Back to Journals » Clinical Ophthalmology » Volume 15
Etiology of Uveitis in Upper Egypt
Authors Abd El Latif E ![]() , Nooreldin A, Shikhoun Ahmed M
, Nooreldin A, Shikhoun Ahmed M ![]() , Elmoddather M, El Gendy W
, Elmoddather M, El Gendy W ![]()
Received 20 November 2020
Accepted for publication 8 January 2021
Published 18 January 2021 Volume 2021:15 Pages 195—199
DOI https://doi.org/10.2147/OPTH.S293131
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Eiman Abd El Latif,1 Asaad Nooreldin,2 Mohammed Shikhoun Ahmed,3 Mohamed Elmoddather,2 Wael El Gendy4
1Department of Ophthalmology, Faculty of Medicine, Alexandria University, Alexandria, Egypt; 2Department of Ophthalmology, Faculty of Medicine, Al-Azhar University, Assiut, Egypt; 3Department of Ophthalmology, Sohag Teaching Hospital, Sohag, Egypt; 4Department of Ophthalmology, Memorial Institute for Ophthalmic Research (MIOR), Giza, Egypt
Correspondence: Eiman Abd El Latif 5 Soliman Mahmoud Street, Cleopatra 12311, Alexandria, Egypt
Tel +211 4867-2963
Email [email protected]
Purpose: To report the causes of uveitis in a referral ocular inflammation clinic in Upper Egypt.
Methods: Retrospective medical chart review of all uveitis cases visiting a referral uveitis clinic during the period between January 2015 and January 2020.
Results: A total of 982 patients were included. Uveitis was bilateral in 51.7% of the patients. Anterior uveitis was the most common type, followed by posterior uveitis, affecting 34.4% and 25.6% of the study cohort, respectively. About one-third of our patients were beneath the age of 18, and among that group, no specific etiology of uveitis could be determined in about a quarter of the patients by the end of the study period, and juvenile idiopathic arthritis was the most common disease entity.
Conclusion: In conclusion, the present report attempted to illustrate the most common causes of uveitis in Upper Egypt. Tuberculosis followed by sarcoidosis were the two leading causes of uveitis in our group of patients.
Keywords: Egypt, uveitis, tuberculosis, sarcoidosis, idiopathic
Introduction
A large number of inflammatory ocular conditions can be grouped under the term “uveitis”. And the etiologies of ocular inflammation vary to a great extent from one geographic place to another and show a prominent ethnic predisposition. Owing to the blinding potential of a large percentage of ocular inflammatory conditions, it is of critical importance to ophthalmologists to be well-oriented with the pattern of uveitis prevalent in the region of the world they serve in, as well as its common causes. This assists them proceed more successfully in their differential diagnosis plan, and timely instigate the most appropriate treatment. In this domain, a number of reports and studies have been published from different countries, in order to report and expose the predominant causes and forms of ocular inflammation in each country.1–6
The present study aims to report the causes of uveitis among patients referred to a tertiary level hospital in Upper Egypt.
Methods
Retrospective review of the medical records of 982 patients with uveitis who visited a uveitis referral clinic in Upper Egypt between January 2015 and January 2020 was conducted. Patients with posttraumatic or postoperative endophthalmitis were excluded from the study. The study protocol was approved by the review board of the participating institution (Faculty of Medicine Research Ethics Committee, Al-Azhar University, Assiut, Egypt). All participants in the current study had provided a written informed consent at their first visit for collection of data from their medical records in epidemiologic studies. The study was conducted in compliance with the tenets of the Declaration of Helsinki, and the confidentiality of the patients’ data was strictly maintained.
All included patients had undergone detailed history taking and full ocular examination. The best-corrected visual acuity, the findings on slit lamp examination, the intraocular pressure measurement by applanation tonometry, and the results of dilated fundus examination (whenever accessible) were all documented. The authors categorized uveitis into 4 categories: anterior, intermediate, posterior, and panuveitis, in accordance with the SUN Working Group Classification of Uveitis.7 The following tests were performed for all patients: complete blood count, erythrocyte sedimentation rate, high sensitivity C-reactive protein, urine analysis, VDRL, tuberculin test, and plain chest X-ray. Selected investigations were performed for some of the study cohorts, as dictated by the specific relevant data in their history and their examination, as well as by the significant systemic manifestations. Examples were human leukocyte antigen (HLA) typing (HLA B27, HLA B51), QuantiFeron TB Gold test, serum antinuclear antibody, serum angiotensin-converting enzyme, serum lysozyme, serologic tests for herpesviridae, toxoplasmosis, and toxocariasis, MRI brain, and CT chest. The diagnosis of any causative disease was made after fulfillment of the diagnostic criteria required for every disease, and after co-consultation of other physicians according to each particular patient’s needs. These included consultations of internists, pulmonologists, rheumatologists, dermatologists, and pediatricians whenever was necessary. Viral uveitis, toxoplasmosis, and toxocariasis were diagnosed based on the typical clinical presentation in agreement with positive serology. In the present report, uveitis cases for which the specific cause could not be reached by the end of the study duration were referred to as idiopathic.
Results
The study enrolled a total of 982 patients. Their mean age at presentation was 33.8 ± 11.1 years, and the entire age range was 2–73 years. The study cohort was composed of 512 males (52.1%) and 470 females (47.7%). With respect to the laterality, uveitis was bilateral in 508 cases (51.7%). About one-third of the patients had anterior uveitis (338 patients, 34.4%), another quarter of the cohort suffered from posterior uveitis (251 patients, 25.6%), and similar proportions were noted for intermediate uveitis and panuveitis (197 patients (20.1%), and 196 patients (20%), respectively).
Regarding the etiology of uveitis, the most prevalent infectious cause was tuberculosis, which affected 179 cases (18.2% of the entire cohort), Figures 1 and 2. The second most common infectious cause was toxoplasmosis, which affected 59 patients (6%). In 50 patients, the cause of uveitis was ocular toxocariasis, which was thus the third common infectious condition (5.1%). On the other hand, the most prevalent noninfectious cause was sarcoidosis, which affected 99 patients (10.1% of the study cohort). Behçet’s disease was diagnosed in 81 patients (8.2%) and was the second most common noninfectious cause of uveitis in the present report. A less frequently observed entity was HLA B27-associated uveitis, which was diagnosed in 44 patients (4.5%). The contribution of different causes of uveitis is summarized in Table 1. In 303 patients (30.9%), however, no underlying cause whether infectious or noninfectious could be determined by the end of the study and in these patients, the uveitis was termed idiopathic.
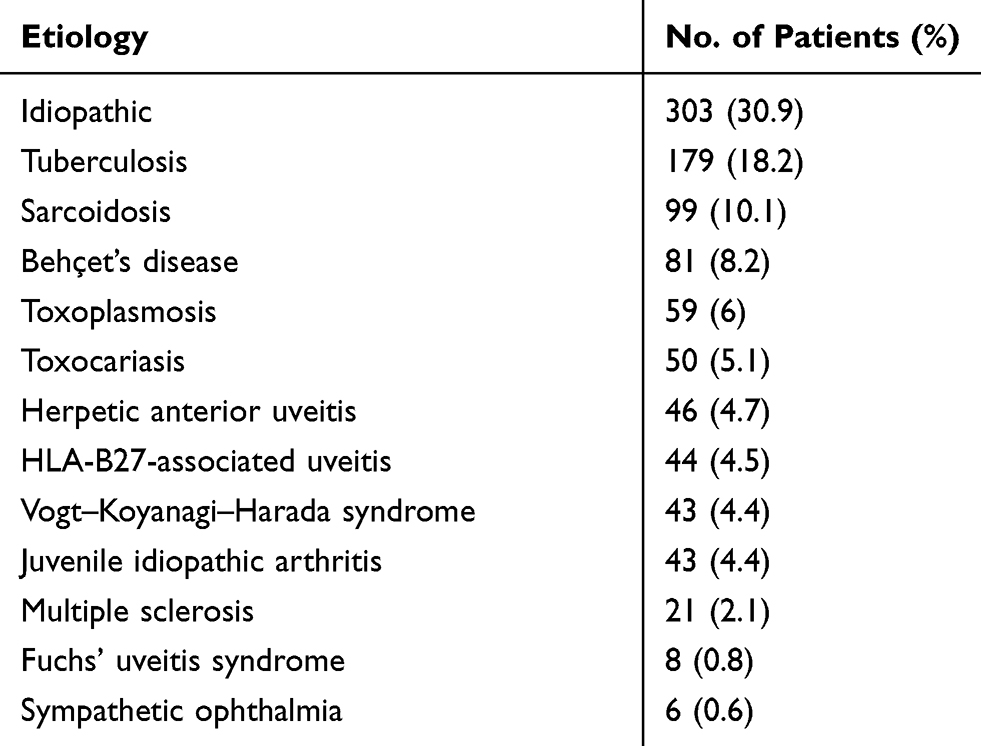 |
Table 1 Contribution of Different Etiologies of Uveitis |
 |
Figure 1 Positive tuberculin reaction in a patient with tuberculous uveitis. |
 |
Figure 2 Intermediate uveitis and peripheral vasculitis in a patient with tuberculosis. |
The authors also looked into the relative prevalence of the different etiologies according to the anatomical location of inflammation.
Out of 338 anterior uveitis cases, 101 cases (29.9%) were idiopathic, and otherwise, viral anterior uveitis was the most common etiology, affecting 46 patients (13.6%). Next to viral anterior uveitis, HLA-B27-associated uveitis and juvenile idiopathic arthritis were the principal causes of anterior uveitis in our cohort, affecting 44 (13%), and 43 (12.7%) patients, respectively.
Out of 197 intermediate uveitis cases, a higher percentage of cases were idiopathic (84 cases, 42.6%), and otherwise, ocular toxocariasis was the most common etiology, affecting 40 patients (20.3%). Tuberculosis and multiple sclerosis were the second and third common causes of intermediate uveitis in our patients, affecting 34 (17.3%) and 21 (10.7%) patients, respectively.
For patients with posterior uveitis, out of 251 cases, 85 cases (33.9%) were idiopathic, and otherwise, the most common etiology was tuberculosis, affecting 71 patients (28.3%). Behçet’s disease followed by toxoplasmosis affected 45 and 42 patients respectively and were responsible for 17.9% and 16.7% of our posterior uveitis cases.
Whereas for patients with panuveitis, out of 196 cases, 33 cases (16.8%) were idiopathic, and otherwise, the most common etiology was Vogt–Koyanagi-Harada syndrome, affecting 43 patients (21.9%), Figures 3–5. Tuberculosis and Behçet’s disease were diagnosed in 42 and 30 patients with panuveitis in our cohort, representing 21.4% and 15.3% of panuveitis cases, respectively.
 |
Figure 3 Vitiligo in a patient with Vogt–Koyanagi–Harada syndrome. |
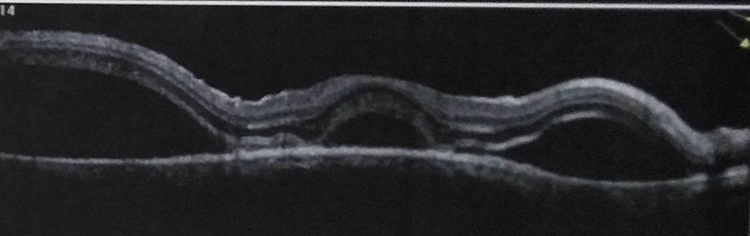 |
Figure 4 Multiple detachments in a patient with Vogt–Koyanagi–Harada syndrome. |
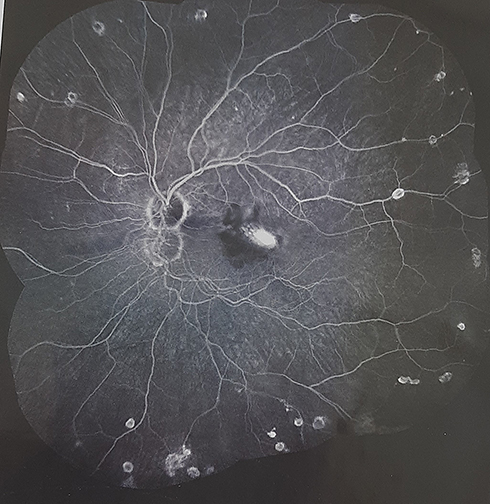 |
Figure 5 Active CNV in a patient with Vogt–Koyanagi–Harada syndrome. |
About one-third of the study cohort were beneath the age of 18 (332 patients, 33.8%), and among that sector, no specific cause was detected in 81 cases (24.4%) of children. Otherwise, the leading causes detected were juvenile idiopathic arthritis (43 cases, 13%), tuberculosis (31 cases, 9.3%), and sarcoidosis (30 cases, 9%).
Discussion
Not only do the causes of uveitis differ from one region of the world to another, in part due to ethnic, racial, geographic, and microorganism prevalence differences, but they also show substantial evolution within the same area over time. This emphasizes the value of epidemiological studies to constantly update the working ophthalmologists with the most recent pattern of uveitis in their area.4,6
In the present report, the mean age of the patients at the time of presentation was 33.8 ± 11.1 years. Our results hereby agree with a huge body of literature that demonstrated that uveitis is most prevalent among the working age including studies from India and Tunisia.8,9 The present study showed uveitis to be slightly more prevalent among males (52.1%). A similar statement of some male preponderance has been published by several studies from developing countries as Bangladesh and India.10,11 On the other hand, reports from some developed countries as Germany and the United States demonstrated either a slight female predominance or equal sex predilection.12,13
In accordance with other studies from Egypt, Tunisia, China, and India, that demonstrated that the most common type of uveitis is anterior uveitis,6,9,14,15 we found that more than one-third of our patients had anterior uveitis (34.4%). In the present study, a specific cause of uveitis could be determined in about 70% of the patients, whereas in about 30% of the patients, no specific cause could be specified by the end of the study period and were thus termed “idiopathic”. Similar rates were published by other authors.9 It is worth noting that there was a variation between the different anatomic types of uveitis regarding the proportion of idiopathic cases. Cases with intermediate uveitis have had the highest percentage of idiopathic cases (42.6%), whereas lower percentages have been found among cases of anterior uveitis, posterior uveitis and panuveitis (29.9%, 33.9%, and 16.8%, respectively). A higher percentage of idiopathic cases among patients with intermediate uveitis than among patients with other types of uveitis has been reported by a number of other studies including studies from Tunisia, Bangladesh, and India.5,6,9–11
In the present study, the most commonly identified etiologies were tuberculosis, sarcoidosis, Behçet’s disease, and toxoplasmosis. Tuberculosis was the most prevalent cause in our patients and was present in about 18% of all cases. Our finding of a high rate of ocular tuberculosis agrees with a previous report from Egypt6 and with what other studies from Bangladesh and Myanmar have published10,16,17. Another important cause of uveitis in the current study is sarcoidosis, which was diagnosed in about one-tenth of the whole study cohort. Similar proportions of uveitis cases caused by sarcoidosis were reported from other countries.18,19 The third most common identifiable cause of uveitis in our study was Behçet’s disease, which affected 8.2% of our patients. Sometimes referred to as the Silk Road disease, the significance of Behçet’s disease in countries located along the Silk Road, has repeatedly been published.20,21 The fourth leading cause of uveitis in our study was ocular toxoplasmosis, which was responsible for about 6% of our cases collectively. It is a ubiquitous parasite with which about one-third of humans worldwide are estimated to be chronically infected, and is an important cause of uveitis.22,23
In conclusion, the present report attempted to illustrate the most common causes of uveitis in Upper Egypt. Tuberculosis followed by sarcoidosis were the two leading causes of uveitis in our group of patients. Idiopathic cases represented about one-third of all cases and were more prevalent among patients with intermediate uveitis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tsirouki T, Dastiridou A, Symeonidis C, et al. A focus on the epidemiology of Uveitis. Ocul Immunol Inflamm. 2016;1–15.
2. Goto H, Mochizuki M, Yamaki K, et al. Epidemiological survey of intraocular inflammation in Japan. Jpn J Ophthalmol. 2007;51:41–44. doi:10.1007/s10384-006-0383-4
3. Rao NA. Uveitis in developing countries. Indian J Ophthalmol. 2013;61(6):253–254. doi:10.4103/0301-4738.114090
4. Cakar Ozdal MP, Yazici A, Tufek M, et al. Epidemiology of uveitis in a referral hospital in Turkey. Turk J Med Sci. 1966;50:337–342. doi:10.3906/sag-1302-132
5. Chang JH-M, Wakefield D. Uveitis: a global perspective. Ocul Immunol Inflamm. 2002;10(4):263–279. doi:10.1076/ocii.10.4.263.15592
6. Abd El Latif E, Ammar H. Uveitis referral pattern in Upper and Lower Egypt. Ocul Immunol Inflamm. 2019;27(6):875–882. doi:10.1080/09273948.2017.1410183
7. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140:509–516.
8. Rathinam SR, Namperumalsamy P. Global variation and pattern changes in epidemiology of uveitis. Indian J Ophthalmol. 2007;55(3):173–183. doi:10.4103/0301-4738.31936
9. Khairallah M, Yahia SB, Ladjimi A, et al. Pattern of uveitis in a referral centre in Tunisia, North Africa. Eye (Lond). 2007;21:33–39.
10. Rahman Z, Ahsan Z, Abdur Rahman N, et al. Pattern of Uveitis in a referral hospital in Bangladesh. Ocul Immunol Inflamm. 2017. doi:10.1080/09273948.2017.1281424
11. Biswas J, Narain S, Das D, et al. Pattern of uveitis in a uveitis clinic in India. Int Ophthalmol. 1996;20(4):223–228. doi:10.1007/BF00175264
12. Grajewski RS, Caramoy A, Frank KF, et al. Spectrum of uveitis in a German tertiary center: review of 474 consecutive patients. Ocul Immunol Inflamm. 2015;1–7.
13. Oruc S, Kaplan AD, Galen M, et al. Uveitis referral pattern in a Midwest University Eye Center. Ocul Immunol Inflamm. 2003;11(4):287–298. doi:10.1076/ocii.11.4.287.18270
14. Yang P, Zhang Z, Zhou H, et al. Clinical patterns and characteristics of uveitis in a tertiary center for uveitis in China. Curr Eye Res. 2005;30(11):943–948. doi:10.1080/02713680500263606
15. Das D, Bhattacharjee H, Bhattacharyya PK, et al. Pattern of uveitis in North East India: a tertiary eye care center study. Indian J Ophthalmol. 2009;57(2):144–146. doi:10.4103/0301-4738.45506
16. Rodriguez A, Calonge M, Pedroza-Seres M, et al. Referral patterns of uveitis in a tertiary eye care center. Arch Ophthalmol. 1996;114:593–599. doi:10.1001/archopht.1996.01100130585016
17. Win MZA, Win T, Myint S, Shwe T, Sandar H. Epidemiology of Uveitis in a tertiary eye center in Myanmar. Ocul Immunol Int. 2016;1–6. doi:10.3109/09273948.2015.1133839
18. McCannel CA, Holland GN, Helm CJ, et al. Causes of uveitis in the general practice of ophthalmology. UCLA Community-Based Uveitis Study Group. Am J Ophthalmol. 1996;121:35–46. doi:10.1016/S0002-9394(14)70532-X
19. Perkins ES. Pattern of uveitis in children. Br J Ophthalmol. 1966;50:169–185. doi:10.1136/bjo.50.4.169
20. Lee LA. Behçet disease. Semin Cutan Med Surg. 2001;20(1):53–57. doi:10.1053/sder.2001.23097
21. Emin O, Serap KA. Behçet disease: new developments in the etiopathogenesis of an Old Silk Road disease. Skinmed. 2018;16(3):176–181.
22. Young-Hoon P, Ho-Woo N. Clinical features and treatment of ocular toxoplasmosis. Korean J Parasitol. 2013;51(4):393–399. doi:10.3347/kjp.2013.51.4.393
23. Holland GN. Ocular toxoplasmosis: a global reassessment. Part 1: epidemiology and course of disease. Am J Ophthalmol. 2003;136(6):973–988. doi:10.1016/j.ajo.2003.09.040
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.