Back to Journals » International Journal of Women's Health » Volume 18
Evaluating Maternal Serum SHH Levels in the First Trimester as a Potential Biomarker for Predicting Preeclampsia
Authors Deng C, Zhang S, Li C, Yang Z, Guo Q, Cheng Y ![]()
Received 10 September 2025
Accepted for publication 15 January 2026
Published 29 January 2026 Volume 2026:18 566603
DOI https://doi.org/10.2147/IJWH.S566603
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Caifeng Deng,1,* Si Zhang,2,* Chanyu Li,1 Zhiling Yang,1 Qin Guo,3 Yanmian Cheng4
1Department of Gynecology and Obstetrics, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, People’s Republic of China; 2Department of Emergency Medicine, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, People’s Republic of China; 3Department of Orthopedics, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, People’s Republic of China; 4Department of Infectious Diseases, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanmian Cheng, Department of Infectious Diseases, The First Affiliated Hospital of Chengdu Medical College, No. 278, The Middle Section of Baoguang Avenue, Xindu District, Chengdu, Sichuan, 610500, People’s Republic of China, Email [email protected] Qin Guo, Department of Orthopedics, The First Affiliated Hospital of Chengdu Medical College, No. 278, The Middle Section of Baoguang Avenue, Xindu District, Chengdu, Sichuan, 610500, People’s Republic of China, Email [email protected]
Objective: To determine whether first-trimester maternal serum Sonic Hedgehog (SHH) predicts subsequent preeclampsia and to compare its predictive performance with soluble fms-like tyrosine kinase-1 (sFlt-1) and placental growth factor (PlGF).
Materials and Methods: In a prospective cohort study, women with singleton pregnancies were enrolled at 8– 13 weeks’ gestation, clinical data were recorded, and fasting serum was collected. SHH, sFlt-1, and PlGF were quantified by ELISA in triplicate with coefficients of variation < 10%. Associations between SHH and subsequent preeclampsia were tested using multivariable logistic regression with adjusted confounders; discriminative ability was evaluated by ROC analysis and stratified for early-onset (≤ 34 weeks) and late-onset (> 34 weeks) preeclampsia.
Results: Among 2532 enrolled pregnancies, 271 developed preeclampsia and 2261 remained normotensive. First-trimester SHH concentrations were significantly lower in pregnancies that later developed preeclampsia, with the greatest decrement in early-onset disease. Compared to the highest SHH tertile, adjusted odds of preeclampsia were higher in the middle (OR 2.64; 95% CI 1.334– 5.38) and lowest tertiles (OR 5.21; 95% CI 3.15– 8.42). SHH achieved an AUC of 0.86 (95% CI 0.62– 0.91), with 81.46% sensitivity and 76.58% specificity at 58.26 ng/mL; sFlt-1 and PlGF yielded AUCs of 0.71 and 0.62, respectively. Performance was strongest for early-onset preeclampsia with an AUC of 0.93 (95% CI 0.67– 0.97); sensitivity 87.73%; specificity 82.43% at 62.37 ng/mL, and modest for late-onset preeclampsia with an AUC of 0.75 (95% CI 0.54– 0.86); sensitivity 73.42%; specificity 68.24% at 55.78 ng/mL.
Conclusion: Lower maternal serum SHH level in the first trimester is independently associated with later development of preeclampsia and provides clinically significant early prediction, particularly for early-onset disease. Incorporating SHH into first-trimester multiparametric screening alongside maternal factors and angiogenic markers may improve risk stratification and enable earlier prophylaxis and individualized antenatal surveillance.
Keywords: Sonic Hedgehog protein, first-trimester, biomarker, preeclampsia, extravillous trophoblast
Introduction
Pre-eclampsia is a serious hypertensive disorder of pregnancy, defined by the new onset of hypertension after 20 weeks of gestation, and it remains a leading global cause of maternal and perinatal morbidity and mortality.1,2 It affects approximately 2–8% of pregnancies and is associated with fetal growth restriction, placental abruption, preterm birth, and maternal cardiovascular complications.3–5 Early prediction and diagnosis remain challenging; however, timely identification of women at increased risk enables intensified antenatal surveillance and prophylactic interventions that can mitigate adverse outcomes for both mothers and fetuses.6,7 Current clinical approaches rely largely on maternal history combined with biophysical assessments, yet these approaches have limited predictive performance in early gestation, especially in the first trimester. Therefore, the discovery of robust first-trimester biomarkers has emerged as a promising strategy to facilitate earlier and more accurate prediction of preeclampsia.
Previous studies have linked the pathogenesis of preeclampsia to the shallow placental implantation and inadequate remodeling of the spiral arteries in the uterus.8–10 Successful placentation is a complex process dependent on highly orchestrated trophoblast biology. Villous cytotrophoblasts differentiate into either syncytiotrophoblasts or invasive extravillous trophoblasts.11 Extravillous trophoblasts can remodel the uterine spiral arteries into the high-capacity, low-resistance vessels necessary to support fetal growth.12 Inadequate extravillous trophoblast invasion and spiral artery transformation lead to uteroplacental malperfusion.13 This state provokes the release of anti-angiogenic and inflammatory factors into the maternal circulation, ultimately causing the maternal syndrome of hypertension and multi-organ dysfunction associated with preeclampsia.8,14 Consequently, molecules that regulate essential trophoblast functions, such as proliferation, differentiation, and invasion, are promising candidate biomarkers for the early prediction of preeclampsia.
SHH protein is the ligand that binds to the receptor Patched 1, leading to the activation of the Sonic Hedgehog signaling pathway.15 The Sonic Hedgehog signaling pathway is critical for normal placentation and plays a key role in regulating these essential trophoblast functions.16,17 Emerging evidence suggests that the placental Sonic Hedgehog signaling pathway is dysregulated in preeclampsia, with decreased levels of Sonic Hedgehog signaling pathway components observed in preeclamptic placentas.18 This dysregulation is thought to impair the trophoblast functions necessary for adequate uterine artery remodeling.19
Given that the process of placentation mainly occurs in the first trimester of pregnancy, we hypothesize that serum levels of SHH protein may be altered in the first trimester of pregnant women who develop preeclampsia later. This study aims to evaluate the predictive value of maternal serum SHH concentrations in the first trimester for the subsequent development of preeclampsia. Validation of SHH as an early predictive biomarker could identify women at high risk of preeclampsia, enabling intensified surveillance and timely preventive interventions to reduce adverse pregnancy outcomes.
Materials and Methods
Study Population
Ethical approval for this prospective, observational study was obtained from the Ethics Committee of The First Affiliated Hospital of Chengdu Medical College, and all participants provided written informed consent. Between January 2020 and December 2023, A total of 2942 pregnant individuals attending the obstetric outpatient clinic for routine antenatal visits in their first trimester of 8–13 weeks of gestation were screened. Eligibility required a singleton pregnancy, ultrasound confirmation of gestational age, and signed consent. Individuals with a history of hypertension, liver or kidney disease, diabetes mellitus, or cardiovascular disease were excluded. Enrolled participants were followed through delivery; those who miscarried or transferred antenatal care to other hospitals during follow-up were subsequently excluded. The final cohort comprised 2532 participants. The patient enrollment diagram was showed in Figure 1.
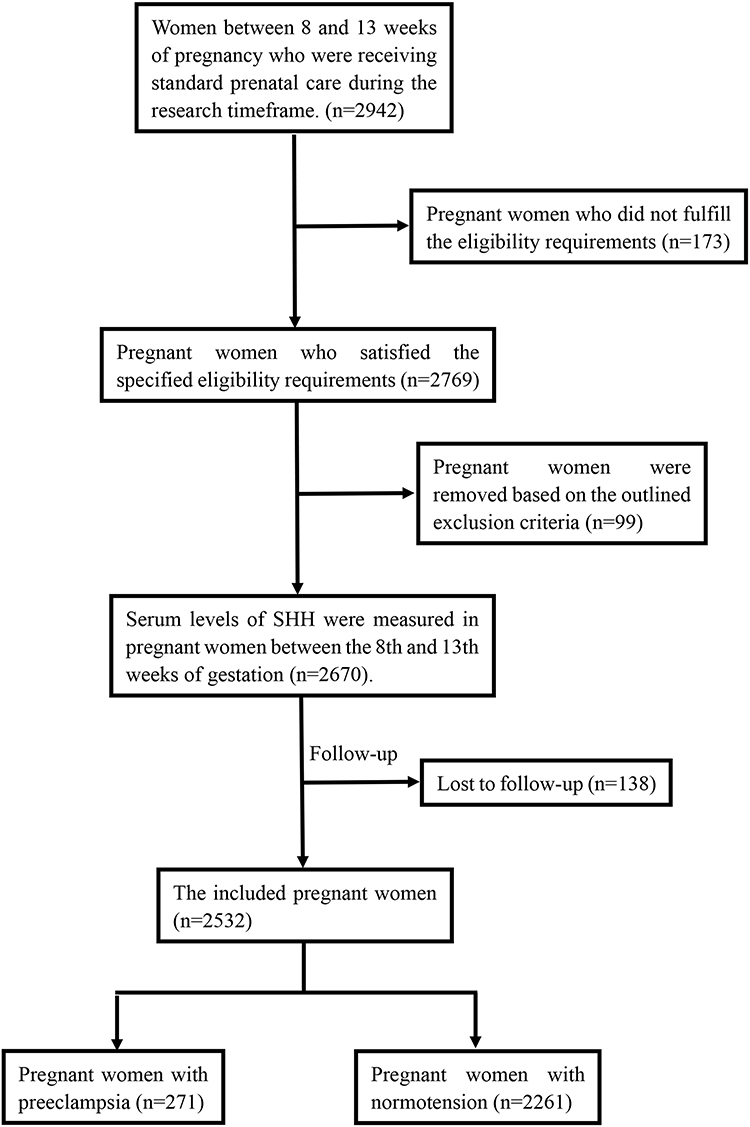 |
Figure 1 The patient enrollment diagram. |
Clinical Data Collection
At the initial obstetric outpatient visit for routine antenatal care, demographic and clinical information were recorded, including maternal age, smoking status, body mass index (BMI), parity, prior medical conditions, and blood pressure. Gestational age at enrollment was verified by ultrasonography. Preeclampsia was diagnosed according to the criteria of the International Society for the Study of Hypertension in Pregnancy (ISSHP).20
Laboratory Data Collection
During the first trimester of 8–13 weeks of gestation, peripheral venous blood was obtained after an overnight fast. Blood samples were centrifuged at 2000 g for 10 minutes to isolate serum, which was then aliquoted and stored at −80 °C until analysis. Routine laboratory tests, including fasting glucose, lipid profile, serum creatinine, liver function panels, and complete blood counts, were performed on automated analyzers according to standardized protocols in the Clinical Laboratory of the First Affiliated Hospital of Chengdu Medical College.
Quantification of Serum SHH, sFlt-1, and PlGF
Maternal serum concentrations of SHH, sFlt-1, and PlGF were assessed at 8–13 weeks of gestation using commercial ELISA kits (SHH: ab 100639, Abcam Co. Ltd., Shanghai, China; sFlt-1: DVR100C, R&D Systems, Minneapolis, MN, USA; PlGF: DPG00, R&D Systems, Minneapolis, MN, USA). All assays were performed strictly following the protocols of the manufacturers. In brief, diluted serum samples were dispensed into the manufacturer’s antibody-coated wells and incubated at room temperature for 2 hours. After thorough washing, horseradish peroxidase–conjugated detection antibodies were added for a 1-hour incubation. Plates were then washed, substrate solution was applied, and reactions proceeded in the dark for 30 minutes before being stopped. Optical density was read at 450 nm with a microplate reader (BioTek Instruments, Winooski, VT, USA). Each specimen was analyzed in triplicate, with the mean value used for subsequent analyses. Intra- and inter-assay coefficients of variation were maintained below 10%.
Statistical Analyses
Statistical analyses were conducted using IBM SPSS Statistics, version 31.0 (IBM Corp., Armonk, NY, USA). Variables with normal distributions are reported as mean ± standard deviation, and group differences were assessed with Student’s t-test. Associations between serum SHH levels and clinical or laboratory measures were evaluated using Pearson’s correlation. The relationship between serum SHH levels and subsequent preeclampsia was examined with logistic regression to adjust for potential confounders; adjusted odds ratios (ORs) and corresponding 95% confidence intervals (CIs) were reported.
To evaluate the early predictive value of serum SHH levels for preeclampsia, receiver operating characteristic (ROC) curve analysis was performed. The area under the ROC curve (AUC) with its 95% CI quantifies discriminative performance. The optimal threshold value was identified by maximizing Youden’s index. All statistical tests were two-sided, and P < 0.05 was considered statistically significant.
Results
Clinical Parameters of the Study Population
Of the 2532 enrolled pregnancies, 271 developed preeclampsia and 2261 remained normotensive. Statistical analyses revealed that pre-pregnancy BMI, maternal age, low-density lipoprotein cholesterol (LDL-C), triglycerides (TG), neonatal birth weight, gestational age at delivery, sFlt-1, and PlGF were significantly different between preeclampsia and normotensive groups (Table 1). In contrast, gestational age at enrollment, systolic and diastolic blood pressure, alanine aminotransferase (ALT), aspartate aminotransferase (AST), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), serum uric acid, and creatinine did not show statistical differences between the two groups (Table 1).
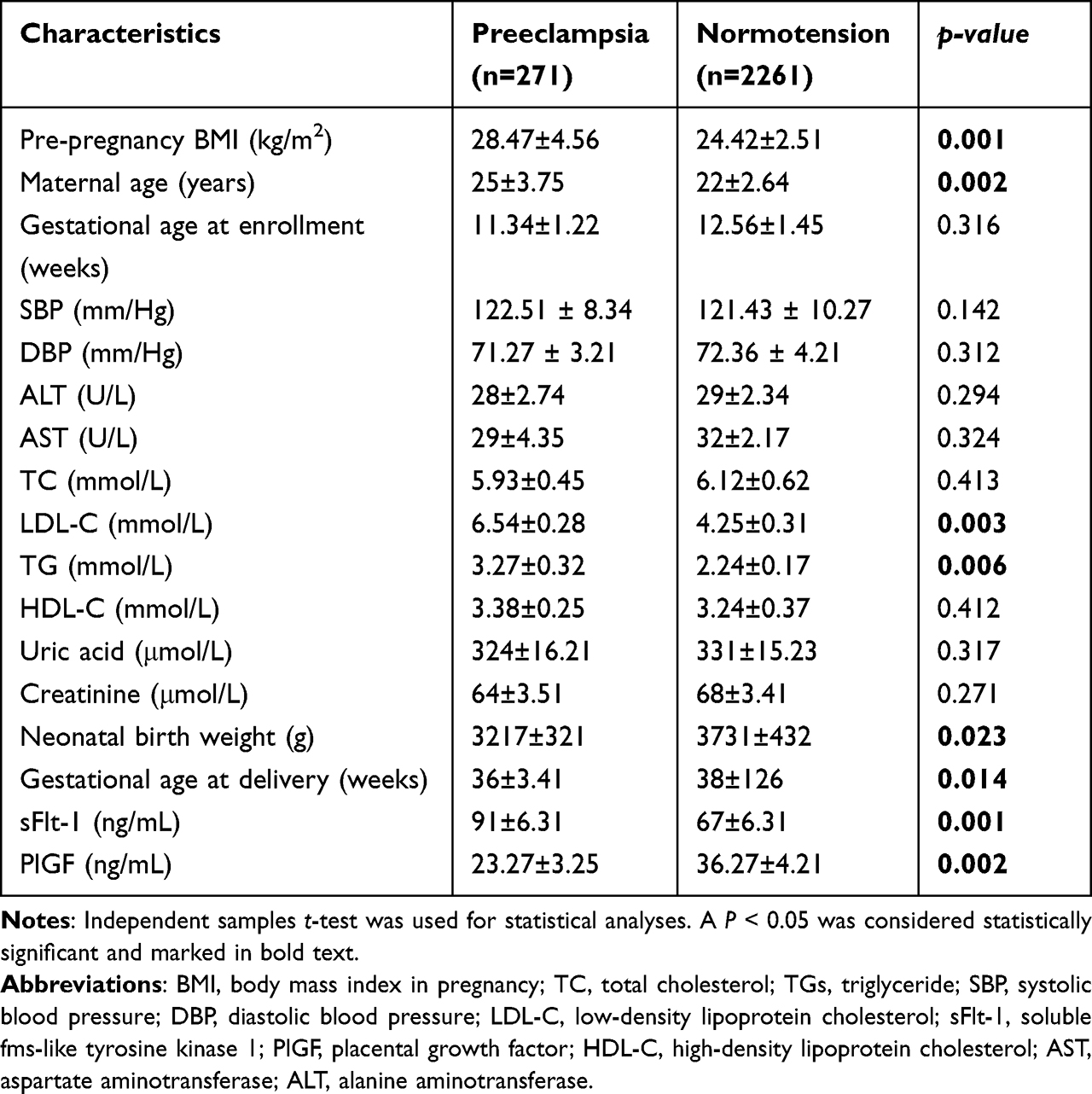 |
Table 1 Baseline Characteristics of the Study Population (n=2532) |
Maternal Serum SHH Levels in the First Trimester
First-trimester maternal serum SHH concentrations were significantly lower in individuals who subsequently developed preeclampsia than in those with normotensive pregnancies (Figure 2A). When preeclampsia was subclassified as early-onset (≤34 weeks) and late-onset (>34 weeks) cases, individuals in the early-onset group had significantly lower serum SHH values than individuals in the late-onset group (Figure 2B).
 |
Figure 2 Maternal serum SHH levels in the first trimester. (A) First-trimester maternal serum SHH concentrations were significantly lower in individuals who subsequently developed preeclampsia than in those with normotensive pregnancies. (B) Individuals in the early-onset preeclampsia group had significantly lower serum SHH values than individuals in the late-onset preeclampsia group. Statistical analyses were conducted using IBM SPSS Statistics, and group differences were assessed with Student’s t-test. A P < 0.05 was considered statistically significant. |
Correlations Between Serum SHH and Clinical Parameters
Pearson correlation analyses investigated the correlations between maternal serum SHH and clinical parameters for the preeclampsia and normotensive groups (Table 2). Negative associations of SHH with pre-pregnancy BMI, maternal age, systolic blood pressure, TGs, TC, sFlt-1, PlGF, and LDL-C were observed in the preeclampsia group (all P < 0.05). No significant associations were observed between SHH and other variables, including gestational age at enrollment, diastolic blood pressure, HDL-C, AST, ALT, creatinine, and uric acid, within the preeclampsia group (p > 0.05). In addition, maternal SHH was not significantly correlated with any measured clinical parameters in the normotensive group.
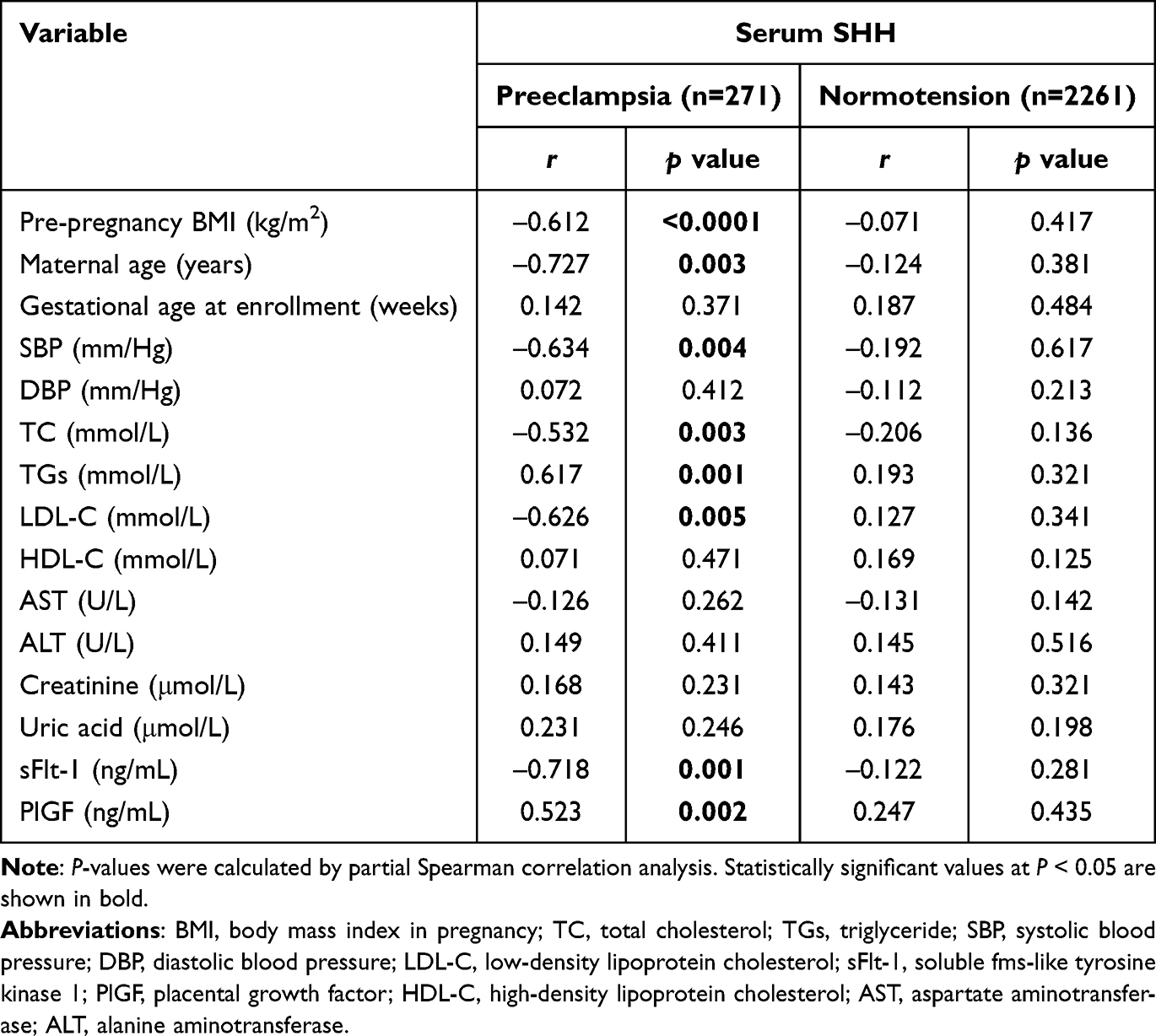 |
Table 2 Correlations Between Serum SHH and Clinical Parameters in the Two Groups |
Association of Serum SHH with Risk of Preeclampsia
The relationship between maternal serum SHH and the risk of preeclampsia was examined using multivariable logistic regression models with adjustment for potential confounders including maternal age, pre-pregnancy BMI, history of preeclampsia, and levels of TC, TG, HDL-C, LDL-C, sFlt-1, and PlGF. SHH concentrations were partitioned into tertiles based on their distribution. Across these tertiles, the prevalence of preeclampsia increased progressively from 6.23% to 28.42%, representing a more than fourfold difference when the highest tertile was compared to the lowest tertile (Table 3). Using the highest tertile as reference, women in the lowest and middle tertiles exhibited greater odds of preeclampsia, with adjusted ORs of 5.21 (95% CI, 3.15–8.42) and 2.64 (95% CI, 1.33–5.38), respectively (Table 3). When modeled as a continuous variable, lower SHH levels were associated with an increased risk of preeclampsia (adjusted OR, - 0.647; 95% CI, 0.321–0.928; p = 0.002).
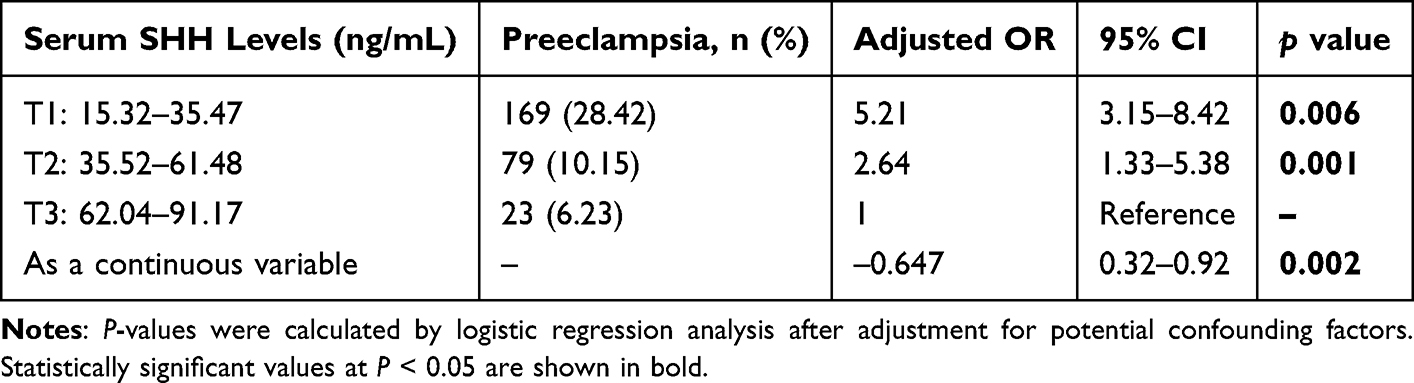 |
Table 3 Association of Serum SHH with Risk of Preeclampsia |
Predictive Performance of SHH for Preeclampsia
Receiver operating characteristic (ROC) analysis was used to assess the discriminatory ability of SHH for preeclampsia, with predictive performance compared with the two established markers, PlGF and sFlt-1. SHH demonstrated the highest predictive performance, yielding an AUC of 0.86 (95% CI, 0.62–0.91), surpassing both sFlt-1 and PlGF (Table 4). The corresponding AUCs were 0.71 (95% CI, 0.48–0.83) for sFlt-1 and 0.62 (95% CI, 0.45–0.84) for PlGF. At a cutoff of 58.26 ng/mL, SHH achieved the greatest sensitivity and specificity of 81.46% and 76.58%, respectively (Table 4). Collectively, these findings support SHH as a reliable biomarker for predicting preeclampsia.
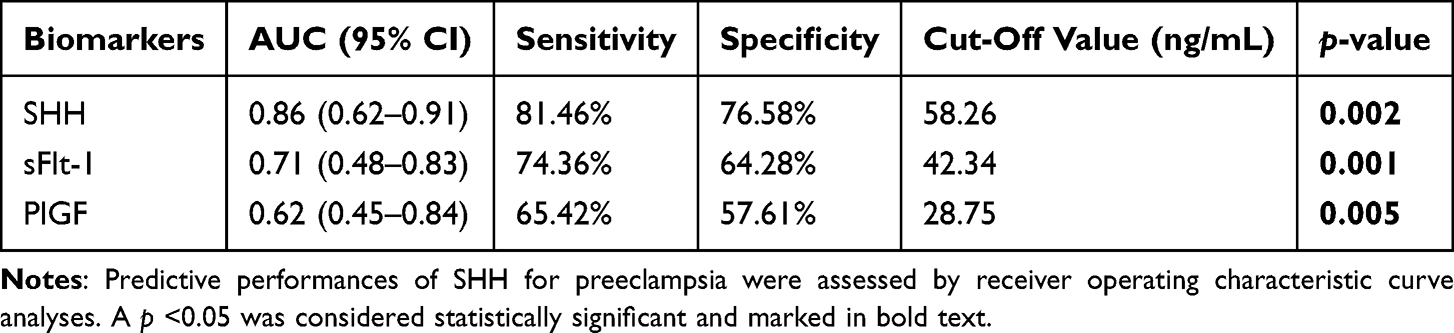 |
Table 4 Predictive Performance of SHH for Preeclampsia |
We further assessed the predictive performance of SHH for early-onset and late-onset preeclampsia. SHH showed stronger discrimination for early-onset preeclampsia, with an AUC of 0.93 (95% CI, 0.67–0.97; p = 0.001), compared with an AUC of 0.75 (95% CI, 0.54–0.86; p = 0.002) for late-onset disease (Table 5). For early-onset cases, a cut-off value of 62.37 ng/mL yielded sensitivity and specificity of 87.73% and 82.43%, respectively. For late-onset cases, a cutoff of 55.78 ng/mL produced sensitivity of 73.42% and specificity of 68.24% (Table 5).
 |
Table 5 Predictive Performance of SHH for Early-Onset and Late-Onset Preeclampsia |
Discussion
In this prospective study, first-trimester maternal serum SHH concentrations were significantly lower in pregnancies that later developed preeclampsia, with the greatest decrement observed in early-onset preeclampsia. SHH remained independently associated with preeclampsia after adjustment for conventional maternal factors and angiogenic markers and demonstrated promising discriminative performance in receiver operating characteristic analysis. These findings align with contemporary first-trimester screening paradigms that emphasize placentation biology and support the addition of mechanistically anchored placental biomarkers to improve early risk stratification.
SHH protein is the ligand that binds to the receptor Patched 1, leading to the activation of the Sonic Hedgehog signaling pathway.21 Our observations are biologically plausible in light of data implicating Sonic Hedgehog signaling as a regulator of trophoblast lineage specification, migration, and invasion, which are processes central to spiral artery remodeling.22–24 Hedgehog signaling is transduced via PTCH1/SMO and GLI transcription factors at the primary cilium of trophoblasts; disruption of ciliary structure or Hedgehog activity impairs motility, tube formation, and trophoblast fusion.18,24 Experimental models relevant to preeclampsia suppress Hedgehog pathway components and blunt trophoblast invasiveness, whereas pathway activation restores angiogenic balance and improves pregnancy outcomes; conversely, inhibition of the Hedgehog pathway abrogates these benefits.9,16,18,22 Together, these data suggest that reduced maternal SHH in early gestation may reflect insufficient placental Hedgehog signaling, heralding shallow trophoblast invasion and subsequent uteroplacental malperfusion, which are characteristics of preeclampsia.
Circulating markers such as sFlt-1 and PlGF have also been investigated for their predictive utility in preeclampsia.25,26 A study in the New England Journal of Medicine reported that an sFlt-1/PlGF ratio ≤38 reliably excluded development of preeclampsia within 1 week, with a negative predictive value of 99.3% (95% CI, 97.9–99.9%), a sensitivity of 80.0%, and a specificity of 78.3%. In contrast, ratios >38 yielded a positive predictive value of 36.7% (95% CI, 28.4–45.7%) for onset within 4 weeks, with a sensitivity of 66.2% and a specificity of 83.1%.27 Notably, these findings pertain to short-term risk assessment in pregnancies between 24 and 36 weeks’ gestation, which may limit their preventive impact earlier in pregnancy. By comparison, our data indicate that SHH can stratify risk as early as the first trimester, enabling clinicians to consider preventive strategies at an earlier stage.
From a clinical perspective, first-trimester identification of women at increased risk of preeclampsia has actionable implications.28,29 Risk-stratified care enables timely low-dose aspirin prophylaxis, optimization of maternal comorbidities, and closer surveillance to reduce severe maternal morbidity and iatrogenic prematurity.30,31 In our cohort, SHH achieved high sensitivity and specificity at an empirically derived cutoff and showed stronger performance for early-onset preeclampsia, the phenotype most tightly linked to placental pathology and adverse neonatal outcomes.32 These characteristics are precisely those desired in a triage biomarker deployed during the first trimester within competing-risks algorithms that already incorporate maternal factors, mean arterial pressure, uterine artery Doppler indices, and angiogenic proteins. Incorporating SHH into such frameworks may improve calibration and net reclassification beyond single-marker strategies, particularly for early-onset disease, where preventive benefit is greatest.
From a global health perspective, an attractive feature of SHH is that it can be measured on conventional ELISA platforms that are widely available, including in many low- and middle-income settings. In contrast to high-cost proprietary assays (eg, sFlt-1–based tests), first-trimester SHH measurement could provide a more affordable biochemical component of early risk stratification, helping to identify women who require closer antenatal surveillance where access to Doppler ultrasound and angiogenic markers is limited. However, our study did not include a formal cost-effectiveness analysis or implementation evaluation, and further work is needed to confirm the practicality and economic value of SHH-based screening in low-resource environments.
An important strength of our study is that all participants were recruited in the first trimester (8–13 weeks) and followed prospectively until delivery, allowing SHH to be evaluated as an early predictor of incident preeclampsia rather than a concurrent marker. This design ensured that maternal serum SHH was measured well before the onset of clinical disease and that the association we observed reflects true predictive value over the subsequent gestational follow-up, rather than a cross-sectional difference. The ability of low first-trimester SHH levels to identify women who later developed especially early-onset preeclampsia underscores its potential value within first-trimester risk-prediction strategies alongside established placental biomarkers.
The study also has limitations. First, it was conducted at a single center, which may limit generalizability to other populations and care settings; external validation is warranted. Second, despite adjustment for numerous potential confounders, residual confounding cannot be excluded; unmeasured factors, such as genetic susceptibility, socioeconomic conditions, and environmental exposures, may influence both serum SHH concentrations and preeclampsia risk. Finally, assay platform differences and preanalytical variability could affect reproducibility; future work should harmonize protocols and assess interlaboratory performance.
Conclusion
First-trimester maternal serum SHH concentrations were significantly lower in pregnancies that later developed preeclampsia and were an independent, clinically meaningful predictor, particularly for early-onset disease. These findings, consistent with the central role of Hedgehog signaling in trophoblast differentiation and invasion, support SHH as a promising addition to first-trimester screening strategies. With external validation and integration into multiparametric algorithms, SHH-based risk stratification could enable earlier interventions and individualized antenatal surveillance, thereby reducing the burden of preeclampsia for mothers and infants.
Abbreviations
AST, aspartate aminotransferase; ALT, alanine aminotransferase; BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; DBP, diastolic blood pressure; LDL-C, low-density lipoprotein cholesterol; sFlt-1, soluble fms-like tyrosine kinase 1; PlGF, placental growth factor; SBP, systolic blood pressure; SHH, Sonic Hedgehog; TC, total cholesterol; TG, triglyceride.
Ethics Approval
Informed consent was obtained from the study participants before the commencement of the study, and the study complies with the Declaration of Helsinki. This study was approved by the Ethics Committee of The First Affiliated Hospital of Chengdu Medical College (No. 23573465).
Acknowledgments
This article used artificial intelligence for language improvement.
Funding
This study was supported by the High Talent Project of Chengdu Medical College (No. CYFY-GQ70), the Sichuan Provincial Medical and Health Promotion Association (No. KY2022QN0294), and the Sichuan Science and Technology Program (No. 2024NSFSC1903).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Snead CM, Strassberg E, Overcash R, et al. Obstetricians’ knowledge and practices regarding the management of preeclampsia. J Matern Fetal Neonatal Med. 2020;33(17):2970–10. doi:10.1080/14767058.2019.1566311
2. Glisic M, Muka T, Franco OH. Cardiovascular screening and prevention strategies in women with history of preeclampsia: one size does not fit all. Eur J Prev Cardiol. 2020;27(13):1386–1388. doi:10.1177/2047487320908977
3. Strijbos LTM, Hendrix MLE, Al-Nasiry S, et al. Which first-trimester risk assessment method for preeclampsia is most suitable? A model-based impact study. Am J Obstet Gynecol MFM. 2023;5(7):100974. doi:10.1016/j.ajogmf.2023.100974
4. Roberge S, Bujold E, Nicolaides KH. Meta-analysis on the effect of aspirin use for prevention of preeclampsia on placental abruption and antepartum hemorrhage. Am J Obstet Gynecol. 2018;218(5):483–489. doi:10.1016/j.ajog.2017.12.238
5. Stubert J, Hinz B, Berger R. The role of acetylsalicylic acid in the prevention of pre-eclampsia, fetal growth restriction, and preterm birth. Dtsch Arztebl Int. 2023;120(37):617–626. doi:10.3238/arztebl.m2023.0133
6. Wataganara T, Leetheeragul J, Pongprasobchai S, et al. Prediction and prevention of pre-eclampsia in Asian subpopulation. J Obstet Gynaecol Res. 2018;44(5):813–830. doi:10.1111/jog.13599
7. Baschat AA. First-trimester screening for pre-eclampsia: moving from personalized risk prediction to prevention. Ultrasound Obstet Gynecol. 2015;45(2):119–129. doi:10.1002/uog.14770
8. Burton GJ, Redman CW, Roberts JM, et al. Pre-eclampsia: pathophysiology and clinical implications. BMJ. 2019;366:l2381. doi:10.1136/bmj.l2381
9. Zhou W, Wang H, Yang Y, et al. Trophoblast cell subtypes and dysfunction in the placenta of individuals with preeclampsia revealed by single‑cell RNA sequencing. Mol Cells. 2022;45(5):317–328. doi:10.14348/molcells.2021.0211
10. Li Y, Feng J, Bian Y, et al. EID1 plays a protective role in early-onset pre-eclampsia via promoting proliferation and invasion in trophoblast cells. Folia Histochem Cytobiol. 2022;60(1):31–43. doi:10.5603/FHC.a2022.0001
11. DaSilva-Arnold S, James JL, Al-Khan A, et al. Differentiation of first trimester cytotrophoblast to extravillous trophoblast involves an epithelial-mesenchymal transition. Placenta. 2015;36(12):1412–1418. doi:10.1016/j.placenta.2015.10.013
12. Li W, Zhang S, Ye S, et al. Evaluation of optimal trophoblastic models to mimic uterine vessel remodeling in human pregnancydagger. Biol Reprod. 2025;113(4):870–885. doi:10.1093/biolre/ioaf108
13. Zhang P. Decidual vasculopathy and spiral artery remodeling revisited II: relations to trophoblastic dependent and independent vascular transformation. J Matern Fetal Neonatal Med. 2022;35(2):395–401. doi:10.1080/14767058.2020.1718646
14. Lopez-Jaramillo P, Barajas J, Rueda-Quijano SM, et al. Obesity and preeclampsia: common pathophysiological mechanisms. Front Physiol. 2018;9:1838. doi:10.3389/fphys.2018.01838
15. Liu F, Feng XX, Zhu SL, et al. Sonic hedgehog signaling pathway mediates proliferation and migration of fibroblast-like synoviocytes in rheumatoid arthritis via MAPK/ERK signaling pathway. Front Immunol. 2018;9:2847. doi:10.3389/fimmu.2018.02847
16. Huang Y, Zheng XD, Li H. Protective role of SIRT1-mediated sonic hedgehog signaling pathway in the preeclampsia rat models. J Assist Reprod Genet. 2021;38(7):1843–1851. doi:10.1007/s10815-021-02158-5
17. Pan YB, Gong Y, Ruan HF, et al. Sonic hedgehog through Gli2 and Gli3 is required for the proper development of placental labyrinth. Cell Death Dis. 2015;6(2):e1653. doi:10.1038/cddis.2015.28
18. Ren Y, Xu Y, Wang Y, et al. Regulation of miR-375 and sonic hedgehog on vascular endothelial growth factor in preeclampsia rats and its effect on trophoblast cells. Biosci Rep. 2020. doi:10.1042/BSR20200613
19. Zhang Y, Zhang Y. Forkhead box C2 promotes the invasion ability of human trophoblast cells through Hedgehog (Hh) signaling pathway. Cell Biol Int. 2018;42(7):859–866. doi:10.1002/cbin.10953
20. Brown MA, Magee LA, Kenny LC, et al. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2018;13:291–310. doi:10.1016/j.preghy.2018.05.004
21. Dayer D, Bayati V, Ebrahimi M. Manipulation of sonic hedgehog signaling pathway in maintenance, differentiation, and endocrine activity of insulin-producing cells: a systematic review. Iran J Med Sci. 2024;49(2):65–76. doi:10.30476/ijms.2023.95425.2678
22. Chen YJ, Lee CI, Tsai PY, et al. Aspirin reverses the inhibitory effect of soluble fms-like tyrosine kinase-1 on trophoblast invasiveness and ciliogenesis through sonic hedgehog signaling in preeclampsia. Biochem Pharmacol. 2025;238:116975. doi:10.1016/j.bcp.2025.116975
23. Takai H, Kondoh E, Mogami H, et al. Placental sonic hedgehog pathway regulates fetal growth via the igf axis in preeclampsia. J Clin Endocrinol Metab. 2019;104(9):4239–4252. doi:10.1210/jc.2019-00335
24. Ritter A, Roth S, Kreis NN, et al. Primary cilia in trophoblastic cells: potential involvement in preeclampsia. Hypertension. 2020;76(5):1491–1505. doi:10.1161/HYPERTENSIONAHA.120.15433
25. Stepan H, Galindo A, Hund M, et al. Clinical utility of sFlt-1 and PlGF in screening, prediction, diagnosis and monitoring of pre-eclampsia and fetal growth restriction. Ultrasound Obstet Gynecol. 2023;61(2):168–180. doi:10.1002/uog.26032
26. Creswell L, O’Gorman N, Palmer KR, et al. Perspectives on the use of Placental Growth Factor (PlGF) in the prediction and diagnosis of pre-eclampsia: recent insights and future steps. Int J Womens Health. 2023;15:255–271. doi:10.2147/IJWH.S368454
27. Zeisler H, Llurba E, Chantraine F, et al. Predictive value of the sFlt-1: PlGF ratio in women with suspected preeclampsia. N Engl J Med. 2016;374(1):13–22. doi:10.1056/NEJMoa1414838
28. Health Ontario. First-trimester screening program for the risk of pre-eclampsia using a multiple-marker algorithm: a health technology assessment. Ont Health Technol Assess Ser. 2023;22(5):1–118. doi:10.25318/1310041501-eng
29. Poon LC, Shennan A, Hyett JA, et al. The International Federation of Gynecology and Obstetrics (FIGO) initiative on pre-eclampsia: a pragmatic guide for first-trimester screening and prevention. Int J Gynaecol Obstet. 2019;145(Suppl 1):1–33. doi:10.1002/ijgo.12802
30. Rolnik DL, Nicolaides KH, Poon LC. Prevention of preeclampsia with aspirin. Am J Obstet Gynecol. 2022;226(2S):S1108–S1119. doi:10.1016/j.ajog.2020.08.045
31. Johnson JM, Walsh JD, Okun NB, et al. The Implementation of Preeclampsia Screening and Prevention (IMPRESS) Study. Am J Obstet Gynecol MFM. 2023;5(2):100815.
32. van Esch JJ, van Heijst AF, de Haan AF, van der Heijden OW. Early-onset preeclampsia is associated with perinatal mortality and severe neonatal morbidity. J Matern Fetal Neonatal Med. 2017;30(23):2789–2794. doi:10.1080/14767058.2016.1263295
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.