Back to Journals » Drug Design, Development and Therapy » Volume 19
Emerging Strategies for Bioactive Agent-Loaded Xenogeneic Bone Scaffolds in Regenerative Medicine: A Comprehensive Review
Authors Zhang J, Qin W, Yue W, Zhang W, Zhao Y, Xu G ![]()
Received 15 August 2025
Accepted for publication 24 November 2025
Published 3 December 2025 Volume 2025:19 Pages 10665—10690
DOI https://doi.org/10.2147/DDDT.S560876
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Jing Zhang,1,2 Wenhe Qin,1,2 Wenjie Yue,1,2 Wanhao Zhang,1,2 Yantao Zhao,3,4 Gang Xu1,2
1Department of Orthopaedics, First Affiliated Hospital of Dalian Medical University, Dalian, 116011, People’s Republic of China; 2Key Laboratory of Molecular Mechanism for Repair and Remodeling of Orthopaedic Diseases (Liaoning Province), Dalian, 116011, People’s Republic of China; 3Senior Department of Orthopedics, The Fourth Medical Center of PLA General Hospital, Beijing, 100048, People’s Republic of China; 4Beijing Engineering Research Center of Orthopaedic Implants, Beijing, 100048, People’s Republic of China
Correspondence: Gang Xu, Email [email protected]
Abstract: The escalating global burden of an aging population and the rising incidence of secondary traumatic injuries have precipitated a mounting worldwide demand for bone grafts. However, autologous bone transplantation-the prevailing clinical “gold standard”-remains insufficient to meet this growing clinical need. Notably, rapid advancements in bone tissue engineering (BTE) have yielded diverse bone graft substitutes designed to recapitulate the three essential characteristics of bone tissue: osteoconductivity, osteoinductivity, and osteogenic potential. Within this domain, core scaffolds functioning as carriers for bioactive agents represent a highly promising strategy for treating bone defects. This review focuses on the design and fabrication of optimal xenogeneic bone scaffolds. It systematically examines commonly loaded bioactive components, including bone morphogenetic proteins (BMPs), platelet-rich plasma (PRP), natural products, active ingredients derived from traditional Chinese medicine ingredients (TCMs), and exosomes. The advantages and limitations inherent to these agents are critically analyzed. Furthermore, the review addresses current challenges and explores future research directions in bone scaffold engineering. By advancing multimodal strategies for modulating the delivery of bioactive agents, we aim to provide more effective therapeutic solutions for patients with critical bone defects.
Keywords: xenograft bone scaffolds, bone morphogenetic proteins, platelet-rich plasma, natural products, traditional Chinese medicine
Introduction
The global population is aging, with a notable increase in the elderly demographic in Asia, where the number of older individuals is rising by 3% annually. This trend has led to a significant increase in the incidence of bone-related diseases worldwide.1 A study indicates that in 2019 alone, approximately 178 million people worldwide experienced fractures, representing a nearly 34% increase over the past three decades.2 Concurrently, around 2.2 million bone grafts were performed globally each year, incurring costs of approximately $2.5 billion, a figure that is gradually rising in response to the expanding aging population.3 Bone is a rigid tissue characterized by a highly vascularized, three-dimensional (3D) composite porous structure, composed of organic and inorganic materials in varying proportions (with organic matter constituting 30% and inorganic matter 70%).4 This tissue serves multiple functions, including protection, movement, mineral storage, accommodation of bone marrow, and maintenance of the body’s structural integrity.5,6 Additionally, bones possess the ability to undergo automatic repair and regeneration in response to certain injuries during their development and continuous remodeling throughout adulthood.7 However, the capacity for self-repair and regeneration themselves is limited when faced with severe bone damage (defined as a bone defect size greater than 2 cm or loss of bone circumference exceeding 50%) resulting from severe trauma, bone diseases, congenital deformities, or cancer.8 Autologous bone grafting is regarded as the “gold standard” for optimal tissue acceptance and osteogenesis, however, it presents challenges such as the need for secondary surgery, donor site injuries, insufficient bone graft volume, limited availability, and potential complications.9,10 Allografts serve as an alternative, yet they carry risk of immunogenic reactions and viral transmission.11 Problems associated with the integration and compatibility of inert non-bioactive metal implants with surrounding tissues and natural bone, mismatch of biodegradable metal grafts with the rate of bone healing, and lack of long-term in vivo safety validation have hindered their widespread clinical application.12 To mitigate these limitations, more effective strategies required, and bone tissue engineering (BTE) utilizing biomaterials, cells, and bioactive molecules has emerged as a promising alternative to autografts and allografts.13 BTE aims to replicate the three primary properties of bone: the osteoconductivity that facilitates new bone growth on the implant surface, the osteoinductiveness of mesenchymal stem cells (MSCs) that generates produce osteoblasts and chondroblasts in response to growth factors, and the osteogenic properties of bone grafting that support the formation and growth of new bone.14–16 This approach allows for load shifting during weight-bearing activities and ensures biocompatibility with host tissues.17–19 BTE is rapidly evolving as a solution for bone defects of varying sizes, centering on the fabrication of scaffolds that provide a biological and mechanical framework for cell adhesion, differentiation, and mineralized matrix deposition.20,21 In recent years, the research frontier in BTE has shifted from inert structural supports to the development of “integrated bioactive scaffolds” capable of actively responding to the complex physiological environment. By incorporating bioactive components (such as metal ions, growth factors, or therapeutic drugs) into biomimetic porous structures, researchers have achieved precise regulation of the bone regeneration process. In-depth in vitro studies have elucidated their multi-faceted mechanisms of action: for instance, Yoda1-loaded polycaprolactone microfibrous scaffolds promote osteogenic differentiation by activating the Piezo1-F-actin signaling axis;22 non-linear metamaterial scaffolds induce tissue strain conducive to bone repair through their unique mechanical design;23 manganese dioxide (MnO2)-loaded scaffolds exhibit excellent reactive oxygen species (ROS) scavenging capacity, thereby protecting cells from oxidative stress-induced damage and promoting osteogenic differentiation;24 furthermore, pH-responsive tea polyphenol-magnesium nanoscale scaffolds can intelligently release antibacterial/osteogenic components and polarize macrophages towards a pro-regenerative M2 phenotype.25 The clarification of these in vitro mechanisms provides a solid foundation for in vivo applications. Animal model studies have confirmed that such functionalized scaffolds significantly enhance bone regeneration by ameliorating the immune microenvironment and promoting angiogenesis. For example, non-linear metamaterial scaffolds have been demonstrated to substantially increase the mineralized area in large segmental bone defects.23 Notably, this strategy also shows great potential for post-resection bone defect repair in osteosarcoma: sonodynamically activated Ir-TiO2/hydroxyapatite scaffolds can generate ROS within the acidic tumor microenvironment to ablate cancer cells, while simultaneously alleviating hypoxia in the neutral bone defect area to facilitate repair.26 Moreover, reprogramming tumor-associated macrophages and other immunomodulatory mechanisms opens new avenues for achieving synergistic anti-tumor and osteogenic therapy.27 Collectively, these systematic studies establish an “ in vitro mechanism exploration - in vivo functional validation” paradigm, highlighting the core value of bioactive scaffolds in guiding functional regeneration through multi-dimensional modulation of the bone microenvironment, thereby laying a robust foundation for advancing their clinical translation. Consequently, bone-engineered scaffolds infused with active ingredients represent a promising strategy for the repair of bone defects. This narrative review aims to synthesize the current landscape of the rapidly evolving field of bone tissue engineering, with a particular focus on the design and efficacy of scaffolds incorporating bioactive components. To this end, a systematic literature search was conducted to identify relevant articles published between 2015 and 2025, placing a strong emphasis on recent advances (2020–2025). The search was performed across PubMed, Web of Science Core Collection, and Scopus using customized query strings that combined keywords from the following categories: bone defects (eg, “bone defect” OR “bone regeneration”), scaffold technology (eg, “bone scaffold” OR “3/4D printed scaffold” OR “intelligent scaffold”), and bioactive components (eg, “bioactive” OR “growth factor” OR “exosome” OR “BMPs” OR “natural polymers” OR “traditional Chinese medicine”). This rigorous methodology ensures a comprehensive and contemporary overview, enabling this review to delineate the characteristics of ideal bone scaffolds, critically evaluate the advantages and limitations of current bioactive strategies, and highlight key challenges and future directions in the field.
Xenograft Bone Scaffolds
To fully comprehend the tools utilized in bone regeneration therapy, it is essential to understand mechanisms underlying bone repair and regeneration. Bone trauma triggers a cascade of events involving the simultaneous interaction of various growth factors, cells, and the extracellular matrix (ECM).28 Bone repair and regeneration can be divided into three distinct phases: ① Inflammatory phase: Following a fracture, a fibrin-rich clot is formed, which releases cytokines that recruit inflammatory cells, including lymphocytes, macrophages, eosinophils, and neutrophils, to the injury site.29 Concurrently, growth factors such as fibroblast growth factor (FGF), platelet-derived growth factor (PDGF), produced by inflammatory cells, stimulate the proliferation and differentiation of MSCs to initiate the repair process and enhance fracture healing.30 ②Fibrovascular phase: This phase is characterized by vascular remodeling and the recruitment of MSCs, which differentiate into chondrocytes and osteoblasts to facilitate bone regeneration.31 ③ Bone formation phase: following the fibrovascular phase, the MSCs present in the callus differentiate into osteoblasts or chondrocytes, thereby accelerating bone formation (Figure 1).28 Osteoclast-mediated bone degradation produces bone isolating factors such as transforming growth factor-beta (TGF-β), along with other essential factors (complement 3a, Wnt10b, BMP-6, and SLIT3) that are critical for osteogenesis.32 The final stage of fracture repair involves the reconstruction of the bone callus into mature lamellar bone.33 As one of the three major components of BTE, bone scaffolds play a crucial role in bone repair and regeneration. They are designed to promote the interaction between cells and the extracellular bone matrix,34 providing a complex micro/nano environment that mimics the ECM function of natural bone tissue.35–37 The ideal bone scaffold should possess the following characteristics: ① First, the scaffold material must be non-toxic, including its degradation products, which should be safely excreted from the body without significant impact on other organs.38 ② It should feature customizable shapes and adequate mechanical properties to provide structural support for specific bone defects, while also exhibiting highly porous 3D structures that facilitate a suitable microenvironment for ECM formation, cellular activity, oxygen diffusion, nutrient delivery, and waste removal.39,40 ③ The scaffold should be biodegradable, with a degradation rate that aligns with the rate of bone formation. Rapid degradation may lead to the loss of scaffold integrity before ECM formation, resulting in mechanical instability, while slow degradation could restrict cell infiltration and nutrient exchange, thereby delaying new bone growth.41–43 ④ The scaffold should be osteoconductive, allowing primary bone and progenitor cells to adhere to and migrate across rough surfaces, ultimately proliferating and laying down new matrix.44 ⑤ It should also be osteoinducible, capable of gradually releasing inducers that promote vascularization and osteogenesis, while recruiting progenitor cells through biomolecular signaling to stimulate new bone formation.37,45 ⑥ It should be biocompatible to minimize the risk of adverse or inflammatory reactions.46 ⑦ Furthermore, it should have the appropriate porosity of the scaffold, the level of porosity in the scaffold directly affects cell attachment, biodegradation, drug release rate, and angiogenesis, pore sizes exceeding 300 µm appear to promote the formation of new bone and capillaries, whereas pore sizes smaller than 100 µm may hinder mass transport and cell migration. Generally, smaller pore sizes (less than 75 µm) are conducive to the formation of fibrous tissues, while intermediate pore sizes (75–100 µm) and larger pore sizes (greater than 200 µm) are better suited for the development of unmineralized and fully mineralized bone tissue.47–49 ⑧Finally, the scaffold should be radiographically permeable, enabling the differentiation between new bone and implanted bone scaffolds, which aids in the effective assessment of bone tissue regeneration.36,46 To enhance the biological activity of bone scaffolds, drugs, growth factors, and other biological components can be incorporated into the material during scaffold preparation. This approach offers the potential for customizing scaffolds for specific patient applications in the future (Figure 2). For example, based on calcined bovine bone, a gene-activated xenograft scaffold was developed to deliver CKIP-1 siRNA, silencing a key negative regulator of osteogenesis. This action upregulates critical osteogenic markers (ALP, COL-1, OCN, BMP-2, Runx2), thereby enabling rapid bone defect repair and high-quality regeneration without compromising biosafety.50 A systematic review have similarly shown that decellularized xenograft bone scaffolds, by significantly mitigating immunogenicity and enhancing bone regeneration coupled with their innate porous and osteoconductive nature, represent a highly promising, cost-effective, and accessible alternative to autologous bone grafts.51
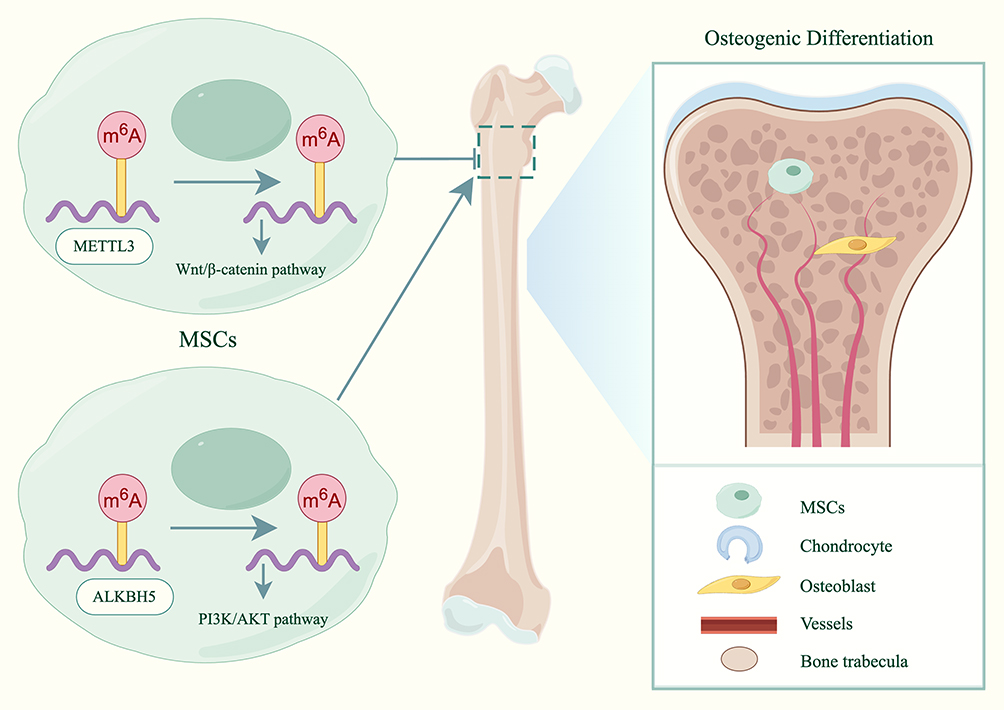 |
Figure 1 Schematic representation of representative pathways influencing MSCs osteogenesis. (By FigDraw). Abbreviation: MSC, mesenchymal stem cells. |
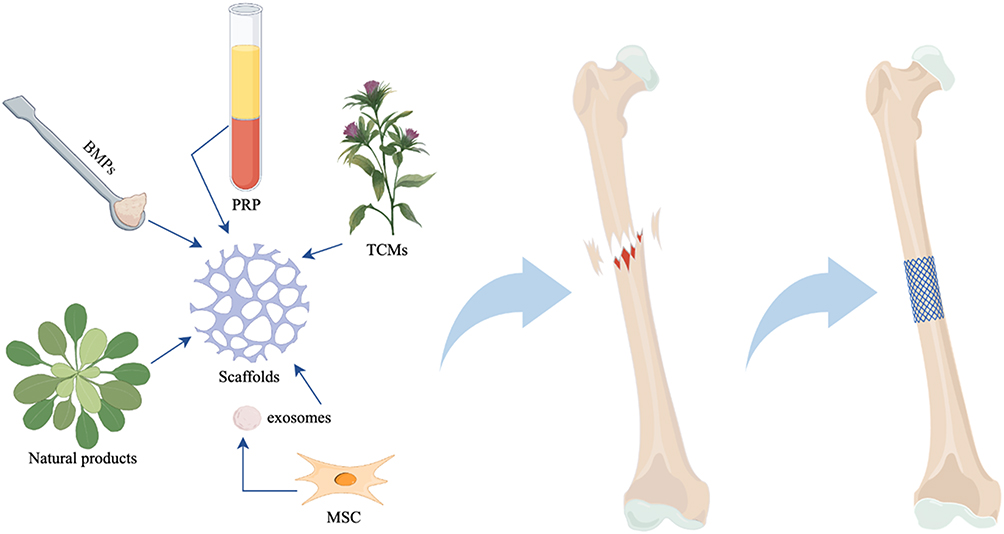 |
Figure 2 Schematic representation of repairing bone defect with scaffold as carrier and loading various active ingredients. (By FigDraw). Abbreviations: BMPs, bone morphogenetic proteins; MSC, mesenchymal stem cells; RPR, platelet-rich plasma; TCMs, Traditional Chinese Medicine ingredients. |
Combined with Bone Morphogenetic Proteins
Since Urist’s discovery of bone morphogenetic protein (BMP) from demineralized bone matrix(DBM),52 there has been no single class of bone substitute that has been as extensively studied and published. BMPs are a group of highly conserved and structurally similar functional proteins that belong to the TGF-β family. These proteins exhibit a variety of biological activities, including the stimulation of DNA synthesis and cell replication, which subsequently promotes the differentiation of MSCs into chondroblasts and preosteoblasts, thereby inducing new bone formation.53,54 Different types of BMPs have different roles in contributing to bone and angiogenesis (Table 1).55–64
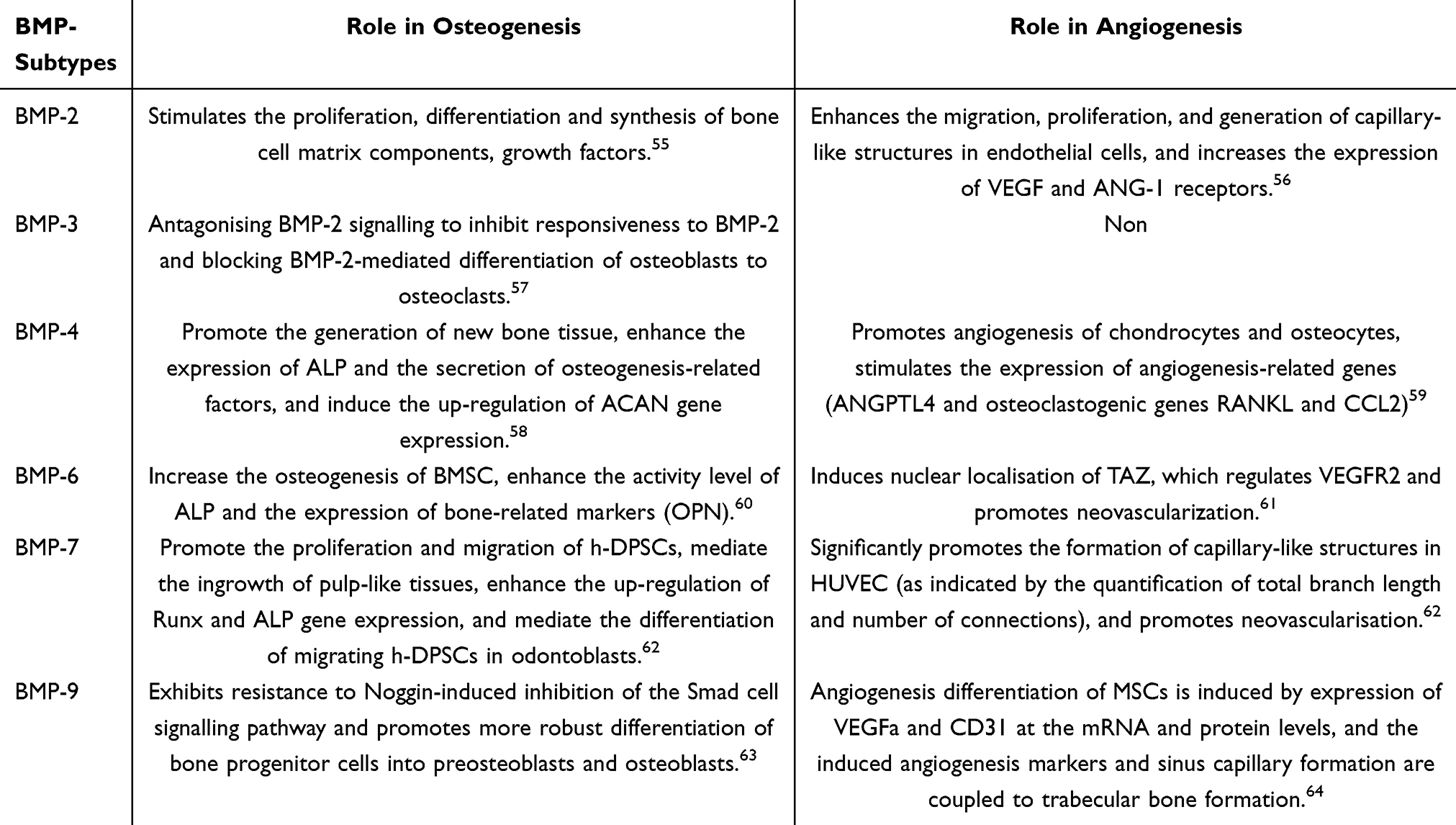 |
Table 1 The Role of Different Subtypes of BMPs in Promoting Angiogenesis and Osteogenesis |
Additionally, BMPs facilitate the differentiation of osteoclasts from hematopoietic stem cells and enhance their activity both directly and indirectly through the RANK-RANKL signaling pathway.65 BMPs play a morphogenic role in the development and maintenance of tissue structures throughout the body by stimulating the mineralization, differentiation, and survival of osteoblasts, which are crucial for maintaining healthy bone.66,67 Among the BMP family members, BMP-2, BMP-4, BMP-6, and BMP-7 are significant coordinators of MSCs, bone marrow (BM) stromal cells, and osteoblast precursor cells, inducing their differentiation into osteoblasts and exerting the greatest influence on osteoblast differentiation,68,69 Furthermore, BMP-2, 4 and 7 are also involved in the self-renewal and maintenance of hematopoietic stem cells (HSCs), as well as in progenitor cell expansion and hematopoietic differentiation, which are vital for hematopoiesis.70 Recombinant BMP-2 (rhBMP-2) is the most widely used osteoinductive BMP in preclinical trials, promoting bone regeneration while stimulating angiogenesis in the defect area. It has been approved by the Food and Drug Administration (FDA) as an osteoinductive growth factor for clinical applications.71 Osteoinductive devices containing rhBMP-2 and bovine collagen carriers have been approved for anterior lumbar interbody fusion (ALIF), acute tibial fractures, and maxillofacial reconstruction.72–75 Gonzaga et al76 evaluated the repair of cranial bone defects associated with rhBMP-2 in rats, utilizing autografts, allograft bone, and xenograft bone. Their findings demonstrated that rhBMP-2 significantly improved bone repair when administered alone or in conjunction with various types of bone grafts. Similarly, Issa et al77 conducted comparative studies that indicated different graft types enhanced bone formation, primarily attributed to rhBMP-2, thereby accelerating the repair process. Echoing these findings, Cohen et al78 elucidated the dual role of different bone graft materials as rhBMP-2 carriers in modulating the bone regeneration microenvironment: on the one hand, the bone scaffolds (particularly alloplast) potently activate osteoblasts by sustaining the long-term release of rhBMP-2, directly promoting bone formation; on the other hand, scaffolds (such as xenograft) can also modulate the immune response of neutrophils via rhBMP-2, thereby fostering a more tolerant local environment for bone regeneration. Consequently, the capacity of different graft materials to enhance bone formation stems not only from their delivery of rhBMP-2 but is also closely linked to the immunomodulatory properties they confer. Pecin et al79 implanted a mixture of autologous blood clots containing rhBMP-6 and ceramic particles into a pet dog with a multi-segment defect of approximately 3cm in the right front leg, resulting from a gunshot wound. A follow-up examination four months post-treatment revealed that the dog’s leg function was nearly fully restored. Concurrently, CT slice analysis of the affected leg indicated recovery, cortical re-bridging, and even renewal of the medullary canal. Su et al80 employed a collagen-hydroxyapatite (CHA) nanocomposite scaffold to load BMP-2, which was then implanted into the femoral defect of rabbits. Micro-CT and histological staining results demonstrated that bone formation occurred more rapidly compared to controls lacking rhBMP-2, achieving a higher degree of mineralization. Moreover, rhBMP-2 not only accelerated and enhanced bone formation but also expedited the degradation of CHA. This further corroborates that BMPs are both necessary and sufficient for ectopic bone induction and serve as potent agents for the repair of large in situ bone defects.81 However, BMPs are soluble proteins, and therapeutic doses of BMP can easily diffuse into surrounding tissues before reaching the defect site. Increasing the dose to sustain bone production in the body may lead to significant side effects, such as hematoma, inflammatory reactions, and heterotopic ossification.82,83 Consequently, BMPs require a carrier system capable of accurately delivering BMPs to the defect site, better maintaining BMP concentration, and facilitating prolonged BMPs release.84,85 An increasing body of research has demonstrated that the combination of BMPs with various types of scaffolds in BTE can not only maximize BMPs affinity, but also optimize bone repair and regeneration to the greatest extent (Table 2).86–95
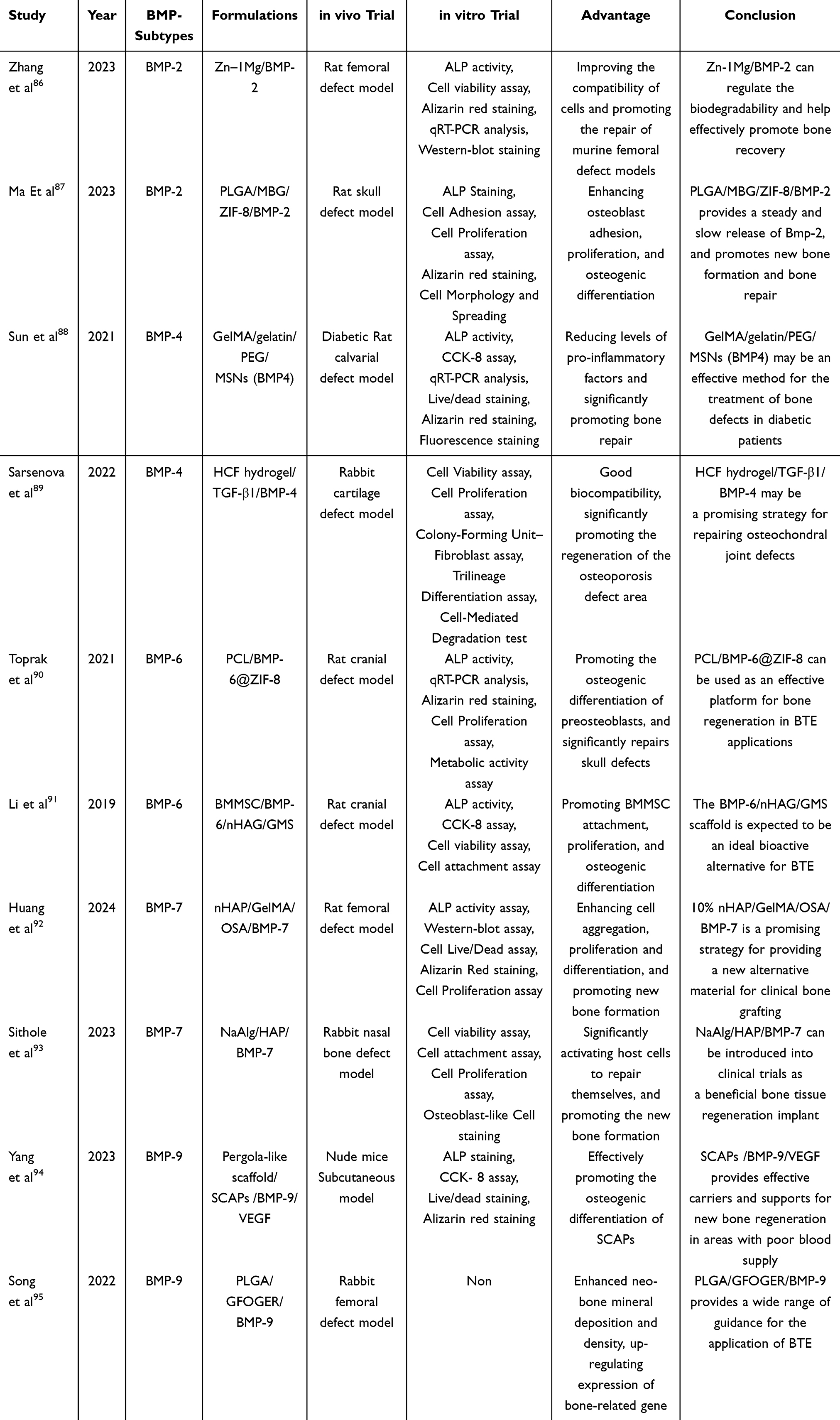 |
Table 2 BMPs Combined with Various Types of Scaffolds in BTE are Reported in the Literature |
Combined with Platelet-Rich Plasma
Platelet-rich plasma (PRP) is a platelet concentrate obtained through the centrifugation of peripheral blood from allogeneic or autologous sources.96,97 It contains platelet concentrations that are 3 to 10 times higher than those found in blood (exceeding 1×109 platelets/mL). This concentrate is rich in fibrin, platelets, and a variety of growth factors, including PDGF-AA, PDGF-BB, PDGF-AB, TGF-β1 and TGF-β3, vascular endothelial growth factor (VEGF), basic fibroblast growth factor (BFGF) and insulin-like growth factor (IGF), which are released upon activation through several methods, such as calcium chloride, thrombin, and soluble type I collagen (COL1).98–100 In related studies, PDGF has been shown to promote angiogenesis, macrophage activation, fibroblast proliferation, chemotaxis, collagen synthesis, and osteocyte proliferation. TGF is involved in the proliferation of fibroblasts, synthesis of COL1 and fibronectin, induction of bone matrix deposition, and inhibition of bone resorption. PDGF can stimulate epidermal regeneration, keratinocyte proliferation, and dermal fibroblast activity to enhance wound healing, as well as promote the production and action of other growth factors. VEGF stimulates vascular endothelial cell vascularization, while IGF exerts a chemotactic effect on fibroblasts, stimulates protein synthesis, and promotes bone formation.101 These growth factors collectively endow PRP with a wide range of regenerative functions, including stem cell proliferation and recruitment, cytokine activation, modulation of fibroblast pathways, regulation of local inflammatory and fibrotic responses, and stimulation of neovascularization.102,103 Furthermore, PRP has demonstrated protective effects against chondrocyte apoptosis, inhibition of the inflammatory process, enhancement of cartilage repair, and stimulation of the migration and chondrogenic differentiation of human subchondral progenitor cells.104,105 These properties have been reported in clinical studies across various medical fields, including orthopedics, plastic surgery, dermatology, and oral implantation.106 Yu et al107 investigated the potential of autologous PRP as a bone inductive factor to enhance bone induction and promote bone regeneration by combining bone marrow-MSCs withβ-tricalcium phosphate (β-TCP) ceramics. The results indicated that MSCs exhibited robust proliferation at all time points when exposed to autologous PRP. Furthermore, osteogenic ability tests revealed that the synthesis levels of alkaline phosphatase (ALP) activity and osteocalcin (OC) were significantly elevated after 7 and 14 days of culture. Several in vitro studies have also demonstrated that the inclusion of PRP enhances MSC proliferation, suggesting that PRP could serve as a valuable adjunct to MSC and fresh demineralized bone (FDB) grafts.108 Variations in concentration lead to differences in the ability to stimulate chemotaxis (directed cell migration) and overall migration rates in MSCs. Holmes et al109 examined the effects of varying concentrations of PRP and bone marrow concentrate (BMC) on MSCs chemotaxis, revealing that all biologics significantly increased the percentage of MSC migration, with no notable differences observed between BMC and high-concentration PRP when compared to low-concentration PRP. Although naturally prepared PRP is theoretically effective in promoting bone tissue regeneration, it is typically administered in the form of a liquid gel, which may not adequately meet the spatial size and mechanical strength requirements necessary for effective bone regeneration.110 Liu et al111 developed a method incorporating PRP-gel, human umbilical cord mesenchymal stem cells (HUMSC), and nanohydroxyapatite, utilizing a novel tissue-engineered bone graft composed of polyamide 66 (nHA-PA66). This study aimed to investigate whether the composite scaffold could enhance angiogenesis and the bone repair capacity in rat femoral large bone defects (LBD). The results demonstrated that the composite scaffold significantly promoted both angiogenesis and bone regeneration in rat LBD, suggesting its potential for further application in the clinical treatment of LBD. A prospective clinical study confirms that the combination of platelet-rich fibrin (PRF) and deproteinized bovine bone mineral (DBBM) safely and effectively achieves horizontal maxillary ridge augmentation, leveraging PRF’s adhesive properties and healing-promotion capacity to enable significant bone gain without conventional barrier membranes and with zero complications.112 Similarly, Hao et al113 created a personalized PCL/β-TCP/PRP active scaffold layer through 3D printing, utilizing bioink derived from the patient’s autologous PRP. This scaffold was applied to patients for the repair and reconstruction of bone defects following tibial tumor resection. The findings indicated that leveraging the combination of PRP and 3D printing technology could lead to significant clinical advancements compared to traditional bone implant materials. However, another study revealed that the combination of PRP and PuraMatrix did not effectively promote bone regeneration.114 The conflicting outcomes regarding the efficacy of PRP in enhancing osteogenic activity may be attributed to various factors, including differences in PRP preparation protocols, concentrations, animal models, the use of autologous versus allogeneic applications, and methods of administration.115,116 The healing and regeneration of bone tissue is a prolonged process that typically requires 3 to 6 months to achieve sufficient strength. To ensure the sustained release of essential growth factors, which maximizes their regenerative potential, it is necessary to incorporate a scaffold with a controlled-release system for PRP.117 Additionally, the bioactive molecules present in PRP play a crucial role in BTE, and their synergistic combination with MSCs after encapsulation within the scaffold demonstrates a promising effect on osteogenesis.118 In conclusion, PRP holds significant potential for applications in BTE.
Combined with Natural Products
Natural products are polymers derived from plants, animals, or microorganisms, primarily including: chitosan, collagen, alginate, cellulose and hyaluronic acid. These materials provide natural cell adhesion sites, mimic the natural ECM of bone, and yield non-cytotoxic degradation products such as carbon dioxide and water.119,120 Natural products are characterized by their convenient extraction, renewability, biodegradability, excellent plasticity, superior biocompatibility and minimal adverse immune effects. As such, they represent an emerging class of materials in the field of biomedicine, with widespread applications in the preparation of BTE scaffold materials. However, due to their large molecular weight, the hydrolysis of these polymers into non-toxic product can be time-consuming.121 For instance, chitosan, a well-known natural polymer sourced from the ocean, serves not only as a scaffold component but also as a therapeutic delivery platform to facilitate bone and cartilage repair both in vitro and in vivo.122 Chitosan can be chemically modified and functionalized with various bioactive materials, including organic molecules and inorganic nanoparticles, to achieve synergistic osteogenesis. Notably, chitosan-based organic matrices can function as templates to regulate the in situ growth of hydroxyapatite (HAP). Additionally, chitosan scaffolds can serve as controlled-release platforms to deliver potent osteoinductive molecules and functional bioactive ions, or can be combined with responsive materials to enhance bone regeneration through exogenous physical stimulation.123 Soriente et al124 prepared chitosan/hydroxyapatite (CS/HA) composite scaffolds featuring a three-dimensional porous structure derived from chitosan, utilizing a combination of the sol-gel method and freeze-drying technique. This approach elicited a favorable biological response in the osteogenic differentiation of human mesenchymal stem cells (hMSCs) into the osteoblast phenotype. Collagen, which is abundantly present in the ECM of various natural tissues such as dentin, bone, skin, tendons, pancreas and cartilage, exhibits a high swelling index and low antigenicity.125 However, its inadequate mechanical properties restrict its direct application as a bone substitute, leading to the development of various high-strength composite scaffolds that incorporate collagen.121 The collagen-based composite scaffolds have been shown to enhance the maintenance and function of cultured osteoblasts in vitro, promote matrix mineralization, and elevate the activity of alkaline phosphatase (ALP) osteoblastase.126 Furthermore, scaffolds implanted in vivo demonstrate significant osteogenic properties in critical bone defects.127 Tsai et al128 prepared a COL-HANF composite scaffold utilizing collagen and Hap-CaO fibers (HANFs), and confirming the composite scaffold’s potential for in bone tissue regeneration through both in vivo and in vitro experiments. Alginate(Alg), a marine-derived polysaccharide, is a sodium and/or potassium salt of alginic acid extracted from brown algae, consisting of polymers with varying concentrations of d-manuronic acid (M) and glucuronic acid (G) residues.129,130 Naruphontjirakul et al131 prepared a composite scaffold of zinc-containing and strontium sol-gel-derived bioactive glass nanoparticles (Zn-Sr-BGNP) incorporated into Alg. This study confirmed that the composite scaffold significantly promotes biological activity, increases osteocyte proliferation, enhances calcium deposition, and facilitates cell attachment, demonstrating great potential for bone tissue regeneration and repair. Complementing the approach of enhancing alginate scaffolds with bioactive inorganic ions, the study by Hamrun et al132 demonstrates that an optimal combination of chitosan, alginate, and fucoidan creates a fully organic scaffold with superior porosity (86.86% porosity), biocompatibility (0.43% hemolysis), and inherent osteogenic activity, driven by fucoidan-mediated upregulation of key bone markers like BMP-2. Cellulose, a linear polysaccharide widely found in various natural sources such as cotton, bast plants, wood, and bamboo, as well as in certain organisms like bacteria, fungi, and algae, is one of the most common polysaccharides utilized for creating bone substitutes.133 Cellulose and its derivatives have been extensively employed to deliver growth factors and antibiotics directly to damaged bone tissue, thereby promoting tissue repair and presenting broad application prospects in bone tissue engineering.134 Patel et al135 developed biodegradable cellulose nanoparticle-reinforced chitosan/silk fibroin (CS/SF/CNPs) scaffolds through 3D printing and characterized them using various spectroscopic techniques. Enhanced bone regeneration was observed in a rat calvarial defect model, confirming this composite scaffold as a promising material for bone healing applications. In summary, leveraging the structural characteristics and performance advantages of natural products in combination with other biomaterials to achieve mutual complementarity and synergistic promotion will facilitate the design of more effective composite scaffolds for bone repair and regeneration (Table 3).136–148
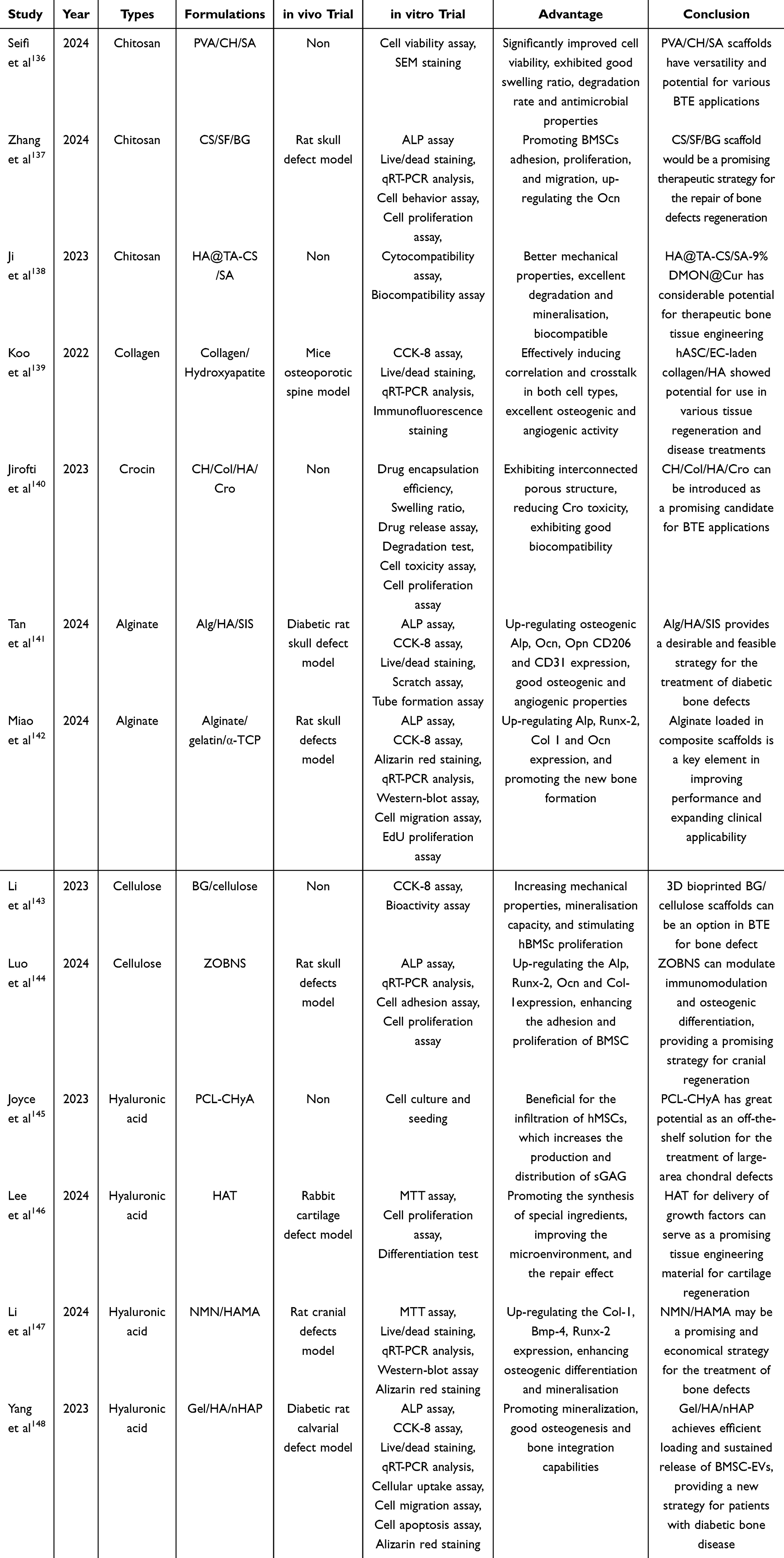 |
Table 3 Natural Products Combined with Scaffolds in BTE are Reported in the Literature |
Combined with Traditional Chinese Medicine Ingredients
Traditional Chinese Medicine ingredients (TCMs) are widely sourced from herbs, animals, and minerals found in nature. Their unique chemical structures confer distinct pharmacological activities, and their ease of extraction and preparation often makes them more cost-effective. Furthermore, the active components of TCMs are generally considered safe alternatives to some synthetic drugs, potentially reducing long-term side effects, a claim supported by centuries of application within the Chinese population.149,150 Pharmacological studies have fully demonstrated the significant potential of TCMs in bone tissue regeneration. Its role extends beyond merely preventing or alleviating osteoporotic symptoms to achieving systemic regulation of bone homeostasis through multi-component and multi-target synergistic mechanisms. On one hand, active constituents of TCMs directly act on bone cells by activating key osteogenic transcription factors such as Runx2 and upregulating osteogenic markers like osteocalcin, while simultaneously modulating the RANKL/RANK/OPG/Wnt/β-catenin signaling axis to suppress osteoclast activity, thereby precisely balancing bone metabolic processes (Figure 3). On the other hand, they improve the pathological bone microenvironment by inhibiting inflammatory responses, mitigating oxidative stress, and exerting estrogen-like effects. These estrogenic actions further enhance intestinal calcium absorption, reduce calcium excretion, and stimulate calcitonin synthesis, collectively contributing to increased bone mineral density.151,152 One notable example is Icariin (ICA), a flavonoid that activates the ER-α-Wnt/β-catenin signaling pathway. This activation is specifically linked to osteoblast proliferation and differentiation, enhancing mineralization and the expression of bone-related genes and proteins. Additionally, ICA induces bone formation by inhibiting the transformation of osteoblasts into adipocytes and the formation and differentiation of osteoclasts.153,154 In earlier related experiments, researchers soaked porous β-TCP in an ICA solution and subsequently implanted it deep into the dorsal muscles of rats. After three months, it was observed that this treatment promoted the proliferation and differentiation of rat Ros17/28 cells and induced new bone formation, while no significant osteogenesis was detected in the control group.155 Additionally, ICA, due to its estrogen-like structure, binds to estrogen receptors and promotes angiogenesis by stimulating endothelial cell migration, proliferation, and tubular formation, thereby influencing bone metabolism.156 One study demonstrated that ICA increased the expression of VEGF in rat adipose-derived stem cells (ASCs), with a concentration of 10–7 M ICA yielding the most pronounced effect in promoting VEGF secretion in ASCs. VEGF exerts a paracrine effect between ICA-induced ASCs and rat endothelial progenitor cells (EPCs), confirming that scaffolds incorporating ICA possess significant osteogenic and angiogenic potential.157 Beyond this, Icariin also directly promotes osteogenic differentiation in Osteonecrosis of femoral head (ONFH) through a synergistic mechanism. Research indicates that it initiates this process by activating the PI3K/AKT pathway, which induces epigenetic reprogramming—specifically, the upregulation of UTX and downregulation of EZH-2. This reduces global H3K27me3 levels, ultimately promoting the expression of key osteogenic genes like RUN-2 and BMP-2.158 However, ICA has low bioavailability and a short half-life (1–2 hours), making it prone to the loss of bioactive components in a fluid environment, and the molecule is easily eliminated from the body.159 Given the duration required for bone repair and healing (3–6 months), it is crucial for BTE to consider combining ICA with appropriate carriers to achieve long-term administration and stable drug release concentrations that to act on surrounding tissues. To delay the release rate of ICA, researchers utilized ICA CS/nHA microspheres, which also provide a suitable microenvironment for the attachment and proliferation of osteoblasts.160 In an experiment investigating a model of tibial plateau defects in adult rabbits, researchers developed a core scaffold containing ICA chitosan microspheres using freeze-drying technology. They conducted 3D CT reconstruction of the tibial plateau bone defect post-implantation at 4 to 12 weeks, which demonstrated osteogenesis in the area of composite scaffold implantation. Additionally, there was an observed increase in the expression of bone mineral density (BMD), connective density (Conn.Dn), ALP, COL1, osteopontin (OPN), and osteocalcin (OC), as assessed through histological and histochemical evaluations.161 However, to effectively implement TCM in the treatment of bone diseases, several issues should be addressed: ① lot-to-lot heterogeneity and reproducibility, ② determination of effective dosage, ③ purity and potential unknown toxicity, and ④ lack of uniform standards. Enhancements in previous methodologies will minimize variability between TCM batches by eliminating impurities and isolating the desired active compounds. Furthermore, TCM-based clinical and preclinical trials should focus on dose optimization, confirmation of toxicity ranges, and the expansion of knowledge regarding pharmacological mechanisms and interactions associated with TCM. Therefore, a comprehensive understanding of the relationship between implantable stents and TCM, along with process optimization and drug loading strategies, is essential (Table 4).162–175
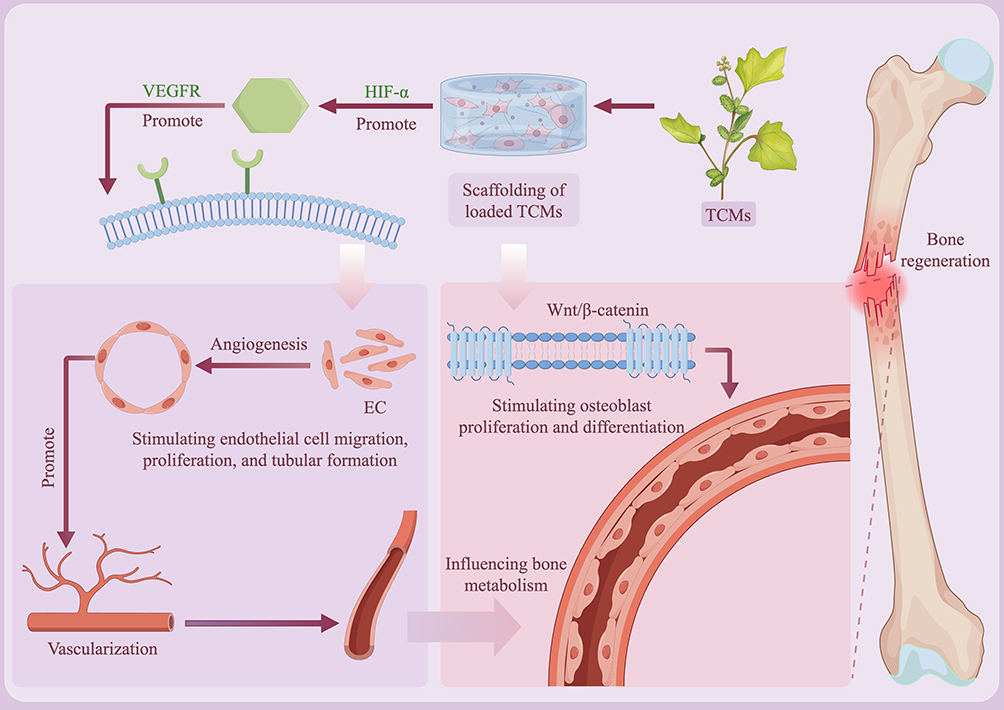 |
Figure 3 Schematic representation of the effects of TCMs on vascularization and osteogenesis, taking ICA as an example. (By FigDraw). Abbreviations: EC, Endothelial Cell; HIF-α, Hypoxia-inducible factor –α; TCMs, Traditional Chinese Medicine ingredients; VEGFR, vascular endothelial growth factor receptor. |
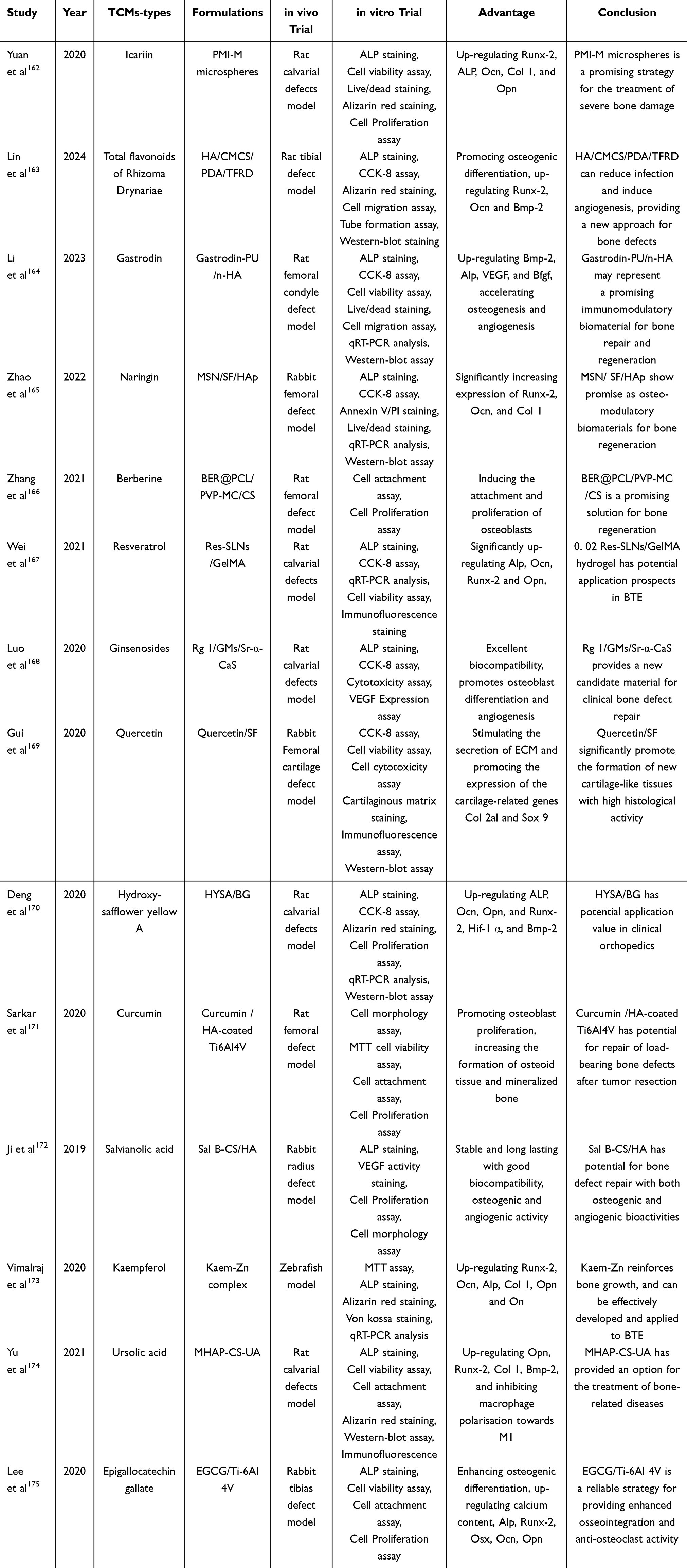 |
Table 4 Representative TCMs Combined with Scaffolds in BTE are Reported in the Literature |
Combined with Exosomes
MSCs play a crucial role in bone repair and regeneration. Their significance lies primarily in two aspects: their ability to migrate to and home in on the site of injury, and their capacity to differentiate into osteoblasts and chondroblasts, ultimately maturing into osteocytes and chondrocytes. This differentiation is essential for the reconstruction and repair of bone tissue defects.176 Furthermore, MSCs possess unique immunomodulatory properties that enable them to evade recognition by the immune system, thereby avoiding attacks from the host’s immune response.177 Additionally, MSCs may enhance bone regeneration by modulating the microenvironment, with the release of paracrine factors and specific microRNAs also contributing to their differentiation.178 Despite the substantial number of clinical trials investigating MSC-based therapies, no single approach has yet received approval for the treatment of bone defects. The clinical application of MSCs for bone repair and regeneration encounters several significant challenges.179 First, there is a need to improve the effectiveness of MSC implantation and their survival at bone defect sites.180 Second, it is crucial to prevent to avoid unnecessary differentiation of MSCs during ex vivo expansion.181 Third, strategies should be developed to apply MSCs to larger bone defects without compromising their biological efficacy.182 Lastly, ethical concerns surrounding MSC-based therapies must be addressed, particularly regarding the potential risk of tumorigenesis.183 As noted, there is increasing evidence that MSCs exert their effects primarily through paracrine mechanisms, with a growing focus on MSC-derived vesicles, various factors (including chemokines, growth factors, and cytokines), ECM, and metabolites that are instrumental in tissue repair and regeneration.184 Extracellular vesicles (EVs) from diverse cellular sources orchestrate key processes in bone regeneration, including osteogenesis, angiogenesis, and immunomodulation. Specifically, EVs derived from mesenchymal stem cells promote osteogenic differentiation via miRNAs such as miR-21 and miR-26a, enhance angiogenesis through factors like HIF-1α and VEGF, and induce M2 macrophage polarization via miR-451a. Osteoclast-derived EVs facilitate bone formation via miR-324 and RANKL reverse signaling, while stimulating vessel formation through PDGF-BB, thereby mediating the “coupling” between bone resorption and formation. Moreover, osteocyte-derived EVs act as mechanical signal carriers to enhance osteogenic potential, and immune cell-derived EVs, such as those from M2 macrophages, activate the BMP2/Smad5 pathway via miR-5106, collectively supporting bone healing.185 MSc-derived exosomes are nanoscale, lipid bilayer- encased structures capable of transporting functional biological macromolecules, including proteins, lipids, RNA, growth factors, and cytokines. These exosomes have garnered significant interest due to their ability to convey information to both adjacent cells and those located distantly from their origin, thereby influencing cellular functions.186,187 Exosomes possess several advantages, such as the capacity to traverse biological barriers into deep tissues, promote regeneration, induce stem cell differentiation, and trigger specific immune responses (Figure 4). Additionally, they demonstrate a natural targeting ability, along with favorable properties including biodegradability, biocompatibility, and stability, which contribute to their safety concerning tumorigenicity and immunogenicity.188–190 The beneficial effects of MSC-derived exosomes on bone repair and regeneration may arise from: ① the direct regulation of osteogenic differentiation in adjacent target cells, facilitated by the activation of MSC exosomes, through various signaling cascades (including BMP/Smad, Wnt/β-catenin, and PI3K/AKT), which induce the proliferation and differentiation of osteoblasts, as well as the recruitment of endogenous MSCs to the site of bone defects, thus promoting bone regeneration.191–193 ② the stimulation of local angiogenesis and inhibition of bone resorption to repair bone defects, where the activation of the AKT/mTOR signaling pathway may enhance osteogenesis, optimizing the microenvironment and creating ideal conditions for bone regeneration.194–196 However, exosomes may be are captured by the reticuloendothelial system or rapidly cleared by the mononuclear phagocyte system in vivo, leading to short retention time and insufficient effective concentration at the lesion site, thereby impairing their regeneration and repair capabilities.197 Additionally, the inherent limited targeting capacity of exosomes makes it difficult to precisely deliver their therapeutic cargo to specific injury sites, which severely restricts their reparative efficacy. By employing engineering strategies such as genetic editing and surface modification to optimize their targeting ability and cargo, combined with advanced delivery systems like hydrogels and 3D-printed scaffolds to achieve localized controlled release, their therapeutic efficacy can be significantly enhanced.198,199 Wan et al200 demonstrated that a composite scaffold composed of the natural polysaccharides gelatin and hyaluronic acid serves as an efficient delivery system for exosomes. By sustaining the release of TGF-β from the exosomes, the scaffold activates the PI3K/Akt signaling pathway, thereby synergistically enhancing osteogenic differentiation and angiogenesis, which ultimately accelerates bone regeneration and repair in a bone defect model. Similarly, Luo et al201 developed a dual-biomimetic system integrating a 3D-printed trabecular-mimetic Ti-6Al-4V scaffold (BTPS) with hypoxia-induced exosome-loaded PEGDA/GelMA microspheres (PGHExo). The BTPS replicated native bone’s geometry and mechanical properties, effectively mitigating stress shielding. Sustained release of exosomes from the microspheres activated key pathways (including MAPK, mTOR, HIF-1, and VEGF), synergistically enhancing osteogenesis and angiogenesis. This combined structural and biochemical strategy significantly improved in vivo bone regeneration and neovascularization, highlighting the powerful synergy between 3D-printed porous scaffolds and exosome-based delivery in bone tissue engineering. The emergence of composite scaffold materials in BTE can further extend the characteristics of exosomes and optimize their application in bone repair and regeneration. However, several key challenges remain, such as the isolation and purification of exosomes, and there is a lack of a unified, efficient, and convenient method to ensure that the isolated exosomes possess standardized characterization and quality control.202 Furthermore, unclear regulatory pathways and the absence of long-term safety evaluation systems collectively represent critical barriers to the broad clinical application of exosomes.199 Additionally, although exosome-loaded scaffold composites have achieved a certain degree of slow release, the optimal release rate for bone regeneration has yet to be explored, Nonetheless, this area remains a promising field for bone repair and regeneration.203
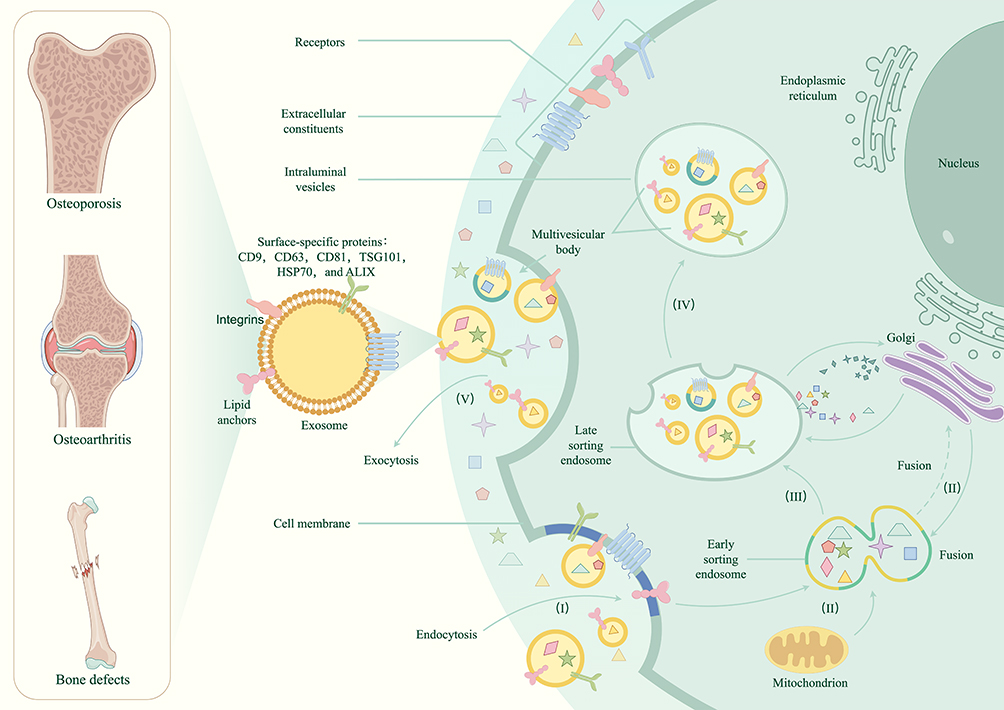 |
Figure 4 Schematic representation of exosome formation and its effect on osteogenesis and cartilage. (By FigDraw). |
Challenges and Prospects
As one of the three core elements of BTE, scaffolds play a crucial role in enhancing cell viability, increasing cell attachment area, facilitating homing, promoting osteogenic differentiation, ensuring host integration, and providing load-bearing support.38 Consequently, a wide variety of scaffold composites have been developed. The combination of an active ingredient or drug with osteogenic potential and a scaffold significantly enhances the effectiveness of bone repair and regeneration. However, these bioactive material-loaded scaffold systems face challenges in the in vivo/vitro environment. The “bioactive” evaluation is reduced to in vitro ALP staining or ex vivo Micro-CT bone mass, and this “cell-molecule game” is severely disconnected from clinical function recovery. Key indicators such as nerve regeneration, mechanical adaptive remodeling, and metabolic homeostasis regulation are missing. It is necessary to establish a “full-dimensional biological activity” evaluation system, including structure (integration of bone-scaffold interface), function (recovery of ability to contrast lateral construction), metabolism (dynamic monitoring of calcium and phosphorus homeostasis), and system regulation (level of systemic inflammatory factors). In addition, traditional studies have focused too much on the direct regulation of MSCs and osteoblasts, while ignoring that macrophage polarization (M1/M2) is the “switch” of bone regeneration. Lack of immune microenvironment responsive loading scaffolds can lead to a vicious cycle of chronic inflammation, fiber encapsulation, and repair failure after implantation. Therefore, scaffold design needs to shift from “osteogenesis-centric theory” to “immune-osteogenic coupling theory”, and immunomodulators should be listed as the core active components in parallel with BMPs, and angiogenesis, stem cell homing and osseointegration repair cascades should be realized by reprogramming macrophage phenotypes.204,205 The long-term treatment of orthopedic-related diseases necessitates the maintenance of good stability and compatibility between the loaded active ingredient and the scaffold, as well as enduring effectiveness to achieve a synergistic effect greater than the sum of its parts. The unknown mechanism of multifactor synergism in composite scaffolds is also another major challenge. For example, the combination of BMP-2 and VEGF can synchronously promote osteogenesis and vascularization, but the difference in the timing of the release of the two (VEGF is released earlier than that of BMP-2) significantly affects the repairing effect.206 And also for example, the multicomponent of TCMs (eg, tanshinone and panax notoginseng saponins) may exhibit synergistic effects of osteogenesis and anti-inflammation through multi-target regulation (eg, activation of the AKT pathway, inhibition of NF-κB inflammatory signaling), exhibiting synergistic effects of bone promotion.207–210 Current research predominantly adheres to a rudimentary “load-and-release” paradigm, overlooking the stage-specific temporal demands of bone healing (eg, sequential prioritization of vascularization preceding osteogenesis) and spatial heterogeneity (the difference in the microenvironment between the center and the edge of the defect). This static delivery approach leads to insufficient bioavailability of the active ingredient, while burst release-induced off-target effects may even impede repair. Next-generation bioactive scaffolds necessitate evolution toward “dynamically programmable delivery systems” that enables the spatiotemporal-precise delivery of active ingredients through smart materials, mimicking endogenous healing signal chains (eg, sequential activation from VEGF to BMP-2).211–213 Furthermore, the paradox of clinical translation, the “healing hallucination” of loaded scaffolds is mostly limited to small animal models, and the conclusion of “high cure rate” based on rodent non-weight-bearing bone defects (cranial/femoral condyle) may seriously mislead the transformation expectations, and such models cannot simulate the blood supply disorders, mechanical loads, and immunosenescence microenvironment of human weight-bearing bones. There is an urgent need to establish clinical predictive evaluation criteria, including the requirement of large animal weight-bearing models (such as sheep tibial segment defects), the inclusion of pathological microenvironment (such as diabetes/osteoporosis/infection), and the endpoint indicators focusing on functional reconstruction (such as biomechanical strength ≥ 80% of natural bone).214,215
BTE integrates multiple disciplines, including immunology, cell biology, materials science, and manufacturing, fostering multidisciplinary collaboration and innovation in the field of bone repair and regeneration. In terms of cost control and regulatory approval, the utilization of waste biomass such as crustacean shells, fish bones, and eggshells as raw materials can significantly reduce the procurement cost of biomaterials.216,217 Furthermore, the regulatory approval (such as CE mark, FDA) of natural material-based products like Bio-Oss (bovine bone-derived) and Algipore (algae-derived) paves a clear regulatory path for the development of more complex smart scaffold systems, thereby accelerating their clinical translation.217 Additionally, the introduction of 4D printing technologies enables the fabrication of personalized scaffolds that integrate microscopic active ingredient loading with macroscopic morphological adaptation.218 Studies have demonstrated that 4D-printed composite scaffolds loaded with osteogenic active components can enhance the bone defect healing rate by nearly 40–50% in animal models.219–221 The convergence of these fields generates novel ideas that enhance the clinical application of bone defect repair and regeneration. Furthermore, the advent of 3D and 4D printing technologies enables the creation of microstructures tailored for loading active ingredients, as well as macrostructures suited for bone defects of varying shapes and sizes, thereby facilitating individualized treatment. These technologies have also improved the capability of composite scaffolds to deliver osteogenic substances through the integration of external fields, such as acoustic, electric, or magnetic fields, demonstrating significant potential in BTE. With the rapid advancement of artificial intelligence (AI) technology, it is possible to combine it with multi-omics technology (genomics, proteomics, metabolomics) to systematically analyze how multiple components in TCMs (such as flavonoids, saponins, etc.) work together on osteogenesis through a complex interaction network.222 Looking ahead, the future development of composite scaffolds in bone repair and regeneration is anticipated to focus on innovations in biomaterials, intelligent design, personalized customization, bioprinting technology, the integration of tissue engineering and stem cell technologies, multifunctionality, comprehensive treatment approaches, and clinical translation. These advancements aim to establish more efficient, safe, and personalized treatment protocols for bone defect repair.
Conclusion
While the application of single active components demonstrates specific efficacy, their inherent limitations—such as side effects, poor in vivo stability, and single-target actions—often hinder their ability to mimic the complex physiological microenvironment and multi-signaling synergy inherent in bone repair. It is the clear recognition of these limitations that has driven the evolution of bone tissue engineering toward intelligent scaffold systems. The overarching goal of such intelligent scaffold design is not the crude stacking of functions, but rather the maximal activation of the body’s innate repair potential with minimal intervention. This necessitates the systematic integration of the unique advantages offered by different components: for instance, the potent osteoinductive capacity of BMPs, the safety and richness of growth factors in PRP, and the multi-target regulatory potential of natural products and TCMs. The “multimodal coordinated regulation” system built upon these elements marks a fundamental paradigm shift in bone repair strategy—from passive physical support to active biological regulation. Such a scaffold is no longer merely an implant, but a “bioactive platform” capable of precisely modulating the local microenvironment in both time and space to orchestrate the repair process. To facilitate the successful translation of this platform from concept to clinical practice, future research must concentrate on addressing several pivotal challenges: conducting robust efficacy validation in large animal models, establishing standardized characterization and quality control protocols for bioactive components (such as exosomes), and actively promoting the development of a forward-looking regulatory framework. Addressing these hurdles will accelerate the clinical adoption of this transformative technology and ultimately bring tangible hope to patients.
Data Sharing Statement
No datasets were generated or analyzed in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by National Natural Science Foundation of China (82204820).
Disclosure
The authors declare no competing interests.
References
1. Michel JP, Leonardi M, Martin M, Prina M. WHO’s report for the decade of healthy ageing 2021-30 sets the stage for globally comparable data on healthy ageing. Lancet Healthy Longev. 2021;2(3):e121–e122. doi:10.1016/S2666-7568(21)00002-7
2. Wu AM, Bisignano C, James SL, et al. Global, regional, and national burden of bone fractures in 204 countries and territories, 1990-2019: a systematic analysis from the Global Burden of Disease Study 2019. Lancet Healthy Longev. 2021;2(9):e580–e592. doi:10.1016/S2666-7568(21)00172-0
3. Kerativitayanan P, Tatullo M, Khariton M, Joshi P, Perniconi B, Gaharwar AK. Nanoengineered osteoinductive and elastomeric scaffolds for bone tissue engineering. ACS Biomater Sci Eng. 2017;3(4):590–600. doi:10.1021/acsbiomaterials.7b00029
4. Yair R, Shahar R, Uni Z. Prenatal nutritional manipulation by in ovo enrichment influences bone structure, composition, and mechanical properties. J Anim Sci. 2013;91(6):2784–2793. doi:10.2527/jas.2012-5548
5. Aguilar A, Zein N, Harmouch E, et al. Application of chitosan in bone and dental engineering. Molecules. 2019;24(16):3009. doi:10.3390/molecules24163009
6. Babilotte J, Guduric V, Le Nihouannen D, Naveau A, Fricain J, Catros S. 3D printed polymer–mineral composite biomaterials for bone tissue engineering: fabrication and characterization. J Biomed Mater Res B: Appl Biomater. 2019;107(8):2579–2595. doi:10.1002/jbm.b.34348
7. Bates P, Yeo A, Ramachandran M. Bone Injury, Healing and Grafting. Basic Orthopaedic Sciences. 2018;2018:205–222.
8. Chen X, Fan H, Deng X, et al. Scaffold structural microenvironmental cues to guide tissue regeneration in bone tissue applications. Nanomaterials. 2018;8(11):960. doi:10.3390/nano8110960
9. Alonzo M, Alvarez Primo F, Anil Kumar S, et al. Bone tissue engineering techniques, advances, and scaffolds for treatment of bone defects. Curr Opin Biomed Eng. 2021;17:100248. doi:10.1016/j.cobme.2020.100248
10. Chen CY, Chen CC, Wang CY, Lee AKX, Yeh CL, Lin CP. Assessment of the release of vascular endothelial growth factor from 3d-printed poly-ε-caprolactone/hydroxyapatite/calcium sulfate scaffold with enhanced osteogenic capacity. Polymers. 2020;12(7):1455. doi:10.3390/polym12071455
11. Ansari M. Bone tissue regeneration: biology, strategies and interface studies. Prog Biomater. 2019;8(4):223–237. doi:10.1007/s40204-019-00125-z
12. Fan L, Chen S, Yang M, Liu Y, Liu J. Metallic materials for bone repair. Adv Healthc Mater. 2024;13(3):e2302132. doi:10.1002/adhm.202302132
13. Bharadwaz A, Jayasuriya AC. Recent trends in the application of widely used natural and synthetic polymer nanocomposites in bone tissue regeneration. Mater Sci Eng C Mater Biol Appl. 2020;110:110698. doi:10.1016/j.msec.2020.110698
14. Roberts TT, Rosenbaum AJ. Bone grafts, bone substitutes and orthobiologics: the bridge between basic science and clinical advancements in fracture healing. Organogenesis. 2012;8(4):114–124. doi:10.4161/org.23306
15. Zhao R, Yang R, Cooper PR, Khurshid Z, Shavandi A, Ratnayake J. Bone grafts and substitutes in dentistry: a review of current trends and developments. Molecules. 2021;26(10):3007. doi:10.3390/molecules26103007
16. Albrektsson T, Johansson C. Osteoinduction, osteoconduction and osseointegration. Eur Spine J. 2001;10 Suppl 2(Suppl 2):S96–S101. doi:10.1007/s005860100282
17. Askari M, Afzali Naniz M, Kouhi M, Saberi A, Zolfagharian A, Bodaghi M. Recent progress in extrusion 3D bioprinting of hydrogel biomaterials for tissue regeneration: a comprehensive review with focus on advanced fabrication techniques. Biomater Sci. 2021;9(3):535–573. doi:10.1039/d0bm00973c
18. Bauer TW, Muschler GF. Bone graft materials. An overview of the basic science. Clin Orthop Relat Res. 2000;371:10–27. doi:10.1097/00003086-200002000-00003
19. Valtanen RS, Yang YP, Gurtner GC, Maloney WJ, Lowenberg DW. Synthetic and bone tissue engineering graft substitutes: what is the future? Injury. 2021;52 Suppl 2:S72–S77. doi:10.1016/j.injury.2020.07.040
20. Liu Q, Lu WF, Zhai W. Toward stronger robocast calcium phosphate scaffolds for bone tissue engineering: a mini-review and meta-analysis. Biomater Adv. 2022;134:112578. doi:10.1016/j.msec.2021.112578
21. Collins MN, Ren G, Young K, Pina S, Reis RL, Oliveira JM. Scaffold fabrication technologies and structure/function properties in bone tissue engineering. Adv Funct Materials. 2021;31(21):2010609. doi:10.1002/adfm.202010609
22. Liu J, Meng Z, Song J, et al. Yoda1-loaded microfibrous scaffolds accelerate osteogenesis through Piezo1-F-actin pathway-mediated YAP nuclear localization and functionalization. ACS Appl Mater Interfaces. 2025;17(21):30559–30572. doi:10.1021/acsami.5c03093
23. Qin Y, Jing Z, Zou D, et al. A metamaterial scaffold beyond modulus limits: enhanced osteogenesis and angiogenesis of critical bone defects. Nat Commun. 2025;16(1):2180. doi:10.1038/s41467-025-57609-9
24. Chen P, Xia Y, Wu Y, Wu X, Wang Y, Dai H. 3D-printed scaffolds with ROS-clearing capacity for critical-sized bone defect regeneration. Biomater Adv. 2025;180:214575. doi:10.1016/j.bioadv.2025.214575
25. He J, Qiao L, Fu Q, et al. Synergistic integration of bio-mineralized nanoparticles and porous microsphere scaffolds for dual bioactive delivery in bone regeneration. J Controlled Release. 2025;386:114097. doi:10.1016/j.jconrel.2025.114097
26. Rong X, Xiao S, Geng W, et al. Sono-activable and biocatalytic 3D-printed scaffolds for intelligently sequential therapies in osteosarcoma eradication and defect regeneration. Nat Commun. 2025;16(1):6150. doi:10.1038/s41467-025-61377-x
27. Zhang H, Wang Y, Qiang H, et al. Exploring the frontiers: the potential and challenges of bioactive scaffolds in osteosarcoma treatment and bone regeneration. Mater Today Bio. 2024;29:101276. doi:10.1016/j.mtbio.2024.101276
28. Zhang LY, Bi Q, Zhao C, Chen JY, Cai MH, Chen XY. Recent advances in biomaterials for the treatment of bone defects. Organogenesis. 2020;16(4):113–125. doi:10.1080/15476278.2020.1808428
29. Claes L, Recknagel S, Ignatius A. Fracture healing under healthy and inflammatory conditions. Nat Rev Rheumatol. 2012;8(3):133–143. doi:10.1038/nrrheum.2012.1
30. Bahney CS, Zondervan RL, Allison P, et al. Cellular biology of fracture healing. J Orthop Res. 2019;37(1):35–50. doi:10.1002/jor.24170
31. Marsell R, Einhorn TA. The biology of fracture healing. Injury. 2011;42(6):551–555. doi:10.1016/j.injury.2011.03.031
32. Matsuoka K, Park K, Ito M, Ikeda K, Takeshita S. Osteoclast-derived complement component 3a stimulates osteoblast differentiation. J Bone Miner Res. 2014;29(7):1522–1530. doi:10.1002/jbmr.2187
33. Teitelbaum SL. Osteoclasts: what do they do and how do they do it? Am J Pathol. 2007;170(2):427–435. doi:10.2353/ajpath.2007.060834
34. Barbosa WT, De Almeida KV, De Lima GG, et al. Synthesis and in vivo evaluation of a scaffold containing wollastonite/β-TCP for bone repair in a rabbit tibial defect model. J Biomed Mater Res B: Appl Biomater. 2020;108(3):1107–1116. doi:10.1002/jbm.b.34462
35. Bhushan S, Singh S, Maiti TK, et al. Scaffold fabrication techniques of biomaterials for bone tissue engineering: a critical review. Bioengineering. 2022;9(12):728. doi:10.3390/bioengineering9120728
36. Hutmacher DW. Scaffolds in tissue engineering bone and cartilage. Biomaterials. 2000;21(24):2529–2543. doi:10.1016/s0142-9612(00)00121-6
37. Aslankoohi N, Mondal D, Rizkalla AS, Mequanint K. Bone repair and regenerative biomaterials: towards recapitulating the microenvironment. Polymers. 2019;11(9):1437. doi:10.3390/polym11091437
38. Roseti L, Parisi V, Petretta M, et al. Scaffolds for bone tissue engineering: state of the art and new perspectives. Mater Sci Eng C Mater Biol Appl. 2017;78:1246–1262. doi:10.1016/j.msec.2017.05.017
39. Hoque ME, Chuan YL, Pashby I. Extrusion based rapid prototyping technique: an advanced platform for tissue engineering scaffold fabrication. Biopolymers. 2012;97(2):83–93. doi:10.1002/bip.21701
40. Seol Y, Park DY, Park JY, Kim SW, Park SJ, Cho D. A new method of fabricating robust freeform 3D ceramic scaffolds for bone tissue regeneration. Biotechnol Bioeng. 2013;110(5):1444–1455. doi:10.1002/bit.24794
41. Gao Y, Li C, Wang H, Fan G. Acceleration of bone-defect repair by using A-W MGC loaded with BMP2 and triple point-mutant HIF1α-expressing BMSCs. J Orthop Surg Res. 2015;10(1):83. doi:10.1186/s13018-015-0219-3
42. Gao C, Deng Y, Feng P, et al. Current progress in bioactive ceramic scaffolds for bone repair and regeneration. Int J Mol Sci. 2014;15(3):4714–4732. doi:10.3390/ijms15034714
43. Wu S, Liu X, Yeung KW, Liu C, Yang X. Biomimetic porous scaffolds for bone tissue engineering. Mater Sci Eng: R: Rep. 2014;80:1–36. doi:10.1016/j.mser.2014.04.001
44. O’Brien FJ. Biomaterials & scaffolds for tissue engineering. Mater Today. 2011;14(3):88–95. doi:10.1016/S1369-7021(11)70058-X
45. Yin S, Zhang W, Zhang Z, Jiang X. Recent advances in scaffold design and material for vascularized tissue-engineered bone regeneration. Adv Healthcare Mater. 2019;8(10):1801433. doi:10.1002/adhm.201801433
46. Bose S, Roy M, Bandyopadhyay A. Recent advances in bone tissue engineering scaffolds. Trends Biotechnol. 2012;30(10):546–554. doi:10.1016/j.tibtech.2012.07.005
47. Bohner M, Baumgart F. Theoretical model to determine the effects of geometrical factors on the resorption of calcium phosphate bone substitutes. Biomaterials. 2004;25(17):3569–3582. doi:10.1016/j.biomaterials.2003.10.032
48. Wubneh A, Tsekoura EK, Ayranci C, Uludağ H. Current state of fabrication technologies and materials for bone tissue engineering. Acta Biomater. 2018;80:1–30. doi:10.1016/j.actbio.2018.09.031
49. Roosa SMM, Kemppainen JM, Moffitt EN, Krebsbach PH, Hollister SJ. The pore size of polycaprolactone scaffolds has limited influence on bone regeneration in an in vivo model. J Biomed Mater Res A. 2010;92A(1):359–368. doi:10.1002/jbm.a.32381
50. Xu G, Hu X, Han L, Zhao Y, Li Z. The construction of a novel xenograft bovine bone scaffold, (DSS)6-liposome/CKIP-1 siRNA/calcine bone and its osteogenesis evaluation on skull defect in rats. J Orthop Transl. 2021;28:74–82. doi:10.1016/j.jot.2021.02.001
51. Amini Z, Lari R. A systematic review of decellularized allograft and xenograft–derived scaffolds in bone tissue regeneration. Tissue Cell. 2021;69:101494. doi:10.1016/j.tice.2021.101494
52. Urist MR, Takeuchi R, Katagiri W, Endo S, Kobayashi T. Bone: formation by autoinduction. Science. 1965;150(3698):893–899. doi:10.1126/science.150.3698.893
53. Vukicevic S, Grgurevic L. BMP-6 and mesenchymal stem cell differentiation. Cytokine Growth Factor Rev. 2009;20(5–6):441–448. doi:10.1016/j.cytogfr.2009.10.020
54. Bordukalo-Nikšić T, Kufner V, Vukičević S. The role of BMPs in the regulation of osteoclasts resorption and bone remodeling: from experimental models to clinical applications. Front Immunol. 2022;13:869422. doi:10.3389/fimmu.2022.869422
55. Wu M, Wu S, Chen W, Li YP. The roles and regulatory mechanisms of TGF-β and BMP signaling in bone and cartilage development, homeostasis and disease. Cell Res. 2024;34(2):101–123. doi:10.1038/s41422-023-00918-9
56. Dadwal UC, Bhatti FUR, Awosanya OD, et al. The effects of bone morphogenetic protein 2 and thrombopoietin treatment on angiogenic properties of endothelial cells derived from the lung and bone marrow of young and aged, male and female mice. FASEB J. 2021;35(9):e21840. doi:10.1096/fj.202001616RR
57. McMahon MS. Bone morphogenic protein 3 signaling in the regulation of osteogenesis. Orthopedics. 2012;35(11):920. doi:10.3928/01477447-20121023-02
58. Brennan MÁ, Barilani M, Rusconi F, et al. Chondrogenic and BMP-4 primings confer osteogenesis potential to human cord blood mesenchymal stromal cells delivered with biphasic calcium phosphate ceramics. Sci Rep. 2021;11(1):6751. doi:10.1038/s41598-021-86147-9
59. Pérez-Lozano ML, Sudre L, van Eegher S, et al. Gremlin-1 and BMP-4 overexpressed in osteoarthritis drive an osteochondral-remodeling program in osteoblasts and hypertrophic chondrocytes. Int J Mol Sci. 2022;23(4):2084. doi:10.3390/ijms23042084
60. Wang JF, Lee M-S, Tsai T-L, et al. Bone morphogenetic protein-6 attenuates type 1 diabetes mellitus-associated bone loss. Stem Cells Transl Med. 2019;8(6):522–534. doi:10.1002/sctm.18-0150
61. Pulkkinen HH, Kiema M, Lappalainen JP, et al. BMP6/TAZ-hippo signaling modulates angiogenesis and endothelial cell response to VEGF. Angiogenesis. 2021;24(1):129–144. doi:10.1007/s10456-020-09748-4
62. Liang C, Liang Q, Xu X, et al. Bone morphogenetic protein 7 mediates stem cells migration and angiogenesis: therapeutic potential for endogenous pulp regeneration. Int J Oral Sci. 2022;14(1):38. doi:10.1038/s41368-022-00188-y
63. Bharadwaz A, Jayasuriya AC. Osteogenic differentiation cues of the bone morphogenetic protein-9 (BMP-9) and its recent advances in bone tissue regeneration. Mater Sci Eng C Mater Biol Appl. 2021;120:111748. doi:10.1016/j.msec.2020.111748
64. Xiao H, Wang X, Wang C, et al. BMP9 exhibits dual and coupled roles in inducing osteogenic and angiogenic differentiation of mesenchymal stem cells. Biosci Rep. 2020;40(6):BSR20201262. doi:10.1042/BSR20201262
65. Vukicevic S, Oppermann H, Verbanac D, et al. The clinical use of bone morphogenetic proteins revisited: a novel biocompatible carrier device OSTEOGROW for bone healing. Int Orthop. 2014;38(3):635–647. doi:10.1007/s00264-013-2201-1
66. Vukicevic S, Peric M, Oppermann H, et al. Bone morphogenetic proteins: from discovery to development of a novel autologous bone graft substitute consisting of recombinant human BMP6 delivered in autologous blood coagulum carrier. Rad CASA-Med Sci. 2020;544(52–53):26–41.
67. Shi C, Zhang H, Louie K, Mishina Y, Sun H. BMP signaling mediated by BMPR1A in osteoclasts negatively regulates osteoblast mineralization through suppression of Cx43. J Cell Biochem. 2017;118(3):605–614. doi:10.1002/jcb.25746
68. Karner CM, Lee S-Y, Long F. Bmp induces osteoblast differentiation through both Smad4 and mTORC1 signaling. Mol Cell Biol. 2017;37(4):e00253–16. doi:10.1128/MCB.00253-16
69. Friedman MS, Long MW, Hankenson KD. Osteogenic differentiation of human mesenchymal stem cells is regulated by bone morphogenetic protein-6. J Cell Biochem. 2006;98(3):538–554. doi:10.1002/jcb.20719
70. Maguer-Satta VÉ, Bartholin L, Jeanpierre S, et al. Regulation of human erythropoiesis by activin A, BMP2, and BMP4, members of the TGFβ family. Exp Cell Res. 2003;282(2):110–120. doi:10.1016/s0014-4827(02)00013-7
71. Xue N, Ding X, Huang R, et al. Bone tissue engineering in the treatment of bone defects. Pharmaceuticals. 2022;15(7):879. doi:10.3390/ph15070879
72. Carragee EJ, Hurwitz EL, Weiner BK. A critical review of recombinant human bone morphogenetic protein-2 trials in spinal surgery: emerging safety concerns and lessons learned. Spine J. 2011;11(6):471–491. doi:10.1016/j.spinee.2011.04.023
73. James AW, LaChaud G, Shen J, et al. A review of the clinical side effects of bone morphogenetic protein-2. Tissue Eng Part B Rev. 2016;22(4):284–297. doi:10.1089/ten.TEB.2015.0357
74. Wei S, Cai X, Huang J, Xu F, Liu X, Wang Q. Recombinant human BMP-2 for the treatment of open tibial fractures. Orthopedics. 2012;35(6):e847–854. doi:10.3928/01477447-20120525-23
75. Govender S, Csimma C, Genant HK, Valentin-Opran A. Recombinant human bone morphogenetic protein-2 for treatment of open tibial fractures: a prospective, controlled, randomized study of four hundred and fifty patients. J Bone Joint Surg Am. 2002;84(12):2123–2134. doi:10.2106/00004623-200212000-00001
76. Gonzaga MG, Dos Santos Kotake BG, De Figueiredo FAT, et al. Effectiveness of rhBMP-2 association to autogenous, allogeneic, and heterologous bone grafts. Microsc Res Tech. 2019;82(6):689–695. doi:10.1002/jemt.23215
77. Issa JP, Gonzaga M, Kotake BG, De Lucia C, Ervolino E, Iyomasa M. Bone repair of critical size defects treated with autogenic, allogenic, or xenogenic bone grafts alone or in combination with rh BMP −2. Clin Oral Implants Res. 2016;27(5):558–566. doi:10.1111/clr.12622
78. Cohen A, Avraham Verkauf T, Casap N, Chackartchi T, Polak D. Adsorption and release pattern of recombinant human bone morphogenic protein 2 onto different bone grafts and its consequent osteoblasts` activation and neutrophils` priming. Arch Oral Biol. 2025;170:106123. doi:10.1016/j.archoralbio.2024.106123
79. Pecin M, Stokovic N, Ivanjko N, et al. A novel autologous bone graft substitute containing rhBMP6 in autologous blood coagulum with synthetic ceramics for reconstruction of a large humerus segmental gunshot defect in a dog: the first veterinary patient to receive a novel osteoinductive therapy. Bone Rep. 2021;14:100759. doi:10.1016/j.bonr.2021.100759
80. Su W, Ma X, Sun Z, et al. RhBMP-2 and concomitant rapid material degradation synergistically promote bone repair and regeneration with collagen–hydroxyapatite nanocomposites. J Mater Chem B. 2018;6(26):4338–4350. doi:10.1039/c8tb00405f
81. Sampath TK, Vukicevic S. Biology of bone morphogenetic protein in bone repair and regeneration: a role for autologous blood coagulum as carrier. Bone. 2020;141:115602. doi:10.1016/j.bone.2020.115602
82. Chen R, Yu Y, Zhang W, et al. Tuning the bioactivity of bone morphogenetic protein-2 with surface immobilization strategies. Acta Biomater. 2018;80:108–120. doi:10.1016/j.actbio.2018.09.011
83. Kadam A, Millhouse PW, Kepler CK, et al. Bone substitutes and expanders in Spine Surgery: a review of their fusion efficacies. Int J Spine Surg. 2016;10:33. doi:10.14444/3033
84. El Bialy I, Jiskoot W, Reza Nejadnik M. Formulation, delivery and stability of bone morphogenetic proteins for effective bone regeneration. Pharm Res. 2017;34(6):1152–1170. doi:10.1007/s11095-017-2147-x
85. Agrawal V, Sinha M. A review on carrier systems for bone morphogenetic protein-2. J Biomed Mater Res B. 2017;105(4):904–925. doi:10.1002/jbm.b.33599
86. Zhang Z, Liu A, Fan J, et al. A drug-loaded composite coating to improve osteogenic and antibacterial properties of Zn–1Mg porous scaffolds as biodegradable bone implants. Bioactive Materials. 2023;27:488–504. doi:10.1016/j.bioactmat.2023.04.017
87. Ma R, Su Y, Cao R, Wang K, Yang P. Enhanced osteogenic activity and bone repair ability of PLGA/MBG scaffolds doped with ZIF-8 nanoparticles loaded with BMP-2. Int J Nanomedicine. 2023;18:5055–5072. doi:10.2147/IJN.S423985
88. Sun X, Ma Z, Zhao X, et al. Three-dimensional bioprinting of multicell-laden scaffolds containing bone morphogenic protein-4 for promoting M2 macrophage polarization and accelerating bone defect repair in diabetes mellitus. Bioact Mater. 2021;6(3):757–769. doi:10.1016/j.bioactmat.2020.08.030
89. Sarsenova M, Raimagambetov Y, Issabekova A, et al. Regeneration of osteochondral defects by combined delivery of synovium-derived mesenchymal stem cells, TGF-β1 and BMP-4 in heparin-conjugated fibrin hydrogel. Polymers. 2022;14(24):5343. doi:10.3390/polym14245343
90. Toprak Ö, Topuz B, Monsef YA, Oto Ç, Orhan K, Karakeçili A. BMP-6 carrying metal organic framework-embedded in bioresorbable electrospun fibers for enhanced bone regeneration. Mater Sci Eng C Mater Biol Appl. 2021;120:111738. doi:10.1016/j.msec.2020.111738
91. Li X, Zhang R, Tan X, Li B, Liu Y, Wang X. Synthesis and evaluation of BMMSC-seeded BMP-6/nHAG/GMS scaffolds for bone regeneration. Int J Med Sci. 2019;16(7):1007–1017. doi:10.7150/ijms.31966
92. Huang S, Wang Z, Sun X, Li K. Bone morphogenetic protein 7-loaded gelatin methacrylate/oxidized sodium alginate/nano-hydroxyapatite composite hydrogel for bone tissue engineering. Int J Nanomedicine. 2024;19:6359–6376. doi:10.2147/IJN.S461996
93. Sithole MN, Kumar P, Du Toit LC, Erlwanger KH, Ubanako PN, Choonara YE. A 3D-printed biomaterial scaffold reinforced with inorganic fillers for bone tissue engineering: in vitro assessment and in vivo animal studies. Int J Mol Sci. 2023;24(8):7611. doi:10.3390/ijms24087611
94. Yang W, Wang C, Luo W, et al. Effectiveness of biomechanically stable pergola-like additively manufactured scaffold for extraskeletal vertical bone augmentation. Front Bioeng Biotechnol. 2023;11:1112335. doi:10.3389/fbioe.2023.1112335
95. Song X, Li X, Wang F, et al. Bioinspired protein/peptide loaded 3D printed PLGA scaffold promotes bone regeneration. Front Bioeng Biotechnol. 2022;10:832727. doi:10.3389/fbioe.2022.832727
96. Oryan A, Alidadi S, Moshiri A. Platelet-rich plasma for bone healing and regeneration. Expert Opin Biol Ther. 2016;16(2):213–232. doi:10.1517/14712598.2016.1118458
97. Dhillon MS, Patel S, John R. PRP in OA knee – update, current confusions and future options. SICOT-J. 2017;3:27. doi:10.1051/sicotj/2017004
98. Meheux CJ, McCulloch PC, Lintner DM, Varner KE, Harris JD. Efficacy of intra-articular platelet-rich plasma injections in knee osteoarthritis: a systematic review. Arthroscopy. 2016;32(3):495–505. doi:10.1016/j.arthro.2015.08.005
99. Marx RE. Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg. 2004;62(4):489–496. doi:10.1016/j.joms.2003.12.003
100. Cavallo C, Roffi A, Grigolo B, et al. Platelet-rich plasma: the choice of activation method affects the release of bioactive molecules. Biomed Res Int. 2016;2016:1–7. doi:10.1155/2016/6591717
101. Engebretsen L, Steffen K, Alsousou J, et al. IOC consensus paper on the use of platelet-rich plasma in sports medicine. Br J Sports Med. 2010;44(15):1072–1081. doi:10.1136/bjsm.2010.079822
102. Hall MP, Band PA, Meislin RJ, Jazrawi LM, Cardone DA. Platelet-rich plasma: current concepts and application in sports medicine. J Am Acad Orthop Surg. 2009;17(10):602–608. doi:10.5435/00124635-200910000-00002
103. LaPrade RF, Geeslin AG, Murray IR, et al. Biologic treatments for sports injuries II think tank-current concepts, future research, and barriers to advancement, part 1: biologics overview, ligament injury, tendinopathy. Am J Sports Med. 2016;44(12):3270–3283. doi:10.1177/0363546516634674
104. Yang J, Lu Y, Guo A. Platelet-rich plasma protects rat chondrocytes from interleukin-1β-induced apoptosis. Mol Med Rep. 2016;14(5):4075–4082. doi:10.3892/mmr.2016.5767
105. Li H, Sun S, Liu H, et al. Use of a biological reactor and platelet-rich plasma for the construction of tissue-engineered bone to repair articular cartilage defects. Exp Ther Med. 2016;12(2):711–719. doi:10.3892/etm.2016.3380
106. Anitua E, Tejero R, Alkhraisat MH, Orive G. Platelet-rich plasma to improve the bio-functionality of biomaterials. BioDrugs. 2013;27(2):97–111. doi:10.1007/s40259-012-0004-3
107. Yu T, Pan H, Hu Y, Tao H, Wang K, Zhang C. Autologous platelet-rich plasma induces bone formation of tissue-engineered bone with bone marrow mesenchymal stem cells on beta-tricalcium phosphate ceramics. J Orthop Surg Res. 2017;12(1):178. doi:10.1186/s13018-017-0665-1
108. Shin HS, Kim MS, Kim BH, Lim HJ, Kim BC, Lee J. Reconstruction of mandibular defects with bone marrow-derived stem cells in odontogenic myxoma. J Craniofac Surg. 2020;31(3):e236–e239. doi:10.1097/SCS.0000000000006147
109. Holmes HL, Wilson B, Goerger JP, et al. Facilitated recruitment of mesenchymal stromal cells by bone marrow concentrate and platelet rich plasma. Choi J, ed. PLoS One. 2018;13(3):e0194567. doi:10.1371/journal.pone.0194567
110. Liu J, Nie H, Xu Z, et al. Construction of PRP-containing nanofibrous scaffolds for controlled release and their application to cartilage regeneration. J Mater Chem B. 2015;3(4):581–591. doi:10.1039/c4tb00515e
111. Liu W, Huang Y, Liu D, et al. The combination of platelet rich plasma gel, human umbilical mesenchymal stem cells and nanohydroxyapatite/polyamide 66 promotes angiogenesis and bone regeneration in large bone defect. Tissue Eng Regen Med. 2022;19(6):1321–1336. doi:10.1007/s13770-022-00471-3
112. Caramês JMM, Vieira FA, Caramês GB, Pinto AC, Francisco HCO, Marques DNDS. Guided bone regeneration in the edentulous atrophic maxilla using Deproteinized Bovine Bone Mineral (DBBM) combined with Platelet-Rich Fibrin (PRF)—a prospective study. JCM. 2022;11(3):894. doi:10.3390/jcm11030894
113. Hao Y, Cao B, Deng L, et al. The first 3D-bioprinted personalized active bone to repair bone defects: a case report. Int J Bioprinting. 2022;9(2):654. doi:10.18063/ijb.v9i2.654
114. Man Y, Wang P, Guo Y, et al. Angiogenic and osteogenic potential of platelet-rich plasma and adipose-derived stem cell laden alginate microspheres. Biomaterials. 2012;33(34):8802–8811. doi:10.1016/j.biomaterials.2012.08.054
115. Franco D, Franco T, Schettino AM, Filho JMT, Vendramin FS. Protocol for obtaining platelet-rich plasma (PRP), platelet-poor plasma (PPP), and thrombin for autologous use. Aesthetic Plast Surg. 2012;36(5):1254–1259. doi:10.1007/s00266-012-9957-3
116. Skwarcz S, Bryzek I, Gregosiewicz A, et al. The effect of activated platelet-rich plasma (PRP) on tricalcium hydroxyapatite phosphate healing in experimental, partial defects of long bone shafts in animal models. Pol J Vet Sci. 2019;22(2):243–250. doi:10.24425/pjvs.2019.127092
117. Rodriguez IA, Growney Kalaf EA, Bowlin GL, Sell SA. Platelet-rich plasma in bone regeneration: engineering the delivery for improved clinical efficacy. Biomed Res Int. 2014;2014:392398. doi:10.1155/2014/392398
118. Qiu G, Shi Z, Xu HHK, et al. Bone regeneration in minipigs via calcium phosphate cement scaffold delivering autologous bone marrow mesenchymal stem cells and platelet-rich plasma. J Tissue Eng Regen M. 2018;12(2):e937–e948. doi:10.1002/term.2416
119. Donnaloja F, Jacchetti E, Soncini M, Raimondi MT. Natural and synthetic polymers for bone scaffolds optimization. Polymers. 2020;12(4):905. doi:10.3390/polym12040905
120. Adithya SP, Sidharthan DS, Abhinandan R, Balagangadharan K, Selvamurugan N. Nanosheets-incorporated bio-composites containing natural and synthetic polymers/ceramics for bone tissue engineering. Int J Biol Macromol. 2020;164:1960–1972. doi:10.1016/j.ijbiomac.2020.08.053
121. Dec P, Modrzejewski A, Pawlik A. Existing and novel biomaterials for bone tissue engineering. Int J Mol Sci. 2022;24(1):529. doi:10.3390/ijms24010529
122. Huang L, Abdalla AME, Xiao L, Yang G. Biopolymer-based microcarriers for three-dimensional cell culture and engineered tissue formation. Int J Mol Sci. 2020;21(5):1895. doi:10.3390/ijms21051895
123. Zhao Y, Zhao S, Ma Z, Ding C, Chen J, Li J. Chitosan-based scaffolds for facilitated endogenous bone re-generation. Pharmaceuticals. 2022;15(8):1023. doi:10.3390/ph15081023
124. Soriente A, Fasolino I, Gomez-Sánchez A, et al. Chitosan/hydroxyapatite nanocomposite scaffolds to modulate osteogenic and inflammatory response. J Biomed Mater Res A. 2022;110(2):266–272. doi:10.1002/jbm.a.37283
125. Abazari MF, Soleimanifar F, Amini Faskhodi M, et al. Improved osteogenic differentiation of human induced pluripotent stem cells cultured on polyvinylidene fluoride/collagen/platelet-rich plasma composite nanofibers. J Cell Physiol. 2020;235(2):1155–1164. doi:10.1002/jcp.29029
126. Aravamudhan A, Ramos DM, Nip J, et al. Cellulose and collagen derived micro-nano structured scaffolds for bone tissue engineering. J Biomed Nanotechnol. 2013;9(4):719–731. doi:10.1166/jbn.2013.1574
127. Miguel FB, Barbosa Júnior A, De paula FL, Barreto IC, Goissis G, Rosa FP. Regeneration of critical bone defects with anionic collagen matrix as scaffolds. J Mater Sci Mater Med. 2013;24(11):2567–2575. doi:10.1007/s10856-013-4980-8
128. Tsai SW, Huang SS, Yu WX, Hsu YW, Hsu FY. Collagen scaffolds containing hydroxyapatite-CaO fiber fragments for bone tissue engineering. Polymers. 2020;12(5):1174. doi:10.3390/polym12051174
129. Resmi R, Parvathy J, John A, Joseph R. Injectable self-crosslinking hydrogels for meniscal repair: a study with oxidized alginate and gelatin. Carbohydr Polym. 2020;234:115902. doi:10.1016/j.carbpol.2020.115902
130. Kolathupalayam Shanmugam B, Rangaraj S, Subramani K, Srinivasan S, Aicher WK, Venkatachalam R. Biomimetic TiO2-chitosan/sodium alginate blended nanocomposite scaffolds for tissue engineering applications. Mater Sci Eng C. 2020;110:110710. doi:10.1016/j.msec.2020.110710
131. Naruphontjirakul P, Panpisut P, Patntirapong S. Zinc and strontium-substituted bioactive glass nanoparticle/alginate composites scaffold for bone regeneration. Int J Mol Sci. 2023;24(7):6150. doi:10.3390/ijms24076150
132. Hamrun N, Herdianto N, Gustiono D, et al. Synthesis, physical characteristics, and biocompatibility test of chitosan-alginate-fucoidan scaffold as an alternative material for alveolar bone substitution. BMC Oral Health. 2025;25(1):1199. doi:10.1186/s12903-025-06591-1
133. Seddiqi H, Oliaei E, Honarkar H, et al. Cellulose and its derivatives: towards biomedical applications. Cellulose. 2021;28(4):1893–1931. doi:10.1007/s10570-020-03674-w
134. Janmohammadi M, Nazemi Z, Salehi AOM, et al. Cellulose-based composite scaffolds for bone tissue engineering and localized drug delivery. Bioact Mater. 2023;20:137–163. doi:10.1016/j.bioactmat.2022.05.018
135. Patel DK, Dutta SD, Hexiu J, Ganguly K, Lim KT. 3D-printable chitosan/silk fibroin/cellulose nanoparticle scaffolds for bone regeneration via M2 macrophage polarization. Carbohydrate Polymers. 2022;281:119077. doi:10.1016/j.carbpol.2021.119077
136. Seifi S, Shamloo A, Barzoki AK, et al. Engineering biomimetic scaffolds for bone regeneration: chitosan/alginate/polyvinyl alcohol-based double-network hydrogels with carbon nanomaterials. Carbohydr Polym. 2024;339:122232. doi:10.1016/j.carbpol.2024.122232
137. Zhang X, Xia Y, Xu J, et al. Cell-free chitosan/silk fibroin/bioactive glass scaffolds with radial pore for in situ inductive regeneration of critical-size bone defects. Carbohydr Polym. 2024;332:121945. doi:10.1016/j.carbpol.2024.121945
138. Ji C, Zhang C, Xu Z, et al. Mussel-inspired HA@TA-CS/SA biomimetic 3D printed scaffolds with antibacterial activity for bone repair. Front Bioeng Biotechnol. 2023;11:1193605. doi:10.3389/fbioe.2023.1193605
139. Koo Y, Lee H, Lim CS, Kwon SY, Han I, Kim GH. Highly porous multiple-cell-laden collagen/hydroxyapatite scaffolds for bone tissue engineering. Int J Biol Macromol. 2022;222(Pt A):1264–1276. doi:10.1016/j.ijbiomac.2022.09.249
140. Jirofti N, Hashemi M, Moradi A, Kalalinia F. Fabrication and characterization of 3D printing biocompatible crocin-loaded chitosan/collagen/hydroxyapatite-based scaffolds for bone tissue engineering applications. Int J Biol Macromol. 2023;252:126279. doi:10.1016/j.ijbiomac.2023.126279
141. Tan J, Chen Z, Xu Z, et al. A 3D-printed scaffold composed of Alg/HA/SIS for the treatment of diabetic bone defects. J Orthop Transl. 2024;48:25–38. doi:10.1016/j.jot.2024.07.006
142. Miao A, Li Q, Tang G, Lu Q. Alginate-containing 3D-printed hydrogel scaffolds incorporated with strontium promotes vascularization and bone regeneration. Int J Biol Macromol. 2024;273(Pt 1):133038. doi:10.1016/j.ijbiomac.2024.133038
143. Li L, Lu P, Liu Y, Yang J, Li S. Three-dimensional-bioprinted bioactive glass/cellulose composite scaffolds with porous structure towards bone tissue engineering. Polymers (Basel). 2023;15(9):2226. doi:10.3390/polym15092226
144. Luo C, Li YM, Jiang K, et al. ECM-inspired calcium/zinc laden cellulose scaffold for enhanced bone regeneration. Carbohydr Polym. 2024;331:121823. doi:10.1016/j.carbpol.2024.121823
145. Joyce M, Hodgkinson T, Lemoine M, González-Vázquez A, Kelly DJ, O’Brien FJ. Development of a 3D-printed bioabsorbable composite scaffold with mechanical properties suitable for treating large, load-bearingarticular cartilage defects. Eur Cell Mater. 2023;45:158–172. doi:10.22203/eCM.v045a11
146. Lee JH, Kim PY, Pyun YC, et al. Cartilage regeneration using transforming growth factor-beta 3-loaded injectable crosslinked hyaluronic acid hydrogel. Biomater Sci. 2024;12(2):479–494. doi:10.1039/D3BM01008B
147. Li J, Yan S, Yang X, Ren X, Qu H, Song J. Nicotinamide mononucleotide based hyaluronic acid methacryloyl hybrid hydrogel regulating stem cells fate for bone regeneration via SIRT1/RUNX2 signaling. Int J Biol Macromol. 2024;261:129905. doi:10.1016/j.ijbiomac.2024.129905
148. Yang T, Dong Y, Wan J, et al. Sustained release of BMSC‐EVs from 3D printing Gel/HA/nHAP scaffolds for promoting bone regeneration in diabetic rats. Adv Healthcare Mater. 2023;12(18):2203131. doi:10.1002/adhm.202203131
149. Guo X, Song P, Li F, et al. Research progress of design drugs and composite biomaterials in bone tissue engineering. Int J Nanomedicine. 2023;18:3595–3622. doi:10.2147/IJN.S415666
150. Zeng KW, Gu MY. Annual advances of integrative pharmacology in 2020. Tradit Med Res. 2021;6(4):31. doi:10.53388/TMR20210616237
151. Habibi Ghahfarrokhi S, Reisi R. Effects of medicinal herbs on osteoporosis: a systematic review based on clinical trials. J Shahrekord Univ Med Sci. 2019;21(5):229–236. doi:10.34172/jsums.2019.40
152. Wang X, Tang P, Yang K, et al. Regulation of bone homeostasis by traditional Chinese medicine active scaffolds and enhancement for the osteoporosis bone regeneration. J Ethnopharmacol. 2024;329:118141. doi:10.1016/j.jep.2024.118141
153. Monavari M, Homaeigohar S, Fuentes-Chandía M, et al. 3D printing of alginate dialdehyde-gelatin (ADA-GEL) hydrogels incorporating phytotherapeutic icariin loaded mesoporous SiO2-CaO nanoparticles for bone tissue engineering. Mater Sci Eng C. 2021;131:112470. doi:10.1016/j.msec.2021.112470
154. Wang F, Yang Z, He W, Song Q, Wang K, Zhou Y. Effects of icariin on the proliferation and osteogenic differentiation of human amniotic mesenchymal stem cells. J Orthop Surg Res. 2020;15(1):578. doi:10.1186/s13018-020-02076-9
155. Zhang X, Guo Y, Li DX, et al. The effect of loading icariin on biocompatibility and bioactivity of porous β-TCP ceramic. J Mater Sci: Mater Med. 2011;22(2):371–379. doi:10.1007/s10856-010-4198-y
156. Song L, Zhao J, Zhang X, Li H, Zhou Y. Icariin induces osteoblast proliferation, differentiation and mineralization through estrogen receptor-mediated ERK and JNK signal activation. Eur J Pharmacol. 2013;714(1–3):15–22. doi:10.1016/j.ejphar.2013.05.039
157. Jing X, Yin W, Tian H, et al. Icariin doped bioactive glasses seeded with rat adipose-derived stem cells to promote bone repair via enhanced osteogenic and angiogenic activities. Life Sci. 2018;202:52–60. doi:10.1016/j.lfs.2018.02.026
158. Ji W, Gong G, Liu Y, Liu Y, Zhang J, Li Q. Icariin promotes osteogenic differentiation of bone marrow mesenchymal stem cells (BMSCs) by activating PI3K-AKT-UTX/EZH2 signaling in steroid-induced femoral head osteonecrosis. J Orthop Surg Res. 2025;20(1):290. doi:10.1186/s13018-025-05697-0
159. Yang W, Yu XC, Chen XY, Zhang L, Lu CT, Zhao YZ. Pharmacokinetics and tissue distribution profile of icariin propylene glycol-liposome intraperitoneal injection in mice. J Pharm Pharmacol. 2012;64(2):190–198. doi:10.1111/j.2042-7158.2011.01388.x
160. Chen J, Pan P, Zhang Y, Zhong S, Zhang Q. Preparation of chitosan/nano hydroxyapatite organic-inorganic hybrid microspheres for bone repair. Colloids Surf, B. 2015;134:401–407. doi:10.1016/j.colsurfb.2015.06.072
161. Zhao H, Tang J, Zhou D, et al. Electrospun icariin-loaded core-shell collagen, polycaprolactone, hydroxyapatite composite scaffolds for the repair of rabbit tibia bone defects. Int J Nanomed. 2020;15:3039–3056. doi:10.2147/IJN.S238800
162. Yuan Z, Wan Z, Wei P, et al. Dual‐controlled release of icariin/Mg 2+ from biodegradable microspheres and their synergistic upregulation effect on bone regeneration. Adv Healthcare Materials. 2020;9(11):e2000211. doi:10.1002/adhm.202000211
163. Lin H, Li Z, Xie Z, et al. An anti-infection and biodegradable TFRD-loaded porous scaffold promotes bone regeneration in segmental bone defects: experimental studies. International Journal of Surgery. 2024;110(6):3269–3284. doi:10.1097/JS9.0000000000001291
164. Li L, Li Q, Gui L, et al. Sequential gastrodin release PU/n-HA composite scaffolds reprogram macrophages for improved osteogenesis and angiogenesis. Bioact Mater. 2023;19:24–37. doi:10.1016/j.bioactmat.2022.03.037
165. Zhao ZH, Ma XL, Ma JX, et al. Sustained release of naringin from silk-fibroin-nanohydroxyapatite scaffold for the enhancement of bone regeneration. Mater Today Bio. 2022;13:100206. doi:10.1016/j.mtbio.2022.100206
166. Zhang Y, Wang T, Li J, et al. Bilayer membrane composed of mineralized collagen and chitosan cast film coated with berberine-loaded PCL/PVP electrospun nanofiber promotes bone regeneration. Front Bioeng Biotechnol. 2021;9:684335. doi:10.3389/fbioe.2021.684335
167. Wei B, Wang W, Liu X, et al. Gelatin methacrylate hydrogel scaffold carrying resveratrol-loaded solid lipid nanoparticles for enhancement of osteogenic differentiation of BMSCs and effective bone regeneration. Regener Biomater. 2021;8(5):rbab044. doi:10.1093/rb/rbab044
168. Luo P, Yu L, Lin Q, Wang C, Yang D, Tang S. Strontium modified calcium sulfate hemihydrate scaffold incorporating ginsenoside Rg1/gelatin microspheres for bone regeneration. Front Bioeng Biotechnol. 2020;8:888. doi:10.3389/fbioe.2020.00888
169. Gui ZP, Hu Y, Zhou YN, Lin KL, Xu YJ. Effect of quercetin on chondrocyte phenotype and extracellular matrix expression. Chin J Nat Med. 2020;18(12):922–933. doi:10.1016/S1875-5364(20)60036-X
170. Deng Z, Chen J, Lin B, et al. A novel 3D printed bioactive scaffolds with enhanced osteogenic inspired by ancient Chinese medicine HYSA for bone repair. Exp Cell Res. 2020;394(2):112139. doi:10.1016/j.yexcr.2020.112139
171. Sarkar N, Bose S. Controlled delivery of curcumin and vitamin K2 from hydroxyapatite-coated titanium implant for enhanced in vitro chemoprevention, osteogenesis, and in vivo osseointegration. ACS Appl Mater Interfaces. 2020;12(12):13644–13656. doi:10.1021/acsami.9b22474
172. Ji C, Bi L, Li J, Fan J. Salvianolic acid B-loaded chitosan/hydroxyapatite scaffolds promotes the repair of segmental bone defect by angiogenesis and osteogenesis. Int J Nanomed. 2019;14:8271–8284. doi:10.2147/IJN.S219105
173. Vimalraj S, Saravanan S, Hariprabu G, et al. Kaempferol-zinc(II) complex synthesis and evaluation of bone formation using zebrafish model. Life Sci. 2020;256:117993. doi:10.1016/j.lfs.2020.117993
174. Yu X, Wang Y, Liu X, Ge Y, Zhang S. Ursolic acid loaded-mesoporous hydroxylapatite/ chitosan therapeutic scaffolds regulate bone regeneration ability by promoting the M2-type polarization of macrophages. Int J Nanomed. 2021;16:5301–5315. doi:10.2147/IJN.S323033
175. Lee S, Chang YY, Lee J, et al. Surface engineering of titanium alloy using metal-polyphenol network coating with magnesium ions for improved osseointegration. Biomater Sci. 2020;8(12):3404–3417. doi:10.1039/d0bm00566e
176. Shang F, Yu Y, Liu S, et al. Advancing application of mesenchymal stem cell-based bone tissue regeneration. Bioact Mater. 2021;6(3):666–683. doi:10.1016/j.bioactmat.2020.08.014
177. Song N, Scholtemeijer M, Shah K. Mesenchymal stem cell immunomodulation: mechanisms and therapeutic potential. Trends Pharmacol Sci. 2020;41(9):653–664. doi:10.1016/j.tips.2020.06.009
178. Hutchings G, Moncrieff L, Dompe C, et al. Bone regeneration, reconstruction and use of osteogenic cells; from basic knowledge, animal models to clinical trials. JCM. 2020;9(1):139. doi:10.3390/jcm9010139
179. Zhou T, Yuan Z, Weng J, et al. Challenges and advances in clinical applications of mesenchymal stromal cells. J Hematol Oncol. 2021;14(1):24. doi:10.1186/s13045-021-01037-x
180. Li M, Jiang Y, Hou Q, Zhao Y, Zhong L, Fu X. Potential pre-activation strategies for improving therapeutic efficacy of mesenchymal stem cells: current status and future prospects. Stem Cell Res Ther. 2022;13(1):146. doi:10.1186/s13287-022-02822-2
181. Jung S, Panchalingam KM, Rosenberg L, Behie LA. Ex vivo expansion of human mesenchymal stem cells in defined serum-free media. Stem Cells Int. 2012;2012:123030. doi:10.1155/2012/123030
182. Bijonowski BM, Yuan X, Jeske R, Li Y, Grant SC. Cyclical aggregation extends in vitro expansion potential of human mesenchymal stem cells. Sci Rep. 2020;10(1):20448. doi:10.1038/s41598-020-77288-4
183. Neri S. Genetic stability of mesenchymal stromal cells for regenerative medicine applications: a fundamental biosafety aspect. Int J Mol Sci. 2019;20(10):2406. doi:10.3390/ijms20102406
184. Marote A, Teixeira FG, Mendes-Pinheiro B, Salgado AJ. MSCs-derived exosomes: cell-secreted nanovesicles with regenerative potential. Front Pharmacol. 2016;7:231. doi:10.3389/fphar.2016.00231
185. Yu T, Zhao IS, Pan H, et al. Extracellular vesicle-functionalized bioactive scaffolds for bone regeneration. Asian J Pharm Sci. 2024;19(5):100945. doi:10.1016/j.ajps.2024.100945
186. Farooqi AA, Desai NN, Qureshi MZ, et al. Exosome biogenesis, bioactivities and functions as new delivery systems of natural compounds. Biotechnol Adv. 2018;36(1):328–334. doi:10.1016/j.biotechadv.2017.12.010
187. Kalluri R, LeBleu VS. The biology, function, and biomedical applications of exosomes. Science. 2020;367(6478):eaau6977. doi:10.1126/science.aau6977
188. Zhu Q, Heon M, Zhao Z, He M. Microfluidic engineering of exosomes: editing cellular messages for precision therapeutics. Lab Chip. 2018;18(12):1690–1703. doi:10.1039/c8lc00246k
189. Sterzenbach U, Putz U, Low LH, Silke J, Tan SS, Howitt J. Engineered exosomes as vehicles for biologically active proteins. Mol Ther. 2017;25(6):1269–1278. doi:10.1016/j.ymthe.2017.03.030
190. Chamberlain CS, Clements AEB, Kink JA, et al. Extracellular vesicle-educated macrophages promote early achilles tendon healing. Stem Cells. 2019;37(5):652–662. doi:10.1002/stem.2988
191. Furuta T, Miyaki S, Ishitobi H, et al. Mesenchymal stem cell-derived exosomes promote fracture healing in a mouse model. Stem Cells Transl Med. 2016;5(12):1620–1630. doi:10.5966/sctm.2015-0285
192. Wang D, Cao H, Hua W, et al. Mesenchymal stem cell-derived extracellular vesicles for bone defect repair. Membranes. 2022;12(7):716. doi:10.3390/membranes12070716
193. Yang H, Cong M, Huang W, et al. The effect of human bone marrow mesenchymal stem cell-derived exosomes on cartilage repair in rabbits. Stem Cells Int. 2022;2022:5760107. doi:10.1155/2022/5760107
194. Liang B, Liang JM, Ding JN, Xu J, Xu JG, Chai YM. Dimethyloxaloylglycine-stimulated human bone marrow mesenchymal stem cell-derived exosomes enhance bone regeneration through angiogenesis by targeting the AKT/mTOR pathway. Stem Cell Res Ther. 2019;10(1):335. doi:10.1186/s13287-019-1410-y
195. Maity S, Das F, Ghosh-Choudhury N, Kasinath BS, Ghosh Choudhury G. High glucose increases miR-214 to power a feedback loop involving PTEN and the Akt/mTORC1 signaling axis. FEBS Lett. 2019;593(16):2261–2272. doi:10.1002/1873-3468.13505
196. Takeuchi R, Katagiri W, Endo S, Kobayashi T. Exosomes from conditioned media of bone marrow-derived mesenchymal stem cells promote bone regeneration by enhancing angiogenesis. PLoS One. 2019;14(11):e0225472. doi:10.1371/journal.pone.0225472
197. Liu X, Yang Y, Li Y, et al. Integration of stem cell-derived exosomes with in situ hydrogel glue as a promising tissue patch for articular cartilage regeneration. Nanoscale. 2017;9(13):4430–4438. doi:10.1039/c7nr00352h
198. Al-Sowayan B, Alammari F, Alshareeda A. Preparing the bone tissue regeneration ground by exosomes: from diagnosis to therapy. Molecules. 2020;25(18):4205. doi:10.3390/molecules25184205
199. Tajafrooz F, Ghofrani S, Sadeghghomi F, et al. Exosome-based therapeutics in bone regeneration: from fundamental biology to clinical translation. Stem Cell Res Ther. 2025;16(1):555. doi:10.1186/s13287-025-04686-8
200. Wan L, Liu F, Wang A, et al. PI3K/Akt pathway-mediated enhancement of bone and vascular regeneration by gelatin/hyaluronic acid/exosome composite scaffold in bone tissue engineering. Biomaterials Advances. 2025;166:214064. doi:10.1016/j.bioadv.2024.214064
201. Luo L, Zheng W, Li J, et al. 3D‐printed titanium trabecular scaffolds with sustained release of hypoxia‐induced exosomes for dual‐mimetic bone regeneration. Adv Sci. 2025;12(23):2500599. doi:10.1002/advs.202500599
202. Huber J, Griffin MF, Longaker MT, Quarto N. Exosomes: a tool for bone tissue engineering. Tissue Eng B: Rev. 2022;28(1):101–113. doi:10.1089/ten.TEB.2020.0246
203. Lu Y, Mai Z, Cui L, Zhao X. Engineering exosomes and biomaterial-assisted exosomes as therapeutic carriers for bone regeneration. Stem Cell Res Ther. 2023;14(1):55. doi:10.1186/s13287-023-03275-x
204. Su N, Villicana C, Yang F. Immunomodulatory strategies for bone regeneration: a review from the perspective of disease types. Biomaterials. 2022;286:121604. doi:10.1016/j.biomaterials.2022.121604
205. Xue P, Wang J, Fu Y, He H, Gan Q, Liu C. Material‐mediated immunotherapy to regulate bone aging and promote bone repair. Small. 2025;21(11). doi:10.1002/smll.202409886
206. Kang F, Yi Q, Gu P, et al. Controlled growth factor delivery system with osteogenic-angiogenic coupling effect for bone regeneration. J Orthop Translat. 2021;31:110–125. doi:10.1016/j.jot.2021.11.004
207. Wang Y, Liu L, Qu Z, et al. Tanshinone ameliorates glucocorticoid-induced bone loss via activation of AKT1 signaling pathway. Front Cell Dev Biol. 2022;10:878433. doi:10.3389/fcell.2022.878433
208. Cheng L, Zhou S, Zhao Y, et al. Tanshinone IIA attenuates osteoclastogenesis in ovariectomized mice by inactivating NF-kB and Akt signaling pathways. Am J Transl Res. 2018;10(5):1457–1468.
209. Ma C, Wang Z, Mo L, et al. Tanshinone I attenuates estrogen-deficiency bone loss via inhibiting RANKL-induced MAPK and NF-κB signaling pathways. Int Immunopharmacol. 2024;127:111322. doi:10.1016/j.intimp.2023.111322
210. Jiang T, Hu G, Yang R, Guan Z. Panax notoginseng saponins regulate angiogenic cytokines through the PI3K/AKT/mTOR signaling pathway to promote fracture healing in ovariectomized rats. J Med Food. 2024;27(9):824–833. doi:10.1089/jmf.2024.k.0014
211. Xing Y, Qiu L, Liu D, Dai S, Sheu CL. The role of smart polymeric biomaterials in bone regeneration: a review. Front Bioeng Biotechnol. 2023;11. doi:10.3389/fbioe.2023.1240861
212. Yuan X, Zhu W, Yang Z, et al. Recent advances in 3D printing of smart scaffolds for bone tissue engineering and regeneration. Adv Mater. 2024;36(34). doi:10.1002/adma.202403641
213. Percival KM, Paul V, Husseini GA. Recent advancements in bone tissue engineering: integrating smart scaffold technologies and bio-responsive systems for enhanced regeneration. Int J Mol Sci. 2024;25(11):6012. doi:10.3390/ijms25116012
214. Schulze F, Lang A, Schoon J, Wassilew GI, Reichert J. Scaffold guided bone regeneration for the treatment of large segmental defects in long bones. Biomedicines. 2023;11(2):325. doi:10.3390/biomedicines11020325
215. Niu Y, Du T, Liu Y. Biomechanical characteristics and analysis approaches of bone and bone substitute materials. J Funct Biomater. 2023;14(4):212. doi:10.3390/jfb14040212
216. Amponsah O, Nopuo PSA, Manga FA, Catli NB, Labus K. Future-oriented biomaterials based on natural polymer resources: characteristics, application innovations, and development trends. Int J Mol Sci. 2025;26(12):5518. doi:10.3390/ijms26125518
217. Zhang B, Baino F. Sustainable bioceramics, biopolymers, and composites for bone applications: from bench to production. Int J Appl Ceram Technol. 2025;e70071. doi:10.1111/ijac.70071
218. Shen C, Shen A. 4D printing: innovative solutions and technological advances in orthopedic repair and reconstruction, personalized treatment and drug delivery. Biomed Eng Online. 2025;24(1):5. doi:10.1186/s12938-025-01334-3
219. Du R, Zhao B, Luo K, et al. Shape memory polyester scaffold promotes bone defect repair through enhanced osteogenic ability and mechanical stability. ACS Appl Mater Interfaces. 2023;15(36):42930–42941. doi:10.1021/acsami.3c06902
220. Liu C, Lou Y, Sun Z, et al. 4D printing of personalized-tunable biomimetic periosteum with anisotropic microstructure for accelerated vascularization and bone healing. Adv Healthcare Mater. 2023;12(22):e2202868. doi:10.1002/adhm.202202868
221. Zhou W, Dong X, He Y, Zheng W, Leng J. In-vitro and in-vivo studies of 4D printed shape memory scaffolds with bioactive fillers and coating for enhanced bone tissue regeneration. Smart Mater Struct. 2022;31(10):105002. doi:10.1088/1361-665X/ac884a
222. Lin Y, Zhang Y, Wang D, Yang B, Shen Y-Q. Computer especially AI-assisted drug virtual screening and design in traditional Chinese medicine. Phytomedicine. 2022;107:154481. doi:10.1016/j.phymed.2022.154481
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.