Back to Journals » Open Access Emergency Medicine » Volume 14
Emergency Medicine Physicians’ Views on Providing Unnecessary Management in the Emergency Department
Authors Alalshaikh A ![]() , Alyahya B, Almohawes M, Alnowiser M
, Alyahya B, Almohawes M, Alnowiser M ![]() , Ghandour M, Alyousef M, Abuguyan F
, Ghandour M, Alyousef M, Abuguyan F ![]() , Almehlisi A, Altuwaijri F
, Almehlisi A, Altuwaijri F ![]() , Alageel M
, Alageel M
Received 29 September 2021
Accepted for publication 15 March 2022
Published 26 April 2022 Volume 2022:14 Pages 183—193
DOI https://doi.org/10.2147/OAEM.S341709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Abdulaziz Alalshaikh,1 Bader Alyahya,1 Mohammed Almohawes,2 Mosaed Alnowiser,2 Mohammed Ghandour,2 Mohammed Alyousef,2 Fahad Abuguyan,1 Abdulaziz Almehlisi,1 Fawaz Altuwaijri,1 Mohammed Alageel1,3
1Emergency Medicine Department, King Saud University, Riyadh, Saudi Arabia; 2College of Medicine, King Saud University, Riyadh, Saudi Arabia; 3Emergency Medicine Department, The University of British Columbia, Vancouver, BC, Canada
Correspondence: Abdulaziz Alalshaikh, PO Box 7805, Riyadh, 11472, Saudi Arabia, Tel +966553993950, Email [email protected] Bader Alyahya, Tel +966555141174, Email [email protected]
Purpose: To assess the views of emergency medicine physicians (EMPs) on the practice of providing unnecessary medical management in the emergency department.
Methods: All EMPs in Saudi Arabia were approached to participate in this cross-sectional study. A self-administered online survey that collected the participants’ demographic information and opinions regarding the unnecessary management provided by EMPs in Saudi Arabia was conducted between December 2020 and February 2021. SPSS 22.0 was used to analyze the data.
Results: A total of 181 EMPs returned the questionnaire. More than 80% of the participants believed that EMPs order unnecessary tests or procedures at least a few times per week. The major reasons for ordering unnecessary medical tests or procedures were “concern about malpractice issues” (60.8%), “not having enough time with a patient for meaningful discussion” (47%), and “just to be safe” (46.4%). More than 55% of the respondents also believed that EMPs are in the best position to address the problem of unnecessary testing.
Conclusion: Most of the EMPs who participated in this study recognized that ordering unnecessary tests is a serious problem that happens on a daily basis. Many factors and reasons were described by the participants, and multiple possible solutions were suggested to help overcome the issue. Evaluating physicians’ perspectives on the issue is a key step in addressing the problem and implementing appropriate interventions.
Keywords: emergency medicine physician, unnecessary investigation, Saudi Arabia, overdiagnosis, over-testing
Introduction
A considerable proportion of the care provided to patients is not clinically indicated and may possibly cause harm.1 For emergency medicine physicians (EMPs), malpractice concerns and diagnostic uncertainty are the most common reasons for ordering unnecessary imaging or treatment.2 Unnecessary services cost the United States health care system approximately 200 billion dollars annually.3 Lyu et al showed that 20.6% of overall medical care was unnecessary, including 22.0% of prescribed medications, 24.9% of tests, and 11.1% of procedures.4 Ordering unnecessary tests is the most common form of defensive medicine reported by 59% of physicians.5 Unnecessary advanced imaging studies seem to be particularly problematic in the emergency department (ED). In one study, 97% of the EMPs evaluated felt that at least some of the advanced imaging studies they requested were not medically indicated.6
A National Survey of Physicians conducted by American Board of Internal Medicine (ABIM), Part of Choosing Wisely campaign, investigated the reasons behind over-testing. Surveyed physicians believed that the reasons include defensive medical practices (52%) and uncertainty in making a clinical diagnosis (36%). The need for more information for reassurance (30%), patient insistence (28%), the need to keep the patient happy (23%), and not having enough time with the patients (13%) were other reasons mentioned.2 Moreover, such factors as unfamiliarity with costs by the health care giver, overdependence on protocols and algorithms, inexperience, as well as gaps in training and education can be part of the problem.7 Kanzaria et al surveyed EMPs in the United States on their perceptions toward ordering unnecessary advanced diagnostic imaging and its contributing factors. Fear of missing a diagnosis and avoidance of malpractice-related consequences were the most common reasons cited for ordering unnecessary tests. However, 39.7% of the participants felt that patient or family expectations were almost always a reason, and 23% indicated that doing so saves time.8
Although overuse of investigations and treatments might satisfy patients who seek them, some studies have shown that overutilization of health care services is not associated with better outcomes.9 In addition, the introduction of electronic health records may lead to the liberal use of investigations and imaging.10 Interestingly, overdiagnosis might put patients at greater risk by exposing those with low risk to invasive procedures, unnecessary radiation, or medically unjustified treatments, such as catheterization and revascularization in chest pain patients after cardiac workup.11 Other examples of overdiagnosis include the inappropriate use of d-dimer as a screening test for pulmonary embolism, treating asymptomatic patients with positive urinalysis results, and requesting computed tomography scans of the brain in patients who present to the ED after minor head injury.12–15 In spite of the wealth of data on the matter, few studies have assessed EMPs’ perceptions on providing unnecessary medical services to patients globally and in Saudi Arabia particularly. This study was conducted to assess the views of EMPs in Saudi Arabia on the practice of ordering unnecessary investigations and treatments.
Methods
Study Design, Setting, and Participants
This was a cross-sectional study that targeted all EMPs who were registered with the Saudi Commission for Health Specialties (SCFHS), which is the regulatory body for health professions, with no restriction on the exact number of their years of practice, age, and sex. Physicians working in other departments or outside Saudi Arabia were excluded. A self-administered online survey questionnaire using Google forms was prepared and sent to the target population via email through several sources, including the SCFHS. The exact number of EMPs approached was unknown to us because the invitation was also sent out by the SCFHS, not only by the research team.
Study Tools
We used a validated survey (Unnecessary Tests and Procedures in the Health Care System) with permission from the ABIM Foundation, which is a copyright-holding foundation.2 The survey questionnaire was piloted on 10 EMPs who were excluded from the actual sample. It collected the participants’ demographic information (eg, sex, age, compensation, and primary workplace) and included questions about the magnitude of the problem as well as possible solutions. The typical time spent to fill the questionnaire was 10 minutes.
We briefed the participants regarding the objectives of the study and their right to withdraw at any time without any obligation toward the study team, and we obtained their informed consent before administering the survey. Participant anonymity was maintained at all times. This study required a minimum sample size of 148 participants to achieve a 95% confidence interval of ±5% width as well as based on assumptions of statistical significance at <0.05 and a 20% non-response rate. It was approved by the institutional review board of King Saud University Medical City (Riyadh, Kingdom of Saudi Arabia) on December 24, 2020. We targeted all EMPs in Saudi Arabia whom we could reach and collected data over 14 days (through January and February 2021).
Statistical Analysis
Data were analyzed using SPSS 22.0 (IBM, New York, NY, USA). Categorical variables were assessed using χ2 analysis and expressed as percentages. P < 0.05 was considered statistically significant.
Results
A total of 181 EMPs returned the questionnaire; their demographic data and responses to our survey are reported in Table 1. Of the respondents, 158 (87.3%) were male, 62.4% were <40 years old, 40.9% were consultants, and 38.7% were residents. More than one-fifth of the participants reported working >20 clinical shifts per month in the ED. Only 15% of the participants had a fee-for-service payment system as one, or their only, source of compensation.
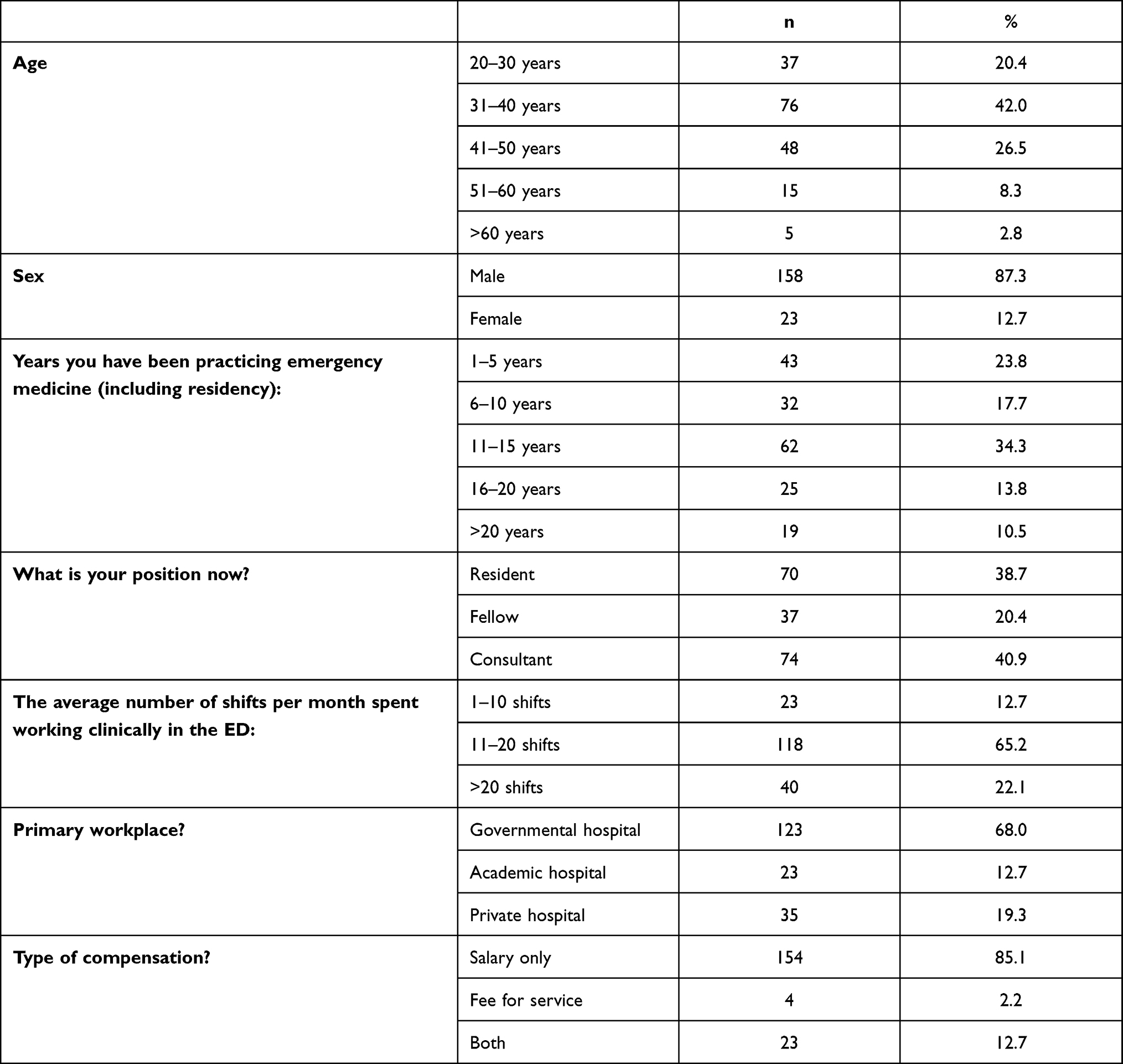 |
Table 1 Characteristics of the Survey Participants (N = 181) |
With regard to the magnitude of the problem, >80% of the participants believed that EMPs order unnecessary tests or procedures at least a few times per week, as shown in Table 2. More than 55% also believed that physicians are in the best position to address the problem of unnecessary testing. Almost half of the participants said that they will refuse to order unnecessary tests even if the patient insisted, and 37% said that they will order the test but will give reasons to convince the patient that it is unnecessary.
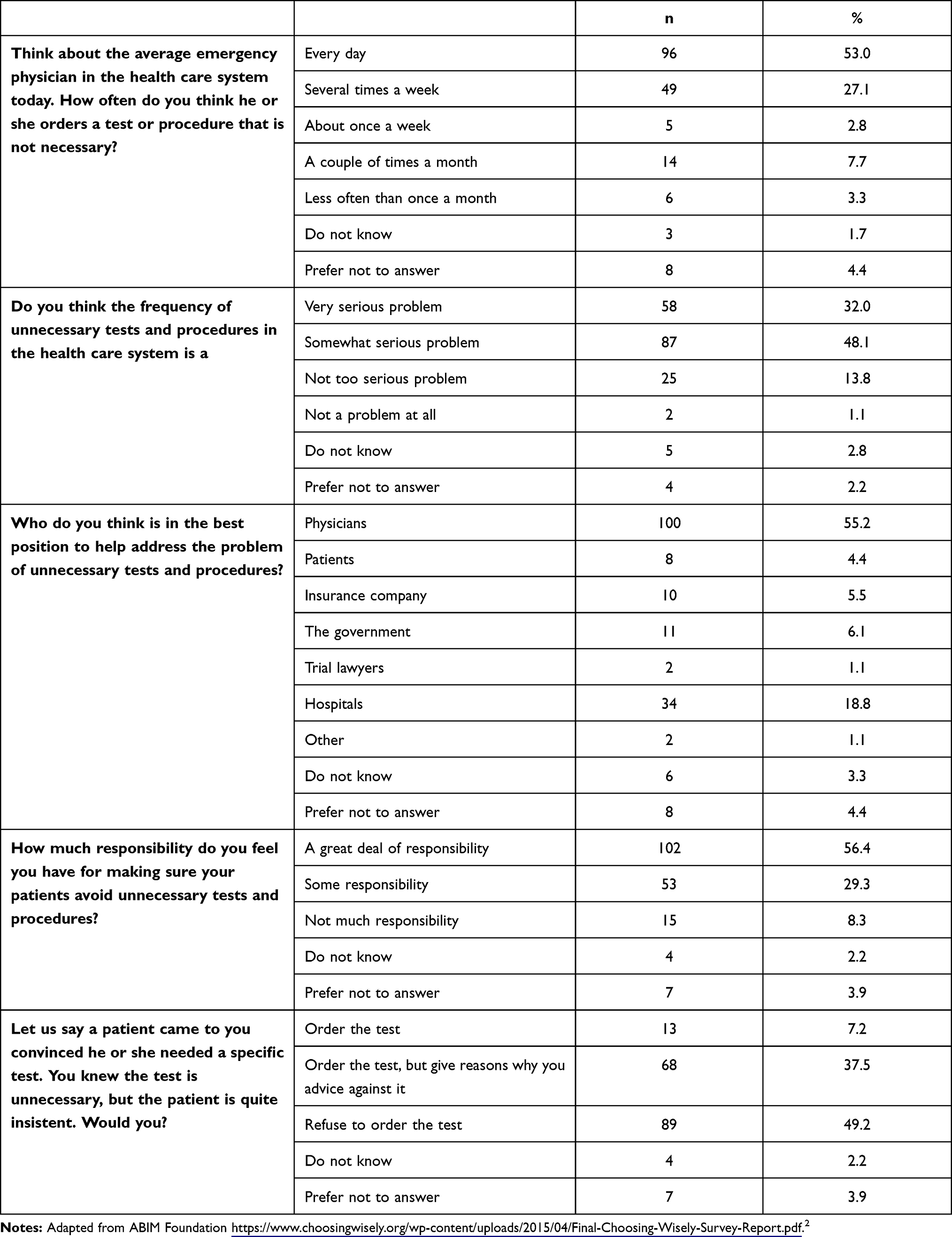 |
Table 2 Responses of the Survey Participants (N = 181) Regarding the Amplitude of Providing Unnecessary Management in Emergency Departments |
As shown in Table 3, the major reasons for ordering unnecessary medical tests or procedures were “concern about malpractice issues” (60.8%), “not having enough time with a patient for meaningful discussion” (47%), and “just to be safe” (46.4%). Meanwhile, the fee-for-service payment system was selected the least as a reason for ordering unnecessary tests or procedures by the respondents, followed by having new technology in their field of practice.
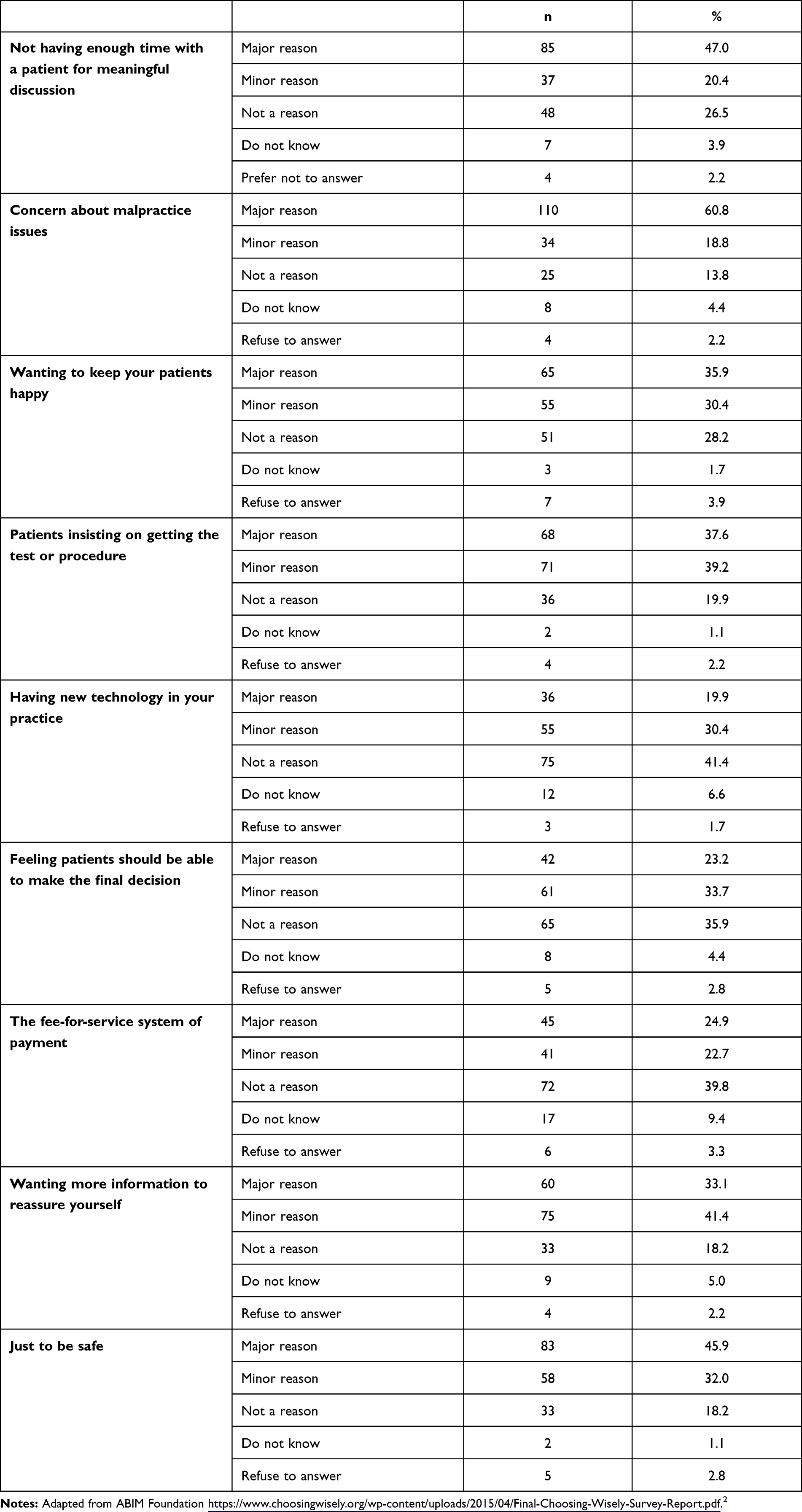 |
Table 3 Reasons of the Survey Participants (N = 181) for Ordering Unnecessary Tests |
Physicians with >10 years of experience were significantly more interested than physicians with less than five years of experience (84% vs 60.5%, P < 0.016) in learning about evidence-based recommendations that address when certain tests and procedures may be unnecessary (Table 4). A higher percentage of EMPs who worked <10 shifts per month were more likely to order unnecessary tests without counseling the patient compared with those who worked 11 to 20 shifts per month (30.4% vs 4.2%).
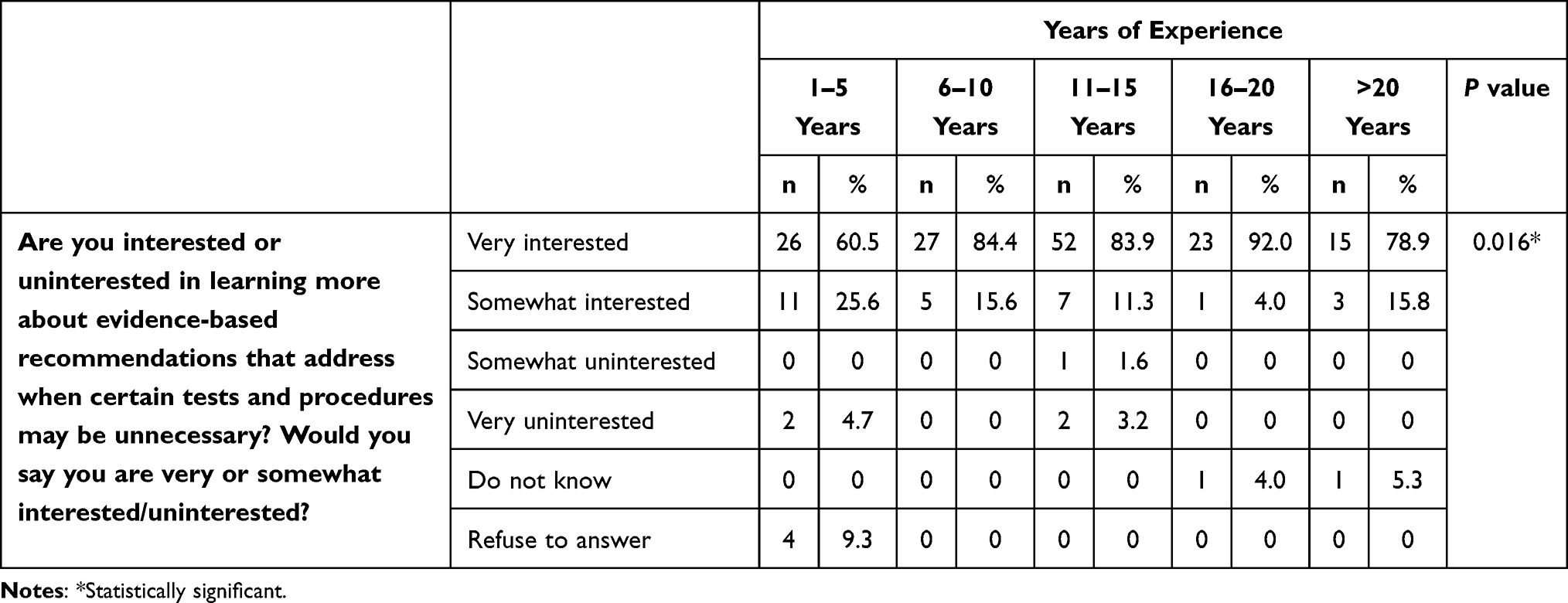 |
Table 4 Relationship Between the Survey Participants’ Interest in Learning and Years of Experience |
When asked about the proposed solutions, 51% of the participants believe that malpractice reform would be very effective. In addition, 48% think that having patient-targeted evidence-based recommendations discussing unnecessary management would be another very effective solution. The great majority of our participants (79%) are interested in learning evidence-based recommendations addressing this issue (Table 5).
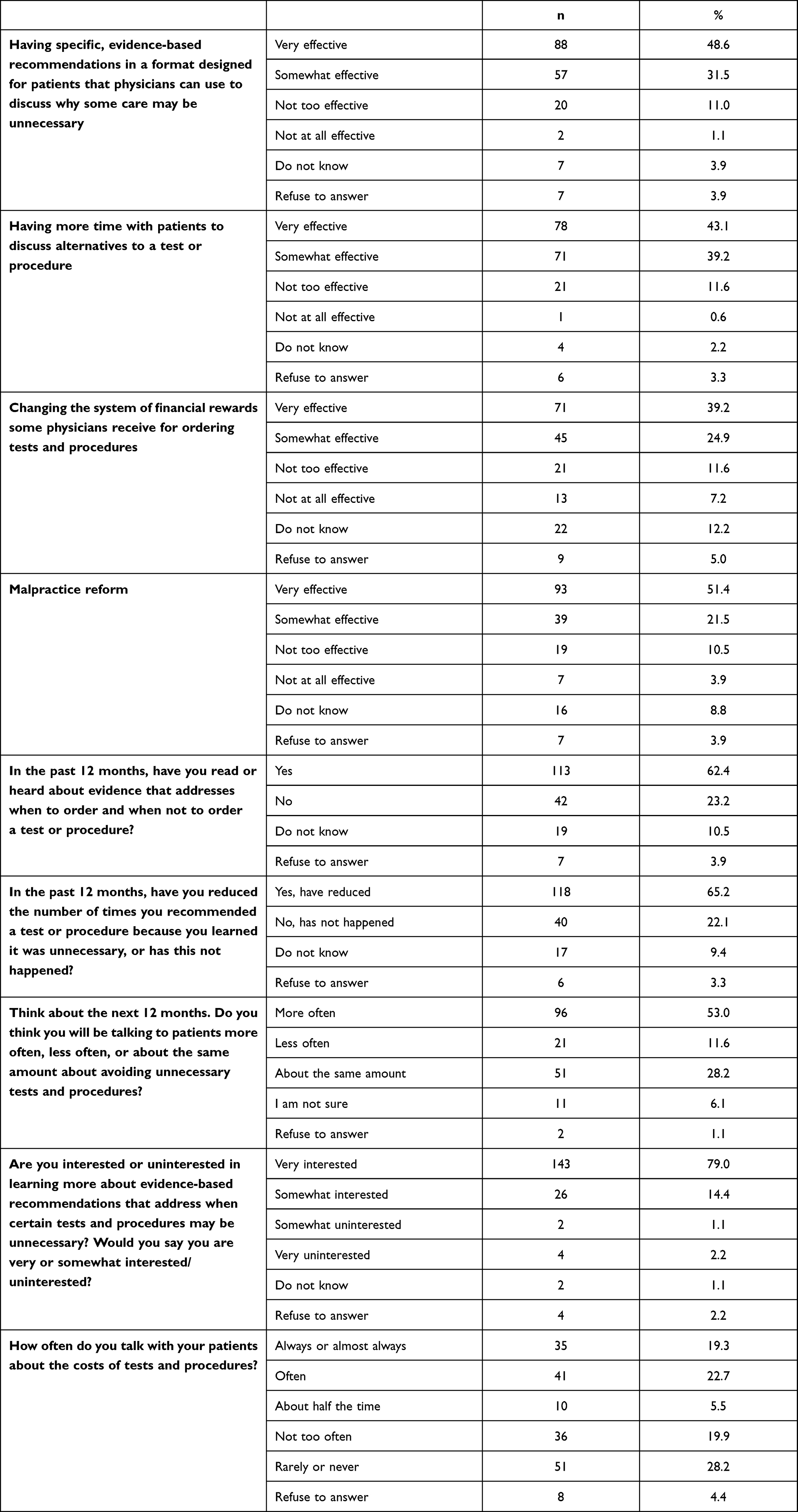 |
Table 5 Possible Solutions Suggested by the Survey Participants (N = 181) to Address the Issue of Providing Unnecessary Management |
Discussion
The main objective of this study was to evaluate EMPs’ perceptions on the issue of providing unnecessary management to patients in the ED. We found that most of our participants identified providing unnecessary management to patients in the ED as a very serious or somewhat serious problem (80%) and believed that physicians are in the best position to address the issue (55%), which are consistent with the findings of the Choosing Wisely Campaign.2 Notably, however, 80.1% of the respondents thought that they or their colleagues ordered unnecessary tests or procedures every day or at least several times per week, which is higher than the rates reported for the Choosing Wisely Campaign (30%) and by Lyu et al (15–30%).2,4 On the other hand, in the study by Kanzaria et al 85% of the EMPs believed that a superabundant number of tests were ordered in their ED.8
Most EMPs reported that concerns of malpractice were their main reason for ordering unnecessary medical services. This finding is similar to that reported in previous studies.2,4,8 The fear of legal threat and malpractice suits can impact physicians’ practice and may lead them to engage in defensive medicine. Compared to the United Kingdom, the culture of litigation and compensation in Saudi Arabia is still developing, with most procedures of mediation and conciliation of potential medical errors being conducted in an informal way. This may explain the lower cost of medical claims and awarded compensations in Saudi Arabia compared with many parts of the world.16
Almost 50% of our respondents considered “not having enough time with a patient for meaningful discussion” as a major reason for ordering unnecessary management, which is higher than the rates reported for the Choosing Wisely Campaign (13%) and by Lyu et al (37.4%).2,4 Spending more time with patients as well as having enough time to explain their condition and the management they need may contribute to solving the issue. Approximately half of the participants stated they would refuse to order unnecessary medical services even if the patient insisted. This finding contradicts our hypothesis that most EMPs would order unnecessary services to seek patient satisfaction, because studies have found a positive correlation between the number of health care services provided and patient satisfaction.17,18 However, this observation could be related to most of our respondents’ sense of great responsibility to make sure that patients avoid unnecessary management.
Interestingly, we found that physicians with more than ten years of experience are significantly more interested than those with five or less years of experience in learning about evidence-based recommendations addressing unnecessary tests or procedures. This could be because physicians with less than five years of experience had recently graduated and are more updated than their older colleagues. Another interesting finding is that EMPs who work less than 10 shifts per month are more likely to order unnecessary tests than those who work 11 to 20 shifts per month. Possibly, those who work more shifts are more confident with their clinical skills and do not need tests to confirm their diagnosis. On the other hand, EMPs who work fewer shifts order tests instead of spending more time with patients to improve their department flow.
In this study, the participants agreed that having more time with patients and having evidence-based recommendations that they can use to convince patients why some services may be unnecessary would be very effective solutions to the issue of providing unnecessary management. Clinical practice guidelines should not encourage increased screening or diagnostic testing without taking the consequences of over-testing and overtreating into account.4 Addressing the impact of providing unnecessary medical health services on both the patient care level and the health care system can help not only facilitate a better quality of care but also reduce the cost of health care. In addition, educating and involving the patient in the clinical decision-making process have been recommended to avoid resorting to the overuse of medical services and overtreatment.4,6–8
This study has several limitations. First, it focused on the views of physicians from Saudi Arabia only; however, the prevalence of the issue of providing unnecessary management in the ED and its financial burden in Saudi Arabia are unknown. Second, although we met our target population size, the possibility of sampling bias cannot be ruled out. Third, this study is limited by its cross-sectional design, which typically limits the confirmation of the temporality and causality of the factors explored. Finally, we were not aware of the exact number of EMPs who were invited to participate in the survey and hence did not calculate the response rate.
Conclusion
In conclusion, we found that most of the EMPs who participated in this study recognized that ordering unnecessary tests is a serious problem that happens on a daily basis. The respondents described many factors and reasons for its incidence, and they suggested multiple possible solutions to help overcome it. Evaluating physicians’ perspectives on the issue is a key step in addressing it and implementing appropriate interventions.
Abbreviations
EMP, emergency medicine physician; ED, emergency department; SCFHS, Saudi Commission for Health Specialties.
Data Sharing Statement
Data related to this study are presented in the Results section. Raw data can be obtained from the corresponding author Abdulaziz Alalshaikh ([email protected]) upon reasonable request.
Ethics Approval and Consent to Participate
Approval for this study was obtained from the ethics committee of the King Saud University College of Medicine (Riyadh, Kingdom of Saudi Arabia) on December 24, 2021. The emergency medicine physicians’ informed consent to participate was obtained before the survey was administered, and the participants were given the right to withdraw at any time without any obligation toward the study team. Participant anonymity was guaranteed and maintained.
Acknowledgments
We would like to thank the ABIM Foundation for granting us the permission to use their survey in this study. We also would like to thank Mr. Ahmad H. Al-Sharqawi for his contribution to data analysis. Moreover, we would like to thank all the people who participated in the research for their patience and kindness.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The funding for this research was obtained by the Department of Emergency Medicine, College of Medicine, King Saud University. The funding body had no role in the design of the study; in data collection, analysis, and interpretation; as well as in writing the manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Newton EH. Addressing overuse in emergency medicine: evidence of a role for greater patient engagement. Clin Exp Emerg Med. 2017;4(4):189. doi:10.15441/ceem.17.233
2. ABIM Foundation. Unnecessary tests and procedures in the health care system physicians say unnecessary tests and procedures are a serious problem, and feel a responsibility to address the issue. ABIM Found; 2014:1–13. Available from: https://www.choosingwisely.org/wp-content/uploads/2015/04/Final-Choosing-Wisely-Survey-Report.pdf.
3. McGinnis JM, Stuckhardt L, Saunders R, Smith M. Best care at lower cost: the path to continuously learning health care in America. 2013.
4. Lyu H, Xu T, Brotman D, et al. Overtreatment in the United States. PLoS One. 2017;12(9):e0181970. doi:10.1371/journal.pone.0181970
5. Ortashi O, Virdee J, Hassan R, Mutrynowski T, Abu-Zidan F. The practice of defensive medicine among hospital doctors in the United Kingdom. BMC Med Ethics. 2013;14(1):1–6. doi:10.1186/1472-6939-14-42
6. Studdert DM, Mello MM, Sage WM, et al. Defensive medicine among high-risk specialist physicians in a volatile malpractice environment. JAMA. 2005;293(21):2609–2617. doi:10.1001/jama.293.21.2609
7. Bhardwaj A. Excessive ancillary testing by healthcare providers: reasons and proposed solutions. J Hosp Med Manag. 2019;04(01):1–6.
8. Kanzaria HK, Hoffman JR, Probst MA, Caloyeras JP, Berry SH, Brook RH. Emergency physician perceptions of medically unnecessary advanced diagnostic imaging. Acad Emerg Med. 2015;22(4):390–398. doi:10.1111/acem.12625
9. Brownlee S, Chalkidou K, Doust J, et al. Evidence for overuse of medical services around the world. Lancet. 2017;390(10090):156–168. doi:10.1016/S0140-6736(16)32585-5
10. Ibrahim Hakim BBA, Hathi S, Nair A, Narula T, Bhattacharya J. Electronic health records and the frequency of diagnostic test orders. Am J Manag Care. 2017;23(1):e16–e23.
11. Foy AJ, Liu G, Davidson WR, Sciamanna C, Leslie DL. Comparative effectiveness of diagnostic testing strategies in emergency department patients with chest pain: an analysis of downstream testing, interventions, and outcomes. JAMA Intern Med. 2015;175(3):428–436. doi:10.1001/jamainternmed.2014.7657
12. Goldstein NM, Kollef MH, Ward S, Gage BF. The impact of the introduction of a rapid D-dimer assay on the diagnostic evaluation of suspected pulmonary embolism. Arch Intern Med. 2001;161(4):567–571. doi:10.1001/archinte.161.4.567
13. Yin P, Kiss A, Leis JA. Urinalysis orders among patients admitted to the general medicine service. JAMA Intern Med. 2015;175(10):1711–1713. doi:10.1001/jamainternmed.2015.4036
14. Shobeirian F, Ghomi Z, Soleimani R, Mirshahi R, Sanei Taheri M. Overuse of brain CT scan for evaluating mild head trauma in adults. Emerg Radiol. 2021;28(2):251–257. doi:10.1007/s10140-020-01846-6
15. Melnick ER, Szlezak CM, Bentley SK, Dziura JD, Kotlyar S, Post LA. CT overuse for mild traumatic brain injury. Jt Comm J Qual Patient Saf. 2012;38(11):483–489. doi:10.1016/s1553-7250(12)38064-1
16. Alkhenizan AH, Shafiq MR. The process of litigation for medical errors in Saudi Arabia and the United Kingdom. Saudi Med J. 2018;39(11):1075. doi:10.15537/smj.2018.11.22854
17. Manzoor F, Wei L, Hussain A, Asif M, Shah SIA. Patient satisfaction with health care services; an application of physician’s behavior as a moderator. Int J Environ Res Public Health. 2019;16(18):3318. doi:10.3390/ijerph16183318
18. Almatrafi D, Altaweel N, Abdelfattah M, et al. Assessment of customer satisfaction with the clinical laboratory services provided in King Abdullah Medical City, Makkah. Egypt J Hosp Med. 2018;70(11):2029–2037. doi:10.12816/0044864
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.