Back to Journals » Drug Design, Development and Therapy » Volume 20
Esketamine-Based Opioid-Free versus Opioid-Based Anesthesia for Recovery Quality After Laparoscopic Transabdominal Preperitoneal Repair: A Randomized Noninferiority Trial
Authors Liu H ![]() , Xing X, Jiang F, Zhang L, Chen L
, Xing X, Jiang F, Zhang L, Chen L ![]()
Received 28 October 2025
Accepted for publication 15 January 2026
Published 27 January 2026 Volume 2026:20 572431
DOI https://doi.org/10.2147/DDDT.S572431
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Huan Liu, Xinyi Xing, Fan Jiang, Lei Zhang, Lijian Chen
Department of Anesthesiology, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, 230022, People’s Republic of China
Correspondence: Lijian Chen, Department of Anesthesiology, The First Affiliated Hospital of Anhui Medical University, 218 Jixi Road, Hefei, Anhui, 230022, People’s Republic of China, Email [email protected]
Purpose: This study aimed to compare the quality of postoperative recovery between esketamine-based opioid-free anesthesia (OFA) and opioid-based anesthesia (OBA) in patients undergoing laparoscopic transabdominal preperitoneal (TAPP) repair.
Patients and Methods: In this prospective, randomized, double-blind, noninferiority trial, 126 adults scheduled for elective laparoscopic TAPP repair were randomized to OFA (n = 63) or OBA (n = 63) group. The OFA group received esketamine (0.5 mg·kg− 1 induction, 0.4– 0.5 mg·kg− 1·h− 1 maintenance), while the OBA group received sufentanil (0.4 μg·kg− 1 induction) and remifentanil (0.1– 0.2 μg·kg− 1·min− 1 maintenance). The primary outcome was the 15-item Quality of Recovery (QoR-15) score at 24 hours postoperatively, with a noninferiority margin of − 8. Secondary outcomes included pain scores, rescue analgesia, sleep quality, safety outcomes.
Results: The OFA group showed a higher QoR-15 score at 24 hours postoperatively than the OBA group (median difference: 2; median [IQR]: 129 [125 to 132] vs 127 [123 to 130]; 95% CI, 0 to 4; P=0.014). Pruritus incidence was lower (P=0.027), vasopressor use was reduced (P = 0.012), and hypotensive episodes tended to be fewer (P=0.106) in the OFA group. Pain scores on coughing at 24 and 48 hours postoperatively were also lower in the OFA group (P=0.002 and P< 0.001, respectively).
Conclusion: Esketamine-based OFA provided a noninferior quality of postoperative recovery compared with OBA in patients undergoing laparoscopic TAPP repair, offering a safer alternative to OFA regimens that minimizes opioid-related complications while maintaining perioperative comfort and supporting enhanced recovery.
Keywords: esketamine, transabdominal preperitoneal, noninferiority trial, opioid-free anesthesia, postoperative recovery
Introduction
Opioids are widely regarded as the most effective analgesics for perioperative management. However, opioid-based anesthesia (OBA) is associated with several adverse events, including postoperative nausea and vomiting (PONV), impaired respiratory function, delayed gastrointestinal recovery, opioid-induced hyperalgesia, and an increased risk of dependence.1–4 These adverse effects are among the factors contributing to the global opioid crisis. In response, enhanced recovery after surgery (ERAS) protocols aim to minimize opioid exposure, thereby promoting faster functional recovery and reducing complications, particularly in minimally invasive procedures. Consequently, opioid-free anesthesia (OFA) has emerged as a multimodal strategy that employs nonopioid agents to provide effective analgesia while minimizing opioid-related risks.5
Among nonopioid agents, esketamine is an effective adjunct in OFA regimens, providing analgesic effects through NMDA receptor antagonism and activation of the sympathetic nervous system.3,6,7 Compared with racemic ketamine, esketamine exhibits higher NMDA receptor affinity and a lower incidence of psychomimetic side effects, which facilitates its use in continuous perioperative infusion.8 In addition to its analgesic effects, preclinical and clinical studies indicate that esketamine exerts anti-inflammatory effects by suppressing IL-6 and TNF-α, potentially enhancing postoperative recovery and patient comfort.9,10
Recent randomized trials have demonstrated that OFA significantly reduces PONV, facilitates early ambulation, and shortens hospital stay across abdominal, spinal, and cardiac surgeries.11–14 Laparoscopic transabdominal preperitoneal (TAPP) repair is a minimally invasive and widely performed technique for inguinal hernia repair, with over 20 million procedures performed annually worldwide.15 While TAPP is compatible with ERAS principles promoting minimally invasive recovery, optimal pain management remains a critical challenge. Despite its minimally invasive nature, moderate-to-severe pain occurs in approximately 50% of patients on the first postoperative day after laparoscopic hernia repair. These patients are often treated with opioids, which may delay ambulation and increase complications.16 Although OFA has demonstrated success in a variety of procedures, including laparoscopic cholecystectomy, thoracic surgery, bariatric surgery, and colorectal surgery, its application in TAPP repair has not been fully investigated, particularly with esketamine-based regimens.11,17–19
This study aimed to test whether esketamine-based OFA provides postoperative recovery quality noninferior to that of OBA in patients undergoing elective TAPP repair. By focusing on esketamine-based OFA in TAPP repair, it is expected to provide clinically relevant evidence that can inform future ERAS protocols, support safer perioperative care, and contribute to global opioid stewardship.
Materials and Methods
Study Design
This study was approved by the Clinical Medical Research Ethics Committee of the First Affiliated Hospital of Anhui Medical University (approval no. PJ 2023–06-17, approval date: 11 May 2023, chairperson: Heng Wang) and was registered with the Chinese Clinical Trial Registry (www.chictr.org.cn, registration no. ChiCTR2300072534, principal investigator: H.L., registration date: 16 Jun 2023). All participants were fully informed about the trial’s purpose and procedures, and written informed consent was obtained before enrollment. The trial was conducted in accordance with the ethical principles of the Declaration of Helsinki and its subsequent amendments, and followed the CONSORT reporting guidelines.
Participants
Patients were recruited for participation between July 6, 2023, and August 7, 2024. The study cohort consisted of patients scheduled for elective laparoscopic TAPP repair. Anesthesia was administered via a laryngeal mask airway according to standardized protocols. Inclusion criteria were: (1) age ≥18 years and (2) American Society of Anesthesiologists (ASA) physical status I–III. Patients with incarcerated or recurrent hernia; severe hypertension (systolic ≥180 mmHg or diastolic ≥110 mmHg despite medical therapy); cognitive impairment or communication difficulties; chronic pain requiring regular analgesics; a history of allergic reactions to study drugs; contraindications to laryngeal mask use; severe cardiovascular disease; liver failure; or obesity (body mass index [BMI] >30 kg·m−2) were excluded.
Randomization and Blinding
Patients were randomly assigned using the Sealed Envelope platform (www.sealedenvelope.com) with a 1:1 allocation ratio and block sizes of 2 and 4. An independent research staff member prepared opaque, sequentially numbered envelopes with the group assignments concealed inside. Immediately before anesthesia induction, a research assistant not involved in the study opened the envelopes, and patients were assigned to either the OFA or OBA group. Only the attending anesthesiologist, who was uninvolved in the trial, was aware of the group assignments. Patients, postoperative outcome assessors, and statistical analysts were blinded to group assignments.
Anesthesia and Study Interventions
All patients adhered to standard preoperative fasting guidelines. Upon arrival in the operating room, standard monitoring was applied, including electrocardiography, pulse oximetry (SpO2), and noninvasive blood pressure measurement. In all patients, anesthesia was induced after preoxygenation with etomidate (0.2 mg·kg−1) and cisatracurium (0.2 mg·kg−1), supplemented by sufentanil (0.4 μg·kg−1) in the OBA group or esketamine (0.5 mg·kg−1) in the OFA group. Propofol (4–6 mg·kg−1·h−1) was used for maintenance in both groups, supplemented by remifentanil (0.1–0.2 μg·kg−1·min−1) in the OBA group and esketamine infusion (0.4–0.5 mg·kg−1·h−1) in the OFA group.20,21 All patients were ventilated via a laryngeal mask airway, with end-tidal CO2 maintained at 35–40 mmHg. Active warming measures were applied to maintain normothermia. Intraoperative hemodynamics were managed according to a standardized protocol applied in both groups. Mean arterial pressure was maintained within 20% of the baseline value. Hypotension, defined as a decrease in mean arterial pressure >20% from baseline, was treated with intravenous norepinephrine (4–8 μg) or ephedrine (6 mg) administered as bolus doses and repeated as needed. Bradycardia, defined as a >20% decrease in heart rate from baseline or a heart rate <50 bpm, was treated with intravenous atropine (0.3 mg). Before the end of surgery, the OBA group received sufentanil (0.2 μg·kg−1) for postoperative analgesia, whereas the OFA group received esketamine (0.25 mg·kg−1).
Post-anesthesia care was conducted according to a standardized protocol for all patients. After recovery of spontaneous breathing and emergence from anesthesia, the laryngeal mask airway was removed. Residual neuromuscular blockade was antagonized with neostigmine (0.05 mg·kg −1) as needed. Postoperative pain was assessed using the numeric rating scale (NRS), and patients with an NRS score ≥4 received intravenous sufentanil (5 μg), repeated as necessary until pain was reduced below an NRS score of 4.11 Patients were transferred to the surgical ward upon reaching a Steward score of 6. Postoperative analgesia in the surgical ward consisted of intravenous flurbiprofen ester (50 mg) administered according to the same standardized protocol.
Study Outcomes
The primary outcome was the 15-item Quality of Recovery (QoR-15) score assessed at 24 hours after surgery (H24) during the hospital stay. The QoR-15 generates a total score ranging from 0 to 150, with higher scores indicating better postoperative recovery.
Secondary outcomes included the QoR-15 score at 72 hours postoperatively (H72). For patients who had been discharged before H72, the QoR-15 was administered via telephone interview.22 Secondary outcomes also comprised numeric rating scale (NRS) pain scores at rest and on coughing at 6, 12, 24, and 48 hours after surgery (H6, H12, H24, and H48). For each patient, the area under the curve (AUC) of NRS scores from H6 to H48 was calculated using the trapezoidal method, separately for pain at rest (AUC_rest) and pain on coughing (AUC_cough). Additional secondary outcomes included the requirement for rescue analgesia within 48 hours postoperatively, duration of post-anesthesia care unit (PACU) stay, and sleep quality on the night of surgery, which was evaluated using a five-point Likert scale (0 = very poor sleep quality; 5 = excellent sleep quality).23
Safety outcomes were recorded intraoperatively and postoperatively. Hemodynamic adverse events included hypotension (mean arterial pressure [MAP] decrease >20% from baseline), hypertension (MAP increase >20% from baseline), bradycardia (heart rate <50 beats·min−1), and tachycardia (heart rate >100 beats·min−1), along with the corresponding pharmacologic interventions (norepinephrine, ephedrine, atropine, nicardipine, or esmolol). Other recorded safety events included PONV, pruritus, dizziness, headache, and hallucinations or nightmares.
Statistical Analysis
Previous studies have established the minimum clinically important difference (MCID) for the QoR-15 as 8 points.24 On this basis, the noninferiority margin was set at −8 points for the between-group difference in QoR-15 scores, reflecting the largest clinically acceptable decrease in postoperative recovery quality. Noninferiority of esketamine-based OFA compared with OBA was concluded if the lower bound of the two-sided 95% confidence interval (CI) for the between-group difference in QoR-15 scores exceeded −8 points. Based on previous studies, assuming a common standard deviation of 15 points, a total sample size of 114 patients (57 per group) was calculated to provide 80% power to demonstrate noninferiority using a one-sided α level of 0.025.25,26 Allowing for an anticipated 10% dropout rate, the final target sample size was increased to 126 patients (63 per group).
Normality of continuous variables was assessed using the Shapiro–Wilk test before parametric analyses. Continuous variables are presented as mean ± standard deviation or median (interquartile range), as appropriate, whereas categorical variables are expressed as counts (percentages). Comparisons were performed according to data distribution: the Student’s t test for normally distributed continuous variables, the Mann–Whitney U-test for non-normally distributed continuous variables, and the chi-square or Fisher’s exact test for categorical variables. The Hodges-Lehmann estimator of the between-group median difference with its 95% CI was reported for non-parametric continuous outcomes. Statistical significance was defined as a two-sided p-value < 0.05. All statistical analyses were performed using SPSS software (version 27; IBM Corp., Armonk, NY, USA).
Results
The CONSORT flow diagram of participant enrollment and allocation is presented in Figure 1. A total of 156 patients were assessed for eligibility between July 2023 and August 2024. After exclusion of 30 patients, 126 participants were randomly assigned in a 1:1 ratio to the OBA or OFA group. All 126 randomized participants (63 in each group) were included in the final analysis.
 |
Figure 1 CONSORT study flow diagram. |
Baseline Demographic Characteristics and Intraoperative Data
Baseline demographic and intraoperative characteristics were comparable between the two groups (Table 1). No clinically meaningful differences were observed with respect to age, sex distribution, ASA physical status, comorbidities, baseline QoR-15 scores, surgical duration, or the proportion of bilateral procedures. The total intraoperative dose of propofol was significantly higher in the OFA group than in the OBA group (P=0.003).
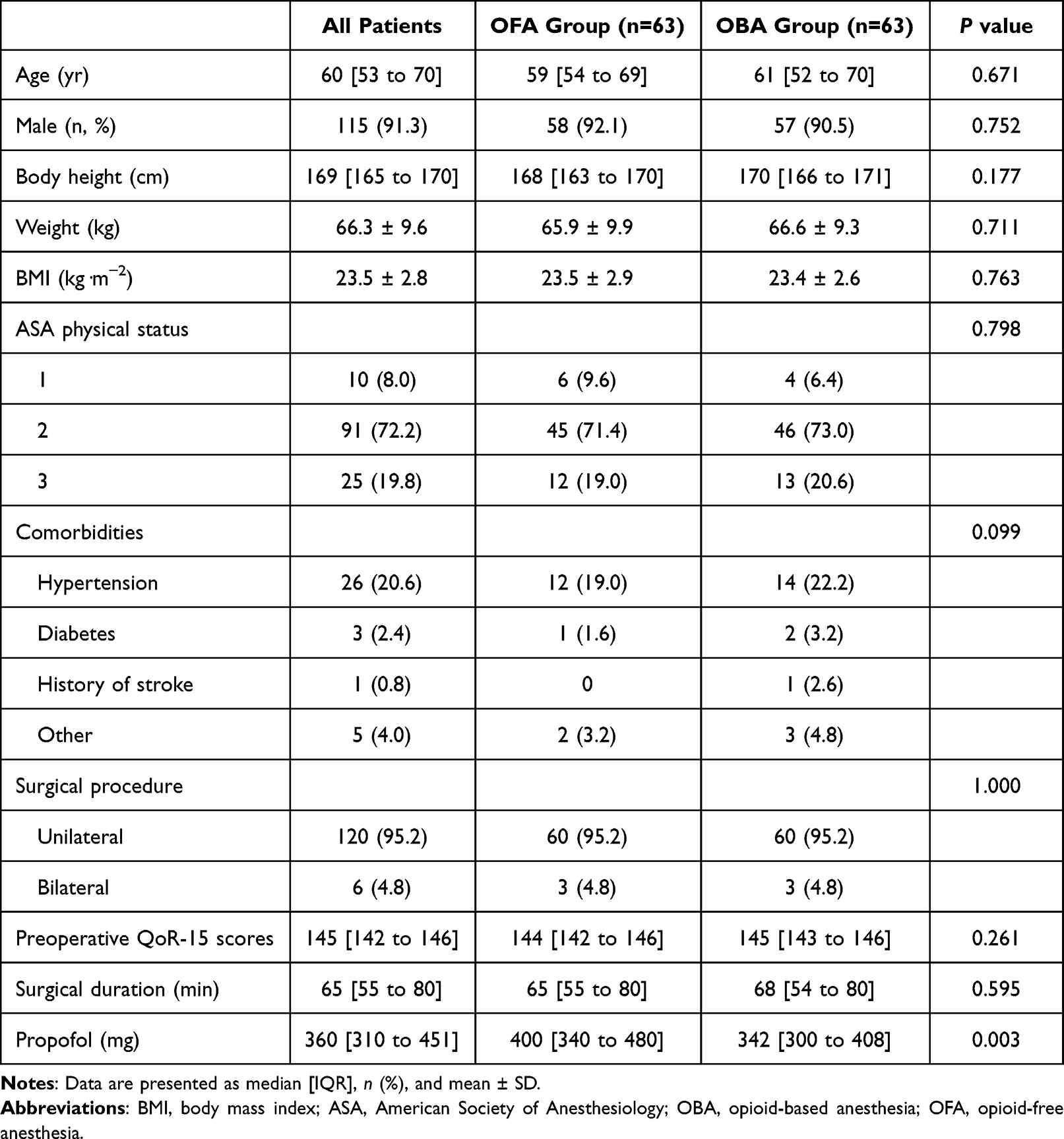 |
Table 1 Demographic Characteristics and Intraoperative Data |
Primary and Secondary Outcomes
Primary and secondary outcomes are summarized in Table 2. The QoR-15 score at H24 was significantly higher in the OFA group than in the OBA group (129 [125 to 132] vs 127 [123 to 130]; 95% CI, 0 to 4; P=0.014), and this difference persisted at H72 (142 [140 to 144] vs 140 [138 to 142]; 95% CI, 1 to 3; P<0.001). The lower bound of the 95% CI exceeded the prespecified noninferiority margin of −8, thereby demonstrating noninferiority of OFA compared with OBA.
 |
Table 2 Primary and Secondary Outcomes |
Postoperative pain scores were comparable between groups at early postoperative time points. Lower pain scores were observed in the OFA group at 24 and 48 hours postoperatively. Consistently, the AUC of NRS pain scores from 6 to 48 hours was lower in the OFA group than in the OBA group, both at rest (12 [9 to 21] vs 21 [12 to 51]; 95% CI, 3 to 15; P=0.002) and on coughing (45 [21 to 78] vs 72 [45 to 114]; 95% CI, 12 to 39; P<0.001). The proportion of patients requiring rescue analgesia did not differ significantly between groups. The duration of PACU stay was longer in the OFA group than in the OBA group (45 [35 to 50] vs 32 [30 to 45]; 95% CI, 5 to 15; P<0.001). Sleep quality on the night of surgery was slightly higher in the OFA group than in the OBA group (5 [4 to 5] vs 4 [4 to 5]; 95% CI, 0 to 1; P=0.018).
Safety Outcomes
Safety outcomes are summarized in Table 3. Compared with the OBA group, the OFA group required significantly fewer interventions for hemodynamic events (11.1% vs 35.0%, 95% CI, −8.1% to −1.3%; P=0.012) and had a lower incidence of pruritus (3.2% vs 14.3%; 95% CI, −24.6% to −1.1%; P=0.027) compared with the OBA group. Lower incidences of hypotension and bradycardia were observed in the OFA group, although the between-group differences did not reach statistical significance. The incidences of hypertension, tachycardia, headache or dizziness, PONV, and postoperative nightmares or hallucinations were low and comparable between groups.
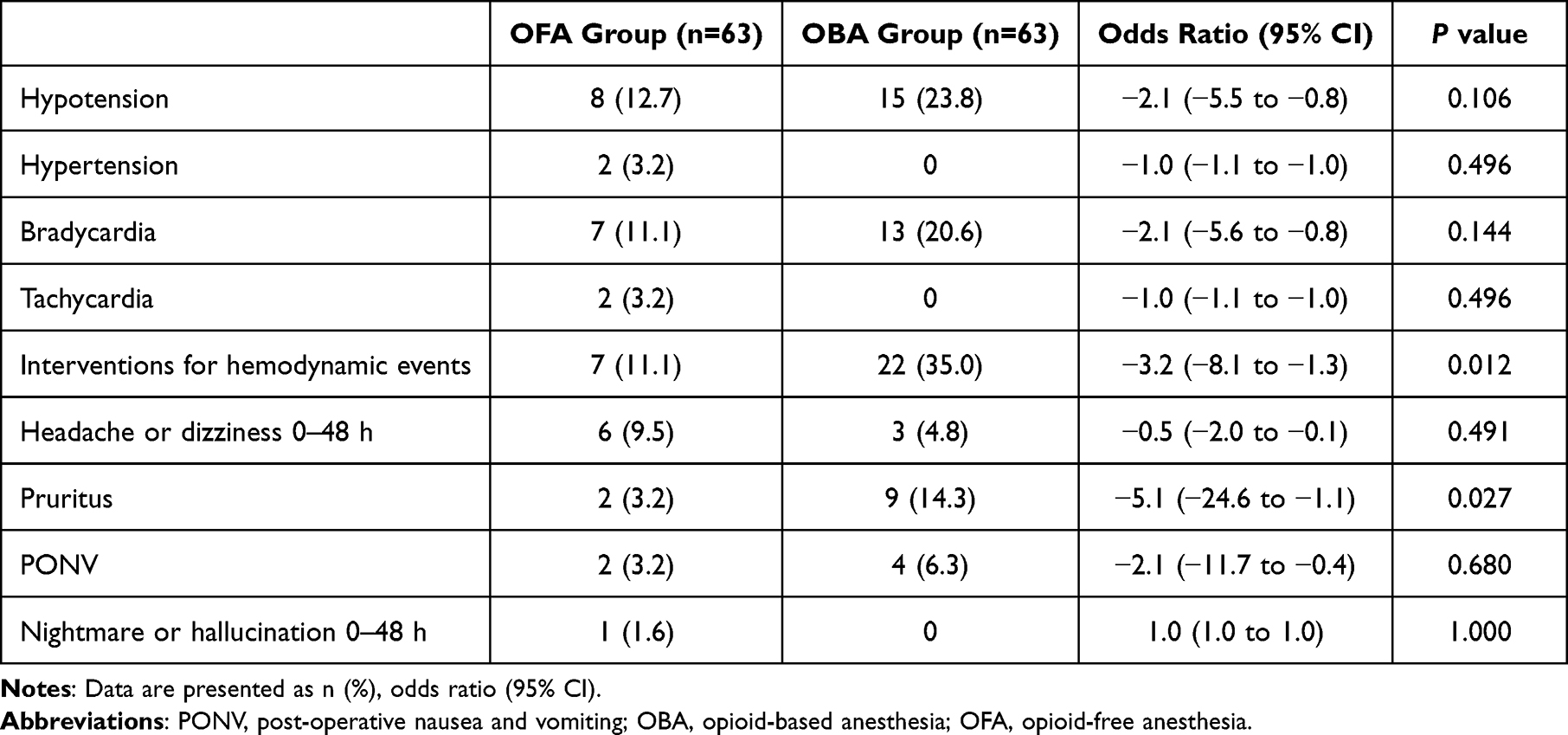 |
Table 3 Safety Outcomes |
QoR-15 Subdomain Scores at H24
Among the QoR-15 subdomains (Table 4), physical comfort scores were significantly higher in the OFA group than in the OBA group (45 [43–47] vs 44 [41–45]; 95% CI, 1 to 3; P<0.001). No significant between-group differences were observed in physical independence, emotional state, psychological support, or pain.
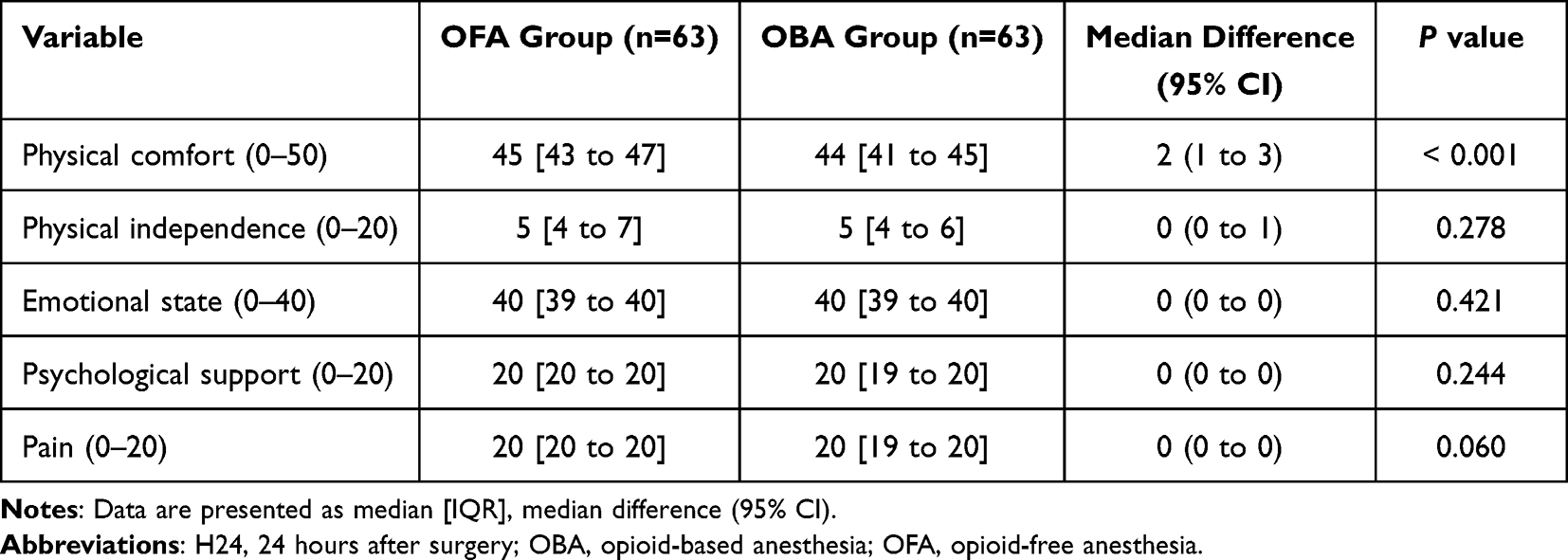 |
Table 4 Subdomain Analysis of the QoR-15 Score at H24 |
Sensitivity Analysis
To assess the robustness of the primary outcome, QoR-15 scores were categorized by recovery quality: excellent (136–150), good (122–135), moderate (90–121), or poor (<90).27 The proportion of patients achieving good or excellent recovery was higher in the OFA group than in the OBA group (88.9% vs 77.8%; P=0.094) (Figure 2).
 |
Figure 2 Distribution of patients according to categories of QoR-15 at H24. OBA, opioid-based anesthesia; OFA, opioid-free anesthesia; Excellent, 136–150; Good, 122–135; Moderate, 90–121; Poor, 0–89. |
Subgroup Analyses
Subgroup analyses were conducted according to three established predictors of recovery: age (<65 vs ≥65 years), BMI (<25 vs ≥25 kg·m−2), and surgery duration (<60 vs ≥60 minutes).24,28,29 Logistic regression was applied to compare the proportion of patients achieving good recovery (QoR-15≥122) between the OFA and OBA groups. No significant interactions were observed between treatment effect and any subgroup, indicating that the treatment effect of OFA on achieving good recovery was consistent across clinically relevant patient subgroups (Figure 3).
 |
Figure 3 Subgroup analysis of patients with good quality of recovery (QoR-15 score ≥122). |
Discussion
In this study, esketamine-based OFA was noninferior to OBA with respect to early postoperative recovery in patients undergoing elective laparoscopic TAPP repair. Comparable QoR-15 scores at 24 and 72 hours indicate that OFA provides a level of recovery equivalent to that of OBA. The noninferiority margin of −8 points was predefined on the basis of the MCID of the QoR-15 validated in abdominal surgery,24 and our results are consistent with thresholds reported in laparoscopic cholecystectomy studies, supporting its applicability to TAPP procedures.17 Additionally, OFA was associated with improved hemodynamic stability and a lower incidence of pruritus, consistent with ERAS objectives of minimizing opioid exposure.
These findings extend the existing evidence supporting the use of OFA in abdominal surgery.30,31 Notably, although laparoscopic TAPP shares the minimally invasive advantages of other laparoscopic procedures, it is characterized by a distinct pain profile, predominantly deep visceral pain related to peritoneal traction.16 Esketamine, a selective NMDA receptor antagonist, exerts inhibitory effects on central sensitization and hyperalgesia,32,33 which may partly explain the improved control of cough-related pain at 24 and 48 hours postoperatively, as well as the higher physical comfort scores observed in the OFA group. Effective control of movement-evoked pain and improved physical comfort are critical determinants of early mobilization after laparoscopic TAPP repair. Compared with opioid-sparing strategies reported in other surgical populations, the OFA regimen in the present study achieved comparable analgesia without compromising recovery-related outcomes, underscoring its potential adaptability across different surgical settings. To our knowledge, this is the first study to evaluate the impact of esketamine-based OFA on postoperative quality of recovery following laparoscopic TAPP repair, providing preliminary evidence to inform future clinical practice and guideline development.
The clinical implications of the secondary outcomes warrant careful interpretation, particularly with respect to their practical relevance. Although the OFA regimen was associated with a prolonged length of stay in the PACU, this finding may be attributable to the synergistic sedative effects of propofol in combination with esketamine.34 Similar observations have been reported in an OFA trial involving thoracic surgery,11 suggesting that delayed PACU discharge may represent a reproducible phenomenon across different surgical populations. To mitigate this limitation, future optimization of OFA protocols could focus on individualized dose adjustments or the use of alternative sedative agents in place of propofol, especially in the context of outpatient or fast-track surgical pathways. Importantly, OFA was associated with hemodynamic advantages, particularly a lower incidence of hypotension and a reduced need for vasopressor. These benefits may help offset the increased demand on PACU resources in high-risk or hemodynamically vulnerable patient populations. These preliminary observations merit confirmation in larger, adequately powered studies. From a safety perspective, the findings further support the potential advantages of OFA. The significantly lower incidence of pruritus is consistent with the avoidance of opioid-induced histamine release, while the observed trend toward fewer hypotensive events may be related to the sympathoexcitatory properties of esketamine.35,36
In addition to the primary outcome, subgroup analyses demonstrated consistent directional trends favoring OFA across categories defined by age, BMI, and surgery duration. Notably, patients with a BMI of <25 kg·m−2 or a duration of surgery of <60 minutes showed clinically meaningful improvements in recovery rates with OFA, although these differences did not reach statistical significance. These consistently favorable patterns across subgroups suggest the potential applicability of OFA across a range of patient characteristics. However, larger, adequately powered studies are required to formally evaluate potential effect modification.
The use of validated, patient-centered outcome measures is essential to capture the multidimensional nature of postoperative recovery, including comfort, pain control, and functional well-being. The QoR-15, endorsed by Myles et al as a core perioperative outcome measure, has been widely adopted for evaluating postoperative recovery and patient comfort following general anaesthesia.37–39 Accordingly, the QoR-15 was selected as the primary outcome in the present study. Its suitability as a primary endpoint is further supported by its extensive international use and the availability of a validated Chinese version with robust psychometric properties (Cronbach’s alpha = 0.76; intraclass correlation coefficient = 0.99).40 Using this validated and patient-centered outcome measure, our findings demonstrate that esketamine-based OFA achieved noninferior postoperative recovery compared with opioid-based anesthesia.
Several methodological limitations should be acknowledged. First, the OFA regimen was developed based on pilot observations and existing literature rather than formal dose-finding studies. Although this approach reflects current clinical practice, further research is required to optimize OFA regimens for laparoscopic TAPP repair and other surgical procedures. Second, the depth of anesthesia was not monitored, as we were concerned about the reliability of electroencephalogram-derived indices in the presence of NMDA receptor antagonism by esketamine.41 Third, recovery quality during the immediate postoperative period was not assessed using standardized quantitative tools. As a result, transient differences between anesthetic techniques during the very early recovery phase may not have been fully characterized. Fourth, our study primarily focused on early postoperative recovery as reflected by the QoR-15 score at 24 hours postoperatively and did not evaluate longer-term outcomes such as chronic pain. Finally, the relatively homogeneous study population constrains the generalizability of our findings to high-risk patients and female populations, who may exhibit distinct pharmacodynamic responses to esketamine.
In conclusion, esketamine-based OFA provides postoperative recovery that is noninferior to OBA in patients undergoing laparoscopic TAPP repair. Although the observed QoR-15 scores were slightly higher in the OFA group, no prespecified superiority hypothesis was tested; therefore, superiority cannot be inferred. Future multicenter studies are warranted to establish standardized OFA protocols, evaluate efficacy across diverse patient populations, and explore the broader applicability of esketamine-based OFA in other surgical settings.
Data Sharing Statement
Deidentified data are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Clinical Medical Research Ethics Committee of the First Affiliated Hospital of Anhui Medical University (approval no. PJ 2023-06-17, approval date: 11 May 2023, chairperson: Heng Wang).
Funding
This study was supported by the Beijing Health Alliance Charitable Foundation (Grant No. S251), the Health Research Program of Anhui (Grant No. AHWJ2024BAf20008), and the Funds of Peak Disciplines of the First Affiliated Hospital of Anhui Medical University, Anhui Province of China (2021-4237).
Disclosure
The authors declare no competing interests in this work.
References
1. Kunovac F, Cicvaric A, Robba C, et al. Gastrointestinal motility disorders correlate with intracranial bleeding, opioid use, and brainstem edema in neurosurgical patients. Neurocritical Care. 2023;39(2):368–12. doi:10.1007/s12028-023-01678-5
2. van Lemmen M, Dahan A, Hang Y, et al. TAK-925 (Danavorexton), an orexin receptor 2 agonist, reduces opioid-induced respiratory depression and sedation without affecting analgesia in healthy men. Anesthesiology. 2025;142(4):628–638. doi:10.1097/aln.0000000000005375
3. Yan H, Chen W, Chen Y, et al. Opioid-Free versus opioid-based anesthesia on postoperative pain after thoracoscopic surgery: the use of intravenous and epidural esketamine. Anesthesia Analg. 2023;137(2):399–408. doi:10.1213/ane.0000000000006547
4. Dieterle M, Zurbriggen L, Mauermann E, et al. Pain response to cannabidiol in opioid-induced hyperalgesia, acute nociceptive pain, and allodynia using a model mimicking acute pain in healthy adults in a randomized trial (CANAB II). Pain. 2022;163(10):1919–1928. doi:10.1097/j.pain.0000000000002591
5. Léger M, Perrault T, Pessiot-Royer S, et al. Opioid-free anesthesia protocol on the early quality of recovery after major surgery (SOFA Trial): a randomized clinical trial. Anesthesiology. 2024;140(4):679–689. doi:10.1097/aln.0000000000004840
6. Wang D, Sun Y, Zhu YJ, et al. Comparison of opioid-free and opioid-inclusive propofol anaesthesia for thyroid and parathyroid surgery: a randomised controlled trial. Anaesthesia. 2024;79(10):1072–1080. doi:10.1111/anae.16382
7. Massoth C, Schwellenbach J, Saadat-Gilani K, et al. Impact of opioid-free anaesthesia on postoperative nausea, vomiting and pain after gynaecological laparoscopy - A randomised controlled trial. J Clin Anesthesia. 2021;75:110437. doi:10.1016/j.jclinane.2021.110437
8. Chen M, Jin J, Bi H, et al. Advances in the study of NMDA receptors in depression pathogenesis and the antidepressant efficacy of their antagonists. Asian J Psych. 2025;108:104502. doi:10.1016/j.ajp.2025.104502
9. Hung KC, Kao CL, Ho CN, et al. Efficacy and safety of esketamine in preventing perioperative neurocognitive disorders: a meta-analysis of randomized controlled studies. Syst Rev. 2025;14(1):68. doi:10.1186/s13643-025-02807-1
10. Ouyang J, Xiao W, Wu D, Bai M, Zhao Q, Li Y. Esketamine alleviated cardiomyocyte ferroptosis induced by oxygen-glucose deprivation/reoxygenation (OGD/R) via cyclic GMP-AMP synthase interactor. Cytotechnology. 2025;77(2):57. doi:10.1007/s10616-025-00723-9
11. Feng CD, Xu Y, Chen S, et al. Opioid-free anaesthesia reduces postoperative nausea and vomiting after thoracoscopic lung resection: a randomised controlled trial. Br J Anaesth. 2024;132(2):267–276. doi:10.1016/j.bja.2023.11.008
12. Gao H, Xu Z, Zhang L, et al. Superiority of opioid free anesthesia with regional block over opioid anesthesia with regional block in the quality of recovery after retroperitoneiscopic renal surgery: a randomized controlled trial. Minerva anestesiologica. 2024;90(10):845–854. doi:10.23736/s0375-9393.24.18186-2
13. Ozgok A, Demir AZ. Opioid-free anesthesia works like a charm in cardiac surgery. Anesthesia Pain Med. 2021;16(2):213–214. doi:10.17085/apm.21017
14. Barakat H, Al Nawwar R, Abou Nader J, Aouad M, Yazbeck Karam V, Gholmieh L. Opioid-free versus opioid-based anesthesia in major spine surgery: a prospective, randomized, controlled clinical trial. Minerva anestesiologica. 2024;90(6):482–490. doi:10.23736/s0375-9393.24.17962-x
15. HerniaSurge Group. International guidelines for groin hernia management. Hernia. 2018;22(1):1–165. doi:10.1007/s10029-017-1668-x
16. Tolver MA, Rosenberg J, Bisgaard T. Early pain after laparoscopic inguinal hernia repair. A qualitative systematic review. Acta anaesthesiologica Scandinavica. 2012;56(5):549–557. doi:10.1111/j.1399-6576.2011.02633.x
17. Hao C, Xu H, Du J, et al. Impact of opioid-free anesthesia on postoperative quality of recovery in patients after laparoscopic cholecystectomy-a randomized controlled trial. Drug Des Devel Ther. 2023;17:3539–3547. doi:10.2147/dddt.s439674
18. Zhou X, Feng W, Wang X, et al. The effect of opioid-free anesthesia with transversus abdominis plane block on patients undergoing laparoscopic sleeve gastrectomy: randomized controlled study. J Pain Res. 2024;17:2881–2890. doi:10.2147/jpr.s471813
19. An G, Wang G, Zhao B, et al. Opioid-free anesthesia compared to opioid anesthesia for laparoscopic radical colectomy with pain threshold index monitoring: a randomized controlled study. BMC anesthesiology. 2022;22(1):241. doi:10.1186/s12871-022-01747-w
20. Wang J, Huang J, Yang S, et al. Pharmacokinetics and safety of esketamine in chinese patients undergoing painless gastroscopy in comparison with ketamine: a randomized, open-label clinical study. Drug Des Devel Ther. 2019;13:4135–4144. doi:10.2147/dddt.s224553
21. Brinck ECV, Maisniemi K, Kankare J, Tielinen L, Tarkkila P, Kontinen VK. Analgesic effect of intraoperative intravenous S-ketamine in opioid-naïve patients after major lumbar fusion surgery is temporary and not dose-dependent: a randomized, double-blind, placebo-controlled clinical trial. Anesthesia Analg. 2021;132(1):69–79. doi:10.1213/ane.0000000000004729
22. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
23. Jebb AT, Ng V, Tay L. A review of key likert scale development advances: 1995-2019. Frontiers in Psychology. 2021;12:637547. doi:10.3389/fpsyg.2021.637547
24. Liang Z, Liu J, Chen S, et al. Postoperative quality of recovery comparison between ciprofol and propofol in total intravenous anesthesia for elderly patients undergoing laparoscopic major abdominal surgery: a randomized, controlled, double-blind, non-inferiority trial. J Clin Anesthesia. 2024;99:111660. doi:10.1016/j.jclinane.2024.111660
25. Meng F, Baradaran A, Jaberi MM, et al. Patient-Reported quality of recovery after local anesthesia versus brachial plexus block in hand surgery: a randomized controlled study. Plastic Reconstructive Surg. 2023;152(6):1287–1296. doi:10.1097/prs.0000000000010688
26. Choi JY, Lee HS, Kim JY, et al. Comparison of remimazolam-based and propofol-based total intravenous anesthesia on postoperative quality of recovery: a randomized non-inferiority trial. J Clin Anesthesia. 2022;82:110955. doi:10.1016/j.jclinane.2022.110955
27. Kleif J, Gögenur I. Severity classification of the quality of recovery-15 score-An observational study. J Surg Res. 2018;225:101–107. doi:10.1016/j.jss.2017.12.040
28. van Kooten RT, Bahadoer RR, Peeters K, et al. Preoperative risk factors for major postoperative complications after complex gastrointestinal cancer surgery: a systematic review. Eur J Surg Oncol. 2021;47(12):3049–3058. doi:10.1016/j.ejso.2021.07.021
29. Shen X, Zhou C, Hua Q, Yang L, Zhao W, Xu P. Impact of operation duration on short-term and long-term prognosis in patients undergoing radical colorectal surgery. J Cancer. 2022;13(4):1160–1167. doi:10.7150/jca.65817
30. Collange V, Berruet JB, Aubrun F, et al. Opioid free versus opioid sparing strategies for multimodal antinociception during laparoscopic colectomy: a randomised controlled trial. Anaesth Crit Care Pain Med. 2024;43(6):101436. doi:10.1016/j.accpm.2024.101436
31. da Silveira CAB, Rasador ACD, Medeiros HJS, et al. Opioid-free anesthesia for minimally invasive abdominal surgery: a systematic review, meta-analysis, and trial sequential analysis. Canad J Anaesthes J Canad D’anesthesie. 2024;71(11):1466–1485. Anesthésie sans opioïdes pour la chirurgie abdominale minimalement invasive: une revue systématique, une méta-analyse et une analyse séquentielle des études. doi:10.1007/s12630-024-02831-0
32. He Q, Liu Q, Liang B, et al. Esketamine use for primary intelligent analgesia in adults with severe burns: a double-blind randomized trial with effects on analgesic efficacy, gastrointestinal function and mental state. Burns. 2024;50(9):107187. doi:10.1016/j.burns.2024.06.004
33. Lu Y, Yin G, Jin C, et al. The application value of esketamine and dexmedetomidine in preventing postoperative delirium and hyperalgesia in elderly patients with thoracic anesthesia. Alternative Therap Health Med. 2024;30(3):80–85.
34. Kan Z, Min W, Dai Y, Zhang P. Intravenous esketamine as an adjuvant for sedation/analgesia outside the operating room: a systematic review and meta-analysis. Front Pharmacol. 2024;15:1287761. doi:10.3389/fphar.2024.1287761
35. Baldo BA. Toxicities of opioid analgesics: respiratory depression, histamine release, hemodynamic changes, hypersensitivity, serotonin toxicity. Arch Toxicol. 2021;95(8):2627–2642. doi:10.1007/s00204-021-03068-2
36. Krantz MJ, Palmer RB, Haigney MCP. Cardiovascular complications of opioid use: JACC state-of-the-art review. J Am College Cardiol. 2021;77(2):205–223. doi:10.1016/j.jacc.2020.11.002
37. Myles PS, Wallace S, Boney O, et al. An updated systematic review and consensus definitions for standardised endpoints in perioperative medicine: patient comfort and pain relief. Br J Anaesth. 2025. doi:10.1016/j.bja.2025.02.025
38. Bailey JG, Hendy A, Neira V, Chedrawy E, Uppal V. Continuous serratus anterior block for sternotomy analgesia after cardiac surgery: a single-centre feasibility study. Br J Anaesth. 2025;134(4):1161–1169. doi:10.1016/j.bja.2024.11.042
39. Yau DKW, Ng FF, Wong MH, et al. Effect of exercise prehabilitation on quality of recovery after cardiac surgery: a single-centre randomised controlled trial. Br J Anaesth. 2025;134(1):45–53. doi:10.1016/j.bja.2024.08.039
40. Bu XS, Zhang J, Zuo YX. Validation of the Chinese version of the quality of recovery-15 score and its comparison with the post-operative quality recovery scale. patient. 2016;9(3):251–259. doi:10.1007/s40271-015-0148-6
41. Mogianos K, Persson AK. Anesthesia depth monitoring during opioid free anesthesia - a prospective observational study. BMC Anesthesiology. 2025;25(1):37. doi:10.1186/s12871-024-02859-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.