Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Emerging Surgical Therapies for Vitiligo: Tissue vs Cell-Based Approaches
Authors Ren C ![]() , Dong L, Zhang J
, Dong L, Zhang J
Received 23 September 2025
Accepted for publication 12 May 2026
Published 19 June 2026 Volume 2026:19 569535
DOI https://doi.org/10.2147/CCID.S569535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jeffrey Weinberg
Ci Ren, Lingyu Dong, Jian Zhang
Department of Dermatologic Surgery, Shenyang Seventh People’s Hospital, Shenyang, Liaoning, People’s Republic of China
Correspondence: Jian Zhang, Department of Dermatologic Surgery, Shenyang Seventh People’s Hospital, No. 13 Dongwei Road, Heping District, Shenyang, Liaoning, 110003, People’s Republic of China, Email [email protected]
Abstract: Vitiligo is a common dermatologic condition characterized by skin depigmentation. The current spectrum of treatments includes topical and systemic therapies, phototherapy, and surgical options. Recent years have witnessed notable advancements in surgical techniques, which are broadly categorized into tissue grafting and cell transplantation. Tissue grafting methods include follicular unit grafting, suction blister epidermal grafting, and thin split-thickness skin grafts. Cell transplantation techniques involve the use of autologous cultured melanocytes, non-cultured epidermal cell suspensions, and non-cultured cell suspensions from hair follicle outer root sheaths. To enhance surgical efficacy, future studies should aim to uncover the therapeutic mechanisms and identify relevant biomarkers.
Keywords: vitiligo, surgical therapy, tissue grafting, cell transplantation, review
Introduction
Vitiligo is a common acquired depigmenting disorder caused by the loss of melanocytes. Currently understood as an autoimmune disease associated with skin cell metabolism and oxidative stress,1 its development involves metabolic, inflammatory, and immune factors. The condition has a global lifetime prevalence of 0.36%2 and substantially impairs the quality of life and psychological health of those affected.
Pharmacological and phototherapy approaches primarily target the underlying autoimmune response and are most effective in active, progressive vitiligo. However, their efficacy is limited in stable, completely depigmented lesions where melanocytes have been irreversibly lost. Surgery overcomes this limitation by directly replenishing melanocytes. In recent years, transplantation techniques—which involve transferring normal skin or cells to depigmented areas—have emerged as a safe and effective approach for patients with stable disease lasting more than one year.1,3–5Following recipient-site preparation using methods such as dermabrasion, laser ablation (eg, CO2 or Er lasers), suction blistering, cryotherapy, or chemical peeling,6,7 tissue grafting or cell transplantation is performed to introduce functional melanocytes into vitiliginous patches and facilitate repigmentation.
This review aims to summarize the various surgical and innovative therapies reported in the literature, with the goal of supporting clinical vitiligo management and inspiring further research into surgical treatment strategies.
Methods
Literature Search Strategy
This study followed the PRISMA statement for literature retrieval. A systematic search was conducted in four major medical databases: PubMed, Embase, Web of Science, and the Cochrane Library. The search period covered from the inception of each database to the search date. The language of the retrieved literature was limited to English.
A combination of MeSH terms and free-text words was used. Using PubMed as an example, the search strategy was: (vitiligo[Title/Abstract] AND (surgery[Title/Abstract] OR surgical[Title/Abstract] OR transplantation[Title/Abstract] OR grafting[Title/Abstract])). The search strategies for other databases were adjusted according to their respective syntax requirements. Additionally, supplementary searches were performed by reviewing the reference lists of the included studies.
Inclusion and Exclusion Criteria
The inclusion criteria were: (1) patients with stable vitiligo; (2) studies reporting outcomes of surgical interventions for vitiligo; (3) studies published in English.
The exclusion criteria were: (1) non-English publications; (2) duplicate publications; (3) studies with unavailable full texts and conference abstracts.
Study Screening and Results
The initial search yielded 1245 records. After removing duplicates, the remaining records underwent title and abstract screening, during which 986 records were excluded. The remaining 259 records were assessed for full-text eligibility. After excluding studies with unavailable full texts and conference abstracts, 66 studies were finally included in this review.
Surgical Techniques
Tissue Grafting
Tissue grafting for vitiligo aims to achieve repigmentation via the autologous transfer of pigmented skin. Its use is limited by donor site availability, making it unsuitable for large areas. The main techniques include:
Mini-Punch Grafts
Conventional punch grafting (4 mm) has been used for the treatment of stable vitiligo, with reported excellent repigmentation rates of 50% and cobblestone appearance in 35% of patients.8 In contrast, mini-punch grafting (1–2 mm) offers advantages for irregular anatomical sites such as the nipple-areola complex, lips, palms, perineum, and soles, with fewer complications.9,10
Hair Follicle Transplantation
Follicular transplantation achieves cutaneous repigmentation by transplanting autologous pigmented follicle units from healthy donor sites, such as the occipital scalp, into vitiliginous patches.
Techniques for Harvesting and Implanting Pigmented Follicular Units
This technique implants hair follicle units—primarily anagen-phase follicles from the occipital scalp—into vitiliginous patches. Follicular melanocytes and stem cells contribute to repigmentation.11 The grafts consist mainly of terminal pigmented hair follicles with minimal dermis and epidermis,12 and even a small number of transplanted melanocytes can produce significant repigmentation.13 The subsequent growth of new pigmented hairs also provides visual coverage for areas with leukotrichia.
The method of harvesting these pigmented follicles is critical to their survival. Traditional harvesting methods using large punches or needles can cause significant perifollicular damage and scarring, compromising graft viability. In contrast, minimally invasive harvesting techniques have been developed to reduce tissue trauma. For instance, follicular unit extraction (FUE) with finer instruments and follicular scraping aim to preserve the integrity of the follicle during extraction, thereby improving graft survival and success rates.14
Management of Leukotrichia (White Hairs) in the Recipient Area
For optimal cosmetic outcomes, persistent white hairs within the vitiligo patch often need to be addressed prior to or in conjunction with surgical repigmentation. The goal here is the selective and permanent destruction of depigmented follicles.
Follicular scraping can be used as an ablative technique directly in the recipient area to remove white hairs. After tumescent anesthesia, a 1–3 cm incision is made down to the subcutaneous layer. Subcutaneous tissue is separated, and curettage is performed until white hairs extract easily. The wound is sutured, with removal after 7–9 days. Pigmented hair transplantation can then be performed into the scarred area 1–3 months later.14 Electrolysis is another effective method that uses low-current direct current to destroy hair follicles via electrochemical reaction, minimizing peripheral tissue damage compared to older techniques. It effectively achieves permanent white hair removal, which can improve the overall aesthetic result and prevent the visual contrast of white hairs against repigmented skin.15 A specialized application involves its use in eyelash vitiligo; electrolysis of the depigmented lash follicle can be followed by immediate reimplantation of a pigmented follicle using a triangular needle to secure the root subdermally, achieving a natural, curved appearance.16
Suction Blister Epidermal Grafting (SBEG)
A commonly used, effective surgical method for small lesions, SBEG involves harvesting the roof of a suction-induced blister from the thigh or abdomen and transplanting it, dermis-side down, onto a dermabraded recipient site. Blister induction time can be reduced by increasing temperature, decreasing blister diameter, or using tumescent anesthesia.17 Alternatives include cryotherapy or heated suction. Correct orientation is critical; identification methods include fibrin clot presence, epidermal curling tendency, and more pronounced wrinkling on the epidermal side under microscopy.18 The graft is covered with glycerin gauze for 7–10 days. Advantages include stable repigmentation; drawbacks include peripheral hypopigmented halos and donor-site hyperpigmentation.19
Thin Skin Grafts
This category includes thin (0.1–0.2 mm) and ultrathin (0.08–0.15 mm) skin grafts harvested at the dermo-epidermal junction using a knife or dermatome.20 Donor skin should be 10%–20% larger than the recipient area,21 typically taken from the buttock, thigh, or scalp.22 These grafts provide rapid, uniform repigmentation. Meshing the graft can expand coverage. Before cell transplantation, this was the most effective surgical method,23 offering superior cosmetic outcomes without cobblestoning compared to SBEG.24
Flip-Top Grafting
After donor skin is harvested and sectioned, 1–5 epidermal flaps (5×5 mm, including minimal papillary dermis) are raised within the vitiligo patch. The grafts are placed under the flaps and sealed with cyanoacrylate. Dressings are removed after one week, with success confirmed by observing pigmentation beneath the flap.25 This method avoids full epidermal removal, reducing scarring and improving survival. Limitations include technical difficulty, small treatment area, and unsuitability for palms/soles.
Smash Grafting
Donor skin is minced into tiny fragments with scissors, mixed with saline, and applied as a semi-solid paste to the recipient site. This simple technique can cover an area up to 10 times larger than the donor site.26 The loss of graft structure allows for even distribution regardless of orientation. Microskin grafting, which employs the same principle, has been successfully used for vitiligo affecting genital areas, achieving nearly complete and uniform repigmentation. However, the overall efficacy of smash grafting requires further validation.27
Epidermal Grafting
Perilesional normal skin serves as the donor site. After applying 2% mupirocin ointment, the site is superficially dermabraded until pinpoint bleeding occurs. The abraded epidermal fragments are collected on a sterile spatula—aided by the ointment—and spread onto the prepared vitiliginous skin. Benefits include single-site surgery, reduced pain, and less dressing use.28 Drawbacks include limited suitability for large areas and possible peripheral hypopigmentation.
An advanced modification involves centrifuging the collected fragments in Ringer’s lactate, mixing the sediment with plasma gel (prepared by combining 0.1 mL autologous serum with 0.9 mL platelet-poor plasma), and applying the mixture to achieve repigmentation comparable to non-cultured melanocyte transplantation.29 Of note, while the traditional method falls under epidermal grafting, the modified version—utilizing centrifugation and plasma gel—processes tissue into a cellular suspension/paste, aligning its mechanism and application more closely with cell transplantation.
A summary table of tissue transplantation for vitiligo is shown in Table 1.
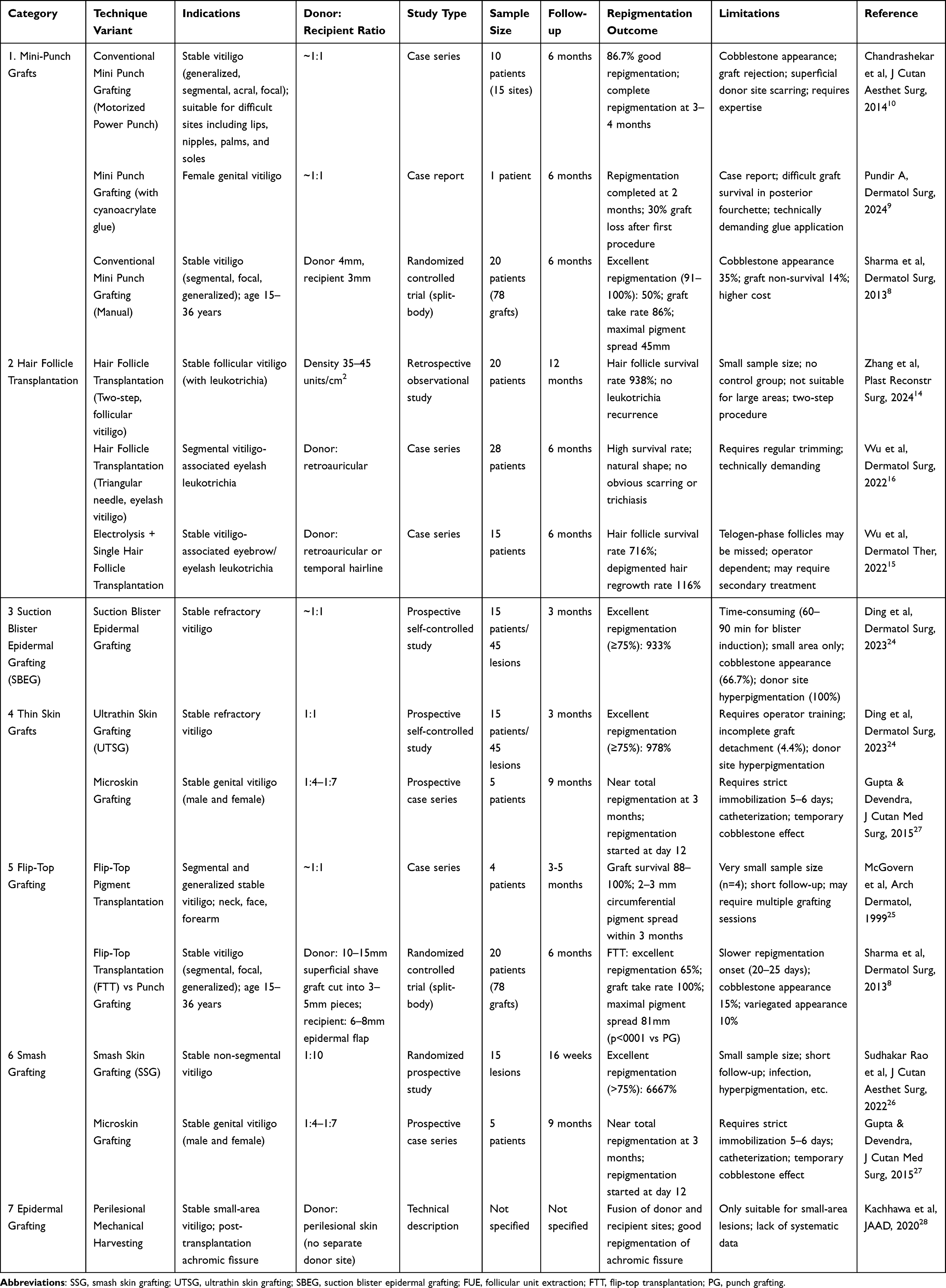 |
Table 1 Tissue Grafting Techniques for Vitiligo |
Cell Transplantation
Cell transplantation techniques for vitiligo include cultured and non-cultured epidermal cell suspensions, as well as non-cultured outer root sheath cell suspensions Potential side effects include hypopigmented halos at the recipient site, and scarring or hyperpigmentation at the donor site.30
Cultured Melanocyte Transplantation (CMT) vs Non-Cultured Epidermal Cell Suspension (NCES)
Cultured Melanocyte Transplantation (CMT)
Melanocytes are expanded in vitro for approximately three weeks before transplantation, achieving a donor-to-recipient area ratio of up to 1:60. The proliferation rate varies by donor site, with facial melanocytes demonstrating the fastest growth and the most sustained proliferation in culture, followed by buttock, abdominal, and limb skin; chest and back skin show the slowest growth.31 The requirement for a GMP-certified laboratory, high risk of contamination, and substantial cost limit its use to extensive vitiligo and restrict routine clinical application. Therefore, this review focuses on non-cultured techniques.
Non-Cultured Epidermal Cell Suspension (NCES)
This method involves transplanting a suspension of melanocytes and keratinocytes on the same day (warm trypsinization) or the next day (cold trypsinization) onto a dermabraded recipient area, bypassing the costly and time-consuming cell culture process. It yields repigmentation outcomes comparable to tissue grafting, with a donor-to-recipient ratio of 1:10 to 1:20, and is an effective, durable, and well-tolerated treatment for stable vitiligo.32 One study reported that 67% of patients achieved over 50% repigmentation 24 weeks after a single session.33 Beyond vitiligo, NCES has been successfully used for repigmenting depigmented areas resulting from burns, herpes zoster, chemical leukoderma, and discoid lupus erythematosus.33–36A retrospective study of 41 patients with stable vitiligo reported an excellent repigmentation rate (91–100%) of 34.1%, notably with all four pediatric patients (under 14 years of age) achieving >76% repigmentation, suggesting favorable outcomes in children.37
Cell Delivery Methods
The standard method involves applying the cell suspension directly onto the prepared recipient site.38,39 Adding hyaluronic acid or hydroxypropyl methylcellulose to the suspension increases viscosity and improves adherence.40,41
Microneedling creates microchannels that facilitate drug or cell delivery. One study reported improved repigmentation after microneedling followed by NCES application, though it may be less effective than dermabrasion.42–44
Using a tattoo device to inject the suspension intradermally offers advantages such as reduced procedure time, less postoperative pain, and potentially superior repigmentation compared to traditional methods, warranting further investigation.45
Trypsinization Protocols
Warm trypsinization (37°C for 45–60 minutes) is widely adopted due to high enzymatic activity and the ability to complete the procedure in one day, enhancing patient convenience. Although cold trypsinization (4°C overnight) may yield higher cell viability and melanin content, clinical repigmentation outcomes between the two methods are comparable.46–48
Trypsin activity can be halted by:
Washing the cell pellet with phosphate-buffered saline (PBS) or Dulbecco’s Modified Eagle Medium (DMEM) removes trypsin.39,49,50
Using autologous serum or fetal bovine serum (FBS), which contains protease inhibitors like α1-antitrypsin, effectively neutralizes trypsin.29,51
Repigmentation on curved or mobile areas (eg, nose, lips) can be uneven due to suspension runoff. Using custom-made elastic impression materials to create well-defined recipient chambers has been shown to improve outcomes by containing the suspension.52,53
Technical Variations and Adjuncts
Several simplified protocols have been developed to make NCES more accessible. The four-compartment (FC) method uses a specially designed Petri dish divided into four compartments to perform trypsinization, washing, and cell separation in sequence, eliminating the need for a centrifuge and trypsin inhibitors while maintaining high cell viability.54 Similarly, the “4-well plate” technique offers another cost-effective, clinic-friendly modification.55,56
The evidence for adding PRP to NCES is mixed. Some studies suggest it enhances repigmentation, possibly through growth factor stimulation, while others show no significant benefit over standard suspensions, particularly on acral sites.57–59
Pre-treatment of the recipient site with 5-FU after microneedling has been proposed to improve repigmentation, potentially by modulating local immune responses and promoting melanocyte migration.60
These laboratory-grown epidermal sheets, with a near-physiological ratio of melanocytes to keratinocytes, represent an advanced alternative. They are particularly suitable for large areas and difficult-to-treat sites like the hands, offering more uniform repigmentation. Limitations include a longer preparation time (2–4 weeks) and higher technical demands.19,52,61
Non-Cultured Hair Follicle Cell Suspension (NC-HFCS)
NC-HFCS is prepared from anagen hair follicles obtained via follicular unit extraction. The suspension contains melanocytes, melanocyte stem cells, and keratinocyte stem cells. Approximately 15–25 follicles can treat a 20 cm2 area. Studies indicate that NC-HFCS and NCES have comparable efficacy, although NCES is often considered more practical and less time-consuming.62 Combining NCES with NC-HFCS may yield better results than NCES alone, possibly due to the immunomodulatory properties and stem cell support provided by follicular cells.63
A summary comparison table of cell transplantation for vitiligo is shown in Table 2.
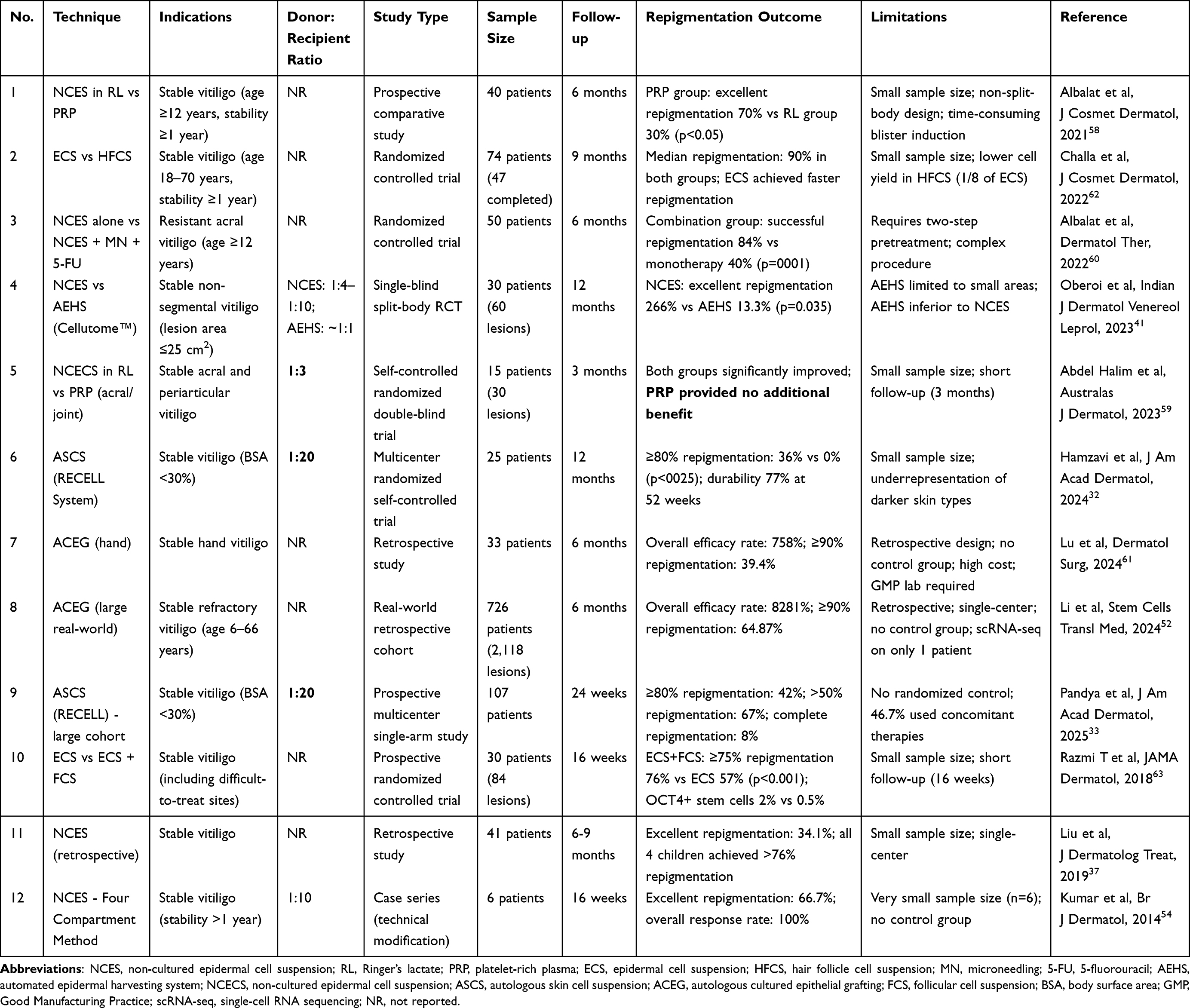 |
Table 2 Cell Transplantation Techniques for Vitiligo |
Summary and Future Perspectives
Surgical treatments for vitiligo have advanced considerably, demonstrating safe and effective outcomes in patients with stable disease. Tissue transplantation (eg, punch grafting, suction blister, smash grafting) remains a simple, low-cost option with proven efficacy, particularly for localized lesions. Cell transplantation (eg, non-cultured melanocyte suspension, cultured melanocytes) offers superior repigmentation uniformity and can cover larger areas, albeit with higher technical demands and costs. The optimal approach should be selected based on individual patient assessment, including lesion location, size, and skin phototype.17
A major gap in the current literature is the lack of systematic comparisons of cost-effectiveness and learning curves across different surgical techniques. Future direct comparative studies are urgently needed to establish clear selection parameters. Additionally, the cellular mechanisms underlying surgical repigmentation remain largely unexplored. Emerging evidence suggests that CD8+ T cell count is negatively correlated with post-surgical repigmentation success, serving as a potential biomarker for identifying ideal surgical candidates.64 miRNAs in exosomes also regulate melanocyte function, offering promising therapeutic prospects.65,66
Looking forward, integrating surgical advances with personalized medicine and regenerative dermatology holds great promise. By combining patient-specific biomarkers (eg, CD8+ T cell levels), exosome-based therapies, and engineered cell or tissue products, future surgical approaches can be tailored to individual immune and regenerative profiles, ultimately enhancing repigmentation outcomes and expanding treatment options for refractory vitiligo.
Ethics Approval and Consent to Participate
This is a review article that synthesizes and analyzes previously published literature. No original human or animal studies were conducted by the authors. Therefore, ethical approval and informed consent are not required for this work.
Acknowledgments
We would like to express our gratitude to Shenyang Seventh People’s Hospital for providing the necessary work platform and logistical support for the smooth conduct of this study, which has created favorable conditions for the implementation of the research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Diotallevi F, Gioacchini H, De Simoni E, et al. Vitiligo, from pathogenesis to therapeutic advances: state of the art. Int J Mol Sci. 2023;24(5):4910. doi:10.3390/ijms24054910
2. Akl J, Lee S, Ju HJ, et al. Estimating the burden of vitiligo: a systematic review and modelling study. Lancet Public Health. 2024;9(6):e386–12. doi:10.1016/S2468-2667(24)00026-4
3. Kawakami T. Surgical procedures and innovative approaches for vitiligo regenerative treatment and melanocytorrhagy. J Dermatol. 2022;49(4):391–401. doi:10.1111/1346-8138.16316
4. van Geel N, Speeckaert R, Taïeb A, et al. Worldwide expert recommendations for the diagnosis and management of vitiligo: position statement from the International Vitiligo Task Force Part 1: towards a new management algorithm. J Eur Acad Dermatol Venereol. 2023;37(11):2173–2184. doi:10.1111/jdv.19451
5. LeWitt TM, Kundu RV. Vitiligo. JAMA Dermatol. 2021;157(9):1136. doi:10.1001/jamadermatol.2021.1688
6. Post NF, Ezekwe N, Narayan VS, et al. The use of lasers in vitiligo, an overview. J Eur Acad Dermatol Venereol. 2022;36(6):779–789. doi:10.1111/jdv.18005
7. Rajput L, Kharghoria G, Patel U, Gupta S. Chemically assisted gauze abrasion: an economical and convenient alternative to mechanical dermabrasion in vitiligo surgery. J Am Acad Dermatol. 2023;89(4):e141–e142. doi:10.1016/j.jaad.2021.07.034
8. Sharma S, Garg VK, Sarkar R, Relhan V. Comparative study of flip-top transplantation and punch grafting in stable vitiligo. Dermatol Surg. 2013;39(9):1376–1384. doi:10.1111/dsu.12263
9. Pundir A. Old is Gold! Outcome of mini punch grafting using cyanoacrylate glue in female genital vitiligo. Dermatol Surg. 2024;50(3):314–316. doi:10.1097/DSS.0000000000004029
10. Chandrashekar B, Madura C, Varsha D. Autologous mini punch grafting: an experience of using motorized power punch in 10 patients. J Cutan Aesthet Surg. 2014;7(1):42–45. doi:10.4103/0974-2077.129977
11. Ghasemi M, Bajouri A, Shafiiyan S, Aghdami N. Hair follicle as a source of pigment-producing cells for treatment of vitiligo: an alternative to epidermis? Tissue Eng Regen Med. 2020;17(6):815–827. doi:10.1007/s13770-020-00284-2
12. Laufer-Britva R, Vathananai W, Jimenez F. Therapeutic applications of hair follicle transplantation beyond hair restoration: a comprehensive review. Dermatol Surg. 2025;51(6):615–621. doi:10.1097/DSS.0000000000004571
13. Kim SR, Han KD, Kim CY. Repigmentation of vitiligo using the follicular unit extraction technique. Dermatol Surg. 2014;40(12):1425–1427. doi:10.1097/DSS.0000000000000161
14. Zhang J, Qu Q, Fan Z, et al. Minimally invasive removal of leukotrichia and hair transplantation: a 2-step surgery in the treatment of stable follicular vitiligo. Plast Reconstr Surg. 2024;154(4):666e–672e. doi:10.1097/PRS.0000000000010804
15. Wu Y, Dai Y, Wang T, Jin H, Peng J, Xu A. The application of electrolysis of depigmented hair using a trichiasis electrolyzer combined with single hair follicle transplantation for the treatment of vitiligo-associated leukotrichia. Dermatol Ther. 2022;35(5):e15400. doi:10.1111/dth.15400
16. Wu Y, Dai Y, Wang T, Song X. How we do it: eyelash implantation using a triangular suture needle. Dermatol Surg. 2022;48(7):793–795. doi:10.1097/DSS.0000000000003485
17. Bhingradia YM, Gupta S, Ghia D, et al. Consensus statement on the surgical management of vitiligo. J Cutan Aesthet Surg. 2025;18(1):27–33. doi:10.25259/JCAS_117_2024
18. Mohammad TF, Hamzavi IH. Surgical therapies for vitiligo. Dermatol Clin. 2017;35(2):193–203. doi:10.1016/j.det.2016.11.009
19. Anbar TS, El-Fakahany HM, El-Khayyat MA, Abdel-Rahman AT, Saad EK. Factors affecting the outcome of the suction blisters using two different harvesting techniques in vitiligo patients. J Cosmet Dermatol. 2020;19(7):1723–1729. doi:10.1111/jocd.13222
20. Xu AE, Gao TW. Baidianfeng. Nanjing: Jiangsu Fenghuang Science and Technology Press; 2020:194–214.
21. Frączek A, Kasprowicz-Furmańczyk M, Placek W, Owczarczyk-Saczonek A. Surgical treatment of vitiligo. Int J Environ Res Public Health. 2022;19(8):4812. doi:10.3390/ijerph19084812
22. Ren C, Dong L, Zhang J. Using scalp instead of buttocks or thigh skin for vitiligo grafting. J Am Acad Dermatol. 2025;93:e175–e176. doi:10.1016/j.jaad.2025.05.1372
23. Razmi TM, Afra TP, Parsad D. Vitiligo surgery: a journey from tissues via cells to the stems! Exp Dermatol. 2019;28(6):690–694. doi:10.1111/exd.13807
24. Ding X, Sun Y, Wang F, Du J. Ultrathin skin grafting versus suction blister epidermal grafting in the treatment of resistant stable vitiligo: a self-controlled comparative study. Dermatol Surg. 2023;49(7):659–663. doi:10.1097/DSS.0000000000003780
25. McGovern TW, Bolognia J, Leffell DJ. Flip-top pigment transplantation: a novel transplantation procedure for the treatment of depigmentation. Arch Dermatol. 1999;135(11):1305–1307. doi:10.1001/archderm.135.11.1305
26. Sudhakar Rao KM, Koti VR, Gaikwad S. Comparison of smash skin grafting and autologous non-cultured epidermal cell suspension in re-pigmentation of stable vitiligo. J Cutan Aesthet Surg. 2022;15(3):288–294. doi:10.4103/JCAS.JCAS_122_21
27. Gupta DK, Devendra S. Microskin grafting for stable vitiligo of the penis and vulva: near total uniform pigmentation. J Cutan Med Surg. 2015;19(5):477–483. doi:10.1177/1203475415577752
28. Kachhawa D, Kachhawa N, Gupta S. Mechanical harvesting of perilesional normally pigmented tissue to merge donor and recipient sites for transplantation in vitiligo. J Am Acad Dermatol. 2022;87(2):e69–e70. doi:10.1016/j.jaad.2020.08.069
29. Elmorsy EH, El Garem YF, Affara SM, Halwag DI. Noncultured trypsinized epidermal cell suspension transplantation after cryoblebbling versus noncultured nontrypsinized epidermal cell graft homogenized with plasma gel after dermabrasion for stable vitiligo. Dermatol Surg. 2024;50(9):855–860. doi:10.1097/DSS.0000000000004231
30. McCrary MR, Gibbs DC, Alharthi M, Krueger LD. Utilization of our toolkit: a systematic review and meta-analysis of surgical therapies in vitiligo treatment. Dermatol Surg. 2022;48(8):815–821. doi:10.1097/DSS.0000000000003503
31. Yang HJ, Yang KC, Wang YF, Yang YT, Ko JL. In vitro proliferation of human epidermal melanocytes biopsied from multiple anatomical sites. J Cosmet Dermatol. 2020;19(11):3077–3082. doi:10.1111/jocd.13348
32. Hamzavi IH, Ganesan AK, Mahmoud BH, et al. Effective and durable repigmentation for stable vitiligo: a randomized within-subject controlled trial assessing treatment with autologous skin cell suspension transplantation. J Am Acad Dermatol. 2024;91(6):1104–1112. doi:10.1016/j.jaad.2024.08.027
33. Pandya AG, Mahmoud BH, Huggins RH, et al. Autologous cell harvesting device provides repigmentation and improves quality-of-life for patients with stable vitiligo lesions in a large and diverse patient population. J Am Acad Dermatol. 2025;93(2):378–386. doi:10.1016/j.jaad.2025.03.066
34. Manning L, Ferreira IB, Gittings P, et al. Wound healing with “spray-on” autologous skin grafting (ReCell) compared with standard care in patients with large diabetes-related foot wounds: an open-label randomised controlled trial. Int Wound J. 2022;19(3):470–481. doi:10.1111/iwj.13646
35. Marzano AV, Alberti-Violetti S, Maronese CA, Avallone G, Jommi C. Vitiligo: unmet need, management and treatment guidelines. Dermatol Pract Concept. 2023;13(4S2):e2023316S. doi:10.5826/dpc.1304S2a316S
36. Mehta N, Taneja N, Gupta S. Non-cultured epidermal cell suspension and laser resurfacing to improve the appearance of thick post-burn skin graft. Indian J Dermatol Venereol Leprol. 2023. doi:10.25259/IJDVL_402_2023
37. Liu B, Chen HH, Liu ZH, et al. The clinical efficacy of treatment using the autologous non-cultured epidermal cell suspension technique for stable vitiligo in 41 patients. J DermatolTreat. 2021;32(1):90–94. doi:10.1080/09546634.2019.1619657
38. Holmes JH. A brief history of RECELL® and its current indications. J Burn Care Res. 2023;44(Suppl_1):S48–S49. doi:10.1093/jbcr/irac121
39. Kahn SA, Carter JE, Wilde S, Chamberlain A, Walsh TP, Sparks JA. Autologous skin cell suspension for full-thickness skin defect reconstruction: current evidence and health economic expectations. Adv Ther. 2024;41(3):891–900. doi:10.1007/s12325-023-02777-7
40. van Geel N, Ongenae K, Naeyaert JM. Surgical techniques for vitiligo: a review. Dermatology. 2001;202(2):162–166. doi:10.1159/000051626
41. Oberoi B, Baveja S, Pathania V, Neema S. Comparative study of the efficacy and safety of two grafting procedures (an automated epidermal harvesting system and non-cultured epidermal cell suspension) in the treatment of stable vitiligo. Indian J Dermatol Venereol Leprol. 2023;89(4):536–542. doi:10.25259/IJDVL_1010_2021
42. Alshiyab D, Ba-Shammakh SA, Haj-Freej HM, et al. The microneedle revolution: transforming vitiligo treatment landscapes–a comprehensive review of the literature. J Cutan Med Surg. 2025;29(1):56–62. doi:10.1177/12034754241290817
43. Nilforoushzadeh MA, Nouri M, Alavi S, et al. Combination of epidermal keratinocyte-melanocyte cells suspension and microneedling: safe surgical approach in vitiligo. J Cosmet Dermatol. 2022;21(10):4669–4676. doi:10.1111/jocd.14987
44. Hasan MS, Almohsen AM, Nasr MI, et al. Dermabrasion versus microneedling in transplantation of autologous noncultured melanocyte-keratinocyte cell suspension in patients with vitiligo. Dermatol Surg. 2023;49(5):494–502. doi:10.1097/DSS.0000000000003738
45. Meena A, Vinay K, Kumaran MS, Kumar S, Bishnoi A, Parsad D. Conventional suspension delivery versus tattooing pen-assisted suspension delivery in non-cultured epidermal cell suspension procedure for vitiligo: a randomized controlled trial. Pigm Cell Melanoma Res. 2024;37(6):839–846. doi:10.1111/pcmr.13187
46. Gauthier Y, Surleve-Bazeille JE. Autologous grafting with noncultured melanocytes: a simplified method for treatment of depigmented lesions. J Am Acad Dermatol. 1992;26(2 Pt 1):191–194. doi:10.1016/0190-9622(92)70024-a
47. Olsson MJ, Juhlin L. Leucoderma treated by transplantation of a basal cell layer enriched suspension. Br J Dermatol. 1998;138(4):644–648. doi:10.1046/j.1365-2133.1998.02177.x
48. Chauhan S, Challa A, Arava SK, Upadhyay AD, Sharma A, Gupta S. Comparison of laboratory and clinical parameters of cold versus warm trypsinization methods of non-cultured epidermal cell suspension preparation in the treatment of stable vitiligo: a randomized trial. Arch Dermatol Res. 2024;316(8):592. doi:10.1007/s00403-024-03350-0
49. Holla AP, Kumar R, Parsad D, Kanwar A. Modified procedure of noncultured epidermal suspension transplantation: changes are the core of vitiligo surgery. J Cutan Aesthet Surg. 2011;4(1):44–45. doi:10.4103/0974-2077.79192
50. Agrawal A, Budania A, Mandiya S. No-laboratory epidermal cell paste-a novel modification for stable vitiligo. Dermatol Surg. 2024;50(10):981–983. doi:10.1097/DSS.0000000000004221
51. Lagerwall C, Shahin H, Abdallah S, et al. Xeno-free workflow exhibits comparable efficiency and quality of keratinocytes isolated from human skin biopsies. Regen Ther. 2021;18:401–407. doi:10.1016/j.reth.2021.09.005
52. Li J, Zeng X, Chen S, et al. The treatment of refractory vitiligo with autologous cultured epithelium grafting: a real-world retrospective cohort study. Stem Cells Transl Med. 2024;13(5):415–424. doi:10.1093/stcltm/szae009
53. Akshi B, Shilpa K, Harish P. A novel point-of-care technique to improve graft uptake in a melanocyte-keratinocyte transplantation procedure for vitiligo of contoured areas such as the external ear. J Am Acad Dermatol. 2022;86(5):e191–e192. doi:10.1016/j.jaad.2020.05.117
54. Kumar R, Parsad D, Singh C, Yadav S. Four compartment method: a simplified and cost-effective method of noncultured epidermal cell suspension for the treatment of vitiligo. Br J Dermatol. 2014;170(3):581–585. doi:10.1111/bjd.12725
55. Goh BK, Chua XM, Chong KL, de Mil M, van Geel NA. Simplified cellular grafting for treatment of vitiligo and piebaldism: the “6-well plate” technique. Dermatol Surg. 2010;36(2):203–207. doi:10.1111/j.1524-4725.2009.01423.x
56. Mrigpuri S, Razmi TM, Sendhil Kumaran M, Vinay K, Srivastava N, Parsad D. Four compartment method as an efficacious and simplified technique for autologous non-cultured epidermal cell suspension preparation in vitiligo surgery: a randomized, active-controlled study. J Eur Acad Dermatol Venereol. 2019;33(1):185–190. doi:10.1111/jdv.15234
57. Rekik M, Mseddi M, Kammoun N, Sellami K, Turki H. Efficacy of autologous platelet-rich plasma in the treatment of vitiligo: a 10-patient prospective study. J Cosmet Dermatol. 2022;21(10):4225–4233. doi:10.1111/jocd.15050
58. Albalat W, Elsayed M, Salem A, Ehab R, Fawzy M. Non-cultured epidermal cells suspended in either platelet-rich plasma or ringer lactate for stable vitiligo: a prospective comparative study. J Cosmet Dermatol. 2022;21(7):3102–3109. doi:10.1111/jocd.14576
59. Abdel Halim DM, Fekry A, Mogawer RM. The value of adding platelet-rich plasma (PRP) to noncultured epidermal cell suspension (NCECS) in surgical treatment of stable resistant vitiligo: a self-controlled randomised double-blinded study. Australas J Dermatol. 2023;64(3):359–367. doi:10.1111/ajd.14080
60. Albalat W, Elsayed M, Salem A, Ehab R, Fawzy M. Microneedling and 5-flurouracil can enhance the efficacy of non-cultured epidermal cell suspension transplantation for resistant acral vitiligo. Dermatol Ther. 2022;35(10):e15768. doi:10.1111/dth.15768
61. Lu H, Wang X, Chen S, Lin J, Wu W, Li J. Autologous cultured tissue engineering epidermal sheet transplantation to treat vitiligo of the hands. Dermatol Surg. 2024;50(12):1114–1119. doi:10.1097/DSS.0000000000004317
62. Challa A, Chauhan S, Pangti R, et al. Evaluation of clinical efficacy and laboratory indicators of non-cultured epidermal cell suspension and hair follicle cell suspension in surgical management of stable vitiligo: a randomized comparative trial. J Cosmet Dermatol. 2022;21(12):6958–6964. doi:10.1111/jocd.15407
63. Razmi TM, Kumar R, Rani S, Kumaran SM, Tanwar S, Parsad D. Combination of follicular and epidermal cell suspension as a novel surgical approach in difficult-to-treat vitiligo: a randomized clinical trial. JAMA Dermatol. 2018;154(3):301–308. doi:10.1001/jamadermatol.2017.5795
64. Refat MA, Strassner JP, Frisoli ML, et al. Lesional CD8+ T-Cell number predicts surgical outcomes of melanocyte-keratinocyte transplantation surgery for vitiligo. J Invest Dermatol. 2023;143(11):2275–2282.e6. doi:10.1016/j.jid.2023.03.1689
65. Shi HX, Zhang RZ, Xiao L, Wang L. Effects of keratinocyte-derived and fibroblast-derived exosomes on human epidermal melanocytes. Indian J Dermatol Venereol Leprol. 2022;88(3):322–331. doi:10.25259/IJDVL_1087_19
66. Yu H, Feng H, Zeng H, et al. Exosomes: the emerging mechanisms and potential clinical applications in dermatology. Int J Biol Sci. 2024;20(5):1778–1795. doi:10.7150/ijbs.92897
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.