Back to Journals » Journal of Blood Medicine » Volume 16
Erythrocyte Alloimmunization and Transfusion Strategies in Sickle Cell Disease: A Single-Center Analysis
Authors Yusuf A ![]() , Ahmad A, El-Beshbishy HA, Gong HB, Chahdah CW, Bakhsh T
, Ahmad A, El-Beshbishy HA, Gong HB, Chahdah CW, Bakhsh T ![]()
Received 16 July 2025
Accepted for publication 25 September 2025
Published 3 October 2025 Volume 2025:16 Pages 445—455
DOI https://doi.org/10.2147/JBM.S548152
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Abdulaziz Yusuf,1,2 Abrar Ahmad,1 Hesham A El-Beshbishy,3 Heba Badie Gong,3 Chahed Walid Chahdah,3 Tahani Bakhsh4
1Department of Biochemistry, Faculty of Science, King Abdulaziz University, Jeddah, Saudi Arabia; 2Blood Bank Department, Dr. Soliman Fakeeh Hospital, Fakeeh Care Group, Jeddah, Saudi Arabia; 3Medical Laboratory Sciences Department, Fakeeh College for Medical Sciences, Fakeeh Care Group, Jeddah, 21461, Saudi Arabia; 4Department of Biological Sciences, College of Science, University of Jeddah, Jeddah, 23218, Saudi Arabia
Correspondence: Abdulaziz Yusuf, Blood Bank Department, Dr. Soliman Fakeeh Hospital, Fakeeh Care Group, Jeddah, Saudi Arabia, Email [email protected]
Aim: Alloimmunization (the production of antibodies against foreign red blood cell (RBC) antigens) is a significant complication in patients with sickle cell disease (SCD) who require chronic transfusion. This retrospective study examined the distribution of ABO and Rh phenotypes in SCD patients at Dr. Soliman Fakeeh Hospital in Jeddah (DSFH-J) and their implications for alloimmunization risk. The high immunogenicity of the K antigen in the Kell system, second only to that of the D antigen in the Rh system, makes it a frequent target.
Results: Among 241 patients with SCD, the most common blood group was O (58.5%), followed by A (26.97%), B (12.03%), and AB (2.9%). The majority of patients (93.36%) were Rh-positive (D antigen-present). Among Rh antigens, the e antigen was the most prevalent (97.51%), while C antigen and c antigen were detected in 68.04% and 75.52% of patients, respectively. Within the Kell system, K was found in 8.29% of the study population. The most common antibodies detected were anti-E (20%) and anti-C (15%), indicating Rh incompatibilities to be a major concern. Kell system antibodies (anti-K) accounted for 12.5% of cases, and unidentified alloantibodies represented 17.5%. Although antibodies from other blood group systems (such as Kidd, Duffy, Lutheran, and MNS) were detected at low frequencies, their presence and known clinical significance in causing transfusion reactions underscore the need for extended RBC phenotyping to include these systems.
Conclusion: The observed distribution of Rh phenotypes and the presence of alloantibodies beyond the prevalent ones highlights the need for extended RBC phenotyping to include other blood group systems, such as Kidd and Duffy. Establishing a national blood donor registry with comprehensive RBC antigen data is a crucial step toward ensuring safer transfusions. Standardizing blood screening protocols across hospitals in Saudi Arabia and introducing routine extended RBC typing before transfusions would minimize alloimmunization risks and improve the overall patient safety.
Keywords: sickle cell disease, RBC alloimmunization, Rh phenotype, blood transfusion
Introduction
Sickle cell disease (SCD) is a hereditary genetic disorder that causes abnormal hemoglobin structure,1 resulting from a mutation in the β-globin gene.2,3 This mutation leads to the production of an abnormal hemoglobin type known as hemoglobin S.3,4 In classic autosomal recessive, inheritance of one normal allele and one abnormal allele results in a sickle cell trait, a carrier state without clinical symptoms.2,5 The condition manifests clinically when two mutated alleles are inherited, or through codominance with other distinct beta globin mutations, encompassing various genotypes. This includes homozygosity for the Beta S allele, which results in sickle cell anemia, considered the most severe form. It is characterized by chronic hemolytic anemia, recurrent pain, increased susceptibility to infection, and other significant complications.2 Red blood cell (RBC) transfusion therapy serves as a cornerstone in the management of SCD, aiming to alleviate symptoms and prevent complications.1,6,7 However, with the increased use of transfusion techniques to manage patients with SCD, alloimmunization has become an important issue.8,9 The development of alloantibodies remains a significant challenge in patients with SCD, limiting the availability of suitable blood for transfusion.9,10
ABO blood groups are a fundamental classification of human blood based on the presence or absence of A and B antigens on the surface of RBCs.11,12 The ABO system is characterized by naturally occurring anti-A and anti-B antibodies.11 These antibodies are responsible for acute hemolytic transfusion reactions if ABO-incompatible blood is transfused.12,13 Individual with type A blood have anti-B antibodies, those with type B have anti-A antibodies, those with type O have both, and those with type AB have neither.14 The prevalence of ABO blood groups exhibits variations across different populations;15 For instance, A subgroups are more frequent in European descent, whereas B subgroups are more frequent among the Japanese population.12,16 Additionally, the frequency of ABO blood groups can influence susceptibility to certain infections, with individuals in the O blood group being protected from severe forms of malaria, but have a greater risk of cholera.12,17 The Rh blood group system is the second most important blood group system in transfusion medicine after ABO.12 It is characterized by a high degree of polymorphism, with 56 defined antigens.18 The most clinically significant Rh antigen is the D antigen, which is highly immunogenic.12,18 Individuals who have the D antigen are referred to as Rh-positive, whereas those who lack it are Rh-negative. In addition to D antigen, other important Rh antigens include C, c, E, and e. These antigens can elicit an immune response and lead to alloimmunization following transfusion.12,19 The frequency of these antigens varies among populations.20 For example, among 28,946 blood donors, the frequency of e antigen was 97.95%, while the frequency of E antigen was 26.0%.12 Given the complexity and polymorphism of the Rh system, accurate Rh typing is crucial in transfusion medicine to ensure compatibility and prevent alloimmunization.12,18 In transfusion therapy, the expression of Rh antigens is a crucial point to consider.18 The incidence of alloimmunization in SCD patients ranges from 7% to 47% and is influenced by factors such as age, ethnicity, sex, RBC exposure, and antigen mismatch.9 Despite Blood transfusions are a critical component in managing SCD, they present numerous associated challenges, particularly alloimmunization. Studies conducted in different regions of Saudi Arabia have highlighted the prevalence of alloantibodies among transfusion-dependent patients, with the Rh and Kell blood group systems being the primary contributors. However, in 2015, a pilot study in Jeddah at King Abdulaziz University Hospital (KAUH) documented a 12.8% rate with Rh (65.1%) and Kell (18.6%) antibodies.9 In Jazan Province, a multicenter study reported an overall rate of 7.6%, with anti-E (25.9%) and anti-K (24.1%) predominating. Rates were lower than in other Saudi regions (eg, 12.8–39.4% in Western Saudi Arabia), attributed to the Rh system and K-matched transfusions.21 In 2024, a study at King Abdulaziz Medical City-Jeddah (KAMC-J) found an alloimmunization rate of 17.4% among pediatric patients with SCD, with anti-K (23.7%), anti-E (19%), and anti-S (9.5%) as the most common antibodies. Patients receiving frequent transfusions, exchange transfusions, or those under 3 years of age have higher alloimmunization risks.22 This increase may reflect changes in transfusion practices, patient demographics, or screening protocols over time. Moreover, studies from Kuwait have highlighted the prevalence of alloantibodies among transfusion-dependent patients, with Rh and Kell blood group systems being the primary contributors. In fact, 65.5% of alloimmunized patients in these studies were found to carry antibodies against the Rh and Kell antigens.23 These findings underscore the importance of implementing extended Rh antigen matching to minimize transfusion-related complications and improve patient outcomes.10,24 With a high prevalence of antibodies targeting Rh phenotypes, optimizing transfusion protocols is crucial for ensuring the effective long-term management of patients with SCD. In this study, we examined the prevalence of RBC antigens among patients with SCD at Dr. Soliman Fakeeh Hospital (DSFH-J) and assessed the impact of Rh phenotype-matched transfusions on alloimmunization rates and overall patient care.
Materials and Methods
Patients and Data Collection
This study was conducted at DSFH-J, Saudi Arabia, from 2021 to 2024, and included 241 patients with SCD. The study was executed under the DSFH-J criteria after obtaining approval from the Institutional Review Board (IRB) (Approval No. 517/IRB/2023). Clinical and laboratory data were gathered from the DSFH information system. These data included diagnoses of SCD for admitted patients, records from the blood transfusion service, and results from routine indirect antiglobulin tests (IAT) performed on patients receiving transfusions. Blood samples were withdrawn from the patients as a protocol for health care examination and routinely checked for blood group, Rh phenotype, and RBC antibody screening. Antibody identification was performed when the antibody screening was positive.
Pre-Transfusion Testing
All samples were tested using the column agglutination method DiaClon ABO DVI+ for blood groups A, B, O, and AB with Rh type followed by C, E, c, e, and K antigens using a column agglutination gel card (Bio-Rad, Germany). The plasma samples were prepared for antibody screening and identification. Automated column agglutination (Daymate S Analyzer, Switzerland) was used for screening, following the manufacturer’s instructions. A three-cell screening panel was used for IAT. All positive antibody screen samples were subjected to antibody-identification screening. The antibodies were manually identified using commercial 11-cell identification panels (Bio-Rad). The screening and identification of red cell antibodies using commercially available O cells met worldwide standards for antibody detection.
Statistical Analysis
Patient characteristics were analyzed using descriptive statistics in SPSS, and the differences between alloimmunized, non-alloimmunized, and autoimmunized patients were assessed for frequencies of antigen as a percentage. P-values were used to calculate the Z-test for population proportions to evaluate the significant association between alloimmunization rate and transfusion data. A significant association was indicated when the P-value was less than or equal to 0.05.
Results
For all patients with SCD the demographic characteristics of 241 sickle cell patients at DSFH-J were analyzed. The Majority of patients (47.3%) were age range 25–45 years, highlighting that a significant proportion of transfusion-dependent individuals were adults. The second largest age group, comprising 30.7% of patients, was younger than 17 years. Meanwhile, 16.6% of the patients belonged to the 17–24 age category, reflecting the transition of adolescent patients into adulthood while still managing complications (Table 1).
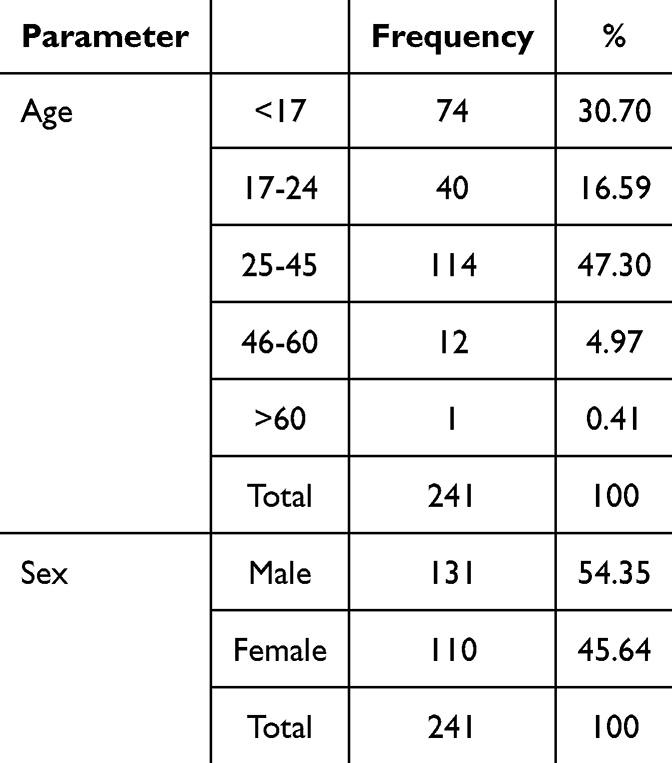 |
Table 1 Demographic Characteristics of Sickle Cell Patients |
Blood group O was the most common (58.5%), followed by groups A (26.97%), B (12.03%), and AB (2.9%). Most patients were Rh-positive (D antigen-present) (93.36%). In terms of the Rh antigens, e antigen was the most prevalent (97.51%), whereas C and c appeared in 68.04% and 75.52% of patients, respectively. Within Kell system, K antigen was found in 8.29% of the study population (Table 2).
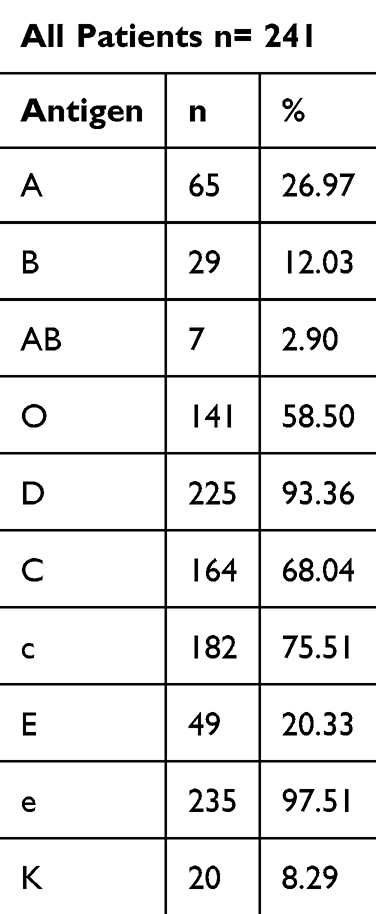 |
Table 2 Distribution of Blood Groups and Rh Phenotypes Among Sickle Cell Patients |
The most common phenotype among the patients was R1r (DCcee), appearing in 34.02% of the cases. This phenotype suggests a strong presence of the D, C, and e antigens, making it significant for transfusion strategies, as individuals with this phenotype are likely to be compatible with donors possessing similar Rh antigen expression. The second most prevalent phenotype, R1R1 (DCCee), was observed in 21.58% of the cases, reinforcing the predominance of D and C antigens within the population. Subsequently, R0r (Dccee) was found in 15.35% of patients, indicating a moderate representation of the D, c, and e antigen combination. These patients may require more precise matching to avoid transfusion-related complications. Meanwhile, the least common phenotypes, RzRz (DCCEE) and r’r’ (dCCee), were present in only 0.41% of cases each, highlighting their rarity and the potential difficulties in finding compatible blood units for individuals with these phenotypes (Table 3). Among the 241 patients, 40 individuals were found to have alloantibodies. These antibodies were distributed across multiple blood group systems, including Rh, MNS, Kell, Lutheran, Kidd, and Duffy. The most common antibodies were anti-E (20%) and anti-C (15%), emphasizing the prevalence of Rh incompatibility. Kell system antibodies made up 12.5%, while Kidd and Duffy blood groups showed minimal occurrences. Unidentified alloantibodies accounted for 17.5% of the cases, showing gaps in the diagnostic classification (Table 4). This study reported an alloimmunization rate of 11.2% among 241 patients with SCD. In comparison, a multicenter study in Jazan Province documented a rate of 12.98%,25 indicating no substantial difference in alloimmunization rates, similar to the Eastern Region’s reported 13.7%.26 A study conducted at King Abdulaziz University Hospital in 2020 reported a significantly higher rate of 39.42%.20 In Oman, the rate was 31.6%,27 and in Kuwait, two cohorts showed rates of 65.5% and 23.6%.23 A study of pediatric patients with SCD in KAMC-J found an alloimmunization rate of 17.4%.22 These findings confirm the statistical significance of the alloimmunization rates, with variations potentially reflecting differences in transfusion protocols, antigen matching practices, and population genetics. P-values indicate statistical significance (Table 5).
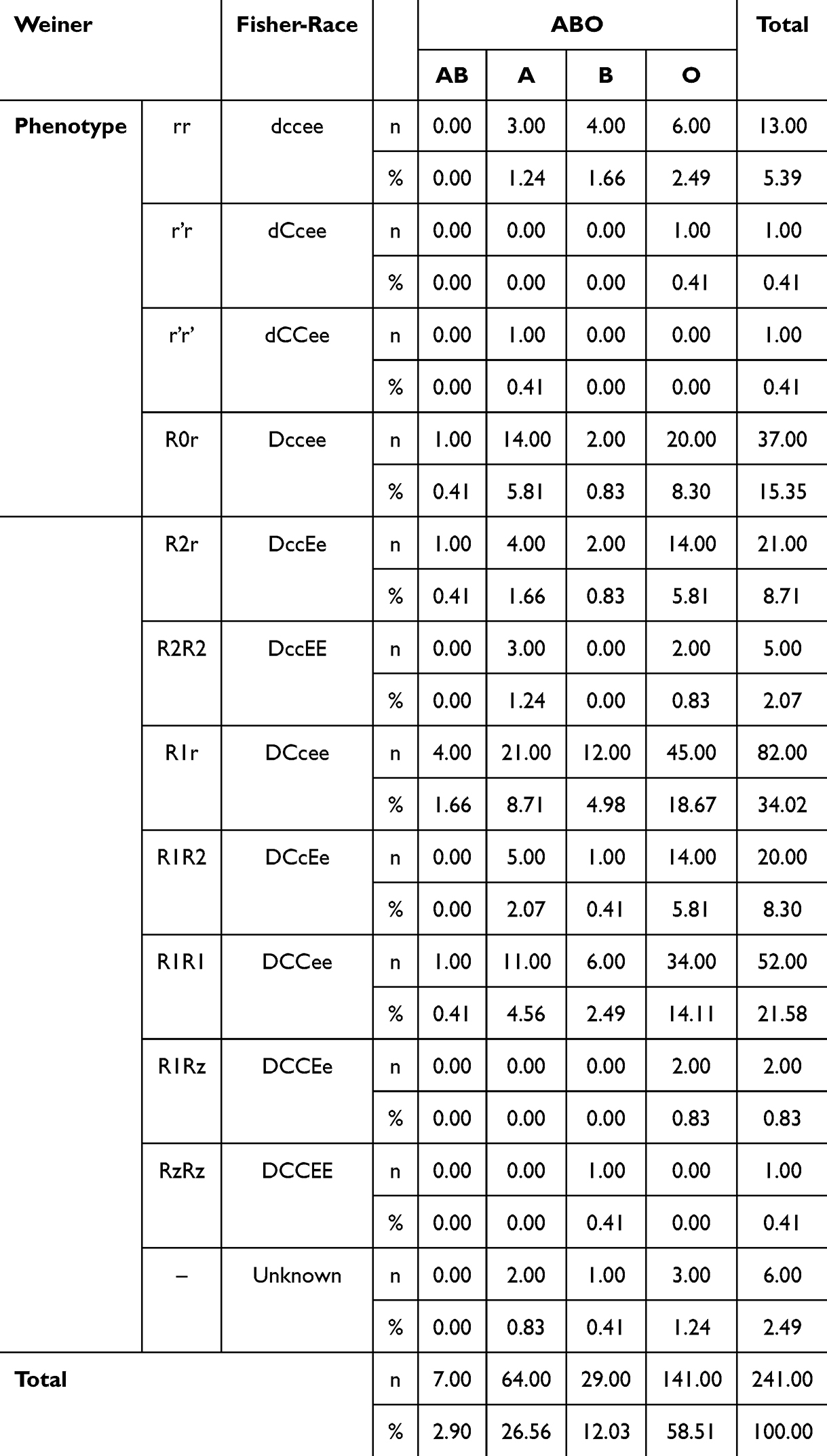 |
Table 3 Distribution of Different Rh Phenotypes Among Patients Based on the Weiner and Fisher-Race Classification Systems |
 |
Table 4 Distribution of Erythrocyte Alloantibodies in Sickle Cell Patients |
 |
Table 5 Alloimmunization Rates Across Different Studies in Saudi Arabia and Neighboring Regions |
Discussion
Blood transfusions are a cornerstone of SCD management, providing critical support to patients experiencing complications, such as vaso-occlusive crises and acute chest syndrome. However, these transfusions carry the risk of alloimmunization, a condition in which the immune system produces antibodies against antigens on the surface of the transfused RBCs. Alloimmunization remains a significant concern in SCD management, as it can lead to complications, such as delayed hemolytic transfusion reactions and difficulties in finding compatible blood for future transfusions.
In our study, we observed an alloimmunization rate of 11.2% among 241 patients with SCD. This finding highlights the ongoing challenge in managing transfusion-related risks in this population. In this context, it is crucial to compare them with global data, which shows varying alloimmunization rates influenced by factors such as genetic diversity, healthcare practices, and transfusion protocols.28 In the United States, alloimmunization rates among transfused patients range from approximately 25% to 30%, with variations influenced by ethnicity and transfusion practices.29 In a systematic review conducted across sub-Saharan Africa, the overall incidence of alloimmunization was 7.4%. However, in certain countries, this rate escalated to as high as 28.0%, highlighting that even with blood group similarities between donors and recipients, the risk of alloimmunization remains significant.30 A comparative analysis of alloimmunization rates across various studies in Jazan, Eastern region of Saudi Arabia, KAUH, Oman, KAMC-J, and Kuwait is shown in Table 5, which highlights the variances in transfusion practices and their respective effects on patient outcomes. The significant variations observed in alloimmunization rates can largely be attributed to several key elements. Diverse transfusion protocols and their implementation play a crucial role. While studies have consistently emphasized the importance of established transfusion protocols as a protective measure against alloimmunization,9 the stringency and specific guidelines of these protocols can vary, potentially leading to differing outcomes. Despite these protocols, the complete elimination of alloimmunization remains a challenge.1 Antigen matching for individuals receiving chronic transfusions is a critical determinant, a strategy that has been demonstrated to reduce both alloimmunization and hemolytic transfusion reactions.31 However, challenges persist due to inherent differences in RBC antigen frequencies between donor populations, often predominantly Caucasian, and SCD patients, who are primarily of African descent.28 In addition, the inherent genetic characteristics of the population significantly impact alloimmunization rates. Genetic diversity between recipients and donors is a major contributing factor.22 A lower incidence of alloimmunization is often linked to racial similarity and homogeneity in RBC antigens between donor and recipient populations. Conversely, disparities in racial antigen profiles can lead to higher alloimmunization frequencies.1
Beyond these primary factors, other variables such as the patient’s age, gender, the cumulative number of packed RBC units transfused, and the presence of autoantibodies also influence the risk of alloimmunization.18 For example, the lower rate observed in Jazan (12.98%)25 has been attributed to routine Rh and Kell matching, whereas KAUH’s higher rate (39.42%)20 may arise from limited antigen matching and a more heterogeneous donor pool. KAMC-J, which reported a rate of 17.4%,22 implemented pediatric-focused transfusion strategies, including early initiation of exchange transfusions and extended phenotyping for high-risk patients. These institutional differences underscore the need for standardized national protocols and region-specific donor registries to mitigate alloimmunization risk. Homogeneity studies have shown that when patients receive blood from donors of the same ethnicity, the risk of alloimmunization is lower.22,32
This study revealed that the most common alloantibodies were anti-E, anti-C and anti-K. This observation aligns with existing research, indicating the significant role of Rh and Kell blood groups in alloimmunization. Another study reported that anti-E and anti-K were the most frequent alloantibodies identified in approximately 18.6% of the total alloantibodies,20 while in Omani SCD patients, anti-E was the most frequent antibody (26.8%), followed by anti-K (12.2%).27 Meanwhile, the KAMC-J Study revealed that alloimmunized patients comprised approximately 17.4% of the population, with anti-K (23.7%) and anti-E (19%) being the most frequent antibodies.22 The presence of these antibodies likely resulted from exposure to incompatible transfusions administered at facilities where extended antigen phenotyping was the standard practice, although adherence was not consistently maintained.24 In a similar study in Palestine, the alloimmunization rate was 7.76%, with the highest occurrence of K antigens (33.3%), followed by anti-E (22.2%), anti-C (11.1%), anti-c (11.1%), and anti-D (11.1%).33 This indicates that the Rh antigens, particularly D antigen, are highly immunogenic,12 which has the capability to trigger the immune response in individuals who lack antigens. Other Rh antigens may have inadequate matching during transfusions is a major cause.34 The K antigen in the Kell system is highly immunogenic, second only to the D antigen in the Rh system.35 While the K antigen is not as common as some Rh antigens, its presence in a subset of the population means that there is a risk of exposure and subsequent alloimmunization in those who lack the antigen, which makes it a frequent target.12 Beyond the prevalent alloantibodies, this study also identified RBC alloantibodies associated with the MNS, Lutheran, Kidd, and Duffy blood group systems. Within the MNS system, anti-N antibodies were detected in 2.5% of the patients. The other antigen-induced antibodies within Lutheran system revealed the presence of anti-Lua antibodies in 5% and anti-Lub antibodies in 2.5% of the patient population. Furthermore, within the Kidd system, anti-Jka antibodies presented in 2.5% of the patients, whereas the Duffy system presented anti-Fya antibodies in 7.5% of the cases. Migration patterns from other regions can alter the genetic distribution of the population, potentially increasing the alloimmunization risk if donors are from different genetic backgrounds. However, the frequency and volume of blood transfusions are directly correlated with an increased risk of alloimmunization, as each transfusion introduces the recipient to new antigens, thereby elevating the probability of antibody formation. Additionally, Rh D positive was observed to be higher than Rh D negative, similar to many studies in Jazan and KAUH.15,20 In these studies, the Rh e antigen was the most prevalent, followed by the C and c antigens, while the E antigen showed the lowest prevalence. However, the Jazan study reported a slightly higher prevalence of the Rh c antigen (86.39%)25 compared to DSFH-J (75.52%), suggesting regional variations in Rh antigen distribution. Furthermore, the prevalence of E antigen (20.33%) in DSFH-J was lower than that in Jazan (26.76%),25 indicating potential differences in immunogenic exposure among patients with SCD. Although the K antigen prevalence in DSFH-J (8.29%) was marginally higher than in Jazan (6.34%),25 the difference was not pronounced and may reflect minor demographic. The presence of rare Rh phenotypes, such as RzRz (DCCEE), which is uncommon in the general population,12,18 presents significant challenges for transfusion.36 Owing to the limited availability of compatible blood, patients with such phenotypes face an elevated risk of alloimmunization,37 complicating the identification of matched donors for those requiring transfusions.
The most prevalent blood type was O, present in 141 individuals. The significance of universal donors has been emphasized in numerous studies, and their contributions are highly valued.38 Blood group A was the second most common group (64 patients). Blood groups B and AB were less represented, with 29 and 7 patients, respectively. Regarding Rh phenotype distribution, the R1r phenotype was most frequently observed across all ABO blood groups, with a total of 82 patients. The R1R1 phenotype was also common and present in 52 patients. A similar study on voluntary blood donors in South India found R1R1 to be 35.2%.39 Data from European ethnicity showed 17.6% and African ethnicity 2.9%. Another study in a South Indian population reported 43.4%.40 Moreover, the presence of additional phenotypes, including R0r and R2r, were observed, which have been noted to potentially induce anti-C alloantibodies when exposed to the common phenotype. Conversely, rare phenotypes, such as r’r, r’r’, R2R2 and RzRz, had minimal representation within the studied population, similar to other studies across most populations. In a study on the Macedonian population, the most frequent Rh phenotype was DCcee (32.7%), and Rh phenotypes with homozygous expression of the E antigen are rare because their frequency in the presence of the D and C antigens is < 1%.12 The prevalence of R2R2 phenotype among Saudi donors has been reported to be 0.2%. Furthermore, patients with multiple antibodies encounter significant challenges in obtaining compatible antigen-negative blood units. Women, particularly those with previous pregnancies, are at a higher risk of alloimmunization due to fetal-maternal antigen exposure.20 This highlights the importance of rigorous blood screening protocols, particularly for patients who undergo frequent transfusions.
To mitigate transfusion complications, this study recommends expanding phenotyping protocols beyond Rh and Kell systems to include Kidd, Duffy, MNSs, Lewis, Lutheran, and P blood groups, which have been implicated in alloimmunization cases. Establishing a national blood donor registry with comprehensive RBC antigen data is proposed as a crucial step toward ensuring safer transfusions.37,41 Such a registry would improve blood matching efficiency and prevent hemolytic reactions, particularly in chronically transfused patients.
Additionally, this study emphasizes the need for policy changes in blood screening protocols across hospitals in Saudi Arabia. Introducing routine extended RBC typing before transfusion minimizes alloimmunization risk and improves overall patient safety. Hospitals should adopt pretransfusion antibody screening to prevent complications and reduce the likelihood of incompatible transfusions.
Limitations
The absence of genotyping analysis for SCD patients who have undergone external post-transfusion procedures may lead to mixed-field reactions. The available data lack sufficient standardized information for a reliable comparison of specific factors such as geographical area, population characteristics, and institutional differences.
Conclusion
This study describes the distribution of Rh phenotypes and ABO blood groups in patients with SCD in DSFH-J. The high prevalence of the R1r phenotype, coupled with the presence of rarer phenotypes and the risk of alloimmunization, illustrates the importance of improved transfusion practices. Implementing extended RBC phenotyping, establishing a national blood donor registry, and standardizing blood screening protocols across hospitals are crucial steps toward mitigating transfusion complications and enhancing patient safety. Furthermore, future research should focus on investigating the genetic basis of Rh and ABO blood group distribution in different regions of Saudi Arabia and assessing the impact of these variations on alloimmunization risk.
Ethics Approval and Informed Consent
The study adhered to the principles of Dr. Soliman Fakeeh Hospital and received ethical approval from the Institutional Review Board with approval No.: 517/IRB/2023. The IRB waived informed permission from the patients due to the retrospective nature of the study, which concentrated on the examination of patients’ medical records. The patients’ information was stored in a secure computerized database. Data were obtained solely with medical record numbers and preserved with Confidentiality. Consequently, the patients remain unidentifiable, and there are no ramifications for their health and wellbeing. The research adheres to the Declaration of Helsinki.
Acknowledgments
The Authors would like to thank the Institutional Review Board for their support and Mohammed Alshafie for his coordination.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. da Cunha Gomes EG, Machado LAF, de Oliveira LC, Neto JFN. The erythrocyte alloimmunisation in patients with sickle cell anaemia: a systematic review. Transfus Med. 2018;29(3):149. doi:10.1111/tme.12543
2. Ambrose EE, Smart LR, Charles M, et al. Surveillance for sickle cell disease, United Republic of Tanzania. Bull World Health Organ. 2020;98(12):859. doi:10.2471/blt.20.253583
3. Schmalzer EA, Chien S, Brown AK. Transfusion therapy in sickle cell disease. J Pediatr Hematol/Oncol. 1982;4(4):395. doi:10.1097/00043426-198224000-00007
4. Chelo D, Kessel F, Hamadou B, et al. Prevalence and factors associated with pulmonary arterial hypertension (PAH) in sickle cell children residing in Yaoundé, Cameroon. J Pediatr Neonatol. 2019;1(1). doi:10.33425/2689-1085.1005
5. Steinberg MH, Sebastiani P. Genetic modifiers of sickle cell disease. Am J Hematol. 2012;87(8):795–803. doi:10.1002/ajh.23232
6. Hyacinth HI, Adams RJ, Voeks JH, Hibbert JM, Gee BE. Frequent red cell transfusions reduced vascular endothelial activation and thrombogenicity in children with sickle cell anemia and high stroke risk. Am J Hematol. 2013;89:47. doi:10.1002/ajh.23586
7. Badawi MA, Adam S, Ghoneim A, et al. Clinical complications of hemoglobinopathies in Western Saudi Arabia and the need for specialized care centers. J King Abdulaziz Univ-Med Sci. 2019;26(1):29. doi:10.4197/med.26-1.5
8. Sakhalkar VS, Roberts K, Hawthorne LM, et al. Allosensitization in patients receiving multiple blood transfusions. Ann N Y Acad Sci. 2005;1054:495. doi:10.1196/annals.1345.072
9. Alboog A, Tayeb T, Alsager MO, et al. Red blood cell alloimmunization in sickle cell disease patients in Jeddah, Saudi Arabia: a pilot study. J King Abdulaziz Univ-Med Sci. 2015;22(3):34. doi:10.4197/med.22-3.5
10. Lasalle-Williams M, Nuss R, Le T, et al. Extended red blood cell antigen matching for transfusions in sickle cell disease: a review of a 14-year experience from a single center (CME). Transfusion. 2011;51:1732. doi:10.1111/j.1537-2995.2010.03045.x
11. Smart E, Armstrong B, Lee R. Blood group systems. ISBT Sci Ser. 2020;15:123. doi:10.1111/voxs.12593
12. Ristovska EC, Bojadjieva ТM, Velkova Е, et al. Rare blood groups in ABO, Rh, Kell systems – biological and clinical significance. PRILOZI. 2022;43(2):77. doi:10.2478/prilozi-2022-0021
13. Saboor M, Zehra A, Hamali HA, et al. Prevalence of A2 and A2B subgroups and Anti-A1 antibody in blood donors in Jazan, Saudi Arabia. Int J Gene Med. 2020;13:787. doi:10.2147/IJGM.S272698
14. Branch DR. Anti‐A and anti‐B: what are they and where do they come from? Transfusion. 2015;55:S74–S79. doi:10.1111/trf.13087
15. Halawani AJ, Arjan AH. ABO, RH, and KEL1 antigens, phenotypes and haplotypes in southwestern Saudi Arabia. Clin Lab. 2021;67. doi:10.7754/clin.lab.2020.200633
16. Omer NE. Frequency of the A2-subgroup among blood group A and blood group AB among students of Faculty of Medicine and Health Sciences at Alimam Almahadi University, White Nile, Sudan. Hematol Transfus Int J. 2015;1(4). doi:10.15406/htij.2015.01.00022
17. Cooling L. Blood groups in infection and host susceptibility. Clin Microbiol Rev. 2015;28(3):801. doi:10.1128/cmr.00109-14
18. Manga J, Mbeti M, Bénech C, et al. First investigation of RH gene polymorphism in patients with sickle cell disease and associated blood donors in Cameroon, Central Africa. Blood transfusion. 2024. doi:10.2450/bloodtransfus.660
19. Blumberg N, Ross K, Avila E, Peck K. Should chronic transfusions be matched for antigens other than ABO and Rho(D)? Vox Sang. 1984;47(3):205–208. doi:10.1111/j.1423-0410.1984.tb01587.x
20. Hindawi S, Badawi MA, El-Fayoumi RI, et al. The value of transfusion of phenotyped blood units for thalassemia and sickle cell anemia patients at an academic center. Transfusion. 2020;60: S15–S21. doi:10.1111/trf.15682
21. Meshi AA, Abu-Tawil H, Hamzi AA, et al. Red cell alloimmunisation among sickle cell disease and thalassemia patients following rh- and K-Matched red cell transfusion in southwestern Saudi Arabia: a multicenter study. Int J Gen Med. 2024;17:2855. doi:10.2147/ijgm.s444949
22. Al-Asmari B, Baothman A, Almohammadi M, Aljuaid M, Jastaniah W. Prevalence of red blood cell alloimmunization among pediatric patients with sickle cell disease in Saudi Arabia. J Pediatr Hematol/Oncol. 2024;46(5):e284–e289. doi:10.1097/mph.0000000000002889
23. Ameen R, Al Shemmari S, Al‐Bashir A. Red blood cell alloimmunization among sickle cell Kuwaiti Arab patients who received red blood cell transfusion. Transfusion. 2009;49:1649. doi:10.1111/j.1537-2995.2009.02185.x
24. Schonewille H, van de Watering LM, Loomans DS, Brand A. Red blood cell alloantibodies after transfusion: factors influencing incidence and specificity. Transfusion. 2006;46(2):250–256. doi:10.1111/j.1537-2995.2006.00708.x
25. Halawani AJ, Mobarki AA, Arjan AH, et al. Red cell alloimmunization and autoimmunization among sickle cell disease and Thalassemia patients in Jazan Province, Saudi Arabia. Int J Gene Med. 2022;Volume 15:4093. doi:10.2147/ijgm.s360320
26. Bashawri L. Red cell alloimmunization in sickle-cell anaemia patients. East Mediterr Health J. 2007;13(5):1181. doi:10.26719/2007.13.5.1181
27. Alkindi S, AlMahrooqi S, AlHinai S, et al. Alloimmunization in patients with sickle cell disease and thalassemia: experience of a single centre in Oman. Mediterranean J Hematol Infect Dis. 2017;9(1):e2017013. doi:10.4084/MJHID.2017.013
28. Adam S, Badawi M. Alloimmunisation and nephropathy in sickle cell disease patients in Jeddah, Saudi Arabia. Voxs. 2017;12:386–392. doi:10.1111/voxs.12362
29. Yazdanbakhsh K, Ware RE, Noizat-Pirenne F. Red blood cell alloimmunization in sickle cell disease: pathophysiology, risk factors, and transfusion management. Blood. 2012;120:528. doi:10.1182/blood-2011-11-327361
30. Pirenne F, Floch A, Diop S. Alloimmunisation against red blood cells in sickle cell disease: transfusion challenges in high-income and low-income countries. Lancet Haematol. 2023;10. doi:10.1016/s2352-3026(23)00066-2
31. Fasano RM, Meyer EK, Branscomb J, et al. Impact of red blood cell antigen matching on alloimmunization and transfusion complications in patients with sickle cell disease: a systematic review. Transfus Med Rev. 2019;33:12–23. doi:10.1016/j.tmrv.2018.07.003
32. Murao M, Viana MB. Risk factors for alloimmunization by patients with sickle cell disease. Braz J Med Biol Res. 2005;38(5):675. doi:10.1590/s0100-879x2005000500004
33. Samarah F, Srour MA, Yaseen D, Dumaidi K. Frequency of red blood cell alloimmunization in patients with sickle cell disease in Palestine. Adv Hematol. 2018;2018:5356245. doi:10.1155/2018/5356245
34. Yaseen A, Suleiman S, Zenah OA, Abu Taha A. Red blood-cell alloantibodies in multiply transfused patients in the occupied Palestinian territory: a pilot study. Lancet. 2018;391. doi:10.1016/s0140-6736(18)30370-2
35. Aykut S, Demir SC, Evruke IC, et al. Approach to pregnancy affected by kell alloimmunization. Case Rep Hematol. 2024;2024:1929147. doi:10.1155/2024/1929147
36. Makroo RN, Bhatia A, Gupta R, et al. Prevalence of Rh, Duffy, Kell, Kidd & MNSs blood group antigens in the Indian blood donor population. Indian J Med Res. 2013;137:521–526.
37. Makarovska-Bojadzieva T, Velkova E, Blagoevska M. The impact of extended typing on red blood cell alloimmunization in transfused patients. Open Access Maced J Med Sci. 2017;5:107. doi:10.3889/oamjms.2017.054
38. Nance S, Scharberg EA, Thornton N, Yahalom V, Sareneva I, Lomas-Francis C. International rare donor panels: a review. Vox Sang. 2015;110:209. doi:10.1111/vox.12357
39. Sarkar R, Philip J, Mallhi RS, Yadav P. Proportion of Rh phenotypes in voluntary blood donors. Med J Armed Forces India. 2013;69:330. doi:10.1016/j.mjafi.2013.05.004
40. Gundrajukuppam DK, Vijaya SB, Rajendran A, Sarella JD. Prevalence of principal rh blood group antigens in blood donors at the blood bank of a tertiary care hospital in southern India. J Clin Diagn Res. 2016;10. doi:10.7860/jcdr/2016/16621.7726
41. Castro O, Sandler SG, Houston-Yu P, Rana S. Predicting the effect of transfusing only phenotype-matched RBCs to patients with sickle cell disease: theoretical and practical implications. Transfusion. 2002;42:684. doi:10.1046/j.1537-2995.2002.00126.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Non-Traumatic Fat Embolism Syndrome in Two HbSS Sickle Cell Disease Patients: A Case Series and Review
Alzayer MA, Abohelaika S, Alhaddad M, Al Zayer M, Alali AJ, Al Abbas AM, Al Eid NJ, Al Saeed FA, Al Saeed HH
Journal of Blood Medicine 2025, 16:437-443
Published Date: 1 October 2025