Back to Journals » Patient Preference and Adherence » Volume 20
Empowerment-Based Continuity of Care for Postoperative Upper Urinary Tract Calculi Patients with Double-J Stents: Effects on Self-Care and Compliance
Authors Li J, Guo S, Zhang W, Li H, Zhang Z, Qin X, Liu A
Received 13 October 2025
Accepted for publication 16 December 2025
Published 8 January 2026 Volume 2026:20 567700
DOI https://doi.org/10.2147/PPA.S567700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jiahui Li,1,* Shaowei Guo,1,* Wenxian Zhang,1 Huinan Li,1 Zhitao Zhang,1 Xiaohui Qin,2 Aying Liu1
1Department of Urology, Affiliated Hospital of Hebei University of Engineering, Handan, 056000, People’s Republic of China; 2Department of Rheumatology and Immunology, Affiliated Hospital of Hebei University of Engineering, Handan, 056000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohui Qin, Email [email protected]
Objective: To evaluate the effectiveness of a continuity-of-care model based on empowerment theory in patients with upper urinary tract calculi undergoing postoperative double-J stent placement.
Methods: A retrospective study was conducted on 124 patients treated from February 2024 to April 2025. Patients were assigned to a control group (routine nursing, n = 62) or an Intervention group (empowerment-based continuity care, n = 62). Compliance behavior, self-care ability (ESCA), self-efficacy (GSES), quality of life (WHOQOL-BREF), postoperative complications, and nursing satisfaction (NSNS) were compared between groups.
Results: The Intervention group showed higher compliance (91.94% vs 79.03%, P < 0.05). Post-intervention ESCA, GSES, and WHOQOL-BREF scores improved in both groups, with greater gains in the Intervention group (P < 0.05). Complication incidence was lower in the Intervention group (4.84% vs 16.13%, P < 0.05), and nursing satisfaction was higher (95.16% vs 82.26%, P < 0.05).
Conclusion: Empowerment-based continuity care significantly enhances self-care ability, adherence behavior, self-efficacy, and quality of life in postoperative double-J stent patients, while reducing complications and improving nursing satisfaction. This model supports patient-centered care and promotes active patient participation.
Project: Construction of an Empowerment Theory Model for Risk Prediction of Elderly Patients with Double-J Stent (Project No. 20250979).
Keywords: empowerment theory, continuity care, upper urinary tract calculi, double-J stent, self-care ability, compliance behavior
Introduction
Upper urinary tract calculi are among the most common diseases of the urinary system, characterized by high incidence, high recurrence rate, and frequent complications. If not treated promptly, they may lead to ureteral stricture, hydronephrosis, infection, or even renal function impairment.1,2 With the advancement of minimally invasive urological techniques, procedures such as percutaneous nephrolithotomy (PCNL) and flexible ureteroscopic lithotripsy (fURS) have become routine treatments for upper urinary tract calculi.3,4 To prevent postoperative ureteral edema, stricture, and to promote drainage, patients often require temporary double-J stent placement. Although the necessity of this procedure has been widely recognized, postoperative discomfort related to the stent (such as lumbar and abdominal pain, urinary frequency and urgency, hematuria, and foreign body sensation) and potential complications (infection, difficulty in discharge, etc.) negatively impact recovery and quality of life.5,6 Currently, after discharge, many patients still lack systematic guidance and nursing support, leading to suboptimal self-management of the stent, insufficient awareness of postoperative complications, and poor follow-up compliance.7 Traditional nursing models mainly focus on inpatient education and routine care; while nurses provide comprehensive pre- and postoperative instruction, they often lack structured, individualized post-discharge continuity interventions to meet patients’ multi-level recovery needs.8
Empowerment theory, originating from psychology and sociology, emphasizes shifting individuals from passive acceptance to active management through information support, skills training, and confidence building. Although most studies have applied this theory to chronic conditions, emerging evidence indicates its effectiveness in acute and short-term clinical contexts, such as postoperative recovery and acute symptom management.9,10 Its core lies in stimulating personal potential, enhancing health-related awareness, control, and decision-making ability, thereby promoting active participation in treatment and recovery. Based on this background, this study, guided by empowerment theory, constructed a systematic, staged, and personalized continuity care program for patients undergoing postoperative double-J stent placement. By comparing outcomes such as compliance behavior, self-care ability, self-efficacy, quality of life, complications, and nursing satisfaction between patients receiving empowerment-based continuity care and those receiving routine nursing, the study aims to evaluate the value and feasibility of this intervention and provide a theoretical basis for clinical nursing practice in urology.
Materials and Methods
Study Subjects and Design
This was a single-center retrospective controlled study. A retrospective analysis was conducted on the nursing intervention data of patients who underwent surgical treatment for upper urinary tract calculi with postoperative double-J stent placement in the Department of Urology of our hospital from February 2024 to April 2025. A total of 124 patients meeting the inclusion criteria were enrolled. (1) Inclusion criteria: ① Age 18–75 years, regardless of gender; ② Clear preoperative imaging diagnosis of upper urinary tract calculi and underwent minimally invasive stone removal procedures such as percutaneous nephrolithotomy or ureteroscopic lithotripsy; ③ Postoperative double-J stent placement with a duration of ≥2 weeks; ④ Normal communication ability and basic reading comprehension, able to cooperate in completing questionnaire assessments; ⑤ Voluntary participation in the study and signed informed consent. (2) Exclusion criteria: ① Combined with severe cognitive impairment, mental illness, or inability to comply with follow-up; ② Combined with urinary malignancy, severe infection, renal failure, or other severe underlying diseases; ③ Severe pre-existing urinary dysfunction (examples include chronic urinary retention, neurogenic bladder, obstructive uropathy, or significant bladder dysfunction) or urogenital malformation before stent placement; ④ Interrupted nursing follow-up due to patient relocation, communication difficulties, or incomplete data during the study intervention. Patients were divided into two groups according to the actual nursing intervention received: Control group (n = 62): received routine follow-up and health guidance nursing after discharge; Intervention group (n = 62): received continuity care intervention guided by empowerment theory after discharge. This study was approved by the Medical Ethics Committee of Affiliated Hospital of Hebei University of Engineering (Approval No. 2024[K]069) and was conducted in strict accordance with the ethical principles of the Declaration of Helsinki.
Nursing Intervention Methods
Control Group
Patients in the control group received basic care and routine health education during hospitalization. The content included: Preoperative guidance: Introduction to the surgical method, expected postoperative symptoms (eg, transient hematuria and mild urinary irritation), dietary precautions, and psychological support to help alleviate anxiety. Postoperative health education: Before discharge, the responsible nurse provided verbal instructions focusing on hydration management, appropriate physical activity, infection prevention, follow-up procedures, and self-monitoring of the double-J stent. Follow-up reminders: Routine telephone reminders were provided to inform patients of regular postoperative check-ups and scheduled stent removal. The frequency was not fixed and depended on medical orders.
Intervention Group
Patients in the intervention group received a structured continuity care intervention guided by empowerment theory in addition to routine care. Before the intervention, a continuity care team was established. All team members received unified training to ensure consistency in theoretical understanding and service delivery. A standardized workflow, supervision mechanism, and emergency response protocol were developed to ensure timely guidance for patients with urgent symptoms. Although PCNL and fURS differ in surgical approach, their postoperative double-J stent–related care and follow-up requirements are clinically consistent, including hydration guidance, symptom monitoring, infection prevention, and scheduled stent removal. Therefore, the same follow-up protocol was applied to both groups of patients. The continuity care consisted of the following components:
(1) Pre-discharge phase: Assessment and initial empowerment activation: ① Nursing needs assessment: On postoperative days 1–2, the responsible nurse conducted standardized one-on-one assessments to evaluate patients’ baseline health knowledge, psychological state, education level, family support, and self-management ability. These findings formed the basis for individualized intervention planning. ② Personalized education: Based on the assessment, tailored education was provided using illustrated manuals, nursing animations, and demonstration models. The key content included: Function and precautions of the double-J stent; Monitoring of expected postoperative symptoms (eg, transient hematuria, mild urgency, dysuria); Identification of true early complications (eg, fever, worsening flank pain, severe hematuria, signs of infection); Hydration and diet management; Recording of urination and daily symptoms; Emotional and stress-relief techniques. ③ Guidance for family involvement: Family involvement is not routinely implemented in all urological perioperative care. In this program, families were formally educated and assigned structured roles to support daily care and emotional management, establishing a coordinated “medical staff–patient–family” model.
(2) Post-discharge phase: Continuity case management: ① Multi-channel information support: A “Nursing Empowerment WeChat Group” was established for remote communication. The nursing team regularly updated multimedia materials including educational videos, hydration/exercise reminders, FAQs, case sharing, and online assessments to improve comprehension and engagement. ② Scheduled telephone follow-ups: Follow-up assessments were conducted at week 1, week 2, week 4 after surgery, and one week after stent removal. Assessment content included: Adaptation to the stent; Hydration behavior; Urination pattern; Recognition of warning symptoms; Psychological status; Execution of self-care behaviors. Management of mild conditions: Symptoms such as transient hematuria, mild bladder irritation, light flank soreness, and mild dysuria, which are considered normal postoperative reactions, were managed through telephone guidance with emphasis on hydration and monitoring. Management of possible complications: Fever, severe flank pain, worsening hematuria, unbearable urinary symptoms, suspected stent migration, or signs of infection required prompt hospital visit according to the established emergency response protocol. ③ Individualized goal management: Stage-specific goals (eg, achieving hydration targets, accurate symptom recording, timely recognition of warning signs) were set and revised at each follow-up. Patients kept a “health diary” documenting water intake, urination, symptoms, and emotional status. A simple reward mechanism was used to enhance motivation and self-efficacy. ④ Psychological and behavioral support: Regular psychological counseling was provided to address anxiety, irritation from stent-related discomfort, and sleep or lifestyle disruptions. The purpose of guiding patients to develop positive expectations was not to alter surgical outcomes or determine stent-removal timing, but to: improve adherence to hydration and self-monitoring, reduce unnecessary fear or avoidance of movement, promote early recognition of complications, enhance rehabilitation engagement.
(3) Follow-up and stent removal phase: Handover, evaluation, and feedback: ① Advance reminders: Patients were reminded 2–3 days in advance to attend hospital follow-up and stent removal to avoid missed appointments. ② Nursing handover report: The responsible nurse summarized the patient’s continuity-care process (eg, follow-up records, diary data, abnormal symptoms) and provided a written handover to clinical staff. ③ Post-removal evaluation: Within one week after stent removal, the nurse conducted a final evaluation and provided recommendations for further rehabilitation and long-term health management.
(4) Additional explanation of workforce and cost: On average, each patient required approximately 15–30 minutes of nursing staff time per week, including telephone follow-ups, data recording, preparation of educational materials, and case management. These time and labor costs were borne by the continuity care team and did not increase patients’ financial burden.
Observation Indicators
Medication Adherence Behaviors
Evaluated based on patients’ adherence to postoperative medication, regular follow-ups, timely stent removal, and dietary control. Evaluation criteria include: complete adherence (fully following medication regimen, review schedule, and lifestyle recommendations), partial adherence (non-adherence <5 times during the entire care period), and non-adherence (non-adherence ≥5 times during the care period). Adherence rate = (complete adherence + partial adherence)/total cases × 100%.
Self-Care Ability Assessment
Conducted Before and After intervention using the Exercise of Self-Care Agency Scale (ESCA, Cronbach’s α = 0.813, validity = 0.832).11 Although patients after PCNL or fURS remain in an acute postoperative phase, assessing self-care ability is still clinically meaningful, as appropriate hydration, symptom monitoring, early complication recognition, and timely follow-up participation are essential for recovery during this period. The ESCA evaluates four dimensions—self-concept, self-care responsibility, self-care skills, and health knowledge. Total score is 172 points; higher scores indicate stronger self-care ability.
Self-Efficacy Assessment
Conducted Before and After intervention using the General Self-Efficacy Scale (GSES, Cronbach’s α = 0.841, validity = 0.802).12 In acute postoperative recovery, self-efficacy strongly influences patients’ confidence in managing discomfort, adhering to hydration and activity guidance, and performing self-monitoring behaviors. Therefore, evaluating self-efficacy is relevant and beneficial in this clinical context. The GSES contains 10 items, scored on a 1–4 scale, with total scores ranging from 10–40. Higher scores represent stronger self-efficacy.
Quality of Life Assessment
Conducted Before and After intervention using the WHOQOL-BREF (Cronbach’s α = 0.854, validity = 0.822),13 covering physical, psychological, social, and environmental domains. Total score is 100; higher scores indicate better quality of life.
Postoperative Complications
Postoperative symptoms such as transient hematuria and mild bladder irritation are generally regarded as expected physiological reactions following ureteroscopic or percutaneous nephrolithotomy procedures rather than true complications. Therefore, in this study, only clinically significant events requiring medical intervention—such as urinary tract infection, severe or persistent hematuria, obvious bladder irritation symptoms affecting daily life, and double-J stent displacement/slippage—were recorded as postoperative complications. Complication rates were uniformly evaluated by the hospital’s clinical team.
Nursing Satisfaction
Assessed using the Newcastle Satisfaction with Nursing Scale (NSNS, Cronbach’s α = 0.815, validity = 0.782).14 Nursing satisfaction is an important indicator of the quality of continuity care, as it reflects patients’ perceptions of communication, responsiveness, emotional support, and service coordination—key components that directly influence adherence, anxiety reduction, and overall recovery experience. The scale includes 19 items scored using a 5-point Likert scale. Satisfaction is classified as: very satisfied (≥76 points), satisfied (57–75 points), average (38–56 points), and dissatisfied (<38 points). Total satisfaction rate = (very satisfied + satisfied)/total cases × 100%.
Statistical Methods
GraphPad Prism 8 was used for data visualization, and SPSS 25.0 for statistical analysis. Categorical data were expressed as n (%) and analyzed with χ2-test. Continuous data were expressed as ( ), with independent sample t-test used for between-group comparisons and paired t-test for within-group comparisons. P < 0.05 was considered statistically significant.
), with independent sample t-test used for between-group comparisons and paired t-test for within-group comparisons. P < 0.05 was considered statistically significant.
Results
Comparison of General Data Between Groups
There were no significant differences in gender, age, stone location, surgical method, or education level between the two groups (P > 0.05), indicating comparability. See Table 1.
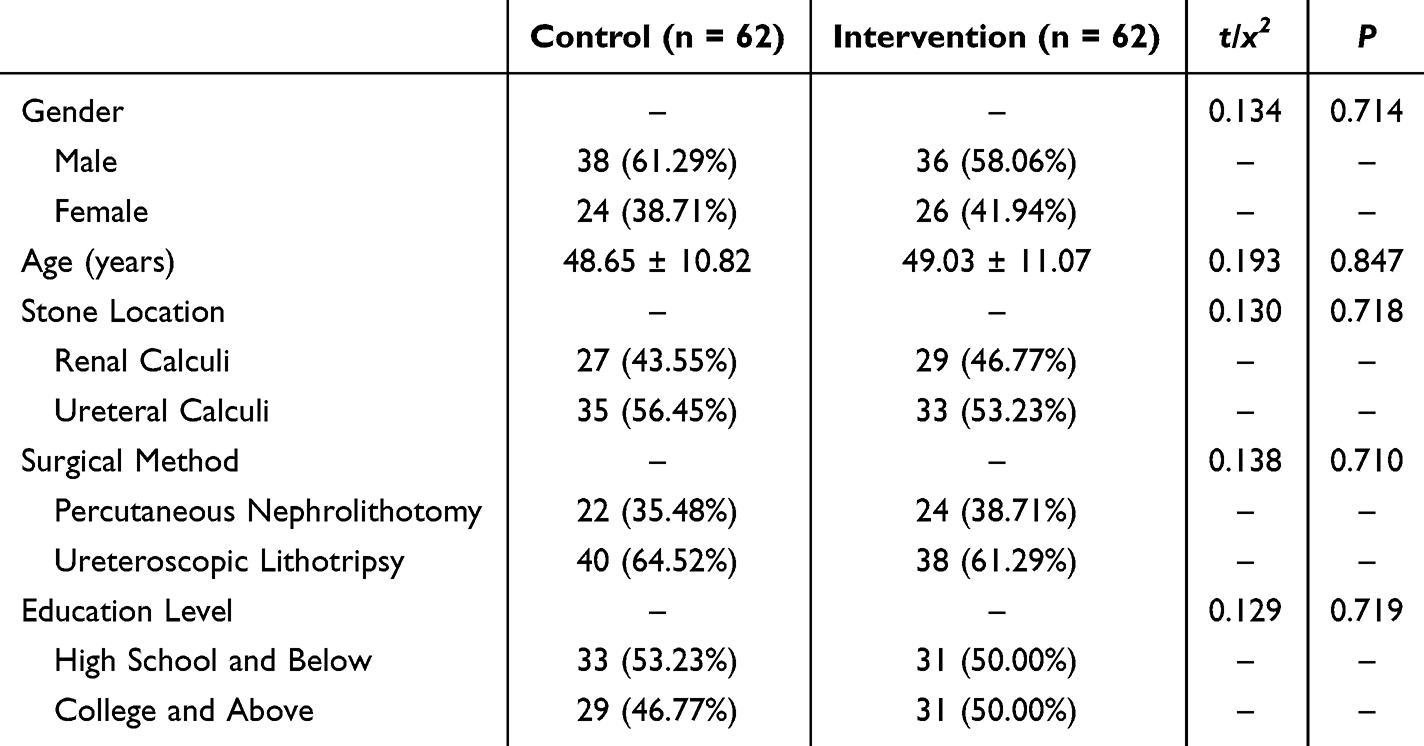 |
Table 1 Comparison of General Data Between the Two Groups ( |

Comparison of Medication Adherence Behaviors Between Groups
In the control group (n = 62), 33 showed complete adherence, 16 partial adherence, and 13 non-adherence. In the Intervention group (n = 62), 44 showed complete adherence, 13 partial adherence, and 5 non-adherence. The adherence rate in the Intervention group (91.94%) was significantly higher than in the control group (79.03%) (P < 0.05). See Figure 1.
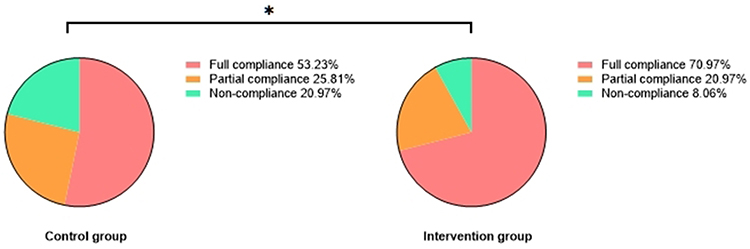 |
Figure 1 Comparison of Medication Adherence Behaviors Between Groups [n (%)]. Note: Between-group comparison, *P < 0.05. |
Comparison of Self-Care Ability Between Groups
Post intervention, the scores for self-concept, self-care responsibility, self-care skills, and health knowledge improved in both groups compared to Pre intervention, with greater improvement in the Intervention group (P < 0.05). See Figure 2.
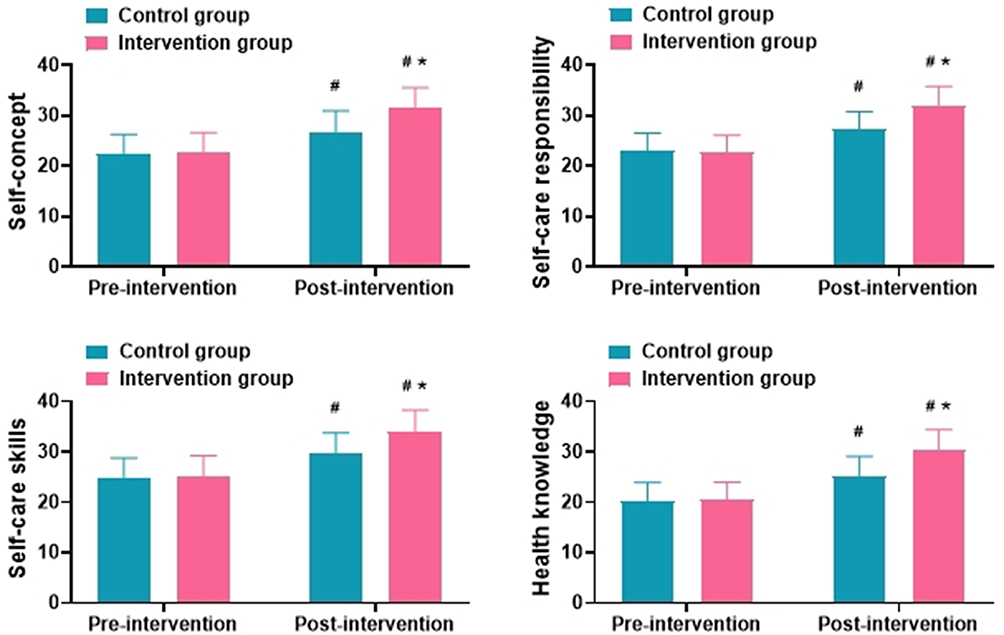 |
Figure 2 Comparison of Self-Care Ability Between Groups ( Note: Compared with same group Pre-intervention, #P < 0.05; Between-group comparison, *P < 0.05. |

Comparison of Self-Efficacy and Quality of Life Between Groups
Post intervention, GSES and WHOQOL-BREF scores increased in both groups compared to Pre intervention, with greater improvement in the Intervention group (P < 0.05). See Figure 3.
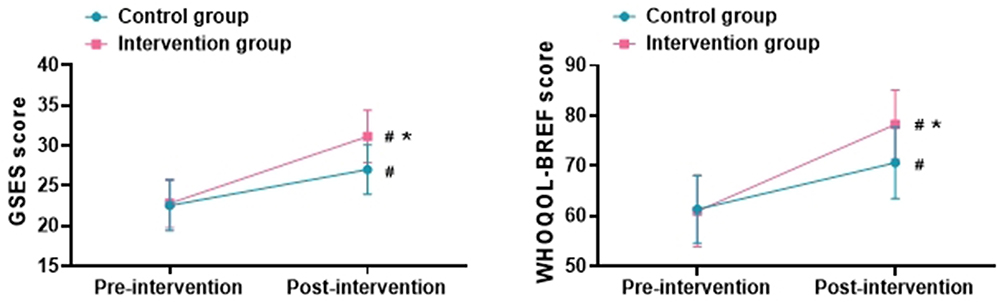 |
Figure 3 Comparison of Self-Efficacy and Quality of Life Between Groups ( Note: Compared with same group Pre-intervention, #P < 0.05; Between-group comparison, *P < 0.05. |

Comparison of Postoperative Complication Rates Between Groups
The complication rate was significantly lower in the Intervention group (4.84%) compared to the control group (16.13%) (P < 0.05). See Table 2.
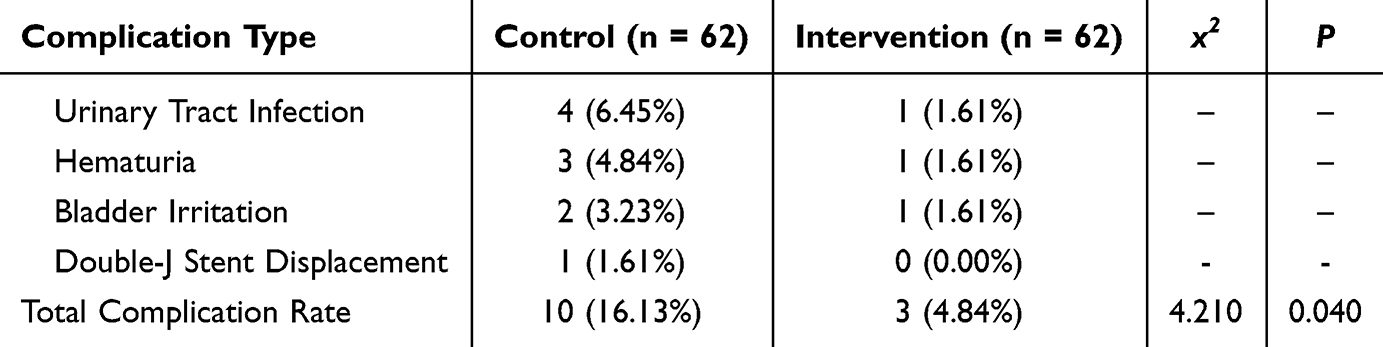 |
Table 2 Comparison of Postoperative Complication Rates Between Groups [n (%)] |
Comparison of Nursing Satisfaction Between Groups
The overall nursing satisfaction rate was higher in the Intervention group (95.16%) than in the control group (82.26%) (P < 0.05). See Table 3.
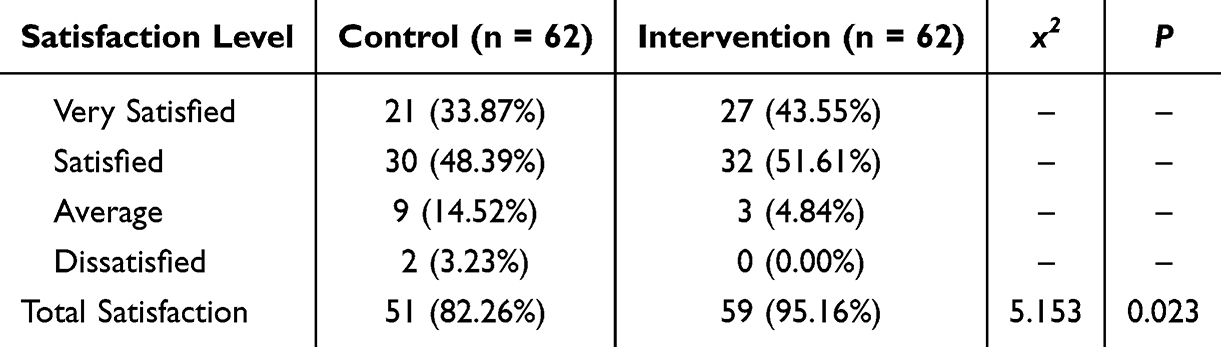 |
Table 3 Comparison of Nursing Satisfaction Between Groups [n (%)] |
Discussion
Double-J stent placement after upper urinary tract stone surgery is one of the common treatment measures in modern urological surgery. Although this method effectively maintains postoperative drainage and reduces the incidence of complications such as ureteral stricture and hydronephrosis, it can also trigger a series of discomfort symptoms, such as frequent urination, urgency, lower abdominal distension and pain, hematuria, and foreign body sensation.15,16 Moreover, due to patients’ lack of knowledge regarding double-J stent management and poor adherence, the incidence of postoperative complications remains high, making it difficult to ensure postoperative recovery and quality of life.17 Therefore, there is an urgent need for scientific nursing interventions to improve patients’ postoperative management ability and adherence behavior. Empowerment theory emphasizes the cultivation of patients’ self-efficacy and health decision-making capacity, focusing on viewing the patient as the main agent of health management. By empowering patients with knowledge, skills, and confidence, it guides them to actively participate in the entire process of disease prevention, treatment, and rehabilitation.18,19 In this study, the continuity of care constructed based on empowerment theory not only included health guidance after discharge but also relied on individualized intervention strategies, integrating multiple methods such as follow-up management, psychological counseling, skills training, and information feedback to facilitate a shift from “passive treatment reception” to “active self-management.” This intervention model breaks through the limitations of traditional nursing services that are confined to the inpatient stage, establishing a continuous and systematic nursing chain and providing solid support for patients’ postoperative recovery.20
The results of this study showed that patients in the Intervention group had significantly better adherence behavior compared to the control group (91.94% vs 79.03%, P < 0.05), which is consistent with findings from previous related studies,21–23 indicating that empowerment-based continuity of care can effectively improve patients’ compliance with medical advice. On one hand, systematic health education and behavioral guidance increased patients’ understanding of the disease,24 making them aware of the importance of standardized double-J stent management; on the other hand, individualized home visits, WeChat follow-ups, and family care support enhanced patients’ sense of responsibility and self-control, thereby strengthening their intrinsic motivation for self-management. In terms of self-care ability, the Intervention group showed significantly better improvements in dimensions such as self-concept, sense of self-care responsibility, self-care skills, and health knowledge compared to the control group (P < 0.05). This suggests that the nursing intervention not only imparted the necessary operational skills but also emphasized the process of cognitive and behavioral transformation in patients.25 Under the empowerment theory, the intervention model fostered behavioral habits based on cognitive changes through encouragement, feedback, and a sense of participation, ultimately internalizing the goals of nursing.
Further analysis in this study found that the continuity of care intervention significantly improved patients’ GSES scores and WHOQOL-BREF scores, with the Intervention group showing greater improvement than the control group (P < 0.05). This result supports the core idea of Bandura’s self-efficacy theory: an individual’s confidence in controlling their disease is a prerequisite for adopting effective health behaviors.26 In a study by Ouyang et al,27 phase-based encouragement, problem-solving training, and outcome feedback effectively enhanced stroke patients’ sense of achievement and control, which was also reflected in this study. Moreover, improvement in quality of life not only stemmed from symptom control itself but was also closely related to positive changes in psychological state.28 Related studies29 have pointed out that empowerment nursing focuses on patients’ subjective experiences and emotional responses, effectively alleviating anxiety, fear, and other negative emotions during the intervention process and helping them better adapt to life conditions.
Regarding complications and satisfaction, the results of this study showed that the postoperative complication rate in the Intervention group was significantly lower than that in the control group (4.84% vs 16.13%, P < 0.05), indicating the significant role of continuity of care interventions in postoperative risk control. Possible mechanisms include: ① patients acquired proper urination techniques, water intake guidance, and early warning signs of stent issues, allowing for timely problem identification; ② healthcare providers performed timely interventions via remote monitoring to prevent problem escalation; ③ with the support of nursing staff, patients were more willing to express discomfort and seek help proactively, thus avoiding small problems turning into major complications.30 At the same time, the Intervention group reported significantly higher nursing satisfaction compared to the control group (95.16% vs 82.26%, P < 0.05), demonstrating that empowerment-based continuity of care can effectively enhance patients’ overall medical experience. The high satisfaction observed is consistent with the intensive and structured nature of the intervention, which included personalized education, frequent follow-up contacts, symptom monitoring, psychological support, and family involvement. Patients experienced increased reassurance, trust, and engagement in their recovery process, which likely contributed to higher perceived quality of care and adherence.31 While this model requires dedicated time and effort from the care team, the observed benefits indicate that such interventions can yield meaningful improvements in patient experience. In practice, appropriate planning and workflow optimization, including use of digital tools for follow-up, can help maintain intervention effectiveness while managing resource demands, supporting its feasibility in routine clinical settings.
This study integrates empowerment theory with the concept of continuity of care to develop a systematic intervention program tailored for patients with double-J stent placement after upper urinary tract stone surgery and evaluates its effects from multiple dimensions. It represents a beneficial expansion of traditional urological nursing models. Compared with previous care methods that focused solely on operational training or psychological counseling, this program places more emphasis on the systematic cultivation of self-management ability and behavior formation, with good practicability and prospects for promotion. However, this study still has some limitations. First, it is a single-center retrospective design with a limited sample size, which may present selection bias; second, self-reported data from patients (eg, ESCA, GSES) may be influenced by subjective factors; additionally, the intervention cycle of the study was relatively short, and it did not observe long-term behavior maintenance. Future studies can verify the wide applicability and long-term effects of this intervention model through multicenter, prospective randomized controlled trials and optimize care pathways by integrating intelligent follow-up platforms to achieve a truly “continuous, empowering, and collaborative” nursing model.
Conclusion
This study demonstrates that the continuity-of-care model based on empowerment theory provides significant benefits for patients undergoing double-J stent placement after upper urinary tract stone surgery. Compared with conventional nursing, this model effectively improved patients’ self-care abilities and adherence behaviors, and significantly enhanced their self-efficacy, quality of life, and nursing satisfaction. The Intervention group achieved better outcomes across all evaluation scales and exhibited a lower incidence of complications than the control group. These findings indicate that systematic and individualized empowerment-based continuity care supports patient-centered practice while promoting patients’ active participation and sense of health responsibility. Future clinical work should focus on standardizing this care model, strengthening nurse training, and further improving the precision of patient education to optimize its broader clinical application.
Funding
Constructing a Predictive Model for Reducing Risk in Elderly Patients with Double-J Stents Based on Empowerment Theory (Hebei Provincial Health Commission, No. 20250979.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xu LW, Yu CH, Hu HY, et al. [Comparison of the efficacy of thulium fiber laser and holmium laser lithotripsy in the treatment of upper urinary tract stones]. Zhonghua Yi Xue Za Zhi. 2023;103(30):2307–10. doi:10.3760/cma.j.cn112137-20230614-01011
2. Ying Z, Dong H, Li C, et al. Efficacy analysis of tip-flexible suction access sheath during flexible ureteroscopic lithotripsy for unilateral upper urinary tract calculi. World J Urol. 2024;42(1):626. doi:10.1007/s00345-024-05325-2
3. Tang RH, Wang HR, Song LQ, et al. [Efficacy and safety of flexible ureteral lithotripsy for upper urinary tract calculi in patients aged 80 years and older]. Zhonghua Yi Xue Za Zhi. 2024;104(24):2229–2233. doi:10.3760/cma.j.cn112137-20231205-01294
4. Yang T, Song R, Meng X, et al. A single center study that evaluates the preclinical use of a newly developed software and moving bed system to facilitate the spontaneous excretion of residual fragments after primary stone treatment (RIRS or PCNL). World J Urol. 2022;40(2):585–591. doi:10.1007/s00345-021-03863-7
5. Wang R, Xu B. [Influence of traditional double-J stent versus Polaris loop stent on the quality of life and erectile function of young and middle-aged men after ureteral laser lithotripsy]. Zhonghua Nan Ke Xue. 2020;26(1):48–53.
6. Corrales M, Keller EX, Barghouthy Y, et al. Silicone double-j stents for long-term ureteral stenting: results from a multicentric PEARLS analysis. World J Urol. 2025;43(1):292. doi:10.1007/s00345-025-05481-z
7. OuYang J, Li J, Wang B, Wu J, Chen J, Zheng X. The effects of a nurse-led HAPA-based discharge planning on post-operative outcomes in urolithiasis patients with double-J stents: protocol for a randomized controlled trial. Ann Med. 2025;57(1):2519676. doi:10.1080/07853890.2025.2519676
8. Du S, Hao Y, Jiao Y. Effect of the holistic nursing model of responsibility system on the mental state of elderly patients with limb fractures fixed by splints in the emergency department [retracted in: J Healthc Eng. 2023 Nov 29;2023:9798461. doi: 10.1155/2023/9798461]. J Healthc Eng. 2023;2023:1271606. doi:10.1155/2023/1271606
9. Xu Q, Jiang H, Li Y, Qi X, Chen L. Construction and verification of rehabilitation nursing program for shoulder and neck discomfort after thyroid cancer surgery: a pilot randomized controlled trial. Medicine. 2024;103(33):e39291. doi:10.1097/MD.0000000000039291
10. Shabany M, NikbakhtNasrabadi A, Mohammadi N, Pruitt SD. Family-centered empowerment process in individuals with spinal cord injury living in Iran: a grounded theory study. Spinal Cord. 2020;58(2):174–184. doi:10.1038/s41393-019-0348-3
11. Li YD, Qu N, Yang J, et al. Effects of an Omaha system-based follow-up regimen on self-care and quality of life in gastrointestinal surgery patients. World J Gastrointest Surg. 2023;15(10):2179–2190. doi:10.4240/wjgs.v15.i10.2179
12. Zhang Q, Lan Q, Cao -Z-Z, et al. [Application of IMCHB based nursing model in self-efficacy and negative emotion of prostate cancer radiotherapy patients]. Zhonghua Nan Ke Xue. 2023;29(10):938–943.
13. Fan LB, Gao B, Mu YZ, et al. [A comparative study on quality of life of pneumoconiosis patients between from rural migrant workers and from a state-owned enterprise in Zhaotong City Yunnan Province]. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. 2021;39(7):515–519. doi:10.3760/cma.j.cn121094-20201009-00563
14. Yin H. Enhanced recovery after surgery (ERAS) in postoperative lung cancer patients: a novel perioperative strategy for preventing venous thromboembolism and improving quality of life. Tohoku J Exp Med. 2024;262(3):201–209. doi:10.1620/tjem.2023.J105
15. Damavand RS, Esmaeili S, Bateni BH, et al. Comparing the effect of peri-operative antibiotic prophylaxis only with continuous low-dose antibiotic treatment on the incidence of urinary tract infection and stent related-symptoms in patients undergoing Double-J (DJ) stent insertion following transurethral lithotripsy (TUL). World J Urol. 2023;41(11):3027–3032. doi:10.1007/s00345-023-04585-8
16. Negi SK, Kumar P, Desai S, et al. The effect of no oral antibiotic versus 7 days oral antibiotic during discharge in double J stented patients on stent related urinary tract infection: a randomized study. Urologia. 2024;91(2):379–383. doi:10.1177/03915603231199524
17. Nogara A, Lucignani G, Turetti M, et al. Prevalence and predictors of stone passage after double J stenting for symptomatic ureteral stones: a cross-sectional, real-life study. World J Urol. 2024;42(1):8. doi:10.1007/s00345-023-04717-0
18. Glachs D, Namli T, Strohmeier F, et al. A predictive model-based decision support system for diabetes patient empowerment. Stud Health Technol Inform. 2021;281:963–968. doi:10.3233/SHTI210321
19. Qin Y, Li M, Nian C, et al. Application and efficacy analysis of empowerment theory-based Pharmacological intervention in the rehabilitation of children with autism. Pak J Pharm Sci. 2025;38(2):439–447.
20. Gearhart MC. Mutual efficacy, self-efficacy, and collective efficacy theory: an examination of empowerment and activism. Soc Work. 2023;68(3):192–200. doi:10.1093/sw/swad018
21. Feng C, Zhang A, Long H, et al. [Effect of whole-course empowerment health intervention on psychological resilience and self-care ability in older patients with severe pneumonia]. Sichuan Da Xue Xue Bao Yi Xue Ban. 2024;55(6):1587–1592. doi:10.12182/20241160608
22. Vasli P, Zahedinia S, Hosseini M, et al. A protection motivation theory-based empowerment intervention for promoting health behaviors in women with human papillomavirus: an experimental study. Sex Transm Dis. 2023;50(11):e34–e36. doi:10.1097/OLQ.0000000000001864
23. Tao Y, Wang Y. Effect of empowerment theory health education on disease control level and compliance of elderly T2DM. Pak J Pharm Sci. 2023;36(2(Special)):643–648.
24. Damgaard AJ, Primdahl J, Esbensen BA, et al. Self-management support needs of patients with inflammatory arthritis and the content of self-management interventions: a scoping review. Semin Arthritis Rheum. 2023;60:152203. doi:10.1016/j.semarthrit.2023.152203
25. Shojaei MS, Tavakoly Sany SB, Ghavami V, et al. An educational intervention based on family-centered empowerment model to modify high-risk behaviors of brucellosis via mother education. Sci Rep. 2022;12(1):18869. doi:10.1038/s41598-022-23385-5
26. Alimohammadi L, Zarei F, Mirghafourvand M. The effect of counseling based on Bandura’s self-efficacy theory on sexual self-efficacy and quality of sexual life. Women Health. 2020;60(4):473–486. doi:10.1080/03630242.2019.1662871
27. Ouyang RG, Long Y, Zhang J-Q, et al. Interventions for improving self-efficacy in patients after stroke based on self-efficacy-related principles of Bandura’s cognition theory: a systematic review and meta-analysis. Top Stroke Rehabil. 2023;30(8):820–832. doi:10.1080/10749357.2023.2172832
28. Liu T, Zhang R, Yao H, et al. Efficacy of an emotion and stress management program based on empowerment theory on family caregivers of stroke survivors. Pak J Med Sci. 2025;41(2):494–500. doi:10.12669/pjms.41.2.11350
29. Göger S, Şener Ş, Cingil LD. The effect of training to diabetes patients according to planned behavior theory on self-efficacy and patient empowerment: a randomized study. Prim Care Diabetes. 2024;18(5):486–492. doi:10.1016/j.pcd.2024.08.002
30. Elyasi M, Lai H, Major PW, et al. Modeling the theory of planned behaviour to predict adherence to preventive dental visits in preschool children. PLoS One. 2020;15(1):e0227233. doi:10.1371/journal.pone.0227233
31. Heywood S, Bunzli S, Dillon M, et al. Trauma-informed physiotherapy and the principles of safety, trustworthiness, choice, collaboration, and empowerment: a qualitative study. Physiother Theory Pract. 2025;41(1):153–168. doi:10.1080/09593985.2024.2315521
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.