generalizability and scalability of interoperability as a needed advancement in medication safety technology.
Abbreviations
AHRQ, Agency for Healthcare Research and Quality; CI, confidence interval; DERS, dose error reduction software; HER, electronic health records; HCUP, Healthcare Cost and Utilization Project; ICU, intensive care unit; ISMP, Institute for Safe Medication Practices; IV, intravenous; NICU, neonatal ICU; pADE, preventable adverse drug event; PICO, population intervention comparator and outcomes; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SLR, systematic literature review; US, United States.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Borrelli, Lucaci, Wilson, Taneja, Weiss, and Beer are employees and/or shareholders of Becton, Dickinson and Company. The authors report no other conflicts of interest in this work.
References
1. Institute of Medicine (US). Committee on Quality of Health Care in America. To Err Is Human: Building a Safer Health System. Kohn LT, Corrigan JM, Donaldson MS, editors. Washington (DC): National Academies Press (US); 2000. PMID: 25077248
2. Bates DW, Singh H. Two decades since to err is human: an assessment of progress and emerging priorities in patient safety. Health Aff. 2018;37(11):1736–1743. doi:10.1377/hlthaff.2018.0738
3. Singh H, Meyer AN, Thomas EJ. The frequency of diagnostic errors in outpatient care: estimations from three large observational studies involving US adult populations. BMJ Qual Saf. 2014;23(9):727–731. doi:10.1136/bmjqs-2013-002627
4. Weiss AJ, Freeman WJ, Heslin KC, Barrett ML. Statistical brief #234: adverse drug events in U.S. hospitals, 2010 versus 2014. Healthcare cost and utilization project (HCUP), agency for healthcare research and quality (QHRQ). Available from: https://hcup-us.ahrq.gov/reports/statbriefs/sb234-Adverse-Drug-Events.pdf.
5. Wolfe D, Yazdi F, Kanji S, et al. Incidence, causes, and consequences of preventable adverse drug reactions occurring in inpatients: a systematic review of systematic reviews. PLoS One. 2018;13(10):e0205426. doi:10.1371/journal.pone.0205426
6. Aspden P, Wolcott J, Bootman JL, Cronenwett LR. Preventing Medication Errors (2007). Institute of Medicine. 2007. Available from: https://nap.nationalacademies.org/catalog/11623/preventing-medication-errors.
7. Wittich CM, Burkle CM, Lanier WL. Medication errors: an overview for clinicians. Mayo Clin Proc. 2014;89(8):1116–1125. doi:10.1016/j.mayocp.2014.05.007
8. Nuckols TK, Paddock SM, Bower AG, et al. Costs of intravenous adverse drug events in academic and nonacademic intensive care units. Med Care. 2008;46(1):17–24. doi:10.1097/MLR.0b013e3181589bed
9. Institute for Safe Medication Practices (ISMP). ISMP Safe Practice Guidelines for Adult IV Push Medications: a compilation of safe practices from the ISMP Adult IV Push Medication Safety Summit. Institute for Safe Medication Practices. 2015. Available from: https://www.ismp.org/sites/default/files/attachments/2017-11/ISMP97-Guidelines-071415-3.%20FINAL.pdf.
10. Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA.;285(16):2114–2120. doi:10.1001/jama.285.16.2114.
11. McDowell SE, Mt-Isa S, Ashby D, Ferner RE. Where errors occur in the preparation and administration of intravenous medicines: a systematic review and Bayesian analysis. Qual Saf Health Care. 2010;19(4):341–345. doi:10.1136/qshc.2008.029785
12. Schnock KO, Dykes PC, Albert J, et al. The frequency of intravenous medication administration errors related to smart infusion pumps: a multihospital observational study. BMJ Qual Saf. 2017;26(2):131–140. doi:10.1136/bmjqs-2015-004465
13. Chin K, Donovan J, Bingham G, Poole S, Tong E. Evaluation of smart pump interoperability with an electronic medical record system to improve infusion safety. Stud Health Technol Inform. 2024;310:1341–1342. doi:10.3233/SHTI231185
14. Antrim A. Improving Patient Safety with Smart Pump-EHR Interoperability. Pharmacy Times. Available from: https://www.pharmacytimes.com/view/improving-patient-safety-with-smart-pumpehr-interoperability.
15. Institute for Safe Medication Practices (ISMP). ISMP Guidelines for Optimizing Safe Implementation and Use of Smart Infusion Pumps. Institute for Safe Medication Practices. 2020. Available from: https://home.ecri.org/blogs/ismp-resources/guidelines-for-optimizing-safe-implementation-and-use-of-smart-infusion-pumps.
16. Kirkendall E, Timmons K, Huth H, Walsh K, Melton K. Human-based errors involving smart infusion pumps: a catalog of error types and prevention strategies. Drug Saf. 2020;43(11):1073–1087. doi:10.1007/s40264-020-00986-5
17. Pedersen CA, Schneider PJ, Ganio MC, Scheckelhoff DJ. ASHP national survey of pharmacy practice in hospital settings: dispensing and administration-2020. Am J Health Syst Pharm. 2021;78(12):1074–1093. doi:10.1093/ajhp/zxab120
18. Schneider PJ, Pedersen CA, Scheckelhoff DJ. ASHP national survey of pharmacy practice in hospital settings: dispensing and administration-2017. Am J Health Syst Pharm. 2018;75(16):1203–1226. doi:10.2146/ajhp180151
19. Tate J, Warburton P. Smart pump/EMR interoperability 2020: first look at customer satisfaction. KLAS Research. 2020. Available from: https://klasresearch.com/report/smart-pump-emr-interoperability-2020-first-look-at-customer-satisfaction/1500.
20. Institute for Safe Medication Practices (ISMP). Smart pumps in practice: survey results reveal widespread use, but optimization is challenging. Institute for Safe Medication Practices. 23: 1–5. Available from: https://www.ismp.org/sites/default/files/attachments/2018-04/20180405.pdf.
21. ECRI Institute. Infusion pump integration. Health Devices. 2013;42(7):210–221.
22. Skog J, Rafie S, Schnock KO, Yoon C, Lipsitz S, Lew P. The impact of smart pump interoperability on errors in intravenous infusion administrations: a multihospital before and after study. J Patient Saf. 2022;18(3):e666–e671. doi:10.1097/PTS.0000000000000905
23. Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. London: The Cochrane Collaboration. 2011. Available from: www.cochrane-handbook.org.
24. Cooper C, Booth A, Varley-Campbell J, Britten N, Garside R. Defining the process to literature searching in systematic reviews: a literature review of guidance and supporting studies. BMC Med Res Methodol. 2018;18(1):85. doi:10.1186/s12874-018-0545-3
25. Greenland S, O’Rourke K. Chapter 33: meta-Analysis. In: Rothman KJ, Greenland S, Lash TL, editors. Modern Epidemiology.
26. Centre for Reviews and Dissemination: systematic reviews: CRD’s guidance for undertaking systematic reviews in health care. York: University of York. Centre for Reviews and Dissemination, 2009. Available from: http://www.york.ac.uk/inst/crd/index_guidance.htm.
27. Cook DJ, Mulrow CD, Haynes RB. Systematic reviews: synthesis of best evidence for clinical decisions. Ann Intern Med. 1997;126:376–380. doi:10.7326/0003-4819-126-5-199703010-00006
28. Mandrik OL, Severens JLH, Bardach A, et al. Critical appraisal of systematic reviews with costs and cost-effectiveness outcomes: an ISPOR good practices task force report. Value Health. 2021;24(4):463–472. doi:10.1016/j.jval.2021.01.002
29. Moher D, Liberati A, Tetzlaff J, Altman DG, Group PRISMA. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi:10.1136/bmj.b2535
30. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 372. n71. doi:10.1136/bmj.n71
31. National Heart Lung and Blood Institute. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. National Institute of Health. 2014. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
32. VanHorn T, Harris J, Mayes S, Infanti LM, Kennedy A. Evaluation of the effect of smart pump interoperability on infusion errors in the pediatric hospital setting. J Pediatr Pharmacol Ther. 2024;29(3):323–330. doi:10.5863/1551-6776-29.3.323
33. Li E, Clarke J, Ashrafian H, Darzi A, Neves AL. The impact of electronic health record interoperability on safety and quality of care in high-income countries: systematic review. J Med Internet Res. 2022;24(9):e38144. doi:10.2196/38144
34. Chaudhry B, Wang J, Wu S, et al. Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Ann Intern Med. 2006;144(10):742–752. doi:10.7326/0003-4819-144-10-200605160-00125
35. Jones SS, Rudin RS, Perry T, Shekelle PG. Health information technology: an updated systematic review with a focus on meaningful use. Ann Intern Med. 2014;160(1):48–54. doi:10.7326/M13-1531
36. Sutherland A, Canobbio M, Clarke J, Randall M, Skelland T, Weston E. Incidence and prevalence of intravenous medication errors in the UK: a systematic review. Eur J Hosp Pharm. 2020;27(1):3–8. doi:10.1136/ejhpharm-2018-001624
37. Westbrook JI, Rob MI, Woods A, Parry D. Errors in the administration of intravenous medications in hospital and the role of correct procedures and nurse experience. BMJ Qual Saf. 2011;20(12):1027–1034. doi:10.1136/bmjqs-2011-000089
38. Wei W, Coffey W, Adeola M, Abbasi G. Impact of smart pump-electronic health record interoperability on patient safety and finances at a community hospital. Am J Health Syst Pharm. 2021;zxab287. doi:10.1093/ajhp/zxab287
39. Ubanyionwu S, Khandekar D, Mara KC, Teaford H. Enterprise standardization and convergence of large-volume infusion pump drug libraries. Am J Health Syst Pharm. 2023;80(23):1743–1751. doi:10.1093/ajhp/zxad172
40. Naguib A, Beer I, Ringwala S, Wilson N, Swenson D. Evaluation of utilization patterns from over one billion infusions: retrospective study on smart pump safety and practice improvement indicators.
41. Gerhart D Jr, O’Shea K, Muller S. Advancing medication infusion safety through the clinical integration of technology. Hosp Pract. 1995;41(4):7–14. doi:10.3810/hp.2013.10.1075
42. Prusch AE, Suess TM, Paoletti RD, Olin ST, Watts SD. Integrating technology to improve medication administration. Am J Health Syst Pharm. 2011;68(9):835–842. doi:10.2146/ajhp100211
43. Biltoft J, Finneman L. Clinical and financial effects of smart pump-electronic medical record interoperability at a hospital in a regional health system. Am J Health Syst Pharm. 2018;75(14):1064–1068. doi:10.2146/ajhp161058
44. Razzano L, Box A, Corrick K, McDowell J, Vitoux RR. Collaboration Fuels Success of Infusion Management Interoperability Initiative. Biomed Instrum Technol. 2018;52(1):38–43. doi:10.2345/0899-8205-52.1.38
45. Bates DW, Boyle DL, Vander Vliet MB, Schneider J, Leape L. Relationship between medication errors and adverse drug events. J Gen Intern Med. 1995;10(4):199–205. doi:10.1007/BF02600255
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.