Back to Journals » Journal of Healthcare Leadership » Volume 17
Emotional Intelligence and Leadership Styles Among Managers in Primary Healthcare Centers, Riyadh, Saudi Arabia
Authors Alasmari AA ![]() , Awad RA
, Awad RA ![]() , Alshowair AM
, Alshowair AM ![]() , Albattal SM, AlMutairi AH, Abdel-Azeem A
, Albattal SM, AlMutairi AH, Abdel-Azeem A ![]() , Kofi M
, Kofi M ![]()
Received 11 February 2025
Accepted for publication 28 May 2025
Published 24 June 2025 Volume 2025:17 Pages 285—295
DOI https://doi.org/10.2147/JHL.S522197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Russell Taichman
Aeshah Abdullah Alasmari,1 Raseel Abdulaziz Awad,2 Abdulmajeed Mohamed Alshowair,3 Saad M Albattal,4 Abdulmajeed Homaidan AlMutairi,4 Amro Abdel-Azeem,5 Mostafa Kofi4
1Family Medicine Department, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 2Al-Murabba PHC, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 3VP Community Health Excellence, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia; 4Family Medicine Department, Prince Sultan Military Medical City, Ministry of Defense Health Services, Riyadh, Saudi Arabia; 5Population Health Management and Research, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia
Correspondence: Mostafa Kofi, Family Medicine Department, Prince Sultan Military Medical City, Ministry of Defense Health Services, Riyadh, Saudi Arabia, Tel +966501436859, Email [email protected] Amro Abdel-Azeem, Population Health Management and Research, Riyadh First Health Cluster Ministry of Health, Riyadh, Saudi Arabia, Tel +966547135224, Email [email protected]
Purpose: Effective leadership is one of the most important factors contributing to an organization’s effectiveness and success. The objective of this study is to identify the leadership styles of primary healthcare managers and explore associated sociodemographic factors.
Methods: A cross-sectional study was conducted at Prince Sultan Military Medical City (PSMMC) in Riyadh, Saudi Arabia, among primary healthcare managers in different aspects of 6 primary healthcare centers (PHC). Data were collected using a self-assessment questionnaire composed of two main sections: sociodemographic characteristics of the participants and the emotional intelligence questionnaire to assess the various competencies of emotional intelligence of leadership style.
Results: A total of 50 primary healthcare managers were included in the study. Approximately half of them (52%) were aged between 35 and 44 years. The highest applied statement was “I know when I am happy (4.42± 0.95)”, whereas the lowest applied statement was “I rarely worry about work or life in general (3.20± 1.26)”. Self-awareness was considered a strength in most of the participants (78%), while, managing emotions needs attention in 52% of them. Intrinsic motivating, empathy, and social skill were considered strengths in most of the participants (70%, 74%, and 68%, respectively). Participants aged (25– 34 years) were more likely than others to need attention in the component of “intrinsic motivating” (31.6%), p=0.053. Single participants were more likely than married participants to need attention in the component of “intrinsic motivating” (70% versus 18.4%). P=0.006. Nurses, pharmacists and radiologists were more likely to need attention in the component of “self-awareness” than doctors and directors, p = 0.041.
Conclusion: This study highlights the significance of emotional intelligence components, such as self-awareness, empathy, and social skills, as strengths among primary healthcare managers in Riyadh, Saudi Arabia. The findings emphasize that enhancing emotional intelligence is essential for fostering effective leadership within primary healthcare sitting.
Keywords: leadership styles, emotional intelligence questionnaire, primary healthcare centers, healthcare management, transformational leadership, vision 2030
Introduction
Leadership style is the value of behavior, which evidently can affect the management and development of the health system.1 The successful leadership leads to innovation.2,3 and plays a basic role in developing quality of care and increasing patient safety.4,5
Historically, leadership is a significant picture of management that has been seen as a dominant, attractive, and powerful factor. Transforming in a healthcare organization faces different issues and risks, particularly the refusal to obligation;6 the cause for that tends to be the absence of effective leadership.7,8 Definitely, every change, small or big, can immediately inspire people, and a result will also improve their productivity.8–12 There is a strong connection between managers and their employees.13
Leadership is a manager’s strength in changing how employees think, feel, and carry out their duties.14,15 Managers in health care have the authority and resources to monitor and support excellent quality and safety.5,16,17 Competent and intelligent managers help to enhance organizational safety and culture.18 When there is effective leadership, there is a successful organization.19
In the healthcare system, there is a constant need to emphasize the notion of leadership. Several strategy documents emphasize the need to educate healthcare workers as team managers based on the understanding of healthcare leadership and management. Many healthcare professionals now confront this difficulty, and they are frequently required to perform dual roles: professional and leadership.6–20
Leadership may face many challenges in managing emotions and intrinsic motivation within primary healthcare. Professionals and other employees are generally resistant to changes that are seen to risk their basic interests, beliefs, and practices, as well as to negatively affect people and reduce their autonomy. As a result, transferring people out of their “comfort zone” implies taking them from a known and comfortable setting to an unpredictable one. Change results in unanticipated processes and situations that bring back many opportunities, but also challenges.21–23
Effective leadership is one of the most important factors that contribute to an organization’s effectiveness and success. Significant favorable relationships have been documented between successful leadership styles and significant levels of satisfaction with patients and reduced unpleasant effects.13
There are several models of emotional intelligence and leadership development practices that differ widely. Additionally,24 Numerous studies have reported that emotional intelligence, as a leadership development strategy, plays vital roles in enhancing physicians’ personal and professional development. They revealed that emotional intelligence is considered a relevant throughout education and clinical practice.24,25
Kingdom Saudi Arabia’s Vision 2030, highlights the eminent need for well-organized leadership programs that focus on developing emotional intelligence and equipping managers with proficient skills to drive organizational success and improve health outcomes. and fostering healthcare transformation.26
This study aims to identify the emotional intelligence and leadership styles of primary healthcare managers and to identify sociodemographic factors associated with it. This study hypnotized that emotional intelligence and leadership style components such as self-awareness, empathy, and social skills, are strengths among primary healthcare managers in Riyadh, Saudi Arabia.
Subjects and Methods
A cross-sectional study was conducted from May to November 2024 at Prince Sultan Military Medical City (PSMMC) centers, in Riyadh, Saudi Arabia among primary healthcare managers in different aspects of 6 primary healthcare centers (PHC). A convenient non-probability sample of 50 eligible primary healthcare managers in different aspects was included. Participants were selected for inclusion in the sample due to geographical proximity and willingness to participate in the research. Managers included directors, doctors, nurses, pharmacists and radiologists.
Data were collected using a self-assessment questionnaire composed of two main sections; sociodemographic characteristics of the participants (age, gender, marital status, profession, qualification, and years of experience in practice) and the NHS Leadership Tool kit Emotional Intelligence Questionnaire, which is a 50 items tool designed to assess the various competences of emotional intelligence. It includes 5 domains (Self-awareness, managing emotions, intrinsic motivation, empathy, and social skill). Responses will be reported on a 5-Likert scale ranging from 1 (does not apply) through 3 (applies half of the time) to 5 (always applies) depending on how strongly each one of the 50 statements applies. The self-awareness domain is indicated by statements 1, 6, 11, 16, 21, 26, 31, 36, 41 and 46. Managing emotions domain is indicated by statements 2, 7, 12, 17, 22, 27, 32, 37, 42 and 47. Intrinsic motivating domain is indicated by statements 3, 8, 13, 18, 23, 28, 33, 38, 43, and 48. The empathy domain is indicated by statements 4, 9, 14, 19, 24, 29, 34, 39, 44, and 49, and the social skill domain is indicated by statements 5, 10, 15, 20, 25, 30, 35, 40, 45 and 50. A total score was computed and interpreted as those scored between 10 and 17 indicated developing priority. Those who scored between 18 and 34 indicated the need for attention while those who scored between 35 and 50 indicated a strength for the participant.27 The questionnaire had been utilized in many previous studies and reported high reliability with Cronbach’s alpha estimated between (0.70 and 0.91).28–30 In this study, the reliability of the emotional intelligence questionnaire was estimated to be high (Cronbach’s alpha = 0.82).
All data were collected, coded in an Excel sheet, and analyzed using the Statistical Package for Social Sciences (SPSS) package version 28. Categorical variables were described by frequencies and percentages, while numerical variables were presented as mean standard deviation. Chi-Square Test was utilized for analysis of data while, Fischer Exact Test was utilized when the assumptions of the Chi-Square Test were not met (more than 20% of cells have expected cell counts less than 5, and no expected cell count is less than 1), A p-value of ≤0.05 was considered statistically significant.
Results
Sociodemographic Characteristics
A total of 50 primary healthcare managers were included in the study. Their sociodemographic characteristics are summarized in Table 1. Slightly more than half of them (52%) were aged between 35 and 44 years, whereas 10% were 45 years and above. Males represented 60% of the participants. Most of them (76%) were married, and 44% were bachelor’s degree holders. Slightly more than half (52%) of the participants had experience exceeding 10 years in primary care. Regarding their profession, 22% were doctors in charge, and 20% were charge nurses.
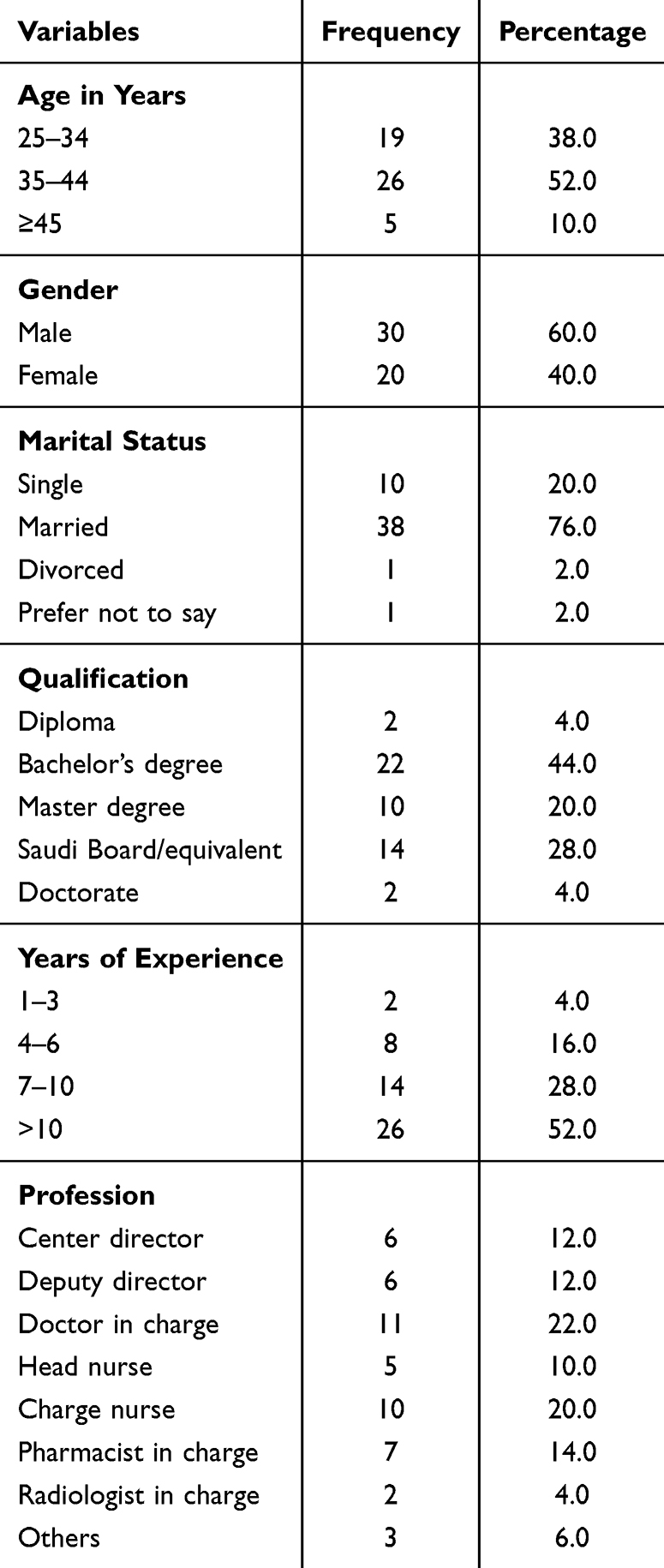 |
Table 1 Sociodemographic Characteristics of the Participants (n=50) |
Emotional Intelligence Questionnaire of Leadership Style
The response of the participants to the 50 items of the emotional intelligence questionnaire of leadership style is presented in Table 2. The highest applied statement was “I know when I am happy (4.42±0.95)”, followed by “I am able to always motivate myself to do difficult tasks (4.24±0.98)”, “I can tell if a team of people is not getting along with each other (4.18±0.96)”, “I know what makes me happy (4.12±1.10)”, and “I am an excellent listener (4.12±0.92)”. On the other hand, the lowest applied statement was “I rarely worry about work or life in general (3.20±1.26)”, followed by “Others can rarely tell what kind of mood I am in (3.26±1.14)”, “Others often do not know how I am feeling about things (3.30±1.15)”, and “Difficult people do not annoy me (3.40±1.14)”. Self-awareness was considered a strength in most of the participants (78%), while managing emotions needs attention in 52% of them. Intrinsic motivating, empathy, and social skills were considered strengths in most of the participants (70%, 74%, and 68%, respectively). Table 3
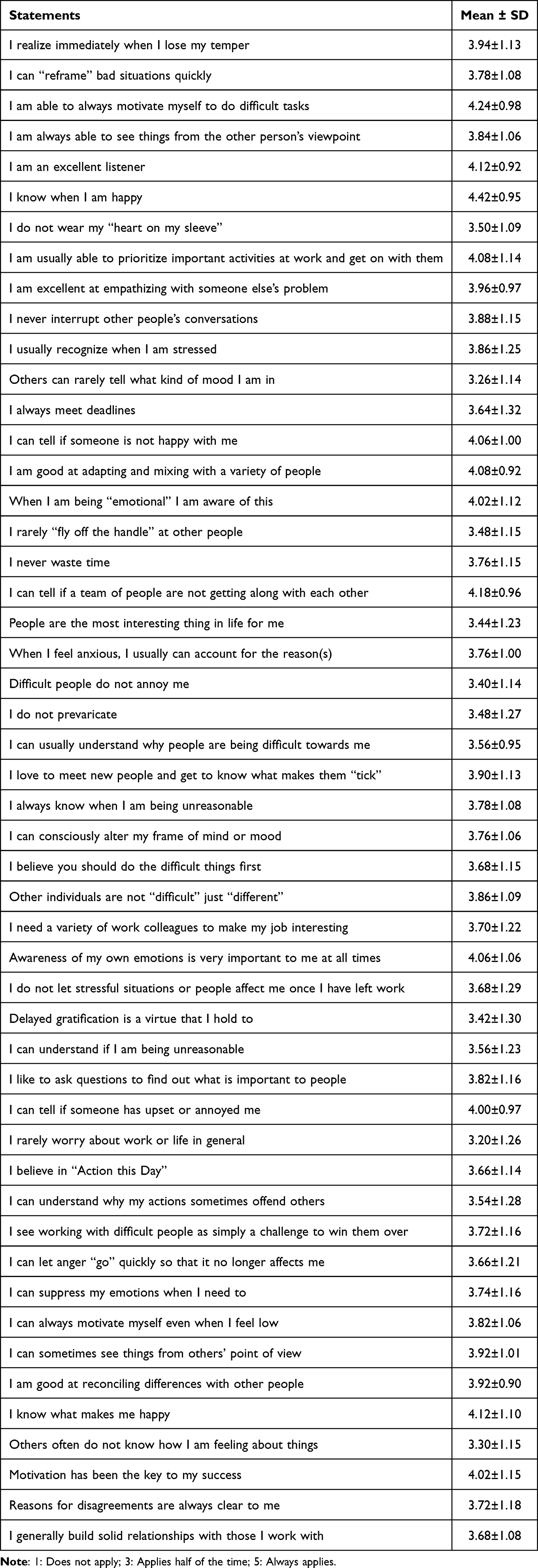 |
Table 2 Response of Participants to Emotional Intelligence Questionnaire of Leadership Style |
 |
Table 3 Different Components of Emotional Intelligence Leadership Style and Their Interpretations |
Sociodemographic Factors Associated with Leadership Style
As clear from Table 4, there was no statistically significant difference between males and females managers in all components of emotional intelligence leadership style. Regarding participant’s age, in the age group (25–34 years) were more likely than others to need attention in the component of “intrinsic motivating” (31.6% versus 26.9% for those in the age group “35–44” and 20% for those aged ≥45 years). This difference was borderline significant, p=0.053. There was no statistically significant difference between different participants’ age groups in all other components of emotional intelligence leadership style. On studying the association between marital status and leadership style, Table 4 shows that single participants were more likely than married participants to need attention in the component of “intrinsic motivating” (70% versus 18.4%). P=0.006. There was no statistically significant difference between single and married participants in all other components of emotional intelligence leadership style.
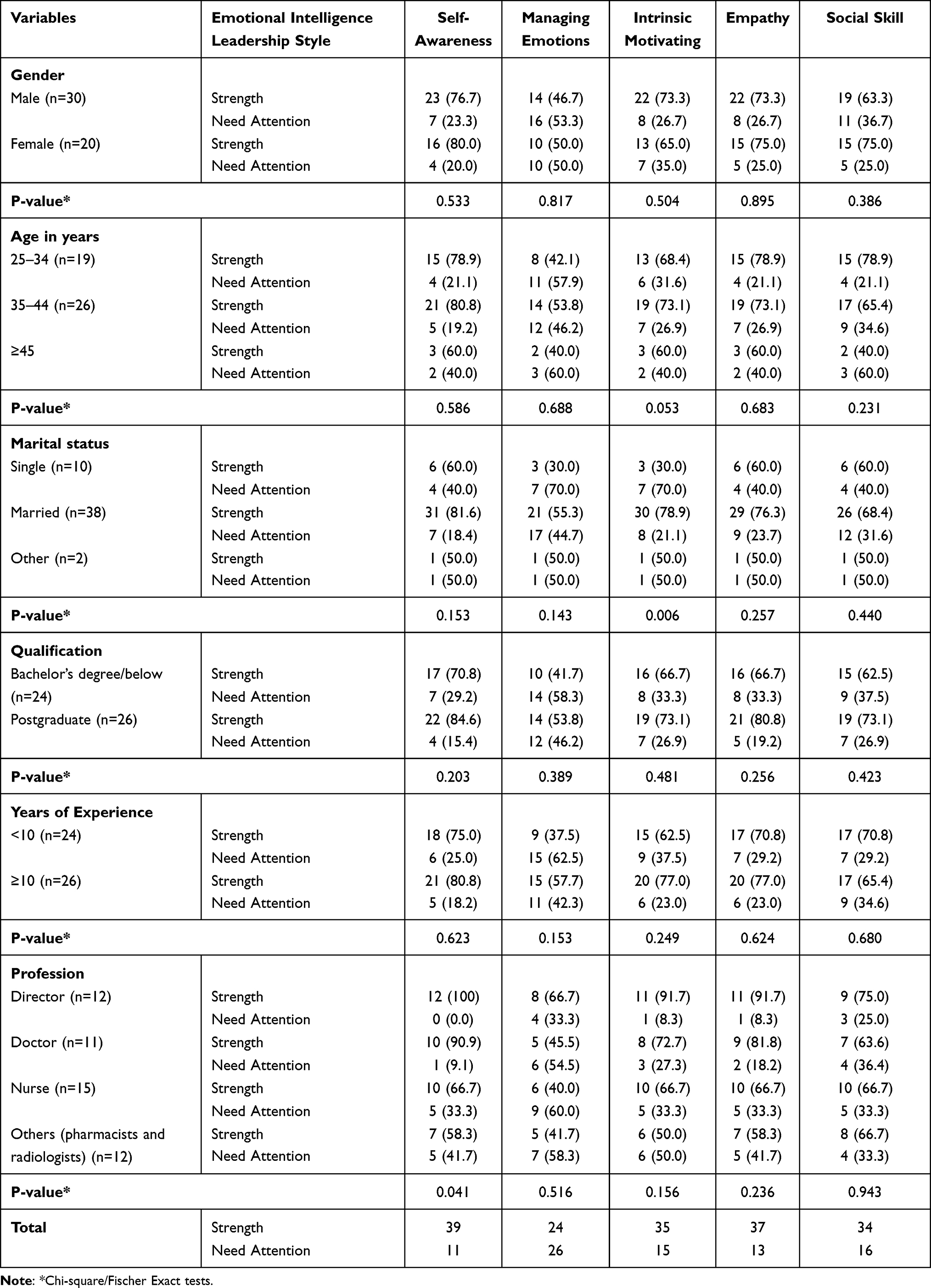 |
Table 4 Association Between Participants’ Sociodemographic Factors and Different Components of Emotional Intelligence Leadership Style |
Regarding participant’s qualifications, it is evident that there was no statistically significant difference between undergraduate and postgraduate qualified participants in all components of emotional intelligence leadership style. There was no statistically significant difference between low and high experienced participants in all components of emotional intelligence leadership style. Nurses and other professions (pharmacists and radiologists) were more likely to need attention in the component of “self-awareness” than doctors and directors, p = 0.041. There was no statistically significant difference between different professions in other components of emotional intelligence leadership style (Table 4).
Discussion
Leadership is a dynamic concept that develops over time. Therefore, it has been defined in various ways and considered a multidimensional process, involving a situation that influences a group in a place that looks for achieving common objectives.31 Effective leadership has a vital role in figuring the culture of a healthcare organization and confirming its ability to deal with healthcare delivery-complex issues. Thus, managers can utilize different leadership styles in healthcare, which offer different ways for them to interact with and motivate people under their responsibility.32 Mintz and Stoller reported that emotional intelligence is considered a leadership development strategy; however, the models of emotional intelligence and leadership development practices differ widely. Additionally, they concluded that emotional intelligence is considered relevant throughout education and clinical practice.24
In the present study, nurses were more likely to need attention in the component of “self-awareness” than doctors and directors. In accordance with that, Younas et al confirmed the importance of self-awareness for nurses in improving nurse-patient relationships as well as patient care.33 Numerous studies have identified the different leadership styles of healthcare leaders; however, owing to utilizing different tools in these studies and using a different tool in the present study, it makes the comparison between them an impractical issue. Coskun et al documented that emotional intelligence and leadership style play vital roles in enhancing physicians’ personal and professional development.25 Nightingale et al, in their integrative review, provided evidence that developing emotional intelligence in nurses may positively impact certain caring behaviors. They revealed that age, experience, burnout, and job satisfaction might also be relevant factors for both caring and emotional intelligence.28 However, Hamid et al at Rawalpindi Medical University detected a low level of emotional intelligence among their students and healthcare professionals. They emphasize the dire need to develop emotional maturity in medical students and clinicians.29
In this study, self-awareness was considered a strength in most of the participants, while managing emotions needs attention in almost half of them, while intrinsic motivating, empathy, and social skills were considered strengths in most of the participants. In Spain, Solà et al described how primary healthcare managers view different leadership styles using the Multifactor Leadership Questionnaire (MLQ). Managers evaluated themselves as both transactional and transformative leaders globally, and when they were grouped by occupation, nurses displayed a greater transactional leadership style than physicians, and men performed the worst in terms of a transactional approach when gender was considered, and they concluded that efficiency and job satisfaction were correlated with both transactional and transformational approaches.34 Dorji et al determined the necessary management skills the managers of primary health care possess and management skill-improving techniques and found that three competency domains and seven important sub-domain competencies were determined, with the people domain being deemed to be the most important necessary ability, followed by the execution and transformation domains. The perception of the highest required competency for the seven key sub-domains was in the communication sub-domain, which was followed by professionalism, managing change, relationship development, analytical thinking, leadership, and creative thought.35 Desta et al compared the leadership, management, and governance (LMG) with non-LMG districts’ capacities and performance at the district level and reported that LMG districts performed better on average than non-LMG districts.36 In Abha, Saudi Arabia (2021), Alqahtani et al explored the association between management styles and job satisfaction of the employees at primary healthcare centers utilizing the Multifactor Leadership Survey and observed that 68% of the managers highly endorsed the transformational leadership style, while “64% highly endorsed management-by-exception, and only 28% highly endorsed the laissez-faire” leadership style.37
It is widely acknowledged that managers in the healthcare industry would benefit greatly from professional education in the many facets of leadership. Several fundamental leadership skills (also known as “differentiating competencies”) must be professionally taught or honed despite inherent leadership abilities. Early in a career, leadership development may start. Despite the acknowledged need, there are not many opportunities for thorough leadership development. Healthcare leadership development programs were first developed largely as internal institutional curricula for the professional growth of teachers or practitioners. In response to the demands of particular cohorts of people, more extensive national leadership programs were created, such as programs for women that aim to increase the number of senior women managers in the health sciences.38 In the present study, no difference was observed between men and women managers. However, also in this study, we did not investigate the attendance of the participants at training leadership programs. The 2030 Saudi vision launched by the Saudi government ensured complementary equality between women and men to achieve ultimate justice, including rights to educate, work, and economic rights, and enabling women to incorporate and practice in commercial business without obtaining prior consent.39
Findings of studies have discovered that healthcare leadership training is most valuable when it occurs over time, is comprehensive and multidisciplinary, and integrates individual/institutional projects designed to allow participants immediate direct implementation of their newly acquired skills. The training should include all of the conventional areas of clinical practice, teaching, and research so that the managers can comprehend all of the operations under his or her direction. Furthermore, the development of future managers through early career leadership training lays the groundwork for people who might want to seek important leadership positions later in their careers. The ideal training for effective managers may be a blend of early and mid-to-late career growth. For a larger number of potential managers in the healthcare industry, more training programs are required to make complete leadership development broadly available.38 In the present study, no difference in leadership style was observed between managers according to their qualifications and years of experience in practice.
Numerous studies have investigated the significance of leadership style for the quality of healthcare provision in nursing homes.40 It has been shown in this regard that effective leadership has an indirect effect on reducing mortality rates by retaining and supporting experienced healthcare staff.32,41 The impact of leadership style on healthcare outcomes in our community should be investigated in a further study. In Indonesia (2020), Tahir et al determined the relationship between organizational and leadership style on one side and the enhancement of primary healthcare services’ quality on the other side and concluded that 66.7% of the participants stated that there was a positive association between organizing and quality improvement, and 72.4% said that there was a positive relationship between leadership style and quality improvement.42 Žibertt and Starc examined the effects of various leadership styles on the success of implementing changes and revealed that laissez-faire leadership and the effectiveness of the introduced modifications were adversely correlated and favorably correlated, respectively. Transformational, transactional, and laissez-faire leadership had positive correlations with the judged effectiveness of leadership styles, and nonetheless, a high correlation between the effectiveness of leadership styles as measured and the satisfaction with the changes made was shown to exist in transformative leadership.6 Franco and Almeida comprehended in a qualitative study the relationship between organizational learning and leadership styles in two continuous care units within Portuguese healthcare organizations and confirmed that organizational learning and leadership play an important role in determining organizational performance and effectiveness within healthcare organizations.43 Regarding the predictors and influencing factors of emotional intelligence, the study of Awe et al in United Kingdom indicated that 82% of the nurses had high emotional intelligence with a statistically significant relationship between empathy and race. Cultural differences, personality traits, self-care, family support, and organizational structure are found to be key predictors of emotional intelligence among respondents.30
Limitations of the Study
With a sample size of 50 participants, the findings of this study may not fully capture the diversity of leadership styles among primary healthcare managers in Riyadh. Variations in leadership practices across different clusters or regions may not be comprehensively represented. Another potential limitation is the self-reporting bias, as participants might overestimate their abilities. Furthermore, incorporating qualitative methods, such as interviews, could enhance understanding of how leadership styles impact workplace dynamics. In addition, the study was conducted at a single institution and at one point in time (sentiment and perceptions) which neglects the change over time. The study primarily explores leadership styles without establishing direct links to patient outcomes or employee satisfaction. This leaves an opportunity for further research to assess the practical implications of leadership practices on healthcare performance and staff well-being. Future research would explore the direct impact of these leadership styles on employee satisfaction and patient care quality.
Recommendations and Practical Implications
- Implement structured training programs tailored to the needs of primary healthcare managers, with a focus on transformational and situational leadership styles.
- Address identified gaps in emotional intelligence by incorporating training on stress management and interpersonal skills. Additionally, it foster collaborative leadership approaches that enhance teamwork across professions, including nurses, doctors, and directors.
- Develop a robust framework for the ongoing evaluation of leadership effectiveness, integrating key metrics such as employee satisfaction, patient outcomes, and team performance.
- Improving emotional intelligence would increase its broader significance as it can enhance team performance, employee retention, and patient outcomes.
- Conducting future research, including longitudinal studies and intervention-based training assessments, would further solidify the impact of emotional intelligence and leadership styles.
Conclusion
This study highlights the significance of emotional intelligence components, such as self-awareness, empathy, and social skills, as strengths among primary healthcare managers in Riyadh, Saudi Arabia. However, challenges in managing emotions and intrinsic motivation were identified as areas requiring targeted development. The findings emphasize that enhancing emotional intelligence is essential for fostering effective leadership within primary healthcare sittings. In alignment with Saudi Arabia’s Vision 2030, there is significant need for well-organized leadership programs. Such initiatives should focus on developing emotional intelligence and equipping managers with proficient skills to drive organizational success and improve outcomes. and fostering healthcare transformation.
Ethical Statement
Ethical approval of the study proposal was obtained from the institution Review Board (IRB) of Prince Sultan Military Medical City (PSMMC). A written informed consent was obtained to participate in the study. Anonymity and confidentiality were strictly maintained throughout the process to encourage honest and unbiased responses. We confirm that all research procedures comply with the declaration of Helsinki.
Author Contributions
All authors made a significant contribution to this research article whether in the conception and design of the idea for the article, acquisition, analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific funding.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Taylor R, Martindale S. Clinical leadership in primary care. Prim Health Care. 2013;23(5):32–37. doi:10.7748/phc2013.06.23.5.32.e795
2. Sellgren S, Ekvall G, Tomson G. Leadership styles in nursing management: preferred and perceived. J Nurs Manag. 2006;14(5):348–355. doi:10.1111/j.1365-2934.2006.00624.x
3. Eisenbeiss SA, van Knippenberg D, Boerner S. Transformational leadership and team innovation: integrating team climate principles. J Appl Psychol. 2008;93(6):1438–1446. doi:10.1037/a0012716
4. Alloubani A, Akhu-Zaheya L, Abdelhafiz IM, Almatari M. Leadership styles’ influence on the quality of nursing care. Int J Health Care Qual Assur. 2019;32(6):1022–1033. doi:10.1108/IJHCQA-06-2018-0138
5. Sfantou D, Laliotis A, Patelarou A, Sifaki- Pistolla D, Matalliotakis M, Patelarou E. Importance of leadership style towards quality of care measures in healthcare settings: a systematic review. Healthcare. 2017;5(4):73–89. doi:10.3390/healthcare5040073
6. Žibert A, Starc A. Healthcare organizations and decision-making: leadership style for growth and development. J Appl Health Sci. 2018;4(2):209–224. doi:10.24141/1/4/2/7
7. Mayo A. Forever change. Training J. 2002:40.
8. Quinn RE. Building the Bridge as You Walk on It. San Francisco: Jossey-Bass; 2004.
9. Kovač J, Muhlbacher J, Kodydek G. Uvod v management sprememb. Kranj: moderorganizacija v okviru Fakul- tete za organizacijske vede. 2012.
10. Lee V, Ridzi F, Lo AW, Coskun E. A healthcare case study of team learner style and change management. J Organ Change Manag. 2011;24(6):830–852. doi:10.1108/09534811111175788
11. Gilley A, McMillan HS, Gilley JW. Organizational change and characteristics of leadership effectiveness. JLOS. 2009;16(1):38–47. doi:10.1177/1548051809334191
12. Higgs MJ, Rowland D. Building change leadership capability: the quest for change competence. J Change Manage. 2000;1(2):116–130.
13. Wong CA, Cummings GG. The relationship between nursing leadership and patient outcomes: a systematic review. J Nurs Manage. 2007;15(5):508–521. doi:10.1111/j.1365-2834.2007.00723.x
14. Xenikou A. Transformational leadership, transactional contingent reward, and organizational identification: the mediating effect of perceived innovation and goal culture orientations. Front Psychol. 2017;8:1754. doi:10.3389/fpsyg.2017.01754
15. Abuhashesh M, Al-Dmour R, Masa’deh R. Factors that affect employees job satisfaction and performance to increase customers’ satisfactions. J Hum Resour Manag Res. 2019;2019. Article ID 354277. doi:10.5171/2019.354277
16. Schein EH, Schein PA. Organizational Culture and Leadership.
17. Asamani JA, Naab F, Ofei AMA, Addo R. Do leadership styles influence productivity? Br J Healthc Manag. 2016;22(2):83–91. doi:10.12968/bjhc.2016.22.2.83
18. Klemenc-Ketiš Z, Susič AP. Safety culture at primary healthcare level: a cross-sectional study among employees with a leadership role. Slovenian J Public Health. 2019;59(1):42–46. doi:10.2478/sjph-2020-0006
19. Alkassabi OY, Al-Sobayel H, Al-Eisa ES, Buragadda S, Alghadir AH, Iqbal A. Job satisfaction among physiotherapists in Saudi Arabia: does the leadership style matter? BMC Health Serv Res. 2018;18(1):422. doi:10.1186/s12913-018-3184-9
20. Kovačič H, Rus A. Leadership competences in Slovenian health care. Zdrav var. 2015;54(1):11–17. doi:10.1515/sjph-2015-0002
21. Greif S, Runde B, Seeberg I. Erfolgsfaktoren beim change management in acht Landern. Wirtschaftspsychologie aktuell. 2005;3(1):22–26.
22. Wanber CR, Banas JT. Predictors and outcomes of openness to changes in a reorganizing workplace. J Appl Psychol. 2000;85(1):132–142. doi:10.1037/0021-9010.85.1.132
23. Eby LT, Adams DM, Russell JEA, Gaby SH. Perceptions of organizational readiness for change: factors related to employees’ reactions to the implementation of team- based selling. Hum Relat. 2000;53(3):419–442. doi:10.1177/0018726700533006
24. Mintz LJ, Stoller JK. A systematic review of physician leadership and emotional intelligence. J Grad Med Educ. 2014;6(1):21–31. doi:10.4300/JGME-D-13-00012.1
25. Coskun O, Ulutas I, Budakoglu II, Ugurlu M, Ustu Y. Emotional intelligence and leadership traits among family physicians. Postgraduate Med. 2018;130(7):644–649. doi:10.1080/00325481.2018.1515563
26. Alanazi AH. Achieving Global Recognition: Higher Education Rankings and the Commitment to Quality in Saudi Arabia’s 2030 Strategic Vision [Doctoral dissertation]. University of Glasgow; 2024.
27. Killian KD. Development and validation of the emotional self‐awareness questionnaire: a measure of emotional intelligence. J Marital Fam Ther. 2012;38(3):502–514. doi:10.1111/j.1752-0606.2011.00233.x
28. Nightingale S, Spiby H, Sheen K, Slade P. The impact of emotional intelligence in health care professionals on caring behaviour towards patients in clinical and long-term care settings: findings from an integrative review. Int J Nurs Stud. 2018;80:106–117. doi:10.1016/j.ijnurstu.2018.01.006
29. Hamid S, Idrees T, Fatima S. Are our future doctors emotionally competent? Emotional intelligence of students at a Medical University in Pakistan; A cross-sectional study. Rawal Med J. 2022;47(3):707.
30. Awe AO, David-Olawade AC, Ayodele-Awe I, et al. Predictors and influencing factors of emotional intelligence among nurses in the North East England, United Kingdom. J Educ Health Promot. 2023;12(1):236. doi:10.4103/jehp.jehp_1656_22
31. Barrett L, Plotnikoff RC, Raine K, Anderson D. Development of measures of organizational leadership for health promotion. Health Educ Behav. 2005;32(2):195–207. doi:10.1177/1090198104271970
32. Sfantou DF, Laliotis A, Patelarou AE, Sifaki-Pistolla D, Matalliotakis M, Patelarou E. Importance of leadership style towards quality of care measures in healthcare settings: a systematic review. Healthcare. 2017;5(4):73. doi:10.3390/healthcare5040073
33. Younas A, Rasheed SP, Sundus A, Inayat S. Nurses’ perspectives of self-awareness in nursing practice: a descriptive qualitative study. Nurs Health Sci. 2020;22(2):398–405. doi:10.1111/nhs.12671
34. Solà GJ, Badia JG, Hito PD, Osaba MAC, Del Val García JL. Self-perception of leadership styles and behaviour in primary health care. BMC Health Serv Res. 2016;16:572. doi:10.1186/s12913-016-1819-2
35. Dorji K, Tejativaddhana P, Siripornpibul T, Cruickshank M, Briggs D. Leadership and management competencies required for Bhutanese primary health care managers in reforming the district health system. J Healthc Leadersh. 2019;11:13–21. doi:10.2147/JHL.S195751
36. Desta BF, Abitew A, Beshir IA, Argaw MD, Abdlkader S. Leadership, governance and management for improving district capacity and performance: the case of USAID transform: primary health care. BMC Fam Pract. 2020;21:252. doi:10.1186/s12875-020-01337-0
37. Alqahtani AMA, Nahar S, Almosa K, et al. Leadership styles and job satisfaction among healthcare providers in primary health care centers. World Fam Med. 2021;19(3):102–112. doi:10.5742/MEWFM.2021.94013
38. Sonnino RE. Health care leadership development and training: progress and pitfalls. J Healthc Leadersh. 2016;8:19–29. doi:10.2147/JHL.S68068
39. GOV. SA. Women empowerment. Available from: https://www.my.gov.sa/wps/portal/snp/careaboutyou/womenempowering/!ut/p/z0/04_Sj9CPykssy0xPLMnMz0vMAfIjo8zijQx93d0NDYz8LYIMLA0CQ4xCTZwN_Ay8TIz0g1Pz9AuyHRUBwQYLNQ!!/.
40. Page AEK. Transforming nurses’ work environments to improve patient safety: the institute of medicine recommendations. Policy Polit Nurs Pract. 2004;5:250–258. doi:10.1177/1527154404269574
41. Houser J. A model for evaluating the context of nursing care delivery. J Nurs Adm. 2003;33:39–47. doi:10.1097/00005110-200301000-00008
42. Tahir M, Amiruddin R, Palutturi S, Rivai F, Saleh LM. The relationship between organizing and leadership style and the quality improvement of primary healthcare services. Enfermería Clínica. 2020;3(S4):39–43. doi:10.1016/j.enfcli.2019.10.036
43. Franco M, Almeida J. Organisational learning and leadership styles in healthcare organisations an exploratory case study. Leadersh Organ Dev J. 2011;32(8):782–806. doi:10.1108/01437731111183739
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.