Back to Journals » Patient Preference and Adherence » Volume 12
Estimation of population-based utility weights for gastric cancer-related health states
Authors Lee HJ, Ock M ![]() , Kim KP, Jo MW
, Kim KP, Jo MW ![]()
Received 18 September 2017
Accepted for publication 20 March 2018
Published 23 May 2018 Volume 2018:12 Pages 909—918
DOI https://doi.org/10.2147/PPA.S151946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Hyeon-Jeong Lee,1 Minsu Ock,2 Kyu-Pyo Kim,3 Min-Woo Jo1
1Department of Preventive Medicine, University of Ulsan College of Medicine, Seoul, Korea; 2Department of Preventive Medicine, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea; 3Department of Oncology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Background: This study aimed to generate utility weights of gastric cancer-related health states from the perspective of the Korean general population.
Methods: The Korean adults (age ≥19 years) included in the study were sampled using multistage quota sampling methods stratified by sex, age, and education level. Nine scenarios for hypothetical gastric cancer-related health states were developed and reviewed. After consenting to participate, the subjects were surveyed by trained interviewers using a computer-assisted personal interview method. Participants were asked to perform standard gamble tasks to measure the utility weights of 5 randomly assigned health states (from among nine scenarios). The mean utility weight was calculated for each health state.
Results: Three hundred twenty-six of the 407 adults who completed this study were included in the analysis. The mean utility weights from the standard gamble were 0.857 (no gastric cancer with Helicobacter pylori infection), 0.773 (early gastric cancer [EGC] with endoscopic surgery), 0.779 (EGC with subtotal gastrectomy), 0.767 (EGC with total gastrectomy), 0.602 (advanced gastric cancer with subtotal gastrectomy and adjuvant chemotherapy), 0.643 (advanced gastric cancer with total gastrectomy and adjuvant chemotherapy), 0.522 (advanced gastric cancer with extended gastrectomy and adjuvant chemotherapy), 0.404 (metastatic gastric cancer with palliative chemotherapy), and 0.399 (recurrent gastric cancer with palliative chemotherapy).
Conclusion: This study was the first to comprehensively estimate the utility weights of gastric cancer-related health states in a general population. The utility weights derived from this study could be useful for future economic evaluations related to gastric cancer interventions.
Keywords: stomach neoplasms, health-related quality of life, utility, population, standard gamble
Background
Gastric cancer is a common and often fatal disease. Specifically, an estimated 951,000 cases of gastric cancer were newly diagnosed in 2012, leading to ranking this disease as the fifth most common type of cancer and third most common cause of cancer-related deaths worldwide.1 Regarding the global burden of disease, 17.9 million disability-adjusted life-years (DALYs) worldwide were attributed to gastric cancer in 2013, which was identified as one of the top 3 causes of DALY among men.2 Currently, Korea has the highest gastric cancer incidence in the world, with rates of 63.3 and 25.1 cases per 100,000 in male and female residents, respectively, and age-standardized mortality rates are 19.3 and 7.1 per 100,000 in male and female residents, respectively.3
The treatment of gastric cancer requires the use of modalities such as surgery, chemotherapy, and radiotherapy, which have been associated with high medical costs, several adverse effects, and low health-related quality of life (HRQOL).4,5 HRQOL can be measured using utility weights, which are scored from 1 for perfect health to 0 for death, and reflect an individual’s preference for a specific health state.6 The utility weight of a health state is a key component of quality-adjusted life year (QALY) calculations. In addition, the cost per QALY has been adopted by many countries as a critical and preferred value when conducting cost–utility analyses regarding decision-making for drug reimbursements and new health care interventions.7
Utility weights can be determined directly or indirectly. Direct methods incorporate valuation techniques such as the standard gamble (SG) and time trade-off (TTO), whereas indirect methods implement generic preference-based HRQOL instruments such as EQ-5D, SF-6D, or 15D, which use tariffs for utility-weight conversion. Although indirect methods are simpler and more time-efficient than direct methods, for hypothetical scenarios, the latter methods have the advantage of more abundantly reflecting disease-specific health states when compared with indirect methods that use generic preference-based HRQOL instruments with limited numbers of dimensions.
Utility weights can be determined from the perspectives of patients, health care professionals, or the general population.8 Patients who have experienced a disease will best understand the disease-related health states but may assign relatively high utility weights because they have adapted to these health states.9 Moreover, some researchers have opined that a utility-weight calculation from the perspective of the general population may be more valid in terms of economic views on the allocation of limited resources.10 However, recent systematic reviews addressing studies of the utilities of gastric cancer-associated health states reported the nonexistence of utility-weight data derived from general populations.11,12
Although many studies have measured the utility weights of gastric cancer-related health states, these studies were restricted to health states associated with particular stages of gastric cancer and to the viewpoint of gastric cancer patients.13 The present study aimed to determine the utility weights of gastric cancer-related health states across a wide range of stages and treatment strategies from the perspective of the general population, using SG.
Methods
Study sample
Adults aged ≥19 years were sampled using a multistage stratified quota sampling method. The sample quota was assigned to 15 districts in Korea. At this time, the allocation criteria were the population numbers of the 15 districts and sociodemographic factors of gender, age, and education level according to the population structure to represent the general Korean population.
Gastric cancer-related hypothetical health states
To include the entire progression of gastric cancer, we created 9 descriptions of gastric cancer-related hypothetical health states using a uniform format that included diagnosis, symptoms, treatment, and disease prognosis with 5-year survival rates. These states included 1) no gastric cancer with Helicobacter pylori infection (NG with HP), 2) early gastric cancer (EGC) with endoscopic surgery (EGC with ES), 3) EGC with subtotal gastrectomy (EGC with STG), 4) EGC with total gastrectomy (EGC with TG), 5) advanced gastric cancer (AGC) with subtotal gastrectomy and adjuvant chemotherapy (AGC with STG/Chemo), 6) AGC with total gastrectomy and adjuvant chemotherapy (AGC with TG/Chemo), 7) AGC with extended gastrectomy and adjuvant chemotherapy (AGC with EG/Chemo), 8) metastatic gastric cancer with palliative chemotherapy (MGC with Chemo), and 9) recurrent gastric cancer with palliative chemotherapy (RGC with Chemo). The descriptions of the health scenarios included sufficient information that was provided in simple language and based on the cancer information service of the National Cancer Information Center,14 Korean clinical practice guideline for gastric cancer,15 and patient education materials to allow the respondents to imagine the hypothetical health scenarios.
Survey
The survey was conducted from August to October 2014 by trained interviewers using a computer-assisted personal interviewing method. We trained interviewers about the meaning of 9 health states and how to conduct SG. After training, we took pairs of interviewers and let them practice interviewing each other. Total training time was about 2.5 h. The respondents were asked to perform SG tasks for 5 health states randomly selected from among the 9 devised states. After completing the SG tasks, the respondents were asked questions to solicit background information such as sex, age, education period, household income, and health care utilization (including ambulatory medical visits and hospitalization). After completion of the survey, respondents randomly selected by sex and age were asked by telephone about their sex, age, and participation in this survey. This survey was approved by the Institutional Review Board of Asan Medical Center Seoul, Korea (Approval number S2014-1396-000), and written informed consent was obtained from all participants prior to enrollment.
Utility-weight measurement methods
A SG method, which is regarded as the gold standard for eliciting utility weights, was used to measure the utility weights of the health states.16 Before beginning SG, the respondents were asked if the health states were better or worse than death. Subsequently, for the SG process, the respondents were asked to choose 1 of 2 alternatives. In this study, one alternative was to live in 1 of 9 health states with certainty for 10 years, and the other was to accept a treatment with 2 possible but uncertain outcomes: perfect health with a probability p vs immediate death with a probability 1-p. A moderate probability p (ie, 0.5) was offered for the perfect health state at the beginning of each SG task and the probability value p was changed until the respondents expressed indifference between the 2 alternatives. At that point, the utility weight for the state was defined as the p-value.
Criteria for the exclusion of data from the analysis
Logical criteria were used to exclude respondents from the analysis. Data were excluded if the respondents did not correctly understand the meanings of SG tasks and the resulting data might be interpreted as invalid. In addition, respondents who assigned the same value to all states or valued all states as worse than death were excluded from the analysis.17 Logical inconsistency was also used as an exclusion criterion. In this study, scenarios were developed according to gastric cancer progression and can be categorized as follows: 1) cancer-free state (NG with HP), 2) EGC states (EGC with ES, STG, or TG), 3) AGC states (AGC with STG/Chemo, TG/Chemo, or EG/Chemo), and 4) metastatic or RGC states (MGC with Chemo or RGC with Chemo). Therefore, in a pair of health states from different categories, a better state would be expected to receive the same or a higher score relative to the other and this pair would be considered logically consistent. Based on this criterion, respondents for whom we found more than 3 logically inconsistent pairs of health states were excluded from the analysis.18
Data analysis
The respondents’ characteristics were summarized using descriptive statistics. The utility weights derived using the SG method were calculated as follows: the probability p at the point of indifference was set as the utility weight for each state if the respondent answered that the state was better than death. In the opposite case (ie, the respondent answered that the state was worse than death), the utility weight for the state was censored at zero. The mean utility weights of the 9 health states were subjected to an analysis of variance (ANOVA) to assess differences, and a Dunnett T3 post hoc analysis was used to compare one mean utility weight with the other. The independent two-sample t-test and ANOVA were used to evaluate mean differences according to respondents’ characteristics. A multivariate regression was performed to identify relationships among the respondents’ characteristics as independent variables, using the utility weights as the dependent variable. All statistical analyses were conducted using STATA 13 (StataCorp, College Station, TX, USA).
Results
A total of 407 adults completed this survey. Of these, 81 respondents were excluded: 16 assigned the same utility weight to all states and 65 had more than 3 inconsistencies. A frequency distribution of the logical inconsistencies is shown in Table S1. Subsequently, 326 respondents were included in the study analysis. The respondents had an average age of 45 years (range: 19–80 years), and half of them were female. The majority of respondents had no experience with ambulatory care visits during the past 2 weeks (89.3%) or hospital admission within the past 1 year (96.0%), or no morbidity (86.8%; Table 1).
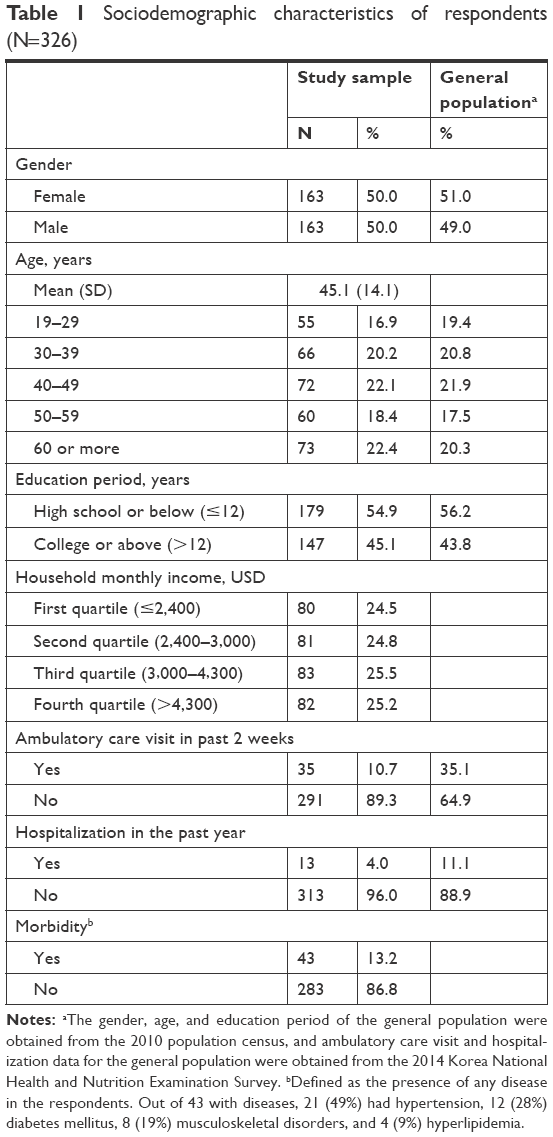 | Table 1 Sociodemographic characteristics of respondents (N=326) |
The mean utility weights of the gastric cancer-related health states are listed in Table 2. The mean utility weights tended to decrease according to gastric cancer progression from NG with HP to RGC with Chemo. The respondents presented similar utility weights for the same stages, regardless of treatment: the utility weights of EGC with ES, EGC with STG, and EGC with TG were 0.773, 0.779, and 0.767, respectively, and those for AGC with STG/Chemo and AGC with TG/Chemo were 0.602 and 0.643, respectively. The respondents also reported similar preferences regarding the scenarios of MGC with Chemo and RGC with Chemo (0.404 and 0.399, respectively).
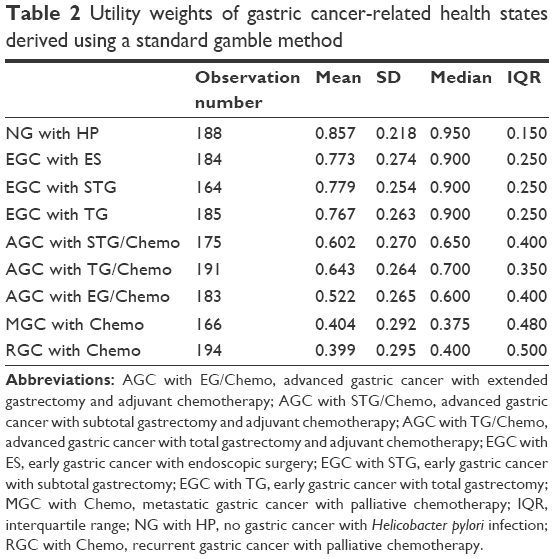 | Table 2 Utility weights of gastric cancer-related health states derived using a standard gamble method |
The utility weights differed statistically across the 9 health states (F=73.171, p<0.001). A Dunnett T3 analysis found no statistical differences between NG with HP and EGC with STG; among EGC with ES, EGC with STG, and EGC with TG; between AGC with STG/Chemo and AGC with TG/Chemo; and between MGC with Chemo and RGC with Chemo (Table S2). Moreover, no statistically significant differences in the mean utility weights were observed according to the respondents’ characteristics such as gender, household monthly income, ambulatory care visit in the past 2 weeks, and morbidity (Table 3).
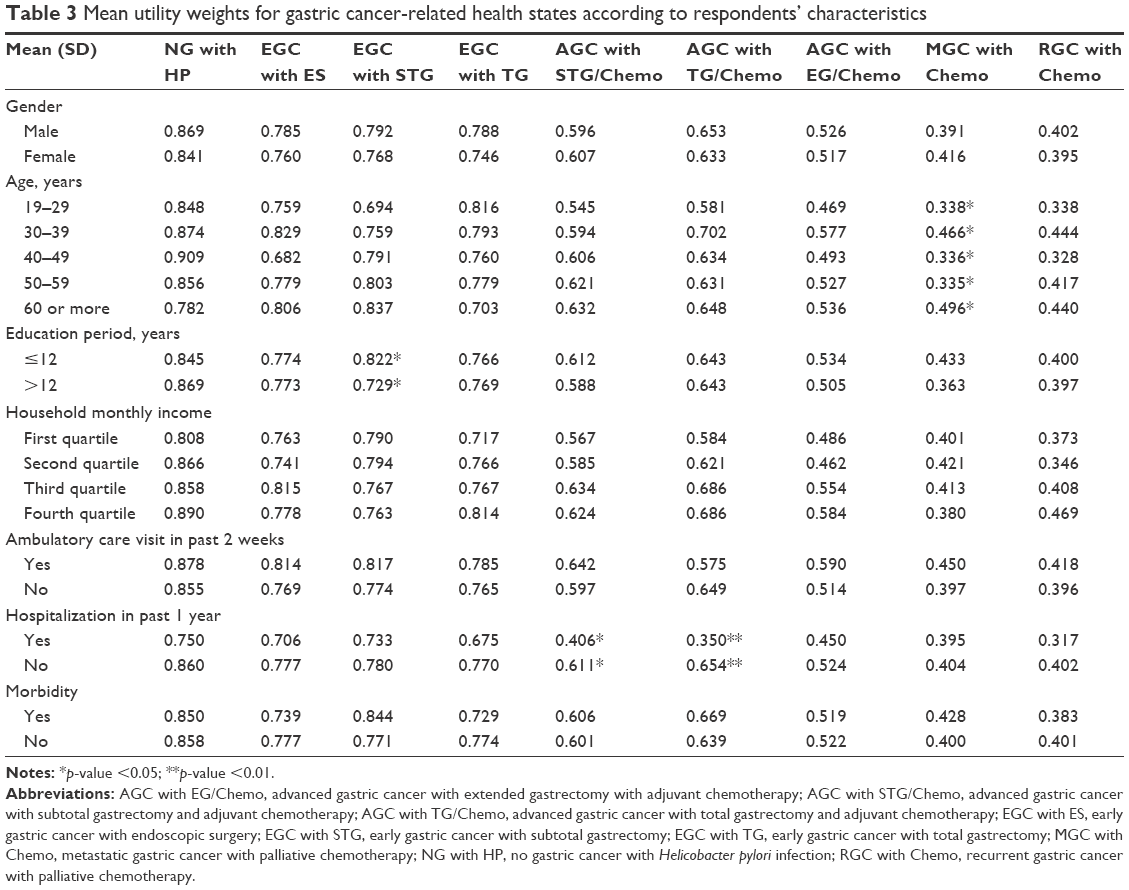 | Table 3 Mean utility weights for gastric cancer-related health states according to respondents’ characteristics |
The multivariate regression identified 4 variables that were significantly related to the utility weights: age, household monthly income, ambulatory care visit in the past 2 weeks, and hospitalization in the past year. Respondents gave higher utility weights if they were aged 30–39 or >60 years, if their household monthly income was above the median, if they had used ambulatory care in the past 2 weeks, or if they had not been hospitalized during the past year (Table 4).
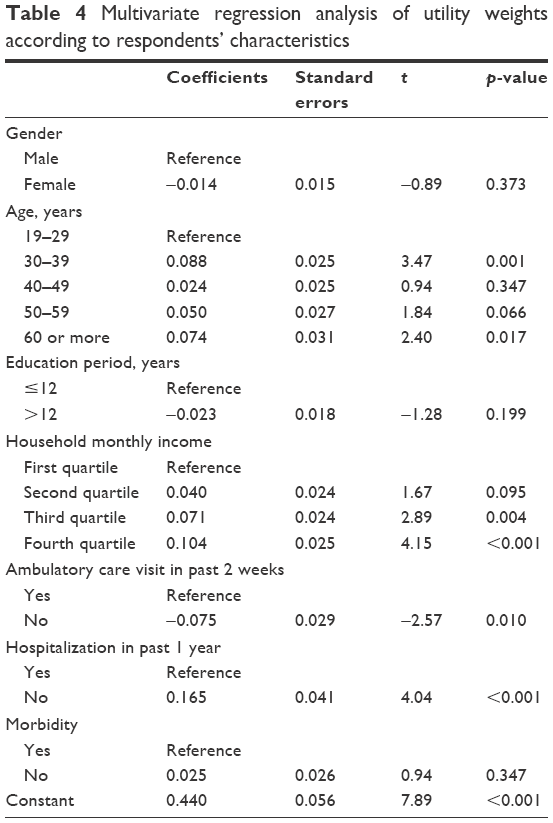 | Table 4 Multivariate regression analysis of utility weights according to respondents’ characteristics |
Discussion
In the current study, respondents from the general population assigned utility weights to gastric cancer-related health states using a SG method. The respondents assigned the highest utility weight to NP with HP and the lowest to RGC with Chemo. The respondents gave lower utility weights to worse stages of gastric cancer.
Interestingly, the utility weights assigned by the general population to scenarios within the same gastric cancer stage did not differ significantly with respect to the treatment method. This suggests that the general population is more affected by the gastric cancer stage than by the treatment method when valuing gastric cancer-related health states. Previous studies of HRQOL of patients who had received STG or TG reported no significant difference between these treatments, and a systematic review of HRQOL after gastrectomy for gastric cancer showed that most studies found no statistically significant difference between STG and TG.12 Bae et al reported that among disease-free gastric cancer survivors, HRQOL did not differ significantly between those who received STG and TG.19
The respondents in this study assigned a mean utility weight of 0.857 to NG with HP. Although this value was the highest among the 9 states, it was relatively low for an absence of gastric cancer. Korea has some of the highest prevalence rates of H. pylori infection and gastric cancer worldwide.20 In addition, a Korean general population-based study reported awareness of H. pylori as a risk factor for gastric cancer.21 This awareness might have affected the valuation for the health state of NG with HP.
Because this study, to the best of our knowledge, was the first to examine the utility weights of gastric cancer-related health states in a general population, we cannot directly compare the results to those of previous studies. However, the utility weights obtained from a general population in the current study were generally lower than those obtained in previous studies of gastric cancer patients. In several studies, patients who underwent surgery for gastric cancer reported utility weights of 0.7713 and 0.8022 with EQ-5D and 0.8523 with TTO. Moreover, a utility weight of 0.83 was reported for patients undergoing chemo/radiotherapy,13 and a study of patients who had attended 2–4 chemotherapy sessions, conducted at ≥20 days after the last session, reported utility weights of 0.55 for EQ-5D, 0.61 for SF-6D, and 0.69 for 15D.24 In the current study, the general population assigned utility weights of 0.767–0.779 for EGC with STG or TG and 0.522–0.643 for AGC with STG/Chemo, TG/Chemo, or EG/Chemo; these were relatively lower than those assigned by patients. Regarding MGC or RGC, patients with advanced adenocarcinoma of the stomach or esophagogastric junction in the recurrent or metastatic state assigned weights of 0.66–0.76 when using EQ-5D.25 These were much higher than the utility weights of 0.399–0.404 assigned to MGC or RGC with Chemo by participants in the current study. However, another earlier TTO-based study reported that patients with MGC assigned a utility weight of 0.35, which was lower than the value assigned in the present study.23
The lower utility weights in this study relative to those in previous studies can be attributed to several factors. First, all previous studies of the utility weights of gastric cancer states were conducted from the patient’s perspective. Patients might have not responded to and consequently been excluded from studies because of a poor health state, and patients who had adjusted well to gastric cancer were likely to be selected for study participation.12 Therefore, when using utility weights of a health state, one must consider whether the values were derived from patients or from the community. Second, the general population might have assigned low utility weights because the health state scenarios used in this study included information about postoperative symptoms or possible complications. Third, the choice of valuation method might have had an effect. Most previous studies of gastric cancer-related utility weights were conducted using an indirect EQ-5D-based method. The EQ-5D, which consists of 5 dimensions, was reported to show a high ceiling effect, and to be insensitive to patients’ health changes.26 Generic tools used to measure utility weights (including EQ-5D) might be less sensitive to changes in a patient’s health state than disease-specific instruments.27 Accordingly, the utility weights obtained using generic tools might be higher than those assigned in the present study.
The multivariate regression in this study identified age, household income, and experiences with ambulatory care visits or hospitalization as factors that significantly influenced a respondent’s valuation of health states. Other reports have indicated that sociodemographic characteristics such as age, income, and education may affect a respondent’s utility weights.28,29 The finding that several sociodemographic variables affected the valuation results in the present study suggests the importance of representative sampling when valuing various health states.
The current study had some limitations. First, although the respondents were generally similar to the general population of the 2010 population census in terms of sex, age, and education period, the current study respondents included fewer participants aged 19–39 years and more respondents aged >40 years when compared with the general population. In addition, the proportions of participants aged >70 years differed with rates of 2.1% in the current study and 9.6% in the general population. Accordingly, the perspective of people aged >70 years might have been disproportionately less reflected in the utility weights from this study. Furthermore, respondents in the current study were much less likely to have used ambulatory care in the past 2 weeks or to have been hospitalized in the past year, compared with participants in the nationwide 2014 Korea National Health and Nutrition Examination Survey; in other words, the study sample was likely healthier than the general population. To evaluate selection bias, we compared the utilities for each health state between participants who have used ambulatory care or been hospitalized in the past and those who have not, and most of the differences were not statistically significant. Second, interviews with gastric cancer patients were not included in scenario development. Each health state description was formatted uniformly, according to clinical guidelines and health education materials, to ensure that respondents were provided structured and sufficient information about gastric cancer-related health states. The scenarios were developed to investigate how respondents would evaluate gastric cancer-related health states when given sufficient information about the diagnosis, symptoms, treatment, and prognosis. Information provided by patients who have experienced gastric cancer and/or postoperative states would help to enrich and verify the scenarios. Third, this study has limitations to its generalization. Although this study attempted to include various gastric cancer-related health states and was conducted in a representative Korean population, the results should be applied cautiously. The hypothetical health states were subdivided according to stage, but even in the same stage, there may be variations in the corresponding health state. In addition, this study was aimed at the general population in Korea, so there are limitations to generalizability because there are reports that utilities vary according to culture or health care delivery systems.30,31 This means that utilities derived from other countries must be used cautiously.
Despite these limitations, the results of this study can be useful for economic evaluation of screening and treatment in gastric cancer. The many studies that performed economic evaluations of screening tests, surgery, or chemotherapy for gastric cancer have used utilities for gastric cancer-related health states.32–34 Given that gastric cancer has a relatively high prevalence and incidence in Asians, these results might be considered if there is a paucity of research on utilities of gastric cancer-related health states in Asia.35
Conclusion
Our study provided utility weights for a wide range of gastric cancer-related states from the perspective of a general population using direct valuation method with SG. In the future, the utility weights derived from this study will be useful for gastric cancer-related economic evaluations.
Acknowledgment
This work was supported by a grant from the National R&D Program for Cancer Control, Ministry of Health and Welfare, Republic of Korea (study number: 1520140).
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E386. | ||
Global Burden of Disease Cancer Collaboration; Fitzmaurice C, Dicker D, Pain A, et al. The global burden of cancer 2013. JAMA Oncol. 2015;1(4):505–527. | ||
Jung KW, Won YJ, Kong HJ, Oh CM, Lee DH, Lee JS. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2011. Cancer Res Treat. 2014;46(2):109–123. | ||
Li X, Cai H, Wang C, Guo C, He Z, Ke Y. Economic burden of gastrointestinal cancer under the protection of the new rural cooperative medical scheme in a region of rural China with high incidence of oesophageal cancer: cross-sectional survey. Trop Med Int Health. 2016;21(7):907–916. | ||
Fuchs H, Holscher AH, Leers J, et al. Long-term quality of life after surgery for adenocarcinoma of the esophagogastric junction: extended gastrectomy or transthoracic esophagectomy? Gastric Cancer. 2016;19(1):312–317. | ||
Torrance GW. Utility approach to measuring health-related quality of life. J Chronic Dis. 1987;40(6):593–603. | ||
Torrance GW. Measurement of health state utilities for economic appraisal. J Health Econ. 1986;5(1):1–30. | ||
De Wit GA, Busschbach JJ, De Charro FT. Sensitivity and perspective in the valuation of health status: whose values count? Health Econ. 2000;9(2):109–126. | ||
Chapman BP, Franks P, Duberstein PR, Jerant A. Differences between individual and societal health state valuations: any link with personality? Med Care. 2009;47(8):902–907. | ||
Russell LB, Gold MR, Siegel JE, Daniels N, Weinstein MC. The role of cost-effectiveness analysis in health and medicine. Panel on Cost-Effectiveness in Health and Medicine. JAMA. 1996;276(14):1172–1177. | ||
Carter GC, King DT, Hess LM, et al. Health state utility values associated with advanced gastric, oesophageal, or gastro-oesophageal junction adenocarcinoma: a systematic review. J Med Econ. 2015;18(11):954–966. | ||
Shan B, Shan L, Morris D, Golani S, Saxena A. Systematic review on quality of life outcomes after gastrectomy for gastric carcinoma. J Gastrointest Oncol. 2015;6(5):544–560. | ||
Areia M, Alves S, Brito D, et al. Health-related quality of life and utilities in gastric premalignant conditions and malignant lesions: a multicentre study in a high prevalence country. J Gastrointestin Liver Dis. 2014;23(4):371–378. | ||
Cancer.go.kr [homepage on the Internet]. Goyang: National Cancer Information Center [updated March 15, 2018; cited May 2, 2014]. Available from: https://www.cancer.go.kr/lay1/program/S1T211C213/cancer/view.do?cancer_seq=4661. Accessed March 2, 2018. | ||
Korean Academy of Medical Sciences. Korean Clinical Practice Guideline for Gastric Cancer. Seoul: DongA-Sa; 2012. | ||
van Osch SM, Stiggelbout AM. The construction of standard gamble utilities. Health Econ. 2008;17(1):31–40. | ||
Ferreira LN, Ferreira PL, Pereira LN, Oppe M. The valuation of the EQ-5D in Portugal. Qual Life Res. 2014;23(2):413–423. | ||
Lee JY, Ock M, Jo MW, et al. Estimating utility weights and quality-adjusted life year loss for colorectal cancer-related health states in Korea. Sci Rep. 2017;7(1):5571. | ||
Bae JM, Kim S, Kim YW, et al. Health-related quality of life among disease-free stomach cancer survivors in Korea. Qual Life Res. 2006;15(10):1587–1596. | ||
Malaty HM, Kim JG, Kim SD, Graham DY. Prevalence of Helicobacter pylori infection in Korean children: inverse relation to socioeconomic status despite a uniformly high prevalence in adults. Am J Epidemiol. 1996;143(3):257–262. | ||
Oh DY, Choi KS, Shin HR, Bang YJ. Public awareness of gastric cancer risk factors and disease screening in a high risk region: a population-based study. Cancer Res Treat. 2009;41(2):59–66. | ||
Zhou HJ, So JB, Yong WP, et al. Validation of the functional assessment of cancer therapy-gastric module for the Chinese population. Health Qual Life Outcomes. 2012;10:145. | ||
Hisashige A, Sasako M, Nakajima T. Cost-effectiveness of adjuvant chemotherapy for curatively resected gastric cancer with S-1. BMC Cancer. 2013;13:443. | ||
Kontodimopoulos N, Aletras VH, Paliouras D, Niakas D. Mapping the cancer-specific EORTC QLQ-C30 to the preference-based EQ-5D, SF-6D, and 15D instruments. Value Health. 2009;12(8):1151–1157. | ||
Curran D, Pozzo C, Zaluski J, et al. Quality of life of palliative chemotherapy naive patients with advanced adenocarcinoma of the stomach or esophagogastric junction treated with irinotecan combined with 5-fluorouracil and folinic acid: results of a randomised phase III trial. Qual Life Res. 2009;18(7):853–861. | ||
Wang P, Luo N, Tai ES, Thumboo J. The EQ-5D-5L is more discriminative than the EQ-5D-3L in patients with diabetes in Singapore. Value Health Reg Issues. 2016;9:57–62. | ||
Marra CA, Woolcott JC, Kopec JA, et al. A comparison of generic, indirect utility measures (the HUI2, HUI3, SF-6D, and the EQ-5D) and disease-specific instruments (the RAQoL and the HAQ) in rheumatoid arthritis. Soc Sci Med. 2005;60(7):1571–1582. | ||
Prosser LA, Payne K, Rusinak D, Shi P, Uyeki T, Messonnier M. Valuing health across the lifespan: health state preferences for seasonal influenza illnesses in patients of different ages. Value Health. 2011;14(1):135–143. | ||
Lee GM, Salomon JA, LeBaron CW, Lieu TA. Health-state valuations for pertussis: methods for valuing short-term health states. Health Qual Life Outcomes. 2005;3:17. | ||
Coons SJ, Rao S, Keininger DL, Hays RD. A comparative review of generic quality-of-life instruments. Pharmacoeconomics. 2000;17:13–35. | ||
Johnson JA, Luo N, Shaw JW, Kind P, Coons SJ. Valuations of EQ-5D health states: are the United States and United Kingdom different? Med Care. 2005;43(3):221–228. | ||
Chang HS, Park EC, Chung W, et al. Comparing endoscopy and upper gastrointestinal X-ray for gastric cancer screening in South Korea: a cost-utility analysis. Asian Pac J Cancer Prev. 2012;13(6):2721–2728. | ||
Wu B, Li T, Cai J, Xu Y, Zhao G. Cost-effectiveness analysis of adjuvant chemotherapies in patients presenting with gastric cancer after D2 gastrectomy. BMC Cancer. 2014;14:984. | ||
Lam SW, Wai M, Lau JE, McNamara M, Earl M, Udeh B. Cost-effectiveness analysis of second-line chemotherapy agents for advanced gastric cancer. Pharmacotherapy. 2017;37(1):94–103. | ||
Rahman R, Asombang AW, Ibdah JA. Characteristics of gastric cancer in Asia. World J Gastroenterol. 2014;20(16):4483–4490. |
Supplementary materials
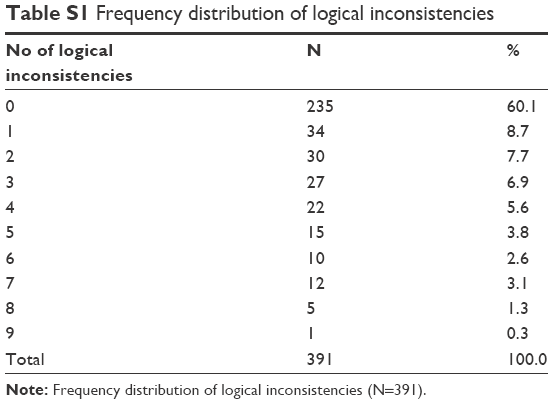 | Table S1 Frequency distribution of logical inconsistencies |
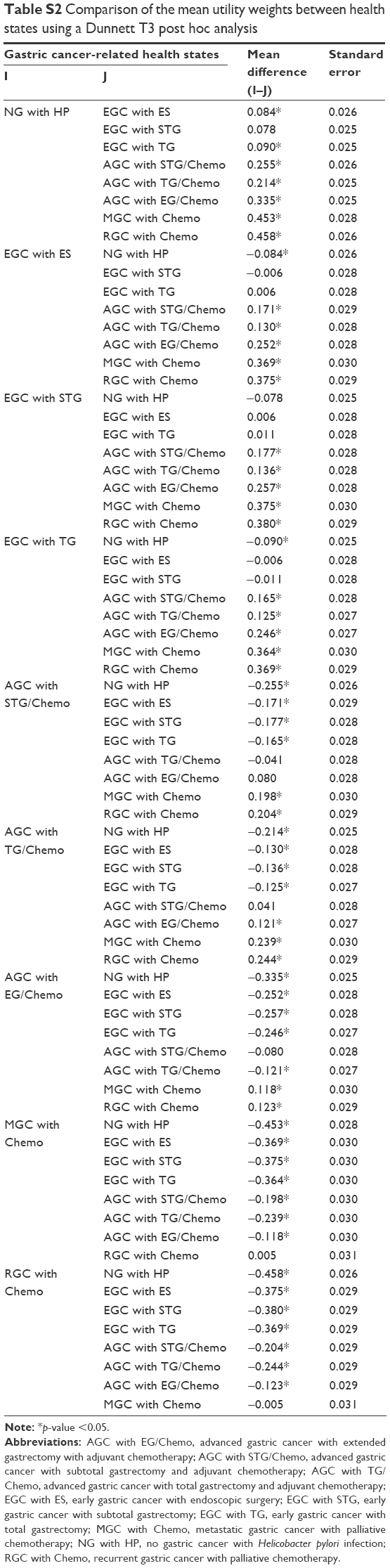 | Table S2 Comparison of the mean utility weights between health states using a Dunnett T3 post hoc analysis |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.