Back to Journals » Clinical and Experimental Gastroenterology » Volume 12
Eosinophilic esophagitis: early diagnosis is the key
Authors Muir AB, Brown-Whitehorn T, Godwin B, Cianferoni A ![]()
Received 3 April 2019
Accepted for publication 9 July 2019
Published 15 August 2019 Volume 2019:12 Pages 391—399
DOI https://doi.org/10.2147/CEG.S175061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Wing-Kin Syn
Amanda B Muir,1 Terri Brown-Whitehorn,2 Bridget Godwin,1 Antonella Cianferoni1
1Gastroenterology Division, The Children’s Hospital of Philadelphia, Philadelphia, PA, USA; 2Allergy Division, The Children’s Hospital of Philadelphia, Philadelphia, PA, USA
Correspondence: Antonella Cianferoni
Gastroenterology Division, The Children’s Hospital of Philadelphia, ARC1216G, 3615 Civic Center Boulevard, Philadelphia, PA 19104, USA
Tel +1 267 294 1952
Email [email protected]
Abstract: Eosinophilic esophagitis (EoE) is a disorder which affects all ages, from infancy through adulthood. It typically affects atopic individuals (Table 1) and is a chronic allergic disorder, with foods ubiquitous in the diet being the most described trigger of this isolated eosinophilic inflammation of the esophagus in both adults and children. This inflammatory process leads to esophageal symptoms such as dysphagia and feeding intolerance. In this review, we provide a brief overview of the current state of EoE therapy and symptomatology and then try to make the case for early diagnosis and treatment to prevent some of the long-term consequences of esophageal inflammation.
Keywords: eosinophilic esophagitis, early, diagnosis, stenosis, pain
Background
Foods were originally shown to be the causative agents in EoE through the use of elimination diets or elemental formulas.1 Elemental diets, with amino acid-based formulas, have demonstrated resolution of symptoms and normalization of biopsies in >95% of pediatric and adult patients.1,2 Because of the poor palatability of elemental formulas, elimination diets based on skin prick tests (SPTs) and atopy patch tests (APTs)3 or removal of the most common food allergens4 have been tried. Empiric food elimination diet without 1–6 of the most common food allergens (milk, wheat, egg, soy, fish/shellfish, and peanut/nuts) has been shown to be more effective than the ones driven by testing, due to poor specificity and sensitivity of SPTs and APTs in the diagnosis of food triggers in EoE.5,6 Therefore, empiric diets are the ones that are most commonly used. Their efficacy rate is however significantly different depending on the studies, varying from 30% to 70%. Unfortunately the most effective empiric diet are the one eliminating more foods and therefore more difficult to follow.5,6 Six-food elimination diets which eliminate milk, wheat, soy, egg, peanut/nuts, and seafood are effective in 70–80% of patients; 4- and 2 food elimination diets that eliminate milk, wheat, soy, and egg or only milk and wheat, respectively, are effective in 50–60% of patients and milk elimination alone has been shown to be effective in 30–60% of patients.5,6 Food allergens trigger EoE largely independent of IgE as demonstrated by the inability of measurement of IgE to predict food triggers,5,6 the failure of Omalizumab in the treatment of EoE {Clayton, 2014 #7121}, and the fact the animal model deprived of IgE can still develop EoE {Simon, 2016 #7726}.7,8
Based on the latest consensus guidelines, there are three accepted treatments of EoE: use of proton pump inhibitor (PPI), steroids, and diet elimination.9 The success rate of PPI as first-line therapy is about 20–50%. Given safety profile PPI are chosen often as first-line therapy. In case of failure, diet therapy or steroids can be initiated.10,11 Overall, the advantages of the diet treatment compared to swallowed steroid are to achieve the remission of the disease without using drugs. Oral steroids, as in all atopic diseases, are very effective in controlling inflammation and symptoms in EoE. In EoE, topical swallowed corticosteroids are indeed effective in inducing EoE remission in 50–90%, with most of the studies showing 70–80% efficacy and allowing most patients to stay on a relatively unlimited diet.12,13 No formulation of topical steroids is FDA approved in the US for EoE and only one formulation (oral budesonide) is specifically approved for EoE in Europe. Therefore, most of the available studies are based on the off-label use for EoE for asthma inhaled steroids: fluticasone or budesonide.
Symptoms vary per age and seem to progress from an inflammatory to a fibro stenotic phenotype (Tables 2).14–16 Infants and toddlers present with gastroesophageal reflux, vomiting, growth and feeding concerns, and irritability. Older school-age children also have reflux but will complain of abdominal pain and heartburn, while teenagers and adults present most often with dysphagia, food impaction, and heartburn. Diagnosis of EoE is not always straightforward and clinicians need to consider EoE in the differential diagnosis in many clinical presentations. Symptoms often overlap with other condition and may occur concomitantly. Other times, symptoms are more sporadic, leading patients to seek care only if symptoms worsen or become more persistent. Patients may not appear to have a feeding/eating disorders, as only 20% of patients present with failure to thrive (mostly in younger patients). In fact, the majority are either normal weight or, at times, obese. Clinicians, therefore, need to be sure to ask the right questions (and in younger children, ask them directly as well), based on risk factors and clinical suspicion (Table 3). Indeed, many patients may compensate for their symptoms by eating slowly, cutting foods into small bites, or drinking increased fluids with meals, and because symptoms become worse slowly over time patients may not even be aware of those strategies unless asked directly by the physician.
 |
Table 1 Atopy as a risk factor for eosinophilic esophagitis |
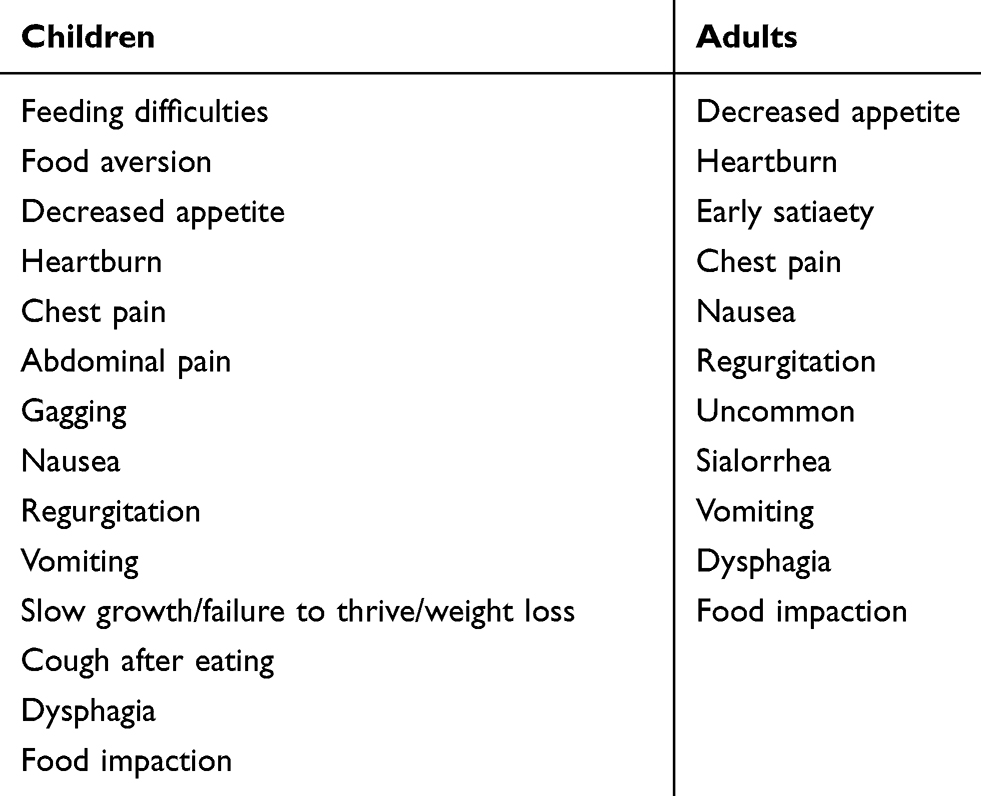 |
Table 2 Symptoms of EoE in children and adults |
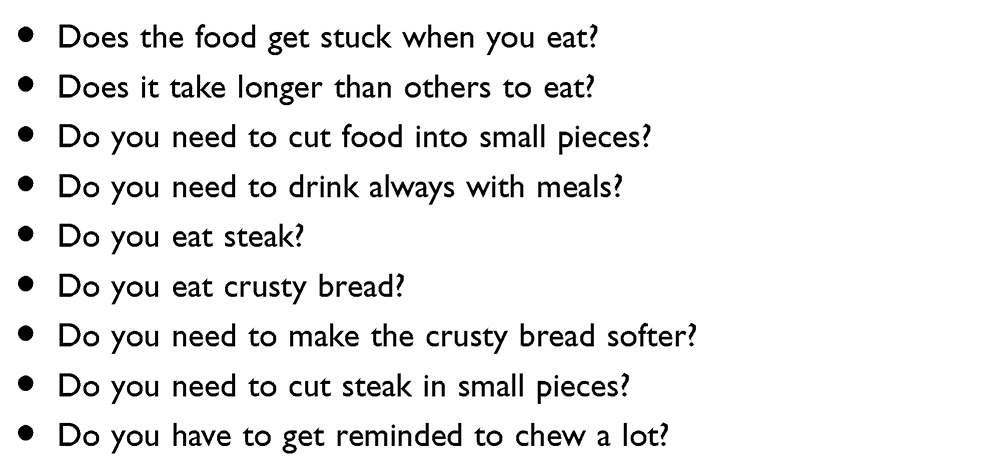 |
Table 3 Questions to ask to elicit symptoms of EoE |
Particularly challenging are those patients with asymptomatic eosinophilia of the esophagus, who are increasingly reported in the literature. Although they can be the ideal patients to treat before fibrosis and symptoms develop, long-term studies are lacking and decision needs to be taken by the clinician on a patient by patient basis based on risk factors comorbidities, etc.20–23
The diagnosis is not easy to achieve, and symptoms are often aspecific, underrecognized by patients and physicians, and the only way to confirm clinical suspicion is to obtain an endoscopy and biopsy, a procedure that either patient, family, or clinician may be hesitant to perform or may not be readily available.24 Therefore, it is not a surprise that a recent review of 708 patients with EoE recruited from 5 US sites by Chehade et al found a significant delay between patient’s symptoms and diagnosis.25 The median time from symptom onset was 4 years in adults (ranging from 1 to 12 years), 2 years in patients between 11 and 17 years (ranging from 1 to 4 years), and 1 year in children <11 years of age (range from 0.5 to 2.3 years). Authors found that age (younger), race (non-white) and having a history of atopic dermatitis (AD) or food allergy (FA) were associated with a shorter time gap to diagnosis. Schoepfer et al described that typically EoE is not diagnosed immediately after symptom onset with a median diagnostic delay time of 6 years. The authors also showed that there is an increasing rates of stricture, the longer is the delay.24 Early diagnosis is therefore paramount, as these delays lead to worsening esophageal abnormalities/fibrosis, possibility of feeding dysfunction, and possibility of psychologic impairment.
Becoming familiar with the typical symptoms of EoE and early systematic screening of at-risk populations are two steps that may help to make an early diagnosis of EoE (Tables 2 and 3). Similarly, understanding common comorbidities is also useful when trying to screen patients; atopic patients (Table 1) and patients affected by certain diseases such as connective tissue disorders and autism spectrum disorders (ASDs) may be at increased risk of developing EoE.26 It is the goal of this review to describe some of the risk factors for developing EoE as well as delve into some of the consequences of delayed diagnosis.
Genetic risk of developing EoE
Like other atopic disorders such as AD, FA, allergic rhinitis (AR), and asthma, EoE has a complex etiology, with genetic predisposition and environmental factors playing a major role in disease development.27–29 Genetic predisposition has been clearly shown to be a critical factor as demonstrated by siblings or identical twins risk.27 The genetic risk in EoE appears to be much higher than in other atopic diseases such as asthma. Indeed, siblings have 40 times higher risk factors vs 2 folds increased risk of asthma. A recent multi center analysis found that 6.5% of patients had parents or siblings with EoE confirming the high inheritability of the disease.25 Confirming the importance of the genetic background in EoE, several loci have been now described to be linked to EoE risk confirming.29–32 However, the rapid increase in EoE prevalence experienced in the Western Country, the fact that fraternal twins are more at risk of developing EoE than siblings, and the possibility of identical twins not to be equally affected suggest a strong environmental component in EoE development as well.29 Multiple independent studies have found a positive association between EoE and several early-life factors such as maternal fever, preterm labor, cesarean delivery, antibiotic, and acid suppressant use in infancy, while there was an inverse association between having a furry pet in infancy and EoE.33–35 The environment–risk gene interaction has been examined in one study and found an association between breastfeeding and SNP rs6736278 on CAPN14 and NICU admission and SNP rs17815905 on LOC283710/KLF13.33
Atopy and risk of developing EoE
Atopy is a risk factor in EoE even if EoE per se is a rare disease so only a small fraction of atopic individual will develop EoE. Indeed, compared to the general population, patients with EoE are much more likely to be atopic.15,25,36 In the United States, 4% of adults and 6% of children have IgE-mediated FA, 8% of adults and 10% of children have asthma, upward of 30% of adults and 40% of children have allergic rhinitis (AR), and 3% of adults and 10% to 20% of children have AD.37–39 In comparison with a world wide registry, 80% of Eosinophilc Gastrointestinal Disease (EGID) patients were atopic (23% had IgE-mediated FA, 38% had asthma, 64% had AR, and 26% had AD).40 Increases in atopy were also seen in a recent review of 428 pediatric patients with EoE from a single site: 60% had asthma, 60% had AR, and 18% had AD.26 Similarly, in a recent multi site cohort review of patients with EoE, researchers found that 27% had a history of food anaphylaxis, 45% had asthma, 60% had AR, and 46% had AD.25
The relationship between IgE-mediated FA and EoE has been also been well documented in other studies. In 2014, Maggadottir et al reported 2 pediatric patients who outgrew their IgE-mediated food reactions, and when their diet contained these specific foods, they developed gastrointestinal (GI) symptoms and were ultimately diagnosed with EoE.41 Symptoms resolved and biopsy improved after removal of that specific food. Of note, in these 2 cases, both patients had normal EGD while on original restricted diet early on due to growth concerns and reflux symptoms. In any patient with a history of IgE-mediated FA who outgrows sensitivity, suspicion for EoE should be high and referrals to gastroenterology made if symptoms develop.
In addition to many patients having concomitant allergic rhinoconjunctivitis, there are patients whose EoE is either in part due to or actually triggered by aeroallergens. In 2003, Fogg et al reported the case of a 21-year-old female with esophageal symptoms and abnormal endoscopies in the spring which resolved and normalized outside of spring.42 A further review of 1180 patients with EoE found that 12% were suspected of aeroallergen triggers by history.43
Immunotherapy treatments of atopic diseases ingested orally have been rarely associated with the development of EoE as well as confirming the importance of topical exposure of allergen to the esophagus as a trigger of EoE. Subcutaneous immunotherapy, to our knowledge, has not been reported to be associated with EoE. Case reports of sublingual immunotherapy (SLIT) to dust mite and pollen immunotherapy have been published. A 10-year-old female developed symptoms (dysphagia) 6 weeks into the initiation of dust SLIT, placed on PPI and ultimately scoped with significant esophageal eosinophilia. SLIT was stopped, PPI was then discontinued, symptoms resolved, and repeat biopsy was normalized.44 Similar reports were published on SLIT for pollen immunotherapy.45,46 These are isolated case reports that confirm that environmental allergens can be a rare trigger of EoE when ingested orally.
Oral immunotherapy (OIT) and SLIT for IgE-mediated FA are also possible risk factors for the development of EoE, confirming a larger role of food allergen in EoE development. Petroni and Spergel47 reviewed 12 OIT studies (milk, egg, and peanut) and revealed that 2.7% of patients developed biopsy-proven EoE. In addition, 34% of OIT patients developed gastrointestinal symptoms (may resolve over time or persist and lead to study/OIT withdrawal). Certainly, not all patients who developed GI symptoms underwent endoscopy. In addition, baseline endoscopies were not performed. Could any of these patients have asymptomatic esophageal eosinophilia prior to initiation of SLIT or OIT? This is certainly a possibility especially because in a recent study patients with food allergies have been found to have about 5–10% of EoE {Hill, 2017 #7744}{Wright, 2018 #9317}. Although more prospective studies are needed to clarify the relationshop between OIT and SLIT and EoE, it is certainly important to screen for EoE all patients before and while undergoing oral or sublingual immunotherapy for either environmental or FA.
In addition to atopy, patients with EoE had evidence of concomitant non atopic disorders. Recently, Capucilli et al reviewed a total of 428 patients who underwent diagnosis for EoE at a single third referral center.26 Significant differences in the rate of comorbid diseases included ASD (7.5% of EoE, 1.9% of non-EoE, P<0.0001); celiac disease (5.6% of EoE, 0.9% of non-EoE, P<0.0001); connective tissue diseases (1.4% of EoE, 0.1% of non-EoE, P<0.0001); cystic fibrosis (0.9% of EoE, 0.05% of non-EoE, P<0.0001); inflammatory bowel disease (0.7% of EoE, 0.2% of non-EoE, P=0.03); type 1 diabetes mellitus (1.2% of EoE, 0.3% of non-EoE, P=0.0069), suggesting that a selected non atopic population could be at risk of EoE. The increased risk of EoE in patients with genetically determined connective tissue and barrier functions, such as Spink 7, may equally be risk factors for EoE development.48,49
Fibrostenosis in EoE
Fibrosis is the process by which excess collagen deposition leads to tissue stiffening. In the context of EoE, fibrosis is a complicated and poorly understood process regulated by fibroblasts, but also invading inflammatory cells and the resident epithelium.50–52 The esophageal mucosa is made of a stratified squamous epithelium, with the underlying lamina propria containing extracellular matrix and fibroblasts. Upon stimulation by offending food antigens, there is a robust T-helper (Th) 2 type inflammatory response with cytokines such as IL13, IL4, and IL5.53,54 Upon stimulation with IL13, esophageal epithelial cells produce chemokine eotaxin-3, the most highly upregulated transcript in EoE,55,56 leading to granulocyte infiltration, specifically eosinophils, mast cells, and basophils.57,58 In addition to Th2 cytokines produced by lymphocytes, the invading granulocytes, epithelial cells, and activated fibroblasts produce TGF-β, IL1β, and tumor necrosis factor-α.59–61 This inflammatory cascade causes epithelial injury as well as fibroblast activation.61–63
Once there has been an inflammatory insult in the esophagus and the remodeling process has started, it may be difficult to halt the remodeling process. Recent work in the esophagus as well in other organ systems such as the liver and lung have shown that fibroblasts are activated by the mechanical stiffness of their environment.62,64 In our recent work, we seeded esophageal fibroblasts on matrices of varying stiffness. Taken together, the Th2 inflammation and its effects on the epithelium and fibroblasts drive the remodeling process of EoE, but once there is stiffness of the esophagus, fibroblast activation may continue despite resolution of the inflammatory process. This causes a positive feedback mechanism in which stiffness causes increased fibroblast activation and vice versa. Thus, early diagnosis and treatment prior to the onset of esophageal stiffening may lead to improved cessation of fibroblast activity.
These cellular mechanisms culminate in esophageal symptomatology. Clinical presentation varies greatly depending on the age of diagnosis.16 Infants and toddlers often present with feeding difficulties and weight loss. Children are more likely to have complaints of vomiting and abdominal pain. Adolescents present with dysphagia and food impaction. This clinical observation was made over 15 years ago by Noel et al16 and been more rigorously studied in larger scale retrospective studies.24,65,66 Dellon et al evaluated 379 patients with EoE and found that younger patients were more likely to have an inflammatory endoscopic phenotype with linear furrows and eosinophilic exudates65 Older patients were more likely to have a fibrostenotic endoscopic phenotype with a ringed esophagus or strictures.65 They found that the increased risk to develop stenosis as measured by Odd Ratio (OR) for fibrostenotic changes increased and was 2.1 for each 10-year increase in age.65 Others have shown that the number of years of untreated disease increases the risk of fibrostenosis and stricture.24,66 Specifically, Warners et al found that strictures and food impactions occurred in patients less commonly in patients with decreased delay in diagnosis.66 Fifty-two percent of those with a diagnostic delay had food impactions and 57% had a stricture. Therefore, those with long-standing undiagnosed inflammation of the esophagus were more likely to have fibrostenosis.66
The presence of fibrostenosis may impact response to therapy. Recent retrospective and prospective studies have shown that a major factor in predicting non response to topical steroid therapy is dilation at first endoscopy.67 Eluri et al not only evaluated clinical, endoscopic, and histologic factors, but also looked at transcriptome data from a 94 gene panel (termed the EoE diagnostic panel or EDP) in biopsy specimens prior to baseline endoscopy.67,68 There was no difference in gene expression in the responders vs non responders. These data suggest that fibrostenotic disease, specifically stricturing disease requiring dilation, may be more difficult to treat than inflammatory disease.
Taken together, in vitro mechanistic studies as well as clinical evaluations show that long-standing EoE leads to enhanced fibroblast activation and increased disease complications (food impaction and stricture). There is often a diagnostic delay in EoE due to vague symptoms; however, in the case of EoE, having a low index of suspicion when patients present with esophageal findings may in fact prevent ongoing remodeling and improve response to therapy.
Feeding dysfunction and EoE
An especially relevant reason for early diagnosis of EoE in children is feeding dysfunction. As discussed, when EoE is undiagnosed for many years, patients may develop strictures and persistent dysphagia requiring dilation for relief. However, in the short term, undiagnosed EoE has consequences as well. It has been reported that anywhere between 14% and 59.8% of patients with EoE develop feeding dysfunction69 Children may refuse solids, have vomiting or gagging with eating and swallowing, and mealtimes may extend for many hours, creating anxiety and frustration for patients and families both. A 2018 prospective study of 91 subjects ages 1 through 7 showed that patients with both Gastroesophageal Reflux Disease (GERD) and EoE have feeding dysfunction even in the setting of adequate nutritional intake in terms of calories, carbohydrates, proteins, and fat70 Interestingly, patients with EoE treated with food allergen restriction showed less feeding dysfunction than those on an open diet, again showing the importance of timely diagnosis and therapy.
The early years of life are crucial to learned feeding behaviors and attitudes, as infancy and toddlerhood are the time periods in which children learn the skills necessary for successful feeding. In a 2010 review of 200 cases of EoE, 16.4% were also found to have a feeding disorder.69 Twenty-one percent of the EoE patients with feeding disorders also had a failure to thrive. Seventy percent of them required feeding therapy. The median age of these patients was 34 months, stressing that even in young children likely not yet developing strictures, there can be significant consequences of undiagnosed EoE.
Feeding difficulties in undiagnosed EoE can extend beyond the toddler years as well. In addition to describing the case of a 20-month-old with feeding refusal and “picky eating” who improved with diagnosis and treatment of his EoE, Menard-Katcher et al also describe a case of a 4-year-old with a 2-year history of refusal of solids, vomiting, and gagging that resolved with treatment of his EoE as well as feeding therapy.71 They also describe a case of a 15-year-old who had a 9-year history of solid food dysphagia, resulting in malnutrition as well as social isolation. These symptoms also improved with treatment of EoE as well as feeding therapy. These cases highlight that not only is the diagnosis of EoE crucial to healing and restoring appropriate feeding behaviors, diagnosis of feeding disorder itself and appropriate referral for feeding therapy are crucial to improvement as well.
EoE as a cause of feeding dysfunction may go undiagnosed particularly in patients with autism. A 2016 review of 45,286 patients with ASD as well as 226,430 match controls found that patients with ASD were more likely to be diagnosed with EoE compared to controls (0.4% vs 0.1%).72 This is important to note when considering populations at risk for late diagnosis of EoE, as patients with ASD commonly have feeding aversion with texture sensitivity, which may be inaccurately attributed to their underlying ASD rather than underlying pathology causing discomfort with eating.
In addition to the challenges the patients themselves experience in terms of feeding and advancing diet in the early years of their lives, a 2019 case–control study of quality of life related to EoE showed that caregivers of children with EoE have a negative impact on their quality of life due to feeding or swallowing problems.73 Caregivers report challenges in making plans to go out, as well as finding other adults to help them care for their children due to fear of feeding difficulties. They also report worry regarding breathing and choking during feeds more frequently than controls. Thirty-one percent of them expressed fear that their child would never eat or drink like other children. It is interesting to note that caregiver concerns did not vary based on disease activity and were comparable to those of caregivers of children who did not have EoE, suggesting that the diagnosis of EoE lends itself to the perception of feeding disorder even once physiologic findings have improved.
Psychosocial dysfunction in EoE
EoE is a chronic illness and as such is associated with inevitable changes in functioning and lifestyle. The impact that those changes have on single individuals is referred to as health-related quality of life (HRQoL), a tools that evaluates domains related to physical, psychological, and social functioning.69 It is well reported that youth and adults with chronic gastrointestinal diseases including EoE often report poor HRQoL. Multiple studies have shown consistently lower scores in HRQoL not only compared to healthy peers but also compared to children with other chronic illness such as cystic fibrosis, inflammatory bowel disease, epilepsy, type 1 diabetes, and sickle cell diseases based on caregiver-proxy reports.70,74 One of the elements crucially linked with poor HRQoL appears to be the presence and severity of EoE clinical symptoms as illustrated by Klinnert et al.74,75 In their 2014 studies, the authors indeed reported that in 97 children (aged 2–18 years, mean age 7.7 years ± 4.8) HRQoL scores were significantly related to symptom scores, with poor HRQoL scores being associated with baseline symptom severity, and there was consequent improvement as symptoms improved during treatment. Interestingly, the study revealed that subjects with lowest symptom severity showed the most improved HRQoL scores during treatment.74 Similar results have been reported in adults when using a specifically designed EoE-QoL score. Indeed, an EoE-specific QoL was strongly associated with patient-reported symptoms as well as endoscopic activity in a study on 99 adult patients affected by EoE. Interestingly, the types of symptoms mostly associated with reduced HRQoL in children and adults are different, with child HRQoL mostly impacted by chronic epigastric pain76 and adult HRQoL mostly related to social and diet limitations as well as anxiety around swallowing and disease in general. These data point to the fact that early treatment is key to reduce the impact of EoE on HRQoL of patients. Indeed, as described before, the disease seems to be progressive with fibrosis and related swallowing issues related to late-stage disease; therefore, early treatment may prevent many long-term consequences such as swallowing difficulties and severity of endoscopic picture in adult which are strongly correlated to poor HQRoL outcomes. Similarly, in children, early treatment may significantly reduce the duration and intensity of symptoms especially chronic epigastric pain improving HQRoL. Indeed, it is well documented that numerous studies indeed indicate that patients with chronic pain are more likely to develop psychological disorders, such as major depressive disorder, than those without chronic pain or those experiencing a shorter duration of pain as reviewed by Fine.77 Moreover, children who had abdominal pain are more at risk of developing psychosomatic pain.78
Children in EoE are often treated with diet and may share a similar psychological risk of other children suffering from food allergies, although specific studies on EoE patients are lacking. Indeed, any FA successful management requires careful attention to external food-related cues, such as being offered food, and internal, somatic cues associated with food-induced allergic reactions, and may lead to adaptive increase in vigilance and consequent increased symptoms of psychopathology.79 Food allergic children are at risk of developing EoE to “safe” food and that per se may amplify psychological problems related to food allergies. Children with FA are indeed at risk of mental health problems as shown in a study on 1420 children representative of a general pediatric North Carolina population. In that study children with FA compared to children without FA were at risk of manifesting separation and generalized anxiety, attention-deficit and hyperactivity disorders, and anorexia nervosa.79 Anorexia nervosa has been reported being associated with other food allergies such as celiac disease.80 This problem may be amplified in food allergic children who are at risk of developing EoE to “safe” foods. As lack of control and uncertainty may increase the risk of psychological disorder and an early diagnosis, screening for pre existing psychological condition may help to minimize psychological impact in those patients.
Conclusion
Clinical studies suggest that the robust nature of the inflammation universally leads to fibrosis and eventual stricture; however vague symptoms often lead to a delay in diagnosis. The combination of the progressive nature of this disease and the diagnostic delay mean that many patients develop fibrosis, feeding issues, as well as psychosocial manifestations before diagnosis. Increased index of suspicion in patients with common comorbidities as well as an in-depth interrogation of feeding behaviors could lead to decreased diagnostic delay, decreased fibrostenotic complications, and subsequent improved patient outcomes.
Acknowledgments
ABM is funded by K08DK106444 and is funded in part by the Consortium of Eosinophilic Gastrointestinal Disease Researchers (CEGIR). CEGIR (U54 AI117804) is part of the Rare Diseases Clinical Research Network (RDCRN), an initiative of the Office of Rare Diseases Research (ORDR), NCATS, and is funded through a collaboration between NIAID, NIDDK, and NCATS. CEGIR is also supported by patient advocacy groups including APFED, CURED, and EFC.
Disclosure
No conflicts of interest are declared by any of the authors in regard to this current publication.
References
1. Kelly KJ, Lazenby AJ, Rowe PC, Yardley JH, Perman JA, Sampson HA. Eosinophilic esophagitis attributed to gastroesophageal reflux: improvement with an amino acid-based formula. Gastroenterology. 1995;109:1503–1512. doi:10.1016/0016-5085(95)90637-1
2. Warners MJ, van Rhijn BD, Verheij J, Smout A, Bredenoord AJ. Disease activity in eosinophilic esophagitis is associated with impaired esophageal barrier integrity. Am J Physiol Gastrointest Liver Physiol. 2017;313:G230–G238. doi:10.1152/ajpgi.00307.2016
3. Spergel JM, Brown-Whitehorn TF, Cianferoni A, et al. Identification of causative foods in children with eosinophilic esophagitis treated with an elimination diet. J Allergy Clin Immunol. 2012;130:461–7 e5. doi:10.1016/j.jaci.2012.05.021
4. Kagalwalla AF, Shah A, Li BU, et al. Identification of specific foods responsible for inflammation in children with eosinophilic esophagitis successfully treated with empiric elimination diet. J Pediatr Gastroenterol Nutr. 2011;53:145–149. doi:10.1097/MPG.0b013e31821cf503
5. Cianferoni A, Shuker M, Brown-Whitehorn T, Hunter H, Venter C, Spergel JM. Food avoidance strategies in eosinophilic oesophagitis. Clin Exp Allergy. 2019;49:269–284. doi:10.1111/cea.13360
6. Lucendo AJ. Meta-analysis-based guidance for dietary management in eosinophilic esophagitis. Curr Gastroenterol Rep. 2015;17:464. doi:10.1007/s11894-015-0464-y
7. Clayton F, Fang JC, Gleich GJ, et al. Eosinophilic esophagitis inadults is associated with IgG4 and not mediated by IgE. Gastroenterology. 2014;147(3):602-9. doi:10.1053/j.gastro.2014.05.036
8. Simon D, Cianferoni A, Spergel JM, et al.Eosinophilic esophagitis is characterized by a non-IgE-mediated foodhypersensitivity. Allergy. 2016;71(5):611-20. doi:10.1111/all.12846
9. Dellon ES, Liacouras CA, Molina-Infante J, et al. Updated international consensus diagnostic criteria for eosinophilic esophagitis: proceedings of the AGREE conference. Gastroenterology. 2018. doi:10.1053/j.gastro.2018.07.009
10. Godwin B, Liacouras C, Mehta V, et al. A review of tertiary referrals for management of pediatric esophageal eosinophilia. Front Pediatr. 2018;6:173.
11. Gomez-Torrijos E, Garcia-Rodriguez R, Castro-Jimenez A, Rodriguez-Sanchez J, Mendez Diaz Y, Molina-Infante J. The efficacy of step-down therapy in adult patients with proton pump inhibitor-responsive oesophageal eosinophilia. Aliment Pharmacol Ther. 2016;43:534–540. doi:10.1111/apt.13496
12. Dellon ES, Katzka DA, Collins MH, et al. Budesonide oral suspension improves symptomatic, endoscopic, and histologic parameters compared with placebo in patients with eosinophilic esophagitis. Gastroenterology. 2017;152:776–86 e5. doi:10.1053/j.gastro.2016.11.021
13. Dellon ES. Management of refractory eosinophilic oesophagitis. Nat Rev Gastroenterol Hepatol. 2017;14:479–490. doi:10.1038/nrgastro.2017.56
14. Liacouras CA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011;128:3–20.e6. doi:10.1016/j.jaci.2011.02.040
15. Liacouras CA, Spergel JM, Ruchelli E, et al. Eosinophilic esophagitis: a 10-year experience in 381 children. Clin Gastroenterol Hepatol. 2005;3:1198–1206.
16. Noel RJ, Rothenberg ME. Eosinophilic esophagitis. Curr Opin Pediatr. 2005;17:690–694.
17. Spergel JM, Brown-Whitehorn TF, Beausoleil JL. 14 years of eosinophilic esophagitis: clinical features and prognosis. J Pediatr Assa
18. Assa'ad AH, Putnam PE, Collins MH. Pediatric patients with eosinophilic esophagitis: an 8-year follow-up. J Pediatr Gastroenterol Nutr. 2009;48(1):30–36.
19. Capucilli P, Cianferoni A, Grundmeier RW, Spergel JM. Comparison of comorbid diagnoses in children with and without eosinophilic esophagitis in a large population. Ann Allergy Asthma Immunol. 2018;121(6):711–716.
20. Adachi K, Mishiro T, Tanaka S, Yoshikawa H, Kinoshita Y. A study on the relationship between reflux esophagitis and periodontitis. Intern Med. 2016;55:2523–2528. doi:10.2169/internalmedicine.55.6898
21. Adachi K, Mishiro T, Tanaka S, Kinoshita Y. Suitable biopsy site for detection of esophageal eosinophilia in eosinophilic esophagitis suspected cases. Dig Endosc. 2016;28:139–144. doi:10.1111/den.12555
22. Abe Y, Iijima K, Ohara S, et al. Localized esophageal eosinophilia: is it an early manifestation of eosinophilic esophagitis or a subtype of gastroesophageal reflux disease? Dig Endosc. 2014;26:337–343. doi:10.1111/den.12150
23. Sanaka MR, Parikh MP, Thota PN, et al. Peroral endoscopic myotomy is effective for patients with achalasia and normal lower-esophageal sphincter relaxation pressures. Clin Gastroenterol Hepatol. 2018. doi:10.1016/j.cgh.2018.08.059
24. Schoepfer AM, Safroneeva E, Bussmann C, et al. Delay in diagnosis of eosinophilic esophagitis increases risk for stricture formation in a time-dependent manner. Gastroenterology. 2013;145:
25. Chehade M, Jones SM, Pesek RD, et al. Phenotypic characterization of eosinophilic esophagitis in a large multi-center patient population from the Consortium for Food Allergy Research. J Allergy Clin Immunol Pract. 2018. doi:10.1016/j.jaip.2018.05.038
26. Capucilli P, Cianferoni A, Grundmeier RW, Spergel JM. Comparison of comorbid diagnoses in children with and without eosinophilic esophagitis in a large population. Ann Allergy Asthma Immunol. 2018. doi:10.1016/j.anai.2018.08.022
27. Alexander ES, Martin LJ, Collins MH, et al. Twin and family studies reveal strong environmental and weaker genetic cues explaining heritability of eosinophilic esophagitis. J Allergy Clin Immunol. 2014;134:1084–92 e1. doi:10.1016/j.jaci.2014.07.021
28. Cianferoni A, Spergel JM, Muir A. Recent advances in the pathological understanding of eosinophilic esophagitis. Expert Rev Gastroenterol Hepatol. 2015;9:1501–1510. doi:10.1586/17474124.2015.1094372
29. Martin LJ, He H, Collins MH, et al. Eosinophilic esophagitis (EoE) genetic susceptibility is mediated by synergistic interactions between EoE-specific and general atopic disease loci. J Allergy Clin Immunol. 2018;141:1690–1698. doi:10.1016/j.jaci.2017.09.046
30. Rothenberg ME, Spergel JM, Sherrill JD, et al. Common variants at 5q22 associate with pediatric eosinophilic esophagitis. Nat Genet. 2010;42:289–291. doi:10.1038/ng.547
31. Fahey LM, Chandramouleeswaran PM, Guan S, et al. Food allergen triggers are increased in children with the TSLP risk allele and eosinophilic esophagitis. Clin Transl Gastroenterol. 2018;9:139. doi:10.1038/s41424-018-0003-x
32. Sherrill JD, Gao PS, Stucke EM, et al. Variants of thymic stromal lymphopoietin and its receptor associate with eosinophilic esophagitis. J Allergy Clin Immunol. 2010;126:160–5 e3. doi:10.1016/j.jaci.2010.04.037
33. Jensen ET, Kappelman MD, Kim HP, Ringel-Kulka T, Dellon ES. Early life exposures as risk factors for pediatric eosinophilic esophagitis. J Pediatr Gastroenterol Nutr. 2013;57:67–71. doi:10.1097/MPG.0b013e318290d15a
34. Radano MC, Yuan Q, Katz A, et al. Cesarean section and antibiotic use found to be associated with eosinophilic esophagitis. J Allergy Clin Immunol Pract. 2014;2:475–7 e1. doi:10.1016/j.jaip.2014.02.018
35. Slae M, Persad R, Leung AJ, Gabr R, Brocks D, Huynh HQ. Role of environmental factors in the development of pediatric eosinophilic esophagitis. Dig Dis Sci. 2015;60:3364–3372. doi:10.1007/s10620-015-3740-7
36. Assa’ad AH, Putnam PE, Collins MH, et al. Pediatric patients with eosinophilic esophagitis: an 8-year follow-up. J Allergy Clin Immunol. 2007;119:731–738. doi:10.1016/j.jaci.2006.10.044
37. Wallace DV, Dykewicz MS, Bernstein DI, et al. The diagnosis and management of rhinitis: an updated practice parameter. J Allergy Clin Immunol. 2008;122:S1–S84. doi:10.1016/j.jaci.2008.07.030
38. Sicherer SH, Sampson HA. Food allergy. J Allergy Clin Immunol. 2006;117:S470–S475. doi:10.1016/j.jaci.2006.02.045
39. Adams PF, Barnes PM, Vickerie JL. Summary health statistics for the U.S. population: National Health Interview Survey, 2007. Vital Health Stat. 2008;10:1–104.
40. Blanchard C, Wang N, Rothenberg ME. Eosinophilic esophagitis: pathogenesis, genetics, and therapy. J Allergy Clin Immunol. 2006;118:1054–1059. doi:10.1016/j.jaci.2006.07.038
41. Maggadottir SM, Hill DA, Ruymann K, et al. Resolution of acute IgE-mediated allergy with development of eosinophilic esophagitis triggered by the same food. J Allergy Clin Immunol. 2014;133:1487–9, 9 e1. doi:10.1016/j.jaci.2014.02.004
42. Fogg MI, Ruchelli E, Spergel JM. Pollen and eosinophilic esophagitis. J Allergy Clin Immunol. 2003;112:796–797.
43. Ram G, Lee J, Ott M, et al. Seasonal exacerbation of esophageal eosinophilia in children with eosinophilic esophagitis and allergic rhinitis. Ann Allergy Asthma Immunol. 2015;115:224–8 e1. doi:10.1016/j.anai.2015.07.004
44. Bene J, Ley D, Roboubi R, Gottrand F, Gautier S. Eosinophilic esophagitis after desensitization to dust mites with sublingual immunotherapy. Ann Allergy Asthma Immunol. 2016;116:583–584. doi:10.1016/j.anai.2016.03.017
45. Miehlke S, Alpan O, Schroder S, Straumann A. Induction of eosinophilic esophagitis by sublingual pollen immunotherapy. Case Rep Gastroenterol. 2013;7:363–368. doi:10.1159/000355161
46. Rokosz M, Bauer C, Schroeder S. Eosinophilic esophagitis induced by aeroallergen sublingual immunotherapy in an enteral feeding tube-dependent pediatric patient. Ann Allergy Asthma Immunol. 2017;119:88–89. doi:10.1016/j.anai.2017.05.004
47. Petroni D, Spergel JM. Eosinophilic esophagitis and symptoms possibly related to eosinophilic esophagitis in oral immunotherapy. Ann Allergy Asthma Immunol. 2018;120:237–40 e4. doi:10.1016/j.anai.2017.11.016
48. Abonia JP, Wen T, Stucke EM, et al. High prevalence of eosinophilic esophagitis in patients with inherited connective tissue disorders. J Allergy Clin Immunol. 2013. doi:10.1016/j.jaci.2013.02.030
49. Rochman M, Azouz NP, Rothenberg ME. Epithelial origin of eosinophilic esophagitis. J Allergy Clin Immunol. 2018;142:10–23. doi:10.1016/j.jaci.2018.05.008
50. Muir AB, Lim DM, Benitez AJ, et al. Esophageal epithelial and mesenchymal cross-talk leads to features of epithelial to mesenchymal transition in vitro. Exp Cell Res. 2013;319:850–859. doi:10.1016/j.yexcr.2012.12.002
51. Muir AB, Dods K, Noah Y, et al. Esophageal epithelial cells acquire functional characteristics of activated myofibroblasts after undergoing an epithelial to mesenchymal transition. Exp Cell Res. 2015;330:102–110. doi:10.1016/j.yexcr.2014.08.026
52. Aceves SS, Newbury RO, Dohil R, Bastian JF, Broide DH. Esophageal remodeling in pediatric eosinophilic esophagitis. J Allergy Clin Immunol. 2007;119:206–212. doi:10.1016/j.jaci.2006.10.016
53. Cianferoni A, Ruffner MA, Guzek R, et al. Elevated expression of activated TH2 cells and milk-specific TH2 cells in milk-induced eosinophilic esophagitis. Ann Allergy Asthma Immunol. 2018;120:177–83 e2. doi:10.1016/j.anai.2017.11.006
54. Merves J, Muir A, Modayur Chandramouleeswaran P, Cianferoni A, Wang ML, Spergel JM. Eosinophilic esophagitis. Ann Allergy Asthma Immunol. 2014. doi:10.1016/j.anai.2014.01.023
55. Blanchard C, Stucke EM, Rodriguez-Jimenez B, et al. A striking local esophageal cytokine expression profile in eosinophilic esophagitis. J Allergy Clin Immunol. 2011;127:
56. Cheng E, Zhang X, Wilson KS, et al. JAK-STAT6 pathway inhibitors block eotaxin-3 secretion by epithelial cells and fibroblasts from esophageal eosinophilia patients: promising agents to improve inflammation and prevent fibrosis in EoE. PLoS One. 2016;11:e0157376. doi:10.1371/journal.pone.0157376
57. Aceves SS, Chen D, Newbury RO, Dohil R, Bastian JF, Broide DH. Mast cells infiltrate the esophageal smooth muscle in patients with eosinophilic esophagitis, express TGF-beta1, and increase esophageal smooth muscle contraction. J Allergy Clin Immunol. 2010;126:1198–204 e4. doi:10.1016/j.jaci.2010.08.050
58. Noti M, Wojno ED, Kim BS, et al. Thymic stromal lymphopoietin-elicited basophil responses promote eosinophilic esophagitis. Nat Med. 2013. doi:10.1038/nm.3281
59. Muir AB, Wang JX, Nakagawa H. Epithelial-stromal crosstalk and fibrosis in eosinophilic esophagitis. J Gastroenterol. 2019;54:10–18. doi:10.1007/s00535-018-1498-3
60. Sayej WN, Menoret A, Maharjan AS, et al. Characterizing the inflammatory response in esophageal mucosal biopsies in children with eosinophilic esophagitis. Clin Transl Immunol. 2016;5:e88. doi:10.1038/cti.2016.30
61. Kasagi Y, Dods K, Wang JX, et al. Fibrostenotic eosinophilic esophagitis might reflect epithelial lysyl oxidase induction by fibroblast-derived TNF-alpha. J Allergy Clin Immunol. 2019;144(1):171–182.
62. Muir AB, Dods K, Henry SJ, et al. Eosinophilic esophagitis-associated chemical and mechanical microenvironment shapes esophageal fibroblast behavior. J Pediatr Gastroenterol Nutr. 2016;63:200–209.
63. Rochman M, Travers J, Miracle CE, et al. Profound loss of esophageal tissue differentiation in patients with eosinophilic esophagitis. J Allergy Clin Immunol. 2017;140:738–49 e3. doi:10.1016/j.jaci.2016.11.042
64. Perepelyuk M, Terajima M, Wang AY, et al. Hepatic stellate cells and portal fibroblasts are the major cellular sources of collagens and lysyl oxidases in normal liver and early after injury. Am J Physiol Gastrointest Liver Physiol. 2013;304:G605–G614. doi:10.1152/ajpgi.00222.2012
65. Dellon ES, Kim HP, Sperry SL, Rybnicek DA, Woosley JT, Shaheen NJ. A phenotypic analysis shows that eosinophilic esophagitis is a progressive fibrostenotic disease. Gastrointest Endosc. 2014;79:577–85 e4. doi:10.1016/j.gie.2013.10.027
66. Warners MJ, Oude Nijhuis RAB, de Wijkerslooth LRH, Smout A, Bredenoord AJ. The natural course of eosinophilic esophagitis and long-term consequences of undiagnosed disease in a large cohort. Am J Gastroenterol. 2018;113:836–844. doi:10.1038/s41395-018-0052-5
67. Eluri S, Runge TM, Hansen J, et al. Diminishing effectiveness of long-term maintenance topical steroid therapy in PPI non-responsive eosinophilic esophagitis. Clin Transl Gastroenterol. 2017;8:e97. doi:10.1038/ctg.2017.27
68. Wolf WA, Cotton CC, Green DJ, et al. Predictors of response to steroid therapy for eosinophilic esophagitis and treatment of steroid-refractory patients. Clin Gastroenterol Hepatol. 2015;13:452–458. doi:10.1016/j.cgh.2014.07.034
69. Hommel KA, Franciosi JP, Gray WN, Hente EA, Ahrens A, Rothenberg ME. Behavioral functioning and treatment adherence in pediatric eosinophilic gastrointestinal disorders. Pediatr Allergy Immunol. 2012;23:494–499. doi:10.1111/j.1399-3038.2012.01297.x
70. Cortina S, McGraw K, Dealarcon A, Ahrens A, Rothenberg ME, Drotar D. Psychological functioning of children and adolescents with eosinophil-associated gastrointestinal disorders. Child Health Care. 2010;39:266–278. doi:10.1080/02739615.2010.515927
71. Menard-Katcher C, Henry M, Furuta GT, Atkins D, Maune NC, Haas AM. Significance of feeding dysfunction in eosinophilic esophagitis. World J Gastroenterol. 2014;20:11019–11022. doi:10.3748/wjg.v20.i31.11019
72. Heifert TA, Susi A, Hisle-Gorman E, et al. Feeding disorders in children with autism spectrum disorders are associated with eosinophilic esophagitis. J Pediatr Gastroenterol Nutr. 2016;63:e69–73. doi:10.1097/MPG.0000000000001282
73. Hiremath G, Rogers E, Kennedy E, Hemler J, Acra S. A comparative analysis of eating behavior of school-aged children with eosinophilic esophagitis and their caregivers’ quality of life: perspectives of caregivers. Dysphagia. 2019. doi:10.1007/s00455-019-09984-x
74. Ingerski LM, Modi AC, Hood KK, et al. Health-related quality of life across pediatric chronic conditions. J Pediatr. 2010;156:639–644. doi:10.1016/j.jpeds.2009.11.008
75. Klinnert MD. Psychological impact of eosinophilic esophagitis on children and families. Immunol Allergy Clin North Am. 2009;29:99–107. doi:10.1016/j.iac.2008.09.011
76. Safroneeva E, Coslovsky M, Kuehni CE, et al. Eosinophilic oesophagitis: relationship of quality of life with clinical, endoscopic and histological activity. Aliment Pharmacol Ther. 2015;42:1000–1010. doi:10.1111/apt.13370
77. Fine PG. Long-term consequences of chronic pain: mounting evidence for pain as a neurological disease and parallels with other chronic disease states. Pain Med. 2011;12:996–1004. doi:10.1111/j.1526-4637.2011.01187.x
78. Sherry DD, McGuire T, Mellins E, Salmonson K, Wallace CA, Nepom B. Psychosomatic musculoskeletal pain in childhood: clinical and psychological analyses of 100 children. Pediatrics. 1991;88:1093–1099.
79. Shanahan L, Zucker N, Copeland WE, Costello EJ, Angold A. Are children and adolescents with food allergies at increased risk for psychopathology? J Psychosom Res. 2014;77:468–473. doi:10.1016/j.jpsychores.2014.10.005
80. Marild K, Stordal K, Bulik CM, et al. Celiac disease and anorexia nervosa: a Nationwide Study. Pediatrics. 2017;139. doi:10.1542/peds.2016-4367
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.