Back to Journals » Journal of Asthma and Allergy » Volume 19
Eosinophilic Gastroenteritis with Atopic Dermatitis: A Case Report and Literature Review
Authors Song H ![]() , Li J, Tang Y, Li X, Li Y, Yang R, Zhuan B, Wang H
, Li J, Tang Y, Li X, Li Y, Yang R, Zhuan B, Wang H ![]()
Received 3 December 2025
Accepted for publication 11 February 2026
Published 20 February 2026 Volume 2026:19 586212
DOI https://doi.org/10.2147/JAA.S586212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Hongbin Song,1 Jing Li,2 Yuanyuan Tang,3 Xianghua Li,1 Yunfeng Li,1 Rui Yang,1 Bing Zhuan,4 Hongtian Wang5
1Department of Dermatology, People’s Hospital of Ningxia Hui Autonomous Region, Ningxia Medical University, Ningxia Clinical Research Institute, Yinchuan, 750002, People’s Republic of China; 2Department of Pathology, People’s Hospital of Ningxia Hui Autonomous Region, Ningxia Medical University, Ningxia Clinical Research Institute, Yinchuan, 750002, People’s Republic of China; 3Department of Gastroenterology, People’s Hospital of Ningxia Hui Autonomous Region, Ningxia Medical University, Ningxia Clinical Research Institute, Yinchuan, 750002, People’s Republic of China; 4Department of Respiratory and Critical Care Medicine, People’s Hospital of Ningxia Hui Autonomous Region, Ningxia Medical University, Ningxia Clinical Research Institute, Yinchuan, 750002, People’s Republic of China; 5Department of Allergy, Beijing Shijitan Hospital, Capital Medical University, Beijing, 100038, People’s Republic of China
Correspondence: Bing Zhuan, Department of Respiratory and Critical Care Medicine, People’s Hospital of Ningxia Hui Autonomous Region, Ningxia Medical University, Ningxia Clinical Research Institute, Yinchuan, 750002, People’s Republic of China, Tel +86 187 0951 8179, Email [email protected] Hongtian Wang, Department of Allergy, Beijing Shijitan Hospital, Capital Medical University, Beijing, 100038, People’s Republic of China, Tel +86 133 9183 6668, Email [email protected]
Abstract: The coexistence of atopic dermatitis and eosinophilic gastroenteritis represents an uncommon clinical phenotype that is often underrecognized, resulting in delayed diagnosis and suboptimal treatment. This report aims to delineate the clinical characteristics of such cases and highlight recent developments in diagnostic and therapeutic approaches, thereby supporting improved clinical decision-making. A 50-year-old man presented with widespread atopic dermatitis-like cutaneous lesions and recurrent gastrointestinal symptoms consistent with eosinophilic gastroenteritis. Symptom exacerbation exhibited seasonal variation, particularly during spring and autumn. Laboratory investigations revealed elevated eosinophil percentages and absolute counts, as well as increased total serum IgE and positive specific IgE to allergens. Histopathological examination of gastroscopy and colonoscopy biopsy specimens demonstrated marked eosinophilic infiltration of the gastrointestinal mucosa, confirming the diagnosis of eosinophilic gastroenteritis accompanied by atopic dermatitis. Although oral antihistamines provided temporary symptomatic relief, clinical symptoms recurred after medication withdrawal. Atopic dermatitis and eosinophilic gastroenteritis appear to share a common allergen-driven pathogenesis. Accurate identification of causative allergens, in conjunction with the assessment of serum IgE levels and eosinophil counts, is critical for effective diagnosis and management. Therapeutic interventions targeting allergic inflammation have demonstrated efficacy in addressing both conditions.
Keywords: gastroenteritis, eosinophils, atopic dermatitis, corticosteroid, abdominal distension
Introduction
Eosinophilic gastroenteritis (EGE) is a rare inflammatory disorder of the gastrointestinal tract that affects both pediatric and adult populations. It is histologically defined by eosinophilic infiltration of the esophagus, stomach, and intestines, and has been increasingly recognized in recent literature despite its low clinical prevalence.1 Despite increasing awareness, true prevalence is likely underestimated due to the nonspecific symptomatology and the often segmental, patchy nature of eosinophilic infiltration that can be missed during routine endoscopy. Epidemiological data from Western countries estimate a prevalence of approximately 5 to 8 cases per 100,000 individuals.2
Atopic diseases can often co-exist. Studies show more than 50% of individuals diagnosed with EGE have concomitant atopic disorders, including allergic asthma, food allergies, atopic dermatitis (AD), and allergic rhinitis.1,3 EGE and other atopic disorders are driven by similar inflammatory molecular mechanisms and exist along the same atopic disease spectrum.4 In this report, we present a case of AD associated with EGE. The patient demonstrated improvement following low-dose corticosteroid treatment, suggesting that AD and EGE share a common pathogenesis, predominantly driven by a Th2 inflammatory response. This study adheres to the Declaration of Helsinki of 1975. Approval for publishing this article has been obtained from the People’s Hospital of Ningxia Hui Autonomous Region.
Case Presentation
A 50-year-old man presented to the dermatology outpatient clinic with erythema and papules localized to the trunk and proximal extremities, with a symptom duration of four months and recurrence noted over the preceding two weeks. The initial onset was characterized by the appearance of scattered, erythematous, rice-grain-sized papules on the abdomen, occurring without a clear precipitating factor and accompanied by minimal pruritus or discomfort. Over time, the lesions gradually extended to involve the trunk and proximal limbs. The patient’s medical history was notable for allergic rhinitis and allergic asthma, both of which had persisted for over six years. From June 2023 to June 2024, he was maintained on inhaled budesonide-formoterol in combination with oral antihistamines and leukotriene receptor antagonists. While symptomatic control was achieved during treatment, recurrence of symptoms was consistently observed upon discontinuation of medication.
Physical examination revealed no abnormalities in the cardiopulmonary or abdominal systems. Dermatologic evaluation identified scattered erythematous papules, approximately the size of rice grains, on the trunk and proximal extremities, with no evidence of erosion, exudation, or desquamation. Further history-taking revealed the onset of unexplained abdominal distension and pain approximately three days prior to the development of cutaneous symptoms. A complete blood count performed at a local facility demonstrated an elevated eosinophil percentage of 14.7% and an absolute eosinophil count of 0.94 x 109/L. Based on these findings, the patient was referred and subsequently admitted to the Department of Gastroenterology for further evaluation. Serological testing revealed a total serum IgE concentration above 100 IU/mL (reference range: 0–100 IU/mL), while allergen-specific IgE assays were negative for common aeroallergens, including dust mites and pollen.
The patient underwent both gastroscopy and colonoscopy, during which mucosal biopsies were obtained. Gastroscopic findings revealed chronic non-atrophic gastritis with erosion, as well as evidence of duodenitis (Figure 1A and B). Colonoscopy demonstrated multiple submucosal protrusions within the transverse colon and mucosal erosions in the descending colon (Figure 1C and D). Histopathological analysis of the gastric mucosal biopsy showed mild chronic inflammation in the gastric body with scattered eosinophilic infiltration within the lamina propria; staining for Helicobacter pylori (HP) was negative (Figure 2A). Additionally, the duodenal bulb and descending portion of the duodenum exhibited chronic active inflammation characterized by marked eosinophilic infiltration of the lamina propria, with counts exceeding 20 eosinophils per high-power field (Figure 2B and C). This degree of eosinophilic infiltration surpasses the commonly accepted regional thresholds—often >15 eosinophils/HPF in the stomach and >20 eosinophils/HPF in the small intestine—thereby supporting the histopathological diagnosis of eosinophilic gastroenteritis. Colonic biopsies further demonstrated (Figure 2D): chronic inflammation of the terminal ileal mucosa with substantial eosinophilic infiltration of the lamina propria (>20 eosinophils per high-power field) and chronic inflammation of the descending colonic mucosa.
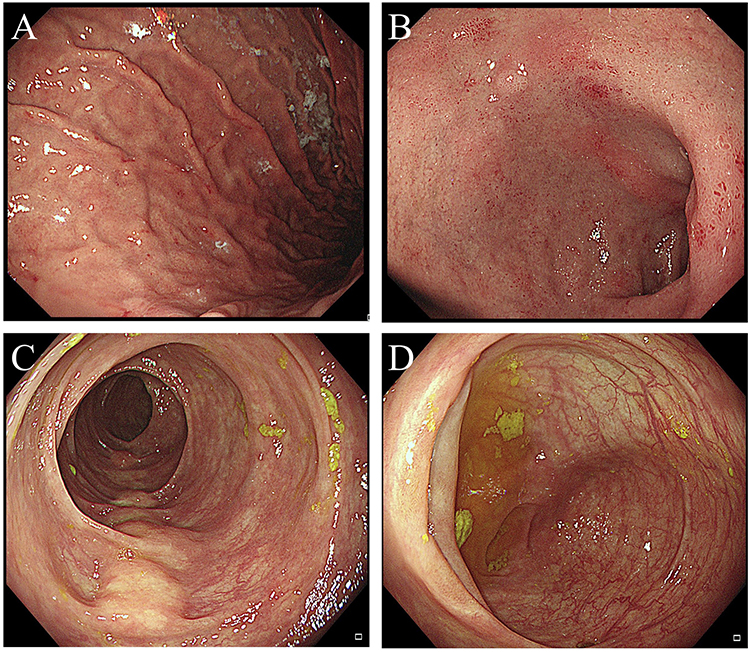 |
Figure 1 Endoscopic findings from gastroscopy and colonoscopy. (A) Chronic non-atrophic gastritis with erosion. (B) Duodenitis. (C) Multiple submucosal elevations in the transverse colon. (D) Erosion in the descending colon. |
 |
Figure 2 Histopathologic findings from gastroscopic and colonoscopic biopsies (×20 magnification). (A) Mild chronic inflammation of the gastric mucosa with scattered eosinophilic infiltration in the lamina propria; Helicobacter pylori negative. (B and C) Chronic active inflammation in the mucosa of the duodenal bulb and descending duodenum, with prominent eosinophilic infiltration of the lamina propria (>20 eosinophils per high-power field (HPF)). (D) Chronic inflammation of the terminal ileum, with a large number of eosinophils infiltrated in the lamina propria (>20 eosinophils per HPF). It is important to note that the yellow arrows highlight the eosinophils present in both gastroscopic and colonoscopic biopsies. |
Based on the endoscopic and histopathological findings, a diagnosis of eosinophilic gastroenteritis was established. The patient was initiated on oral prednisone acetate at a dose of 40 mg daily. Following treatment, there was significant improvement in gastrointestinal symptoms, including abdominal distension and pain, as well as in cutaneous manifestations consistent with atopic dermatitis. The patient was subsequently discharged. The intended tapering plan aimed to gradually reduce the corticosteroid dose over several weeks; however, due to patient nonadherence, the course was prematurely altered, possibly contributing to symptom relapse and eosinophil rebound.
Approximately two weeks prior to readmission, the rash on the trunk and limbs recurred and progressively worsened. Repeat laboratory testing at a local hospital revealed a further elevation in eosinophil levels, with an eosinophil percentage of 20% and an absolute count of 1.1 × 109/L. To strengthen diagnostic accuracy, parasitic infections were ruled out via negative stool ova and parasite examinations, and peripheral smear findings were unremarkable, excluding hematologic causes of eosinophilia. The patient self-administered eight tablets of prednisone acetate daily, which corresponded to an estimated total of 40 mg daily, aligning with the previously effective dosage, but without notable improvement, prompting return to the hospital for further evaluation.
The final diagnosis was AD accompanied by EGE. A skin biopsy was recommended to assess eosinophilic infiltration of the dermal tissue; however, the patient declined the procedure. Management was continued with oral prednisone acetate (eight tablets daily) in conjunction with topical application of hydrocortisone butyrate cream. The patient remains under active outpatient follow-up.
Discussion
Eosinophilic gastrointestinal disorders (EGID) represent a spectrum of conditions marked by pathological eosinophilic infiltration in the esophagus, stomach, small intestine, or colon, resulting in organ dysfunction and associated clinical symptoms.5 This group encompasses eosinophilic esophagitis (EoE), eosinophilic gastritis (EG), eosinophilic gastroenteritis (EGE), eosinophilic enteritis (EE), and eosinophilic colitis (EC).3 Notably, EoE is the most prevalent EGID, affecting 0.5–1 per 1000 individuals in the general population.6 In contrast, the prevalence of other conditions, such as EGE, is relatively low.
The typical age of EGE onset ranges from 30 and 50 years, with no significant sex predilection; however, some studies suggest a slightly higher prevalence among women.7 The current case involves a 50-year-old man, aligning with the established age range.
In 1990, Talley et al8 proposed widely accepted diagnostic criteria for EGE, which require the presence of gastrointestinal symptoms and histologically confirmed eosinophilic infiltration in one or more segments of the gastrointestinal tract, in the absence of parasitic infection or other systemic eosinophilic diseases. Therefore, histopathological confirmation via endoscopic biopsy remains essential for diagnosis. However, delayed access to endoscopy or the omission of biopsy and tissue analysis can result in significant diagnostic delays. Previous studies have reported an average diagnostic delay of 3.6 years following symptom onset,9 and data from the US Food and Drug Administration in 2021 suggest that delays may extend to 4–9 years in some cases.10 In addition to endoscopic evaluation, non-invasive diagnostic strategies have gained interest. These include fecal eosinophil quantification and assessment of biomarkers such as eosinophil cationic protein (ECP), total serum IgE, and allergen-specific IgE levels. However, fecal ECP levels are not yet standardized for routine clinical use, and variability in assay methods currently limits their diagnostic reliability. Elevated concentrations of total and specific IgE are commonly observed and support the hypothesis that allergen exposure plays a central role in the pathogenesis of both EGE and atopic dermatitis.
From an immunopathological perspective, EGE is considered a type I hypersensitivity disorder driven predominantly by a Th2 inflammatory response. Interleukins IL-4, IL-5, and IL-13 are central to disease progression. IL-4 and IL-5 promote the differentiation and recruitment of Th2 cells, while IL-13 contributes to allergic inflammation through the upregulation of eosinophil chemokine-3 and vascular cell adhesion molecules. Both TSLP and IL-33 have also been shown to drive Th2-mediated inflammation in atopic dermatitis, supporting their role as key upstream mediators in allergic multimorbidity. Shoda et al11 have identified thymic stromal lymphopoietin (TSLP) and IL-33 as important cytokines involved in allergic conditions associated with EGE.
More than half of the patients diagnosed with EGE have a history of allergic diseases, including asthma, eczema, or rhinitis. This observation indicates a potential atopic predisposition in the pathogenesis of EGE.12,13 Cha et al14 were the first to report a case of EGE associated with eosinophilic dermatitis in 2010. The patient, a 24-year-old woman, presented with acute right lower quadrant abdominal pain and was initially diagnosed with acute appendicitis, leading to laparoscopic appendectomy. Intraoperative findings, however, did not confirm suppurative appendicitis. Postoperatively, the patient developed persistent and progressive eosinophilia, eosinophilic ascites, and histological evidence of eosinophilic infiltration in the appendiceal wall, gastric mucosa, and duodenal mucosa. A concurrent abdominal skin biopsy revealed marked eosinophilic infiltration, which improved following administration of low-dose corticosteroid treatment. Chen et al15 evaluated the association between AD and EoE among participants in the All of Us Research Program. They found that individuals with AD were significantly more likely to be diagnosed with EoE compared to those without AD (0.8% vs 0.3%, p < 0.001). After controlling for age, sex, ethnicity, race, food allergy, asthma, and allergic rhinitis, the adjusted odds ratio for EoE in individuals with AD was 1.82 (95% confidence interval [CI] 1.42–2.30, p < 0.011). This evidence supports the theory that EoE is a later manifestation of the atopic march, a stereotypical progression of allergic diseases that begins with AD and is followed by food allergies, asthma, and allergic rhinitis.16 Both EoE and AD are characterized by T2 inflammation and a compromised epithelial barrier. Recent studies have demonstrated that EoE and AD share a common set of disease-specific ribonucleic acid transcripts, particularly centered around the IL-13 pathway.
While spontaneous remission may occur in approximately 30% to 40% of EGE cases over the short term, the majority of patients require long-term treatment.1 Currently, there is no universally accepted treatment algorithm. Management strategies primarily include: environmental interventions aimed at minimizing allergen exposure and implementing elimination diets to exclude suspected food allergens; and allergen-specific immunotherapy, which remains the only etiologically targeted intervention. First-line pharmacologic therapies consist of oral antihistamines, leukotriene receptor antagonists such as montelukast, mast cell stabilizers including cromolyn sodium, ketotifen, and selective Th2 cytokine inhibitors (eg, IL-4 and IL-5 inhibitors such as mepolizumab).17 However, the role of allergens in the etiology of EGE remains incompletely understood, and the clinical application of allergen detection is limited. Nevertheless, in pediatric and select adult cases, dietary antigen avoidance based on empirical or allergy-directed elimination strategies has been associated with symptomatic and histologic remission, suggesting that allergen-driven mechanisms are relevant in some phenotypes. As such, systemic glucocorticoids continue to represent the cornerstone of treatment. In the present case, the patient responded favorably to initial oral corticosteroid therapy. However, recurrence of symptoms, including rash and elevated peripheral eosinophil levels, was observed following cessation of treatment. This highlights the need for further investigation into the efficacy and long-term safety of corticosteroid reinitiation in patients with recurrent EGE.
Recent advances in biologic therapies have introduced novel options for managing eosinophilic and allergic diseases. Omalizumab, a recombinant humanized IgG1 monoclonal antibody, selectively binds to circulating and membrane-bound IgE, thereby blocking its interaction with FcεRI and CD23. It also downregulates FcεRI expression on antigen-presenting cells and inhibits mast cell and basophil activation.18 Omalizumab has been approved for the treatment of severe allergic asthma and chronic urticaria and has shown efficacy in several other IgE-mediated conditions, including seasonal and perennial allergic rhinitis, peanut and latex allergies, atopic dermatitis, idiopathic allergic reactions, mastocytosis, eosinophilic gastroenteritis, and nasal polyposis.19 Han et al20 reported successful management of severe asthma associated with EGE using a combination of omalizumab and mepolizumab. Although omalizumab has demonstrated efficacy in isolated case reports and small case series, its use in EGE remains off-label and requires further validation in controlled trials to determine appropriate indications, dosing, and long-term safety. In the current case, the patient’s elevated total serum IgE prior to treatment—and the subsequent relapse following corticosteroid withdrawal—suggest that anti-IgE therapy may be a viable alternative. Consideration of biologic agents such as omalizumab could be warranted in future treatment planning.
Dupilumab, a monoclonal antibody targeting the IL-4/13 receptor, has been utilized in the treatment of atopic diseases, including severe asthma and moderate-to-severe atopic dermatitis. Recent studies have highlighted the efficacy of dupilumab in treating EoE,21 and it is anticipated to be beneficial for non-EoE EGIDs as well.22 Tsuge et al23 reported a pediatric case of egg-induced EGE accompanied by a duodenal ulcer, where the administration of dupilumab resulted in ulcer healing, resolution of eosinophilic infiltration, cessation of systemic steroid therapy, and the development of egg tolerance. Given that EGE is a rare condition, further large-scale longitudinal cohort studies are necessary to validate the efficacy of dupilumab.
In conclusion, EGE is an uncommon and heterogeneous gastrointestinal disorder with a complex immunopathology that often contributes to diagnostic challenges. The coexistence of EGE with allergic diseases, such as AD, suggests that EGE may represent a later manifestation of the atopic march. Continuous advancements in diagnostic modalities and targeted therapies offer promising avenues for improving outcomes and deepening the understanding of its pathogenesis and management.
Generative AI Statement
The authors declare that no generative AI was used in the creation of this manuscript.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the first author, Hongbin Song, without undue reservation.
Ethics Statement
As this study constitutes a single case report, ethics committee approval was not necessary. Approval for the publication of this article has been secured from the People’s Hospital of Ningxia Hui Autonomous Region. The participant provided written informed consent to participate in this study. Additionally, written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Acknowledgments
We thank Phoebe Chi, MD, from Liwen Bianji (Edanz) (www.liwenbianji.cn), for editing a draft of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Open Research Fund of Ningxia Clinical Research Institute, People’s Hospital of Ningxia Hui Autonomous Region (2024KF09), and Key R&D Program Talent Introduction Special Project of Ningxia Hui Autonomous Region (2024BEH04005).
Disclosure
The authors declare no competing interests in this work.
References
1. Sunkara T, Rawla P, Yarlagadda KS, Gaduputi V. Eosinophilic gastroenteritis: diagnosis and clinical perspectives. Clin Exp Gastroenterol. 2019;12:239–7. doi:10.2147/CEG.S173130
2. Mansoor E, Saleh MA, Cooper GS. Prevalence of eosinophilic gastroenteritis and colitis in a population-based study, from 2012 to 2017. Clin Gastroenterol Hepatol. 2017;15(11):1733–1741. doi:10.1016/j.cgh.2017.05.050
3. Gonsalves N. Eosinophilic gastrointestinal disorders. Clin Rev Allergy Immunol. 2019;57(2):272–285. doi:10.1007/s12016-019-08732-1
4. Sindher SB, Barshow S, Tirumalasetty J, et al. The role of biologics in pediatric food allergy and eosinophilic gastrointestinal disorders. J Allergy Clin Immunol. 2023;151(3):595–606. doi:10.1016/j.jaci.2023.01.007
5. Spergel JM, Book WM, Mays E, et al. Variation in prevalence, diagnostic criteria, and initial management options for eosinophilic gastrointestinal diseases in the United States. J Pediatr Gastroenterol Nutr. 2011;52(3):300–306. doi:10.1097/MPG.0b013e3181eb5a9f
6. Lam AY, Lee JK, Coward S, et al. Epidemiologic burden and projections for eosinophilic esophagitis-associated emergency department visits in the United States: 2009–2030. Clin Gastroenterol Hepatol. 2023;21(12):3041–50.e3. doi:10.1016/j.cgh.2023.04.028
7. Kinoshita Y, Ishihara S. Eosinophilic gastroenteritis: epidemiology, diagnosis, and treatment. Curr Opin Allergy Clin Immunol. 2020;20(3):311–315. doi:10.1097/ACI.0000000000000635
8. Talley NJ, Shorter RG, Phillips SF, Zinsmeister AR. Eosinophilic gastroenteritis: a clinicopathological study of patients with disease of the mucosa, muscle layer, and subserosal tissues. Gut. 1990;31(1):54–58. doi:10.1136/gut.31.1.54
9. Chehade M, Kamboj AP, Atkins D, Gehman LT. Diagnostic delay in patients with eosinophilic gastritis and/or duodenitis: a population-based study. J Allergy Clin Immunol Pract. 2021;9(5):2050–9.e20. doi:10.1016/j.jaip.2020.12.054
10. Rothenberg ME, Hottinger SKB, Gonsalves N, et al. Impressions and aspirations from the FDA GREAT VI workshop on eosinophilic gastrointestinal disorders beyond eosinophilic esophagitis and perspectives for progress in the field. J Allergy Clin Immunol. 2022;149(3):844–853. doi:10.1016/j.jaci.2021.12.768
11. Shoda T, Matsuda A, Arai K, et al. Sera of patients with infantile eosinophilic gastroenteritis showed a specific increase in both thymic stromal lymphopoietin and IL-33 levels. J Allergy Clin Immunol. 2016;138(1):299–303. doi:10.1016/j.jaci.2015.11.042
12. Yun MY, Cho YU, Park IS, et al. Eosinophilic gastroenteritis presenting as small bowel obstruction: a case report and review of the literature. World J Gastroenterol. 2007;13(11):1758–1760. doi:10.3748/wjg.v13.i11.1758
13. Caldwell JH, Tennenbaum JI, Bronstein HA. Serum IgE in eosinophilic gastroenteritis. Response to intestinal challenge in two cases. N Engl J Med. 1975;292(26):1388–1390. doi:10.1056/NEJM197506262922608
14. Cha JM, Lee JI, Joo KR, Shin HP. Eosinophilic gastroenteritis with eosinophilic dermatitis. Yonsei Med J. 2010;51(1):145–147. doi:10.3349/ymj.2010.51.1.145
15. Chen GF, Cohen JM. Association between atopic dermatitis and eosinophilic esophagitis: a cross-sectional study in the all of us research program. Int J Dermatol. 2023;62(10):e556–7. doi:10.1111/ijd.16690
16. Silverberg JI. Comorbidities and the impact of atopic dermatitis. Ann Allergy Asthma Immunol. 2019;123(2):144–151. doi:10.1016/j.anai.2019.04.020
17. El-Alali EA, Abukhiran IM, Alhmoud TZ. Successful use of montelukast in eosinophilic gastroenteritis: a case report and a literature review. BMC Gastroenterol. 2021;21(1):279. doi:10.1186/s12876-021-01854-x
18. Foster B, Foroughi S, Yin Y, Prussin C. Effect of anti-IgE therapy on food allergen specific T cell responses in eosinophil associated gastrointestinal disorders. Clin Mol Allergy. 2011;9(1):7. doi:10.1186/1476-7961-9-7
19. Babu KS, Polosa R, Morjaria JB. Anti-IgE--emerging opportunities for Omalizumab. Expert Opin Biol Ther. 2013;13(5):765–777. doi:10.1517/14712598.2013.782391
20. Han D, Lee JK. Severe asthma with eosinophilic gastroenteritis effectively managed by mepolizumab and omalizumab. Ann Allergy Asthma Immunol. 2018;121(6):742–743. doi:10.1016/j.anai.2018.07.030
21. Dellon ES, Rothenberg ME, Collins MH, et al. Dupilumab in adults and adolescents with eosinophilic esophagitis. N Engl J Med. 2022;387(25):2317–2330. doi:10.1056/NEJMoa2205982
22. Dellon ES, Spergel JM. Biologics in eosinophilic gastrointestinal diseases. Ann Allergy Asthma Immunol. 2023;130(1):21–27. doi:10.1016/j.anai.2022.06.015
23. Tsuge M, Shigehara K, Uda K, et al. Successful use of dupilumab for egg-induced eosinophilic gastroenteritis with duodenal ulcer: a pediatric case report and review of literature. Allergy Asthma Clin Immunol. 2023;19(1):103. doi:10.1186/s13223-023-00859-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dupilumab Treatment Efficacy and Impact on Clinical Scores, Serum Biomarkers, and Itch in Adult Patients with Atopic Dermatitis: A Retrospective Analysis
Rossi M, Bettolini L, Artelli GL, Fraghì A, Tomasi C, Calzavara-Pinton P
Journal of Asthma and Allergy 2023, 16:1233-1240
Published Date: 9 November 2023
Clinical Profile of Elderly Atopic Dermatitis in China
Wu M, Li F, Xu G, Chen X, Zhang Y, Yao X
Clinical, Cosmetic and Investigational Dermatology 2026, 19:569869
Published Date: 8 January 2026