Back to Journals » Journal of Asthma and Allergy » Volume 19
Eosinophil-Derived Neurotoxin: A Potential Biomarker for Allergic Bronchopulmonary Aspergillosis
Authors Zou M, Pan Y, Yang Y, Liu X, Zeng R, Dong L ![]()
Received 24 December 2025
Accepted for publication 20 March 2026
Published 31 March 2026 Volume 2026:19 587227
DOI https://doi.org/10.2147/JAA.S587227
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Minfang Zou,1,2 Yun Pan,3,4 Yan Yang,2,5 Xiaofei Liu,3,4 Rong Zeng,3,4 Liang Dong6
1Department of General Practice, Qilu Hospital of Shandong University, Jinan, Shandong, People’s Republic of China; 2Department of NHC Key Laboratory of Otorhinolaryngology, Shandong University, Jinan, Shandong, People’s Republic of China; 3Department of Respiratory, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Shandong Institute of Respiratory Diseases, Featured Laboratory of Respiratory Immunology and Regenerative Medicine in Universities of Shandong, Jinan Clinical Research Center for Respiratory Disease, Jinan, Shandong, People’s Republic of China; 4Shandong Provincial Key Medical and Health Laboratory of Translational Medicine in Microvascular Aging, The First Affiliated Hospital of Shandong First Medical University & Shandong Province Qianfoshan Hospital, Jinan, Shandong, People’s Republic of China; 5Department of Otolaryngology, Qilu hospital of Shandong University, Jinan, Shandong, People’s Republic of China; 6Department of Respiratory, Shandong Provincial Qianfoshan Hospital, Shandong University, Jinan, Shandong, People’s Republic of China
Correspondence: Liang Dong, Department of Respiratory, Shandong Provincial Qianfoshan Hospital, Shandong University, Jinan, 250021, People’s Republic of China, Tel +86 531 89262203, Fax +86 531 89262203, Email [email protected]
Objective: Eosinophil-derived neurotoxin (EDN) has emerged as a potential biomarker in asthma. Allergic bronchopulmonary aspergillosis (ABPA) is a severe complication of asthma. This study aimed to investigate serum EDN levels in ABPA and assess the diagnostic utility of serum EDN in distinguishing ABPA from Aspergillus fumigatus–sensitized asthma (ASA).
Methods: This is a single-center retrospective analysis of data from patients initially diagnosed with ABPA and asthma between 2021 and 2023. Eighteen patients with ABPA, 11 with unsensitized asthma (UA), 10 with ASA, and 18 healthy controls were enrolled. Serum EDN levels were measured by enzyme-linked immunosorbent assay (ELISA). Comparisons among groups were performed using Mann–Whitney U-test with Bonferroni correction for multiple comparisons. Correlations between EDN and clinical parameters were assessed using Spearman rank correlation analysis. Receiver operating characteristic (ROC) curve analysis was used to evaluate diagnostic performance.
Results: Serum EDN levels were significantly higher in ABPA patients (median 132.8 ng/mL, IQR: 106.1– 256.4) compared to healthy controls (39.7 ng/mL, IQR: 26.6– 53.5), UA (59.4 ng/mL, IQR: 48.9– 70.1), and ASA (67.6 ng/mL, IQR: 33.3– 104.0) after Bonferroni correction (all p < 0.0083). EDN strongly correlated with eosinophil counts (ρ= 0.73, p < 0.01) and A. fumigatus-specific IgE (ρ= 0.70, p < 0.01), and moderately with total IgE (ρ= 0.45, p < 0.05) and bronchiectasis (ρ= 0.40, p < 0.05). ROC analysis showed that EDN (AUC = 0.844, 95% CI: 0.693– 0.996) had comparable diagnostic performance to total IgE (AUC = 0.833, 95% CI: 0.668– 0.999) in differentiating ABPA from ASA, with sensitivity of 83.3% (95% CI: 0.608 to 0.942) and specificity of 80.0% (95% CI: 0.490 to 0.965) at a cutoff of 96.26 ng/mL.
Conclusion: EDN levels are significantly elevated in ABPA and correlates with key disease markers, including eosinophil counts, A. fumigatus-specific IgE and bronchiectasis on chest CT. EDN demonstrates diagnostic potential comparable to total IgE in distinguishing ABPA from other asthma phenotypes. These findings suggest EDN may serve as a useful biomarker for ABPA, though validation in larger, multi-center cohorts is warranted.
Keywords: allergic bronchopulmonary aspergillosis, asthma, eosinophil-derived neurotoxin, ABPA, biomarker, Aspergillus fumigatus–sensitized asthma
Introduction
Allergic bronchopulmonary aspergillosis (ABPA) is an immunological pulmonary disorder caused by Aspergillus fumigatus,1 first described by Hinson et al in 1952.2 It occurs most frequently in patients with bronchial asthma or cystic fibrosis,1 but it may also develop in individuals with bronchiectasis or chronic obstructive pulmonary disease (COPD).3
Compared with European and American countries, ABPA in China predominantly affects patients with asthma. The prevalence of ABPA is approximately 11% among adults with asthma and can reach as high as 37% in asthmatic individuals sensitized to Aspergillus.4 The diagnosis of ABPA is based on a combination of clinical, immunological, and radiological features, with serological findings playing a particularly important role.5 Although the diagnostic criteria for ABPA have been continuously updated in recent years,5–9 the optimal cut-off values for key immunological parameters remain controversial.
ABPA is characterized by a pronounced Th2-driven immune response, and the eosinophilic component is considered a hallmark feature of the disease.10,11 Direct interactions between eosinophils and Aspergillus fumigatus conidia can trigger the formation of eosinophil extracellular traps (EETs), which contribute to key pathological processes in ABPA, including airway mucus plugging, bronchiectasis, and airway remodeling.12 In addition to its pathophysiological role, peripheral blood eosinophil count is also included as one of the diagnostic criteria for ABPA. Aspergillus fumigatus–sensitized asthma (ASA) refers to asthma with only Aspergillus sensitization but no clinical and radiological features of ABPA, characterized by airway hyperreactivity as the core manifestation.13 Non-fungal sensitized asthma (NFSA) denotes ordinary asthma without fungal sensitization, and its common aeroallergens include dust mites and pollen.13 In this study, this group is termed unsensitized asthma (UA). Patients with ASA experience worsening asthma control due to repeated fungal exposure, with continued progression to ABPA driven by increased Th2 immune responses.10 However, distinguishing eosinophil-mediated ABPA from ASA,NFSA, or other eosinophilia-associated conditions can be challenging, as these disorders share overlapping clinical manifestations and blood eosinophil counts lack optimal diagnostic accuracy.14,15 Moreover, eosinophil counts or percentages in peripheral blood do not reliably reflect eosinophil activity and can be significantly affected by oral glucocorticoid therapy, thereby increasing the likelihood of missed or delayed diagnosis in patients with ABPA.
A prompt diagnosis of ABPA is essential for improving lung function and overall quality of life.16 However, overdiagnosis or inappropriate attribution of other conditions to ABPA may lead to unnecessary use of corticosteroids and antifungal agents, thereby increasing healthcare costs and the risk of adverse effects.16 Eosinophils are recognized as key markers of allergic inflammation and are considered major effector cells in allergic processes.17 Eosinophil granule proteins—including major basic protein (MBP), eosinophil cationic protein (ECP), eosinophil-derived neurotoxin (EDN), and eosinophil peroxidase (EPO)—are known effector molecules responsible for many of the biological functions of eosinophils.18 Compared with eosinophil counts alone, measurement of eosinophil granule proteins such as EDN and ECP has been reported to more accurately reflect the degree of eosinophilic inflammation. ECP has a high isoelectric point and carries a strong positive charge in blood, which causes it to adhere to cell membranes or the walls of collection tubes, complicating accurate quantification. In contrast, EDN has an isoelectric point of 8.3, close to neutral, making its measurement in blood more reliable and reproducible.19 Plasma EDN levels have therefore been proposed as a noninvasive biomarker for diagnosing or monitoring allergic diseases such as asthma20 and eosinophilic esophagitis (EoE).21
To the best of our knowledge, no previous studies have investigated serum EDN levels in patients with ABPA. Therefore, the aim of this study was to evaluate serum EDN levels in individuals with ABPA in comparison with those in asthma patients with or without Aspergillus fumigatus sensitization, as well as healthy controls, and to determine whether EDN may serve as a useful biomarker for the diagnosis of ABPA.
Materials and Methods
The retrospective study was conducted between 2021.09 and 2023.07 in Qilu Hospital of Shandong University (Jinan, Shandong, China).This study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the Ethics Review Committee of Qilu Hospital of Shandong University (KYLL-2019-2-053), and all included patients signed informed consent form before study commencement.
Study Populations
In this study, 39 patients (18 patients with ABPA, 11 patients with unsensitized asthma (UA), and 10 patients with Aspergillus-sensitized asthma (ASA)) and 18 healthy people were enrolled in the Department of Respiratory, Qilu Hospital of Shandong University (Jinan, Shandong, China).
Subjects were excluded if they had any of the following condition: (a) age <18 years or age >75 years; (b) use of oral or inhaled corticosteroids within the past 4 weeks; (c) complicated with other diseases including severe heart failure, chronic renal failure, chronic liver failure, chronic pulmonary diseases, cancer and others; (d) pregnancy; (e) smoking history; (f) respiratory infection for less than 4 weeks; (g) unable to provide informed consent. This corticosteroid exclusion criterion was intentionally applied to evaluate native EDN levels without the confounding effects of corticosteroid therapy, ensuring that measured EDN concentrations reflected underlying disease activity rather than treatment-related suppression.
Diagnosis Criteria
All of the asthmatic patients were required to meet the following eligibility criteria: a clinical history of asthma symptoms including wheeze, cough, chest tightness and/or dyspnea; airflow variability with a 12% and 200mL increase in FEV1 after inhalation of 400µg salbutamol; airway hyper-responsiveness (PC20 methacholine <8mg/mL).
The diagnosis of unsensitized asthma need to meet the following criteria: (a) asthma; (b) A. fumigatus-specific IgE <0.35kUA/L. Aspergillus-sensitized asthma was diagnosed basing on the following criteria: (a) asthma; (b) A. fumigatus-specific IgE ≥0.35kUA/L, but not fulfilling the criteria for the diagnosis of ABPA.
The diagnosis of ABPA was based on the criteria of ISHAM working group.8 The subject met the two obligatory criteria: (a) A. fumigatus-specific IgE level ≥0.35 kUA/L; (b) elevated total IgE levels (≥500 IU/mL); and at least two of the following criteria: (i) presence of IgG antibodies against A. fumigatus in serum, (ii) total eosinophil count ≥ 500 cells/μL, and (iii) Thin-section chest computed tomography consistent with ABPA (bronchiectasis, mucus plugging and high-attenuation mucus) or fleeting opacities on chest radiograph consistent with ABPA.
Laboratory Tests
Serum Total IgE, A. fumigatus-Specific IgE and A. fumigatus-Specific IgG Levels
Serum total IgE, A. fumigatus-specific IgE were analyzed using the automated fluorescent enzyme immunoassay (Phadia, Thermofisher Scientific, Stockholm, Sweden) using the ImmunoCAP technology according to the procedures offered by the manufacture. We use assay Enzyme Immunoassay (EIA) (Dynamiker, Tianjin, China) for determining A. fumigatus-specific IgG levels. (positive: >120AU/mL; intermediate: 80–120 AU/mL; negative: <80 AU/mL).
Peripheral Blood Eosinophil Counts
Peripheral blood eosinophil counts were determined by the clinical laboratory of Qilu Hospital, Shandong University (Jinan, Shandong, China).
Detection of EDN
Venous blood samples were collected at the initial visit, centrifuged at 3000 rpm for 10 minutes, and serum was stored at −80°C until analysis. All samples underwent only one freeze-thaw cycle. EDN levels were measured in duplicate using an ELISA kit (MBL International, Nagoya, Japan) according to the manufacturer’s instructions. The assay calibration range was [8.3–66.4 ng/mL]; samples above the upper limit were diluted and re-assayed. Intra- and inter-assay coefficients of variation were [10%] and [15%], respectively. Hemolyzed or lipemic samples were excluded. Laboratory personnel were blinded to clinical diagnoses.
Lung Function
Lung function tests were performed on MasterScreenTM Pneumo spirometer (Jaeger Co, Hoechberg, Germany) in all patients. Forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), forced expiratory volume in 1s in predicted percentage (%FEV1) and the FEV1/FVC ratio were recorded according to the American Thoracic Society and European Respiratory Society (ATS/ERS) recommendations.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA) and GraphPad Prism version 10.0 (GraphPad Software, San Diego, CA, USA). Non-parametric tests were used due to non-normal distribution of data. Numerical data were presented as median with interquartile range (25th–75th percentile), and categorical variables as frequency (percentage). Comparisons between two groups were performed using the Mann–Whitney U-test. For comparisons involving three or more groups, the Kruskal–Wallis test was used, followed by post-hoc pairwise comparisons with Bonferroni correction to adjust for multiple testing. Correlations between serum EDN and clinical parameters were assessed using Spearman rank correlation analysis; a complete correlation matrix is provided in the supplementary materials (Figure S1). Receiver operating characteristic (ROC) curve analysis was performed to evaluate the diagnostic performance of EDN and total IgE. The area under the curve (AUC), optimal cutoff value (based on Youden’s index), sensitivity, specificity, and their 95% confidence intervals (CI) were calculated. As the cutoff was derived from and evaluated on the same cohort, it should be considered exploratory and requires further validation. All tests were two-sided, and P values < 0.05 were considered statistically significant, except where Bonferroni-corrected thresholds applied.
Results
39 patients (ABPA [n=18], UA [n=11], ASA [n=10]) and 18 healthy people were enrolled in our study. Demographic and clinical parameters of the study subjects were compared (Table 1). No significant differences were observed among the four groups regarding gender ratio, body mass index(BMI) and age. The median FEV1 (percentage predicted) was significantly lower in patients with ABPA and ASA than in patients with UA. The levels of serum total IgE and total eosinophil counts were significantly elevated in ABPA relative to asthma group, and the differences were statistically significant (Table 1). The level of A. fumigatus-specific IgE and IgG were significantly higher in ABPA groups than ASA groups. The prevalence of bronchiectasis was significantly higher in the ABPA group compared to both the UA group and the ASA group. No significant difference was observed between the UA and ASA groups.
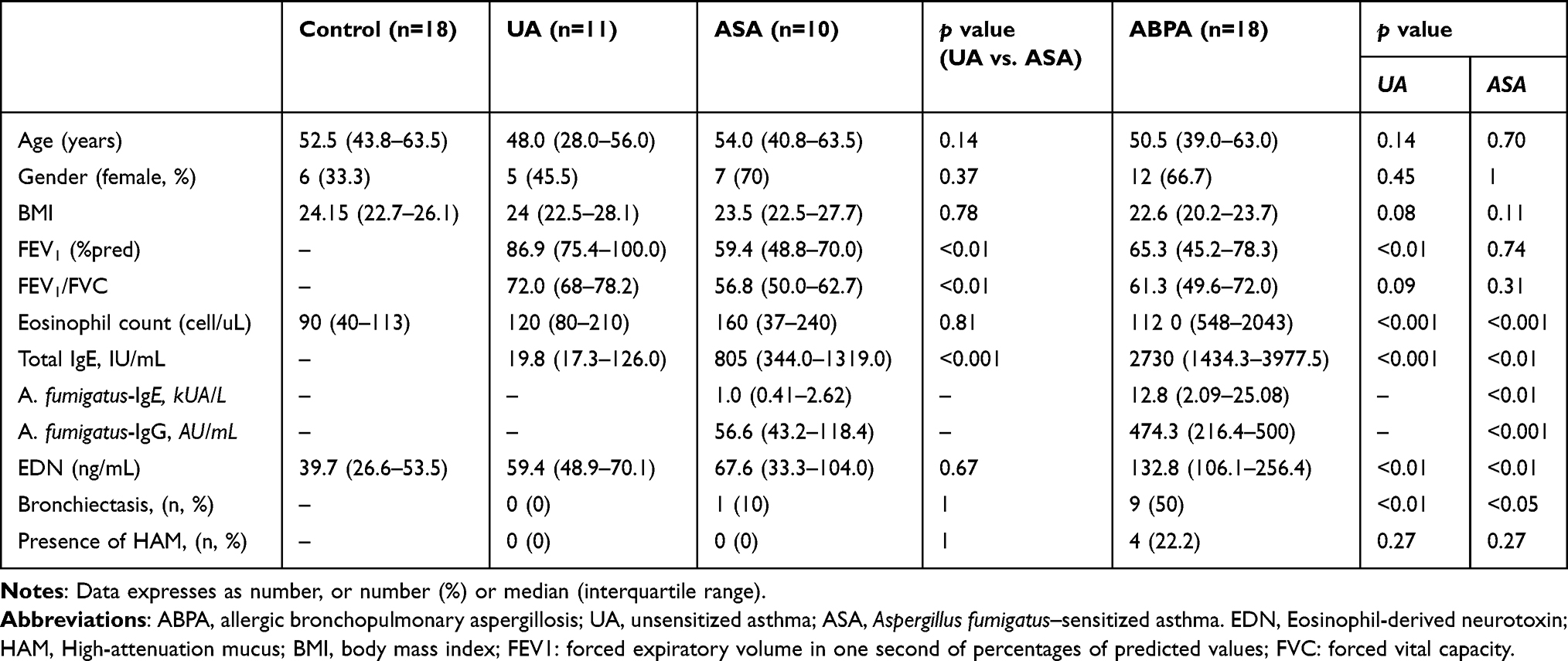 |
Table 1 Clinical Characteristics Among the Four Studied Groups |
Serum Levels of EDN Were Higher in ABPA Patients Than Asthma Groups
Serum EDN levels significantly differed between groups of patients. The levels of EDN in the serum were significantly higher in both asthma patients (59.6 ng/mL [42.7–93.4]) and ABPA patients (132.8 ng/mL [106.1–256.4]) compared to the healthy control group (39.7 ng/mL [26.6–53.5]; p=0.007 and p<0.001). Moreover, ABPA patients exhibited significantly higher levels of EDN in their serum compared to asthma patients. When dividing asthma patients into non-Aspergillus sensitized and Aspergillus sensitized groups, serum level of EDN in patients with ABPA (132.8 ng/mL [106.1–256.4]) was much higher than in patients with ASA (67.6 ng/mL [33.3–104.0]; p=0.003) and in patients with UA (59.4 ng/mL [48.9–70.1]; p= 0.001) (Table 1). Besides, we observed that although the level of EDN in the serum was higher in Aspergillus sensitized asthma patients than in the non-Aspergillus sensitized group, this difference was not statistically significant. After Bonferroni correction for multiple comparisons, significant differences in serum EDN levels were observed across groups. EDN levels were significantly higher in the ABPA group compared to both the Healthy (p < 0.0167) and Asthma (p < 0.0167) groups (Figure 1A). In Figure 1B, which included all four groups, EDN levels in ABPA were significantly higher than in Healthy controls, UA, and ASA after Bonferroni correction (all p < 0.0083). No significant differences were observed among the Healthy, UA, and ASA groups.
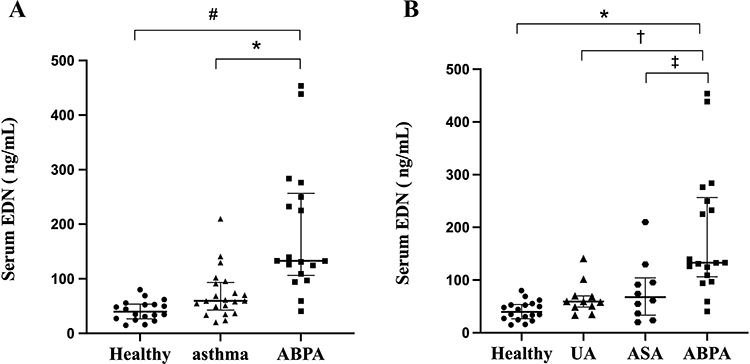 |
Figure 1 Serum Eosinophil-Derived Neurotoxin level among the studied groups. (A) Median (IQR) of EDN (ng/mL) in the three studied groups. Data were analyzed using Mann–Whitney U-test with Bonferroni correction for three comparisons. Significance threshold: p < 0.0167. *p < 0.0167 vs. Healthy; #p < 0.0167 vs. Asthma. (B) Median (IQR) of EDN (ng/mL) in the four studied groups. Data were analyzed using Mann–Whitney U-test with Bonferroni correction for six comparisons. Significance threshold: p < 0.0083. *p < 0.0083 vs. Healthy; †p < 0.0083 vs. UA; ‡p < 0.0083 vs. ASA. Abbreviations: ABPA, allergic bronchopulmonary aspergillosis; UA, unsensitized asthma; ASA, Aspergillus fumigatus–sensitized asthma. EDN, Eosinophil-derived neurotoxin. |
Serum EDN Levels Were Associated with Peripheral Blood Eosinophil Counts, Serum Total IgE, A. fumigatus-Specific IgE and Bronchiectasis on Chest CT
We found that the level of serum EDN positively correlated with peripheral blood eosinophils (Spearman’s ρ= 0.732, p < 0.001), serum total IgE (ρ= 0.449, p < 0.05), A. fumigatus-specific IgE (ρ= 0.700, p < 0.001) and A. fumigatus-specific IgG (ρ= 0.631, p < 0.001). Patients with bronchiectasis on chest CT had significantly higher EDN levels compared to those without (Mann–Whitney U-test, p < 0.05). In contrast, there was no statistically significant difference in serum EDN levels between the two groups of patients with and without highly attenuated mucus (p = 0.262). (Figure 2).
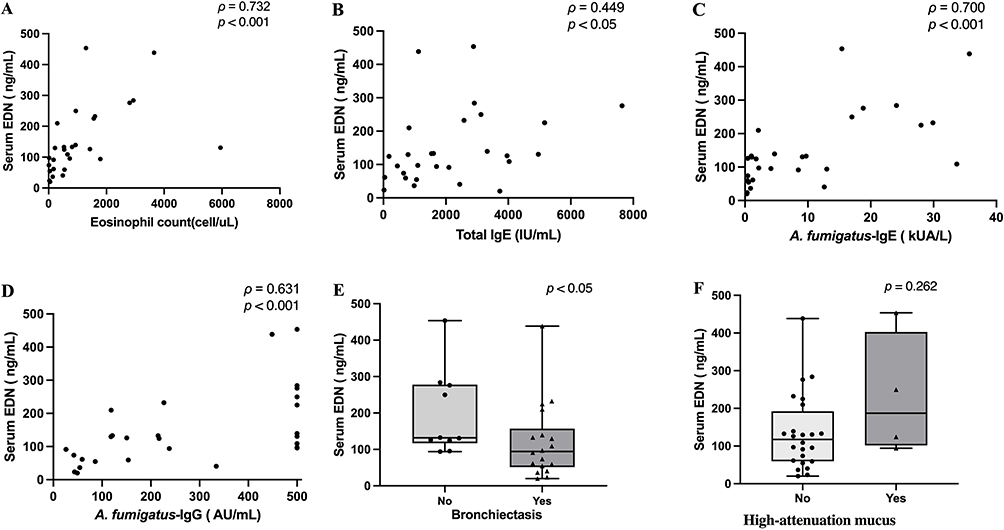 |
Figure 2 Correlations of Serum Eosinophil-Derived Neurotoxin with clinical parameters. Eosinophil-Derived Neurotoxin were positively correlated to peripheral blood eosinophil counts (A), serum total IgE levels (B), Aspergillus fumigatus-specific IgE levels (C), Aspergillus fumigatus-specific IgG (D), Bronchiectasis (E), and negatively correlated to High-attenuation mucus (F). Spearman correlation for (A–D); Mann–Whitney U-test for (E and F); data in (E and F) shown as scatter plots with median. Abbreviations: EDN, Eosinophil-derived neurotoxin; IgE, immunoglobulin E. |
A correlation matrix including all clinical parameters was generated and is provided in the supplementary materials (Figure S1). EDN showed strong positive correlations with eosinophil counts (ρ = 0.73, p < 0.001) and A. fumigatus-specific IgE (ρ = 0.70, p < 0.001), and moderate correlations with total IgE (ρ = 0.45, p < 0.05) and bronchiectasis (ρ = 0.40, p < 0.05). No significant correlations were observed between EDN and age, sex, BMI, or lung function parameters.
Diagnostic Value of Serum EDN Levels to Diagnose ABPA from ASA
ROC curves were calculated to determine the diagnostic value of EDN for diagnosing ABPA from ASA. The diagnostic accuracy of serum EDN, described as ROC AUC, was 0.844 (p = 0.003, 95% CI: 0.693 to 0.996) (Figure 3). The optimal cutoff value for EDN was 96.26 ng/mL, with a sensitivity of 83.3% (95% CI: 0.608 to 0.942), a specificity of 80.0% (95% CI: 0.490 to 0.965). ROC curve of serum total IgE was also analyzed. The area under the curve was 0.833 (p = 0.004, 95% CI: 0.668 to 0.999) (Figure 3). The optimal cut-off value for total IgE was 1080 IU/mL, with a sensitivity of 88.9% (95% CI: 0.653 to 0.986), a specificity of 80.0% (95% CI: 0.444 to 0.975). However, given the exploratory nature of this cutoff, these estimates should be interpreted with caution.
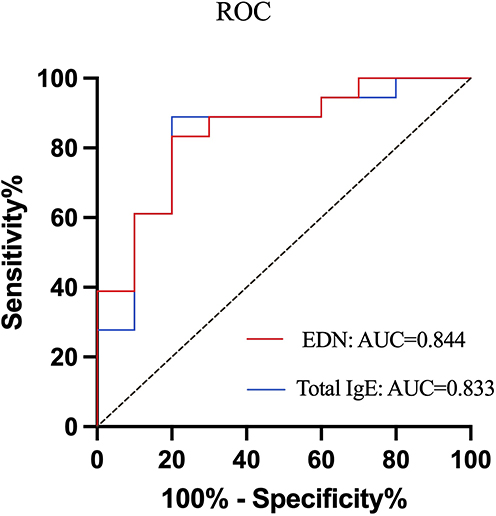 |
Figure 3 ROC curve for serum Eosinophil-Derived Neurotoxin and Total IgE. ROC curve analysis revealed that both EDN and IgE had high sensitivity and specificity (EDN sensitivity 83.3%, specificity 80.0%, AUC: 0.844). Abbreviation: IgE, immunoglobulin E. |
Discussion
Eosinophil-derived neurotoxin (EDN) has been increasingly utilized in recent years as a marker of eosinophilic inflammatory diseases.19–22 In the present study, we found that serum EDN levels were significantly elevated in patients with ABPA compared to those with UA, ASA, and healthy controls. This elevation persisted after Bonferroni correction for multiple comparisons. Furthermore, EDN demonstrated diagnostic performance comparable to total serum IgE in distinguishing ABPA from ASA, with an AUC of 0.844 and a sensitivity/specificity profile similar to that of total IgE. EDN is primarily derived from eosinophils and reflects the extent of eosinophil activation and degranulation.23 Given that ABPA is a Th2-mediated disease characterized by eosinophilic inflammation,24 our finding of elevated EDN in ABPA is biologically plausible and consistent with the role of eosinophils in this condition. EDN correlated positively with total IgE, blood eosinophil counts, and Aspergillus fumigatus-specific IgE in our cohort, further supporting its association with type 2 inflammatory pathways. To the best of our knowledge, serum EDN levels in patients with ABPA have not previously been reported, making this the first study to explore its potential as a diagnostic biomarker in this population.
In our study, serum EDN levels in patients with ABPA were significantly higher than those in asthma patients and healthy controls. However, no significant differences were observed between asthmatic patients with Aspergillus fumigatus sensitization and those without sensitization. Only a limited number of studies have examined ECP and EDN levels in ABPA. Early research reported that sputum, plasma, or serum ECP levels tended to be higher in ABPA-positive patients than in those without ABPA, although the differences did not reach statistical significance.24,25 We believe that discrepancies between previous findings and ours may be partly explained by differences in study populations. Specifically, eosinophilic inflammation in asthma-associated ABPA may be more pronounced than in cystic fibrosis–associated ABPA, potentially influencing eosinophil-derived protein levels. This assumption was later supported by subsequent research. Wark et al demonstrated that sputum ECP levels in ABPA were significantly higher than those in fungal-sensitized and non–fungal-sensitized asthma, and these elevations were not correlated with total serum IgE levels.26
EDN is a potentially attractive analytical biomarker that can be reliably quantified, unlike other eosinophil granule proteins which are inherently sticky due to their potent polycationic properties.27 Several characteristics support its utility as an ideal biomarker: EDN concentrations remain stable in serum for at least seven days and show minimal variation during storage.28 Serum samples maintain stability after repeated freeze-thaw cycles and can be stored for up to one year without significant degradation.28 Unlike eosinophil counts, which are affected by diurnal variations and have limitations as markers of eosinophil activation,28,29 EDN exhibits no significant circadian rhythm and demonstrates strong stability.23,28 Furthermore, EDN can be quantitatively measured in various biological fluids, including serum, sputum, plasma, bronchoalveolar lavage fluid, and urine,28,30 offering considerable flexibility in clinical sampling. These properties, including reliable quantification, storage stability, absence of diurnal variation, and versatility across sample types, collectively support the potential clinical utility of EDN as a stable and accessible marker of eosinophilic inflammation in ABPA and related disorders.28,30,31
ABPA is currently considered an exaggerated form of Aspergillus sensitization. Patients with fungal-sensitized asthma may progress to ABPA due to an enhanced Th2 immune response.30 The prevalence of ABPA in Aspergillus-sensitized bronchial asthma is 40%.32 ABPA with serological evidence alone (ABPA-S) is regarded as the earliest stage of ABPA, characterized by a lower degree of immune activity.33 Therefore, it can be hypothesized that ASA and ABPA represent different stages of fungal sensitization with varying immune responses, ranging from asthma at one end to ABPA at the other.30 In our study, ABPA patients showed higher baseline levels of total IgE, blood eosinophils counts, A. Aspergillus-specific IgE and EDN compared to those of patients with asthma. This indicates that ABPA patients with elevated EDN levels exhibited a more intense inflammatory response in their bodies.
Distinguishing between ASA and ABPA is clinically important. While patients with ASA can often be managed with inhaled corticosteroids alone, ABPA typically requires systemic antifungal therapy.16 In fact, if the diagnostic steps are not strictly followed, ABPA can easily be misdiagnosed as ASA.34 It is possible that many patients with ASA actually have ABPA and have been incorrectly labeled as having ASA. Once glucocorticoids are administered, IgE levels drop rapidly. If IgE levels are checked during these stages, patients with ABPA are mislabeled as having ASA. If we categorize the patients in the study based on the minimum diagnostic criteria for ABPA (IgE > 500 IU/mL), it is possible that more ASA patients would meet the criteria for ABPA.8 Fungal colonization load may occur in the absence of IgE sensitization, a condition known as fungal bronchitis. Fungal bronchitis can be characterized by chronic cough phlegm, asthma control and lung function decline, oral azole drug treatment is effective. Total IgE evidence associated with the severity of disease is limited, but it is still widely used to distinguish between ABPA and fungal sensitization diagnosis of main mark.35 Our study indicates that serum EDN is comparable to total IgE in differentiating ABPA from ASA.
Despite established diagnostic criteria, ABPA remains underdiagnosed, primarily due to its overlap with ASA and limited clinical awareness. Therefore, it is crucial to seek reliable tests or biomarkers for the diagnosis of ABPA to prevent overdiagnosis and missed diagnosis. But as far as we know, there are no studies in the current literature on the role of EDN in the diagnosis of ABPA and the relationship between EDN and hematological parameters. In our study, serum EDN at a cut-off value >96.26 ng/mL demonstrated 83.3% sensitivity, 80.0% specificity, and an AUC of 0.844 in differentiating ABPA from ASA. Additionally, Spearman correlation analysis revealed that EDN was significantly positively correlated with total IgE, blood eosinophil counts, and A. fumigatus-specific IgE levels. These findings suggest that serum EDN is comparable to total IgE in distinguishing ABPA from ASA, and may offer greater stability than eosinophil counts as a diagnostic marker. The clinical utility of EDN, however, must be interpreted in the context of disease prevalence. The current study employed a case-control design in which the proportion of ABPA patients among the asthma and ABPA groups (~46%) was artificially enriched compared to real-world settings. The prevalence of ABPA among adults with asthma is approximately 11%, and can reach as high as 37% in asthmatic individuals sensitized to Aspergillus.4 Under these real-world prevalence conditions, the positive predictive value (PPV) of the EDN cutoff would be lower than that observed in our enriched sample, despite its favorable sensitivity and specificity. Therefore, in routine clinical practice, EDN results should be interpreted alongside clinical, serological, and radiological findings. Validation in prospective cohorts reflecting true disease prevalence is warranted to confirm the clinical applicability of EDN in ABPA diagnosis.
Therefore, in view of the increasing prevalence of ABPA, we recommend more research on the role of EDN in the diagnosis of ABPA. The main advantage of this study was that we are the first study to investigate serum EDN in asthma-related ABPA. In summary, we compared the EDN of ABPA with that of asthma patients and correlated the EDN with basic hematological parameters. We found that the serum EDN level in patients with ABPA was significantly elevated, comparable to the total serum IgE level, and could be used as a marker to distinguish ABPA from fungal sensitized asthma. Therefore, more research is necessary to investigate the potential of EDN as a simple, inexpensive, and widely applied biomarker. Monitoring serum EDN levels may serve as a supplementary tool for clinical diagnosis and screening of ABPA patients, which will provide additional meaningful indicators for clinical assessment and scientific research.
A key concern was whether EDN provides information beyond established markers. The correlation matrix (Figure S1) shows that EDN strongly correlated with eosinophil counts (ρ= 0.73) and A. fumigatus-IgE (ρ= 0.70), but shared variance was only 53% and 49%, respectively, indicating EDN is not entirely redundant. EDN also correlated with bronchiectasis (ρ= 0.40), a clinically important outcome less strongly associated with eosinophils (ρ= 0.54) and IgE (ρ= 0.26). No significant correlations with age, sex, or BMI suggest minimal confounding. While these findings suggest EDN may capture unique aspects of ABPA, multivariable analysis was not feasible due to sample size limitations. Larger studies are needed to confirm independent diagnostic value.
Our study has several limitations. First, the small sample size and single-center design may introduce bias and limit generalizability. Second, the exclusion of patients using corticosteroids, while necessary to assess native EDN levels, means our cohort does not reflect real-world populations where ICS is standard. Third, the EDN cutoff (96.26 ng/mL) was derived and evaluated in the same dataset, potentially yielding optimistic diagnostic estimates, and lacked internal or external validation. Despite these limitations, the study has notable strengths, including patient groups with detailed characterization, controls matched for age, and rigorous statistical correction for multiple comparisons. Our findings provide a strong rationale for future multi‑center studies with larger, independent cohorts to validate the diagnostic utility of EDN in ABPA and to explore its role in different disease stages and treatment contexts.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Natural Science Foundation of Shandong Provincial (ZR2025QC931), the National Natural Science Foundation of China (82270032, 82470028), and the Jinan Clinical Medicine Research Program for Respiratory Disease (Grant No. 202132002).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Shah A, Panjabi C. Allergic bronchopulmonary aspergillosis: a perplexing clinical entity. Allergy Asthma Immunol Res. 2016;8(4):282–10. doi:10.4168/aair.2016.8.4.282
2. Hinson KF, Moon AJ, Plummer NS. Broncho-pulmonary aspergillosis; a review and a report of eight new cases. Thorax. 1952;7(4):317–333. doi:10.1136/thx.7.4.317
3. Tiew PY, Lim AYH, Keir HR, et al. High frequency of allergic bronchopulmonary aspergillosis in bronchiectasis-COPD overlap. Chest. 2022;161(1):40–53. doi:10.1016/j.chest.2021.07.2165
4. Agarwal R, Muthu V, Sehgal IS, et al. Prevalence of Aspergillus sensitization and allergic bronchopulmonary aspergillosis in adults with bronchial asthma: a systematic review of global data. J Allergy Clin Immunol Pract. 2023;11(6):1734–51e3. doi:10.1016/j.jaip.2023.04.009
5. Agarwal R, Chakrabarti A, Shah A, et al. Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria. Clin Exp Allergy. 2013;43(8):850–873. doi:10.1111/cea.12141
6. Rosenberg M, Patterson R, Mintzer R, Cooper BJ, Roberts M, Harris KE. Clinical and immunologic criteria for the diagnosis of allergic bronchopulmonary aspergillosis. Ann Intern Med. 1977;86(4):405–414. doi:10.7326/0003-4819-86-4-405
7. Asano K, Hebisawa A, Ishiguro T, et al. New clinical diagnostic criteria for allergic bronchopulmonary aspergillosis/mycosis and its validation. J Allergy Clin Immunol. 2021;147(4):1261–8e5. doi:10.1016/j.jaci.2020.08.029
8. Agarwal R, Sehgal IS, Muthu V, et al. Revised ISHAM-ABPA working group clinical practice guidelines for diagnosing, classifying and treating allergic bronchopulmonary aspergillosis/mycoses. Eur Respir J. 2024;63(4):2400061. doi:10.1183/13993003.00061-2024
9. Muthu V, Singh P, Choudhary H, et al. Diagnostic cutoffs and clinical utility of recombinant Aspergillus fumigatus antigens in the diagnosis of allergic bronchopulmonary aspergillosis. J Allergy Clin Immunol Pract. 2020;8(2):579–587. doi:10.1016/j.jaip.2019.08.041
10. Agarwal R. Severe asthma with fungal sensitization. Curr Allergy Asthma Rep. 2011;11(5):403–413. doi:10.1007/s11882-011-0217-4
11. Okada N, Yamamoto Y, Oguma T, et al. Allergic bronchopulmonary aspergillosis with atopic, nonatopic, and sans asthma-Factor analysis. Allergy. 2023;78(11):2933–2943. doi:10.1111/all.15820
12. Muniz VS, Silva JC, Braga YAV, et al. Eosinophils release extracellular DNA traps in response to Aspergillus fumigatus. J Allergy Clin Immunol. 2018;141(2):571–85e7. doi:10.1016/j.jaci.2017.07.048
13. Chen H, Zhang X, Zhu L, et al. Clinical and immunological characteristics of -sensitized asthma and allergic bronchopulmonary aspergillosis. Front Immunol. 2022;13:939127. doi:10.3389/fimmu.2022.939127
14. Asano K, Ueki S, Tamari M, Imoto Y, Fujieda S, Taniguchi M. Adult-onset eosinophilic airway diseases. Allergy. 2020;75(12):3087–3099. doi:10.1111/all.14620
15. Agarwal R, Aggarwal AN, Garg M, Saikia B, Chakrabarti A. Cut-off values of serum IgE (total and A. fumigatus-specific) and eosinophil count in differentiating allergic bronchopulmonary aspergillosis from asthma. Mycoses. 2014;57(11):659–663. doi:10.1111/myc.12214
16. Agarwal R, Muthu V, Sehgal IS. Clinical manifestation and treatment of allergic bronchopulmonary Aspergillosis. Semin Respir Crit Care Med. 2024;45(1):114–127. doi:10.1055/s-0043-1776912
17. Kim CK, Callaway Z, Pawankar R. Eosinophil granule proteins as a biomarker in managing asthma and allergies. Asia Pac Allergy. 2023;13:66–71. doi:10.5415/apallergy.0000000000000104
18. Malik A, Batra JK. Antimicrobial activity of human eosinophil granule proteins: involvement in host defence against pathogens. Crit Rev Microbiol. 2012;38(2):168–181. doi:10.3109/1040841X.2011.645519
19. Kunc P, Pokusa M, Hajduchova D, et al. Biomarkers reflecting the severity of bronchial asthma in children. J Asthma Allergy. 2024;17:1227–1237. doi:10.2147/JAA.S486958
20. Thulin H, Mansouri L, Altman M, et al. Biomarkers for a less invasive strategy to predict children with eosinophilic esophagitis. Allergy. 2024;79(12):3464–3474. doi:10.1111/all.16275
21. Zhang Y, Liu Z, Yuan F, Huang X, Wu D. Distinct inflammatory patterns and nasal bacterial dysbiosis in uncontrolled chronic rhinosinusitis. Eur Arch Otorhinolaryngol. 2025;282(6):3085–3096. doi:10.1007/s00405-025-09376-y
22. Taniuchi S, Chihara J, Kojima T, Yamamoto A, Sasai M, Kobayashi Y. Serum eosinophil derived neurotoxin may reflect more strongly disease severity in childhood atopic dermatitis than eosinophil cationic protein. J Dermatol Sci. 2001;26(1):79–82. doi:10.1016/S0923-1811(00)00151-1
23. Kwon N, Pizzichini E, Bansal AT, et al. Factors that affect blood eosinophil counts in a non-asthmatic population: post hoc analysis of data from Brazil. World Allergy Organ J. 2020;13(5):100119. doi:10.1016/j.waojou.2020.100119
24. Keown K, Abbott S, Kuzeljevic B, Rayment JH, Chilvers MA, Yang CL. An investigation into biomarkers for the diagnosis of ABPA and aspergillus disease in cystic fibrosis. Pediatr Pulmonol. 2019;54(11):1787–1793. doi:10.1002/ppul.24465
25. Skov M, Koch C, Reimert CM, Poulsen LK. Diagnosis of allergic bronchopulmonary aspergillosis (ABPA) in cystic fibrosis. Allergy. 2000;55(1):50–58. doi:10.1034/j.1398-9995.2000.00342.x
26. Wark PA, Saltos N, Simpson J, Slater S, Hensley MJ, Gibson PG. Induced sputum eosinophils and neutrophils and bronchiectasis severity in allergic bronchopulmonary aspergillosis. Eur Respir J. 2000;16(6):1095–1101. doi:10.1034/j.1399-3003.2000.16f13.x
27. Gleich GJ, Adolphson CR. The eosinophilic leukocyte: structure and function. Adv Immunol. 1986;39:177–253. doi:10.1016/s0065-2776(08)60351-x
28. Rutten B, Young S, Rhedin M, et al. Eosinophil-derived neurotoxin: a biologically and analytically attractive asthma biomarker. PLoS One. 2021;16(2):e0246627. doi:10.1371/journal.pone.0246627
29. Durrington HJ, Gioan-Tavernier GO, Maidstone RJ, et al. Time of day affects eosinophil biomarkers in asthma: implications for diagnosis and treatment. Am J Respir Crit Care Med. 2018;198(12):1578–1581. doi:10.1164/rccm.201807-1289LE
30. Kang YR, Kim H, Lee CE, et al. Serum and urine eosinophil-derived neurotoxin (EDN) levels predict biologic response in severe asthma. World Allergy Organ J. 2025;18(1):100990. doi:10.1016/j.waojou.2024.100990
31. Malinovschi A, Rydell N, Fujisawa T, Borres MP, Kim CK. Clinical potential of eosinophil-derived neurotoxin in asthma management. J Allergy Clin Immunol Pract. 2023;11(3):750–761. doi:10.1016/j.jaip.2022.11.046
32. Agarwal R, Aggarwal AN, Gupta D, et al. Aspergillus hypersensitivity and allergic bronchopulmonary aspergillosis in patients with bronchial asthma: systematic review and metanalysis. Int J Tubercul Lung Dis. 2009;13:936–944.
33. Greenberger PA, Miller TP, Roberts M, et al. Allergic bronchopulmonary aspergillosis in patients with and without evidence of bronchiectasis. Ann Allergy. 1993;70:333–338.
34. Vicencio AG, Muzumdar H, Tsirilakis K, et al. Severe asthma with fungal sensitization in a child: response to itraconazole therapy. Pediatrics. 2010;125:e1255–8. doi:10.1542/peds.2009-2443
35. Rick EM, Woolnough K, Pashley CH, Wardlaw AJ. Allergic fungal airway disease. J Investig Allergol Clin Immunol. 2016;26(6):344–354. doi:10.18176/jiaci.0122
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.