Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 13
Enhancing our understanding of the time course of acute exacerbations of COPD managed on an outpatient basis
Authors Oliveira A ![]() , Afreixo V
, Afreixo V ![]() , Marques A
, Marques A ![]()
Received 31 May 2018
Accepted for publication 12 September 2018
Published 20 November 2018 Volume 2018:13 Pages 3759—3766
DOI https://doi.org/10.2147/COPD.S175890
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Ana Oliveira,1–3 Vera Afreixo,3,4 Alda Marques2,3
1Faculty of Sports, University of Porto, Porto, Portugal; 2Respiratory Research and Rehabilitation Laboratory Lab3R, School of Health Sciences, University of Aveiro, Aveiro, Portugal; 3Institute for Biomedicine, iBiMED, University of Aveiro, Aveiro, Portugal; 4Center for Research and Development in Mathematics and Applications, CIDMA, University of Aveiro, Aveiro, Portugal
Purpose: Acute exacerbations of COPD (AECOPD) are associated with pulmonary/systemic changes; however, quantification of those changes during AECOPD managed on an outpatient basis and factors influencing recovery are lacking. This study aimed to characterize patients’ changes during AECOPD and identify factors influencing their recovery.
Methods: Body mass index, the modified British Medical Research Council questionnaire, number of exacerbations in the previous year, and the Charlson comorbidity index (independent variables) were collected within 24–48 hours of hospital presentation (T0). Peripheral oxygen saturation (SpO2), forced expiratory volume in one second, percentage predicted (FEV1% predicted), maximum inspiratory pressure, quadriceps muscle strength, 5 times sit-to-stand, and COPD assessment test (CAT) (dependent variables) were collected at T0 and approximately at days 8 (T1), 15 (T2), and 45 (T3) after T0.
Results: A total of 44 outpatients with AECOPD (31♂; 68.2±9.1 years; 51.1±20.3 FEV1% predicted) were enrolled. All variables improved overtime (P<0.05); however, at day 8, only SpO2 and CAT (P≤0.001) showed significant improvements. Changes in FEV1% predicted and SpO2 were not influenced by any independent measure, while changes in other outcome measures were influenced by at least one of the independent measures. Independently of the time of data collection, being underweight or overweight and having increased dyspnea, previous exacerbations, and severe comorbidities negatively affected patients’ outcomes.
Conclusion: FEV1% predicted and SpO2 were not influenced by any independent measure and, thus, seem to be robust measures to follow-up outpatients with AECOPD. No single indicator was able to predict patients’ recovery for all measures; thus, a comprehensive assessment at the onset of the AECOPD is required to personalize interventions.
Keywords: COPD exacerbations, management, outcome measures, outpatients
Introduction
COPD is frequently punctuated by acute exacerbations (acute exacerbations of COPD [AECOPD]), which account for more than half of the hospitalizations1 in COPD and are the main responsible for patients’ clinical deterioration and increased health care costs.2 Globally, more than 50% of COPD-related costs are due to AECOPD3 and in USA, costs are estimated in $7.100 per patient/exacerbation.4
Long-term consequences of AECOPD are known, such as clinical important physiological and functional deteriorations,2 resulting in significant declines in lung function, muscle strength, and quality of life and increased mortality.2,5 AECOPD are also responsible for significant patients’ clinical deterioration during its time course; however, most of the information available is on lung function and dyspnea6–8 in hospitalized patients.5,7,9–11 Little information is still available on more functional parameters, such as muscle strength, activities of daily living, and impact of the disease. Moreover, hospitalized patients differ from outpatients not only in their management but also in the disease severity,12 which may influence their pattern of recovery. Thus, understanding outpatients’ recovery seems crucial to timely manage and appropriately plan their follow-ups.
Factors associated with the progression and prognosis of AECOPD during hospitalizations have already been studied and include patients’ anthropometrics, stage of the disease (according to dyspnea and number of AECOPD in the previous year), severity of comorbidities, and acute physiological derangements.13 Such information is essential to design management strategies and discharge plans during hospital stay. However, more than 80% of AECOPD are managed on an outpatient basis12 and knowledge on factors influencing the time course of AECOPD managed in this setting is scarce. This unawareness impairs the standardization, optimization, and personalization of the treatment and ultimately contributes to the existing high rate of AECOPD relapses.14
This study aimed to characterize patients’ lung function, oxygen saturation, muscles strength, impact of the disease, and functionality during the time course of AECOPD managed on an outpatient basis. Additionally, it was aimed to identify the factors influencing this recovery period.
Methods
Study design and participants
A longitudinal observational study was conducted in nonhospitalized patients with AECOPD recruited from the urgent care of a Central Hospital. Inclusion criteria were the diagnosis of an AECOPD according to the GOLD criteria.12 Exclusion criteria were hospitalization (defined as the need to be admitted as an inpatient at the respiratory or intensive care unit for further assessment/treatment after consultation with the urgency clinician); patients requiring emergency intubation and/or mechanical ventilation; and patients with compromised neurological status or hemodynamic instability or presence of severe co-existing respiratory, neurological (eg, Parkinson’s disease), cardiac (eg, uncontrolled symptomatic heart failure), musculoskeletal (eg, kyphoscoliosis), or signs of psychiatric impairments. Eligible patients were identified by clinicians and contacted by the researchers to schedule an appointment within 48 hours of the hospital visit.
Approval was obtained from the ethics committee of the Centro Hospitalar do Baixo Vouga (13NOV’1514:40065682) and from the National Data Protection Committee (8828/2016). Written informed consent was obtained before data collection.
Sample size
In order to test the time effect (four measurements) over quantitative variables, a sample size estimation was performed to detect moderate effect sizes (f=0.25) as significant, with 80% power, 5% significance level. The minimum sample size estimated was 35 participants. In health-related longitudinal studies, dropout rates are of approximately 20%–45%;15,16 thus, 44 participants with AECOPD were aimed to be recruited.
Data collection
Patients were asked to attend to the following four assessment sessions: within 48 hours of the urgent care visit (T0, exacerbation onset) and approximately 8 days (T1, during exacerbation), 15 days (T2, following exacerbation),7 and 45 days after the hospital visit (T3, at stability postexacerbation). Data were collected at the urgent care, in the facilities of the University of Aveiro, or at patients’ home.
Sociodemographic (age and gender), anthropometric (height, weight, and body mass index [BMI]), and general clinical (smoking habits, number of exacerbations in the previous year, medication, comorbidities, and dyspnea) data were first collected. The severity of comorbid diseases was recorded and scored according to the Charlson comorbidity index (CCI).17 Dyspnea was assessed with the modified British Medical Research Council (mMRC) questionnaire.18
In each data collection moment, peripheral oxygen saturation (SpO2), collected with a pulse oximeter (Pulsox 300i; Konica Minolta, Tokyo, Japan), lung function, respiratory muscle strength, quadriceps muscle strength (QMS), impact of the disease, and functionality were collected by a physiotherapist following the described standardized order.
Impact of the disease was measured with the COPD assessment test (CAT), a disease-specific questionnaire with eight items (ie, cough, sputum, chest tightness, breathlessness going up hills/stairs, activity limitations at home, confidence leaving home, sleep, and energy).23
Lung function was assessed with a portable spirometer (MicroLab 3535; CareFusion, Kent, UK),19 and respiratory muscle strength was measured at the mouth as maximum inspiratory pressure (PImax) using an electronic pressure transducer (MicroRPM; Micromedical, Kent, UK)20 according to the European Respiratory Society and American Thoracic Society guidelines.
QMS was measured as quadriceps peak torque during an isometric contraction of the quadriceps of the dominant side with a handheld dynamometer (microFET2; Hoggan Health, Salt Lake City, Utah).21 The best of three acceptable and reproducible maneuvers was considered for analysis. Quadriceps peak torque was calculated in the percentage of predicted (QMS% predicted).22
Functionality was assessed with the 5 times sit-to-stand test (5STS). A straight-backed armless chair with a hard seat stabilized against a wall was used, and the protocol of Jones et al24 was followed. The best of three acceptable and reproducible maneuvers was considered for analysis.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics 24.0 (IBM Corporation, Armonk, NY, USA), and plots were created using GraphPad Prism 5.01 (GraphPad Software, Inc., La Jolla, CA, USA). The level of significance was set at 0.05.
Descriptive statistics was used to describe the sample. The evolution of each dependent variable during AECOPD and the identification of variables that could influence the evolution of the dependent variables were analyzed with generalized estimating equation’ (GEE) models with a gama link function and independent correlation structure. This method is an extension of generalized linear models to longitudinal data permitting the inclusion of time-dependent variables and the analysis of incomplete data (without imputing missing data), common in longitudinal health studies.25
To explore the influence of time independently, a first analysis was performed using SpO2, FEV1 percentage predicted (FEV1% predicted), PImax, QMS% predicted, CAT, and 5STS as dependent variables and time as the only independent variable. Then, to identify variables that could influence the evolution of the dependent variables, BMI (ie, underweight <18.50, normal weight <24.99, and overweight ≥25.00),26 number of exacerbations in the previous year (ie, 0–1 and ≥2),17 comorbidities (mild: CCI ≤2, moderate: CCI ≤4, and severe: CCI ≥5),17 and dyspnea (mild: mMRC <2 and severe: mMRC ≥2)12 were included as independent variables. A clinical criterion was used to select the dependent and independent variables included in the models (variables commonly reported and associated with the response to treatments in COPD and with AECOPD in the literature).13,27–29
Results
Participants
Seventy-eight nonhospitalized patients with AECOPD were referred for possible inclusion in the study. Of whom, 34 patients were excluded because at T0 they had a pulmonary function and clinical history incompatible with a diagnosis of COPD (n=22), did not meet the definition for AECOPD (n=1), presented lung neoplasia (n=2) and severe heart failure (n=1), were unable to comply with testing (n=3), and showed decline to participate in the study (n=5). Forty-four nonhospitalized patients with AECOPD (31♂; 68.18±9.09 years; 51.11±20.27 FEV1% predicted) were invited and agreed to participate in the study. Participants’ characteristics are summarized in Table 1.
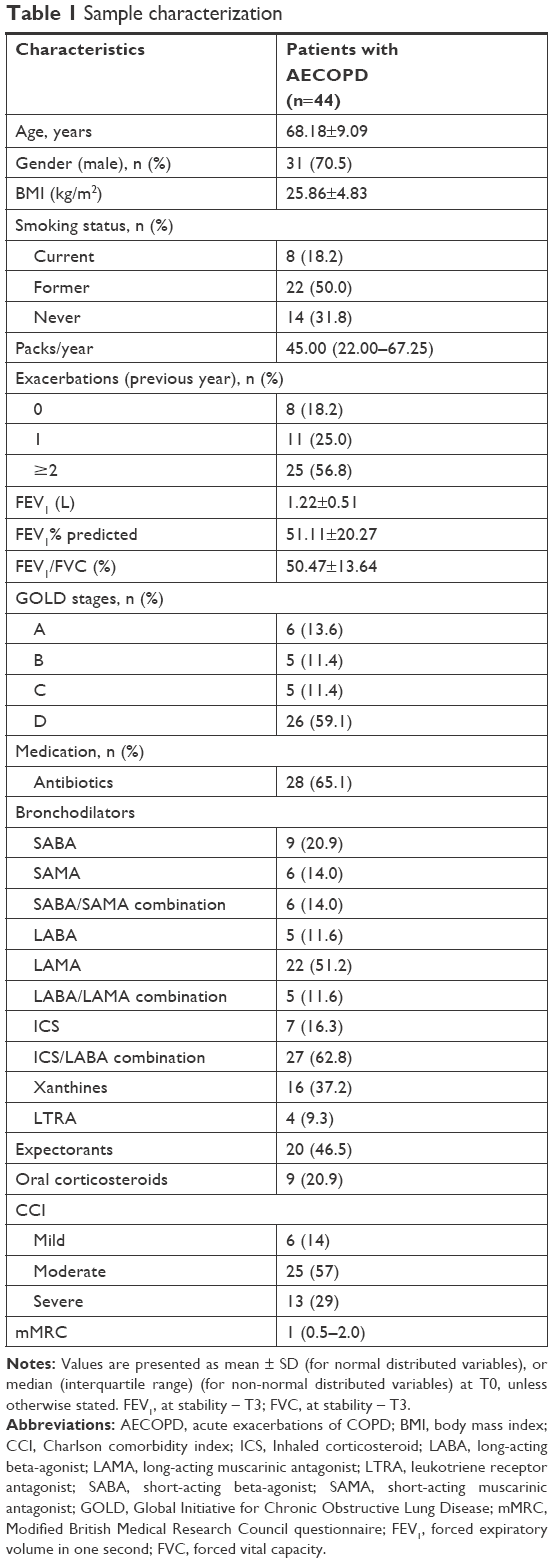 | Table 1 Sample characterization |
Time course of AECOPD
The variation of each variable within the time course of the AECOPD is found in Figure 1. At day 8, only SpO2 and CAT (P≤0.001) have shown significant improvements. At day 15, FEV1% predicted (P=0.007) and 5STS (P<0.001) had improved from the onset of the AECOPD and at day 45, all variables presented significant improvements (P<0.05). A detailed description of the variables analyzed per moment of data collection is found in Tables S1 and S2.
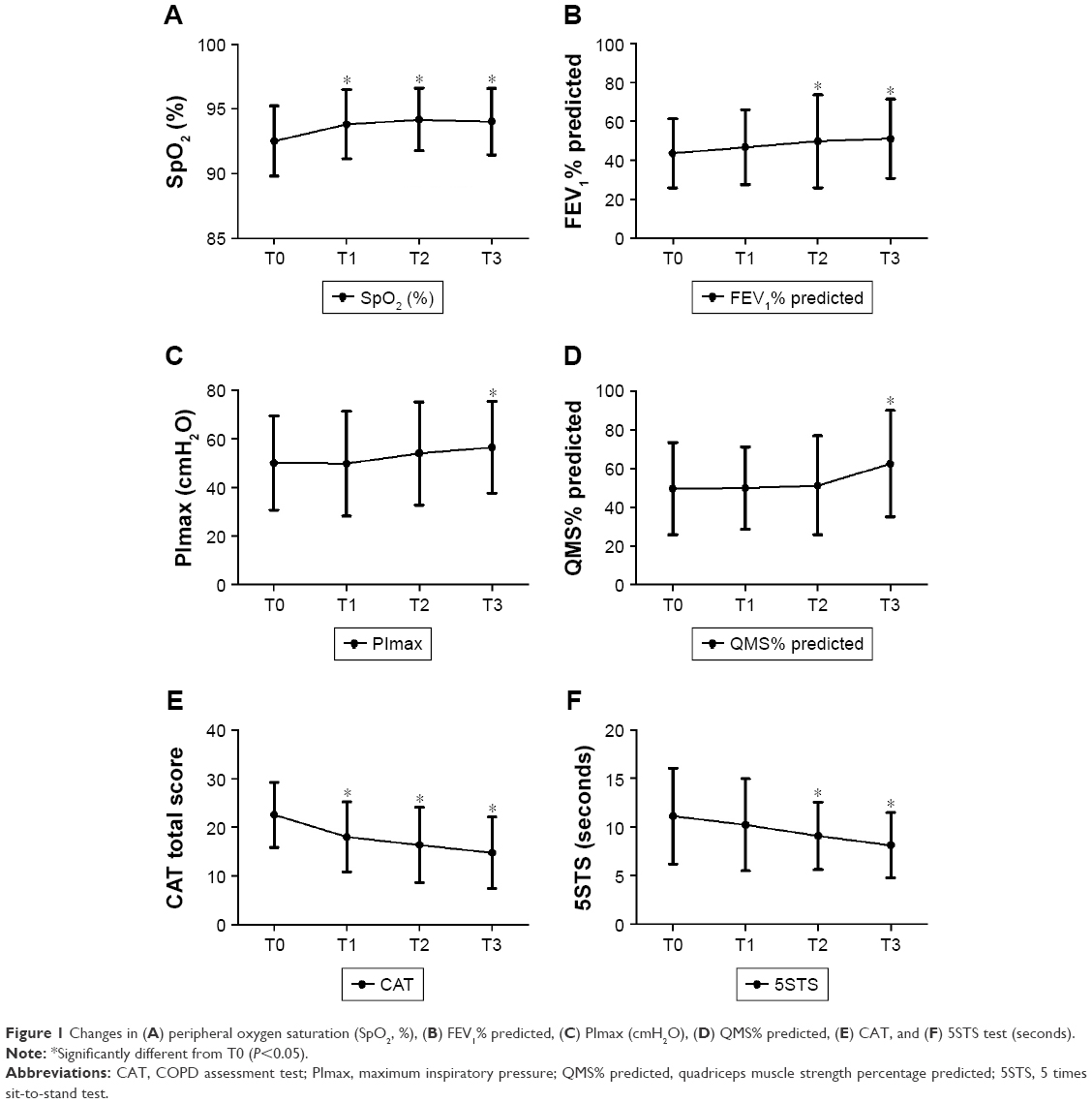 | Figure 1 Changes in (A) peripheral oxygen saturation (SpO2, %), (B) FEV1% predicted, (C) PImax (cmH2O), (D) QMS% predicted, (E) CAT, and (F) 5STS test (seconds). |
Factors influencing recovery from AECOPD
Complete results of the independent variables’ (ie, BMI, number of exacerbations in the past year, CCI, and mMRC) effects in each of the dependent variables (ie, SpO2, FEV1% predicted, PImax, QMS% predicted, CAT, and 5STS) are found in Table S3.
Peripheral oxygen saturation
No significant interactions were found between the independent variables and SpO2 (P>0.05). However, patients presenting two or more AECOPD had mean values of SpO2 lower than those with one or no AECOPD (mean difference −1.56%±0.53%; P=0.003) independently of the moment of data collection. Other independent variables were not found to significantly affect SpO2 (P>0.05) (Figure S1).
FEV1% predicted
No significant interactions were found between the independent variables and FEV1% predicted (P>0.05). However, underweight patients presented lower FEV1% predicted than overweight (mean difference −18.98%±4.49% predicted) and normal weight (mean difference −17.84%±4.15% predicted) patients, independently of the moment of data collection (P<0.001). Other independent variables were not found to significantly affect FEV1% predicted (P>0.05) (Figure S2).
PImax
Significant interactions between time and number of exacerbations in the previous year (P=0.007), comorbidities (P=0.025), and dyspnea (P=0.012) were found to affect changes in PImax during AECOPD. Other independent variables were not found to significantly affect PImax (P>0.05) (Figure S3).
QMS% predicted
Significant interactions between time and number of exacerbations in the previous year (P=0.035) and comorbidities (P=0.020) were found to affect changes in QMS% predicted during AECOPD. Additionally, QMS% predicted was lower in more dyspneic patients (mMRC ≥2) than in less dyspneic patients (mMRC <2; mean difference −24.27%±11.74% predicted; P=0.011), independently of the moment of data collection. Other independent variables were not found to significantly affect QMS% predicted (P>0.05) (Figure S4).
CAT
Significant interactions between time and BMI (P=0.039) were found to affect changes in CAT during AECOPD. Additionally, CAT scores were higher in overweight patients (BMI ≥25) than in patients with normal BMI (mean difference 4.59±1.77; P=0.042) and in more dyspneic patients (mMRC ≥2; mean difference 7.98±1.84; P<0.001), independently of the moment of data collection. Other independent variables were not found to significantly affect CAT (P>0.05) (Figure S5).
5STS
Significant interactions between time and BMI (P=0.008), comorbidities (P=0.001), and dyspnea (P=0.003) were found to affect changes in 5STS during AECOPD. Additionally, patients with severe comorbidities took longer to complete the 5STS than those with mild (mean difference 2.72±1.35) and moderate (mean difference 2.73±1.14) comorbidities in the CCI independently of the moment of data collection (P=0.013). Other independent variables were not found to significantly affect 5STS (P>0.05) (Figure S6).
Discussion
This study added important findings on the time course of AECOPD managed on an outpatient basis, namely: 1) SpO2 and CAT improve after 7 days of the onset of an AECOPD, FEV1% predicted and 5STS improve after 15 days, and muscle strength improve after 45 days of the AECOPD; 2) changes in SpO2 and FEV1% predicted are not influenced by BMI, dyspnea, previous AECOPD, or comorbidities; however, changes in other outcome measures were influenced by at least one independent variable; and 3) independently of the time of data collection, low/high BMI, increased dyspnea, previous exacerbations, and severe comorbidities significantly affect patients’ outcomes during AECOPD.
Most burdensome symptoms and limitations perceived by each patient improved in the first week (difference of approximately five points in CAT), exceeding the minimal clinical important difference (MCID) of two points,30,31 and minor improvements were observed in the following weeks. These results matched those previously reported in hospitalized patients,10,32 in which major improvements have been obtained during the first 5 days of hospital admission.10 Improvements in CAT exceeding the MCID (from −3 to −1030,33) have been shown, with higher magnitudes observed in more severe exacerbations and in hospitalized patients.10 Assessment of CAT, especially in the first week following the AECOPD, is important, and different MCID might be needed for hospitalized and nonhospitalized patients with AECOPD. Additionally, a negative effect of overweight in CAT has been found, mimicking previous studies conducted in inpatients.10 These results shown that, independently of the setting of treatment, an excess of weight significantly impairs patients’ improvements in their health status.
The use of SpO2 and lung function to monitor patients with AECOPD have been controversial, as these measures have shown poor reliability and/or sensitivity to change.34,35 Several studies have used SpO2 as an outcome measure; however, the changes reported vary widely8,36,37 and, in the absence of an MCID for this parameter, it is not clear whether these changes are clinically significant, especially in patients not presenting hypoxemia at baseline assessment. Lung function measurements during AECOPD are not currently recommended by the GOLD;35 however, they are widely used.7,8,11 Results previously obtained are not homogeneous with some authors reporting improvements in lung function, namely FEV1,7,8 and others finding no improvements after an AECOPD,11 which impairs conclusions regarding its usefulness and responsiveness during exacerbations. Using the minimal detectable difference recommended by the European Respiratory Society (ie, increment of 9% in FEV1% predicted),38 important improvements in FEV1 were only achieved at T3 (mean difference 9.3% from T0), meaning that, at stability, most patients may have achieved full recovery. These results should nonetheless be interpreted with caution as the minimal detectable difference used has only been established for bronchodilator responsiveness in stable patients with COPD.38 Nevertheless, our study showed that both SpO2 and lung function are outcomes that can be simply obtained and seem not to be influenced by independent variables. Future studies are needed to further assess their adequacy to be used in monitoring AECOPD and establish their MCID.
Changes in muscle strength measures, such as PImax and QMS% predicted, were only significant after 45 days of AECOPD, and the pattern of their recovery was influenced by several independent measures, ie, dyspnea, previous exacerbations, and comorbidities. Recovery of physical parameters is often impaired during AECOPD and may never fully recover.2 In hospitalized patients, decreases in muscle strength occur even during the course of AECOPD,5 which was not observed in this study, possibly because patients continued to perform their daily activities at home, even if at a slower pace. The inclusion of strengthening exercises in hospitalized patients during AECOPD has been recommended to further enhance their recovery.5 This addition may be equally valid and fruitful in outpatients, since it may fasten patients’ functional recovery to perform their daily and job-related activities.
Generally, more dyspneic patients, under-/overweight, with more exacerbations/year and more comorbidities, recovered slower, except for QMS and 5TST. These findings may be justified by the fact that these more fragile patients presented poorer values at baseline and, thus, had more room for improvement. In the 5STS test, at T0 the overall sample completed the test in >10 seconds, leaving them a marginal room for progress.24,39 This suggests that the 5STS presents a ceiling effect and may not be the most adequate outcome measure to monitor functionality in more functional patients but may be suitable for more severe and older patients.
Independently of the time of data collection, underweight patients presented more airway obstruction; overweight patients presented higher impacts of the disease; dyspneic patients presented lower QMS; frequent exacerbators presented lower oxygenation values; and patients with more comorbidities performed worse in 5STS. It is known that all of these parameters are potential predictors of COPD trajectory,28 and thus, it was expected that they would also play a role during the recovery of AECOPD. Nevertheless, it was not possible to find one single independent variable that influenced and differentiated improvements in all outcome measures. These results further highlight the multidimensional and systemic component of AECOPD and the importance of studying the role of emerging biomarkers,40,41 together with clinical variables, to predict the trajectory of COPD, and specifically AECOPD.
Limitations
This study has some limitations that must be acknowledged. First, as effects of therapies were not of interest in this study, all patients were treated according to clinicians’ best judgment. However, it must be acknowledged that different combinations of treatments might have influenced the outcomes of individual patients. Second, although a sample calculation has been computed to test the time effects in the dependent variables studied, the study was not powered for its secondary analysis (ie, identify the factors influencing this recovery from AECOPD), resulting in a possible small sample size for this analysis. Consequently, patients’ distribution among categories of independent variables (eg, BMI – underweight, normal weight, and overweight) were not homogeneous, which could have affected the results observed. Additionally, other variables that are known to influence COPD trajectory and that could also play a role in the time course of AECOPD, such as forced vital capacity, medication, and nature of previous exacerbations, could not been integrated in the models developed. Increasing the number of independent variables would have augmented the risk of having correlations among the variables and, thus, decreased the robustness and the accuracy of the models. Further studies, powered for a high number of variables, should clarify the role of the clinical variables explored and consider their potential interaction with other demographic, chemical, and biological variables to better understand the time course of AECOPD managed on an outpatient basis. Although this was not the main objective of the present article, our exploratory results are valuable, as they contributed to unravel the most promising variables to assess in clinical practice and may be used to compute appropriate sample sizes in future research. Third, most outcome measures used depend on patients’ motivation and evaluator expertise. To minimize these influences, a trained physiotherapist conducted all data collection and only variations of less than 20% between the two better results (except for lung function and inspiratory muscle strength, where the European Respiratory Society and American Thoracic Society guidelines19,20 were followed) in each measurement were considered for analysis. Finally, patient’s stable state prior to the exacerbation was not assessed and, thus, it is not known if patients returned or not to their baseline status. Still, information of the course of exacerbations managed on an outpatient basis is still provided and may be useful to personalize interventions in this population.
Conclusion
During an AECOPD managed on an outpatient basis, SpO2 and CAT improve after 7 days of the onset, FEV1% predicted and 5STS improve after 15 days, and muscle strength measures improved only after 45 days of the AECOPD. FEV1% predicted and SpO2 recovery are not influenced by independent patients’ characteristics, such as BMI, dyspnea, previous AECOPD, or comorbidities and, thus, may be potentially useful to monitor AECOPD recovery. Low/high BMI, increased dyspnea, previous exacerbations, and severe comorbidities significantly affect patients’ outcomes during AECOPD. No single indicator was able to predict patients’ recovery for all measures assessed; thus, a comprehensive assessment at the onset of the AECOPD is needed to personalize interventions to outpatients with AECOPD.
Acknowledgments
This work was funded by Programa Operacional de Competitividade e Internacionalização – POCI, through Fundo Europeu de Desenvolvimento Regional – FEDER (POCI-01-0145-FEDER-007628) and Fundação para a Ciência e Tecnologia (FCT) under the projects UID/BIM/04501/2013, PTDC/DTP-PIC/2284/2014, and SFRH/BD/101951/2014. The authors also would like to acknowledge Hélder Melro, Ana Machado, and Sara Miranda for their assistance in data collection and all patients and physicians from the Centro Hospitalar do Baixo Vouga for their collaboration in this study.
Author contributions
AO and AM were responsible for the study conception and design. AM is the guarantor. AO performed data collection and was responsible for drafting the manuscript. AO and VA performed data analysis. AO and AM obtained the funding. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Gulati S, Wells JM. Bringing Stability to the Chronic Obstructive Pulmonary Disease Patient: Clinical and Pharmacological Considerations for Frequent Exacerbators. Drugs. 2017;77(6):651–670. | ||
Anzueto A. Impact of exacerbations on COPD. Eur Respir Rev. 2010;19(116):113–118. | ||
Celli BR, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2013;23(6):932–946. | ||
Guarascio AJ, Ray SM, Finch CK, Self TH. The clinical and economic burden of chronic obstructive pulmonary disease in the USA. Clinicoecon Outcomes Res. 2013;5:235–245. | ||
Spruit MA, Gosselink R, Troosters T, et al. Muscle force during an acute exacerbation in hospitalised patients with COPD and its relationship with CXCL8 and IGF-I. Thorax. 2003;58(9):752–756. | ||
Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(5 Pt 1):1418–1422. | ||
Seemungal TA, Donaldson GC, Bhowmik A, Jeffries DJ, Wedzicha JA. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161(5):1608–1613. | ||
Parker CM, Voduc N, Aaron SD, Webb KA, O’Donnell DE. Physiological changes during symptom recovery from moderate exacerbations of COPD. Eur Respir J. 2005;26(3):420–428. | ||
Koutsokera A, Kiropoulos TS, Nikoulis DJ, et al. Clinical, functional and biochemical changes during recovery from COPD exacerbations. Respir Med. 2009;103(6):919–926. | ||
Feliz-Rodriguez D, Zudaire S, Carpio C, et al. Evolution of the COPD Assessment Test score during chronic obstructive pulmonary disease exacerbations: determinants and prognostic value. Can Respir J. 2013;20(5):e92–e97. | ||
Mesquita R, Donária L, Genz IC, Pitta F, Probst VS. Respiratory muscle strength during and after hospitalization for COPD exacerbation. Respir Care. 2013;58(12):2142–2149. | ||
GOLD. Global Strategy for the Diagnosis, Management and Prevention of COPD. Global Initiative for Chronic Obstructive Lung Disease (GOLD); 2018. Available from: https://goldcopd.org/wp-content/uploads/2017/11/GOLD-2018-v6.0-FINAL-revised-20-Nov_WMS.pdf. Accessed March 2, 2018. | ||
Singanayagam A, Schembri S, Chalmers JD. Predictors of mortality in hospitalized adults with acute exacerbation of chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2013;10(2):81–89. | ||
Adams SG, Melo J, Luther M, Anzueto A. Antibiotics are associated with lower relapse rates in outpatients with acute exacerbations of COPD. Chest. 2000;117(5):1345–1352. | ||
Bildt C, Alfredsson L, Punnett L, Theobald H, Torgén M, Wikman A. Effects of drop out in a longitudinal study of musculoskeletal disorders. Occup Environ Med. 2001;58(3):194–199. | ||
Søyseth V, Johnsen HL, Kongerud J. Prediction of dropout from respiratory symptoms and airflow limitation in a longitudinal respiratory study. Scand J Work Environ Health. 2008;34(3):224–229. | ||
Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. | ||
Doherty DE, Belfer MH, Brunton SA, Fromer L, Morris CM, Snader TC. Chronic obstructive pulmonary disease: consensus recommendations for early diagnosis and treatment. J Fam Pract. 2006;55(11):S1. | ||
Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. | ||
American Thoracic Society/European Respiratory Society. ATS/ERS Statement on respiratory muscle testing. Am J Respir Crit Care Med. 2002;166(4):518–624. | ||
Troosters T, Probst VS, Crul T, et al. Resistance training prevents deterioration in quadriceps muscle function during acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2010;181(10):1072–1077. | ||
Bohannon RW. Reference values for extremity muscle strength obtained by hand-held dynamometry from adults aged 20 to 79 years. Arch Phys Med Rehabil. 1997;78(1):26–32. | ||
Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. | ||
Jones SE, Kon SS, Canavan JL, et al. The five-repetition sit-to-stand test as a functional outcome measure in COPD. Thorax. 2013;68(11):1015–1020. | ||
Ma Y, Mazumdar M, Memtsoudis SG. Beyond repeated-measures analysis of variance: advanced statistical methods for the analysis of longitudinal data in anesthesia research. Reg Anesth Pain Med. 2012;37(1):99–105. | ||
World Health Organization [homepage on the Internet]. BMI classification; 2006. Available from: http://apps.who.int/bmi/index.jsp?introPage=intro_3.html. Accessed May 24, 2018. | ||
Spruit MA, Augustin IM, Vanfleteren LE, et al. Differential response to pulmonary rehabilitation in COPD: multidimensional profiling. Eur Respir J. 2015;46(6):1625–1635. | ||
Guerra B, Gaveikaite V, Bianchi C, Puhan MA. Prediction models for exacerbations in patients with COPD. Eur Respir Rev. 2017;26(143):160061. | ||
Viniol C, Vogelmeier CF. Exacerbations of COPD. Eur Respir Rev. 2018;27(147):170103. | ||
Kon SS, Canavan JL, Jones SE, et al. Minimum clinically important difference for the COPD Assessment Test: a prospective analysis. Lancet Respir Med. 2014;2(3):195–203. | ||
Jones PW, Harding G, Wiklund I, et al. Tests of the responsiveness of the COPD assessment test following acute exacerbation and pulmonary rehabilitation. Chest. 2012;142(1):134–140. | ||
García-Sidro P, Naval E, Martinez Rivera C, et al. The CAT (COPD Assessment Test) questionnaire as a predictor of the evolution of severe COPD exacerbations. Respir Med. 2015;109(12):1546–1552. | ||
Miravitlles M, García-Sidro P, Fernández-Nistal A, Buendía MJ, Espinosa de Los Monteros MJ, Molina J. Course of COPD assessment test (CAT) and clinical COPD questionnaire (CCQ) scores during recovery from exacerbations of chronic obstructive pulmonary disease. Health Qual Life Outcomes. 2013;11(1):147–149. | ||
Al Rajeh AM, Hurst JR. Monitoring of Physiological Parameters to Predict Exacerbations of Chronic Obstructive Pulmonary Disease (COPD): A Systematic Review. J Clin Med. 2016;5(12):108–118. | ||
Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. | ||
Eaton T, Young P, Fergusson W, et al. Does early pulmonary rehabilitation reduce acute health-care utilization in COPD patients admitted with an exacerbation? A randomized controlled study. Respirology. 2009;14(2):230–238. | ||
Torres-Sánchez I, Valenza MC, Sáez-Roca G, Cabrera-Martos I, López-Torres I, Rodríguez-Torres J. Results of a Multimodal Program During Hospitalization in Obese COPD Exacerbated Patients. COPD. 2016;13(1):19–25. | ||
Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC. Lung volumes and forced ventilatory flows. Eur Respir J. 1993;6 Suppl 16:5–40. | ||
Bernabeu-Mora R, Medina-Mirapeix F, Llamazares-Herrán E, Oliveira-Sousa SL, Sánchez-Martinez MP, Escolar-Reina P. The accuracy with which the 5 times sit-to-stand test, versus gait speed, can identify poor exercise tolerance in patients with COPD: A cross-sectional study. Medicine. 2016;95(35):e4740. | ||
Wang Z, Bafadhel M, Haldar K, et al. Lung microbiome dynamics in COPD exacerbations. Eur Respir J. 2016;47(4):1082–1092. | ||
Wan ES. Examining genetic susceptibility in acute exacerbations of COPD. Thorax. 2018;73(6):507–509. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.