Back to Journals » Cancer Management and Research » Volume 12
Emerging Treatment Options for the Treatment of Metastatic Urothelial Cancer: Therapeutic Potential of Enfortumab Vedotin
Authors Jain RK, Skelton WP IV ![]() , Zhang J
, Zhang J ![]()
Received 28 May 2020
Accepted for publication 4 August 2020
Published 11 September 2020 Volume 2020:12 Pages 8379—8386
DOI https://doi.org/10.2147/CMAR.S224223
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Rohit K Jain, William Paul Skelton IV, Jingsong Zhang
Department of Genitourinary Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA
Correspondence: Jingsong Zhang
Department of Genitourinary Oncology, H. Lee Moffitt Cancer Center and Research Institute, 12902 USF Magnolia Drive, Tampa, FL 33612, USA
Email [email protected]
Abstract: Enfortumab vedotin (EV) is an antibody–drug conjugate with humanized anti-Nectin-4 antibody linked with a microtubule-disrupting agent called monomethyl auristatin E. Nectin-4 is a cellular adhesion protein that is overexpressed in urothelial cancer. EV was approved in December 2019 for patients with locally advanced or metastatic urothelial cancer who previously received platinum-based chemotherapy and immune checkpoint inhibitors. Here, we reviewed the clinical efficacy and safety data that led to the accelerated approval of EV for treating patients with metastatic urothelial cancer. Emerging clinical data on EV-based combinational therapeutic trials for metastatic urothelial cancer were also reviewed.
Keywords: enfortumab vedotin, urothelial cancer, antibody-drug conjugate
Introduction
Urothelial cancer (UC) is the sixth most common cancer in the United States and the ninth most common cancer in the world.1 Most patients are diagnosed after presenting with hematuria, which is often painless and intermittent. Approximately 30% of patients with UC present with muscle-invasive disease, which has a high risk for metastasis. Recurrent non–muscle-invasive bladder cancers often progress to the muscle-invasive stage after the cancers become refractory to intravesical therapies. Despite the approval of anti–programmed cell death 1 (PD-1) and anti–programmed cell death ligand 1 (PD-L1) therapies for metastatic urothelial cancer (mUC), a recent review of the Global Cancer Incidence, Mortality and Prevalence data reported a dismal 5% five-year survival rate for patients with this disease.2 There is an unmet need to develop more effective therapies for mUC patients.
The standard frontline therapy for patients with mUC is cisplatin-based chemotherapy with either gemcitabine/cisplatin or dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin (dd-MVAC).3 For patients with mUC who have impaired renal function, hearing loss, severe neuropathy, or poor performance status, cisplatin is not an option. These cisplatin-ineligible patients can be treated with either a carboplatin-based regimen or immune checkpoint inhibitors (ICIs) with either atezolizumab or pembrolizumab if their disease is PD-L1+ on immunohistochemistry.3 In the second-line setting, 5 ICIs are currently approved to treat mUC after progression through platinum-based chemotherapy: pembrolizumab, nivolumab, atezolizumab, durvalumab, and avelumab. Among these ICIs, pembrolizumab is the only one with proven overall survival (OS) benefit when compared to second-line chemotherapy in randomized phase 3 trials.4,5 Until the recently accelerated approval of enfortumab vedotin (EV), there were a lack of effective treatments for mUC progression following treatment with platinum-based chemotherapy and ICIs.
EV is a humanized Nectin-4–targeting antibody–drug conjugate (ADC) with a microtubule inhibitor payload called monomethyl auristatin E (MMAE). It was co-developed by Seattle Genetics and Astellas Pharma Inc. Here, we reviewed the mechanism of action, clinical efficacy, and safety data on EV in treating mUC. Ongoing clinical trials with EV-based combination therapies were also reviewed.
Mechanisms of Action of EV
Nectin-4 is an adhesion molecule that belongs to the Nectin family. It is a 66KDa type I transmembrane protein and has an extracellular domain, which includes 3 Ig-like subdomains, a transmembrane helix, and an intracellular region.6 Nectin-4 is normally expressed at low levels in skin cells, sweat glands, hair follicles, transitional epithelium of the bladder, salivary gland ducts, as well as the esophagus, breast ducts, and stomach.7 It is involved in cell growth, proliferation, and migration by creating hemophilic and heterophilic trans-interactions at adherent junctions, which facilitate Ca2+-independent cellular adhesions and recruit cadherins with cytoskeletal rearrangements.8 Nectin-4 only shares 25% to 30% sequence with the other Nectin family members. It is considered to be a unique target.9 Challita-Eid et al examined nectin-4 expression via immunohistochemical staining in bladder, breast, pancreatic, lung, ovarian, esophageal, and head/neck cancers.7 Positive Nectin-4 membrane staining was identified in 69% of the 2394 total cases examined.7 Forty-one percent of cases had strong nectin-4 staining, which is defined as an H-score (Histochemical scoring system) >200. The malignancies with the highest expression of nectin-4 were bladder cancer (83%), breast cancer (78%), and pancreatic cancer (71%). Expression of nectin-4 in these cancers was also associated with poor prognosis.7,10 Of note, 60% of the 524 bladder cancer cases had moderate to strong membrane staining for nectin-4. The expression of nectin-4 is noted to be limited in normal tissues. These data constituted the basis for the development of an ADC targeting Nectin-4.
EV is an ADC made of a fully human anti–Nectin-4 immunoglobulin G1 kappa monoclonal antibody (AGS-22CE). It is linked to a small microtubule-disrupting agent, MMAE, via a protease cleavable maleimidocaproyl valine-citrulline linker.11 The conjugation between the antibody and MMAE occurs through the interchain disulfide bonds, yielding a drug to antibody ratio of approximately 3.8. EV binds to the V domain of Nectin-4 protein. Once bound to Nectin-4 protein on the cell surface, it internalizes into the cell. Proteolytic cleavage of the valine-citrulline linker occurs in the lysosome. The released free MMAE subsequently binds to the tubules and disrupts the polymerization, leading to cell cycle arrest and apoptosis.
When tested in the mouse xenograft models of human bladder, breast, lung, and pancreatic cancers, EV caused tumor regression in 5/13 mouse models (38%) and significant inhibition of tumor growth in 12/13 models (92%).7 A single dose of EV at 4 mg/kg resulted in the complete eradication of mouse bladder cancer xenografts in 5/6 mice (83%). An alternate dosing strategy of 0.8 mg/kg every 4 days for a total of 5 doses (total of 4 mg/kg) resulted in significant inhibition of tumor growth when compared with control (P <.0001). EV administered at a lower dose of 0.4 mg/kg did not result in antitumor activity when compared with controls (P >.05). These mouse xenograft data demonstrated a dose-dependent antitumor effect of EV and constituted the basis for EV testing in early phase human clinical trials.
Clinical Studies
EV-101 (ASG-22CE-13-2) was a phase 1 trial of EV in mUC and other solid tumors that expressed nectin-4.11 The study’s primary endpoints were to assess pharmacokinetics and safety, and secondary endpoints included tumor response, overall response rate (ORR), progression free survival (PFS), and OS. Patients with mUC who experienced treatment failure with at least 1 prior chemotherapy regimen, unless deemed ineligible for cisplatin, were enrolled. Initially, patients were prescreened for nectin-4 overexpression via immunohistochemistry (H-score ≥150). This requirement was waived in the later part of the trial for the mUC cohort because >80% of tested mUC samples had nectin-4 overexpression.
In the dose-escalation phase, EV was studied at doses of 0.5, 0.75, 1, and 1.25 mg/kg administered intravenously on days 1, 8, and 15 of a 28-day cycle.11 The preliminary results of the pharmacokinetic profile suggested activity and tolerability at the maximum tolerated dose (recommended phase 2 dose) of 1.25 mg/kg. At the time of interim analysis, a 30% ORR was observed. Of note, the response rate among patients with liver metastasis was 40%.
One hundred twelve mUC patients were subsequently enrolled in the dose-expansion phase and treated with EV at a dose of 1.25 mg/kg. The enrolled patients were heavily pretreated with platinum- and taxane-based chemotherapy, and 89 patients also received ICIs. The ORR was 43%, with 5 subjects (4.5%) achieving complete remission (CR), and the median duration of response (DOR) was 7.4 months (95% CI, 5.6–9.6). Median OS was 12.3 months (95% CI, 9.3–15.3). An ORR of 42% and 36% was observed in patients with prior ICI exposure and liver metastases, respectively. The most common treatment-related adverse events (TRAEs) of any grade were fatigue (53%), alopecia (46%), and anorexia (42%). The incidence of ≥ grade 3 TRAEs was seen in ≥5% of patients; these included anemia (8%), hyperglycemia (6%), hyponatremia (7%), and urinary tract infection (7%) (Table 1). Four fatal TRAEs were also reported, which included respiratory failure, urinary tract obstruction, diabetic ketoacidosis, and multi-organ failure. These data indicate that single-agent EV is active and tolerable and confers survival benefit in patients with mUC, including those with liver metastases. Study results on the cohorts of non-small cell lung cancer, ovarian cancer, and mUC patients with chronic renal insufficiency are pending.
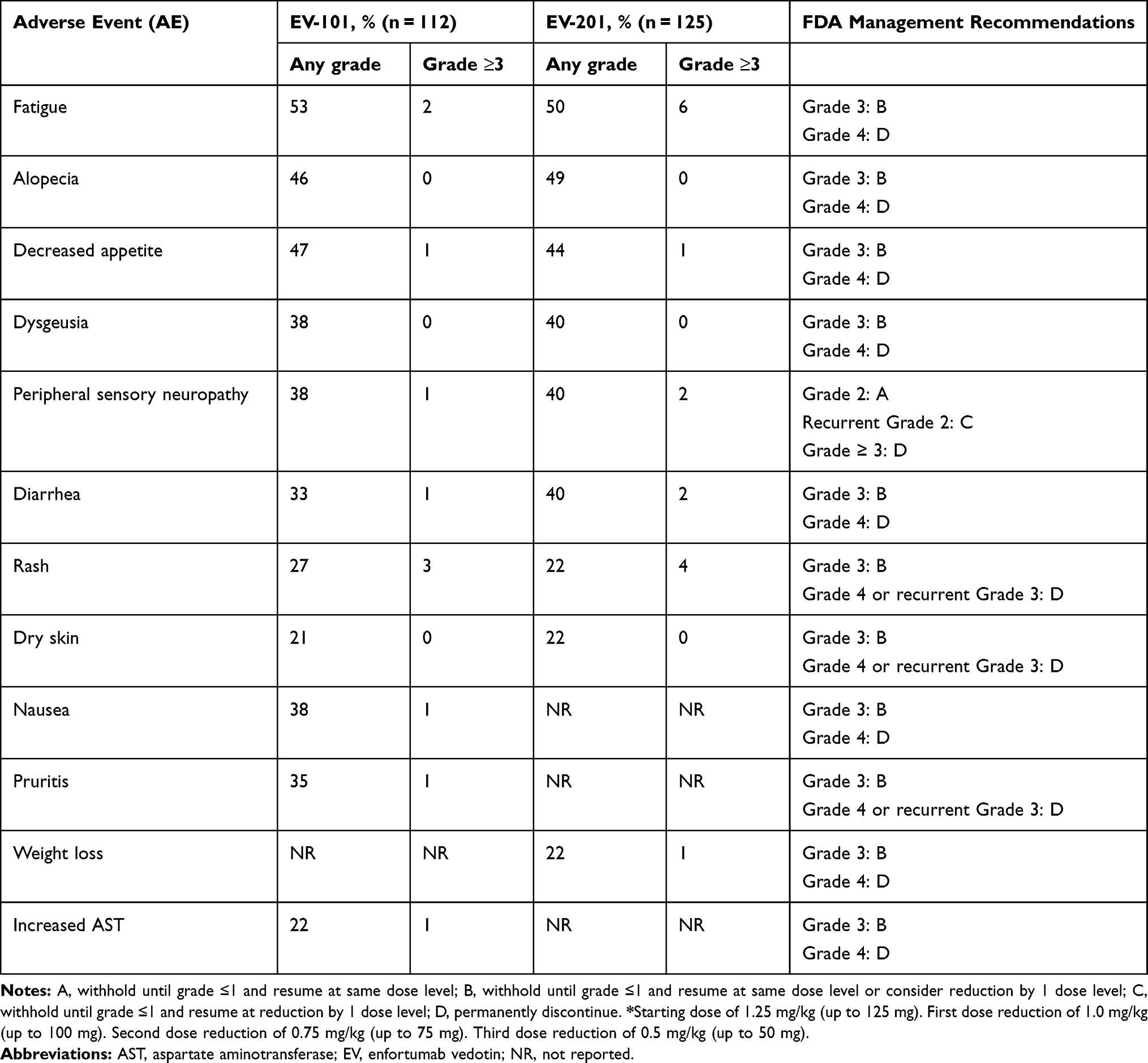 |
Table 1 Treatment-Related Adverse Events of Enfortumab Vedotin Monotherapy When Administered at a Dose of 1.25 mg/kg* |
Takahashi et al conducted a phase 1 study (NCT03070990) examining EV administered to Japanese patients with locally advanced or mUC.12 Enrolled patients had experienced treatment failure with at least 1 prior chemotherapy regimen (unless they were unfit for cisplatin) and had an ECOG performance status of 0 or 1. The study had 2 arms that compared different dosing regimens and enrolled a total of 19 patients, 17 of whom received EV. Patients assigned to arm A received 1.0 mg/kg of EV given over 30 minutes on days 1, 8, and 15 of each 28-day cycle; patients assigned to arm B received 1.25 mg/kg of EV at the same dosing schedule, which was based on findings from the EV-101 study.11 Among 15 evaluable patients, 1 achieved CR (6%), 5 partial remission (PR) (29%), 7 stable disease (41%), and 2 progressive disease (PD). The ORR was 35.3% (44% in arm A and 25% in arm B), and the disease control rate (DCR) was 76% (100% in arm A and 50% in arm B). At the time of publication of the study, the durations of response ranged from 3.7 to 9.3 months. The median PFS was 8.1 months (95% CI, 3.5-not reached). The most common TRAEs were dysgeusia (53%), alopecia (53%), dry skin (47%), pruritus (47%), anemia (41%), decreased appetite (41%), and pyrexia (35%). Fifty-nine percent of patients developed ≥ grade 3 TRAEs, with the most common being anemia (18%) and hypertension (12%). Three patients withdrew from the study due to TRAEs, 2 in arm A (1 due to peripheral sensory neuropathy and the other transaminitis) and 1 in arm B (the patient experienced pneumonia and rash). No patients died due to treatment-related side effects; however, 1 patient died 14 days after the last dose due to disease progression. In the Japanese patient population, the pharmacokinetic profile, treatment responses, and side effects of EV were similar to those in the North American cohort in EV-101.
EV-201 (SGN22E-001) was an open-label, single-arm, 2-cohort, phase 2 study assessing the efficacy and safety of EV at a dose of 1.25 mg/kg on days 1, 8, and 15 of a 28-day cycle in advanced mUC patients previously treated with platinum-based chemotherapy and ICIs.13 Cohort 1 included 128 patients who progressed on both platinum-based chemotherapy and ICI; cohort 2 enrolled patients who only received prior ICI. The primary endpoint was the evaluation of ORR by blinded independent central review (BICR), and secondary endpoints included PFS, OS, and ORR by BICR and investigators as well as OS, safety, and tolerability. In cohort 1, treatment with EV resulted in an ORR of 44%, including a CR rate of 12%. An ORR of 38% and 41% was observed in patients with liver metastases and prior ICI exposure, respectively. The ORRs in ICI responders and ICI non-responders were 56% and 41%, respectively. Responses were seen irrespective of PD-L1 expression, with ORRs of 26% (PD-L1 high) and 47% (PD-L1 low). The median DOR was 7.6 months (95% CI, 4.93–7.46), and time to response was 1.84 months. Median PFS was 5.8 months (95% CI, 4.9–7.5), and median OS was 11.7 months (95% CI, 9.1-NR).
Ninety-four percent of patients in EV-201 cohort 1 developed TRAEs, which most commonly included fatigue (50%), decreased appetite (44%), alopecia (49%), dysgeusia (40%), and peripheral sensory neuropathy (40%). Grade 3 or higher TRAEs were seen in 54% of patients and included anemia (7%), neutropenia (8%), and fatigue (6%) (Table 1). Nineteen percent of patients developed serious adverse events (AEs), and peripheral sensory neuropathy was the most common reason for treatment withdrawal (6%). Among the AEs, peripheral neuropathy, rash, hyperglycemia, and infusion-related reactions were prespecified for analysis. Fifty percent of the patients experienced treatment-related peripheral neuropathy, with 94% being ≤ grade 2. Peripheral sensory neuropathy was more common than motor neuropathy, with a median time to onset of 2.43 months (range, 0.03–7.39) and time to improvement of 1.18 months (range, 0.26–4.86). Seventy-six percent of patients noted resolution or at least grade 1 neuropathy at last follow-up. Forty-eight percent of patients developed a treatment-related rash, of which 75% was ≤ grade 2. The rash usually developed after 4 days of infusion and resolved with either discontinuation or systemic corticosteroids. Complete resolution of rash was seen in 73% of patients, and 20% of patients had some improvement at last follow-up. Treatment-related hyperglycemia occurred in 11% of patients, irrespective of baseline status. Sixty-eight percent of patients with baseline hyperglycemia did not develop any TRAEs. Eight percent of patients without baseline hyperglycemia developed TRAEs. Total of 7/14 patients with these events developed ≤ grade 2 hyperglycemia. The median time of onset was 0.58 months (range, 0.26–9.23), 57% of patients with hyperglycemia had resolution of all events, and 14% experienced some improvement. Based on these results, on December 18, 2019 the Food and Drug Administration granted accelerated approval of EV for patients with mUC who previously received PD-1/PD-L1 inhibitors and platinum-based treatments in the neoadjuvant/adjuvant locally advanced or metastatic setting.14
Toxicity Management of EV
In the EV-201 trial, patients had adequate organ function, grade 1 or less peripheral neuropathy and ECOG PFS of 0 or 1 prior to enrollment. Among these relatively fit patients, dose interruptions occurred in 64% of patients and dose reduction occurred in 34% of patients. Peripheral neuropathy, rash, and fatigue were the most common AEs that led to EV dose interruption and dose reduction. Sixteen percent of patients discontinued EV due to AEs and peripheral neuropathy was the most common AE that led to EV discontinuation. Management guidelines on the common TRAEs are listed in Table 1. The presentation and management of peripheral neuropathy is similar to other microtubule-disrupting chemotherapies like docetaxel and paclitaxel. Given that nectin-4 is expressed in skin, skin reactions occurred in 54% of 310 patients treated with EV. The most common presentation was maculopapular rash, which is often pruritic and responded well to topical corticosteroids and antihistamines. Grade 3–4 skin reaction occurred in 10% of patients and included bullous dermatitis, exfoliative dermatitis, and palmar-plantar erythrodysesthesia. EV needs to be permanently discontinued for grade 4 or recurrent grade 3 skin reactions. Ocular disorders are common with EV and mostly presented with dry eyes followed by blurry vision. Ophthalmic examinations are not required prior to starting EV. Prophylactic artificial tears for dry eyes is recommended. Ophthalmic examinations are indicated for patients with more symptomatic ocular disorders and require treatments such as ophthalmic topical steroids. Compared to ocular disorders, hyperglycemia is a less common but more serious TRAE of EV. Death and diabetic ketoacidosis were reported in early phase trials. Although patients with higher body index and higher baseline hemoglobin A1C had higher incidence of grade 3–4 hyperglycemia, hyperglycemia has occurred in patients with or without pre-existing diabetes mellitus. The underlying etiology is not clear, but hyperglycemia has been observed in other ADCs containing MMAE. Blood glucose needs to be monitored and EV needs to be held if blood glucose level is above 250 mg/dL. Treatment with EV can be resumed at the same dose level after the blood glucose level is reduced to ≤250 mg/dl. MMAE is metabolized in the liver with a half-life of 2.4 days. A nearly 50% increase in unconjugated MMAE was observed in patients with mild hepatic impairment. EV needs to be held for patients with grade 3 AST abnormalities until it improves to grade 1. No significant difference in exposure of EV was observed in patients with mild, moderate, or severe renal impairment compared to patients with normal renal function. Thirty-eight percent of patients in the EV-201 trial have creatine clearance between 30 and 60. No dose reductions of EV are required for patients with renal impairment.
Ongoing EV-Based Combinational Trials in Patients with mUC
Data from preclinical studies performed with brentuximab vedotin, a CD30-directed ADC comprising the same linker and MMAE payload as EV, suggested that MMAE has the potential for immune modulation in addition to its antimitotic activity. These studies reported that MMAE could lead to immunogenic cell death, antigen presentation, and tumor immune infiltration.15 These results led to the hypothesis that combining PD-1/PD-L1 inhibitors with an MMAE containing ADCs, such as EV, leads to synergistic antitumor responses. EV-103 (NCT03288545) is a phase 1b, multi-cohort, multi-center study comparing EV as monotherapy and/or with combination therapies consisting of ICI, chemotherapy, or ICI + chemotherapy in patients with locally advanced or mUC (Table 2). As outlined in Table 3, this trial is comprised of a dose-escalation phase of EV + pembrolizumab as first-line or second-line in cisplatin-ineligible patients and a dose-expansion phase in multiple cohorts: cohort A (EV + pembrolizumab as first-line), cohort B (EV + pembrolizumab as second-line), cohort D (EV + cisplatin as first-line), cohort E (EV + carboplatin as first-line), cohort F (EV + gemcitabine as first- or second-line), and cohort G (EV + cisplatin/carboplatin + pembrolizumab as first-line). The trial also has 2 cohorts to examine muscle-invasive UC: cohort H (EV) and cohort J (EV + pembrolizumab). The primary outcome measure is safety/tolerability, with secondary measures including ORR, PFS, DCR, DOR, OS, and recommended dose. The recommended dose of EV was determined to be 1.25 mg/kg on days 1 and 8 every 3 weeks in combination with pembrolizumab for the expansion cohorts.
 |
Table 2 Ongoing Clinical Trials with Enfortumab Vedotin in Advanced or Metastatic Bladder Cancer Patients |
 |
Table 3 Breakdown of the Different Cohorts of the EV301 Trial |
Hoimes et al presented the initial results of cohort A, in which 45 cisplatin-ineligible patients with mUC were enrolled for frontline treatment.16 These patients received EV at a dose of 1.25 mg/kg on days 1 and 8 every 3 weeks + pembrolizumab at a dose of 200 mg on day 1 every 3 weeks. Patients treated with this combination therapy were reported to have an ORR of 71% (95% CI, 55.7%- 83.6%), with 13% achieving CR, 58% PR, and 22% stable disease. The DCR (CR, PR, or stable disease [SD]) was 93% (95% CI, 81.7%-98.6%), with only 2% (1 patient) with PD. Follow-up data (median 11.5 months) of this cohort were presented by Rosenberg et al.17 The reported ORR was 73.3% (95% CI, 58.1–85.4), with 15.6% of patients achieving CR and a DCR of 93.3%. Median PFS was 12.3 months (95% CI, 7.98-not reached); median OS was not reached; and the 12-month OS rate was 81.6% (95% CI, 62–91.8). The median DOR was not reached. Of the 33 responders, 55% had ongoing responses, 33% had PD, and 12% started a new treatment before their disease progressed. Ninety-six percent of patients developed TRAEs of any grade. The most common TRAEs were fatigue (49%), alopecia (49%), peripheral sensory neuropathy (49%), and diarrhea (44%). Grade 3 or higher TRAEs were noticed among 58% of patients, including fatigue (9%), maculopapular rash (9%), diarrhea (7%), and peripheral sensory neuropathy (4%). Increased lipase was noted in 18% of patients, although this was not associated with clinical pancreatitis. Sixteen percent of patients developed serious AEs, with resolution among 6 patients and 1 treatment-related death (multisystem organ failure). Thirteen percent of patients discontinued treatment due to TRAEs, for which the most common reason was peripheral sensory neuropathy. TRAEs of clinical interest included rash, hyperglycemia, peripheral neuropathy, and immune-mediated side effects. The majority of TRAEs were low-grade, and 18% of patients received corticosteroids. Thus, this combination shows promising activity with a tolerable side effect profile.17 The trial currently has an estimated enrollment of 407 patients and is estimated to be completed by July 2023.
EV-301 (NCT03474107) is a phase 3 multi-center trial examining patients who progressed on both platinum-based chemotherapy and immunotherapy (Table 2). Enrollment began in June 2018, with a total of 608 patients randomized to 2 arms. The trial compares EV (on days 1, 8, and 15 of each 28-day cycle) to chemotherapy (either docetaxel, vinflunine, or paclitaxel given on day 1 of each 21-day cycle). The study’s primary endpoint is OS, and its secondary endpoints are PFS, ORR, DOR, and safety/tolerability. The trial is estimated to be completed in September 2021 (NCT03474107).
EV-302 is an open-label phase 3 study (NCT04223856) examining EV + pembrolizumab with or without chemotherapy vs chemotherapy alone (Table 3). The study has 3 arms: arm A (EV + pembrolizumab), arm B (gemcitabine + cisplatin/carboplatin), and arm C (EV + pembrolizumab + cisplatin/carboplatin). Primary outcomes are PFS and OS, and secondary outcomes include ORR, DOR, disease control rates, and TRAEs. The study is open for enrollment with the goal of enrolling 1095 patients by November 2023.
Conclusions
The treatment landscape of mUC is continuously evolving. Cisplatin-based chemotherapy remains the frontline treatment for treating this disease, followed by PD-1 and PD-L1 ICIs. Systemic therapeutic options after these treatments are very limited. Often, patients with mUC may be cisplatin-ineligible, further limiting available therapeutic options. Erdafitinib is US Food and Drug Administration approved for patients with FGFR2/3-activating mutations in a post-platinum setting, with or without ICI exposure.18 However, the promising results of this agent are only applicable to a minority of patients.
EV has demonstrated clinical efficacy and safety in clinically challenging scenarios, such as liver metastasis and impaired renal function. In the heavily pretreated patient population, EV showed a response rate of 44%, with a 9% CR and a median OS of 11.7 months, which are unprecedented outcomes. EV was generally well tolerated, with the majority of AEs categorized as mild to moderate severity. In addition to AEs commonly associated with cytotoxic chemotherapy, 3 AEs of special interest include peripheral neuropathy, rash, and hyperglycemia reported irrespective of known baseline hyperglycemia.
With the integration of EV into the clinical management of mUC, it would be important to understand the mechanism of treatment resistance. Of note, very few patients enrolled in the early phase EV studies underwent a post-progression biopsy. These biopsies would help to understand whether loss of nectin-4 expression is a mechanism of resistance and whether treatment with EV enhances the infiltration of CD8+ T cells into the tumor microenvironments. Based on the available clinical data on IO-based trials in mUC, the EV pembrolizumab combination has reported the most impressive clinical response rate so far. Biomarker researches embedded in the ongoing EV-based mUC trials, particularly trials in the neoadjuvant setting, would be crucial for developing predictive biomarkers and for designing future studies to improve the outcome of UC. With more treatment options available for UC in the near future, one size fits all approaches will no longer be applicable to treating this heterogenous cancer.
Acknowledgments
Editorial assistance was provided by the Moffitt Cancer Center’s Scientific Editing Department by Dr. Paul Fletcher & Daley Drucker. No compensation was given beyond their regular salaries.
Disclosure
Rohit K Jain has received honoraria from DAVA Oncology, Advisory board for Pfizer and speaker program from Astellas Pharma Inc/ Seattle Genetics. Jingsong Zhang has received honoraria for advisory boards and speaker programs from AstraZeneca, Merck, Seattle Genetics and Astellas Pharma Inc. The authors report no other conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. doi:10.3322/caac.21590
2. Saginala K, Barsouk A, Aluru JS, Rawla P, Padala SA, Barsouk A. Epidemiology of bladder cancer. Med Sci (Basel). 2020;8(1):15.
3. National Comprehensive Cancer Network. Bladder cancer (Version 3.2020). Available from: https://www.nccn.org/professionals/physician_gls/pdf/bladder_blocks.pdf.
4. Jain RK, Snyders T, Nandgoapal L, Garje R, Zakharia Y, Gupta S. Immunotherapy advances in urothelial carcinoma. Curr Treat Options Oncol. 2018;19(12):79. doi:10.1007/s11864-018-0598-x
5. Bellmunt J, de Wit R, Vaughn DJ, et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N Engl J Med. 2017;376(11):1015–1026. doi:10.1056/NEJMoa1613683
6. Takai Y, Ikeda W, Ogita H, Rikitake Y. The immunoglobulin-like cell adhesion molecule nectin and its associated protein afadin. Annu Rev Cell Dev Biol. 2008;24:309–342. doi:10.1146/annurev.cellbio.24.110707.175339
7. Challita-Eid PM, Satpayev D, Yang P, et al. Enfortumab vedotin antibody-drug conjugate targeting nectin-4 is a highly potent therapeutic agent in multiple preclinical cancer models. Cancer Res. 2016;76(10):3003–3013. doi:10.1158/0008-5472.CAN-15-1313
8. Rikitake Y, Takai Y. Interactions of the cell adhesion molecule nectin with transmembrane and peripheral membrane proteins for pleiotropic functions. Cell Mol Life Sci. 2008;65(2):253–263. doi:10.1007/s00018-007-7290-9
9. Reymond N, Fabre S, Lecocq E, Adelaide J, Dubreuil P, Lopez M. Nectin4/PRR4, a new afadin-associated member of the nectin family that trans-interacts with nectin1/PRR1 through V domain interaction. J Biol Chem. 2001;276(46):43205–43215. doi:10.1074/jbc.M103810200
10. Fabre-Lafay S, Monville F, Garrido-Urbani S, et al. Nectin-4 is a new histological and serological tumor associated marker for breast cancer. BMC Cancer. 2007;7:73. doi:10.1186/1471-2407-7-73
11. Rosenberg J, Sridhar SS, Zhang J, et al. EV-101: a Phase I study of single-agent enfortumab vedotin in patients with nectin-4-positive solid tumors, including metastatic urothelial carcinoma. J Clin Oncol. 2020;38(10):1041–1049. doi:10.1200/JCO.19.02044
12. Takahashi S, Uemura M, Kimura T, et al. A phase I study of enfortumab vedotin in Japanese patients with locally advanced or metastatic urothelial carcinoma. Invest New Drugs. 2019.
13. Rosenberg JE, O’Donnell PH, Balar AV, et al. Pivotal trial of enfortumab vedotin in urothelial carcinoma after platinum and anti-programmed death 1/programmed death ligand 1 therapy. J Clin Oncol. 2019;37(29):2592–2600. doi:10.1200/JCO.19.01140
14. FDA. FDA Grants Accelerated Approval to Enfortumab Vedotin-Ejfv for Metastatic Urothelial Cancer; 2019.
15. Gardai SJ, Epp A, Law CL. Brentuximab vedotin-mediated immunogenic cell death. Cancer Res. 2015;75(15Suppl 1):Abstract 2469. doi:10.1158/0008-5472.CAN-14-3569
16. Hoimes CJ, Rosenberg JE, Petrylak DP, Carret A, Melhem-Bertrandt AM. EV-103: enfortumab vedotin plus pembrolizumab and/or chemotherapy for locally advanced or metastatic urothelial cancer. J Clin Oncol. 2019;37(15_suppl):TPS4593. doi:10.1200/JCO.2019.37.15_suppl.TPS4593
17. Rosenberg JE, Flaig TW, Friedlander TW, et al. Study EV-103: preliminary durability results of enfortumab vedotin plus pembrolizumab for locally advanced or metastatic urothelial carcinoma. J Clin Oncol. 2020;38(suppl 6):abstr 441. doi:10.1200/JCO.2020.38.6_suppl.441
18. Montazeri K, Bellmunt J. Erdafitinib for the treatment of metastatic bladder cancer. Expert Rev Clin Pharmacol. 2020;13(1):1–6. doi:10.1080/17512433.2020.1702025
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.