Back to Journals » Clinical Ophthalmology » Volume 19
En-Face OCT and Microperimetric Analysis of Intraretinal Microcysts in Eyes After Pars Plana Vitrectomy for Epiretinal Membrane
Authors Kaluzny JJ ![]() , Zabel P
, Zabel P ![]() , Suwala KA, Jaworski D
, Suwala KA, Jaworski D ![]() , Gebska-Toloczko M, Woznicki K, Pek-Grzybowska R
, Gebska-Toloczko M, Woznicki K, Pek-Grzybowska R
Received 21 February 2025
Accepted for publication 21 May 2025
Published 7 August 2025 Volume 2025:19 Pages 2587—2593
DOI https://doi.org/10.2147/OPTH.S524057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jakub J Kaluzny,1,2 Przemyslaw Zabel,1,3 Karolina Anna Suwala,1,2 Damian Jaworski,3 Martyna Gebska-Toloczko,1,2 Krzysztof Woznicki,4 Renata Pek-Grzybowska4
1Department of Sensory Organ Studies, Nicolaus Copernicus University, Collegium Medicum, Bydgoszcz, Poland; 2Oftalmika Eye Hospital, Bydgoszcz, Poland; 3Department of Ophthalmology, Nicolaus Copernicus University, Collegium Medicum, Bydgoszcz, Poland; 4Department of Ophthalmology, The Ludwik Blazek Multi-Specialist Hospital, Inowroclaw, Poland
Correspondence: Jakub J Kaluzny, Department of Sensory Organ Studies, Nicolaus Copernicus University in Torun, Collegium Medicum in Bydgoszcz, ul. Sandomierska 16, Bydgoszcz, 85-830, Poland, Tel +48 525855408, Email [email protected]
Purpose: To compare the location of microcystic macular edema (MME) with areas of retinal nerve fiber layer (RNFL) damage in the macula detected on en-face SDOCT in eyes that underwent pars plana vitrectomy (PPV) due to the epiretinal membrane (ERM).
Patients and Methods: Thirty-five eyes were enrolled at least 6 months after PPV with removal of ERM and inner limiting membrane (ILM). In each eye, en-face SDOCT and microperimetry were performed. The area of RNFL damage was measured and compared with the position of MME and correlated with the volume of retinal layers and retinal sensitivity (AT).
Results: MME was observed in 17 eyes (48.6%) in the area devoid of ILM, often in places with arcuate damage to the RNFL bundle. The mean area of RNFL damage in eyes with MME was 9.03 ± 5.3 mm2 and was significantly larger than in eyes where microcysts were not present, where it measured 3.92 ± 3.3 mm2. A significant negative correlation was observed between the area of RNFL damage and GCL volume and AT.
Conclusion: The topographic analysis of the MME position in eyes after PPV due to ERM confirmed the association of this pathology with ganglion cells and RNFL damage related to the removal of the ILM and ERM. There are probably two pathways leading to the development of MME: one starting from Muller cell damage during ILM peeling and the other due to retrograde death of ganglion cells in the areas of arcuate RNFL defects.
Keywords: epiretinal membrane, microcystic macular edema, en-face OCT, retinal nerve fiber layer, ganglion cell layer, microperimetry
Introduction
Due to its high resolution, Spectral Domain Optical Coherence Tomography (SDOCT) allows for the detection of even small amounts of fluid located within the retina. In 2012, the first descriptions of microcystic changes located in the retina of patients with multiple sclerosis appeared.1 They were characterized as perifoveal, thin, multiple hyporeflective cystoid spaces within an inner nuclear layer (INL). This condition was called microcystic macular edema (MME). It was described in various diseases involving damage to the optic nerve, starting from genetic, inflammatory origin diseases and ending with chronic glaucoma.2,3 Similar changes were also observed in 5.7–60.9% of eyes undergoing pars plana vitrectomy (PPV) due to an epiretinal membrane (ERM).4,5 Although the association between MME and ganglion cell layer (GCL) thickness reduction was found in this group of patients, the cause of such changes and the relationship with intraoperative ERM and inner limiting membrane (ILM) removal remains unclear. Dysli et al, demonstrated the origin of MME as the result of retrograde maculopathy related to ganglion cell loss.6 A recent study by Govetto et al, showed that postoperative MME is unlikely related to neurodegenerative processes and is rather attributable to Muller cell disruption.7 It is unclear if ganglion cell loss causes an alteration in Muller cell function, resulting in an impaired water pumping function, or whether Muller cell damage leads to trauma to retinal ganglion cells.
Except for structural abnormalities, the presence of MME also affects retinal function. Although visual field defects in eyes after PPV for ERM were related to retinal nerve fiber layer (RNFL) and GCL thinning, current studies have demonstrated that postoperative intraretinal microcysts also influence retinal sensitivity.8,9 A comparison of microperimetry and en-face OCT can reveal the structural abnormality responsible for scotomas observed in patients after surgery.
Our study aimed to compare the location of MME with areas of retinal nerve fiber layer (RNFL) damage in the macula detected on en-face SDOCT in eyes that underwent PPV due to ERM. Since this examination allows for measuring the area of RNFL damage and the area of MME, it will be possible to examine the correlation between these variables. Precise determination of the location of regions of RNFL damage and the presence of MME will also allow for the examination of the influence of these structural disorders on retinal sensitivity in microperimetry. We would like to verify the hypothesis that the decrease in retinal sensitivity in patients after PPV with ERM removal occurs in areas of RNFL damage and MME.
Materials and Methods
The study was a retrospective analysis of medical records of patients operated on for ERM by one surgeon (JJK) in the years 2021–2023 in two centers: Oftalmika Eye Hospital in Bydgoszcz and the Ophthalmology Department of the Multi-Specialist Hospital in Inowroclaw. The analysis included preoperative data and results from ophthalmological examinations conducted 6–12 months after surgery. The Bioethics Committee of Collegium Medicum, Nicolaus Copernicus University, approved the study (KB 225/2021). Due to the study’s retrospective nature, the Bioethics Committee agreed that patient-informed consent was unnecessary if deidentified data were analyzed. All patient confidential data was protected. This study adhered to the tenets of the Declaration of Helsinki.
The study included patients who underwent PPV due to decreased visual acuity and metamorphopsia related to the presence of idiopathic ERM. Exclusion criteria for participation in the study were the presence of an ERM secondary to another macular disease process, glaucoma, axial length > 26.0 mm, presence of another macular disease, diabetic retinopathy and previous eye surgeries except for uncomplicated phacoemulsification of cataract (at least 2 weeks before PPV) in any eye. The exclusion criterion was also the presence of cystoid macular edema after operation. Only pseudophakic eyes without signs of posterior capsule opacification were included in the study. ERM was defined as a demarcated hyperreflective line on the retinal surface visible on SDOCT cross-sections. It was classified according to the scale described by Govetto as follows: stage 1 is a mild ERM with preserved foveal depression and well-defined retinal layers; stage 2 is an ERM with loss of foveal depression; stage 3 is an advanced ERM with loss of foveal depression and presence of ectopic inner retinal layers over the central fovea; stage 4 is an advanced ERM with ectopic inner foveal layers and disruption of all retinal layers.7,10
All eyes included in the study underwent PPV using 25+G or 27G instruments (Alcon, Fort Worth, Texas, US) the Constellation apparatus (Alcon, Fort Worth, Texas, US) and the Lumera 700 surgical microscope (Zeiss, Oberkochen, Germany). The procedures were performed under local retrobulbar anesthesia. After excision of the cortical part of the vitreous body, ERM was stained using Membrane Blue Dual (Dorc, Zuidland, Netherlands). The ERM and ILM were removed using endoforceps. In the postoperative period, patients were treated with antibiotics and steroid drops.
Ophthalmological examinations performed before and after surgery included assessment of best corrected visual acuity (BCVA) using ETDRS charts, intraocular pressure measurement, and evaluation of the anterior segment and fundus in biomicroscopy. SDOCT (Spectralis OCT, Heidelberg Engineering, Germany) was performed in all examined eyes before and after the operation. The preoperative exam consisted of 61 horizontal cross-sections covering the macular area. To enable postoperative evaluation in the form of en-face images 384 horizontal SDOCT scans covering the macular area of 30 by 30 degrees were registered. Postoperative en-face SDOCT images obtained from the RNFL and INL slabs were analyzed. The areas of RNFL damage were manually marked as regions of nerve fiber loss, and they were identified as oval or arcuate areas of decreased reflectivity on en-face SDOCT. Microcyst clusters were identified as deposits of small hyporeflective spaces visible on en-face SDOCT images acquired from the INL. The surface area of RNFL damage and microcyst areas were measured using the software available in the device (Heidelberg Eye Explorer®, version 1.10.4.0). The volume of individual retinal layers was also measured, including the central area of the macula with a diameter of 3 mm. Results were presented in mm3 and as a percentage of the total retinal volume in the examined area.
After surgery, based on SDOCT cross-sections, eyes were divided into two groups: group 1 consisted of eyes with detected MME, while group 2 did not show the presence of microcysts. Three retinal specialists performed this separation independently, and only eyes with complete agreement among observers were included for the analysis.
Microperimetry was performed only after the operation using the Maia device (Centervue, Italy), using the full 4–2 threshold strategy covering 68 measurement points within the central 10 degrees. They were located in ten rows vertically and horizontally. The two central rows, vertically and horizontally, consisted of 10 measurement points. The peripheral rows consisted of 8, 6, and 2 points. The collective parameter analyzed was the average threshold (AT), the average sensitivity of all tested points in decibels (dB). Only technically good results without loss of fixation were analyzed. In each eye, the position of individual retinal sensitivity measurement points was examined by comparing the microperimetry result with the en-face SDOCT image.
Statistical analysis included checking the compliance of the distribution of individual features with the normal distribution using the Shapiro–Wilk test. Depending on the type of data distribution, the Student’s T test or Mann–Whitney U-test was used to compare the significance of differences between means. Next, Pearson and Spearman correlation coefficients and their statistical significance were calculated. Unless otherwise indicated, the data are given as mean values and ± standard deviation (SD) with the p-value threshold for statistical significance of less than 0.05.
Results
The study included 33 patients (16 women and 17 men) with an average age of 73.1 ± 7.4 years. Because two patients underwent surgery on both eyes, 35 eyes were enrolled in the study. MME was detected in 17 operated eyes (group 1), whereas SDOCT did not show the presence of microcysts in 18 operated eyes (group 2), which accounted for 48.6% and 51.4% of operated eyes, respectively.
Before surgery, ERM in group 1 was more advanced than in group 2, as evidenced by lower BCVA (0.55 logMar and 0.39 logMar, respectively) and higher mean foveal retinal thickness (575.0 µm and 496.8 µm, respectively). According to the Govetto classification, the highest fourth stage of ERM occurred in 9 eyes (69.2%) from group 1 and five eyes (31.25%) from group 2, and grade 3 in 7 and 10 eyes (41.18% and 55.5%), respectively. Grade 2 was observed in one eye in group 1 (5.9%) and three eyes in group 2 (16.7%). In the preoperative examination, microcysts were present in 5 eyes (29.4%) from group 1 and four from group 2 (22.2%). After PPV, eyes from group 1 were characterized by worse functional test results than those from group 2. Postoperative BCVA in group 1 was 0.22 logMar and AT 18.9 dB, while in eyes from group 2, it was 0.14 logMar and 22.1 dB, but these differences were not statistically significant. In both groups, retinal thickness in the fovea decreased compared to the preoperative examination to a similar level, measuring 392.5 µm in group 1 and 382.7 µm in group 2. A comparison of pre and postoperative parameters in both groups is presented in Table 1. In all eyes from group 1, microcysts appeared in the area devoid of ILM as a result of the procedure performed, often in places of the arcuate damage to the RNFL bundle (Figure 1). Such damage to the nerve fiber bundle was visible in the en-face OCT examination in 11 eyes from group 1 (64.7%) and in 5 eyes (27.8%) from group 2. Microcysts unrelated to localized RNFL defects were most often located in the temporal and inferior parts of the macula. The mean area of RNFL damage in eyes from group 1 was 9.03 ± 5.3 mm2 and was significantly larger than in eyes from group 2, where it measured 3.92 ± 3.3 mm2 (p ≤ 0.001). There was no significant correlation between the area of RNFL damage and the area of microcysts in the en-face OCT examination in eyes from group 1.
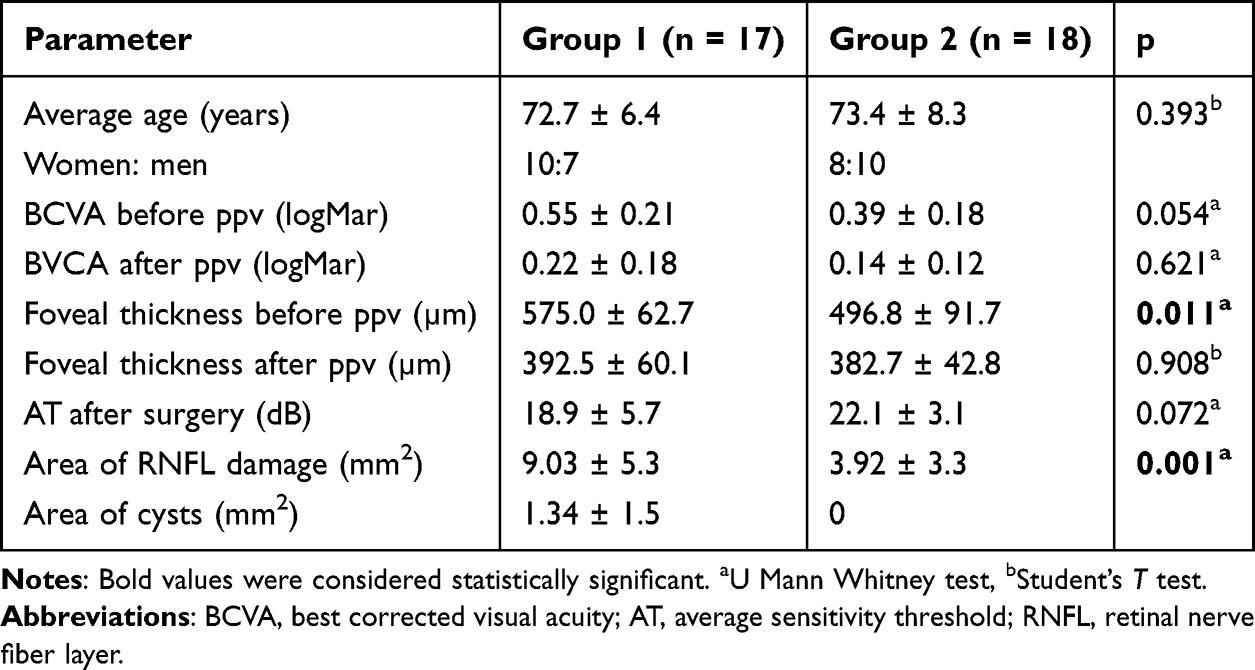 |
Table 1 Comparison of Structural and Functional Parameters Before and After the Surgery Between Groups |
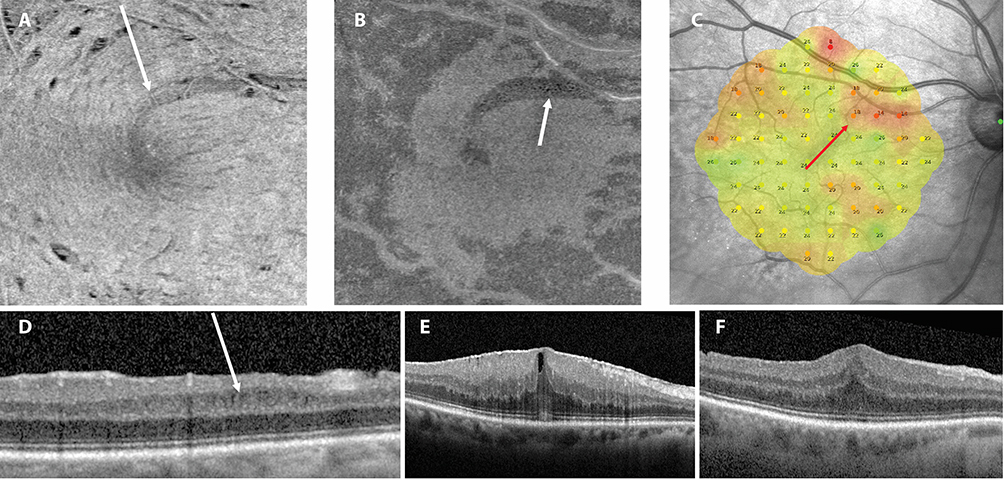 |
Figure 1 Occurrence of intraretinal microcysts in the projection of the arcuate retinal nerve fiber layer defect: (A) En-face SDOCT slab below ILM shows a hyporeflective area of the arcuate RNFL lesion (arrow), (B) En-face SDOCT slab of the ONL – small hyporeflective dots corresponding to microcysts in the projection of the RNFL lesion (arrow), (C) Reduced retinal sensitivity at the site of the RNFL lesion in microperimetry (red arrow), (D) Microcysts in the inner nuclear layer on SDOCT cross-section (arrow), (E) Central SDOCT scan before vitrectomy, (F) Central SDOCT scan after vitrectomy. Abbreviations: SDOCT, Spectral Domain Optical Coherence Tomography; ILM, Inner Limiting Membrane; RNFL, Retinal Nerve Fiber Layer; ONL, Outer Nuclear Layer. |
The volumes of individual retinal layers in the macula did not differ significantly between groups except for the GCL, which was thinner in group 1 but only when presented as a percentage of the entire macular volume, measuring 9.24% and 10.26% of total retinal volume, respectively, for group 1 and group 2 (p ≤ 0.05). The INL volume, when calculated in mm3 and as a percentage, was significantly higher in group 1 (Table 2). A significant negative correlation was observed between GCL volume and the area of RNFL damage, and a positive correlation was observed between the volume of INL, OPL, and IPL and the area of microcysts. These correlations are presented in Table 3.
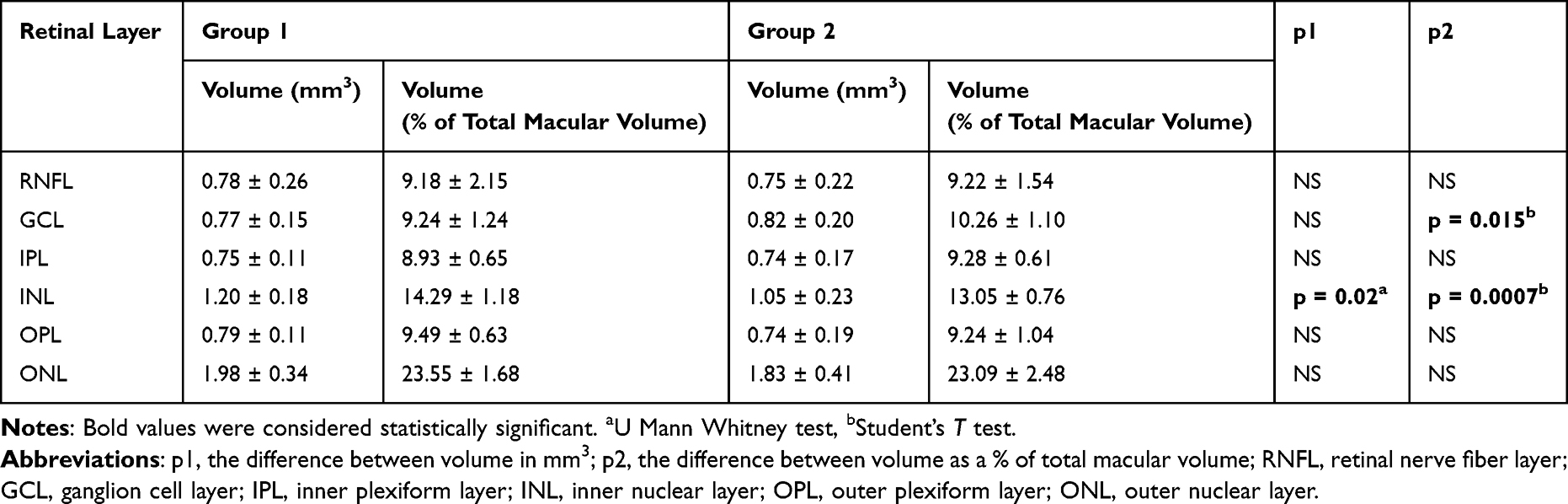 |
Table 2 The Volume of Individual Layers of the Retina in the Macula in Eyes with Microcysts (Group 1) and Without Them (Group 2) |
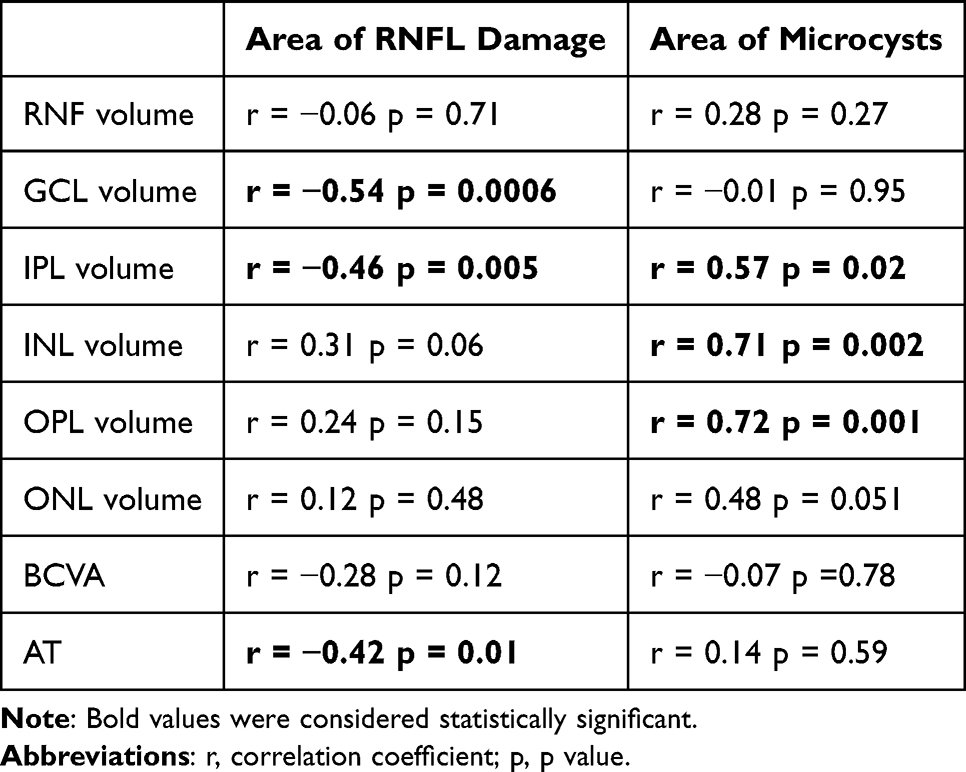 |
Table 3 Spearman Correlation Coefficients Between Area of RNFL Damage, Area of Microcyst, and Retinal Layers Volume and Selected Functional Parameters |
The AT in the macula was lower in group 1 compared to group 2, but this difference was only close to the level of statistical significance (Table 1). The points of reduced sensitivity in microperimetry corresponded to the areas of RNFL damage and, to a lesser extent, to the locations where microcyst clusters were found (Figure 2). A correlation was found between the area of RNFL damage and the AT (r = −0.42; p ≤ 0.05), as well as a correlation between the volume of GCL and AT (r = 0.48; p ≤ 0.01).
 |
Figure 2 Retinal sensitivity reduction in the eye after PPV with epiretinal membrane removal: (A) RNFL damage on the en-face SDOCT image. The boundaries of the damaged area are marked with arrows, (B) Microcysts located nasally to the fovea on the en-face SDOCT image (arrow), (C) Microperimetry shows two areas of reduced sensitivity, more significant from the temporal side corresponding to RMFL damage (thick red arrow) and less intense nasally to the fovea at the location of the microcyst (thin red arrow), (D) The central SDOCT section shows deep RNFL damage temporally from the fovea (thin arrow) and cysts located within the INL (thick arrow). Abbreviations: PPV, Pars Plana Vitrectomy; SDOCT, Spectral Domain Optical Coherence Tomography. |
Discussion
Topographic analysis of the MME position in eyes after PPV due to ERM indicates a relationship between the occurrence of microcysts and RNFL damage. Changes in the RNFL, referred to as the Dissociated Optic Nerve Fiber Layer (DONFL), were described in 43% of eyes after PPV in the areas of ILM and ERM peeling already in 2001.11 Subsequent studies demonstrated that these damages appear as dimples in the RNFL, which are readily visible on en-face SDOCT.12,13 In our study, the area of the RNFL damage was measured, and the result was compared between eyes with and without MME. It turned out that the mean area of the RNFL damage in eyes with MME was significantly larger than in eyes without microcysts. A detailed analysis of the microcysts locations revealed that they are often located at the site of damage to the retinal nerve fiber bundle. Such arcuate hyporeflective areas on the en-face SDOCT image were more often visible in the group of eyes with MME than in the group without microcysts. The above facts suggest that microcysts formed after vitrectomy primarily due to RNFL damage caused by ERM and ILM peeling. The primary cause of MME is probably damage to the Muller cell processes during ILM peeling, which causes trauma to retinal ganglion cells and, secondarily, the reduction of retinal nerve fibers.7,14,15 However, a strong topographical correlation between bundles of RNFL damage and the location of microcysts suggests a retrograde influence of damaged nerve fibers on ganglion cells.
Thinning of GCL in the ILM peeling area has been documented both after vitrectomy due to ERM and FTMH.6,16,17 RNFL and GCL thickness reduction were also observed in different types of optic neuropathies, demonstrating a similar mechanism of MME development related to ganglion cell damage.2 However, since there are studies where the frequency of MME is similar in the case of combined removal of ERM and ILM and only ERM, the significance of ILM peeling requires further studies.15 The next issue that needs explanation is the position of MME in the whole area of RNFL damage. Except for retinal nerve fiber bundles, microcysts were often located not in the place of deepest RNFL dimples but rather in places where the damage to nerve fibers was not so severe (Figure 2). This indicates that no retrograde way of MME can dominate in the area of ERM-ILM peeling except places where arcuate bundles of damaged RNFL directly influenced ganglion cells.
The second issue addressed by our study is the influence of MME on retinal function. Consistent with other authors, we did not observe a relationship between the presence of microcysts and BCVA after surgery.14,18,19 However, similar to the work of Matos et al, eyes with MME were characterized by lower retinal sensitivity compared to eyes without this symptom in SDOCT, but this difference was in the margin of statistical significance.9 Because the significant correlation of retinal sensitivity was observed with an area of RNFL damage and volume of GCL but not with an area of microcysts, the presence of MME has a lower impact on retinal function than RNFL and GCL damage. However, since the reduction of retinal sensitivity in the area of ILM peeling has been documented in the literature, it can be assumed that the presence of MME, as a consequence of significant damage to ganglion cells and retinal nerve fibers, will be associated with a substantial reduction in retinal sensitivity.20–22
The most important limitation of our study was its retrospective nature. The lack of preoperative en-face OCT and microperimetry did not allow for the exclusion of changes that could have influenced the final results. In addition, there was some variability in the observation time and surgical technique. The mean observation time and percentage of 25+ G and 27 G PPV performed in both groups were similar and probably did not significantly impact the results. Another limitation was the manual marking of the RNFL damage area and MME area. These changes were usually well-visible in the en-face SDOCT image, and the location of this border was usually unambiguous, but there were areas where subjective interpretation was possible.
In conclusion, the en-face OCT analysis of the MME position in eyes after PPV due to ERM confirmed the association of this pathology with ganglion cells and RNFL damage related to the ILM and EMR peeling. The MME pathway can likely start both from Muller cell and RNFL damage with secondary impact on retinal ganglion cells. The presence of microcysts, similar to reduced retinal sensitivity, is rather a sign of ganglion cell death than the cause of functional deterioration of the retina.
Disclosure
The authors have not received grant support or research funding, and they do not have any proprietary interests in the materials described in the article.
References
1. Gelfand JM, Nolan R, Schwartz DM, Graves J, Green AJ. Microcystic macular oedema in multiple sclerosis is associated with disease severity. Brain. 2012;135:1786–1793. doi:10.1093/brain/aws098
2. Kessel L, Hamann S, Wegener M, Tong J, Fraser CL. Microcystic macular oedema in optic neuropathy: case series and literature review. Clin Exp Ophthalmol. 2018;46(9):1075–1086. doi:10.1111/ceo.13327
3. Gaudric A, Audo I, Vignal C, et al. Non-vasogenic cystoid maculopathies. Prog Retin Eye Res. 2022;91:101092. doi:10.1016/j.preteyeres.2022.101092
4. Shiode Y, Morizane Y, Toshima S, et al. Surgical outcome of idiopathic epiretinal membranes with intraretinal cystic spaces. PLOS ONE. 2016;11(12):e0168555. doi:10.1371/journal.pone.0168555
5. Hsieh MH, Chou YB, Huang YM, et al. Inner nuclear layer microcyst configuration, distribution, and visual prognosis in patients with epiretinal membrane after vitrectomy and membrane peeling. Sci Rep. 2019;9(1):11570. doi:10.1038/s41598-019-48097-1
6. Dysli M, Ebneter A, Menke MN, et al. Patients with epiretinal membranes display retrograde maculopathy after surgical peeling of the internal limiting membrane. Retina. 2019;39(11):2132–2140. doi:10.1097/IAE.0000000000002266
7. Govetto A, Francone A, Lucchini S, et al. Microcystoid macular edema in epiretinal membrane: not a retrograde maculopathy. Am J Ophthalmol. 2025;272:48–57. doi:10.1016/j.ajo.2024.12.027
8. Akino K, Nagai N, Watanabe K, et al. Risk of newly developing visual field defect and neurodegeneration after pars plana vitrectomy for idiopathic epiretinal membrane. Br J Ophthalmol. 2021;105(12):1683–1687. doi:10.1136/bjophthalmol-2020-317478
9. Matos AMF, Defina RLS, Costa-Cunha LVF, et al. Correlation between retinal sensitivity assessed by microperimetry and structural abnormalities on optical coherence tomography after successful epiretinal membrane surgery. Int J Retina Vitreous. 2024;10(1):24. doi:10.1186/s40942-024-00542-8
10. Govetto A, Lalane RA, Sarraf D, Figueroa MS, Hubschman JP. Insights into epiretinal membranes: presence of ectopic inner foveal layers and a new optical coherence tomography staging scheme. Am J Ophthalmol. 2017;175:99–113. doi:10.1016/j.ajo.2016.12.006
11. Tadayoni R, Paques M, Massin P, et al. Dissociated optic nerve fiber layer appearance of the fundus after idiopathic epiretinal membrane removal. Ophthalmology. 2001;108(12):2279–2283. doi:10.1016/s0161-6420(01)00856-9
12. Mitamura Y, Suzuki T, Kinoshita T, et al. Optical coherence tomographic findings of dissociated optic nerve fiber layer appearance. Am J Ophthalmol. 2004;137(6):1155–1156. doi:10.1016/j.ajo.2004.01.052
13. Alkabes M, Salinas C, Vitale L, et al. En face optical coherence tomography of inner retinal defects after internal limiting membrane peeling for idiopathic macular hole. Invest Ophthalmol Vis Sci. 2011;52(11):8349–8355. doi:10.1167/iovs.11-8043
14. Liu J, Chen Y, Wang S, Zhang X, Zhao P. Evaluating inner retinal dimples after inner limiting membrane removal using multimodal imaging of optical coherence tomography. BMC Ophthalmol. 2018;18(1):155. doi:10.1186/s12886-018-0828-9
15. Güler M, Urfalıoğlu S, Damar Güngör E, Atalay E, Köküsarı G. Clinical and optical coherence tomography analysis of intraretinal microcysts in patients with epiretinal membrane. Semin Ophthalmol. 2021;36(8):787–793. doi:10.1080/08820538.2021.1906915
16. Cunha LP, Matos AMF, Defina RLS, et al. Assessment of ganglion cell complex thickness and its correlation with retinal sensitivity using microperimetry 6 months after epiretinal membrane surgery. Int J Retina Vitreous. 2024;10(1):58. doi:10.1186/s40942-024-00576-y
17. Baba T, Sato E, Oshitari T, Yamamoto S. Regional reduction of ganglion cell complex after vitrectomy with internal limiting membrane peeling for idiopathic macular hole. J Ophthalmol. 2014;2014:372589. doi:10.1155/2014/372589
18. Yang X, Wang Z, Yu Y, et al. Clinical features and prognosis in idiopathic epiretinal membranes with different types of intraretinal cystoid spaces. Retina. 2022;42(10):1874–1882. doi:10.1097/IAE.0000000000003537
19. Post M, Durajczyk M, Okruszko A, et al. Prognostic factors of visual acuity and macular morphology improvement after idiopathic epiretinal membrane surgery. Klin Oczna/Acta Ophthalmol Polonica. 2022;124(3):142–149. doi:10.5114/ko.2022.117375
20. Tadayoni R, Svorenova I, Erginay A, Gaudric A, Massin P. Decreased retinal sensitivity after internal limiting membrane peeling for macular hole surgery. Br J Ophthalmol. 2012;96(12):1513–1516. doi:10.1136/bjophthalmol-2012-302035
21. Deltour JB, Grimbert P, Masse H, Lebreton O, Weber M. Detrimental effects of active internal limiting membrane peeling during epiretinal membrane surgery: microperimetric Analysis. Retina. 2017;37(3):544–552. doi:10.1097/IAE.0000000000001179
22. Kaluzny JJ, Zabel P, Kaluzna M, et al. Macular sensitivity in the area of internal limiting membrane peeling in eyes after pars plana vitrectomy with the temporal inverted internal limiting membrane flap technique for a full-thickness macular hole. Retina. 2021;41(8):1627–1634. doi:10.1097/IAE.0000000000003096
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.