Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Empathy In Neurodegenerative Diseases: A Systematic Review
Authors Pick E ![]() , Kleinbub JR
, Kleinbub JR ![]() , Mannarini S
, Mannarini S ![]() , Palmieri A
, Palmieri A ![]()
Received 3 August 2019
Accepted for publication 31 October 2019
Published 22 November 2019 Volume 2019:15 Pages 3287—3304
DOI https://doi.org/10.2147/NDT.S225920
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Emanuele Pick,1 Johann R Kleinbub,1 Stefania Mannarini,1,2 Arianna Palmieri1,3
1Department of Philosophy, Sociology, Education, and Applied Psychology, University of Padova, Padova, Italy; 2Interdepartmental Center for Family Research, University of Padova, Padova, Italy; 3Padova Neuroscience Center, University of Padova, Padova, Italy
Correspondence: Emanuele Pick
Department of Philosophy, Sociology, Education, and Applied Psychology, University of Padova, Via Venezia, 14, Padova 35131, Italy
Tel +39 049 8276696
Email [email protected]
Introduction: Empathy, in its affective and cognitive components, is a crucial interpersonal ability. It is broadly studied in the field of psychopathology, whereas its study in the neurodegenerative diseases is relatively recent. Existing literature, though, focused on a reduced subset of considered diseases, which often found a compromise in empathy abilities. Organized knowledge about a more comprehensive set of diseases is lacking.
Method: The present PRISMA systematic review was aimed at collecting the current available literature concerning empathic alterations in adult patients affected by neurodegenerative diseases. It considered the different empathy components, evaluated existing patterns, the impact on patients’ lives, and treatment considerations.
Results: Overall, the 32 retrieved studies describe a spread deterioration of empathic abilities in patients, with each disease displaying its own pattern of empathy functioning. Literature in this field is fragmented and of heterogeneous quality, and further studies are warranted to increase evidence of many preliminary results.
Discussion: In conclusion, we highlight the crucial importance of acknowledging empathy deficits in these diseases, showing their repercussion on both patients’ and caregivers’ quality of life, the establishment of a functional doctor–patient relationship, and the development of efficacious psychological intervention. These clinical approaches can be enriched by the knowledge of the spared abilities of patients affected by neurodegenerative diseases.
Keywords: neurodegenerative diseases, empathy, mentalizing, doctor-patient relationship, psychological intervention, quality of life
Plain Language Summary
Empathy is a complex construct that can be studied in its affective and cognitive perspectives. These two components seem to have distinct neural correlates. Although the focus of scientific literature on this phenomenon has drastically increased in the last years, few systematic essays have offered a general overview about this construct in neurological diseases involving the central as well as the peripheral nervous system. Our integrative effort considered published literature in scientific databases in the last 30 years, aiming to examine articles that evaluated empathy dimensions in neurological patients. In detail, we underlined the compromised and spared empathic functions for each disorder. Moreover, we inspected the neural substrates compromised in these patients. Since empathy is crucial in both medical and psychological therapeutic relations, the main objective of our systematic review is to provide neurologists and clinical psychologists with an accurate perspective of the peculiarly compromised and/or spared functions in these patients. Our purpose is to provide those taking care of these patients with information useful in building a better working alliance and, in general, a better understanding of the peculiar psychological profile of these patients.
Introduction
Rationale
Empathy is broadly studied in the field of psychopathology and brain lesions, whereas its study in the neurodegenerative disorders is relatively recent. Neurodegenerative disorders are characterized by progressive loss of selectively vulnerable populations of neurons, with the consequent alteration of physical and cognitive functions. Nonetheless, empathy deficits are often perceived more detrimental to quality of life than physical symptoms1 and affect caregivers’ quality of life as well.2 In the last years, these studies have been collected in literature reviews,3–8 systematic reviews,9–11 and meta-analyses.1,12–17 Existing literature, though, focused either on specific empathy components or a reduced subset of considered diseases.
Empathy
Empathy is a multifaceted psychological construct that reflects the cognitive and emotional reactions of one individual to the observed and inferred experiences of another.18,19
Starting in the 1980s20,21 and 1990s,22,23 researchers begun the scientific investigation of empathy, through the development of validated instruments and the assessments of clinical populations. Since then, empathy has been confirmed as a crucial component of personal and clinical relationships, but the construct defied the researchers’ effort of finding a common definition,22 consequently hindering its measurement. A recent review,23 indeed, reports the presence of a plethora of instruments aiming to measure empathy as a whole or in its different aspects, with each instrument referring to a different theoretical construct. While most developed measurement tools consist in questionnaires, recent studies are exploring further approaches in measuring empathy, for instance by assessing interpersonal physiological activity.24
Among the most solid models of empathy, Decety and Jackson18 propose a general distinction between two main components. The first, affective empathy, refers to automatic and implicit processes such as mimicry and emotional contagion. The second, mentalizing or cognitive empathy, regards the recognition and understating of others’ states and is itself composed of an affective and a cognitive component. This conceptualization is supported by broad neural evidence finding distinct areas throughout the Central Nervous System that underlie the different facets of empathy. Shamay-Tsoory25 proposed an elegant and comprehensive neuroanatomical model integrating the neuronal and functional components of empathy. According to this model, regions underlying the functions of affective empathy are the inferior frontal gyrus (IFG), inferior parietal lobule, anterior cingulate cortex (aCC), and anterior insula.25 Conversely, cognitive empathy relies on the medial prefrontal cortex (mPFC), the superior temporal sulcus, the temporoparietal junction, and the temporal poles.25 Further evidence toward Decety’s and Jackson’s distinction was recently reported by Sessa et al26 who found that separate EEG event-related potentials were associated alternatively to affective vs cognitive empathy stimuli.
Objective And Research Question
This work is set forth to systematically review the current available literature concerning empathic alterations in adult patients affected by neurodegenerative diseases, considering the different empathy components, and evaluate existing patterns, impact on patients’ lives, and treatment considerations. Overall, the aim of the study is to provide a valuable guide for physicians and clinicians treating these patients, as well as a basis for future studies.
Methods
Search Strategy
Our search strategy was developed in accordance with PRISMA guidelines.27 A systematic search of online databases using key phrases was conducted to identify cross-sectional studies published from January 1, 1988 to July 31, 2019. The choice of diseases to be included in the search terms was based on the manual by Angelini and Battistin.28 Neurodegenerative diseases were selected based on two reasons, the first one being their high frequency in population. The second one being their potential impact, despite their lower frequency, on caregivers or physicians care (i.e., Alzheimer disease, frontotemporal dementia, Lewy bodies disease, Parkinson disease, prion disease, Huntington disease, chorea minor, ataxias, amyotrophic lateral sclerosis, primary lateral sclerosis, hereditary spastic paraparesis, spinal and bulbar muscular atrophy, and myotonic dystrophy). To the best of our knowledge, existing reviews focus only on the most common neurodegenerative diseases while systematic knowledge on the less common neurodegenerative diseases is lacking. Since, as we expected, fewer articles would be retrieved for less common diseases, we decided to consider a wide time-span in order to maximize the number of search results. Thirteen independent literature searches were performed in Scopus, PubMed, and PsycINFO online databases, each using the word “empathy” in logical conjunction (“AND”) with each disease name. The complete list of disease keywords was: Alzheimer, Frontotemporal, Lewy, Parkinson, Prion, Huntington, Chorea Minor, Ataxia, Amyotrophic Lateral Sclerosis, Primary Lateral Sclerosis, Hereditary Spastic Paraparesis, Spinal and Bulbar Muscular Atrophy, and Myotonic dystrophy. Search areas for Scopus included the “title/abstract/keywords” for the neurological diseases set and the word Empathy. Last search was performed on August 1, 2019. Furthermore, relevant studies not resulting from the bibliographic search were included when found in the reference list of each retrieved article, as well as in the “cited by” section each article, in each database.
Screening And Eligibility
Abstracts were reviewed for eligibility and only original research articles, written in English and published in international peer-reviewed journals, were considered. All eligible articles underwent a second in-depth inspection to check for the following inclusion criteria: assessing adult patients, empathy assessed through quantitative measures, performing a comparison with a healthy control group and being a cross-sectional study. Criteria are listed in Table 1.
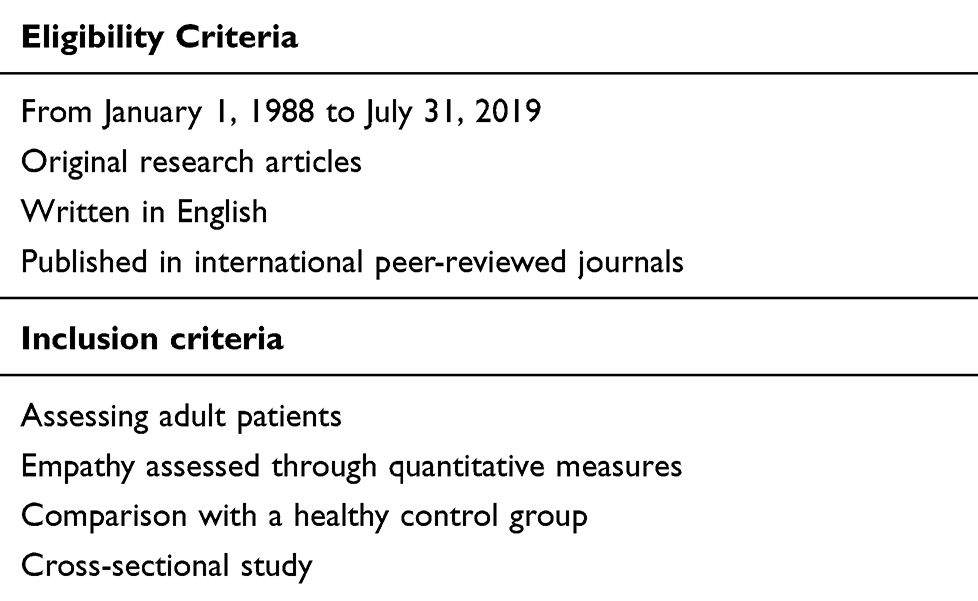 |
Table 1 Summary Of Eligibility And Inclusion Criteria |
In the case of multiple studies analyzing the same dataset with the same methodology, since including both articles might result in an overestimation of the results (i.e., duplication bias29), only the oldest publication was retained in the qualitative synthesis.
The whole search procedure, and the number of articles for each stage, is summarized in a PRISMA flow diagram (Figure 1). For all selection choices, a criterion of inclusiveness was preferred to a quality one, in order to report an exhaustive state of the art of the literature.
 |
Figure 1 Flow diagram for qualitative systematic review of empathy functioning in neurodegenerative diseases. |
Data Extraction
The following relevant information was extracted by one author (E.P.) from the retrieved articles: (a) type and number of participants; (b) type of empathy; (c) methods used; and (d) main results.
Given the paucity of retrieved studies for some diseases, no risk of bias assessment in individual studies was performed.
Results
The number of retrieved articles for each disease is shown in Table 2. The total number of analyzed articles was 32. Table 3 reports the complete article list and the results summary. It should be noted that since five articles investigated more than one disease, they were retrieved from their respective literature searches but have been qualitatively analyzed only once.
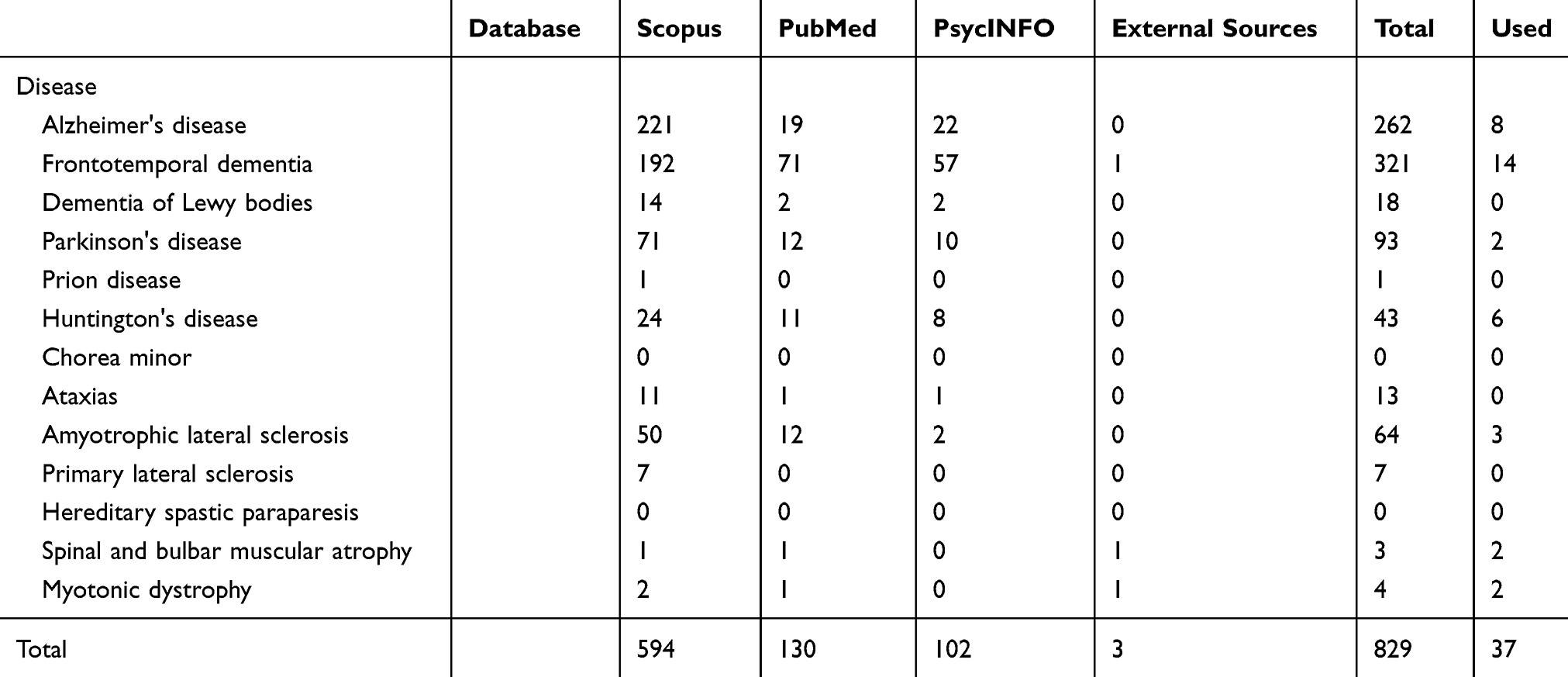 |
Table 2 Summary Of The Number Of Articles Retrieved For Each Source Of Information, For Each Disease |
 |
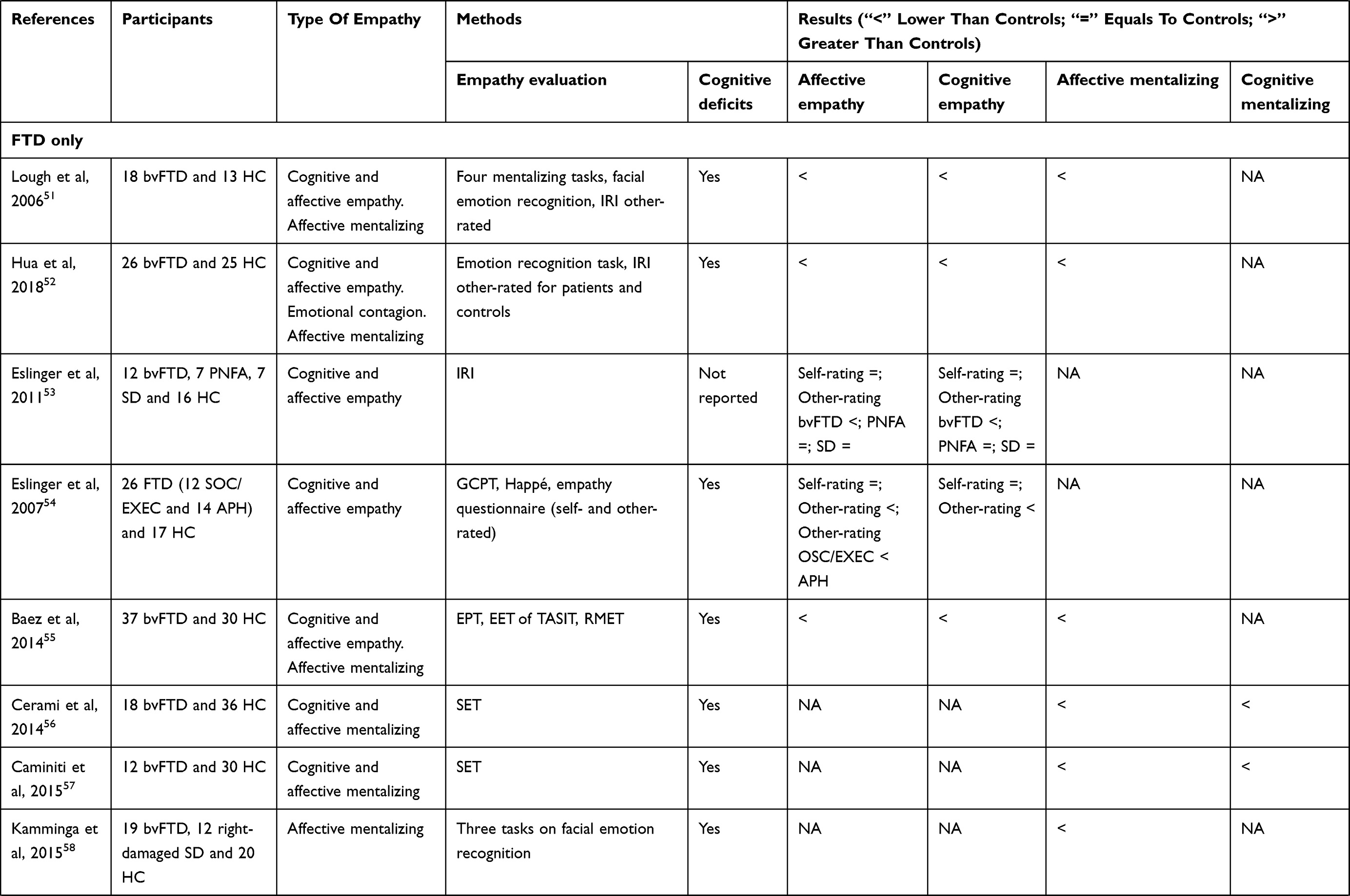 | 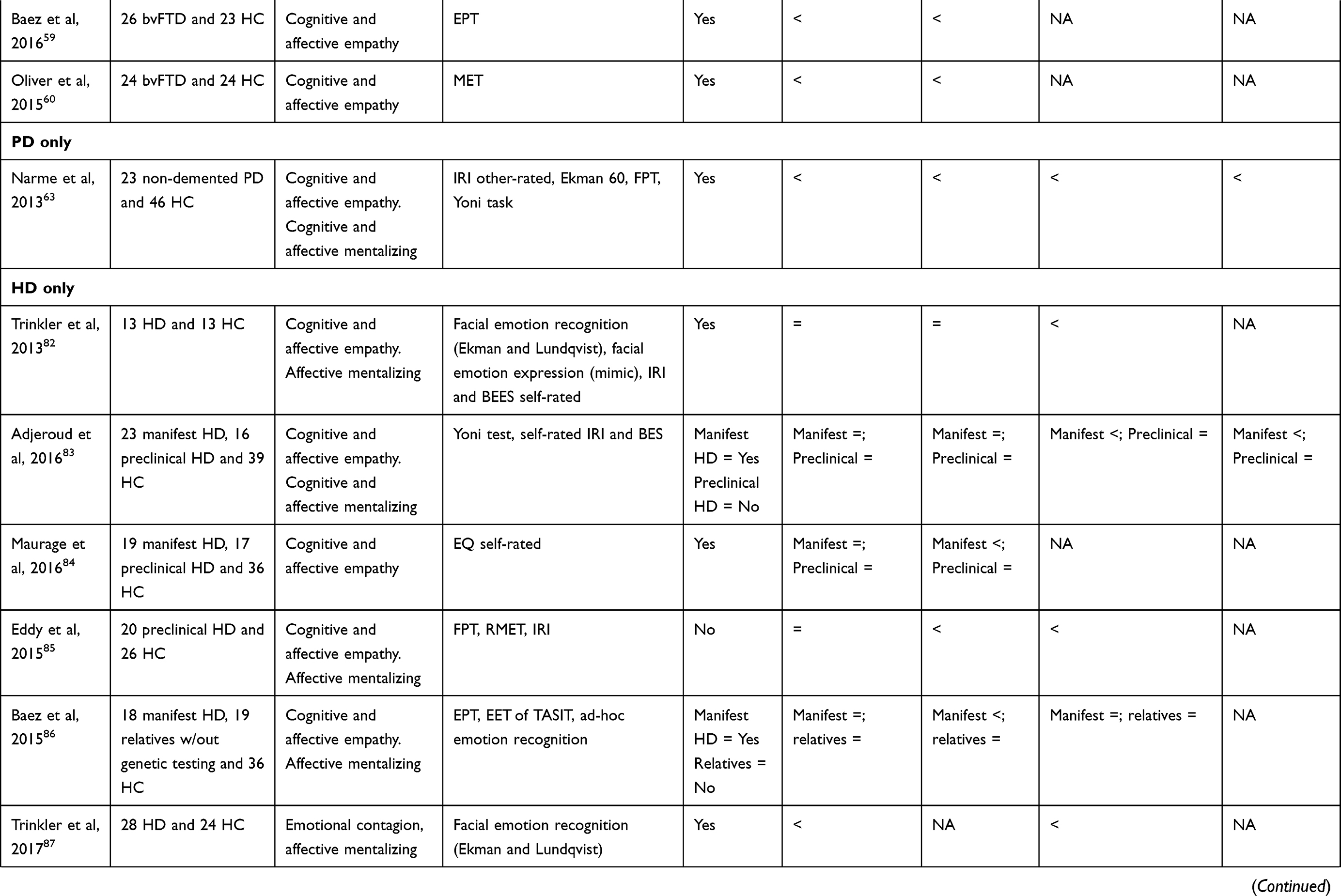 | 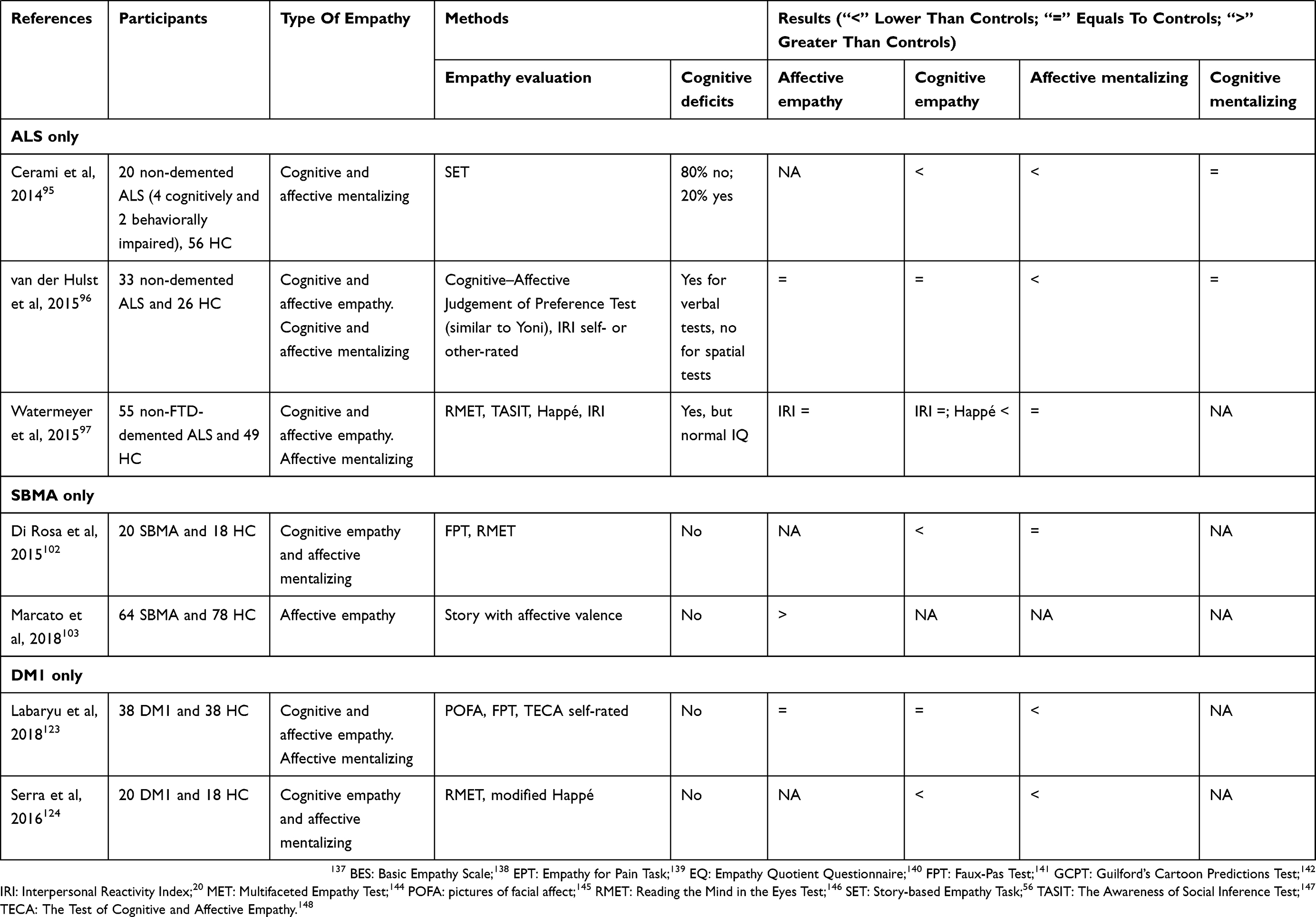 |
Table 3 Review Results Sorted By Disease |
Primary Dementias
Alzheimer's Disease
Alzheimer's disease (AD) is the most common form of dementia with an approximate range of incidence of 500 to 7000–8000 per 100,000 person-years in people aged 65 or more.30 AD is caused by an accumulation of amyloid plaques in neurons with a consequent widespread loss of gray matter (GM) and characterized by progressive cognitive decline with remarkably impaired episodic memory due to degeneration of medial temporal lobes.31 Brain imaging in patients with AD shows predominant left-sided GM atrophy32 and decreased metabolic activity especially in posterior cingulate cortex.33
In patients with AD, various studies reported the affective component of empathy as preserved while the cognitive one was impaired, in questionnaires rated by caregivers.34–37 This dissociation has been detected also when patients self-rate their own empathy.38 In contrast, some authors find no decrement in empathy as reported by caregivers.39 Caregiver-rated questionnaires are the standard assessment approach in the presence of patients’ frank cognitive impairment.40,41 Visual recognition of emotional facial expressions, a process necessary in affective mentalizing, is generally preserved in AD patients, with the exception of fearful and ambiguous expressions;34,35 in another face recognition task, using fMRI, left-lateralized decrease in neuronal activity was observed in patients with AD compared to healthy controls.42 This peculiar pattern in mentalizing tasks is compatible with structural lesions present in patients with AD32 that overlap areas considered as neural substrate of cognitive empathy.19,43
In summary, both caregivers and patients with AD perceive affective empathy as spared, while deficits are reported for cognitive empathy. Surprisingly, the ability to recognize emotional facial expressions is not completely damaged. Neuroimaging data seem to support these conclusions. Eventually, caregivers’ psychological distress might arise when they fail to acknowledge the subtle empathic deficits of their relatives with AD.44
Frontotemporal Dementia
Frontotemporal dementia (FTD) is a group of heterogeneous dementias characterized by a loss in behavioral control (behavioral variant FTD, bvFTD) and/or loss in language abilities (semantic dementia, SD; progressive non-fluent aphasia, PNFA), associated with general degeneration in frontal and anterior temporal lobes.45 FTD is less common than AD, with an incidence ranging 1.3–16.7 cases for 100,000 person-years as the age of onset increases, and the behavioral variant is the predominant presentation.46 Specifically, in patients with bvFTD degeneration of paralimbic brain areas including mPFC, aCC and frontoinsular cortices are prominent.47,48 Functional imaging presents frontal hypoperfusion.49
In patients with bvFTD, typical core symptoms are behavioral egocentrism and interpersonal difficulties which are reflected by their disrupted empathy and emotions.50 Most studies report that both cognitive and affective components of empathy were rated lower in patients than in controls.37,51–53 In contrast, a research on 18 patients with bvFTD found impairment only in cognitive empathy.39
Affective empathy assessed in patients with bvFTD through the electromyographical (EMG) reactivity for facial muscles implicated in negative emotional reactions (i.e., frowning) was not different from controls. Instead, patients displayed an augmented EMG reactivity in facial muscles implicated in positive emotions (i.e., smiling) irrespective of the presented facial emotional expression.52 Patients with bvFTD scored low on visual and verbal tasks of vignettes depicting social situations, measuring the cognitive and the affective components of mentalizing.51,54,55 More prominent deficits appeared in affective mentalizing.56,57 Verbal abilities covariated with verbally presented mentalizing tasks indicating that deficits in mentalizing might be partly dependent on the verbal difficulties in some patients with bvFTD.51 Moreover, patients with bvFTD could not identify and discriminate violations of social norms.51,55 In tasks presenting faces with emotional expression, a measure of affective mentalizing, patients with bvFTD have been found consistently impaired in selecting the appropriate emotional category for the presented face.52,55,58 They struggled in deciphering ambiguous emotions on a videotape but correctly inferred well-defined positive or negative emotions.34 In the context of empathy for pain, Baez et al55,59 presented images of people inflicting pain to others which were rated by patients as having lower levels of intentionality compared to the ratings given by healthy controls. Patients with bvFTD were also less aroused, on a self-rating scale, by images of realistic situations with negative valence, while neutral and positive valence images were as arousing as controls.60
In the second manifestation of FTD, SD, patients are characterized by anterior temporal atrophy mostly localized in the left hemisphere61 with consequent reduced metabolism.62
The overall view on empathy in SD shows inconsistencies. Rankin et al39 found that both cognitive and affective empathy were perceived as impaired by caregivers, while Eslinger et al reported no deficits.53 A group of patients with SD, who had right hemispheric lesions, presented poorer performance in a facial matching task for emotional expression compared to healthy controls.58
Other studies not reporting the FTD subtypes found an overall decrement in caregiver-perceived empathy of patients, with greater impairment of affective mentalizing.54,63
Lastly, patients with PNFA present disruption of large-scale neural networks centered in left inferior frontal and anterior superior temporal regions64,65 and left frontal hypometabolism.66 The retrieved evidence does not support empathy deficits for patients with PNFA.53
In summary, core deficit in patients with bvFTD is both affective and cognitive empathy. In particular, patients cannot discriminate between harmful versus non-harmful intentions and lack the capacity to respond with the appropriate facial expression to the emotions of other people, probably because they are unable to correctly identify the perceived emotion. Moreover, for patients with bvFTD, it is difficult to anticipate people’s behavior in social context, especially if the context itself is ambiguous. Whilst patients are quite unaware of their deficits, these are well recognized by caregivers. Deficits similar to bvFTD seem present in patients with SD, although our knowledge is less thorough due to the limited amount of research performed so far. Finally, the only study retrieved on patients with PNFA does not indicate empathy deficits.
Parkinson's Disease
Parkinson's disease (PD) is the second most common neurodegenerative disease after AD, with an incidence of 160 per 100,000 person-years people aged 65 years or older.67 PD is caused by a loss of dopaminergic neurons in the pars compacta of the substantia nigra,68 with hallmark motor manifestations being bradykinesia, rigidity, and rest tremor.69 Non-motor symptoms are present as well, with cognitive deficits in executive functioning, memory, and neuropsychiatric symptoms that can lead to overt dementia in 70% of the cases.70–72 Neuroimaging indicates a widespread GM atrophy in non-demented patients with PD, especially in right prefrontal cortex and bilateral temporal lobes.72 In functional brain imaging, significant perfusion decrements were limited to the frontal lobe area in the same population.73 When demented patients with PD are considered, GM atrophy spreads also to subcortical structures72 and hypoperfusion to temporal and parietal areas.73 The distinction between demented and non-demented patients is important because the two eligible studies resulting from the bibliographic search considered only patients suffering from PD without overt dementia.
Although empathy deficits are not a hallmark of patients with PD, according to Narme et al,63 both cognitive and affective empathy are perceived as low in non-demented patients with PD by their caregivers. The assessment of cognitive empathy elicited from verbal stimuli resulted in a diminished accuracy in explaining faux pas, with overall mentalizing impairments. The poor level of stimuli comprehension caused by patients’ cognitive alterations exaggerated the degree of the assessed empathic impairment.63 Similarly, the recognition for the visual presentation of emotional facial stimuli was diminished in patients with PD relatively to controls.44,63 In this case, the performance might have been affected by patients’ difficulty in processing facial stimuli.63 Interestingly, caregivers who were less aware of patient’s empathy difficulties displayed increased level of depression and burden.44 Empathy deficits cannot be generalized as most studies were conducted on non-demented patients, who account for only about 30% of the PD population.
To sum up, patients with PD present deficits of both affective and cognitive empathy with brain atrophy and hypoperfusion that seem severe enough to make patients fail in empathic tasks of faux pas interpretation and facial emotion recognition, although not so detrimental as to give overt dementia. Areas important for affective and cognitive empathy25,43 are those impaired in PD.72,73 Although these deficits are not a hallmark of non-demented patients with PD, they are severe enough to be perceived by caregivers.
Huntington's Disease
Huntington's disease (HD) is caused by an expansion of the CAG trinucleotide repeat in the huntingtin gene, exiting in choreiform movements, rigidity, cognitive impairments, and behavioral disturbances.74 Epidemiology indicates an incidence spanning 0.05–0.8 cases per 100,000 person-years across all ages.75 The hallmark structural changes in the brain of patients with HD occur in basal ganglia since the caudate nucleus decreases in volume.76,77 More recent findings show that the neurodegenerative process of HD seems to impact also cortical structures brain-wise78,79 and in particular reduces GM volume in pCC and sensorimotor cortex.80 Glucose metabolism is reduced not only in striatum but is detected also in frontal and temporal cortices.81
Contrary to primary dementias, patients with HD usually present a degree of cognitive impairment ranging from null to mild. Empathy assessment can thus be performed through self-report questionnaires. These measures typically report no difference between patients and control groups,82–84 with the exception of one study85 that shows a decrement in both affective and cognitive empathy in 20 preclinical patients with HD. In another study, the affective component resulted spared when the patients were asked how bad they felt for a person in physical pain.86 The mild cognitive impairment affecting patients with HD might cause difficulties in discriminating social emotional stimuli removed from the context. Indeed, in emotional face discrimination tasks, patients with manifest or preclinical HD made more errors than controls indicating lower affective mentalizing.82,85–87 Interestingly, though, this deficit vanished when the face was presented in a richer environment with contextual cues (i.e., a videotape).61 The core deficit of HD patients appears to be in the domain of cognitive empathy, and especially cognitive mentalizing. In fact, performance dropped in tasks where the objective was to grasp the presence of embarrassing events or the intentionality of a painful action.85,86 These results indicate a lack of understanding for accidental embarrassing or painful scenarios. Mentalizing deficits hold also with simpler stimuli for patients with manifest HD, while for patients with preclinical HD impairments are present in second-order mentalizing processes only.83 Finally, Trinkler et al87 measured facial EMG activity during passive view of emotional faces. Healthy controls automatically modulated EMG activity in the different facial muscles depending on the facial expression presented, while patients did not.
In conclusion, the structural and functional neural abnormalities of patients with HD76–81 not only are reflected in motor and cognitive symptoms but extend to the interpersonal and empathic domains. Specifically, impairments in cognitive empathy and in the most automatic part of affective empathy might be a reflection of the neural areas which are commonly involved in those functions.19,43,88
In brief, in patients with HD, the affective component of empathy seems relatively spared. The core deficit seems to be in cognitive mentalizing. The deficits might be mitigated if patients are supported with sufficient contextual cues and a richer social environment.
Neuromuscular Diseases
Amyotrophic Lateral Sclerosis
Amyotrophic lateral sclerosis (ALS) has an incidence of 2.16 cases per 100,000 person-years.89 Etiology is largely unknown90 and degeneration of upper and lower motor neurons in ALS pathology results in symptoms such as weakness, muscle atrophy, slurred speech, and dysphagia.90 Extra-motor manifestation of cognitive impairment lays on a continuum, from 35–40% showing no deficits whatsoever to 50% of the patients with ALS showing mild cognitive impairment, and a 10–15% reaching criteria for diagnosis of FTD.91 Cognitive deficits are associated with mild-to-severe psychological symptoms, as well as suicidal ideation.92 Structural neuroanatomical investigations detected GM reduction in motor areas, in left IFG and in left superior temporal gyrus.93 Heterogeneity of cognitive impairments is reflected by decreased metabolism in the frontal areas extending bilaterally to the parietal regions for patients with cognitive impairments, while for patients without cognitive impairments, metabolism was lower in the left superior frontal gyrus.94 Research on empathy commonly studies patients with ALS without comorbid dementia, although about 30–35% of the sampled patients suffer from cognitive or behavioral impairments. Affective empathy and cognitive mentalizing seem relatively preserved in patients with ALS95–97 with only a subsample of van der Hulst et al96 showing deficits, and to which patients are unaware of. Lack of awareness that becomes evident in the comparison between self-report questionnaires and caregivers’ reports.96 Another common finding is a marked deficit in affective mentalizing assessed through inference of mental characteristics of fictitious characters.95–97 But in this case, patients seem aware of the deficit according to van der Hulst et al.96 In a different task, showing faces and interaction of real people, Watermeyer et al97 found no deficits in patients with ALS, indicating spared affective and cognitive mentalizing.
In summary, the drive to share other people’s feelings and to resonate with them (i.e., affective empathy) seems spared in patients with ALS. Patients show predominantly affective and cognitive mentalizing deficits that might be a consequence of the neural structures typically involved in this disease93,94 and that are classically linked to empathy functioning in healthy individuals.43 Although impairment in cognitive empathy seems pervasive, according to the reviewed studies, it mostly derives from a subset of patients. Specifically, van der Hulst et al96 observed that 61% of the participating patients were free from cognitive empathy deficits whatsoever. Similarly, the other two studies retrieved indicate that only 5–18% of the patients with ALS have severe deficits compared to controls.95,97 Deficits in cognitive mentalizing disappear when stimuli are more ecological. Interestingly patients were aware of their affective mentalizing deficits.
Spinal And Bulbar Muscular Atrophy
Spinal and bulbar muscular atrophy (SBMA), also known as Kennedy’s disease, is a rare genetic disease with an incidence of 0.19 cases per 100,000 person-years in the male population.98 It has classically been considered as a lower motor neuron disease, but now it is better described as a multisystem disease.99 Common clinical manifestations are heterogeneous and manifest through muscle weakness and endocrine dysfunctions100 due to androgen receptor insensitivity caused by genetic mutation.101 Patients with SBMA display null102,103 to mild104–106 cognitive deficits. Neuroimaging studies indicate cerebral involvement in patients with SBMA who show a subtle reduction of GM and white matter in brainstem, primary motor cortex, and frontal areas.107,108 Accordingly, reduced metabolic activity is present in frontal areas.109
Recent scientific developments showed interest in the empathic abilities of patients with SBMA. Performance for affective mentalizing, in a facial emotion recognition task, resulted spared.102 In a further task, employing a verbal assessment of cognitive mentalizing, patients’ performance dropped compared to controls.102 A surprising result was recently found by Marcato et al.103 The authors reported a better performance than healthy controls in a prose memory task with emotional/affective valence, in a large sample of patients suffering from SBMA and without signs of cognitive impairment. The result that cognitive mentalizing is impaired in a context of relative preservation of cognitive functions has been hypothesized to derive from the specific pattern of subtle frontal lobe impairment. While classical neuropsychological tests are not able to detect the slight changes in frontal cognitive functions, cognitive mentalizing deficits could be detected with more fine-grained tests110 thanks to the association between cognitive empathy and executive functions.111 It was hypothesized that the better performance in the affective prose memory test derived from a possible protective role of androgen receptors deficit for the emotional aspects. Research shows that a single testosterone administration in females impairs their capacity to infer emotion and mental states of others.112 Indeed, testosterone has a role in mediating sexual dimorphism and several behaviors and attitudes,113,114 and in males, it is one of the most common androgens. Baron-Cohen115 formalized this concept in his Empathizing-Systemizing theory, based on the observation that women show on average a stronger drive to empathize than men.
In conclusion, the deficit of androgen receptors might lead patients with SBMA to a surprisingly enhanced, or at least spared, ability to connect with others via more affective routes. Conversely, the subtle metabolic and structural alterations in frontal cortical areas might be a possible cause for the inability of patients with SMBA to infer the intentions of others. This ability, indeed, highly depends on the correct functioning of frontal brain areas.25,43
Myotonic Dystrophy Type 1
Myotonic dystrophy type 1 (DM1) is the most common adult-onset muscular dystrophy with an incidence ranging 28.9–44.6 per 100,000 person-years.116 DM1 is caused by an autosomal-dominant GTC-repeat expansion117 and is a multisystem disease with symptoms ranging from muscle weakness, cardiovascular dysfunctions, and endocrine abnormalities, up to cognitive deficits.118 Patients with DM1 do not display a unique cognitive phenotype, rather it lays on a continuum ranging from no deficits to specific clusters of dysfunctions,119 probably because of the high variability in the neural structures involved. For example, Romeo et al120 found two patterns of brain involvement: a diffuse white matter decrease in temporal and insular areas, and a focal to diffuse white matter decrease in fronto-parietal areas. About half of the participants had no white matter atrophy at the time of investigation. Similarly, some authors point to deficits in functions subserved by fronto-temporal areas such as language and executive functions,121 while others reported deficits in cognitive flexibility and visuoconstructive ability subserved by fronto-parietal areas.122
A group of patients with DM1 with normal IQ level was tested in their affective empathy as well as their affective and cognitive parts of mentalizing.123 Authors found that self-reported empathy was comparable to that of healthy controls (both cognitive and affective), as was the performance on a verbal cognitive mentalizing task. A contrasting result emerged from the work by Serra et al.124 The authors investigated cognitive empathy in a group of 20 patients suffering from DM1, with normal IQ and no cognitive impairment. Patients underperformed controls in a verbal cognitive mentalizing task, also performing poorly in a facial emotion recognition task. Their brains showed abnormal disconnections within temporal and temporo-occipital regions,124 areas classically deputed to mentalizing.43
To conclude, patients with DM1 presented self-reported empathy comparable to that of controls. Some deficits emerged in cognitive empathy, but there is no consensus about which subcomponent of mentalizing is more impaired. Further studies are needed for a cohesive picture about the empathy specificities of DM1 patients and to generalize their relations to the neural structures involved.
Discussion
Summary Of Main Findings
This study represents the most comprehensive systematic review on empathy alterations in neurodegenerative disorders. While other literature review efforts were recently published, this systematic review provides a more inclusive list of considered diseases and makes explicit distinction between different empathy components.18
Overall, the retrieved studies describe a spread deterioration of empathic abilities in neurological patients. In general, each disease displays its own pattern of empathy functioning. Affective empathy seems the most variable component. Patients with either AD, HD, ALS, or DM1 show a preservation of this domain; on the contrary, it is clearly impaired in those who suffer from FTD or PD, while in patients with SBMA, it seems surprisingly enhanced. Regarding cognitive empathy, there is a general impairment in all diseases, with patients suffering from HD, ALS, or DM1 showing only minor deficits. While not all studies make explicit distinctions between empathy subcomponents, available evidence shows that affective mentalizing is preserved in patients with SBMA, slightly impaired in those with AD, HD, or ALS, and clearly impaired in those who suffer from FTD, PD, or DM1. Cognitive mentalizing is unimpaired in patients with ALS, minor deficits are found in those with AD or SBMA, while the function is markedly impaired in those who suffer from FTD, PD, or HD. In accordance with the literature taken into consideration, compromised and preserved components of empathy turned out to be substantially consistent with the neurological impairment peculiar for each disorder.
As highlighted by the literature on the measurement of empathy,23 it is interesting to note that this systematic review confirms the great variability in instruments used, as can be seen in Table 3. Its limiting consequences will be debated in the Limitations section. Although our search included papers published in the last 30 years, the oldest article retrieved was published in 2005. The relative recency of this literature is comparable to broader trends in patient care. Today’s consensus125 is that a positive doctor–patient relationship is a cornerstone of efficacious medical intervention. A good relationship is associated with patient compliance with treatments, perception of care and, ultimately, clinical outcome.126 Research in this field, though, has mostly focused on the doctor’s empathy, showing that physicians presenting higher levels of empathy are able to promote a more efficacious doctor–patient relationship.127 An efficacious relationship, though, requires the active involvement of both the doctor and the patient128 and is strongly influenced by the patients’ characteristics as well:129 a particularly crucial matter in the case of neurodegenerative diseases where these functions are often compromised.
Although, to the best of our knowledge, there is currently no publication investigating the influence of the patient’s empathy in the doctor–patient relationship, our results lead to the reasonable hypothesis that the broad spectrum of empathy alterations in neurodegenerative disorders may be an obstacle to efficacious clinical relationships. The knowledge of the peculiar alteration of each disease could prove of great importance to clinicians, who may tailor their communication strategies in a person-centered manner, according to the capacity of each patient to develop trust towards the medical team, and consequently increase the chances of patients’ compliance with medical procedures.126
The European Academy of Neurology guidelines encourage a multidisciplinary team composed also of psychologists to take care of patients and caregivers, with the aim of improving their quality of life, psychological health and coping with other distressful feelings (e.g., loneliness).130–132 Also regarding psychological interventions, clinicians’ communication can be enriched by the knowledge of which abilities and resources are spared in a given patient. For instance, patients with preserved affective empathy may benefit from experiential treatments or strategies appealing to patient’s feelings and emotions,133 eventually informed by emerging interpersonal physiology techniques.134 On the contrary, techniques promoting mentalizing abilities135 might be more effective in patients with spared cognitive empathy. For example, in the case of AD where psychological intervention represents the first-line approach for most individuals’ neuropsychiatric symptoms,136 knowing that these patients are characterized by the preservation of affective empathy and a clear deficit in cognitive empathy may help in the development and delivery of efficacious treatments. In a recent study,2 an explicitly tailored mind–body intervention proved particularly efficacious in improving anxiety and quality of life in patients with ALS, probably thanks to their spared competence in the affective domains of empathy.
Limitations
Primarily, limitations of this review pertain to the limited number of studies performed in this area. As can be seen in Table 2, eligible studies ranged from 2 to 14 for each disease. Given that this interest in neurological patient empathy seems to be a new trend, it is somewhat expected that there are few studies in the literature, yet evidence for most selected disorders cannot be considered conclusive. There are also limitations with the individual studies reviewed. First, most studies were based on small samples. While this is a common limitation of studies on rare diseases, in most cases, the group-comparison analyses were probably underpowered. Second, empathy was evaluated through a broad range of measures and approaches and then by referring, in turn, to multiple empathy models. This variability in measurements adds to the individual variability in empathic abilities of the patients considered. Thus, it limits the possibility of direct comparisons between the studies, and our cohesive picture of patients’ deficits and residual components.
Conclusions
In conclusion, the research on empathy alterations in neurodegenerative diseases is recent, heterogeneous, and describes a broad variability of deficits across different pathologies. Overall, the results highlight the importance of this field of study in helping patients and caregivers to cope with diseases and for the development of ad-hoc psychological strategies. Further studies should focus on potential positive alterations as in the case of SBMA.
Abbreviations
aCC, anterior cingulate cortex; AD, Alzheimer's disease; ALS, amyotrophic lateral sclerosis; BEES, Balanced Emotional Empathy Scale; BES, Basic Empathy Scale; bvFTD, behavioral variant FTD; DM1, myotonic dystrophy type 1; EMG, electromyography; EPT, Empathy for Pain Task; EQ, Empathy Quotient questionnaire; fMRI, functional magnetic resonance imaging; IFG, inferior frontal gyrus; FPT, Faux-Pas Test; FTD, frontotemporal dementia; GCPT, Guilford’s Cartoon Predictions Test; GM, grea matter; HD, Huntington's disease; IRI, Interpersonal Reactivity Index; MET, Multifaceted Empathy Test; mPFC, medial prefrontal cortex; PD, Parkinson's disease; PNFA, progressive non-fluent aphasia; POFA, pictures of facial affect; RMET, Reading the Mind in the Eyes Test; SBMA, spinal and bulbar muscular atrophy; SD, semantic dementia; SET, Story-based Empathy Task; TASIT, The Awareness of Social Inference Test; TECA, The Test of Cognitive and Affective Empathy.
Data Availability
All data relevant to the study are included in the article.
Author Contributions
AP and SM conceptualized the idea. AP and EP designed the article. EP acquired and analyzed the data. EP and JRK wrote the main manuscript. AP, EP, and JRK interpreted the results. AP, JRK, and SM critically revised the manuscript for important intellectual content. All authors approved the final version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of the work are appropriately investigated and resolved.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gray HM, Tickle-Degnen L. A meta-analysis of performance on emotion recognition tasks in parkinson’s disease. Neuropsychology. 2010;24(2):176–191. doi:10.1037/a0018104
2. Kleinbub JR, Palmieri A, Broggio A, et al. Hypnosis-based psychodynamic treatment in ALS: a longitudinal study on patients and their caregivers. Front Psychol. 2015;6:822. doi:10.3389/fpsyg.2015.00822
3. Bartochowski Z, Gatla S, Khoury R, Al-Dahhak R, Grossberg GT. Empathy changes in neurocognitive disorders: a review. Ann Clin Psychiatry. 2018;30(3):220–232.
4. Kennedy DP, Adolphs R. The social brain in psychiatric and neurological disorders. Trends Cogn Sci. 2012;16(11):559–572. doi:10.1016/J.TICS.2012.09.006
5. Kemp J, Després O, Sellal F, Dufour A. Theory of Mind in normal ageing and neurodegenerative pathologies. Ageing Res Rev. 2012;11(2):199–219. doi:10.1016/J.ARR.2011.12.001
6. Strikwerda-Brown C, Ramanan S, Irish M. Neurocognitive mechanisms of theory of mind impairment in neurodegeneration: a transdiagnostic approach. Neuropsychiatr Dis Treat. 2019;15:557–573. doi:10.2147/NDT.S158996
7. Fischer A, Landeira-Fernandez J, Sollero de Campos F, Mograbi DC. Empathy in Alzheimer’s Disease: review of findings and proposed model. J Alzheimer’s Dis. 2019;69(4):921–933. doi:10.3233/JAD-180730
8. Fittipaldi S, Ibanez A, Baez S, Manes F, Sedeno L, Garcia AM. More than words: social cognition across variants of primary progressive aphasia. Neurosci Biobehav Rev. 2019;100:263–284. doi:10.1016/j.neubiorev.2019.02.020
9. Elamin M, Pender N, Hardiman O, Abrahams S. Social cognition in neurodegenerative disorders: a systematic review. J Neurol Neurosurg Psychiatry. 2012;83(11):1071–1079. doi:10.1136/jnnp-2012-302817
10. Poletti M, Enrici I, Bonuccelli U, Adenzato M. Theory of mind in Parkinson’s disease. Behav Brain Res. 2011;219(2):342–350. doi:10.1016/J.BBR.2011.01.010
11. Kipps CM, Hodges JR. Theory of mind in frontotemporal dementia. Soc Neurosci. 2006;1(3–4):235–244. doi:10.1080/17470910600989847
12. Carr AR, Mendez MF. Affective empathy in behavioral variant frontotemporal dementia: a meta-analysis. Front Neurol. 2018;9:417. doi:10.3389/fneur.2018.00417
13. Bora E, Velakoulis D, Walterfang M. Social cognition in Huntington’s disease: a meta-analysis. Behav Brain Res. 2016;297:131–140. doi:10.1016/J.BBR.2015.10.001
14. Bora E, Walterfang M, Velakoulis D. Theory of mind in Parkinson’s disease: a meta-analysis. Behav Brain Res. 2015;292:515–520. doi:10.1016/j.bbr.2015.07.012
15. Bora E, Walterfang M, Velakoulis D. Theory of mind in behavioural-variant frontotemporal dementia and Alzheimer’s disease: a meta-analysis. J Neurol Neurosurg Psychiatry. 2015;86:714–719. doi:10.1136/jnnp-2014-309445
16. Bora E. Meta-analysis of social cognition in amyotrophic lateral sclerosis. Cortex. 2017;88:1–7. doi:10.1016/j.cortex.2016.11.012
17. Bora E, Velakoulis D, Walterfang M. Meta-analysis of facial emotion recognition in behavioral variant frontotemporal dementia: comparison With Alzheimer disease and healthy controls. J Geriatr Psychiatry Neurol. 2016;29(4):205–211. doi:10.1177/0891988716640375
18. Decety J, Jackson PL. The functional architecture of human empathy. Behav Cogn Neurosci Rev. 2004;3(2):71–100. doi:10.1177/1534582304267187
19. Zaki J, Ochsner KN. The neuroscience of empathy: progress, pitfalls and promise. Nat Neurosci. 2012;15(5):675–680. doi:10.1038/nn.3085
20. Davis MH. A multidimensional approach to individual differences in empathy. JSAS Cat Sel Doc Psychol. 1980;10(85):1–17.
21. Baron-Cohen S, Leslie AM, Frith U. Does the autistic child have a “theory of mind”? Cognition. 1985;21(1):37–46. doi:10.1016/0010-0277(85)90022-8
22. Cuff BMP, Brown SJ, Taylor L, Howat DJ. Empathy: a review of the concept. Emot Rev. 2016;8(2):144–153. doi:10.1177/1754073914558466
23. Neumann DL, Chan RCK, Boyle GJ, Wang Y, Rae Westbury H. Measures of empathy: self-report, behavioral, and neuroscientific approaches. In: Boyle GJ, Saklofske DH, Matthews G, editors. Measures of Personality and Social Psychological Constructs. Cambridge, MA: Academic Press; 2015:257–289. doi:10.1016/B978-0-12-386915-9.00010-3
24. Kleinbub JR, Palmieri A, Orsucci FF, et al. Measuring empathy: a statistical physics grounded approach. Phys A Stat Mech Its Appl. 2019;526. doi:10.1016/j.physa.2019.04.215
25. Shamay-Tsoory SG. The neural bases for empathy. Neurosci. 2011;17(1):18–24. doi:10.1177/1073858410379268
26. Sessa P, Meconi F, Han S. Double dissociation of neural responses supporting perceptual and cognitive components of social cognition: evidence from processing of others’ pain. Sci Rep. 2014;4:7424. doi:10.1038/srep07424
27. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi:10.1136/bmj.b2535.
28. Angelini C, Battistin L, eds. Neurologia Clinica. Bologna, IT: Società Editrice Esculapio; 2014.
29. Tramèr MR, Reynolds DJ, Moore RA, McQuay HJ. Impact of covert duplicate publication on meta-analysis: a case study. BMJ. 1997;315(7109):635–640. doi:10.1136/bmj.315.7109.635
30. Mayeux R. Alzheimer’s disease: epidemiology. In: Duyckaerts C, Litvan I editors, Handbook of Clinical Neurology. Vol. 89. Elsevier; 2008:195–205. doi:10.1016/S0072-9752(07)01218-3
31. Reitz C, Mayeux R. Alzheimer disease: epidemiology, diagnostic criteria, risk factors and biomarkers. Biochem Pharmacol. 2014;88(4):640–651. doi:10.1016/j.bcp.2013.12.024
32. Whitwell JL, Shiung MM, Przybelski SA, et al. MRI patterns of atrophy associated with progression to AD in amnestic mild cognitive impairment. Neurology. 2008;70(7):512–520. doi:10.1212/01.WNL.0000280575.77437.A2
33. Nestor PJ, Fryer TD, Ikeda M, Hodges JR. Retrosplenial cortex (BA 29/30) hypometabolism in mild cognitive impairment (prodromal Alzheimer’s disease). Eur J Neurosci. 2003;18(9):2663–2667. doi:10.1046/j.1460-9568.2003.02999.x
34. Fernandez-Duque D, Hodges SD, Baird JA, Black SE. Empathy in frontotemporal dementia and Alzheimer’s disease. J Clin Exp Neuropsychol. 2010;32(3):289–298. doi:10.1080/13803390903002191
35. Narme P, Mouras H, Roussel M, Devendeville A, Godefroy O. Assessment of socioemotional processes facilitates the distinction between frontotemporal lobar degeneration and Alzheimer’s disease. J Clin Exp Neuropsychol. 2013;35(7):728–744. doi:10.1080/13803395.2013.823911
36. Sturm VE, Yokoyama JS, Seeley WW, Kramer JH, Miller BL, Rankin KP. Heightened emotional contagion in mild cognitive impairment and Alzheimer’s disease is associated with temporal lobe degeneration. Proc Natl Acad Sci. 2013;110(24):9944–9949. doi:10.1073/pnas.1301119110
37. Dermody N, Wong S, Ahmed R, Piguet O, Hodges JR, Irish M. Uncovering the neural bases of cognitive and affective empathy deficits in Alzheimer’s disease and the behavioral-variant of frontotemporal dementia. Knopman D, ed. J Alzheimer’s Dis. 2016;53(3):801–816. doi:10.3233/JAD-160175
38. Nash S, Henry JD, McDonald S, Martin I, Brodaty H, Peek-O’Leary M-A. Cognitive disinhibition and socioemotional functioning in Alzheimer’s disease. J Int Neuropsychol Soc. 2007;13(6):1060–1064. doi:10.1017/S1355617707071184
39. Rankin KP, Kramer JH, Miller BL. Patterns of cognitive and emotional empathy in frontotemporal lobar degeneration. Cogn Behav Neurol. 2005;18(1):28–36. doi:10.1097/01.wnn.0000152225.05377.ab
40. Siegler IC, Dawson DV, Welsh KA. Caregiver ratings of personality change in Alzheimer’s disease patients: a replication. Psychol Aging. 1994;9(3):464–466. doi:10.1037/0882-7974.9.3.464
41. Rankin KP, Gorno-Tempini ML, Allison SC, et al. Structural anatomy of empathy in neurodegenerative disease. Brain. 2006;129(11):2945–2956. doi:10.1093/brain/awl254
42. Lee TMC, Sun D, Leung M-K, Chu L-W, Keysers C. Neural activities during affective processing in people with Alzheimer’s disease. Neurobiol Aging. 2013;34(3):706–715. doi:10.1016/j.neurobiolaging.2012.06.018
43. Mar RA. The neural bases of social cognition and story comprehension. Annu Rev Psychol. 2011;62(1):103–134. doi:10.1146/annurev-psych-120709-145406
44. Martinez M, Multani N, Anor CJ, et al. Emotion detection deficits and decreased empathy in patients with Alzheimer’s disease and Parkinson’s disease affect caregiver mood and burden. Front Aging Neurosci. 2018;10:120. doi:10.3389/fnagi.2018.00120
45. Olney NT, Spina S, Miller BL. Frontotemporal Dementia. Neurol Clin. 2017;35(2):339–374. doi:10.1016/j.ncl.2017.01.008
46. Onyike CU, Diehl-Schmid J. The epidemiology of frontotemporal dementia. Int Rev Psychiatry. 2013;25(2):130–137. doi:10.3109/09540261.2013.776523
47. Rosen HJ, Allison SC, Schauer GF, Gorno-Tempini ML, Weiner MW, Miller BL. Neuroanatomical correlates of behavioural disorders in dementia. Brain. 2005;128(11):2612–2625. doi:10.1093/brain/awh628
48. Seeley WW, Crawford R, Rascovsky K, et al. Frontal paralimbic network atrophy in very mild behavioral variant frontotemporal dementia. Arch Neurol. 2008;65(2):249–255. doi:10.1001/archneurol.2007.38
49. Varma AR, Adams W, Lloyd JJ, et al. Diagnostic patterns of regional atrophy on MRI and regional cerebral blood flow change on SPECT in young onset patients with Alzheimer’s disease, frontotemporal dementia and vascular dementia. Acta Neurol Scand. 2002;105(4):261–269. doi:10.1034/j.1600-0404.2002.1o148.x
50. Rascovsky K, Hodges JR, Knopman DS, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain a J Neurol. 2011;134(9):2456–2477. doi:10.1093/brain/awr179
51. Lough S, Kipps CM, Treise C, Watson P, Blair JR, Hodges JR. Social reasoning, emotion and empathy in frontotemporal dementia. Neuropsychologia. 2006;44(6):950–958. doi:10.1016/j.neuropsychologia.2005.08.009
52. Hua AY, Sible IJ, Perry DC, et al. Enhanced positive emotional reactivity undermines empathy in behavioral variant frontotemporal dementia. Front Neurol. 2018;9:402. doi:10.3389/fneur.2018.00402
53. Eslinger PJ, Moore P, Anderson C, Grossman M. Social cognition, executive functioning, and neuroimaging correlates of empathic deficits in frontotemporal dementia. J Neuropsychiatry Clin Neurosci. 2011;23(1):74–82. doi:10.1176/jnp.23.1.jnp74
54. Eslinger PJ, Moore P, Troiani V, et al. Oops! Resolving social dilemmas in frontotemporal dementia. J Neurol Neurosurg Psychiatry. 2007;78:457–460. doi:10.1136/jnnp.2006.098228
55. Baez S, Manes F, Huepe D, et al. Primary empathy deficits in frontotemporal dementia. Front Aging Neurosci. 2014;6(262). doi:10.3389/fnagi.2014.00262
56. Cerami C, Dodich A, Canessa N, et al. Neural correlates of empathic impairment in the behavioral variant of frontotemporal dementia. Alzheimer’s Dement. 2014;10(6):827–834. doi:10.1016/j.jalz.2014.01.005
57. Caminiti SP, Canessa N, Cerami C, et al. Affective mentalizing and brain activity at rest in the behavioral variant of frontotemporal dementia. Neuroimage. 2015;9:484–497. doi:10.1016/j.nicl.2015.08.012
58. Kamminga J, Kumfor F, Burrell JR. Differentiating between right-lateralised semantic dementia and behavioural-variant frontotemporal dementia: an examination of clinical characteristics and emotion processing. J Neurol Neurosurg Psychiatry. 2015;86:1082–1088. doi:10.1136/jnnp-2014-309120
59. Baez S, Morales JP, Slachevsky A, et al. Orbitofrontal and limbic signatures of empathic concern and intentional harm in the behavioral variant frontotemporal dementia. Cortex. 2016;75:20–32. doi:10.1016/J.CORTEX.2015.11.007
60. Oliver LD, Mitchell DGV, Dziobek I, et al. Parsing cognitive and emotional empathy deficits for negative and positive stimuli in frontotemporal dementia. Neuropsychologia. 2015;67:14–26. doi:10.1016/J.NEUROPSYCHOLOGIA.2014.11.022
61. Rabinovici GD, Rascovsky K, Miller BL. Frontotemporal lobar degeneration: clinical and pathologic overview. Handb Clin Neurol. 2008;89:343–364. doi:10.1016/S0072-9752(07)01233-X
62. Hodges JR, Patterson K, Oxbury S, Funnell E. Semantic dementia. Progressive fluent aphasia with temporal lobe atrophy. Brain. 1992;115(Pt 6):1783–1806. doi:10.1093/brain/115.6.1783
63. Narme P, Mouras H, Roussel M, Duru C, Krystkowiak P, Godefroy O. Emotional and cognitive social processes are impaired in Parkinson’s disease and are related to behavioral disorders. Neuropsychology. 2013;27(2):182–192. doi:10.1037/a0031522
64. Grossman M. The non-fluent/agrammatic variant of primary progressive aphasia. Lancet Neurol. 2012;11(6):545–555. doi:10.1016/S1474-4422(12)70099-6
65. Montembeault M, Brambati SM, Gorno-Tempini ML, Migliaccio R. Clinical, anatomical, and pathological features in the three variants of primary progressive aphasia: a review. Front Neurol. 2018;9:692. doi:10.3389/fneur.2018.00692
66. Rabinovici GD, Jagust WJ, Furst AJ, et al. Aβ amyloid and glucose metabolism in three variants of primary progressive aphasia. Ann Neurol. 2008;64(4):388–401. doi:10.1002/ana.21451
67. Ascherio A, Schwarzschild MA. The epidemiology of Parkinson’s disease: risk factors and prevention. Lancet Neurol. 2016;15(12):1257–1272. doi:10.1016/S1474-4422(16)30230-7
68. Forno LS. Neuropathology of Parkinsonʼs Disease. J Neuropathol Exp Neurol. 1996;55(3):259–272. doi:10.1097/00005072-199603000-00001
69. Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30(12):1591–1601. doi:10.1002/mds.26424
70. Dubois B, Burn DJ, Goetz CG, et al. Diagnostic procedures for Parkinson’s disease dementia: recommendations from the movement disorder society task force. Mov Disord. 2007;22(16):2314–2324. doi:10.1002/mds.21844
71. Verbaan D, Marinus J, Visser M, et al. Cognitive impairment in Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2007;78(11):1182–1187. doi:10.1136/jnnp.2006.112367
72. Burton EJ, McKeith IG, Burn DJ, Williams ED, O’Brien JT. Cerebral atrophy in Parkinson’s disease with and without dementia: a comparison with Alzheimer’s disease, dementia with Lewy bodies and controls. Brain. 2004;127(4):791–800. doi:10.1093/brain/awh088
73. Antonini A, De Notaris R, Benti R, De Gaspari D, Pezzoli G. Perfusion ECD/SPECT in the characterization of cognitive deficits in Parkinson’s disease. Neurol Sci. 2001;22(1):45–46. doi:10.1007/s100720170039
74. Kay C, Hayden MR, Leavitt BR. Epidemiology of Huntington disease. In: Feigin AS, Anderson KE editors, Handbook of Clinical Neurology. Vol. 144. Elsevier B.V.; 2017:31–46. doi:10.1016/B978-0-12-801893-4.00003-1
75. Pringsheim T, Wiltshire K, Day L, Dykeman J, Steeves T, Jetté N. The incidence and prevalence of Huntington’s disease: a systematic review and meta-analysis. Mov Disord. 2012;27(9):1083–1091. doi:10.1002/mds.25075
76. Van Den Bogaard SJA, Dumas EM, Acharya P, et al. Early atrophy of pallidum and accumbens nucleus in Huntington’s disease. J Neurol. 2011;258:412–420. doi:10.1007/s00415-010-5768-0
77. Aylward EH, Brandt J, Codori AM, Mangus RS, Barta PE, Harris GJ. Reduced basal ganglia volume associated with the gene for Huntington’s disease in asymptomatic at-risk persons. Neurology. 1994;44(5):823–828. doi:10.1212/WNL.44.5.823
78. Tabrizi SJ, Scahill RI, Owen G, et al. Predictors of phenotypic progression and disease onset in premanifest and early-stage Huntington’s disease in the TRACK-HD study: analysis of 36-month observational data. Lancet Neurol. 2013;12(7):637–649. doi:10.1016/S1474-4422(13)70088-7
79. Paulsen JS, Nopoulos PC, Aylward EH, et al. Striatal and white matter predictors of estimated diagnosis for Huntington disease. Brain Res Bull. 2010;82(3–4):201–207. doi:10.1016/j.brainresbull.2010.04.003
80. Rosas HD, Reuter M, Doros G, et al. A tale of two factors: what determines the rate of progression in Huntington’s disease? A longitudinal MRI study. Mov Disord. 2011;26(9):1691–1697. doi:10.1002/mds.23762
81. Ciarmiello A, Cannella M, Lastoria S, et al. Brain white-matter volume loss and glucose hypometabolism precede the clinical symptoms of Huntington’s disease. J Nucl Med. 2006;47(2):215–222.
82. Trinkler I, Cleret de Langavant L, Bachoud-Lévi A-C. Joint recognition-expression impairment of facial emotions in Huntington’s disease despite intact understanding of feelings. Cortex. 2013;49(2):549–558. doi:10.1016/j.cortex.2011.12.003
83. Adjeroud N, Besnard J, El Massioui N, et al. Theory of mind and empathy in preclinical and clinical Huntington’s disease. Soc Cogn Affect Neurosci. 2016;11(1):89–99. doi:10.1093/scan/nsv093
84. Maurage P, Lahaye M, Grynberg D, et al. Dissociating emotional and cognitive empathy in pre-clinical and clinical Huntington’s disease. Psychiatry Res. 2016;237:103–108. doi:10.1016/j.psychres.2016.01.070
85. Eddy CM, Rickards HE. Theory of mind can be impaired prior to motor onset in Huntington’s disease. Neuropsychology. 2015;29(5):792–798. doi:10.1037/neu0000190
86. Baez S, Herrera E, Gershanik O, et al. Impairments in negative emotion recognition and empathy for pain in Huntington’s disease families. Neuropsychologia. 2015;68:158–167. doi:10.1016/j.neuropsychologia.2015.01.012
87. Trinkler I, Devignevielle S, Achaibou A, et al. Embodied emotion impairment in Huntington’s Disease. Cortex. 2017;92:44–56. doi:10.1016/j.cortex.2017.02.019
88. Adolphs R, Damasio H, Tranel D, Cooper G, Damasio AR. A role for somatosensory cortices in the visual recognition of emotion as revealed by three-dimensional lesion mapping. J Neurosci. 2000;20(7):2683–2690. doi:10.1523/JNEUROSCI.20-07-02683.2000
89. Logroscino G, Traynor BJ, Hardiman O, et al. Incidence of amyotrophic lateral sclerosis in Europe. J Neurol Neurosurg Psychiatry. 2010;81(4):385–390. doi:10.1136/jnnp.2009.183525
90. Rowland LP, Shneider NA. Amyotrophic Lateral Sclerosis. N Engl J Med. 2001;344(22):1688–1700. doi:10.1056/NEJM200105313442207
91. Goldstein LH, Abrahams S. Changes in cognition and behaviour in amyotrophic lateral sclerosis: nature of impairment and implications for assessment. Lancet Neurol. 2013;12(4):368–380. doi:10.1016/S1474-4422(13)70026-7
92. Palmieri A, Sorarù G, Albertini E, et al. Psychopathological features and suicidal ideation in amyotrophic lateral sclerosis patients. Neurol Sci. 2010;31(6):735–740. doi:10.1007/s10072-010-0332-3
93. Shen D, Cui L, Fang J, Cui B, Li D, Tai H. Voxel-wise meta-analysis of gray matter changes in amyotrophic lateral sclerosis. Front Aging Neurosci. 2016;8:64. doi:10.3389/fnagi.2016.00064
94. Matías-Guiu JA, Pytel V, Cabrera-Martín MN, et al. Amyloid- and FDG-PET imaging in amyotrophic lateral sclerosis. Eur J Nucl Med Mol Imaging. 2016;43(11):2050–2060. doi:10.1007/s00259-016-3434-1
95. Cerami C, Dodich A, Canessa N, et al. Emotional empathy in amyotrophic lateral sclerosis: a behavioural and voxel-based morphometry study. Amyotroph Lateral Scler Front Degener. 2014;15(1–2):21–29. doi:10.3109/21678421.2013.785568
96. van der Hulst E-J, Bak TH, Abrahams S. Impaired affective and cognitive theory of mind and behavioural change in amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry. 2015;86:1208–1215. doi:10.1136/jnnp-2014-309290
97. Watermeyer TJ, Brown RG, Sidle KCL, et al. Executive dysfunction predicts social cognition impairment in amyotrophic lateral sclerosis. J Neurol. 2015;262(7):1681–1690. doi:10.1007/s00415-015-7761-0
98. Guidetti D, Sabadini R, Ferlini A, Torrente I. Epidemiological survey of X-linked bulbar and spinal muscular atrophy, or Kennedy disease, in the province of Reggio Emilia, Italy. Eur J Epidemiol. 2001;17(6):587–591. doi:10.1023/A:1014580219761
99. Finsterer J, Sorarù G. onset manifestations of spinal and bulbar muscular atrophy (Kennedy’s Disease). J Mol Neurosci. 2016;58(3):321–329. doi:10.1007/s12031-015-0663-x
100. Fratta P, Nirmalananthan N, Masset L, et al. Correlation of clinical and molecular features in spinal bulbar muscular atrophy. Neurology. 2014;82(23):2077–2084. doi:10.1212/WNL.0000000000000507
101. Kennedy WR, Alter M, Sung JH. Progressive proximal spinal and bulbar muscular atrophy of late onset. A sex-linked recessive trait. Neurology. 1968;18(7):671–680. doi:10.1212/WNL.18.7.671
102. Di Rosa E, Sorarù G, Kleinbub JR, et al. Theory of mind, empathy and neuropsychological functioning in X-linked Spinal and Bulbar Muscular Atrophy: a controlled study of 20 patients. J Neurol. 2015;262(2):394–401. doi:10.1007/s00415-014-7567-5
103. Marcato S, Kleinbub JR, Querin G, et al. Unimpaired neuropsychological performance and enhanced memory recall in patients with Sbma: a large sample comparative study. Sci Rep. 2018;8(1):13627. doi:10.1038/s41598-018-32062-5
104. Soukup GR, Sperfeld AD, Uttner I, et al. Frontotemporal cognitive function in X-linked spinal and bulbar muscular atrophy (SBMA): a controlled neuropsychological study of 20 patients. J Neurol. 2009;256(11):1869–1875. doi:10.1007/s00415-009-5212-5
105. Guidetti D, Vescovini E, Motti L, et al. X-linked bulbar and spinal muscular atrophy, or Kennedy disease: clinical, neurophysiological, neuropathological, neuropsychological and molecular study of a large family. J Neurol Sci. 1996;135(2):140–148. doi:10.1016/0022-510X(95)00283-8
106. Kasper E, Wegrzyn M, Marx I, et al. Minor cognitive disturbances in X-linked spinal and bulbar muscular atrophy, Kennedy’s disease. Amyotroph Lateral Scler Frontotemporal Degener. 2014;15(1–2):15–20. doi:10.3109/21678421.2013.837927
107. Kassubek J, Juengling FD, Sperfeld AD. Widespread white matter changes in Kennedy disease: a voxel based morphometry study. J Neurol Neurosurg Psychiatry. 2007;78(11):1209–1212. doi:10.1136/jnnp.2006.112532
108. Pieper CC, Konrad C, Sommer J, Teismann I, Schiffbauer H. Structural changes of central white matter tracts in Kennedy’s disease - a diffusion tensor imaging and voxel-based morphometry study. Acta Neurol Scand. 2013;127(5):323–328. doi:10.1111/ane.12018
109. Lai T-H, Liu R-S, Yang B-H, et al. Cerebral involvement in spinal and bulbar muscular atrophy (Kennedy’s disease): a pilot study of PET. J Neurol Sci. 2013;335(1–2):139–144. doi:10.1016/J.JNS.2013.09.016
110. Adenzato M, Poletti M. Theory of Mind abilities in neurodegenerative diseases: an update and a call to introduce mentalizing tasks in standard neuropsychological assessments. Clin Neuropsychiatry. 2013;10(5):226–234.
111. Russell J. How executive disorders can bring about an inadequate “theory of mind.”. In: Autism as an Executive Disorder. New York, NY: Oxford University Press; 1997:256–304.
112. van Honk J, Schutter DJ, Bos PA, Kruijt A-W, Lentjes EG, Baron-Cohen S. Testosterone administration impairs cognitive empathy in women depending on second-to-fourth digit ratio. Proc Natl Acad Sci U S A. 2011;108(8):3448–3452. doi:10.1073/pnas.1011891108
113. Miller DI, Halpern DF. The new science of cognitive sex differences. Trends Cogn Sci. 2014;18(1):37–45. doi:10.1016/J.TICS.2013.10.011
114. Bremner JD, Soufer R, McCarthy G, et al. Gender differences in cognitive and neural correlates of remembrance of emotional words. Psychopharmacol Bull. 2001;35(3):55–78.
115. Baron-cohen S. The extreme male brain theory of autism. Trends Cogn Sci. 2002;6(6):248–254. doi:10.1016/S1364-6613(02)01904-6
116. Emery AEH. Population frequencies of inherited neuromuscular diseases—A world survey. Neuromuscul Disord. 1991;1(1):19–29. doi:10.1016/0960-8966(91)90039-U
117. Mahadevan M, Tsilfidis C, Sabourin L, et al. Myotonic dystrophy mutation: an unstable CTG repeat in the 3ʹ untranslated region of the gene. Science. 1992;255(5049):1253–1255. doi:10.1126/science.1546325
118. Harper PS. Myotonic Dystrophy: Major Problems in Neurology.
119. Peric S, Rakocevic Stojanovic V, Mandic Stojmenovic G, et al. Clusters of cognitive impairment among different phenotypes of myotonic dystrophy type 1 and type 2. Neurol Sci. 2017;38:415–423. doi:10.1007/s10072-016-2778-4
120. Romeo V, Pegoraro E, Ferrati C, et al. Brain involvement in myotonic dystrophies: neuroimaging and neuropsychological comparative study in DM1 and DM2. J Neurol. 2010;257(8):1246–1255. doi:10.1007/s00415-010-5498-3
121. Modoni A, Silvestri G, Vita MG, Quaranta D, Tonali PA, Marra C. Cognitive impairment in myotonic dystrophy type 1 (DM1). J Neurol. 2008;255(11):1737–1742. doi:10.1007/s00415-008-0017-5
122. Sistiaga A, Urreta I, Jodar M, et al. Cognitive/personality pattern and triplet expansion size in adult myotonic dystrophy type 1 (DM1): CTG repeats, cognition and personality in DM1. Psychol Med. 2010;40(3):487. doi:10.1017/S0033291709990602
123. Labayru G, Arenzana I, Aliri J, Zulaica M, López de Munain A, Sistiaga AA. Social cognition in myotonic dystrophy type 1: specific or secondary impairment? PLoS One. 2018;13(9):e0204227. doi:10.1371/journal.pone.0204227
124. Serra L, Cercignani M, Bruschini M, et al. “I know that you know that i know”: neural substrates associated with social cognition deficits in DM1 patients. PLoS One. 2016;11(6):e0156901. doi:10.1371/journal.pone.0156901
125. Fuertes JN, Toporovsky A, Reyes M, Osborne JB. The physician-patient working alliance: theory, research, and future possibilities. Patient Educ Couns. 2017;100(4):610–615. doi:10.1016/J.PEC.2016.10.018
126. Kelley JM, Kraft-Todd G, Schapira L, Kossowsky J, Riess H. The Influence of the patient-clinician relationship on healthcare outcomes: a systematic review and meta-analysis of randomized controlled trials. Timmer A, ed. PLoS One. 2014;9(4):e94207. doi:10.1371/journal.pone.0094207
127. Hojat M, Louis DZ, Markham FW, Wender R, Rabinowitz C, Gonnella JS. Physiciansʼ empathy and clinical outcomes for diabetic patients. Acad Med. 2011;86(3):359–364. doi:10.1097/ACM.0b013e3182086fe1
128. Di Blasi Z, Harkness E, Ernst E, Georgiou A, Kleijnen J. Influence of context effects on health outcomes: a systematic review. Lancet. 2001;357(9258):757–762. doi:10.1016/S0140-6736(00)04169-6
129. Calvo V, Palmieri A, Marinelli S, Bianco F, Kleinbub JR. Reciprocal empathy and working alliance in terminal oncological illness: the crucial role of patients’ attachment style. J Psychosoc Oncol. 2014;32(5):517–534. doi:10.1080/07347332.2014.936651
130. Andersen PM, Abrahams S, Borasio GD, et al. EFNS guidelines on the Clinical Management of Amyotrophic Lateral Sclerosis (MALS) - revised report of an EFNS task force. Eur J Neurol. 2012;19(3):360–375. doi:10.1111/j.1468-1331.2011.03501.x
131. Sorbi S, Hort J, Erkinjuntti T, et al. EFNS-ENS Guidelines on the diagnosis and management of disorders associated with dementia. Eur J Neurol. 2012;19(9):1159–1179. doi:10.1111/j.1468-1331.2012.03784.x
132. Boffo M, Mannarini S, Munari C. Exploratory structure equation modeling of the UCLA loneliness scale: a contribution to the Italian adaptation. TPM - Testing, Psychom Methodol Appl Psychol. 2012;19(4):345–363. doi:10.4473/TPM19.4.7
133. Roter DL, Hall JA, Merisca R, Nordstrom B, Cretin D, Svarstad B. Effectiveness of interventions to improve patient compliance: a meta-analysis. Med Care. 1998;36(8):1138–1161. doi:10.1097/00005650-199808000-00004
134. Kleinbub JR. State of the art of interpersonal physiology in psychotherapy: a systematic review. Front Psychol. 2017;8:2053. doi:10.3389/fpsyg.2017.02053
135. Fonagy P, Allison E. The role of mentalizing and epistemic trust in the therapeutic relationship. Psychother. 2014;51(3):372–380. doi:10.1037/a0036505
136. National Institute for Health and Clinical Excellence. NICE SCIE guideline to improve care of people with dementia. Available from: https://www.nice.org.uk/guidance?action=download&o=30323&r=true. 2006. Accessed March 14, 2019.
137. Mehrabian A, Epstein N. A measure of emotional empathy. J Pers. 1972;40(4):525–543. doi:10.1111/j.1467-6494.1972.tb00078.x
138. Jolliffe D, Farrington DP. Development and validation of the basic empathy scale. J Adolesc. 2006;29(4):589–611. doi:10.1016/J.ADOLESCENCE.2005.08.010
139. Decety J, Michalska KJ, Kinzler KD. The contribution of emotion and cognition to moral sensitivity: a neurodevelopmental study. Cereb Cortex. 2012;22(1):209–220. doi:10.1093/cercor/bhr111
140. Baron-Cohen S, Wheelwright S. The empathy quotient: an investigation of adults with asperger syndrome or high functioning autism, and normal sex differences. J Autism Dev Disord. 2004;34(2):163–175. doi:10.1023/B:JADD.0000022607.19833.00
141. Stone VE, Baron-Cohen S, Knight RT. Frontal lobe contributions to theory of mind. J Cogn Neurosci. 1998;10(5):640–656. doi:10.1162/089892998562942
142. O’Sullivan M, Guilford J. Tests of Social Intelligence. Palo Alto, CA: Consulting Psychologists Press; 1965.
143. Dziobek I, Rogers K, Fleck S, et al. Dissociation of cognitive and emotional empathy in adults with asperger syndrome using the Multifaceted Empathy Test (MET). J Autism Dev Disord. 2008;38(3):464–473. doi:10.1007/s10803-007-0486-x
144. Ekman P, Friesen W. Pictures of Facial Affect. Palo Alto, CA: Consulting Psychologists Press; 1976.
145. Baron-Cohen S, Jolliffe T, Mortimore C, Robertson M. Another advanced test of theory of mind: evidence from very high functioning adults with autism or asperger syndrome. J Child Psychol Psychiatry. 1997;38(7):813–822. doi:10.1111/jcpp.1997.38.issue-7
146. McDonald S, Flanagan S, Rollins J, Kinch J. TASIT: a new clinical tool for assessing social perception after traumatic brain injury. J Head Trauma Rehabil. 2003;18(3):219–238. doi:10.1097/00001199-200305000-00001
147. Lopez-Pérez B, Fernaéndez-Pinto I, Abad F. TECA: Test De Empatia Cognitiva Y Afectiva. Madrid, ES: TEA Ediciones; 2008.
148. Crespi C, Cerami C, Dodich A, et al. Microstructural correlates of emotional attribution impairment in non-demented patients with amyotrophic lateral sclerosis. PLoS One. 2016;11:e0161034. doi:10.1371/journal.pone.0161034
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.