Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Erythema Annulare Centrifugum On The Face
Authors Chen X ![]() , Yu Q, Chang D, Tang C
, Yu Q, Chang D, Tang C
Received 9 September 2025
Accepted for publication 2 December 2025
Published 7 February 2026 Volume 2026:19 565708
DOI https://doi.org/10.2147/CCID.S565708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Xinlong Chen, Qiao Yu, Degui Chang, Chenjian Tang
Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China
Correspondence: Chenjian Tang, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China, Email [email protected] Degui Chang, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China, Email [email protected]
Abstract: A 57-year-old female presented with recurrent erythema on the face and right upper limb for over 8 years, with exacerbation noted in the past 2 months. Skin biopsy revealed partial epidermal keratinization, mild acanthosis with slight spongiosis, and dermal perivascular lymphocytic infiltration, leading to a diagnosis of erythema annulare centrifugum. The patient was treated with topical tacrolimus ointment, resulting in significant improvement within one week. This case highlights the importance of recognizing the clinical features associated with this condition. Early identification and intervention can provide relief and improve the quality of life for patients suffering from this chronic dermatological issue.
Keywords: erythema, annulare, centrifugum
Introduction
Erythema annulare centrifugum (EAC) is a rare inflammatory dermatosis characterized by the appearance of annular erythematous lesions that expand centrifugally, often with central clearing. The etiology of EAC remains largely idiopathic, although it has been associated with various triggers, including infections, medications, and malignancies.1,2 The disease is divided into two clinical variants, superficial and deep, which have corresponding histopathological findings. Epidermal pathology, manifesting as a trailing scale, is characteristic of the superficial variant. In contrast, the deep variant is characterized by pathology in the mid and lower dermis, which produces non-scaly and more elevated lesions.3,4 The pathophysiological mechanisms underlying EAC involve immune-mediated responses, leading to localized inflammation and vascular changes in the skin. Clinically, patients may present with lesions that can persist for weeks to months, often causing significant discomfort and cosmetic concerns. Diagnosis is primarily based on clinical examination and histopathological findings, which typically reveal perivascular lymphocytic infiltrates and varying degrees of epidermal changes.
Case Presentation
A 57-year-old female presented with a complaint of recurrent erythema on the face, and right upper limb for over 8 years, with exacerbation noted over the past 2 months (Figure 1a and b). It recurs approximately once every 3 to 6 months. The physical examination revealed multiple centrifugal circular erythema on the patient’s skin, with clear edges and normal skin in the center. The erythema presented varying degrees of redness, and some areas were accompanied by mild desquamation. During the examination, the patient did not show any other skin lesions or systemic symptoms. Local palpation did not reveal any tenderness, and there was no enlargement of lymph nodes. Fungal smear, fungal fluorescence staining, and fungal culture tests were all negative. Skin pathology results revealed: focal incomplete keratinization of the epidermis, mild acanthosis of the stratum spinosum accompanied by slight edema, lymphocytic infiltration around superficial to mid-dermal small blood vessels (Figure 2a and b). Based on the characteristics of the patient’s skin lesions and pathological features, it is considered to be superficial centrifugal circular erythema. The patient was treated with topical tacrolimus ointment for one week, resulting in improvement of the condition (Figure 3).
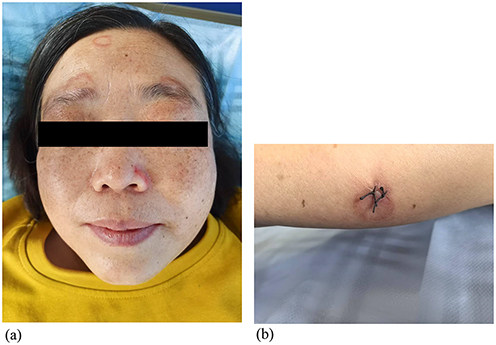 |
Figure 1 Clinical presentation of skin lesions (Before treatment). (a) Face, (b) limbs. |
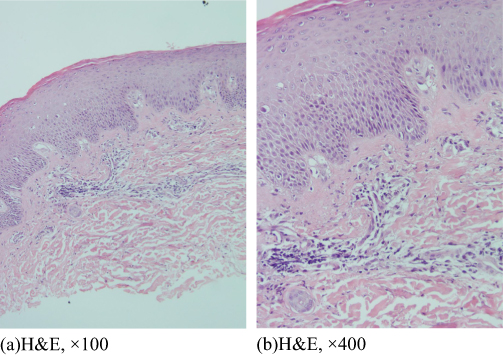 |
Figure 2 Histopathological examination. (a) HE staining at 100x magnification, (b) HE staining at 400x magnification. |
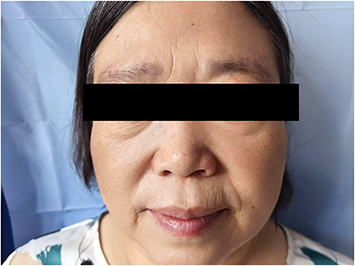 |
Figure 3 Clinical presentation of skin lesions (After treatment). |
Discussion
This case presents a 57-year-old female patient with a longstanding history of erythema on the face and right upper limb, which had exacerbated over the past two months. Based on the characteristics of the patient’s skin lesions and pathological features, it is considered to be superficial centrifugal circular erythema. The significance of this case lies in its rarity, as centrifugal annular erythema is not commonly diagnosed, especially in this demographic. The patient’s age and gender may influence the clinical presentation and progression of the condition, suggesting the need for heightened awareness among clinicians when encountering similar cases.
Although numerous studies have explored the characteristics and causes of EAC,5 in this case, the patient’s disease course lasted for 8 years and no potential triggers have been identified. There are reports in the relevant literature of EAC cases that persisted for many years without a clear cause. One study pointed out that a patient’s EAC lasted for 50 years without finding a trigger factor.6 Additionally, another study documented a female patient who experienced multiple recurrent episodes of EAC in the past two years, but the specific cause could not be determined either.7
Centrifugal annular erythema is characterized by annular, erythematous lesions that can often be misdiagnosed due to overlapping features with other dermatoses. The differential diagnosis of centrifugal annular erythema encompasses a range of conditions, including hypereosinophilic syndrome, where it may present as an initial manifestation;8 autoimmune disorders, such as systemic lupus erythematosus in infants associated with maternal autoimmune diseases;9 lymphoproliferative disorders such as mycosis fungoides, which can mimic this erythema clinically;10,11 Skin fungal infection12 and other variants like the Colcott-Fox type, often sporadic and associated with additional cutaneous findings.13
Studies have shown that the current main treatments include oral antibiotics or combined treatments with topical glucocorticoids and oral antihistamines. The recurrence rate of this condition is approximately 13.2%.5 Although topical glucocorticoid treatment was effective, since the patient’s skin lesions were on the face, we chose tacrolimus ointment for treatment. Histopathological findings indicate partial keratinization and superficial dermal lymphocytic infiltration, which correlates with the patient’s extended duration of symptoms.14 The connection between the prolonged erythema and the histological features supports the hypothesis that chronic inflammation contributes to the observed skin changes.
The treatment of this patient with tacrolimus ointment yielded significant improvement within one week, suggesting its efficacy as a therapy for centrifugal annular erythema. Tacrolimus is known to act as an immunomodulator, reducing inflammation by inhibiting T-lymphocyte activation and cytokine release. This mechanism is particularly beneficial in conditions characterized by inflammatory responses, including various forms of dermatitis and erythema.
Conclusion
In conclusion, this case is notable due to the patient’s age and the chronicity of her symptoms, highlighting the importance of considering EAC as a differential diagnosis in patients presenting with persistent erythematous lesions, particularly when accompanied by a history of prolonged skin changes.
Ethics Approval
The publication of case report does not require ethical approval. We confirm that no institutional approval was required for publishing the case details.
Informed Consent for Publication
The patient had signed informed consent and provided informed consent for the publication of the case details and any accompanying images.
Funding
Surface Project of Sichuan Provincial Administration of Traditional Chinese Medicine (25MSZX109).
Disclosure
Chenjian Tang is the main corresponding author for this study. The authors report no conflicts of interest in this work.
References
1. Ohmori S, Sugita K, Ikenouchi-Sugita A, Nakamura M. Erythema annulare centrifugum associated with herpes zoster. J UOEH. 2012;34(3):225–4. doi:10.7888/juoeh.34.225
2. Ena L, Mazzarello V, Ferrari M, Ena P. Recurrent erythema annulare centrifugum due to influenza type A. Case Rep Dermatol. 2021;13(1):134–140. doi:10.1159/000512869
3. Bolognia JL, Jorizzo JL, Schaffer JV. Chapter 19 Figurate ErythemasDermatology. Vol. 1. Elsevier Saunders; 2018:320–331.
4. McDaniel B, Cook C. Erythema Annulare Centrifugum. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
5. Geng RSQ, Sood S, Lee A, et al. Treatment outcomes in erythema annulare centrifugum: a systematic review. J Cutan Med Surg. 2024;28(6):607–609. doi:10.1177/12034754241287551
6. Mir A, Terushkin V, Fischer M, Meehan S. Erythema annulare centrifugum. Dermatol Online J. 2012;18(12):21. doi:10.5070/D31HS6V82M
7. Roy AK, Ghosh SK. Erythema annulare centrifugum. Indian J Dermatol Venereol Leprol. 1996;62(6):377–378.
8. Woscoff A, Dancziger E, Zamparo DI. Síndrome hipereosinofílico. Eritema anular centrífugo como manifestación inicial [Hypereosinophilic syndrome. Centrifugal annular erythema as an initial manifestation]. Med Cutan Ibero Lat Am. 1978;6(5–6):267–272.
9. Hammar H, Rönnerfält L. Annular erythemas in infants associated with autoimmune disorders in their mothers. Report on three cases. Dermatologica. 1977;154(2):115–127.
10. Saada D, Lami MC, Vabres P, Levillain P, Guillet G. Mycosis fongoïde à type d’érythème annulaire centrifuge [Mycosis fungoides presenting as annular erythema]. Ann Dermatol Venereol. 2005;132(1):35–37. doi:10.1016/S0151-9638(05)79193-6
11. Moura FN, Thomas L, Balme B, Dalle S. Mycosis fungoides mimicking an annular erythema. Clin Exp Dermatol. 2009;34(8):e581–e583. doi:10.1111/j.1365-2230.2009.03249.x
12. Gunaydin SD, Arikan-Akdagli S, Akova M. Fungal infections of the skin and soft tissue. Curr Opin Infect Dis. 2020;33(2):130–136. doi:10.1097/QCO.0000000000000630
13. Larrègue M, Beuve-Mery M, Dupuy M, Tremoulet-Labarthe O, Bressieux JM. Erythème annulaire centrifuge type Colcott-Fox (erythema gyratum perstans) [Centrifugal annular erythema of Colcott Fox type (erythema gyratum perstans)]. Ann Pediatr. 1977;24(11):763–769.
14. Erduran F. Evaluation of clinicopathological features and associated conditions in erythema annulare centrifugum: a retrospective observational analysis of 63 patients. Dermatol Pract Concept. 2024;14(1):e2024039. doi:10.5826/dpc.1401a39
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.