Back to Journals » Open Access Emergency Medicine » Volume 14
Emergency Medical Services Prehospital Response to the COVID-19 Pandemic in the US: A Brief Literature Review
Authors Ventura CAI ![]() , Denton EE, David JA, Schoenfelder BJ
, Denton EE, David JA, Schoenfelder BJ ![]() , Mela L, Lumia RP, Rudi RB, Haldar B
, Mela L, Lumia RP, Rudi RB, Haldar B
Received 11 March 2022
Accepted for publication 23 May 2022
Published 30 May 2022 Volume 2022:14 Pages 249—272
DOI https://doi.org/10.2147/OAEM.S366006
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Christian Angelo I Ventura,1– 3 Edward E Denton,3– 5 Jessica Anastacia David,6 Brianna J Schoenfelder,7 Lillian Mela,8 Rebecca P Lumia,9 Rachel B Rudi,3 Barnita Haldar3,10
1Department of Graduate Medical Sciences, Boston University School of Medicine Boston, Boston, MA, USA; 2Department of Health, Behavior and Society (Incoming), Johns Hopkins Bloomberg School of Public Health Baltimore, Baltimore, MD, USA; 3EMS Pandemic Response Research Laboratory Lawrenceville, Lawrenceville, NJ, USA; 4Department of Emergency Medicine, University of Arkansas for Medical Sciences Little Rock, Little Rock, AR, USA; 5Fay W. Boozman College of Public Health, University of Arkansas for Medical Sciences Little Rock, Little Rock, AR, USA; 6Department of Biochemistry and Microbiology, Rutgers University New Brunswick, Brunswick, NJ, USA; 7Department of Neuroscience, Temple University Philadelphia, Philadelphia, PA, USA; 8Department of Nursing, Simmons University Boston, Boston, MA, USA; 9Department of Biology, Northeastern University Boston, Boston, MA, USA; 10Department of Cell, Developmental, and Integrative Biology, University of Alabama at Birmingham School of Medicine Birmingham, Birmingham, AL, USA
Correspondence: Christian Angelo I Ventura, Tel +1 (732) 372-2141, Email [email protected]; [email protected]
Abstract: This study aimed to analyze prehospital Emergency Medical Services (EMS) response to the COVID-19 pandemic in the US through a brief systematic review of available literature in context with international prehospital counterparts. An exploration of the NCBI repository was performed using a search string of relevant keywords which returned n=5128 results; articles that met the inclusion criteria (n=77) were reviewed and analyzed in accordance with PRISMA and PROSPERO recommendations. Methodical quality was assessed using critical appraisal tools, and the Egger’s test was used for risk of bias reduction upon linear regression analysis of a funnel plot. Sources of heterogeneity as defined by P < 0.10 or I^2 > 50% were interrogated. Findings were considered within ten domains: structural/systemic; clinical outcomes; clinical assessment; treatment; special populations; dispatch/activation; education; mental health; perspectives/experiences; and transport. Findings suggest, EMS clinicians have likely made significant and unmeasured contributions to care during the pandemic via nontraditional roles, ie, COVID-19 testing and vaccine deployment. EMS plays a critical role in counteracting the COVID-19 pandemic in addition to the worsening opioid epidemic, both of which disproportionately impact patients of color. As such, being uniquely influential on clinical outcomes, these providers may benefit from standardized education on care and access disparities such as racial identity. Access to distance learning continuing education opportunities may increase rates of provider recertification. Additionally, there is a high prevalence of vaccine hesitancy among surveyed nationally registered EMS providers. Continued rigorous investigation on the impact of COVID-19 on EMS systems and personnel is warranted to ensure informed preparation for future pandemic and infectious disease responses.
Keywords: EMS, COVID-19, prehospital, pandemic response, EMT, paramedic
Introduction
Prehospital clinical care under the purview of Emergency Medical Services (EMS) has been traditionally understudied in the United States, as illustrated by the scarcity of literature as compared to other allied health professions. Under the federal oversight of the National Highway Traffic Safety Administration (NHTSA), EMS models of care vary drastically, shaped largely by geographic assignment, local community partners, and additional presiding authorities. Common models include municipality-based, private nonprofit, and private for-profit services.1
Within these structural differences exist a subset variance of agencies’ scope of practice. In accordance with the National EMS Scope of Practice Model, the Basic Life Support (BLS) scope extends to Emergency Medical Responders (EMRs) and Emergency Medical Technicians (EMTs), while the Advanced Life Support (ALS) scope is characteristic of Advanced EMTs (AEMTs) and Paramedics (EMT-Ps).2 As of January 2022, COVID-19, the respiratory infection caused by novel SARS-CoV-2, is a leading cause of death in the US.3 This global pandemic has established an unprecedented call for rigorous investigation of resource capacity and competency amid allied health care industries to ascertain structural deficits and strengths that have implications for future pandemic response. Further, preliminary mixed-method studies on EMS pandemic response in the context of the COVID-19 pandemic have identified deficits in the domains of resource availability, continued education, administrative protocols, and decontamination practices.4
Although evidently there is an apparent scarcity of academic literature centering US EMS systems in response to the COVID-19 pandemic, it may be useful to summatively review existing literature of satisfactory methodical quality to highlight research areas that warrant further investigatory attention, as no review of this scope and nature currently exists. In this study, we aimed to systematically review peer-reviewed literature indexed in PubMed pertaining to COVID-19 considerations, effects, and implications on US EMS systems and clinicians within the context of prehospital international counterparts by employing artificial intelligence and conventional PRISMA and PROSPERO recommendations.
Methods
Search Strategy
On 07 March 2022 a PubMed National Center for Biotechnology Information (NCBI) repository search was conducted using the keywords “COVID,” “COVID-19,” “SARS-COV-2,” “CORONAVIRUS,” “EMERGENCY MEDICAL SERVICES,” “EMS”, “EMT”, “PREHOSPITAL,” “OUT OF HOSPITAL,” and “PARAMEDIC.” The returned English results were uploaded to Rayyan.ai for comprehensive abstract and full text review.5
Data Extraction
Duplicate results were assessed for and removed. Editorials, commentaries, and non-peer reviewed manuscripts were excluded. Two investigators independently reviewed abstracts to identify articles eligible for full text review. The investigators then independently reviewed full text articles to identify studies that met the PICOS-guided inclusion criteria.6 Studies were excluded if there were concerns regarding methodical quality or integrity of the data as per discretion of the two investigators and a third consultant. SIGN appraisal tools were used to exclude retrospective and cohort-based studies that did not meet an acceptable level of evidence for inclusion in the review.7 Conflicts were resolved through discussion and by mediation from a third or fourth consultant when necessary. Study methods were consistent with PRISMA recommendations, and although PROSPERO registration was not sought, the work remained faithful to conventional review standards.8,9
Analysis
Stata/BE software was used to assess aggregate prevalence of data. Heterogeneity was defined as P < 0.10 or I^2 > 50% which warranted a fixed effects approach.10 Otherwise, a random effects approach was assumed. We then sought to investigate sources of heterogeneity. During full text review, studies were primarily taxonomized in one of the following ten domains: i. structural/systemic, ii. clinical outcomes, iii. clinical assessment, iv. treatment, v. special populations, vi. dispatch/activation, vii. education, viii. mental health, ix. perspectives/experiences, x. transport.
Methodical Quality
Investigators determined risk of bias for prevalence studies based upon appropriateness of sampling, sampling methods, use of standard assessment methods, and setting characteristics. The criteria were adapted from either the Joanna Briggs Institute Critical Appraisal Checklist for Studies Reporting Prevalence Data or the Joanna Briggs Institute Critical Appraisal Tool for Quasi-Experimental Studies.11,12 A 95% confidence interval was used to standardize prevalence and pooling of data, and the linear regression based Egger’s test was used to analyze the presence of any publication bias after a funnel plot was created and assessed.13 P > 0.05 deemed no risk of publication bias. Microsoft Excel was used to calculate standard deviation and mean. Sensitivity analyses assessed for source of heterogeneity and stability of results. Because the work did not involve the use of human research subjects, it did not require approval or review by an institutional review board or bioethics committee.
Diversity in the Research Team
The work represents a cross-institutional and multi-disciplinary collaboration amongst public health oriented researchers, EMS clinicians, and physician scientists.
Results
The NCBI repository returned n=5128 results, with n=77 utilized for analysis and inclusion in this study. Results were excluded if they did not satisfy the inclusion criteria. Figure 1 depicts an overview of the exclusion schema. AI identified n=111 duplicative results, n=4916 results were excluded due to irrelevance with respect to the area of investigation, and n=24 studies were excluded after investigators performed full text reviews and found studies to be of unsatisfactory evidence levels in accordance with SIGN appraisal guidelines. Table 1 depicts characteristics of studies selected for inclusion, with high confidence in stability and quality of the aggregate data.
 |  |  | 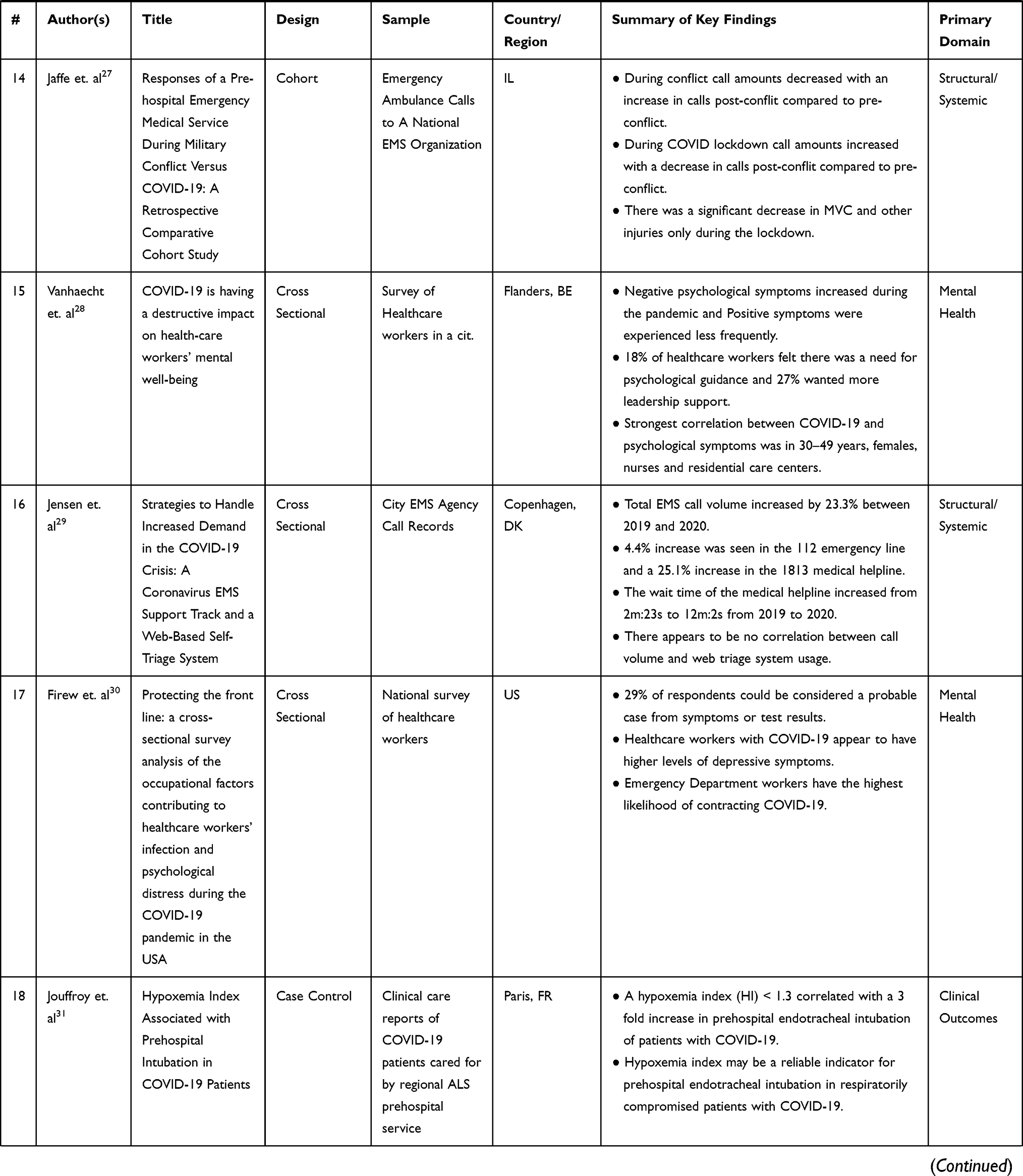 |  |  | 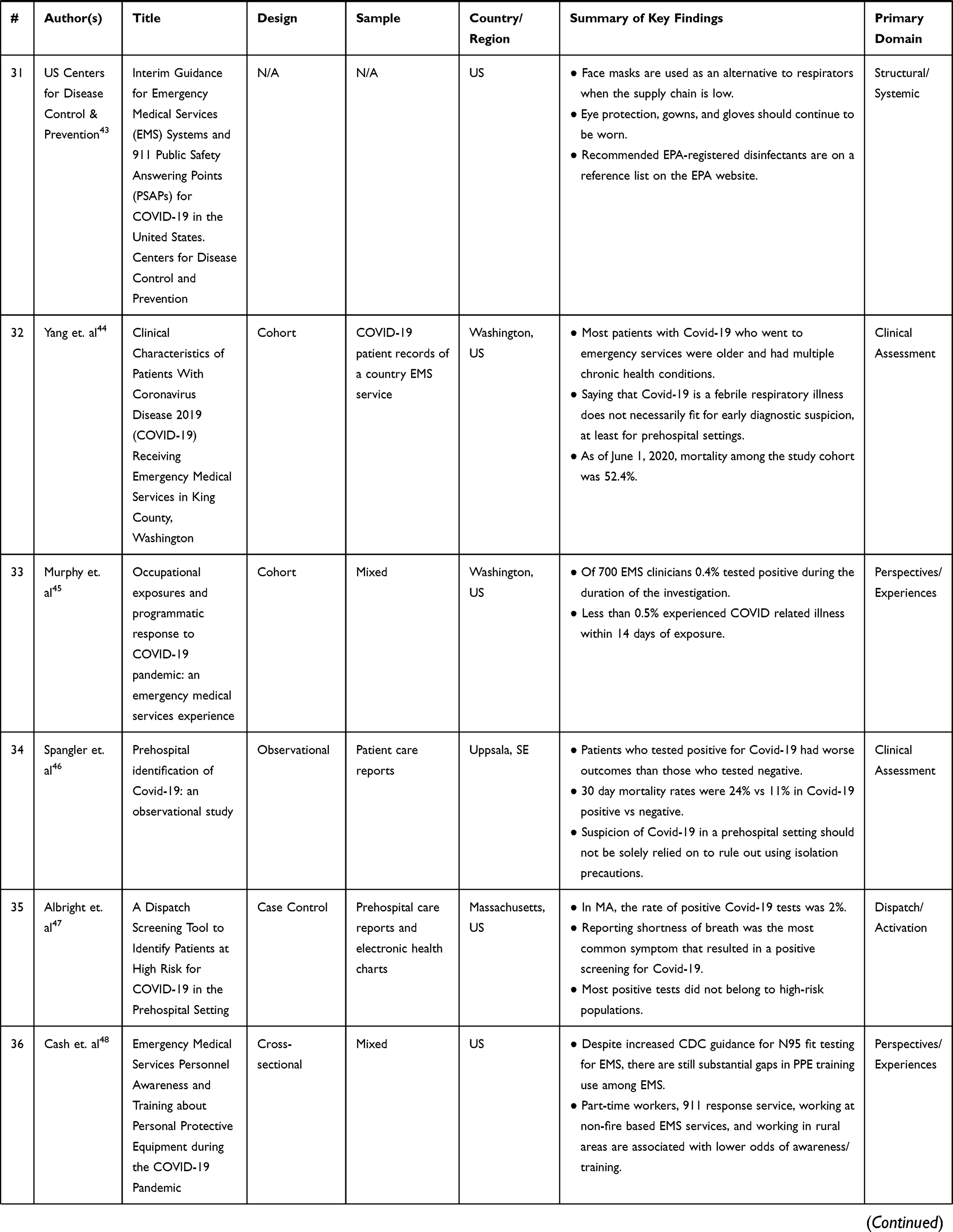 |  |  |  |  |  |  |  |  |
Table 1 Characteristics of Studies Selected for Inclusion |
 |
Figure 1 Schematic selection of relevant articles for inclusion in review. |
Of the included studies, 44% were US-based. Primary taxonomy schema revealed the following prevalence of data: n=16 structural/systemic, n=23 clinical outcomes, n=7 clinical assessment, n=4 treatment, n=3 special populations, n=2 dispatch/activation, n=6 education, n=3 mental health, n=6 perspectives/experiences, and n=7 transport (see Table 1).
Discussion
Structural Considerations
Of the studies selected for inclusion in the “structural/systemic” domain, only 25% pertained to regions within the US. Only one study at the start of the pandemic (April 2020) rigorously assessed resource capacity and clinical competency at the national level, in response to the COVID-19 pandemic. Study participants were licensed practicing EMS clinicians in all 50 US states including the District of Columbia. Ventura et al report regular dissatisfactory decontamination practices both prior to and during the pandemic, required prolonged use of N95 respirators past the recommended efficacy period, and overall inadequate education for infection control and clinical considerations for COVID-19 patients.4 Notably, this captures a vulnerable representation of the US EMS system when there was minimal consensus on COVID-19 clinical symptomatology, transmissibility, appropriate precautionary measures, and discovery of vaccines. Globally, highly populated regions in the US, Germany, Turkey, Ireland and Denmark observed an increase in emergency medical calls of varying chief complaints, with many agency and regiospecific ambulance agencies reporting call volumes exceeding 60% compared to 2019.14,16,33 Based upon analysis of 911 de-identified patient care reports from the National EMS Information System (NEMSIS), between January 2018 to December 2020, Methley et al report an increase in frequency of on-scene death (1.3% to 2.4%), cardiac arrest (1.3% to 2.2%), and opioid related emergencies (0.6% to 1.1%) at the national level.6 States such as Kentucky observed higher rates of opioid related 911 calls, with a 50% increase in suspected opioid overdose death calls, while calls for other chief complaints remained static or declined.14 This is consistent with an apparent national trend of a worsening opioid epidemic, which we hypothesize has been only exacerbated by COVID-19. In February 2022, the American Medical Association issued a statement alleging an increase in drug related deaths in all US states and territories.90 To that end, it is critical to acknowledge that recent studies suggest black and brown communities are likely to be disproportionately harmed by both the opioid epidemic and the COVID-19 pandemic, as rates of morbidity and mortality are generally higher in this clinical population.91–94 Because EMS clinicians are crucial in overdose resuscitation and sustaining life of patients experiencing opioid overdose, prehospital providers may be uniquely responsible for understanding foundational systemic issues, such as racial inequity, and how they translate to emergency clinical care, which is not currently requisite by national EMS curriculum standards despite the measurable impact of care and access disparities experienced by patients of color.95–105
Mental Health
It has been well established in the literature that the COVID-19 pandemic has correlated with worse mental health outcomes in healthcare workers (HCWs).20 The strongest correlation among COVID-19 and psychological symptoms appeared in female-identifying HCWs ages 30–49 years.28 There is a continued need for strong psychological support and further investigation into determinants of poor mental health outcomes to develop evidence driven preventive measures.
EMS Activation
911 dispatchers at public safety answering points (PSAPs) are critical to functional operations of the EMS system. Albright et al investigated the efficacy of a dispatch screening tool to identify high suspicion of COVID-19 in patients based upon a questionnaire deployed by the 911 call taker in a study based in Massachusetts. The authors report a sensitivity of 74.9% (CI, 69.21–80.03) and a specificity of 67.7% (CI, 66.91–68.50) where n=263.47 Amiry and Maguire report an exponential increase in emergency medical calls globally during the pandemic, so further investigation into ways PSAPs can best support responding clinicians using evidence based practices may be warranted.21
Clinical Assessment, Treatment, and Outcomes
In a cohort study based in King County, Washington, US, Yang et al found that EMS responded to approximately 16% of COVID-confirmed cases. From study initiation to June 2020 (four months), the study cohort mortality was 52.4%. Fever, tachypnea, and hypoxia was only present in a limited quantity of patients.44 This is consistent with international prehospital consensus that suspicion of COVID-19 based solely on symptomatology should not be solely relied on for contemplating precautionary measures and isolation procedures. In a prehospital study in Denmark, patients under 60 years old were more likely to present with a loss of taste and/or smell upon assessment, however fever and cough were equally distributed across all age groups.49 In England, Marincowitz et al studied the accuracy of prognostic triage tools used prehospitally in the Yorkshire and Humber region. The WHO algorithm, PRIEST, NEWS2, and PMEWS tools all had high sensitivity for detecting COVID-19 infection.65 In Uppsala, Sweden, Mälberg et al report correlational findings of physiological respiratory parameters with patients suspected of having COVID-19. They found that the odds of COVID-19 diagnosis increased with respiratory rate, lower tidal volume, and negative inspiratory pressure.65 In Paris, France, Jouffroy et al report that pulse oximetry may be a reliable indicator for the need of mechanical ventilation in COVID-19 patients.38 It is important to acknowledge, however, that clinically significant inaccuracy of pulse oximetry for detecting hypoxia in darker skin patients has been well established in the literature.106,107 While many methods for assessing risk of COVID-19 infection exist, a universal guidance for prehospital assessment has not been established.
As COVID-19 is categorized as a respiratory illness, the majority of available articles on prehospital treatment had a significant focus on airway and breathing management. A study out of Paris reported that of the 15% of suspected COVID-19 patients who were found to be in cardiac arrest upon arrival, while the majority did not have prior cardiovascular risk factors present. This suggests that it is critical to provide sufficient respiratory support in the prehospital setting. It was found that of the suspected COVID-19 patients who were assessed by EMS personnel, 42% of BLS cases and 52% of ALS cases provided non-invasive ventilation, however, prehospital intubation was significantly less common as it was only present in 18% of ALS cases.50, Jouffroy et al report that of all COVID−19 suspected patients, 53.4% showed signs of respiratory distress. Most of these patients presented with respiratory rates of approximately 30/min and oxygen saturations of 72%. Additionally, all patients required some method of high flow oxygen treatment.88
Studies, such as one conducted by Hart et al, provides recommendations for personal protection protocols for EMS providers. They suggest that if endotracheal intubation is needed, it should only be attempted once and with the assistance of video laryngoscopy to minimize time exposure to aerosols. A HEPA filter should then be added following the placement of an advanced airway to further minimize risk for contamination of the provider and all other equipment present in the ambulance. In the event that advanced airway intervention is not possible or clinically indicated, it is suggested to use two individuals for BVM ventilation to ensure that an air-tight seal is made with the mask. In agreement with other established protocols, they stress that donning of PPE should be performed before any contact is made with a suspected COVID-19 patient.58
As mentioned previously, there is a shortage of available resources not just pre-hospital but in-hospital as well. Considerations need to be made to ensure resources are used in the most efficient manner. Natalzia et al proposes a protocol to maximize cardiac arrest resources in EMS in which one should only initiate resuscitation of a patient in cardiac arrest if the arrest is witnessed or a shockable rhythm is present. They state that this protocol could account for 70.5% of favorable neurological outcomes and provide 6.3 additional available hospital beds per patient.89
Education
As part of their initial education program, EMS students must generally acquire co-requisite field experience.1 During the early era of the COVID-19 pandemic, it may have been difficult to participate in field experience opportunities due to facility policy limitations designed to reduce transmission. Grawey et al examined an alternative model to the traditional ambulance “ride along” by providing a field-like experience in an emergency department setting. Grawey et al report that this alternative experience was likely as effective as traditional prehospital clinical internships. Additionally, they found university medical students to have increased knowledge regarding EMS roles and responsibilities, which may have beneficial implications for transfer of care.23 With regard to continuing education, the Commission on Accreditation for Prehospital Continuing Education (CAPCE) saw a 179% increase in EMS refresher courses during 2018 to 2020, with a 185% increase in asynchronous online learning.54 This may suggest that distance learning as a method for recertifying provider credentials may increase rates of recertification, in contrast with in-person continuing education programs.
Vaccine Perspectives and Prevalence
US EMS clinicians have also assumed nontraditional healthcare roles during the COVID-19 pandemic, such as in the case of a scope of practice expansion which allowed EMS clinicians to administer the COVID-19 to patients in states like New York, Massachusetts, and Vermont. Because EMS clinicians are highly trained in specific psychomotor clinical skills and knowledgeable in fundamental methods of patient assessment and treatment, it is likely that EMS in general has served unmeasurable utility through contributions in traditional and nontraditional roles. In April 2021, Gregory et al conducted a cross sectional study of nationally certified EMS clinicians rostered with the National Registry of Emergency Medical Technicians (NREMT). Of a sample size of n=2584, 70% reported receiving a COVID-19 vaccine. Of the sampled population, 53% had concerns regarding the safety of COVID vaccines, 39% felt it was not necessary, and 84% of providers who did not receive any dose of the COVID vaccine did not plan to get it in the future.25 The significant vaccine hesitancy amongst EMS clinicians poses a compelling public health concern, and approaches to mediate this, such as through local education and role modeling, may be necessary.108
Limitations
Little literature exists on the interrogated area of investigation, and studies that are relevant to the area are often preliminary and may require continued study and design modifications to increase external validity. While all attempts to achieve a high level of internal validity were made as captured by robust quality assessments at each level of investigation, it was not possible to accommodate for every confounder. While this review is not exhaustive, the authors affirm satisfaction in the methods and results available at the time of study.
Conclusion
US EMS clinicians are healthcare workers that have often held many roles and responsibilities during the COVID-19 pandemic. Within the subset domains of i. structural/systemic, ii. clinical outcomes, iii. clinical assessment, iv. treatment, v. special populations, vi. dispatch/activation, vii. education, viii. mental health, ix. perspectives/experiences, and x. transport, there is minimal high quality literature that faithfully reflect the status of modern American EMS in response to the COVID-19 pandemic. The available data reflect strides in contemporary approaches to assessment, treatment, transport, and education, but fall short in accounting for care and access disparities influenced by social determinants. Continued investigation on the impact of COVID-19 on EMS systems and personnel is warranted to ensure informed, appropriate, and evidence-based preparation for future pandemic and infectious disease response.
Institutional Disclaimer
The work is solely that of the authors and does not necessarily represent the views, policies, or opinions of their affiliated institutions, employers, or partners. It was not reviewed or endorsed by any specific institution in particular.
Acknowledgments
The authors would like to sincerely thank Paramedic Catherine Smith, EMT Rosa Turinetti, and Judith Inumerable for their expert opinions and experiences.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The work is not funded by any specific source.
Disclosure
The investigators report no known conflicts of interest, financial or otherwise.
References
1. Pollak AN. Emergency care and transportation of the sick and injured. Jones Bartlett Learning. 2021;2021:1
2. National Association of State EMS Officials. National EMS Scope of Practice Model 2019. Washington, DC: National Highway Traffic Safety Administration;2019.
3. Ortaliza J. Covid-19 leading cause of death ranking. Peterson KFF Health Sys Track. 2022;9:15
4. Ventura C, Gibson C, Collier GD. Emergency medical services resource capacity and competency amid COVID-19 in the United States: preliminary findings from a national survey. Heliyon. 2020;6. doi:10.1016/j.heliyon.2020.e03900
5. Page MJ, McKenzie JE, Bossuyt PM, et al. Rayyan — a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210. doi:10.1186/s13643-016-0384-4
6. Methley AM, Campbell S, Chew-Graham C, et al. PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res. 2014;14(1):579. doi:10.1186/s12913-014-0579-0
7. Scottish Intercollegiate Guidelines Network. Methodology checklist 1: systematic reviews and meta-analyses. Available from: https://www.sign.ac.uk/what-we-do/methodology/checklists/.
8. Moher D, Liberati A, Tetzlaff J, Altman DG. Group Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
9. Harris JD, Quatman CE, Manring MM, Siston RA, Flanigan DC. How to write a systematic review. Am J Sports Med. 2014;42(11):2761–2768. doi:10.1177/0363546513497567
10. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
11. Quality appraisal of case series studies checklist. Edmonton (AB) institute of health economics; 2014.
12. “Critical Appraisal Checklists”. The Joanna Briggs institute critical appraisal tools for use in JBI systematic reviews; 2014.
13. Lin L, Chu H. Quantifying publication bias in meta-analysis. Biometrics. 2018;74(3):785–794. doi:10.1111/biom.12817
14. Slavova S, Rock P, Bush HM, Quesinberry D, Walsh SL. Signal of increased opioid overdose during COVID-19 from emergency medical services data. Drug Alcohol Depend. 2020;214:108176. doi:10.1016/j.drugalcdep.2020.108176
15. Tien H, Sawadsky B, Lewell M, Peddle M, Durham W. Critical care transport in the time of COVID-19. CJEM. 2020;22(S2):S84–S88. doi:10.1017/cem.2020.400
16. Dahmen J, Bäker L, Breuer F, et al. COVID-19-stresstest für die sicherstellung der notfallversorgung: strategie und Maßnahmen der notfallrettung in Berlin [COVID-19 Stress test for ensuring emergency healthcare: strategy and response of emergency medical services in Berlin]. Anaesthetist. 2021;70(5):420–431. German. doi:10.1007/s00101-020-00890-8
17. Levy MJ, Klein E, Chizmar TP, et al. Correlation between emergency medical services suspected COVID-19 patients and daily hospitalizations. Prehosp Emerg Care. 2021;25(6):785–789. doi:10.1080/10903127.2020.1864074
18. Şan İ, Usul E, Bekgöz B, Korkut S. Effects of COVID-19 pandemic on emergency medical services. Int J Clin Pract. 2021;75(5):e13885. doi:10.1111/ijcp.13885
19. Handberry M, Bull-Otterson L, Dai M, et al. Changes in emergency medical services before and during the COVID-19 pandemic in the United States. Clin Infect Dis. 2021;73(Suppl 1):S84–S91. doi:10.1093/cid/ciab373
20. Soto-Cámara R, García-Santa-Basilia N, Onrubia-Baticón H, et al. Psychological impact of the COVID-19 pandemic on out-of-hospital health professionals: a living systematic review. J Clin Med. 2021;10(23):5578. doi:10.3390/jcm10235578
21. Amiry A A, Maguire BJ. Emergency Medical Services (EMS) calls during COVID-19: early lessons learned for systems planning (A narrative review). Open Access Emerg Med. 2021;13:407–414. doi:10.2147/OAEM.S324568
22. Satty T, Ramgopal S, Elmer J, Mosesso VN, Martin-Gill C. EMS responses and non-transports during the COVID-19 pandemic. Am J Emerg Med. 2021;42:1–8. doi:10.1016/j.ajem.2020.12.078
23. Grawey T, Hinze J, Weston B. ED EMS time: a COVID-friendly alternative to ambulance ride-alongs. AEM Educ Train. 2021;5(4):e10689. doi:10.1002/aet2.10689
24. Fernandez AR, Crowe RP, Bourn S, et al. COVID-19 preliminary case series: characteristics of EMS encounters with linked hospital diagnoses. Prehosp Emerg Care. 2021;25(1):16–27. doi:10.1080/10903127.2020.1792016
25. Gregory ME, Powell JR, MacEwan SR, et al. COVID-19 vaccinations in EMS professionals: prevalence and predictors. Prehosp Emerg Care. 2021:1–9. doi:10.1080/10903127.2021.1993391
26. Eftekhar Ardebili M, Naserbakht M, Bernstein C, Alazmani-Noodeh F, Hakimi H, Ranjbar H. Healthcare providers experience of working during the COVID-19 pandemic: a qualitative study. Am J Infect Control. 2021;49(5):547–554. doi:10.1016/j.ajic.2020.10.001
27. Jaffe E, Sonkin R, Alpert EA, Zerath E. Responses of a pre-hospital emergency medical service during military conflict versus COVID-19: a retrospective comparative cohort study. Mil Med. 2021;usab437. doi:10.1093/milmed/usab437
28. Vanhaecht K, Seys D, Bruyneel L, et al. COVID-19 is having a destructive impact on health-care workers’ mental well-being. Int J Qual Health Care. 2021;33(1):mzaa158. doi:10.1093/intqhc/mzaa158
29. Jensen T, Holgersen MG, Jespersen MS, et al. Strategies to handle increased demand in the COVID-19 crisis: a coronavirus EMS support track and a web-based self-triage system. Prehosp Emerg Care. 2021;25(1):28–38. doi:10.1080/10903127.2020.1817212
30. Firew T, Sano ED, Lee JW, et al. Protecting the front line: a cross-sectional survey analysis of the occupational factors contributing to healthcare workers’ infection and psychological distress during the COVID-19 pandemic in the USA. BMJ Open. 2020;10(10):e042752. doi:10.1136/bmjopen-2020-042752
31. Jouffroy R, Kedzierewicz R, Derkenne C, et al. Hypoxemia index associated with prehospital intubation in COVID-19 patients. J Clin Med. 2020;9(9):3025. doi:10.3390/jcm9093025
32. Tabah A, Ramanan M, Laupland KB, et al. Personal protective equipment and intensive care unit healthcare worker safety in the COVID-19 era (PPE-SAFE): an international survey. J Crit Care. 2021;63:280–281. doi:10.1016/j.jcrc.2020.06.005
33. Prezant DJ, Lancet EA, Zeig-Owens R, et al. System impacts of the COVID-19 pandemic on New York City’s emergency medical services. J Am Coll Emerg Physicians Open. 2020;1(6):1205–1213. doi:10.1002/emp2.12301
34. Berry CL, Corsetti MC, Mencl F. Helicopter emergency medical services transport of COVID-19 patients in the “first wave”: a National survey. Cureus. 2021;13(8):e16961. doi:10.7759/cureus.16961
35. Xie Y, Kulpanowski D, Ong J, Nikolova E, Tran NM. Predicting Covid-19 emergency medical service incidents from daily hospitalisation trends. Int J Clin Pract. 2021;75(12):e14920. doi:10.1111/ijcp.14920
36. Maqueda Gonzalez R, Cerdán Santacruz C, García Septiem J, et al. Proctologic emergency consultation during COVID-19: comparative cross-sectional cohort study. Cir Esp. 2021;99(9):660–665. doi:10.1016/j.cireng.2021.10.003
37. Greenhalgh M, Dupley L, Unsworth R, Boden R. Where did all the trauma go? A rapid review of the demands on orthopaedic services at a UK Major Trauma Centre during the COVID-19 pandemic. Int J Clin Pract. 2021;75(3):e13690. doi:10.1111/ijcp.13690
38. Bourn SS, Crowe RP, Fernandez AR, et al. Initial prehospital Rapid Emergency Medicine Score (REMS) to predict outcomes for COVID-19 patients. J Am Coll Emerg Physicians Open. 2021;2(4):e12483. doi:10.1002/emp2.12483
39. Nishikimi M, Rasul R, Sison CP, et al. Intubated COVID-19 predictive (ICOP) score for early mortality after intubation in patients with COVID-19. Sci Rep. 2021;11(1):21124. doi:10.1038/s41598-021-00591-1
40. Feng J, Yang Y, Zheng X, et al. Impact of COVID-19 on emergency patients in the resuscitation room: a cross-sectional study. J Clin Lab Anal. 2022;36(3):e24264. doi:10.1002/jcla.24264
41. Garcia-Castrillo L, Petrino R, Leach R, et al. European society for emergency medicine position paper on emergency medical systems’ response to COVID-19. Eur J Emerg Med. 2020;27(3):174–177. doi:10.1097/MEJ.0000000000000701
42. Albrecht R, Knapp J, Theiler L, Eder M, Pietsch U. Transport of COVID-19 and other highly contagious patients by helicopter and fixed-wing air ambulance: a narrative review and experience of the Swiss air rescue Rega. Scand J Trauma Resusc Emerg Med. 2020;28(1):40. doi:10.1186/s13049-020-00734-9
43. US Centers for Disease Control and Prevention. Interim guidance for Emergency Medical Services (EMS) systems and 911 public safety answering points (PSAPs) for COVID-19 in the United States; 2020.
44. Yang BY, Barnard LM, Emert JM, et al. Clinical characteristics of patients with coronavirus disease 2019 (COVID-19) receiving emergency medical services in King County, Washington. JAMA Netw Open. 2020;3(7):e2014549. doi:10.1001/jamanetworkopen.2020.14549
45. Murphy DL, Barnard LM, Drucker CJ, et al. Occupational exposures and programmatic response to COVID-19 pandemic: an emergency medical services experience. Emerg Med J. 2020;37(11):707–713. doi:10.1136/emermed-2020-210095
46. Spangler D, Blomberg H, Smekal D. Prehospital identification of Covid-19: an observational study. Scand J Trauma Resusc Emerg Med. 2021;29(1):3. doi:10.1186/s13049-020-00826-6
47. Albright A, Gross K, Hunter M, O’Connor L. A dispatch screening tool to identify patients at high risk for COVID-19 in the prehospital setting. West J Emerg Med. 2021;22(6):1253–1256. doi:10.5811/westjem.2021.8.52563
48. Cash RE, Rivard MK, Camargo CA Jr, Powell JR, Panchal AR. Emergency medical services personnel awareness and training about personal protective equipment during the COVID-19 pandemic. Prehosp Emerg Care. 2021;25(6):777–784. doi:10.1080/10903127.2020.1853858
49. Moeller AL, Mills EHA, Collatz Christensen H, et al. Symptom presentation of SARS-CoV-2-positive and negative patients: a nested case-control study among patients calling the emergency medical service and medical helpline. BMJ Open. 2021;11(5):e044208. doi:10.1136/bmjopen-2020-044208
50. Jouffroy R, Lemoine S, Derkenne C, et al. Prehospital management of acute respiratory distress in suspected COVID-19 patients. Am J Emerg Med. 2021;45:410–414. doi:10.1016/j.ajem.2020.09.022
51. Shekhar AC, Effiong A, Ruskin KJ, Blumen I, Mann NC, Narula J. COVID-19 and the prehospital incidence of acute cardiovascular events (from the Nationwide US EMS). Am J Cardiol. 2020;134:152–153. doi:10.1016/j.amjcard.2020.08.003
52. Glenn MJ, Rice AD, Primeau K, et al. Refusals after prehospital administration of naloxone during the COVID-19 pandemic. Prehosp Emerg Care. 2021;25(1):46–54. doi:10.1080/10903127.2020.1834656
53. Jarvis S, Salottolo K, Berg GM, et al. Examining emergency medical services’ prehospital transport times for trauma patients during COVID-19. Am J Emerg Med. 2021;44:33–37. doi:10.1016/j.ajem.2021.01.091
54. March JA, Scott J, Camarillo N, Bailey S, Holley JE, Taylor SE. Effects of COVID-19 on EMS refresher course completion and delivery. Prehosp Emerg Care. 2021;1–6. doi:10.1080/10903127.2021.1977876
55. Saberian P, Conovaloff JL, Vahidi E, Hasani-Sharamin P, Kolivand PH. How the COVID-19 epidemic affected prehospital emergency medical services in Tehran, Iran. West J Emerg Med. 2020;21(6):110–116. doi:10.5811/westjem.2020.8.48679
56. Oulasvirta J, Pirneskoski J, Harve-Rytsälä H, et al. Paediatric prehospital emergencies and restrictions during the COVID-19 pandemic: a population-based study. BMJ Paediatr Open. 2020;4(1):e000808. doi:10.1136/bmjpo-2020-000808
57. Hadley ME, Vaught AJ, Margolis AM, et al. 911 EMS activations by pregnant patients in Maryland (USA) during the COVID-19 pandemic. Prehosp Disaster Med. 2021;36(5):570–575. doi:10.1017/S1049023X21000728
58. Hart J, Tracy R, Johnston M, et al. Recommendations for prehospital airway management in patients with suspected COVID-19 infection. West J Emerg Med. 2020;21(4):809–812. doi:10.5811/westjem.2020.5.47540
59. Mohammadi F, Tehranineshat B, Bijani M, Khaleghi AA. Management of COVID-19-related challenges faced by EMS personnel: a qualitative study. BMC Emerg Med. 2021;21(1):95. doi:10.1186/s12873-021-00489-1
60. Lancet EA, Gonzalez D, Alexandrou NA, et al. Prehospital hypoxemia, measured by pulse oximetry, predicts hospital outcomes during the New York City COVID-19 pandemic. J Am Coll Emerg Physicians Open. 2021;2(2):e12407. doi:10.1002/emp2.12407
61. Powell M, Ward B, Dickson R, Patrick C. Prehospital sinus node dysfunction and asystole in a previously healthy patient with COVID-19. Prehosp Emerg Care. 2021;1–5. doi:10.1080/10903127.2021.1924325
62. Velasco C, Wattai B, Buchle S, et al. Impact of COVID-19 pandemic on the incidence, prehospital evaluation, and presentation of ischemic stroke at a nonurban comprehensive stroke center. Stroke Res Treat. 2021;2021:6624231. doi:10.1155/2021/6624231
63. Solà-Muñoz S, Yuguero O, Azeli Y, et al. Impact on polytrauma patient prehospital care during the first wave of the COVID-19 pandemic: a cross-sectional study. Eur J Trauma Emerg Surg. 2021;47(5):1351–1358. doi:10.1007/s00068-021-01748-3
64. Siman-Tov M, Strugo R, Podolsky T, Blushtein O. An assessment of treatment, transport, and refusal incidence in a national EMS’s routine work during COVID-19. Am J Emerg Med. 2021;44:45–49. doi:10.1016/j.ajem.2021.01.051
65. Marincowitz C, Sutton L, Stone T, et al. Prognostic accuracy of triage tools for adults with suspected COVID-19 in a prehospital setting: an observational cohort study. Emerg Med J. 2022. doi:10.1136/emermed-2021-211934
66. Ong J, Pourmand A, O’Connell F. An international perspective of out-of-hospital cardiac arrest and cardiopulmonary resuscitation during the COVID-19 pandemic. Am J Emerg Med. 2021;48:340–341. doi:10.1016/j.ajem.2021.06.001
67. Yu J-H, Liu C-Y, Chen W-K, et al. Impact of the COVID-19 pandemic on Emergency Medical Service response to out-of-hospital cardiac arrests in Taiwan: a retrospective observational study. Emerg Med J. 2021;38(9):679–684. doi:10.1136/emermed-2020-210409
68. Azbel M, Heinänen M, Lääperi M, Kuisma M. Effects of the covid-19 pandemic on trauma-related Emergency Medical Service Calls: a retrospective cohort study. BMC Emerg Med. 2021;21(1). doi:10.1186/s12873-021-00495-3
69. Seo AR, Lee WJ, Woo SH, Moon J, Kim D. Pre-hospital delay in patients with acute stroke during the initial phase of the Coronavirus Disease 2019 outbreak. J Korean Med Sci. 2022;37(6). doi:10.3346/jkms.2022.37.e47
70. Mälberg J, Hadziosmanovic N, Smekal D. Physiological respiratory parameters in pre-hospital patients with suspected COVID-19: a prospective cohort study. PLoS One. 2021;16(9):e0257018. doi:10.1371/journal.pone.0257018
71. Ng QX, Lee EZH, Tay JAM, Arulanandam S. Impact of covid ‐19 ‘circuit‐breaker’ measures on Emergency Medical Services Utilisation and out‐of‐hospital cardiac arrest outcomes in Singapore. Emerg Med Australas. 2020;33(1):149–151. doi:10.1111/1742-6723.13668
72. Cash RE, Leggio WJ, Powell JR, et al. Emergency medical services education research priorities during COVID‐19: a modified delphi study. J Am Coll Emerg Physicians Open. 2021;2(4). doi:10.1002/emp2.12543
73. Borkowska MJ, Smereka J, Safiejko K, et al. Out-of-hospital cardiac arrest treated by emergency medical service teams during COVID-19 pandemic: a retrospective cohort study. Cardiol J. 2021;28(1):15–22. doi:10.5603/cj.a2020.0135
74. Kalani N, Hatami N, Ali S, et al. Self-Referred Walk-in (SRW) versus emergency medical services brought Covid-19 patients. Bull Emerg Trauma. 2022;10(1):21–26. doi:10.30476/BEAT.2021.92229.1299
75. Talikowska M, Ball S, Tohira H, et al. No apparent effect of the COVID-19 pandemic on out-of-hospital cardiac arrest incidence and outcome in Western Australia. Resusc Plus. 2021;8:100183. doi:10.1016/j.resplu.2021.100183
76. Saberian P, Falahi S, Baratloo A, et al. Changes in COVID-19 IgM and IgG antibodies in emergency medical technicians (EMTs). Am J Emerg Med. 2022;52:59–63. doi:10.1016/j.ajem.2021.11.019
77. Ageta K, Naito H, Yorifuji T, et al. Delay in emergency medical service transportation responsiveness during the COVID-19 pandemic in a minimally affected region. Acta Med Okayama. 2020;74(6):513–520. doi:10.18926/AMO/61210
78. Hunt N, Masiewicz S, Herbert L, et al. Novel negative pressure helmet reduces aerosolized particles in a simulated prehospital setting. Prehosp Disaster Med. 2022;37(1):33–38. doi:10.1017/S1049023X22000103
79. Tanaka S, Nakagawa K, Ozone Y, et al. Evaluation of the physiological changes in prehospital health-care providers influenced by environmental factors in the summer of 2020 during the COVID-19 pandemic. Acute Med Surg. 2021;8(1):e699. doi:10.1002/ams2.699
80. Melgoza E, Beltrán-Sánchez H, Bustamante AV. Emergency medical service use among latinos aged 50 and older in California counties, except los angeles, during the early COVID-19 pandemic period. Front Public Health. 2021;9:660289. doi:10.3389/fpubh.2021.660289
81. Goldberg SA, Bonacci RA, Carlson LC, Pu CT, Ritchie CS. Home-based testing for SARS-CoV-2: leveraging prehospital resources for vulnerable populations. West J Emerg Med. 2020;21(4):813–816. doi:10.5811/westjem.2020.5.47769
82. Saberian P, Rafiemanesh H, Sadeghi M, Hasani-Sharamin P, Dadashi F, Baratloo A. The geographical distribution of probable COVID-19 patients transferred by Tehran emergency medical services; a cross sectional study. Arch Acad Emerg Med. 2021;9(1):e25. doi:10.22037/aaem.v9i1.1177
83. Tušer I, Bekešienė S, Navrátil J. Emergency management and internal audit of emergency preparedness of pre-hospital emergency care. Qual Quant. 2020;1–13. doi:10.1007/s11135-020-01039-w
84. Masuda Y, Teoh SE, Yeo JW, et al. Variation in community and ambulance care processes for out-of-hospital cardiac arrest during the COVID-19 pandemic: a systematic review and meta-analysis. Sci Rep. 2022;12(1):800. doi:10.1038/s41598-021-04749-9
85. Hasani-Sharamin P, Saberian P, Sadeghi M, Mireskandari SM, Baratloo A. Characteristics of emergency medical service missions in out-of-hospital cardiac arrest and death cases in the periods of before and after the COVID-19 pandemic. Prehosp Disaster Med. 2021;36(6):676–683. doi:10.1017/S1049023X21001138
86. Jaffe E, Sonkin R, Podolsky T, Alpert EA, Siman-Tov M. The role of Israel’s emergency medical services during a pandemic in the pre-exposure period. Disaster Med Public Health Prep. 2020;1–5. doi:10.1017/dmp.2020.369
87. Masterson S, Heffernan E, Keegan D, et al. Rapid response and learning for later: establishing high quality information networks and evaluation frameworks for the National Ambulance Service response to COVID-19 - The ENCORE COVID Project Protocol. HRB Open Res. 2021;3:68. doi:10.12688/hrbopenres.13149.2
88. Le Borgne P, Oberlin M, Bassand A, et al. Pre-hospital management of critically Ill patients with SARS-CoV-2 infection: a retrospective multicenter study. J Clin Med. 2020;9(11):3744. doi:10.3390/jcm9113744
89. Natalzia P, Murk W, Thompson JJ, et al. Evidence-based crisis standards of care for out-of-hospital cardiac arrests in a pandemic. Resuscitation. 2020;156:149–156. doi:10.1016/j.resuscitation.2020.07.021
90. AMA overdose epidemic report. Available from: Ama-Assn.org.https://www.ama-assn.org/system/files/ama-overdose-epidemic-report.pdf.
91. Patel I, Walter LA, Li L. Opioid overdose crises during the COVID-19 pandemic: implication of health disparities. Harm Reduct J. 2021;18(1). doi:10.1186/s12954-021-00534-z
92. Price-Haywood EG, Burton J, Fort D, Seoane L. Hospitalization and mortality among black patients and white patients with Covid-19. N Engl J Med. 2020;382(26):2534–2543. doi:10.1056/NEJMsa2011686
93. Millett GA, Jones AT, Benkeser D, et al. Assessing differential impacts of COVID-19 on black communities. Ann Epidemiol. 2020;47:37–44. doi:10.1016/j.annepidem.2020.05.003
94. Abuelgasim E, Saw LJ, Shirke M, Zeinah M, Harky A. COVID-19: unique public health issues facing Black, Asian and minority ethnic communities. Curr Probl Cardiol. 2020;45(8):100621. doi:10.1016/j.cpcardiol.2020.100621
95. Ventura C. The Emergency Medical Responder: training and Succeeding as an EMT/EMR. Springer; 2021.
96. Paradies Y. A systematic review of empirical research on self-reported racism and health. Int J Epidemiol. 2006;35(4):888–901. doi:10.1093/ije/dyl056external
97. Simons RL, Lei MK, Beach SRH, et al. Discrimination, segregation, and chronic inflammation: testing the weathering explanation for the poor health of Black Americans. Dev Psychol. 2018;54(10):1993–2006. doi:10.1037/dev0000511external
98. Berchick ER, Barnett JC, Rachel D Upton current population reports, P60–267 (RV), health insurance coverage in the United States: 2018, U.S. Washington, DC: Government Printing Office; 2019.
99. Care Without Coverage: Too Little, Too Late. Institute of medicine (US) committee on the consequences of uninsurance. Washington (DC): National Academies Press (US); 2002.
100. Institute of Medicine. Unequal treatment: confronting racial and ethnic disparities in health care. Washington, DC: The National Academies Press; 2003.
101. U.S. National Library of Medicine. Native Voices: timeline: government admits forced sterilization of Indian Women. 2011 [cited 2020 Jun 24]. Available from: https://www.nlm.nih.gov/nativevoices/timeline/543.htmlexternalicon.
102. Novak NL, Lira N, O’Connor KE, Harlow SD, Kardia SLR, Stern AM. Disproportionate sterilization of latinos under California’s eugenic sterilization program, 1920–1945. Am J Public Health. 2018;108(5):611–613. doi:10.2105/AJPH.2018.304369
103. Stern AM. Sterilized in the name of public health: race, immigration, and reproductive control in modern California. Am J Public Health. 2005;95(7):1128–1138. doi:10.2105/AJPH.2004.041608
104. Prather C, Fuller TR, Jeffries WL, et al. Racism, African American Women, and their sexual and reproductive health: a review of historical and contemporary evidence and implications for health equity. Health Equity. 2018;2(1):249–259. doi:10.1089/heq.2017.0045
105. U.S. Department of Health and Human Services. Social Determinants of Health; 2020.
106. Bickler PE, Feiner JR, Severinghaus JW. Effects of skin pigmentation on pulse oximeter accuracy at low saturation. Anesthesiology. 2005;102(4):715–719. doi:10.1097/00000542-200504000-00004
107. Feiner JR, Severinghaus JW, Bickler PE. Dark skin decreases the accuracy of pulse oximeters at low oxygen saturation: the effects of oximeter probe type and gender. Anesth Analg. 2007;105(6 Suppl):S18–S23. doi:10.1213/01.ane.0000285988.35174.d9
108. Troiano G, Nardi A. Vaccine hesitancy in the era of COVID-19. Public Health. 2021;194:245–251. doi:10.1016/j.puhe.2021.02.025
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Impact of the Coronavirus Disease 2019 (Covid-19) Pandemic on the Use of Emergency Medical Services System in Bangkok, Thailand
Huabbangyang T, Trakulsrichai S, Yuksen C, Sricharoen P
Open Access Emergency Medicine 2022, 14:429-440
Published Date: 4 August 2022
Artificial Intelligence Chatbots and Emergency Medical Services: Perspectives on the Implications of Generative AI in Prehospital Care
Ventura CAI, Denton EE
Open Access Emergency Medicine 2023, 15:289-292
Published Date: 7 September 2023