Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 8
Emerging utility of once-weekly exenatide in patients with type 2 diabetes
Authors Goud A, Zhong J, Rajagopalan S
Received 25 May 2015
Accepted for publication 29 August 2015
Published 21 October 2015 Volume 2015:8 Pages 505—512
DOI https://doi.org/10.2147/DMSO.S69354
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Aditya Goud, Jixin Zhong, Sanjay Rajagopalan
Division of Cardiovascular Medicine, Department of Medicine, University of Maryland, Baltimore, MD, USA
Abstract: Type 2 diabetes mellitus (T2DM) is a major risk factor for the development of cardiovascular disease (CVD). Due to the ever increasing incidence of both T2DM and CVD and coexistence of these disorders, numerous agents have been developed over the years to target complications. We focus on the efficacy and safety perspective of a long-acting formulation of the glucagon-like peptide-1 analog exenatide. Our review focuses on the various landmark trials, efficacy, safety profile, and patient perspectives of weekly exenatide that delineates its current and future role in the treatment of patients with T2DM and CVD.
Keywords: incretin, glucagon-like peptide, hyperglycemia, glucose lowering
Introduction
Type 2 diabetes mellitus (T2DM) and obesity are growing exponentially, with an estimated 29 million people affected in the USA alone with diabetes and an estimated 34% of the population considered obese.1,2 Incretin-based therapies have clearly revolutionized the management of T2DM as they address a key pathophysiological defect in this disorder. When used as monotherapy or in conjunction with other drugs in the treatment for T2DM, incretin-based therapies such as glucagon-like peptide-1 (GLP-1) receptor agonists or a dipeptidyl-peptidase-4 (DPP-4) inhibitor are effective agents in reducing glycated hemoglobin (HBA1c). GLP-1 receptor agonists additionally affect weight and blood pressure. In this review, the pharmacology, physiology, and clinical effects of a long-acting formulation of exenatide are reviewed and their effects on glycemia lowering weight loss and other cardiovascular effects discussed.
Review of pharmacology, mode of action, pharmacokinetics of extended release form of exenatide
GLP-1 and gastric inhibitory polypeptide are peptide hormones secreted by the enteroendocrine cells in the intestines. GLP-1 is synthesized by the L-cells present in the distal small gut, while gastric inhibitory polypeptide-1 is secreted by the proximal gut. GLP-1 stimulates insulin and inhibits glucagon secretion from the β- and α-cells, respectively, in a glucose-dependent manner. It also inhibits gastric emptying and reduces appetite, thus helping in weight reduction, especially in overweight individuals.3 Exenatide is a DPP-4 resistant form of GLP-1 that was originally identified in the Gila monster.4 Exenatide is a 39-amino acid peptide that shares 53% of its amino acid sequence identity with human GLP-1, and both have common glucoregulatory actions.5 Due to its pharmacological resemblance to native GLP-1, exenatide binds to and activates GLP-1 receptors, resulting in actions similar to native GLP-1 and reduces both fasting and prandial glucose levels.5 The pharmacokinetics of exenatide, although longer than native GLP-1, still requires twice-daily dosing. To overcome this short half-life, a long-acting depot formulation of exenatide was developed in 2003. This weekly exenatide preparation is encapsulated in 0.06 mm diameter microspheres of medical grade, biodegradable polymer, poly lactic-co-glycolic acid.6 When this formulation is injected subcutaneously, the microspheres degrade slowly, allowing gradual, controlled release of the drug into the systemic circulation over ~10 weeks. There is an initial period of release of surface-bound exenatide, followed by a gradual release of exenatide from the microspheres, resulting in two peaks of exenatide in plasma at around week 2 and weeks 6–7, respectively, representing the hydration and erosion of the microspheres.7
Exenatide 2 mg once weekly results in a minimal therapeutic concentrations (>50 pg/mL) in ~2 weeks and steady-state concentrations of ~300 pg/mL within 6–7 weeks.7 The median half-life of exenatide once weekly is ~2 weeks. After discontinuation, concentrations decrease to subtherapeutic levels (<50 pg/mL) in ~6–7 weeks.7 It is predominantly eliminated via glomerular filtration and has a mean apparent clearance of 9.1 L/h. Mean apparent volume of distribution is 28.3 L.
Efficacy studies
Although GLP-1-based therapy is currently not a first-line therapy for T2DM, it could be considered as an add-on therapy for patients who are poorly controlled on maximal doses of one or two oral agents.8 Exenatide once weekly has been shown to reduce A1c levels in patients with type 2 diabetes who are inadequately controlled with oral hypogylcemics and/or diet and exercise.9,10 Numerous trials have been performed comparing once-weekly exenatide to other antihyperglycemic drugs (Table 1). The six pivotal DURATION trials (The Diabetes Therapy Utilization: Researching Changes in A1c, Weight, and Other Factors Through Intervention With Exenatide Once Weekly) compare extended release exenatide to other antihyperglycemics. These trials generally had an inclusion criterion of HbA1c 7.1%–11% and body mass index of 24–40 kg/m2. Primary end point for these trials typically included change in A1c levels, whereas secondary end point is study dependent but included change in fasting blood glucose levels, change in body weight, and safety end points.
 | Table 1 The six pivotal studies comparing exenatide weekly to various comparators |
Glycemic effects
Versus exenatide daily
DURATION-1 and -5 were randomized control trials with open-label comparison of safety and efficacy profile of weekly versus 10 μg twice-daily exenatide use.
In DURATION-1, 295 patients with type 2 diabetes (HbA1c =8.3% [standard deviation {SD} =1.0], mean fasting plasma glucose [FPG] =9 [SD =2] mmol/L, weight =102 [SD =20] kg, diabetes duration =6.7 [SD =5.0] years) were assigned to either exenatide 2 mg administered weekly or 10 μg administered twice daily. At the end of the 30-week period, the exenatide weekly group had a significantly greater change in HbA1c than exenatide daily (−1.9 [standard error {SE} =0.1%] vs −1.5 [0.1%], 95% confidence interval [CI] =−0.54% to −0.12%, P=0.0023). Also a significant proportion of the patients receiving once-weekly exenatide achieved target HbA1c levels of 7.0% or less (77% vs 61% of evaluable patients, P=0.0039). Weekly exenatide resulted in significantly greater improvements in FPG (–41 mg/dL vs –25 mg/dL; P<0.0001), while improvements in prandial plasma glucose were greater with the twice-daily formulation (–124 mg/dL vs –95 mg/dL; P=0.0124). Reductions in body weight were similar in both treatment groups.11
In the DURATION-5 trial, weekly exenatide was compared against 5 μg exenatide twice daily for 4 weeks followed by 10 μg for 20 weeks. The study population included 252 type 2 diabetics (baseline [mean ± SD]: HbA1c 8.4%±1.2%, FPG 171±47 mg/dL, weight 96±20 kg) who were drug naïve (19%) or previously treated with one (47%) or multiple (35%) oral antidiabetic medications. Results were similar to that of DURATION-1 trial, with weekly exenatide producing significantly greater changes from baseline versus twice daily in HbA1c (−1.6%±0.1% vs −0.9%±0.1%; P<0.0001) and FPG (−35±5 mg/dL vs −12±5 mg/dL; P=0.0008) without any major hypoglycemic events.12 Weekly exenatide was associated with greater injection site reactions compared to twice-daily exenatide. Both DURATION-2 and -4 were associated with similar degree of weight loss effects with reduction in blood pressures that were comparable.
Versus oral hypoglycemic drugs
DURATION-2 trial compared once-weekly exenatide with maximum approved doses of sitagliptin or pioglitazone in patients treated with metformin monotherapy. Exenatide reduced HbA1c (mean difference =−1.5%, 95% CI =−1.7 to −1.4) significantly more than sitagliptin (mean difference =−0.9%, 95% CI =−1.1 to −0.7) or pioglitazone (mean difference =−1.2%, 95% CI =−1.4 to −1.0). Weight loss with exenatide (difference =−2.3 kg, 95% CI =−2.9 to −1.7) was significantly greater than that achieved with sitagliptin (difference =−1.5 kg, 95% CI =−2.4 to −0.7, P=0.0002) or pioglitazone (difference =−5.1 kg, 95% CI =−5.9 to −4.3). However, reductions in FPG with exenatide once weekly (−32 mg/dL) was significantly greater than those achieved with sitagliptin (–16 mg/dL; P=0.0038 vs exenatide), but not pioglitazone (–27 mg/dL; P=0.3729 vs exenatide). Thus, addition of weekly exenatide to metformin achieved better glucose control than did addition of maximum daily doses of either sitagliptin or pioglitazone.13 Weekly exenatide was associated with weight loss compared to weight gain in the pioglitazone arm.
DURATION-4 was a randomized, controlled, double-blind 26-week study that compared efficacy and safety of exenatide once weekly, metformin 2,500 mg/d, pioglitazone 45 mg/d, or sitagliptin 100 mg/d as initial monotherapy in 820 patients with uncontrolled type 2 diabetes. HbA1c reductions (%) at 26 weeks with once-weekly exenatide versus metformin, pioglitazone, and sitagliptin were −1.53 vs −1.48 (P=0.620), −1.63 (P=0.328), and −1.15 (P<0.001), respectively. Weight changes (kg) were −2.0 with weekly exenatide, −2.0 with metformin (P=0.892 vs intervention [weekly exenatide]), +1.5 (P<0.001) with pioglitazone, and −0.8 kg with sitagliptin (P<0.001). Thus, both exenatide once weekly and metformin resulted in a similar mean weight loss of 2 kg. Treatment with pioglitazone resulted in weight gain. Reductions in FPG with exenatide once weekly (−40.5 mg/dL) were similar to those with metformin (−35.7 mg/dL) and pioglitazone (−46.3 mg/dL) and significantly greater than that with sitagliptin (−20.4 mg/dL; P<0.001). All results were reported for the intent-to-treat population.14
Versus insulin
In the recently completed DURATION-3 trial, a multinational open-label randomized trial, exenatide once weekly was compared with insulin glargine in patients suboptimally controlled with metformin monotherapy or metformin and sulfonylurea combination therapy for at least 3 months. Insulin glargine was initiated at 10 U/day and titrated up according to FPG. At 3 years, HbA1c change was −1.01% (SE =0.07) in the exenatide group versus −0.81% (0.07) in the glargine group (least-squares mean difference =−0.20%, SE =0.10, 95% CI =−0.39 to −0.02, P=0.03).15
Versus other GLP-1R agonist
DURATION-6, a 26-week, open-label, randomized, parallel-group study, compared exenatide once weekly to liraglutide 1.8 mg daily as add-on therapy to metformin, a sulfonylurea, and/or pioglitazone in 911 patients with uncontrolled type 2 diabetes. Preliminary results indicated that mean change in HbA1c was greater in patients in the liraglutide group (−1.48%, SE =0.05; n=386) than in those in the exenatide group (−1.28%, SE =0.05; n=390) with the treatment difference (0.21%, 95% CI =0.08–0.33) not meeting the prespecified noninferiority criteria. Liraglutide-treated patients lost significantly more weight and a greater proportion achieved an HbA1c <7%.
Thus, based on the aforementioned trials, exenatide extended-release has shown to effectively reduce glucose levels as well as helps in weight loss. These results are persistent >2 years as demonstrated in the continuation phase of DURATION trials, which showed that after 2 years, HbA1c and fasting blood glucose showed a mean reduction of −1.7% and −40.1 mg/dL, respectively.16,17
Nonglycemic effects
Exenatide once weekly has well-documented evidence to support improvement of glycemic parameters. However, it has also been shown to have some benefit in improving other cardiovascular risk factors apart from blood glucose, such as blood pressure, lipids, and body weight.
Weekly exenatide for 30 weeks reduced apolipoprotein B and the apolipoprotein B to apolipoprotein A1 ratio (P<0.05), independent of glycemic improvement and weight loss.18 Patients with abnormal baseline (LDL ≥100 mg, HDL ≤40/50 mg/dL [male/female], or triglyceride ≥150 mg/dL) showed greater improvements in all lipid parameters (LDL, mean: −12.7 [SE =1.61] mg/dL, P<0.0001; HDL: 2.5 [SE =0.34] mg/dL, P<0.0001; triglycerides: −21% [SE =1.9], P<0.0001) in contrast to the moderate improvements in all patients receiving exenatide weekly.19
In meta-analysis, GLP-1Ra have been shown to reduce systolic blood pressure (SBP) by −1.79 mmHg (95% CI =−2.94 to −0.64) compared to placebo and by −2.39 mmHg (95% CI =−3.35 to −1.42) compared to active control. Reductions in diastolic blood pressure (DBP) failed to reach statistical significance and were −0.54 mmHg (−1.15 to 0.07) compared to placebo and −0.50 mmHg (−1.24 to 0.24) compared to active control.20 Consistent with these observations, clinically significant reductions in blood pressure were observed at week 52 (SBP: −3.6 [0.56] mmHg, P<0.0001; DBP: −1.2 [0.34] mmHg P<0.001) with weekly exenatide. Greater improvements were observed in patients with elevated baseline SBP (≥130 mmHg): SBP: −8.5 (0.85) mmHg, P<0.0001; DBP: −3.0 (0.50) mmHg, P<0.0001, or elevated baseline SBP and DBP (≥130/80 mmHg): SBP: −8.9 (1.10) mmHg, P<0.0001, DBP: −5.0 (0.58) mmHg, P<0.0001.19 A large meta-analysis showed that weekly exenatide as well as its daily preparation achieved a significant reduction in SBP compared to comparator therapy that included placebo and other hypoglycemic drugs (weighted mean difference =2.22 mmHg; 95% CI =−2.97 to −1.47).21 Meta-analysis using a random-effect model showed that GLP-1 agonists produce a significant increase in heart rate with a weighted mean difference of 1.86 bpm (95% CI =0.85–2.87) versus placebo and 1.90 bpm (95% CI =1.30–2.50) versus active control, whereas weekly exenatide produced a more significant change 2.14 bpm (95% CI =1.11–3.17) versus active control.20 GLP-1 therapy is associated with a loss in weight of −2.56 kg (95% CI =−3.12 to −2.00; n=7,258 active treatment and n=5,492 in comparator).21 A post hoc analysis pooled data from patients taking weekly exenatide showed reductions from baseline (least-squares mean [95% CI]) in body weight (−2.5 kg [−2.8 kg to −2.3 kg]) after 24–30 weeks of treatment.22 However, no significant difference in weight loss was seen between the different types of GLP-1 agonists.23 Thus, a small but significant reduction in body weight is seen with all GLP-1 therapy.
Safety and tolerability
Hypoglycemia associated with many antidiabetic medications is a significant side effect that limits the use of agents such as sulfonylureas and insulin. GLP-1-based therapies are associated with minimal risk of hypoglycemia. In trials used on top of metformin, there is minimal increase in hypoglycemia.9 In contrast, use of concomitant sulfonylurea or insulin does increase the risk of hypoglycemia, particularly in older individuals.11,12
The commonest adverse effect reported in all clinical trials with GLP-1 receptor agonists are gastro-intestinal, mainly nausea that is likely related to the gastric-slowing effects. However, these mild side effects improve with persistent use beyond 8 weeks. Other notable side effects are injection site reactions. Over all withdrawal rates in DURATION trials ranged from approximately 10% to 25%, but discontinuation rates due to adverse events were low. In contrast to exenatide twice daily, exenatide weekly appears to have a lower incidence of side effects. In DURATION-1, exenatide weekly was associated with a lower incidence of nausea compared to exenatide twice daily (26% vs 35%, respectively). Furthermore, patients on exenatide weekly had a lower incidence of vomiting (11% vs 19%). The hypoglycemia incidence of exenatide weekly was lower compared to insulin treatment (8% vs 26%), although the discontinuation rate due to adverse events was higher (9.0% vs 2.0%) in DURATION-3 trial. The discontinuation rates due to adverse events were similar to exenatide twice daily (DURATION-5), metformin (DURATION-4), and pioglitazone (DURATION-4), but higher than DPP4 inhibitor sitagliptin (DURATION-2 and -4) (Table 2).
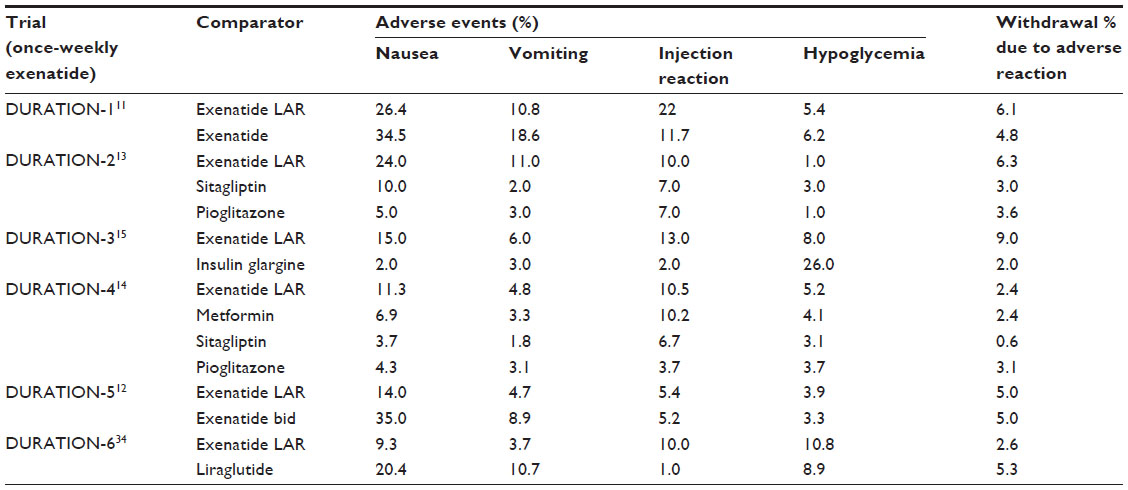 | Table 2 Adverse events and withdrawal rates |
Use in the presence of renal dysfunction
Exenatide is mainly excreted by glomerular filtration followed by proteolytic degradation.24 A warning issued by the Food and Drug Administration states that it should not be used in patients with severe renal impairment (creatinine clearance <30 mL/min) or end-stage renal disease. For patients with mild-to-moderate renal impairment (creatinine clearance 30–50 mL/min), down-titration of concomitant medications, in particular, sulfonylureas, may become necessary to manage hypoglycemia and other adverse effects since the injector apparatus for weekly exenatide comes prepackaged with a single, fixed amount of drug for subcutaneous administration and decreasing its dosage may not be an option. In patients with end-stage renal disease on hemodialysis, exenatide has been shown to be poorly tolerated,25 because in the absence of adequate renal clearance, the drug may accumulate and further worsen renal function by inducing hypovolemia due to the nausea and vomiting. A causal relationship was raised between worsening kidney function and exenatide in recent case reports. However, a meta-analysis examining six randomized trials (16–30 weeks) comparing daily exenatide, weekly exenatide, and placebo showed no overall difference in the decline of glomerular filtration rates between the comparators.26,27 Thus, a claim of a causal link between exenatide use and worsening kidney function remains unsupported.
Patient perspectives such as quality of life, satisfaction, preference, adherence
Treatment burden and adverse effects can have an appreciable negative impact on patients’ quality of life (QOL) with prior studies showing that interventions with a high treatment burden for treating glucose (glycemic disutility) may substantially attenuate benefit as measured by quality-adjusted life-years.28 Health economic analyses into the cost-effectiveness of both GLP-1Ra and DPP-4i have suggested that while both GLP-1Ra and DPP-4i may incur a significant cost to health care systems, their improved side-effect profiles resulting in improved QOL when compared to conventional therapies such as sulfonylureas may be substantial. For instance, relative to glyburide as second-line therapy, the use of incretin agents is associated with an additional 0.09–0.12 quality-adjusted life-years per patient, a result comparable to benefits accrued by a number of highly effective preventive and treatment strategies.29 A randomized, double-blind, double-dummy, multicenter clinical trial was conducted with 514 patients and was designed to assess the clinical outcomes, patient-reported outcomes, and safety of 26 weeks of treatment with exenatide weekly compared with maximum approved doses of sitagliptin or pioglitazone in patients with T2DM.30 Weekly exenatide showed improvements in HbA1c, weight, and fasting glucose levels with negligible risk of hypoglycemia. At the end of 26 weeks, patients completed self-reported measurements on QOL, the impact of weight on QOL-lite;31 health utility, the EuroQol five dimensions measure,31,32 psychological well-being, the psychological general well-being index,32 and diabetes treatment satisfaction, the Diabetes Treatment Satisfaction Questionnaire status version. The exenatide weekly group experienced significantly greater improvement than the pioglitazone group in total weight-related QOL and resulted in significantly greater improvement in public distress, physical function, and work. There were no statistically significant differences between the exenatide weekly and sitagliptin groups in total weight-related QOL. The EuroQol five-dimension measure, a generic measure that provides a single index value that can be used in clinical and economic evaluation of health outcomes, showed significant improvement in the exenatide weekly and sitagliptin treatment group (all P<0.05), but not in the pioglitazone group.31 Although all components of the Diabetes Treatment Satisfaction Questionnaire status version and psychological general well-being index improved at the end of treatment, there were no statistically significant differences between the three groups. Several studies suggest that greater treatment satisfaction is associated with greater treatment adherence.33,34 However, no studies have been done so far to discern whether this added convenience translates into higher treatment compliance.
Conclusion
The current role of GLP-1 receptor agonists such as weekly exenatide is as an adjunct therapy to other antihyperglycemic treatment along with diet and exercise. Exenatide weekly is an attractive option in many patients, as the convenience of dosing together with evidence suggesting superiority in terms of glycemia lowering and better gastrointestinal (GI) side-effect profile argues for its preferential use compared to twice-daily exenatide. The risk of injection site reactions is higher compared to twice-daily therapy. The risk of hypoglycemia is generally low with preparation, with no evidence suggesting enhanced weight loss. The cardiovascular benefits of once-weekly exenatide are currently being tested as part of a large multinational randomized controlled clinical trial. The Exenatide Study of Cardiovascular Event Lowering Trial: A Randomized, Placebo-Controlled Clinical Trial to Evaluate Cardiovascular Outcomes after Treatment with ExQW in Patients with T2DM (EXSCEL, NCT01144338) will test major adverse cardiovascular outcomes including heart failure in 9,500 patients and is expected to announce the outcomes in April 2018. Due to its pharmacokinetics and renal excretion, it is best avoided in patients with creatinine clearance <30 mL/min. Health economic analyses into the cost-effectiveness of both GLP-1Ra have suggested that while GLP-1Ra may incur a significant cost to health care systems, their improved side-effect profile and reduced treatment burden compared to conventional therapies such as insulin and sulfonylureas may be attractive to patients with T2DM.
Acknowledgment
This work was supported by grants from NIH (K01 DK105108), AHA (15SDG25700381 and 13POST17210033), and Mid-Atlantic Nutrition Obesity Research Center (NORC Pilot and Feasibility Program) to JZ.
Disclosure
The authors report no conflicts of interest in this work.
References
2014 Statistics Report Data and Statistics Diabetes CDC. 2014. Available from: http://www.cdc.gov/diabetes/data/statistics/2014StatisticsReport.html. Accessed December 31, 2014. | |
Centers for Disease Control and Prevention. About NCHS. NCHS Fact Sheets – NCHS Data on Obesity; 2014 [updated June 4, 2014]. Available from: http://www.cdc.gov/nchs/data/factsheets/factsheet_obesity.htm. Accessed October 5, 2015. | |
Drucker DJ. Enhancing incretin action for the treatment of type 2 diabetes. Diabetes Care. 2003;26(10):2929–2940. | |
Furman BL. The development of Byetta (exenatide) from the venom of the Gila monster as an anti-diabetic agent. Toxicon. 2012;59(4):464–471. | |
Seewoodhary J, Griffin L, Bain SC. Critical appraisal of once-weekly formulation of exenatide in the control of type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2010;3:165–172. | |
DeYoung MB, MacConell L, Sarin V, Trautmann M, Herbert P. Encapsulation of exenatide in poly-(D,L-lactide-co-glycolide) microspheres produced an investigational long-acting once-weekly formulation for type 2 diabetes. Diabetes Technol Ther. 2011;13(11):1145–1154. | |
Fineman M, Flanagan S, Taylor K, et al. Pharmacokinetics and pharmacodynamics of exenatide extended-release after single and multiple dosing. Clin Pharmacokinet. 2011;50(1):65–74. | |
American Diabetes Association. Standards of medical care in diabetes – 2015: summary of revisions. Diabetes Care. 2014;38(Suppl_1):S4–S4. | |
Diamant M, Van Gaal L, Stranks S, et al. Once weekly exenatide compared with insulin glargine titrated to target in patients with type 2 diabetes (DURATION-3): an open-label randomised trial. Lancet. 2010;375(9733):2234–2243. | |
Kim D, MacConell L, Zhuang D, et al. Effects of once-weekly dosing of a long-acting release formulation of exenatide on glucose control and body weight in subjects with type 2 diabetes. Diabetes Care. 2007;30(6):1487–1493. | |
Drucker DJ, Buse JB, Taylor K, et al; DURATION-1 Study Group. Exenatide once weekly versus twice daily for the treatment of type 2 diabetes: a randomised, open-label, non-inferiority study. Lancet. 2008; 372(9645):1240–1250. | |
Blevins T, Pullman J, Malloy J, et al. DURATION-5: exenatide once weekly resulted in greater improvements in glycemic control compared with exenatide twice daily in patients with type 2 diabetes. J Clin Endocrinol Metab. 2011;96(5):1301–1310. | |
Bergenstal RM, Wysham C, Macconell L, et al; DURATION-2 Study Group. Efficacy and safety of exenatide once weekly versus sitagliptin or pioglitazone as an adjunct to metformin for treatment of type 2 diabetes (DURATION-2): a randomised trial. Lancet. 2010;376(9739):431–439. | |
Russell-Jones D, Cuddihy RM, Hanefeld M, et al; DURATION-4 Study Group. Efficacy and safety of exenatide once weekly versus metformin, pioglitazone, and sitagliptin used as monotherapy in drug-naive patients with type 2 diabetes (DURATION-4): a 26-week double-blind study. Diabetes Care. 2012;35(2):252–258. | |
Diamant M, Van Gaal L, Guerci B, et al. Exenatide once weekly versus insulin glargine for type 2 diabetes (DURATION-3): 3-year results of an open-label randomised trial. Lancet Diabetes Endocrinol. 2014;2(6):464–473. | |
Taylor K, Gurney K, Han J, Pencek R, Walsh B, Trautmann M. Exenatide once weekly treatment maintained improvements in glycemic control and weight loss over 2 years. BMC Endocr Disord. 2011;11:9. | |
Diamant M, Van Gaal L, Stranks S, et al. Safety and efficacy of once-weekly exenatide compared with insulin glargine titrated to target in patients with type 2 diabetes over 84 weeks. Diabetes Care. 2012;35(4):683–689. | |
Chiquette E, Toth PP, Ramirez G, Cobble M, Chilton R. Treatment with exenatide once weekly or twice daily for 30 weeks is associated with changes in several cardiovascular risk markers. Vasc Health Risk Manag. 2012;8:621–629. | |
Bergenstal RM, Li Y, Porter TKB, Weaver C, Han J. Exenatide once weekly improved glycaemic control, cardiometabolic risk factors and a composite index of an HbA1c <7%, without weight gain or hypoglycaemia, over 52 weeks. Diabetes Obes Metab. 2013;15(3):264–271. | |
Robinson LE, Holt TA, Rees K, Randeva HS, O’Hare JP. Effects of exenatide and liraglutide on heart rate, blood pressure and body weight: systematic review and meta-analysis. BMJ Open. 2013;3(1):e001986. | |
Katout M, Zhu H, Rutsky J, et al. Effect of GLP-1 mimetics on blood pressure and relationship to weight loss and glycemia lowering: results of a systematic meta-analysis and meta-regression. Am J Hypertens. 2013;27(1):130–139. | |
Grimm M, Han J, Weaver C, et al. Efficacy, safety, and tolerability of exenatide once weekly in patients with type 2 diabetes mellitus: an integrated analysis of the DURATION trials. Postgrad Med. 2013;125(3):47–57. | |
Potts JE, Gray LJ, Brady EM, Khunti K, Davies MJ, Bodicoat DH. The effect of glucagon-like peptide 1 receptor agonists on weight loss in type 2 diabetes: a systematic review and mixed treatment comparison meta-analysis. PLoS One. 2015;10(6):e0126769. | |
Yoo BK, Triller DM, Yoo DJ. Exenatide: a new option for the treatment of type 2 diabetes. Ann Pharmacother. 2006;40(10):1777–1784. | |
Barnett AH, Burger J, Johns D, et al. Tolerability and efficacy of exenatide and titrated insulin glargine in adult patients with type 2 diabetes previously uncontrolled with metformin or a sulfonylurea: a multinational, randomized, open-label, two-period, crossover noninferiority trial. Clin Ther. 2007;29(11):2333–2348. | |
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2014;38(1):140–149. | |
Tuttle KR, Heilmann C, Hoogwerf BJ, Brown C, Anderson PW. Effects of exenatide on kidney function, adverse events, and clinical end points of kidney disease in type 2 diabetes. Am J Kidney Dis. 2013;62(2):396–398. | |
Vijan S, Sussman JB, Yudkin JS, Hayward RA. Effect of patients’ risks and preferences on health gains with plasma glucose level lowering in type 2 diabetes mellitus. JAMA Intern Med. 2014;174(8):1227–1234. | |
Sinha A, Rajan M, Hoerger T, Pogach L. Costs and consequences associated with newer medications for glycemic control in type 2 diabetes. Diabetes Care. 2010;33(4):695–700. | |
Best JH, Rubin RR, Peyrot M, et al. Weight-related quality of life, health utility, psychological well-being, and satisfaction with exenatide once weekly compared with sitagliptin or pioglitazone after 26 weeks of treatment. Diabetes Care. 2011;34(2):314–319. | |
Clarke P, Gray A, Holman R. Estimating utility values for health states of type 2 diabetic patients using the EQ-5D (UKPDS 62). Med Decis Making. 2002;22(4):340–349. | |
Matza LS, Boye KS, Yurgin N. Validation of two generic patient-reported outcome measures in patients with type 2 diabetes. Health Qual Life Outcomes. 2007;5:47. | |
Charpentier G, Fleury F, Dubroca I, Vaur L, Clerson P. Electronic pill-boxes in the evaluation of oral hypoglycemic agent compliance. Diabetes Metab. 2005;31(2):189–195. | |
Pollack MF, Purayidathil FW, Bolge SC, Williams SA. Patient-reported tolerability issues with oral antidiabetic agents: associations with adherence; treatment satisfaction and health-related quality of life. Diabetes Res Clin Pract. 2010;87(2):204–210. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.