Back to Journals » Clinical Ophthalmology » Volume 19
Enhancing Phacoemulsification Safety: How Low Fluidic Settings Influence Active Surge Mitigation Actuation
Authors Kuzmanović Elabjer B ![]() , Štrbac T
, Štrbac T ![]() , Ćubela I
, Ćubela I ![]() , Bušić M, Bjeloš M
, Bušić M, Bjeloš M
Received 12 May 2025
Accepted for publication 27 August 2025
Published 11 September 2025 Volume 2025:19 Pages 3331—3338
DOI https://doi.org/10.2147/OPTH.S539817
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Biljana Kuzmanović Elabjer,1– 3 Tea Štrbac,1 Iva Ćubela,1 Mladen Bušić,1– 3 Mirjana Bjeloš1– 3
1University Eye Department, University Hospital “Sveti Duh”, Zagreb, Croatia; 2Faculty of Medicine Osijek, University Josip Juraj Strossmayer in Osijek, Osijek, Croatia; 3Faculty of Dental Medicine and Health Osijek, University Josip Juraj Strossmayer in Osijek, Osijek,Croatia
Correspondence: Tea Štrbac, Email [email protected]
Introduction: Active Surge Mitigation (ASM) is a feature of the Centurion Vision System ACTIVE SENTRY® Handpiece designed to minimize post-occlusion surge by dynamically adjusting fluidics. Stable anterior chamber conditions are critical during phacoemulsification, and low intraocular pressure (IOP) fluidics may enhance surgical safety by reducing stress on ocular tissues. This study evaluated demographic, biometric, and intraoperative factors influencing ASM activation during phacoemulsification at low IOP settings (30 mmHg), a vacuum of 575 mmHg, and an aspiration flow of 28 cc/min.
Methods: This retrospective study was conducted at the University Eye Clinic, University Hospital “Sveti Duh” in Zagreb, Croatia, between January 19 and April 12, 2024. Preoperative parameters included age, gender, biometric data from the Zeiss IOL Master 700, and lens hardness, classified according to the Lens Opacities Classification System (LOCS III). The presence of Pseudoexfoliation Syndrome (PEX) and Intraoperative Floppy Iris Syndrome (IFIS) was noted. Intraoperative metrics recorded were total case time, cumulative dissipated energy (CDE), ultrasound time (U/S time), and the number of ASM actuations.
Results: ASM actuations were not normally distributed (median = 1; mean = 2.4). Significant positive correlations were identified with age (P = 0.014), lens thickness (P = 0.039), and U/S time (P = 0.015), while no significant differences were observed for anterior chamber depth (ACD), gender, PEX, or IFIS. Logistic regression identified age as a predictor of ASM values ≥ 1.
Conclusion: At low IOP settings, surge events during phacoemulsification are rare. ASM activation is influenced by patient age, lens thickness, and U/S time but not by ACD, gender, PEX, or IFIS. Low IOP fluidics combined with ASM contributes to stable and safe chamber dynamics across diverse patient profiles.
Keywords: low IOP settings, active sentry handpiece, ASM actuation, surge events
Introduction
Phacoemulsification, the gold standard for cataract surgery, continues to enhance surgical efficiency while maintaining and improving patient safety.1 Until recently, gravity fluidic systems were the only option for phacoemulsification, with irrigation flow rates dependent on the height of the fluid bottle. Raising the bottle height can help reduce post-occlusion surges, but it also increases the infusion of the irrigation fluid, leading to elevated and fluctuating intraocular pressure (IOP). These temporary IOP spikes can cause corneal edema, significant endothelial cell loss, and retinal injury.2,3 Low IOP fluidic settings offer many advantages over the high IOP settings.4 However, maintaining a lower intraocular pressure can lead to an unstable anterior chamber depth (ACD) and a higher risk of post-occlusion surge.2,5 Active Fluidics™ Technology with ACTIVE SENTRY® Handpiece of the Centurion Vision System uses an integrated pressure sensor to detect real-time fluctuations making low IOP fluidic settings safer.6 During surgery, the sensor can prevent or mitigate a surge events with its engagement recorded as ASM (Active Surge Mitigation) actuations.
We selected the Centurion Vision System with ACTIVE SENTRY® for this study because of its unique combination of real-time sensor feedback and advanced surge mitigation, which are not universally present in other platforms. While other phacoemulsification machines—such as the Whitestar Signature Pro (Johnson & Johnson Vision) with Fusion Fluidics and the Stellaris Elite (Bausch + Lomb)—have integrated forms of active fluidics or pressurized infusion, the Centurion’s dual feedback mechanism and documented safety profile make it a benchmark for studying low IOP surgery.
Our study aimed to evaluate anterior chamber stability during phacoemulsification using the handpiece with a built-in pressure sensor with low IOP fluidic setting, recording the number of ASM actuation. Additionally, we analyzed the association of demographic and biometric factors, lens hardness, and the presence of complicating conditions such as pseudoexfoliation (PEX) and intraoperative floppy iris syndrome (IFIS), with ASM actuations.
To our knowledge, although some studies have examined the clinical benefits of low IOP settings, comprehensive analyses of real-time ASM actuation with ACTIVE SENTRY® remain limited. This study aims to bridge that gap, providing new evidence on how active fluidic control enhances both efficiency and patient safety.
Materials and Methods
This retrospective study included 211 eyes of patients of both genders who underwent phacoemulsification at the University Eye Clinic, University Hospital “Sveti Duh” in Zagreb, Croatia, between January 19 and April 12, 2024. The study period of four months was chosen to include a continuous series of consecutive cases performed after the implementation of low IOP fluidic settings and the ACTIVE SENTRY® Handpiece in our clinic. The study group enrolled all patients undergoing cataract surgery during this period without exclusion criteria.
Preoperative and intraoperative parameters were analyzed. Preoperative parameters included demographic information, such as age and gender, and biometric measurements obtained using the Zeiss IOL Master 700, which measured anterior chamber depth (ACD/mm), lens thickness (LT/mm), and axial length (AL/mm). Lens hardness was graded using the Lens Opacities Classification System III (LOCS III), and the presence of pseudoexfoliation (PEX) and intraoperative floppy iris syndrome (IFIS) was noted. All preoperative assessments (LOCS III, PEX, and IFIS) were performed by the operating surgeon (BKE). Intraoperative parameters recorded were total case time, cumulative dissipated energy (CDE), total ultrasound time (U/S time), and the number of ASM actuations. The refractive power of the implanted IOL was documented. All procedures were performed by a single experienced surgeon (BKE) using the Centurion Vision System (Alcon, Fort Worth, TX) equipped with the ACTIVE SENTRY® Handpiece with integrated pressure sensor. All cases were performed using the same standardized low fluidic settings: infusion pressure of 30 mmHg, bottle height of 41 cm, vacuum of 575 mmHg, and aspiration flow rate of 28 cc/min, regardless of cataract grade. Postoperative outcomes were analyzed retrospectively, with follow-up data collected at one month after surgery for all patients. For patients with IFIS or PEX, data were reviewed for an extended period of three months to ensure comprehensive assessment due to their increased risk of postoperative complications.
Statistical analysis was performed using IBM SPSS version 25.0 (IBM Corp), including descriptive statistics, bivariate analysis, and logistic regression modeling. A p-value of 0.05 or less was considered statistically significant.
Ethical Considerations
This retrospective study was conducted at the University Eye Department, University Hospital “Sveti Duh”, Zagreb, Croatia. Ethical approval was obtained from the Institutional Review Board of University Hospital “Sveti Duh”. The requirement for patient informed consent was waived by the ethics committee due to the retrospective nature of the study, which involved the analysis of anonymized data collected during routine clinical care. No identifiable patient information was used, and no experimental treatments or interventions were performed. The study was conducted in accordance with the ethical standards of the institutional and national research committee and with the 1964 Declaration of Helsinki and its later amendments. All patient data were handled with strict confidentiality and data protection protocols.
Results
The study cohort included participants aged between 39 and 98 years, with a median age of 73. Among the 211 eyes, 62.6% were from female participants and 37.4% from male participants. Preoperative assessments showed that the most common LOCS III score was 3.0 (35.1% of participants), with 24.2% having a score of 4.0 (Figure 1). PEX was observed in 8.1% of participants, while IFIS was present in 10.0%. No major intraoperative complications (eg, posterior capsule rupture, vitreous loss) were recorded during the study period. In the PEX group, two cases of lens subluxation were observed. Both were successfully managed with the use of iris retractors to stabilize the capsule and the implantation of capsular tension rings during lens removal.
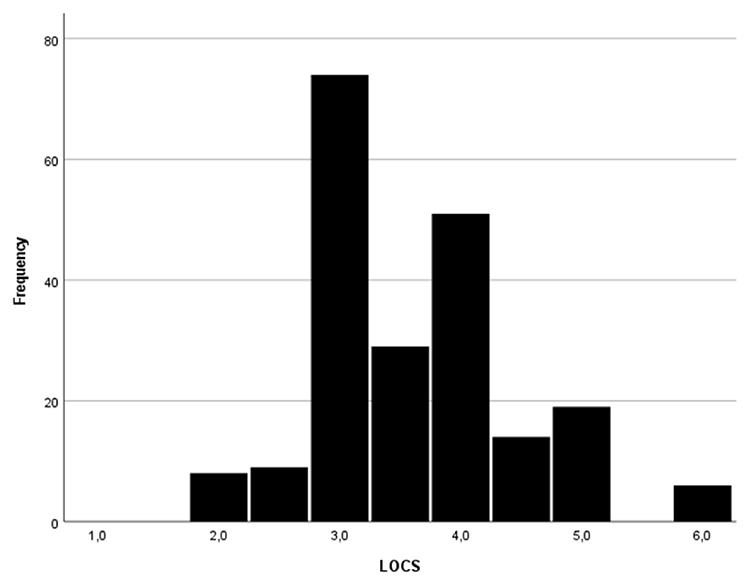 |
Figure 1 Distribution of Lens Opacities Classification System (LOCS) scores in the study population. The histogram shows the frequency of each LOCS grade. |
Intraoperative evaluations revealed ASM actuation values ranged from 0 to 26, with a median of 1.0. One-Sample Kolmogorov–Smirnov (K-S) test was performed to evaluate the distribution of ASM actuation values, revealing a significant deviation from normal distribution (Figure 2). Detailed descriptive analyses of anterior chamber depth, axial length, lens thickness, intraocular lens power, case duration, cumulative dissipated energy, and ultrasound time are provided in Tables 1 and 2. Spearman correlation analysis showed positive correlations of ASM with age (rho=0.169. P=0.014), lens thickness (rho=0.143. P=0.039) and ultrasound time (rho=0.168, P=0.015) (Table 3). These results suggest that older age, increased lens thickness and prolonged ultrasound time may be associated with more frequent engagement of the pressure-sensing mechanism. No meaningful correlations were observed with anterior chamber depth, axial length, or IOL power.
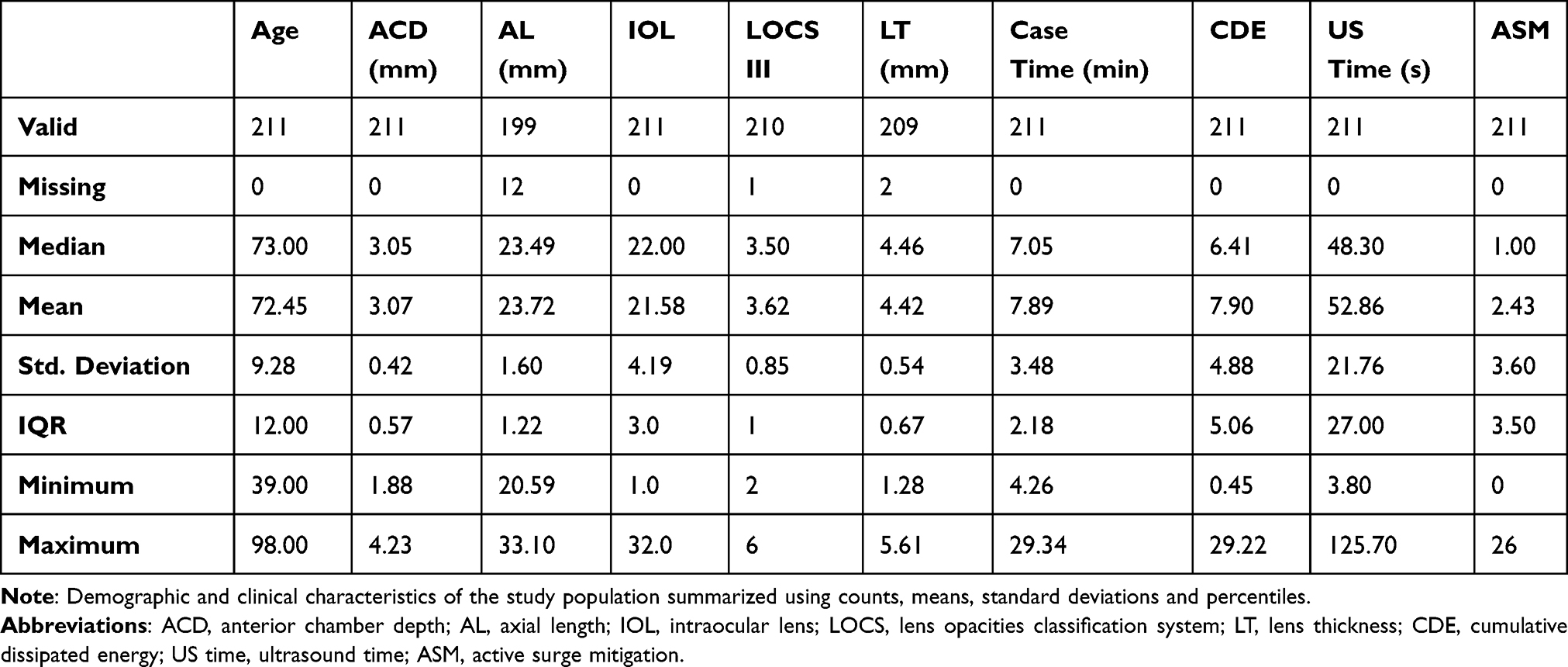 |
Table 1 Descriptive Analysis of Preoperative and Intraoperative Parameters |
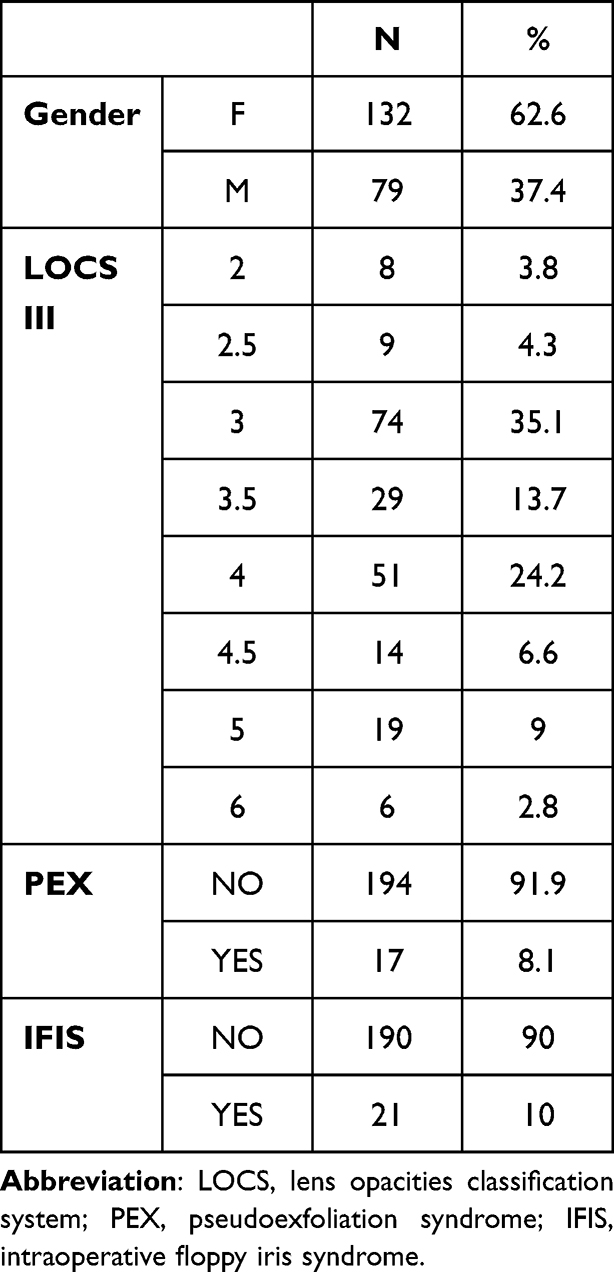 |
Table 2 Descriptive Statistics of Patient Characteristics Expressed in Percentages |
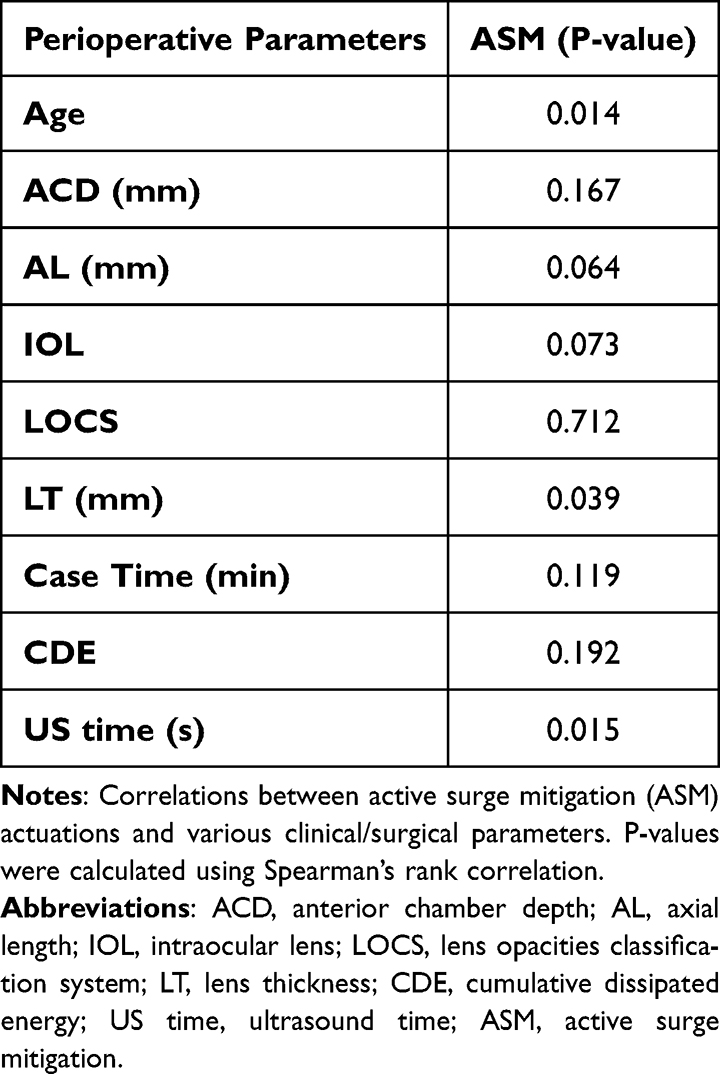 |
Table 3 Preoperative and Intraoperative Parameters in Correlation with ASM |
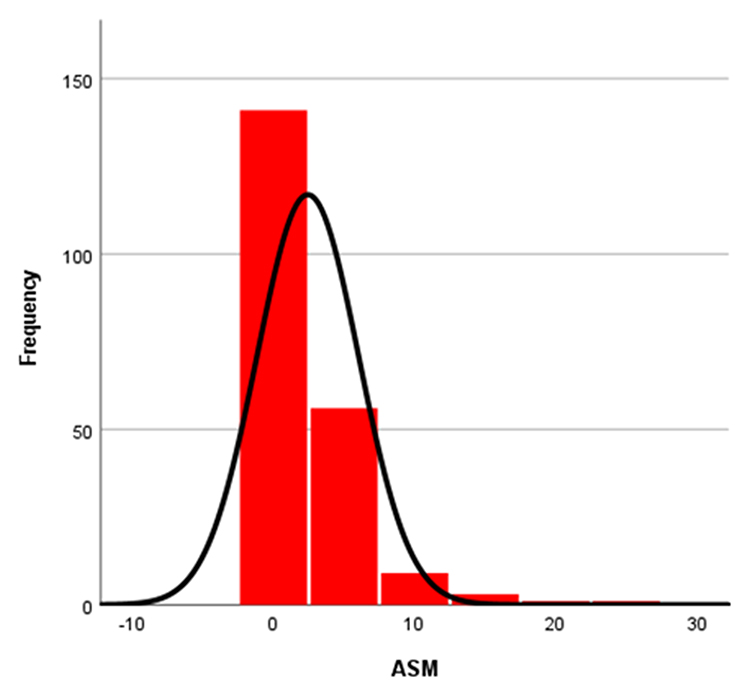 |
Figure 2 Histogram of intraoperative ASM actuation values (range: 0–26; median: 1.0) overlaid with a normal distribution curve. The One-Sample Kolmogorov–Smirnov (K-S) test indicated a significant deviation from normality (Mean = 2.4, SD = 3.6). |
The Mann–Whitney U-test revealed no significant differences in ASM numbers between genders (P=0.570), PEX (P=0.990), or IFIS (P=0.260) (Table 4).
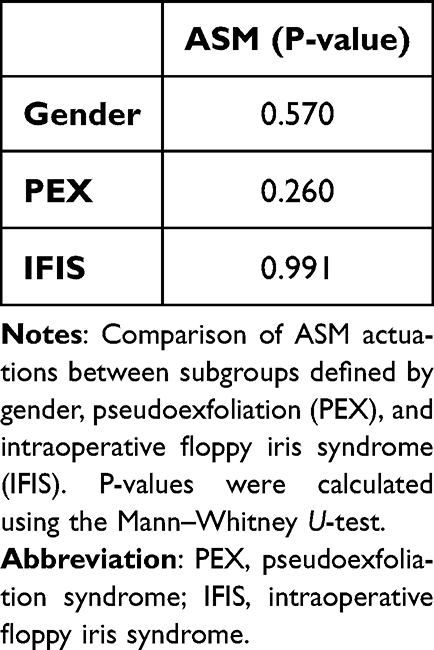 |
Table 4 Correlation Between ASM Actuations and Gender, PEX, and IFIS |
To better understand predictors of higher ASM engagement, binary logistic regression was used to create a prediction model for affiliation to a group with an ASM value ≥1. The model was statistically significant (P=0.005), explained 82% of the variance of the dependent variable (ASM), and correctly classified 66% of respondents. Age was a significant predictor, with each additional year increasing the odds of ASM values ≥1 by 4,3% (OR=1.043 (95% CI 1.005–1.082). These results are presented in Table 5.
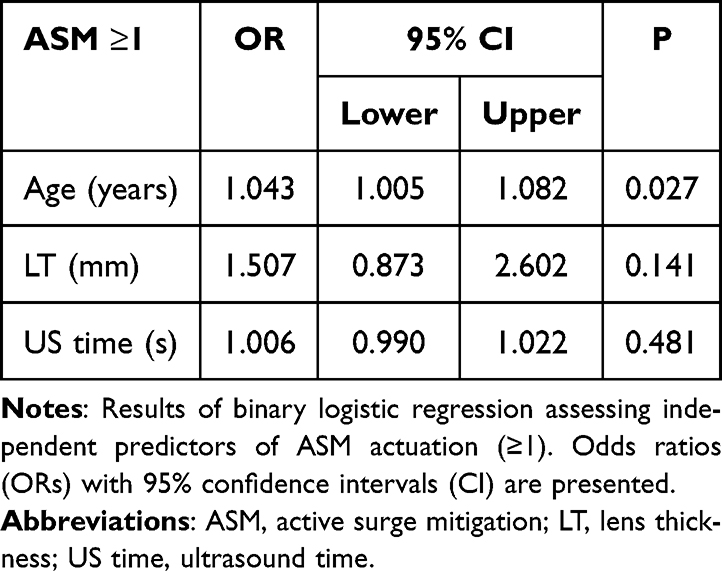 |
Table 5 The Multivariate Regression Model (Binary Logistic Regression) |
Discussion
The implementation of the CENTURION Vision System represents a significant advancement in fluidics, significantly enhancing anterior chamber stability and allowing surgeons to work with a wide range of parameter settings.7 An increasing number of surgeons now perform cataract surgery at IOP levels close to physiological values without compromising anterior chamber stability or surgical outcomes. Evidence suggests these settings can reduce postoperative corneal edema, decrease corneal endothelial cell loss, lower postoperative inflammation, and, provide better protection of the posterior segment.3,8,9
Our study aimed to identify which preoperative and intraoperative parameters significantly influence ASM actuations during phacoemulsification at low fluidic settings and to compare these findings to those under high fluidic settings. This is among the first studies to investigate the impact of these variables on ASM actuation in a low fluidic environment. The study cohort reflects our population of patients undergoing cataract surgery with a median age of 74, with nearly twice as many female patients. Lens hardness was classified using the LOCS III system, with a median value 3.5. We intentionally included patients with various risk factors and complex cataract cases to evaluate their impact on the number of ASM actuations.
Our results suggest that ASM actuation occurs less frequently at an IOP setting of 30 mmHg compared to previous observations made using a higher standard IOP setting of 48 mmHg in similar surgical conditions. At lower IOP settings, ASM activations occur less frequently because the fluidic system experiences fewer post-occlusion surge events due to reduced pressure differentials. A 2022 study reached a similar conclusion, comparing the number of surge events and the efficacy of phacoemulsification between a low IOP setting of 20 mmHg and a standard setting of 60 mmHg.10 Wang et al also revealed a lower ASM frequency at low intraoperative IOP settings; however, their study included only patients with nucleus grade 3 cataracts without any other oculopathy.11
Our findings show that key factors affecting ASM actuation include advanced age, lens thickness, and ultrasound time. Specifically, each additional year of age increased the odds ASM values ≥1 by 4.3%. These results align with a 2022 study that similarly found fewer surge events and lower total case time at lower IOP settings.10
Interestingly, previous studies showed no statistically significant difference in cumulative dissipated energy (CDE) between the two IOP settings.10,11 In our current study, the descriptive analysis revealed a median CDE of 6.41 (range 4.6–9.69), which appears higher than values reported under standard IOP settings in similar surgical contexts. This discrepancy requires further investigation to confirm the impact of lower IOP settings on CDE, as higher CDE values contribute to postoperative endothelial damage.
As observed in our previous study with standard IOP settings, there was no statistically significant correlation between PEX or IFIS and ASM actuation under low IOP settings, likely due to limited number of patients with these conditions.
This study has several limitations. First, its retrospective design may introduce selection bias and limit the ability to establish causality. Second, the sample size, while sufficient for statistical analysis, may not fully represent the broader population of patients undergoing phacoemulsification with varying lens densities and comorbidities. Third, lens hardness grading using the LOCS III system, though standardized, is semi-quantitative and subject to interobserver variability. Lastly, we did not assess postoperative outcomes such as endothelial cell loss, corneal edema, or visual recovery, which could further validate the clinical impact of ASM activation at low IOP settings.
Conclusion
Phacoemulsification at low IOP settings with an integrated pressure-sensor handpiece reduces the likelihood of surge events and improves anterior chamber stability. ASM activations increase with patient age, lens thickness, and longer ultrasound time, while anterior chamber depth, gender, PEX, and IFIS show no significant associations. These results align with previous findings under standard IOP settings and highlight the benefits of low IOP fluidics in enhancing surgical safety.
Funding
No funding or grant support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ibarz-Barberá M, Orts-Vila P, Martínez-Galdón F, Martín-García N, Tañá-Rivero P. Surgical efficiency comparison between two phacoemulsification systems. Clin Ophthalmol Auckl NZ. 2024;18:1095–1102. doi:10.2147/OPTH.S453899
2. Suzuki H, Igarashi T, Takahashi H. Effect of a new phacoemulsification and aspiration handpiece on anterior chamber stability. J Cataract Refract Surg. 2023;49(1):91–96. doi:10.1097/j.jcrs.0000000000001071
3. Liu Y, Hong J, Chen X. Comparisons of the clinical outcomes of Centurion® active fluidics system with a low IOP setting and gravity fluidics system with a normal IOP setting for cataract patients with low corneal endothelial cell density. Front Med. 2023;10:1294808. doi:10.3389/fmed.2023.1294808
4. Scarfone HA, Rodriguez EC, Rufiner MG. Vitreous-lens interface changes after cataract surgery using active fluidics and active sentry with high and low infusion pressure settings. J Cataract Refract Surg. 2024;50(4):333–338. doi:10.1097/j.jcrs.0000000000001359
5. Kang S, Park S, H N, Kwak J, K S. Real-time intraocular pressure measurement during phacoemulsification in dogs ex vivo. J Vet Med Sci. 2015;77(6):685–692. doi:10.1292/jvms.14-0412
6. Bulut A. Comparison of phacoemulsification parameters using active-fluidic pressure control system versus gravity-fluidic system. Eurasian J Med Investig. 2021. doi:10.14744/ejmi.2021.25231/
7. CRSToday | more physiologic iop in cataract surgery matters: here’s why [Internet]. 2024. Available from: https://crstoday.com/articles/more-physiologic-iop-in-cataract-surgery-matters-heres-why/more-physiologic-iop-in-cataract-surgery-matters-heres-why.
8. Vasavada AR, Praveen MR, Vasavada VA, et al. Impact of high and low aspiration parameters on postoperative outcomes of phacoemulsification: randomized clinical trial. J Cataract Refract Surg. 2010;36(4):588–593. doi:10.1016/j.jcrs.2009.11.009
9. Rauen MP, Joiner H, Kohler RA, O’Connor S. Phacoemulsification using an active fluidics system at physiologic versus high IOP: impact on anterior and posterior segment physiology. J Cataract Refract Surg. 2024;50(8):822–827. doi:10.1097/j.jcrs.0000000000001457
10. Beres H, de Ortueta D, Buehner B, Scharioth GB. Does low infusion pressure microincision cataract surgery (LIPMICS) reduce frequency of post-occlusion breaks? Romanian J Ophthalmol. 2022;66(2):135–139.
11. Wang S, Tao J, Yu X, Diao W, Bai H, Yao L. Safety and prognosis of phacoemulsification using active sentry and active fluidics with different IOP settings - a randomized, controlled study. BMC Ophthalmol. 2024;24(1):35. doi:10.1186/s12886-024-03626-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.