Back to Journals » Clinical Interventions in Aging » Volume 20
Enhanced Recovery After Surgery (ERAS) Program for InterTAN Nail Surgery in Intertrochanteric Femoral Fracture (ITF) Patients Over 75 years Old
Authors Wu J, Wang P, Gao Z, Lu S
Received 31 March 2025
Accepted for publication 9 August 2025
Published 22 August 2025 Volume 2025:20 Pages 1305—1313
DOI https://doi.org/10.2147/CIA.S527660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Jingwei Wu,1– 3 Peng Wang,1– 3 Zhihua Gao,1– 3 Shibao Lu1– 3
1Department of Orthopedics, Xuanwu Hospital of Capital Medical University, Beijing, 100053, People’s Republic of China; 2National Clinical Research Center for Geriatric Diseases, Beijing, 100053, People’s Republic of China; 3Beijing Municipal Geriatric Medical Research Center, Beijing, 100053, People’s Republic of China
Correspondence: Shibao Lu, Department of Orthopedics, Xuanwu Hospital of Capital Medical University, 45 Changchun Street, Xicheng, Beijing, 100053, People’s Republic of China, Email [email protected]
Background: Enhanced Recovery After Surgery (ERAS) has been extensively applied across numerous surgical specialties. However, there remains a paucity of research regarding the implementation of ERAS in advanced age patients (≥ 75 years) who undergo InterTAN nail surgery for intertrochanteric femoral fractures (ITF). This study aimed to assess if our ERAS protocol improves satisfaction and clinical outcomes in such patients.
Methods: This was a retrospective cohort study included advanced age patients who underwent InterTAN nail surgery. The ERAS group included patients who underwent surgery between January 2022 and December 2024, while the non - ERAS group consisted of those who had the same surgery between January 2019 and December 2023. Demographics, comorbidities, surgical details, ERAS compliance, outcomes, complications, and length of stay (LOS) were evaluated.
Results: A total of 144 patients were included in the ERAS group and 135 in the non - ERAS group. Analysis of demographic data showed no statistically significant intergroup differences. ERAS compliance was 100%. There were no significant differences between the ERAS and non - ERAS groups in terms of operative side, anesthesia type, operating time, intraoperative blood loss, and postoperative Visual Analogue Scale scores. Moreover, 30 - day follow - up revealed no significant differences in readmission rates and mortality between the two groups. However, the LOS was significantly shorter in the ERAS group (5.68± 2.34 days vs 6.54± 2.04 days in the non - ERAS group; p = 0.03). The overall complication rate was also significantly lower in the ERAS group (10/144 vs 23/135; P < 0.01).
Conclusion: In this cohort of advanced age patients with ITF managed via our ERAS program, it was evidenced that this program is safe and can effectively reduce the LOS and the incidence of complications.
Keywords: enhanced recovery after surgery, intertrochanteric femoral fracture, geriatric
Introduction
With the advancement of medical standards and the increase in life expectancy, China has emerged as one of the countries with the largest elderly population and the most rapid population aging globally. The incidence of intertrochanteric femoral fracture (ITF) is rising annually. ITF is typically a low - energy injury, predominantly affecting elderly patients with osteoporosis. It is considered one of the most debilitating types of osteoporotic fractures. Due to the elevated risks of morbidity, mortality, and disability, it has earned the sobriquet “the last fracture of life”.1,2 This fracture is associated with elevated short - term and long - term all - cause mortality rates in both genders. In the first year following the fracture, the mortality rate is three times higher than that of the general geriatric population.3 Prolonged immobilization often associated with ITF treatment is likely to increase the incidence of adverse clinical outcomes, such as infections and pressure sores.4 Moreover, ITF in elderly patients has a significant societal impact. These patients are at risk of: (1) being unable to return to their previous living situations; (2) requiring a higher level of care and supervision; (3) experiencing a decline in quality of life; (4) having reduced mobility and ambulation; and (5) sustaining secondary osteoporotic fractures, including a second or contralateral hip fracture.5 Clinical guidelines recommend that reparative surgery for ITF should be carried out within 24 to 48 hours of hospital admission.6
It is recognized that advanced age patients (≥75 years) may have more severe comorbidities, functional deterioration and psychological alterations.7 These factors not only complicate the overall clinical situation but also present additional challenges in the treatment process. Furthermore, these factors have been demonstrated to act as predictors for postoperative adverse events.8 The presence of these risk factors can lead to various complications, a prolonged length of stay (LOS) in the hospital, and higher mortality rates.9
Enhanced Recovery After Surgery (ERAS) represents a comprehensive series of perioperative optimization strategies grounded in evidence-based medical data. Its primary objective is to mitigate the physical and psychological traumatic stress experienced by patients during the perioperative period. By doing so, ERAS effectively reduces the incidence of complications and facilitates a more rapid postoperative recovery.10 Currently, ERAS is widely recommended and implemented across a diverse range of surgical procedures.11–14 The multi-faceted preoperative, intraoperative, and postoperative measures incorporated within the ERAS protocol have the theoretical potential to decrease the occurrence of complications associated with InterTAN nail surgery. Notwithstanding the growing adoption of ERAS in various surgical contexts, the real-world benefits and safety profile of ERAS specifically in elderly patients (aged ≥ 75 years) undergoing InterTAN nail surgery remain largely unexplored. To the best of our knowledge, there is a paucity of data regarding its practical implications in this particular patient population. Therefore, the overarching aim of the present retrospective cohort study was to systematically evaluate the efficacy and safety of an ERAS program in optimizing the perioperative outcomes of elderly patients with intertrochanteric femoral fractures (ITF) who underwent InterTAN nail surgery.
Methods
Study Design and Data Collection
This study was a retrospective analysis of data sourced from our institution’s orthopedic surgical database. This database comprehensively and meticulously records the detailed medical records of elderly patients (aged≥75 years) who underwent InterTAN nail surgery for ITF. The patients were divided into two groups: the ERAS group, consisting of those who underwent the surgery between January 2022 and December 2024, and the non-ERAS group, which was matched for age and sex and included patients who had the same surgery between January 2019 and December 2023. The surgeries in both groups were carried out by the same surgical team, and the principles of surgical treatment adhered strictly to the relevant clinical guidelines.5 The non-ERAS group received treatment following traditional perioperative protocols. The inclusion criteria for the study required that patients be diagnosed by two trauma specialists based on specific clinical symptoms and signs, such as hip pain, shortening, and external rotation of the affected leg, as well as imaging examinations. Exclusion criteria included patients with open fractures, metastatic pathological fractures, those who were unable to walk independently prior to the fracture, and individuals who were unable to follow either verbal or written instructions. Throughout all the surgeries, the concepts of precision and minimal invasiveness were consistently applied.
The demographic characteristics, comorbid conditions, as well as operative and anesthetic details of the patients are summarized in Table 1. The outcome measures analyzed in this study included treatment-related complications, LOS in the hospital, postoperative pain levels, and the rates of 30-day readmission and mortality. All data were collected through a manual review of the electronic medical records to ensure accuracy and completeness.
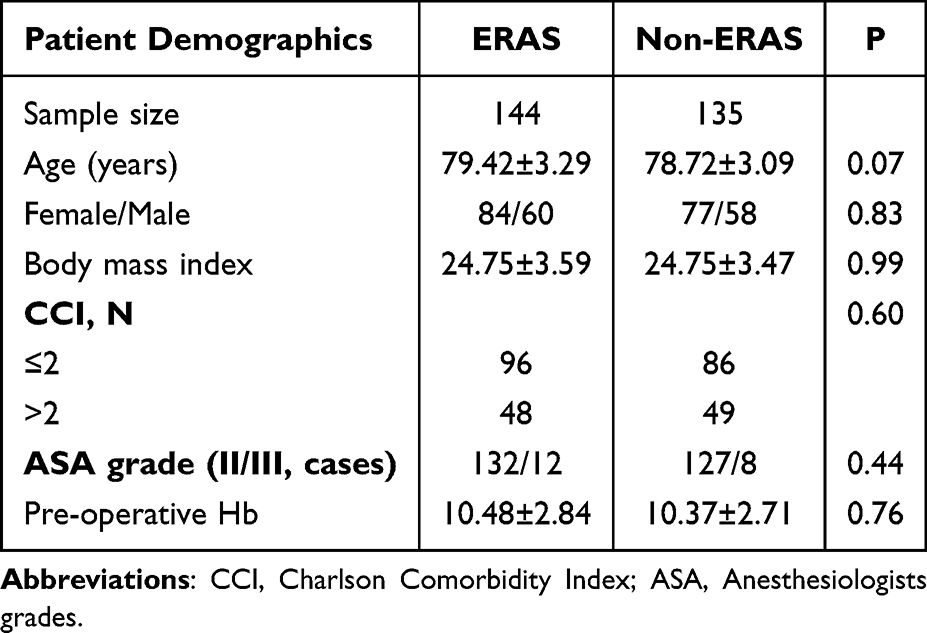 |
Table 1 Patient demographics |
ERAS Program
The ERAS program was initially put forward and meticulously planned in 2017. The specific ERAS program tailored for elderly patients (aged≥75 years) undergoing intramedullary nail fixation surgery was developed by integrating experiences from other ERAS projects and drawing upon the extensive clinical expertise of numerous specialists. The core expert team was composed of anesthesiologists, trauma surgeons, nutritionists, physical therapists, internists, geriatricians, and nurses.
Following the approval granted by the Ethical Committee for Human Subjects of the Xuanwu Hospital of Capital Medical University (approval date: April 3, 2018; approval number: 2018086), the ERAS program for patients undergoing intramedullary nail fixation surgery was officially put into practice starting from January 2022.
The ERAS interventions employed in the current study were systematically categorized into three phases: preoperative, intraoperative, and postoperative. The detailed measures and protocols for each phase are comprehensively presented in Table 2, which provides a clear and organized overview of the entire ERAS program implementation.
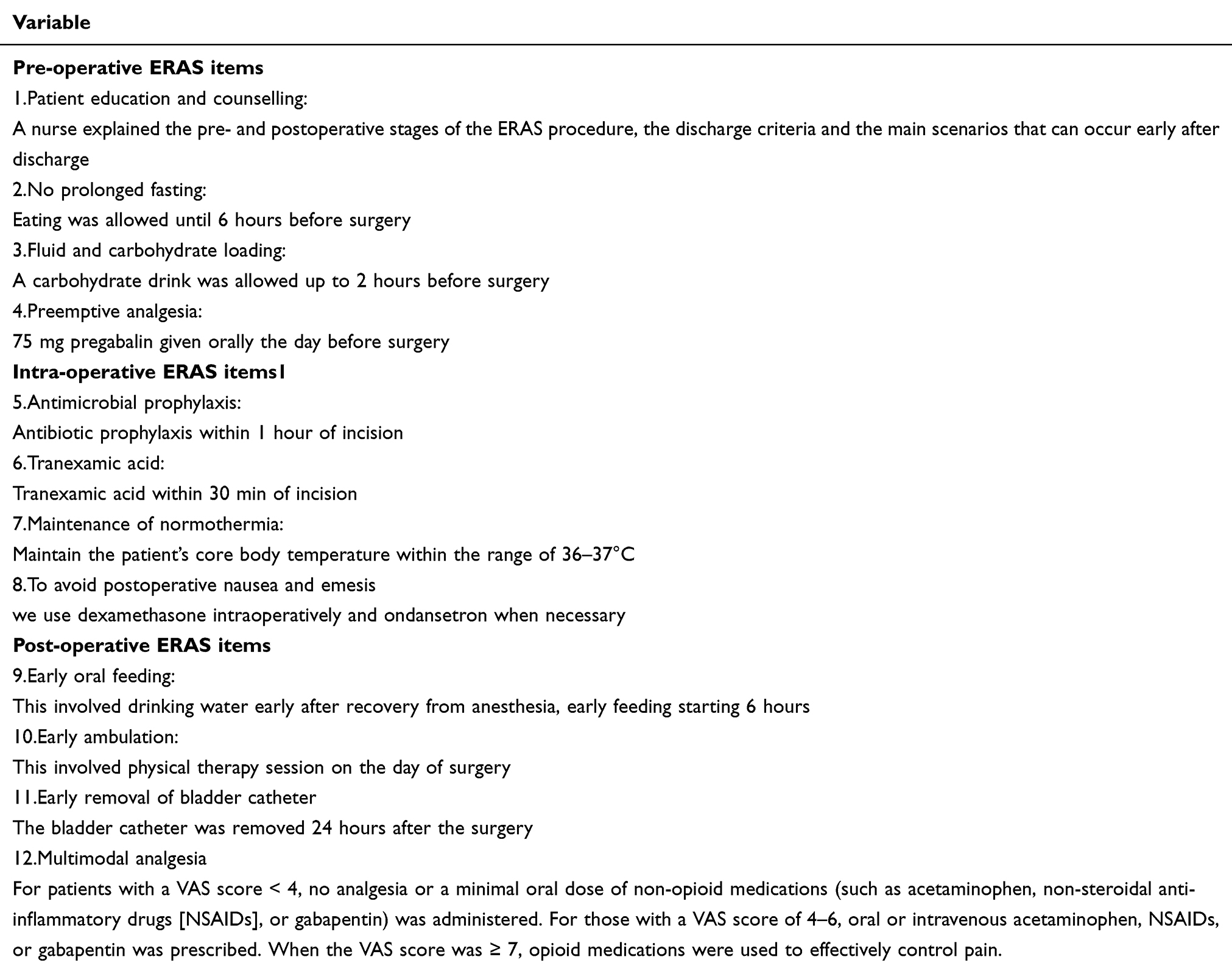 |
Table 2 ERAS Protocol |
Control Group
To evaluate the influence of the ERAS program on patient outcomes, we compared it with a control cohort of elderly patients (aged≥75 years) who underwent intramedullary nail fixation surgery. The surgeries in both groups were carried out by the same surgical team.
In the non-ERAS group, patients were required to undergo preoperative fasting for at least 8 hours, and oral feeding was initiated on the first postoperative day. Perioperative analgesia was prescribed based on the attending physicians’ clinical experience. Patient-controlled analgesia (PCA) was used, which consisted of sufentanil and other agents diluted in 100 mL of saline. In contrast, the intraoperative measures implemented in the ERAS group were scarcely applied in the non-ERAS group. Regarding the removal of the postoperative urinary catheter, the decision was made according to the attending physicians’ discretion.
Statistical Analysis
All statistical analyses in this study were conducted using SPSS software, version 17.0 (SPSS, Inc., Chicago, IL, USA). To assess the differences between the ERAS (Enhanced Recovery After Surgery) group and the non-ERAS group, various statistical tests were employed for patient demographics, comorbidity data, baseline health indicators, and clinical outcomes.
For the comparison of continuous variables, if the data were normally distributed, a Student’s t-test was used. In cases where the data did not follow a normal distribution, the Mann–Whitney U-test was applied instead. To determine the equality of variances between the ERAS and non-ERAS groups, an F-test was first conducted. If the variances were found to be unequal according to the F-test results, the Satterthwaite two-sample t-test was utilized for the comparison. Conversely, when the variances were equal, the standard two-sample t-test was employed.
For categorical variables, a chi-squared (χ²) test was used to examine the associations between the groups. A p-value less than 0.05 was considered statistically significant, indicating a meaningful difference between the ERAS and non-ERAS groups.
Results
Demographics
The ERAS group comprised 144 patients, including 60 men and 84 women. Their mean age was 79.42 ± 3.29 years, and the mean body mass index (BMI) was 24.75 ± 3.59. In contrast, the non-ERAS group consisted of 135 patients, with 58 men and 77 women. The mean age in this group was 78.72 ± 3.09 years, and the mean BMI was 24.75 ± 3.47.
Table 1 presents a detailed comparison of the baseline demographic characteristics and operative details between the two groups. Notably, there were no statistically significant differences in the Charlson Comorbidity Index (CCI) scores, which reflect the overall burden of comorbidities, nor in the American Society of Anesthesiologists (ASA) grades, indicating a comparable preoperative health status in terms of fitness for anesthesia and surgery. Additionally, the preoperative hemoglobin levels did not show any significant disparity between the ERAS and non-ERAS groups, suggesting similar hematological conditions prior to the intervention.
Compliance with the ERAS Program
The ERAS program implemented in the current study consisted of 11 distinct intervention components. Remarkably, all of these perioperative ERAS elements were uniformly applied in 100% of the cases, as comprehensively illustrated in Table 3.
 |
Table 3 ERAS Pathway Compliance |
Outcomes
The main clinical outcomes are summarized in Table 4. When comparing the ERAS group and the non-ERAS group, no significant differences were found in terms of the operative side, type of anesthesia administered, operating duration, or intraoperative blood loss. Additionally, there were no notable disparities in the Visual Analogue Score (VAS) measurements on the 1st and 2nd days post-surgery between the two groups.
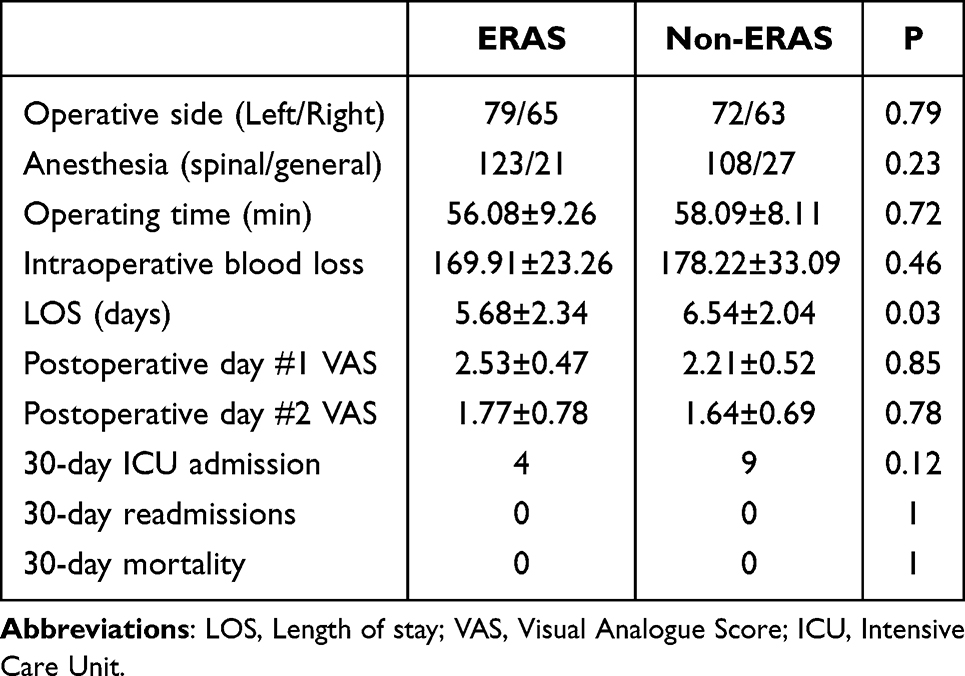 |
Table 4 Postoperative Outcomes |
Although the ERAS group exhibited a lower rate of 30-day admission to the Intensive Care Unit (ICU) compared to the non-ERAS group, this difference did not reach statistical significance (p = 0.12; Table 4). Furthermore, the incidence of 30-day readmissions and mortality was zero in both groups (Table 4). However, a statistically significant reduction in the LOS was observed in the ERAS group, with an average LOS of 5.68±2.34 days, compared to 6.54±2.04 days in the non-ERAS group (p = 0.03).
Table 5 details the occurrences of both major and minor complications. The overall complication rate in the ERAS group was significantly lower than that in the control (non-ERAS) group, with 10 out of 144 cases in the ERAS group and 23 out of 135 cases in the control group (P < 0.01). Regarding specific types of complications, there was no significant difference in the incidence of major complications between the two groups, with 4 out of 144 cases in the ERAS group and 6 out of 135 cases in the control group (P = 0.45). In contrast, the incidence of minor complications was notably lower in the ERAS group, with 6 out of 144 cases compared to 17 out of 135 cases in the control group (P = 0.01) (Table 5). This discrepancy was primarily attributed to a significantly decreased incidence of nausea and emesis in the ERAS group when compared to the non-ERAS group (P < 0.01; Table 5).
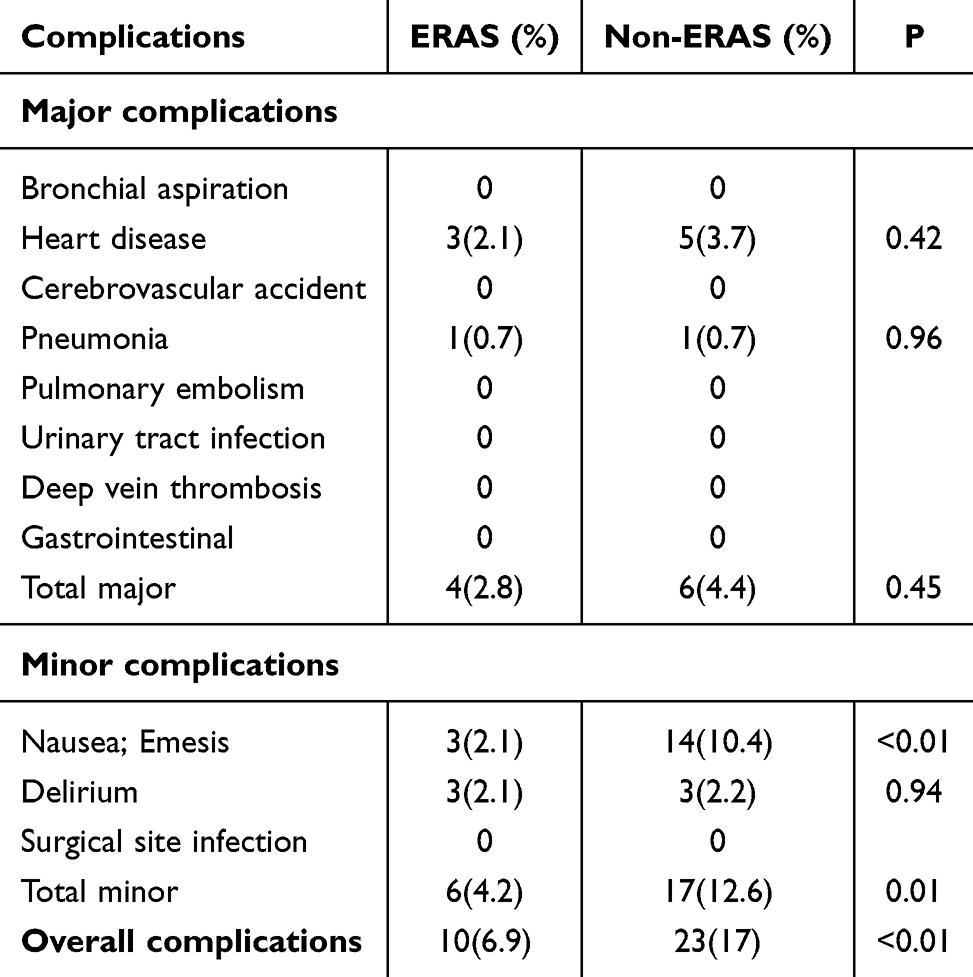 |
Table 5 Over Complication Data |
Discussion
In the current study, when compared with the control (non-ERAS) group, the ERAS group showed identical 30-day ICU admission rates, 30-day readmission rates, and 30-day mortality rates. However, the ERAS group demonstrated a significant reduction in both the LOS and the incidence of complications, without leading to an increase in the VAS. On average, the LOS in the ERAS group was approximately 1 day shorter than that in patients following the conventional perioperative protocol.
ITF is predominantly prevalent in the geriatric population, rendering them highly susceptible to a spectrum of complications, including pressure sores, urinary tract infections, and aspiration pneumonia. These complications can precipitate a significant increase in disability and mortality rates.15 To effectively reduce the mortality and disability rates associated with ITF, the medical literature overwhelmingly concurs that the principal aim of managing intertrochanteric fractures should be to achieve stable fracture fixation. This stable fixation serves as a prerequisite for early patient mobilization, thereby facilitating the restoration of limb function. An early surgical intervention is of utmost significance for attaining favorable functional outcomes and preventing severe postoperative complications related to both the implant and the patient.16 Nevertheless, age-related decline in physiological reserves and functional capabilities is an ineluctable process that impacts all organ systems. This physiological phenomenon typically gives rise to the manifestation of multiple comorbid conditions in elderly patients. A reduced ability to withstand surgical complications and slower recovery times in patients ≥75 years. To enhance the surgical safety of advanced age patients, it is essential to reduce surgical stress and boost the patients’ capacity to withstand surgical stress.
The ERAS program is no longer novel. The components of the ERAS program consist of a series of perioperative optimization measures aimed at reducing perioperative stress, this program has been reported to have positive effects on surgical outcomes.17–19 Compared with other ERAS protocols during pre-, intra-, and postoperative stages for ITF studies,20–22 the pillars of our ERAS protocol are similar, the most frequently emphasized elements include no prolonged fasting and eating, control of bleeding, maintenance of normothermia, multimodal analgesia, early removal of bladder catheter and early mobilization.
Multimodal, non - opioid - based analgesia has become the linchpin of the ERAS protocol in our institution for attaining efficacious analgesia subsequent to InterTAN nail surgery. Adequately managed pain is extensively recognized as a pivotal metric for surgical success and the recovery trajectory. It also functions as a proxy for patient satisfaction. Multiple factors contribute to postoperative pain in patients undergoing InterTAN nail surgery. In addition to the nociceptive pain originating from the surgical incision, these patients experience musculoskeletal pain resulting from surgical traction and the manipulation of bones and muscles.23 Despite opioids remaining an effective modality for pain management, substantial evidence has uncovered a broad spectrum of adverse effects associated with their use. These encompass nausea, ileus, respiratory depression, hyperalgesia, and delirium related to opioid analgesia.24 Multimodal analgesia involves the employment of multiple pain - control mechanisms that act in a synergistic manner. This strategy not only augments the analgesic effect but also diminishes the requisite doses of opioids, thus reducing the risk of opioid - related side - effects.25 The ERAS program described in the current study integrated preemptive analgesia, local anesthesia and perioperative oral non - opioid medications to minimize the postoperative reliance on opioids. The results demonstrated that, under the condition of effectively relieving pain, the ERAS group also reduced the incidence of postoperative nausea.
The development of medical treatment and improvements in trauma surgery techniques have enabled aggressive surgical treatment in ITF geriatric patients. However, various perioperative complications are a common occurrence in geriatric patients undergoing InterTAN nail surgery.15 Traditional perioperative management methods lack corresponding measures to reduce stress responses in geriatric patients, which is a pivotal element in geriatric medicine. Although it has been generally recognized that ERAS measures can reduce the surgical stress response, there is still a lack of reports on the safety of applying its relatively aggressive measures in the population of geriatric patients undergoing InterTAN nail surgery. In the present study, the incidence rate of overall complications in the ERAS group was 6.9%, which was significant lower than that in the control group. Our ERAS program is based on a series of perioperative protective strategies. For instance, by shortening the duration of fasting and water deprivation, we can reduce the occurrence of insulin resistance and perioperative electrolyte disorders. Maintaining normothermia during the operation can decrease the incidence of intraoperative homeostatic imbalance. The application of tranexamic acid during the operation helps to reduce intraoperative blood loss. Early removal of the urinary catheter after the operation can lower the incidence of perioperative urinary tract infections. Early postoperative ambulation can increases intestinal peristalsis and lung capacity, promotes lower limb muscle strength recovery, maintains hip activity and prevents the formation of deep venous thrombosis after operation.
In the present study, the average LOS in the ERAS group (5.68±2.34 days) was significant shorter than that in the non-ERAS group (6.54±2.04 days) without increasing the 30-day readmissions rates and 30-day mortality rates. ITF patients who received ERAS program care had a lower incidence of postoperative complications, better subsequent mobility, and were more likely to be discharged home earlier instead of requiring longer nursing care in the hospital. Therefore, the costs were correspondingly reduced.
Nevertheless, the current study is beset with several limitations. Firstly, it adopts a retrospective design and has a relatively small sample size. Secondly, the ERAS and non - ERAS groups were evaluated at disparate time points, which might have introduced bias into the analysis of the study. Additionally, frailty assessment was not incorporated. Frailty, an age - associated and progressive reduction in multiple physiological reserves, is known to lead to unfavorable postoperative outcomes. Incorporating frailty assessment would render the study more persuasive. Therefore, further multicenter investigations with a larger cohort and extended long - term follow - up are warranted to validate the safety and effectiveness of the proposed ERAS protocol for geriatric patients following InterTAN nail surgery.
Conclusions
This research demonstrates that the implementation of the ERAS pathway can remarkably decrease the LOS and complications following InterTAN nail surgery for ITF patients. In comparison with traditional perioperative management, it not only ensures superior early functional outcomes but also does not elevate the incidence of postoperative readmissions or mortality rates. This indicates that the ERAS pathway is a viable and beneficial strategy for optimizing the perioperative management of ITF patients undergoing InterTAN nail surgery, contributing to enhanced patient recovery and reduced healthcare burdens. These details may serve as a reference for the future guidelines of standard ERAS programs in ITF fracture surgery.
Abbreviations
ITF, intertrochanteric femoral fracture; ERAS, enhanced recovery after surgery; LOS, length of stay; BMI, body mass index; ASA, American Society of Anesthesiologists; VAS, Visual Analogue Score; ICU, Intensive Care Unit.
Data Sharing Statement
The data set used during the current study is available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was reviewed and approved by the institutional review board following the declaration of Helsinki principles in Xuanwu Hospital Capital Medical University (permit data 2018.4.3; no. 2018086). Informed consent was provided by all participating individuals.
Acknowledgments
We thank the staff at the Department of Orthopedics, Xuanwu Hospital Capital Medical University, and all the patients who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no financial and non-financial competing interests.
References
1. Javaid K, Zhang C, Feng J, et al. Incidence of and trends in hip fracture among adults in urban China: a nationwide retrospective cohort study. PLoS Med. 2020;17(8). doi:10.1371/journal.pmed.1003180
2. Wei J, Zeng L, Li S, Luo F, Xiang Z, Ding Q. Relationship between comorbidities and treatment decision-making in elderly Hip fracture patients. Aging Clin Experim Res. 2019;31(12):1735–1741. doi:10.1007/s40520-019-01134-5
3. Katsoulis M, Benetou V, Karapetyan T, et al. Excess mortality after hip fracture in elderly persons from Europe and the USA: the CHANCES project. J Intern Med. 2017;281(3):300–310. doi:10.1111/joim.12586
4. Moja L, Piatti A, Pecoraro V, et al. Timing matters in hip fracture surgery: patients operated within 48 hours have better outcomes. A meta-analysis and meta-regression of over 190,000 patients. PLoS One. 2012;7(10):e46175. doi:10.1371/journal.pone.0046175
5. Roberts KC, Brox WT, Jevsevar DS, Sevarino K. Management of hip fractures in the elderly. J Am Acad Orthop Surg. 2015;23(2):131–137. doi:10.5435/JAAOS-D-14-00432
6. O’Connor MI, Switzer JA. AAOS clinical practice guideline summary: management of hip fractures in older adults. J Am Acad Orthop Surg. 2022;30(20):e1291–e1296. doi:10.5435/JAAOS-D-22-00125
7. Zhang LM, Hornor MA, Robinson T, Rosenthal RA, Ko CY, Russell MM. Evaluation of postoperative functional health status decline among older adults. JAMA Surg. 2020;155(10):950–958. doi:10.1001/jamasurg.2020.2853
8. Jang JM, Choi HS, Lee JS, Jeong KY, Hong HP, Ko SH. Femoral intertrochanteric fractures of the patients in the emergency department due to minor falls: special consideration in the middle-old to oldest-old patients. Ann Geriatr Med Res. 2019;23(3):125–132. doi:10.4235/agmr.19.0027
9. Liu SK, Ho AW, Wong SH. Early surgery for Hong Kong Chinese elderly patients with hip fracture reduces short-term and long-term mortality. Hong Kong Med J. 2017;23(4):374–380. doi:10.12809/hkmj165005
10. Elsarrag M, Soldozy S, Patel P, et al. Enhanced recovery after spine surgery: a systematic review. Neurosurg Focus. 2019;46(4):E3. doi:10.3171/2019.1.FOCUS18700
11. Meillat H, Brun C, Zemmour C, et al. Laparoscopy is not enough: full ERAS compliance is the key to improvement of short-term outcomes after colectomy for cancer. Surg Endosc. 2020;34(5):2067–2075. doi:10.1007/s00464-019-06987-5
12. Naftalovich R, Singal A, Iskander AJ. Enhanced recovery after surgery (ERAS) protocols for spine surgery - review of literature. Anaesthesiol Intensive Ther. 2022;54(1):71–79. doi:10.5114/ait.2022.113961
13. Chorath K, Luu N, Go BC, Moreira A, Rajasekaran K. ERAS protocols for thyroid and parathyroid surgery: a systematic review and meta-analysis. Otolaryngol Head Neck Surg. 2022;166(3):425–433. doi:10.1177/01945998211019671
14. Nelson G, Fotopoulou C, Taylor J, et al. Enhanced recovery after surgery (ERAS(R)) society guidelines for gynecologic oncology: addressing implementation challenges - 2023 update. Gynecol Oncol. 2023;173:58–67. doi:10.1016/j.ygyno.2023.04.009
15. Liao CS, He FZ, Li XY, Han PF. Proximal femoral nail antirotation versus InterTan nail for the treatment of intertrochanteric fractures: a systematic review and meta-analysis. PLoS One. 2024;19(7):e0304654. doi:10.1371/journal.pone.0304654
16. Nishiura T, Nozawa M, Morio H. The new technique of precise insertion of lag screw in an operative treatment of trochanteric femoral fractures with a short intramedullary nail. Injury. 2009;40(10):1077–1083. doi:10.1016/j.injury.2009.03.049
17. Longo F, Panza E, Rocca L, et al. Enhanced recovery after surgery (ERAS) in pancreatic surgery: the surgeon’s point of view. J Clin Med. 2024;13(20):6205. doi:10.3390/jcm13206205
18. Guo T, Ding F, Fu B, et al. Efficacy and safety of enhanced recovery after surgery (ERAS) protocols for patients undergoing minimally invasive transforaminal lumbar interbody fusion surgery: a systematic review and meta-analysis. World Neurosurg. 2024;188:199–210e1. doi:10.1016/j.wneu.2024.05.133
19. Schmid ME, Stock S, Girdauskas E. Implementation of an innovative ERAS protocol in cardiac surgery: a qualitative evaluation from patients’ perspective. PLoS One. 2024;19(5):e0303399. doi:10.1371/journal.pone.0303399
20. Kang Y, Liu J, Chen H, et al. Enhanced recovery after surgery (ERAS) in elective intertrochanteric fracture patients result in reduced length of hospital stay (LOS) without compromising functional outcome. J Orthop Surg Res. 2019;14(1):209. doi:10.1186/s13018-019-1238-2
21. Zhu W, Yan Y, Sun Y, et al. Implementation of enhanced recovery after surgery (ERAS) protocol for elderly patients receiving surgery for intertrochanteric fracture: a propensity score-matched analysis. J Orthop Surg Res. 2021;16(1):469. doi:10.1186/s13018-021-02599-9
22. Liu SY, Li C, Zhang PX. Enhanced recovery after surgery for hip fractures: a systematic review and meta-analysis. Perioper Med. 2021;10(1):31. doi:10.1186/s13741-021-00201-8
23. Beverly A, Kaye AD, Ljungqvist O, Urman RD. Essential elements of multimodal analgesia in enhanced recovery after surgery (ERAS) guidelines. Anesthesiol Clin. 2017;35(2):e115–e143. doi:10.1016/j.anclin.2017.01.018
24. Huang L, Zhang T, Wang K, Chang B, Fu D, Chen X. Postoperative multimodal analgesia strategy for enhanced recovery after surgery in elderly colorectal cancer patients. Pain Ther. 2024;13(4):745–766. doi:10.1007/s40122-024-00619-0
25. Carron M, Tamburini E, Linassi F, Pettenuzzo T, Boscolo A, Navalesi P. Efficacy of nonopioid analgesics and adjuvants in multimodal analgesia for reducing postoperative opioid consumption and complications in obesity: a systematic review and network meta-analysis. Br J Anaesth. 2024;133(6):1234–1249. doi:10.1016/j.bja.2024.08.009
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.