Back to Journals » International Medical Case Reports Journal » Volume 15
Endophthalmitis Secondary to Occult Intraocular Eyelashes Following Perforating Gunshot Injury: A Case Report
Authors Ghoraba HH, Leila M ![]() , Ghoraba HH
, Ghoraba HH ![]() , Abdelfattah HM, Elgemai EEM
, Abdelfattah HM, Elgemai EEM
Received 31 August 2022
Accepted for publication 27 October 2022
Published 10 November 2022 Volume 2022:15 Pages 657—660
DOI https://doi.org/10.2147/IMCRJ.S387929
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video 1 of "Endophthalmitis secondary to occult lashes" [ID 387929].
Views: 135
Hammouda Hamdy Ghoraba,1 Mahmoud Leila,2 Hashem H Ghoraba,1 Haithem Maamoun Abdelfattah,3 Emad Eldin Mohamed Elgemai4
1Retina Department, Magrabi Eye Hospital, Tanta, Egypt; 2Retina Department, Research Institute of Ophthalmology, Giza, Egypt; 3Ophthalmology Department, Benha Teaching Hospital, Benha, Egypt; 4Ophthalmology Department, Damanhour Teaching Hospital, Damanhour, Egypt
Correspondence: Mahmoud Leila, Retina Department, Research Institute of Ophthalmology, 2 Al-Ahram Street, Giza, Egypt, Email [email protected]
Purpose: This is a retrospective case report in which we describe our findings in two cases of endophthalmitis associated with perforating gunshot injury, in which we documented intraocular intrusion of multiple eyelashes as a plausible source of infection.
Patients and Methods: Two male patients, 22 and 29 years old, respectively, presented with endophthalmitis following primary repair of rupture globe secondary to gunshot injury. Both patients had vitrectomy and silicone oil injection. Preoperative imaging and intraoperative findings confirmed the perforating nature of the projectile.
Results: In both patients, we detected eyelashes that were concealed either in the pars plana region or within vitreous exudates. Silicone oil was not removed in both patients to prevent phthisis bulbi and because there was no potential for visual improvement. The postoperative course in both cases was uneventful.
Conclusion: Gunshot injuries can inoculate eyelashes impregnated with infectious microorganisms into the eye. In cases presenting with endophthalmitis associated with a gunshot injury, we recommend meticulous examination of the posterior segment and the pars plana region during vitrectomy to exclude the presence of occult lashes.
Keywords: gunshot injury, endophthalmitis associated with perforating IOFB, post-traumatic endophthalmitis, case report
Introduction
Ammunition from firearms acquires high kinetic energy upon exit from the muzzle. Friction along the trajectory of the projectile converts this energy to a high core temperature that renders the projectile practically sterile upon impact with the eye.1–3 Nevertheless, the incidence of endophthalmitis associated with intraocular foreign bodies (IOFB) derived from ammunition fragments is substantial. A rigorous analysis of the microbial profile of patients with endophthalmitis associated with IOFB explains this paradox. Several reports documented a high prevalence of Staphylococcus species, particularly Staphylococcus epidermidis in isolates sequestered from cases of post-traumatic endophthalmitis. Staphylococcus epidermidis is a common normal skin flora and its presence in these cases suggests that particulate matter was introduced from the ocular surface into the intraocular compartment by the IOFB through the entry wound.4–8 In this report, we present two cases of endophthalmitis associated with perforating gunshot injury, in which we documented intraocular intrusion of multiple eyelashes as a plausible source of infection. All surgical procedures described herein were performed by a single surgeon (HG) in a retina tertiary center.
Case Presentation
Case 1
Our first patient was a 22-year-old male who presented with a diminution of vision, pain, and redness in the left eye. He had a gunshot injury to his left eye for 1-week duration. Primary repair was done elsewhere. His BCVA was 20/25 in the right eye and hand movement (HM) in the left eye. Examination revealed sutured corneal entry wound, corneal edema, basal iridectomy, aphakia, hypopyon, and yellow fundus reflex. The patient had organized exudates occupying almost the entire pupillary area (Figure 1). There was no view of the ocular fundus. B-scan ultrasonography revealed a vitreous abscess and thickened retina-choroid-sclera (RCS) complex (2.4 mm). No IOFB could be detected on ultrasonography. CT scan revealed a retrobulbar metallic foreign body. The patient was admitted for pars plana vitrectomy (PPV). At the start of surgery, aqueous and vitreous samples were obtained for culture and sensitivity. For an aqueous sample, we used a 23-gauge needle mounted on a 3 mL syringe. For the vitreous sample, we used a vitreous cutter under air through the infusion port to avoid hypotony. Standard 23-gauge PPV consisted of core vitrectomy, and shaving of the vitreous base as safely as possible. Routinely, the surgeon did not attempt to induce posterior vitreous detachment (PVD) to avoid iatrogenic breaks in the presence of an inflamed retina, but in this patient, PVD was already induced. Intra-operatively, the exit port of the foreign body was detected at the nasal retina underlying subretinal hemorrhage. Intraoperatively, the surgeon retrieved multiple eyelashes that were either concealed within clumps of purulent intravitreal exudates or lodged in the pars plana. The retina was inspected at 360° using scleral indentation to exclude retinal breaks. Finally, fluid–air exchange and silicone oil (SO) injection were performed. At the end of surgery, two sclerotomies were closed by 7/0 vicryl, and antibiotics were administered into the vitreous cavity through the third one. We used vancomycin (1mg/0.1mL), and ceftazidime (2.25mg/0.1mL). Postoperatively, the patient received fortified antibiotics, topical steroids, and cycloplegics. The course of follow-up over the ensuing 4 years was uneventful. At his last visit, BCVA was counting fingers (CF) at 1 meter. Supplementary Video S1.
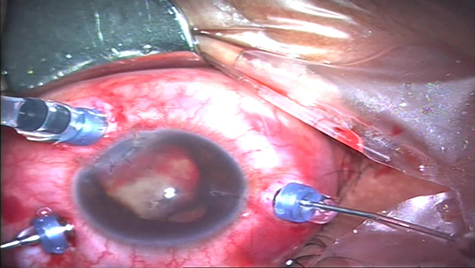 |
Figure 1 The left eye of a 22-year-old male patient following a gunshot injury. Note the sutured corneal entry wound, basal iridectomy, and organized exudates in the pupillary area. The patient was aphakic at the presentation. |
Case 2
The second patient was a 29-year-old male who presented with a diminution of vision in his right eye. He had a gunshot injury to his right eye for a 3-week duration. Primary repair was done elsewhere. His BCVA was the perception of light (PL) in the right eye and 20/20 in the left eye. Examination revealed sutured corneal entry wound and subluxated cataractous lens (Figure 2). There was no view of the ocular fundus. B-scan ultrasonography revealed a vitreous abscess and markedly thickened RCS complex (2.6 mm). No IOFB could be detected on ultrasonography. CT-scan revealed three metallic foreign bodies, the largest of which was lodged at the orbital apex. The patient was admitted for pars plana lensectomy and standard 23-gauge PPV. Surgical steps were similar to those of the first patient. Intra-operatively, the surgeon the exit port of the foreign body through the macula underneath the submacular hemorrhage. Multiple eyelashes were retrieved from the pars plana area. At the final visit 1-year postoperatively, the retina was stable under SO, with consecutive optic atrophy (Supplementary Video S2). In both patients, SO was not removed as there was no potential for visual improvement and to prevent the development of phthisis bulbi.
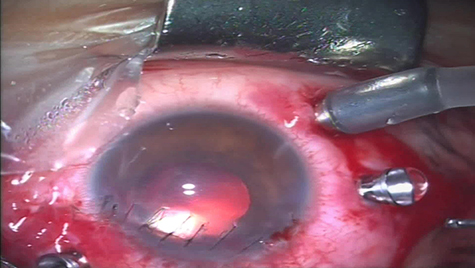 |
Figure 2 The right eye of a 29-year-old male patient following a gunshot injury, immediately after performing a pars plana lensectomy. Note the sutured corneal entry wound. |
Discussion and Conclusions
In the present report, both patients developed endophthalmitis associated with a gunshot injury. In these patients, the gunshot fragments could not have been the vehicle for organisms causing endophthalmitis as they perforated the globe and were not retained intraocular. Moreover, the fact that these fragments perforated the globe is indicative of their inherent high kinetic energy that rendered their trajectory heat-sterilized. We purport that the lashes retrieved during surgery, rather than the gunshot fragments, acted as a vehicle for organisms from the ocular surface to cause endophthalmitis. Unfortunately, both patients were not received in our tertiary center upon injury, rather they had primary repair elsewhere and they both received systemic, periocular, and topical antibiotics before being referred to us. This explains the negative results of aqueous and vitreous samples that we sequestered during surgery. Therefore, we were not able to confirm the presence of organisms commonly associated with lashes as Staphylococcus epidermidis. Nevertheless, our findings are similar to reports from published literature regarding endophthalmitis developing despite heat-sterilized foreign bodies.3–6,8 In addition, several studies reported that the microbial profile in patients with endophthalmitis associated with IOFB consisted of organisms that dwell in the ocular surface or soil-borne bacteria, which indicates intrusion of particulate matter from the ocular surface in the former or heavy contamination of the projectile as in mud-blast explosions in the latter.6–8
Gunshot injuries can inoculate eyelashes impregnated with infectious microorganisms into the eye. In cases presenting with endophthalmitis associated with a gunshot injury, we recommend meticulous examination of the posterior segment and the pars plana region during vitrectomy to exclude the presence of occult lashes, which if present must be removed completely.
Abbreviations
BCVA, best-corrected visual acuity; CF, counting fingers; CT-scan, computed tomography scan; HM, hand movement; IOFB, intraocular foreign body; mg, milligram; ml, milliliter; mm, millimeter; RCS, retina-choroid-sclera; PL, perception of light; PPV, pars plana vitrectomy; PVD, posterior vitreous detachment; SO, silicone oil.
Data Sharing Statement
All data about the present case report are confidential as per the patients’ data protection policy of Magrabi Eye Hospital, Tanta, Egypt. Access to these data will be granted exclusively to people or entities who meet the criteria for access to confidential data and only upon written request. All requests should be addressed to the Medical Director: Professor Hammouda Ghoraba, MD, Magrabi Eye Hospital, 107 El-Gaish Street, Tanta Qism 2, Tanta, Gharbia Governorate, Egypt.
Ethics and Patient Consent
Written informed consent has been provided by the patients to have the case details and accompanying images and/or videos published. This report does not contain any personally identifying information. This report acted on the tenets of the Declaration of Helsinki (2013 revision). The institutional review board of Magrabi Eye Hospital approved publishing the details of the cases.
Institution
The study was conducted in a retina tertiary care center (Magrabi Eye Hospital), in Tanta, Egypt.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding or grant support to report.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Colyer MH, Weber ED, Weichel ED., et al. Delayed intraocular foreign body removal without endophthalmitis during operations Iraqi freedom and enduring freedom. Ophthalmology. 2007;114(8):1439–1447. doi:10.1016/j.ophtha.2006.10.052
2. Justin GA, Baker KM, Brooks DI, Ryan DS, Weichel ED, Colyer MH. Intraocular foreign body trauma in operation Iraqi freedom and operation enduring freedom. Ophthalmology. 2018;125(11):1675–1682. doi:10.1016/j.ophtha.2018.06.006
3. Ghoraba HH, Leila M, Zaky AG, et al. Long-term outcome of pars plana vitrectomy for retained posterior segment intraocular foreign body secondary to gunshot injury. Clin Ophthalmol. 2021;15:1897–1904. doi:10.2147/OPTH.S311163
4. Cornut PL, Youssef EB, Bron A, et al. The French Institutional Endophthalmitis Study (FRIENDS) group. A multicenter prospective study of post-traumatic endophthalmitis. Acta Ophthalmol. 2013 Aug;91(5):475–482. doi:10.1111/j.1755-3768.2011.02349.x
5. Ehlers JP, Kunimoto DY, Ittoop S, Maguire JI, Ho AC, Regillo CD. Metallic intraocular foreign bodies: characteristics, interventions, and prognostic factors for visual outcome and globe survival. Am J Ophthalmol. 2008;146(3):427–433. doi:10.1016/j.ajo.2008.05.021
6. Chaudhry IA, Shamsi FA, Al-Harthi E, Al-Theeb A, Elzaridi E, Riley FC. Incidence and visual outcome of endophthalmitis associated with intraocular foreign bodies. Graefe’s Arch Clin Exp Ophthalmol. 2008;246(2):181–186. doi:10.1007/s00417-007-0586-5
7. Bhagat N, Nagori S, Zarbin M. Post-traumatic infectious endophthalmitis. Surv Ophthalmol. 2011;56:214–251. doi:10.1016/j.survophthal.2010.09.002
8. Anderson WD. Prophylactic antibiotics and endophthalmitis in Vietnam. Am J Ophthalmol. 1973;75:481–485. doi:10.1016/0002-9394(73)91161-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Salvage of a Penetrating Bilateral Testicular Gunshot Injury Using an Autologous Free Tunica Albuginea Graft from the Excised Contralateral Testis: A Case Report
Saad A, Al-Abed O, Hakouk S, Aldakak MA
Research and Reports in Urology 2026, 18:627689
Published Date: 7 July 2026