Back to Journals » Open Access Emergency Medicine » Volume 14
Emergency Decompression of Obstructive Uropathy Using Percutaneous Nephrostomy: Disease Pattern and Treatment Outcome at Two Urology Centers in Ethiopia
Authors Gebreselassie KH ![]() , Gebrehiwot FG
, Gebrehiwot FG ![]() , Hailu HE
, Hailu HE ![]() , Beyene AD
, Beyene AD ![]() , Hassen SM, Mummed FO
, Hassen SM, Mummed FO ![]() , Issack FH
, Issack FH ![]()
Received 16 October 2021
Accepted for publication 21 December 2021
Published 11 January 2022 Volume 2022:14 Pages 15—24
DOI https://doi.org/10.2147/OAEM.S344744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Kaleab Habtemichael Gebreselassie,1 Fitsum Gebreegziabher Gebrehiwot,1 Haimanot Ewnetu Hailu,2 Andualem Deneke Beyene,3 Seid Mohammed Hassen,1 Ferid Ousman Mummed,1 Feysel Hassen Issack1
1Urology Unit, Department of Surgery, Saint Paul’s Hospital Millennium Medical College (SPHMMC), Addis Ababa, Ethiopia; 2Department of Public Health, Saint Paul’s Hospital Millennium Medical College (SPHMMC), Addis Ababa, Ethiopia; 3Department of Surgery, School of Medicine, College of Health Sciences, Addis Ababa University (AAU), Addis Ababa, Ethiopia
Correspondence: Kaleab Habtemichael Gebreselassie
Department of Surgery, Urology Unit, St. Paul’s Hospital Millennium Medical College, PO Box: 59004, Addis Ababa, Ethiopia
Tel +251-913632425
Email [email protected]
Purpose: Obstructive uropathy (OU) is a potentially life-threatening urologic emergency that requires urgent decompression. Percutaneous nephrostomy (PCN) is a commonly performed procedure to decompress OU. The objective of this study is to assess disease patterns and treatment outcome at two urologic centers in Ethiopia.
Methods: A cross-sectional study was conducted on 110 patients who underwent emergency PCN from October 1, 2019 to September 30, 2020. Data were collected by a retrospective chart review. SPSS 25 was used for analysis. Descriptive statistics and logistic regression were utilized to assess disease pattern and significant predictors. A p-value of < 0.05 on multivariate logistic regression was considered statistically significant.
Results: Females accounted for 70% of cases and mean age at presentation was 48 ± 12.9 years. Bilateral OU was diagnosed in 60% of patients and 77.3% of obstructions occurred at the level of the ureter. Malignancies were diagnosed in > 80% of patients among which cervical cancer was the commonest (37.3%) followed by bladder cancer (17.3%). Acute kidney injury (AKI) accounted for 70% of the presenting indications for PCN. Success rate after emergency PCN was 75.5% and 41.8% of the cases developed post-procedure complications. Factors that predicted successful outcome include male gender [AOR = 5.72 (1.13– 28.92), 95% CI; p = 0.035], severe hydronephrosis pre-operatively [AOR = 7.12 (1.32– 38.45), 95% CI; p = 0.022], and use of combined imaging (ultrasound and fluoroscope) to guide PCN [AOR = 12.91 (1.13– 46.54), 95% CI; p = 0.039]. On the other hand, postoperative complication is a negative predictor [AOR = 0.26 (0.08– 0.86), 95% CI; p = 0.027].
Conclusion: In this study, overall success of emergency PCN is low. Presence of severe hydronephrosis predicts technical ease and better outcome of PCN. Procedures performed under ultrasound and fluoroscope guidance also improve outcome. Postoperative complication rate is high in this study and mandates strict preventive measures as it predicts unfavorable outcome.
Keywords: obstructive uropathy, percutaneous nephrostomy, emergency decompression, Ethiopia
Introduction
Obstructive uropathy (OU) is a restriction in normal downstream urine flow because of either benign or malignant urinary tract obstruction leading to hydronephrosis and progressive renal damage. According to European Association of Urology (EAU) treatment guideline, OU is a potentially life-threatening condition that can lead to sepsis and/or acute kidney injury (AKI) and requires an emergency decompression by either retrograde placement of ureteric stents or percutaneous insertion of a nephrostomy tube into the obstructed pelvicalyceal system.1–3
The condition is a common public health problem accounting for nearly 10% of all chronic kidney disease (CKD) cases in the general population and urgent treatment is the primary preventive mechanism. The epidemiological data regarding the pattern and distribution as well as treatment outcome of OU in the general population are primarily from emergency treatment centers where the disease is commonly encountered. Both males and females of all age groups potentially can develop OU but there is an increased prevalence at 40–50 years of age.1,4,5
Urinary obstruction can occur at any anatomic level of the urinary tract (from the kidneys down to the urethral meatus) due to intrinsic or external pathologies. The distal part of ureter is the most commonly obstructed segment due to pathologies arising from the ureter itself or nearby pelvic structures such as bladder and ovaries. Many studies indicate that more than 70% of OU cases in adults are caused by benign and malignant pelvic pathologies in both men and women. On the other hand, children with OU commonly have congenital urinary tract pathology.1,3,6,7
The clinical presentation of OU in the emergency department can be quite variable depending on the location, degree, and chronicity of the obstruction. Flank pain is the most common presenting symptom in patients with acute OU and many of them also present with a variety of infectious and metabolic disturbances that require urgent attention and management.2,3,8,9
PCN is a procedure of establishing a drainage tract by puncturing the kidney directly through the skin commonly under the guidance of an imaging modality such as an ultrasound and/or fluoroscope. It can also be used as an access tract for diagnostic and therapeutic urologic procedures. Currently, PCN is commonly performed by on-call urologists and urology residents. However, interventional radiologists also have a role in some centers. The procedure was first described by Goodwin in 1955 and has since become a routine emergency urologic procedure. It has the advantages of being rapid, can be performed as an outpatient procedure with minimal anesthesia/analgesia, and has few complications.4,10–12
According to various Western and Asian studies, urgent PCN has significantly reduced the morbidity and mortality associated with OU and has satisfactory clinical outcomes. Multiple factors have been reported to affect the outcome of OU decompression using PCN, such as the presence of marked hydronephrosis, low body mass index (BMI), and the use of ultrasound guidance to perform the procedure.13–15
In Ethiopia, multi-center studies are scarce. There is no published study to date from urologic or emergency surgical care centers in the country regarding the pattern of OU and clinical outcome of its emergency decompression using PCN. In economically advanced nations, newer techniques of the procedure are also being introduced after assessing the limitations and procedure-related complications associated with ultrasound or fluoroscopy-guided PCN.
For instance, some studies from developed countries are currently advocating CT scan-guided emergency PCN in order to maximize a favorable clinical outcome.16,17 Such a recommendation towards a change in the usual trend of the procedure requires an initial baseline study like ours before its application in a resource-limited third world country like Ethiopia .
The focus of our study is to determine the pattern of OU occurrence in terms of socio-demographic distribution, etiology, clinical presentation, as well as the clinical outcome and associated factors of emergency treatment by PCN in the two largest urologic centers of the country.
Materials and Methods
Study Setting
The study was conducted at Tikur Anbessa Specialized Hospital (TASH) and St. Paul’s Hospital Millennium Medical College (SPHMMC), which have the two largest urologic centers in the country. In both institutions, Emergency Medicine and Critical Care (EMCC) physicians initially evaluate all emergency cases, including patients with OU. The diagnosis of OU was made in consultation with the urologist/urology resident on call based on clinical evaluation, laboratory work-up and imaging studies with abdominal ultrasonography and/or computed tomography. After stabilization of their general condition, the patients are transferred to the respective urology minor procedure rooms for emergency decompression by either PCN or stenting. Patients with non-malignant obstruction often undergo PCN on the affected side if an initial trial of retrograde stenting is failed. On the other hand, malignant obstructions are managed by direct decompression by PCN. In both institutions, the procedure is often performed under local anesthesia in the minor procedure rooms.
Study Design and Participants
A facility-based cross-sectional study was conducted at TASH and SPHMMC by reviewing medical charts of patients with OU who underwent emergency decompression by PCN tube insertion from October 1, 2019 to September 30, 2020 GC. The exclusion criteria were incomplete data on the medical charts and OU patients aged <14 years at the time of the procedure. Chart numbers of all OU patients who underwent PCN in the specified period were collected from the urologic operation registry logbook and then each chart was retrieved from the archive rooms of both hospitals. Accordingly, 145 patients were diagnosed with OU and underwent PCN at the two urologic centers. Among these, 35 charts were excluded from the study based on the exclusion criteria specified. Finally, data from 110 patient charts were included in this study (TASH = 87 charts and SPHMMC = 23 charts).
Data Collection Tool and Procedure
A data collection checklist was prepared to extract the necessary information from patient charts. Two trained general practitioners were involved in the data collection process at both hospitals. The eligibility of each chart was checked before the data collection process started. Each data collection checklist was coded and had 5 parts: socio-demography, clinical presentation, surgical procedure, procedure-related complication, and clinical outcome. Information regarding patient symptoms at presentation, baseline laboratory values, cause of OU, anatomic location of the obstruction, degree of hydronephrosis, anesthesia type used for the procedure, intraoperative complications, post-procedure laboratory values, and post-PCN complications were extracted using the checklist.
Surgical Procedure
All patients underwent emergency PCN using the Seldinger technique. In this technique, the patient is put in either lateral decubitus or prone position and the flank area is cleansed and draped with sterile towels. A general, regional or local anesthesia can be utilized for this procedure. In most cases, 10 mL of 2% lignocaine solution is administered to the skin, subcutaneous tissue and facial layers of the flank area. An ultrasound scan of the obstructed kidney is performed before the procedure to decide on the line of puncture and entry into the kidney. In both hospitals, a Siemens ACUSON NX2 machine with a 3.5 MHz transducer is used. The site of puncture is posterior to the ipsilateral posterior axillary line and below the lower border of the 11th or 12th ribs. The lower posterior calyx is preferred for puncture using an 18 gauge trocar needle. The procedure is guided by an imaging modality such as ultrasound, fluoroscope, or both. PCNs performed at SPHMMC utilized both ultrasound (to guide the puncture) and fluoroscope machine (to insert guide wire and assist antegrade stenting if needed). Correct entry into the kidney is confirmed when urine flow through the sheath is witnessed, after which the needle is removed keeping the trocar in place. A 0.038-inch guide wire is inserted followed by serial dilatation of the tract over the guide wire using plastic dilators. Finally, an 8–12 Fr nephrostomy tube is advanced over the guide wire and procedure is concluded by stitching the tube to the skin using non-absorbable sutures.
Definitions and Outcome Measurements
Patient outcome was dichotomized into successful and unsuccessful categories and was assessed in terms of procedural success (ie proper placement of the PCN tube) as well as improvement in the baseline clinical indications. These clinical indications for emergency PCN are elevated serum Cr level, flank pain and leukocytosis. In this regard, a successful outcome is defined as a correct insertion of PCN tube (evidenced by drainage of urine through the PCN tube) followed by improvement in the clinical indications (ie reduction in serum Cr level by at least 15% from the baseline value, subjective improvement in flank pain severity or normalization of leukocytosis to WBC <10,000 cells/mm3). Clinical improvement is defined based on patient follow-up data (physician notes and laboratory results) documented in the charts after the procedure.
Data Processing and Analysis
Data were entered into Epi Info 7 and cleaned. They were then exported into and analyzed using Statistical Package for Social Sciences (SPSS) version 25. Continuous variables were expressed using measures of central tendency and variability. Binary logistic regression was used to analyze the outcome variable. Determinant factors with a p <0.25 on bivariate analysis were transferred to multivariate analysis and an odds ratio (OR) with 95% confidence interval (CI) was used to measure the strength of association. A cut-off value of p <0.05 was used to determine the level of statistical significance.
Ethical Consideration
To maintain anonymity, specific patient identifiers like names and phone numbers were omitted from the checklist. Ethical clearance letters with reference numbers of PM/23/490 and 862/2020 were obtained from the respective institutional review boards (IRBs) of SPHMMC and TASH. The study was conducted in compliance with the standards of the Declaration of Helsinki and informed consent was not taken from patients as the study used secondary data from medical charts and was maintained with confidentiality.
Results
Socio-Demographic Characteristics
A total of 110 OU patients underwent emergency PCN and females accounted for 70%. The male to female ratio was 1: 2.3. The mean age (± SD) at the time of operation was 48 ± 12.9 years and more than half of the patients fell under the age range of 41–60 years (Figure 1). Regarding living address of the operated patients, 62 (56.4%) of them came from the capital city.
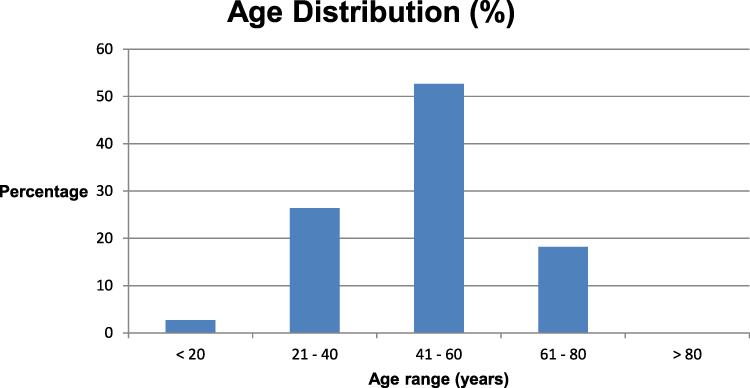 |
Figure 1 Distribution of patients with obstructive uropathy by age. |
Baseline Clinical Characteristics
Majority of patients had a bilateral OU (60%) and most of the obstructions occurred at the level of the ureter (77.3%). Malignant diseases were diagnosed in majority of the operated patients (>80%), among which locally advanced cervical cancer was the commonest etiology (37.3%) followed by bladder cancer (17.3%). Regarding the indication for PCN tube placement, AKI accounted for 70% (77) of the indications, whereas infection of the obstructed system and flank pain were diagnosed in the remaining 16.4% and in 13.6% of the cases, respectively. Associated comorbidities such as hypertension and diabetes were diagnosed in 45.5% (50) of the patients while the remaining 54.5% (60) did not have any concomitant illness. All of the operated patients had a baseline ultrasound scan of the abdomen and, among these, 26.4% (29) of them had severe hydronephrosis whereas 73.6% (81) patients had moderate hydronephrosis at presentation. Details of baseline clinical characteristics are described in Table 1.
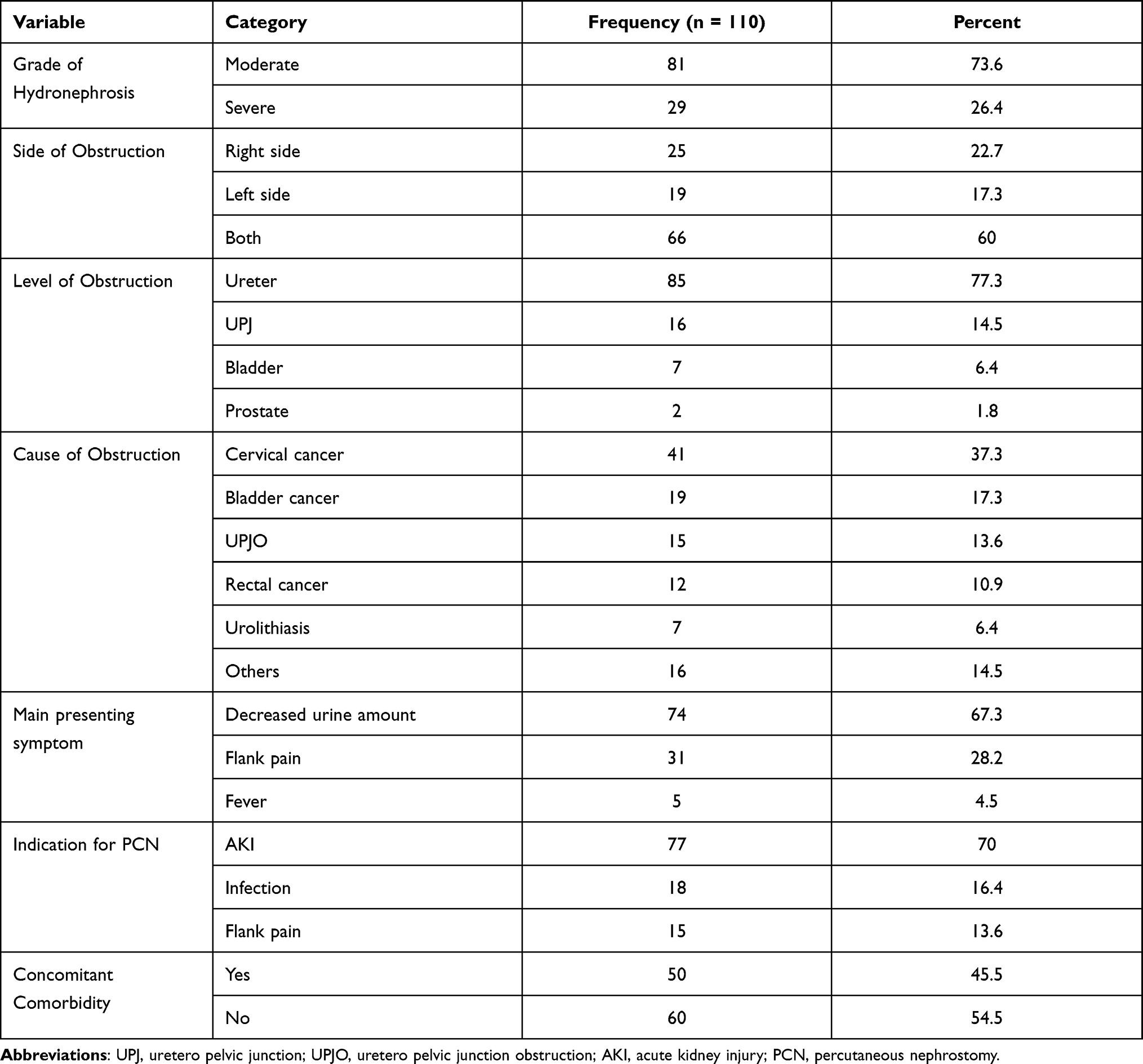 |
Table 1 Baseline Clinical Characteristics of Emergency Patients with Obstructive Uropathy |
Procedure-Related Findings
Among the 110 operated patients in both urologic centers, the procedure is performed on the right kidney in 56.4% (62) patients and on the left kidney in 43.6% (48) patients. No procedure was performed to both the right and left kidney at the same time. The type of imaging modality used to guide the procedure include ultrasonography in 75.5% (83) patients whereas a combination of both fluoroscope and ultrasonography was used in 24.5% (27) patients.
Fluoroscopy alone was not used as a mode of guidance in both urology centers. Regarding the mode of anesthesia utilized, local anesthetic agents were used in 93.6% (104) of the patients while general and spinal anesthesia were used in 3 patients each. Urologists and urology residents performed 79.1% (87) of the procedures while interventional radiologists performed the remaining 20.9% (23). All operated patients were kept in the respective hospitals for a minimum of 6–12 hours and their urine output was monitored.
Outcome of Emergency PCN
Out of the total 110 procedures performed, PCN tube was successfully inserted into the obstructed kidney in 81% (89) patients and technically failed in the remaining 19%. A successful clinical outcome after correct PCN tube insertion is evidenced in 75.5% (83). Six patients (6.5%) who underwent correct PCN tube insertion failed to clinically improve in the post-procedure period.
About 67% of patients with successful outcome had moderate hydronephrosis on pre-procedure ultrasound scan while the remaining 32.5% had a severe one. A total of 46 patients (41.8%) developed post-procedure complications in the first month after PCN. Among these, more than half occurred in female patients.
Tube-related complications commonly included nephrostomy tube blockade, tube dislodgement, and surgical site infection (Figure 2).
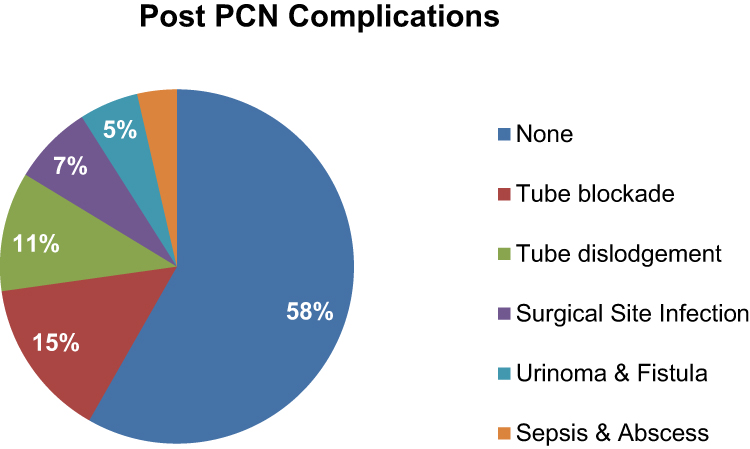 |
Figure 2 Complication rate after emergency PCN. |
Factors Associated with Outcome of Emergency PCN
The results of the univariate and multivariate analyses of association between identified clinical factors and overall success rate of image-guided PCN are depicted in Table 2. In our study, being male was associated with an increased likelihood of successful overall outcome of image-guided PCN [AOR = 5.72 (1.13–28.92) at 95% CI; p = 0.035]. Having a severe degree of hydronephrosis on the preoperative ultrasound study was also associated with an increased overall success rate [AOR = 7.12 (1.32–38.45) at 95% CI; p = 0.022]. Similarly, the use of combined ultrasound and fluoroscope as a modality of guidance to the procedure and having AKI as an indication of the operation are associated with higher likelihood of successful overall outcome [AOR = 12.91 (1.13–46.54) at 95% CI; p = 0.039] and [AOR = 5.64 (1.15–27.44) at 95% CI; p= 0.032], respectively. Absence of comorbidity at the time of presentation also increased likelihood of overall procedure success [AOR = 3.97 (1.10–14.36) at 95% CI; p = 0.035]. Contrary to this, the presence of any postoperative complication was associated with a decreased probability of PCN success [AOR = 0.26 (0.08–0.86) at 95% CI; p = 0.027].
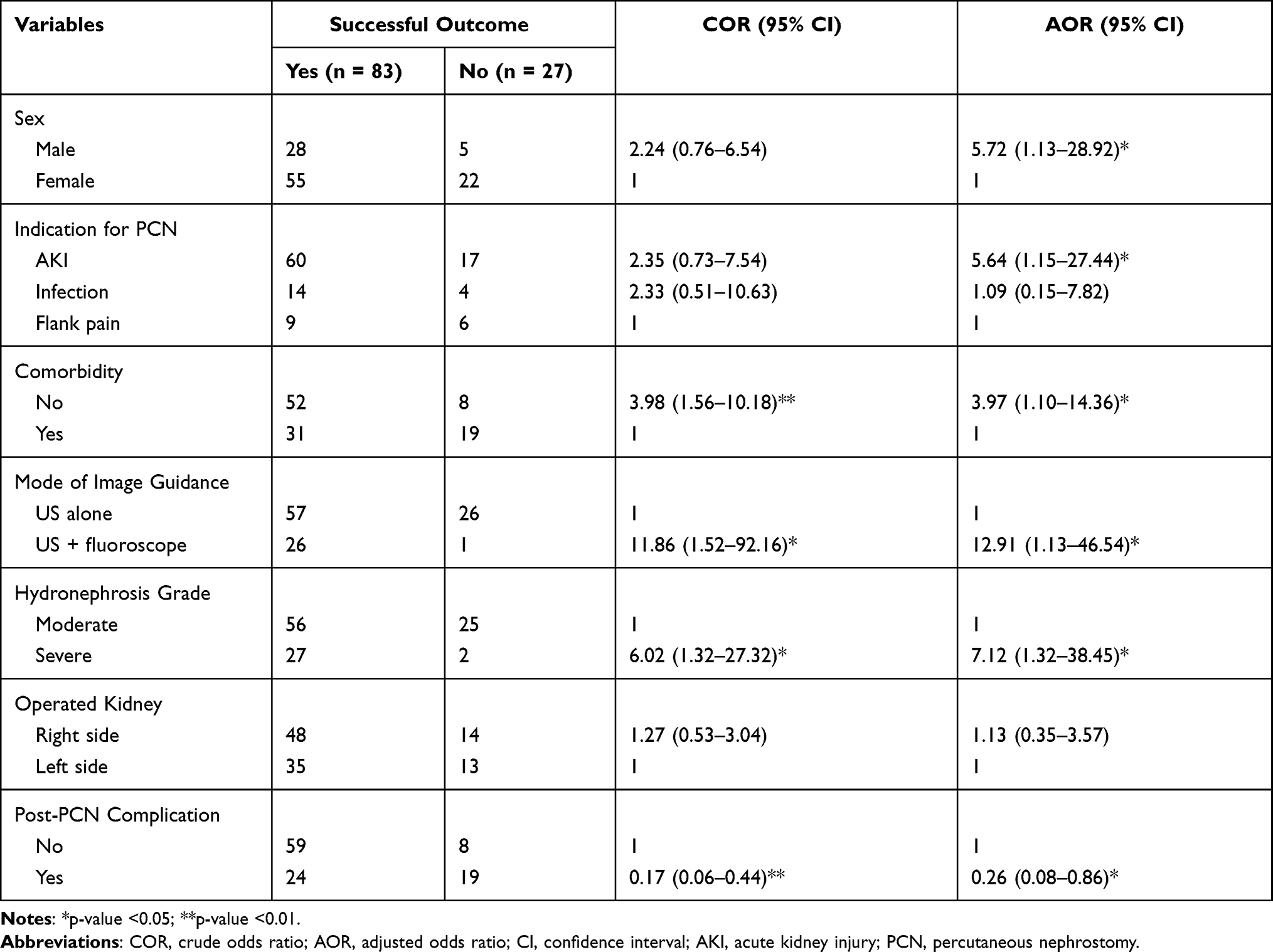 |
Table 2 Factors Associated with Outcome of Emergency PCN |
Discussion
This study assessed the overall success rate and determinant factors of image-guided PCN tube placement in patients diagnosed with OU by retrospectively reviewing 110 patient cards. OU is a major disease burden in urologic practice in both males and females of all age groups and can occur at any anatomic level of the urinary tract.
There is a consistent report in the literature regarding the age pattern at presentation of these patients for PCN (i.e. 40–50 years) and our study also showed 48.2 years (SD = 12.9) as the mean age at presentation. On the other hand, there are inconsistencies on the gender distribution. Some studies reported image-guided PCN to be performed in males more commonly than in females while other studies showed females with OU to be commonly encountered during this procedure.1,16,18–21 Our study shows a female predominance (70%), which is partly explained by the finding that cervical cancer is the commonest cause of OU in this study (37.3%) and more than 50% of OU patients with bladder cancer were females. However, being male was associated with an increased likelihood of successful outcome of emergency PCN [AOR = 5.72 (1.13–28.92) at 95% CI; p = 0.035]. This can be partly explained by a better tolerance of procedure-related pain and lower incidence of post-procedure complications among men.
Regarding the causes of OU, many literatures showed that most cases are secondary to lower urinary tract pathologies which are primarily malignant.11,21 Our study also showed a similar finding in which more than 80% of the obstructive pathologies were caused by pelvic malignancies and the ureter was essentially the commonest part of urinary tract involved (77%).
The bi-laterality of OU among patients who are candidates for PCN is variable in most studies, ranging from 35 to 55%.8,9,14 Our study showed that 77 (60%) of the studied patients presented with involvement of both kidneys and all of them were diagnosed with AKI, which is explained by the finding that >80% of our patients had pelvic malignancies, such as cervical, bladder and rectal cancers, which increase the likelihood of the involvement of both renal systems. Consistent with the above findings, AKI was the commonest indication for PCN (70%), followed by infection (16%) and flank pain (14%). The fact that 60% of our patients had bilateral obstruction strongly supports the high prevalence of AKI among our patients. In addition to this, we found that image-guided PCN performed for an indication of AKI is associated with a six-fold increased likelihood of a successful outcome [AOR = 5.64 (1.15–27.44) at 95% CI; p = 0.032]. This finding supports the observation stated by various studies in which post-obstructive AKI accounts for 72–90% of the indications for PCN and has a higher probability of a successful outcome; this can be explained by the usual presence of marked hydronephrosis in such patients.2,9,10
PCN is a kidney-saving and, for that matter, life-saving emergency procedure with a high success rate.11,21 In the year 1974, Pedersen first described ultrasound-guided placement of PCN tube into an obstructed kidney and reported a success rate of 75%.1 In the literature, many factors are mentioned as determinants of successful outcome such as degree of hydronephrosis, imaging technique used, and experience of the surgeon. Among these, the first two factors are considered widely accepted predictors. On the other hand, other reports indicate an 83–95% success rate regardless of the type of imaging modality used and the grade of hydronephrosis.1,8,11
In our study, we found a success rate of 75.5%, which is lower than the rates in the above studies. This can be explained by the fact that majority of our patients had a moderate hydronephrosis (73.6%) and nearly two-thirds of the procedures (75.5%) were done under ultrasound guidance alone. We identified a seven-fold increased likelihood of successful overall outcome in patients with severe hydronephrosis [AOR = 7.12 (1.32–38.45) at 95% CI; p = 0.022] as compared to those with moderate hydronephrosis, which is coherent with many literatures which previously stated that successful outcome of emergency PCN is directly proportional to the grade of pelvicalyceal dilatation.8,11 This observation clearly indicates the technical ease to puncture a well dilated kidney as the anatomic landmarks and adjacent organs are well delineated.
We also found that the use of combined image guidance system is associated with an increased probability of overall success [AOR = 12.91 (1.13–46.54) at 95% CI; p = 0.039] as compared to the use of ultrasound alone. It has been reported that combining fluoroscopy with ultrasound has a significant benefit in accessing the calyceal system and accurately placing the guide wire and nephrostomy tube.
In this study, 6 patients were identified where PCN was technically successful but the patients failed to clinically improve likely due to complications related to the tube. This indicates that a successful nephrostomy tube insertion does not guarantee a successful clinical outcome and functionality of the tube should be assessed post-operatively.
Emergency PCN tube placement is considered an effective procedure with high safety profile in many studies.22–24 Generally, according to Society of Interventional Radiology (SIR) standards of practice committee classification of complications by outcome, overall complication rate of 10% is recommended as the upper limit in patients undergoing PCN.24 However, in our study we found a high overall complication rate (41.8%). On the other hand, the presence of a post-operative complication is significantly associated with a negative overall outcome of emergency PCN [AOR = 0.26 (0.08–0.86) at 95% CI; p = 0.027] as compared to patients with no complications.
In a hospital-based study done in Spain, many of these complications are labeled as minor and a 38% incidence is reported.23 However, our study clearly showed that these complications independently affect overall outcomes of emergency PCN tube insertion and labeling them as minor complications seems to undermine their negative impact on clinical improvement.
Conclusion
In general, based on our study, the overall success of emergency PCN is low. The likelihood of success is higher in male patients with severe hydronephrosis. The use of combined imaging modality using ultrasound and fluoroscope to guide the procedure also increases the likelihood of success. With a strict adherence to radiation safety protocols while using fluoroscope together with a US, overall outcome of the procedure can be maximized while reducing radiation-related risks.
Post-operative complications significantly reduce the success rate of PCN and are identified as possible reasons for failure of clinical improvement despite having a technically successful procedure. Nephrostomy-related complications such as tube blockade and dislodgement are common in those patients with unsatisfactory clinical outcomes, most of whom are already debilitated by malignancy. Hence, we recommend a strict post-operative follow-up to timely manage tube-related morbidities and attain optimum clinical improvement. Limitations of this study include lack of data regarding body habitus of the patients, type and size of the nephrostomy tubes and the skill of the operator.
Abbreviations
OU, Obstructive Uropathy; PCN, Percutaneous Nephrostomy; AKI, Acute Kidney Injury; EAU, European Association of Urology; ECCM, Emergency and Critical Care Medicine; CKD, Chronic Kidney Disease; BMI, Body Mass Index; CT, Computed Tomography; TASH, Tikur Anbessa Specialized Hospital; SPHMMC, St. Paul’s Hospital Millennium Medical College; SPSS, Statistical Package for Social Sciences; WBC, White Blood Cell; Cr, Creatinine.
Data Sharing Statement
The datasets used in this study are available and can be accessible upon a reasonable request.
Ethics Approval
Institutional Review Boards (IRBs) of both Tikur Anbessa Specialized Hospital and St. Paul’s Hospital Millennium Medical College evaluated the research proposal and each granted a signed letter of ethical clearance. Consent for publication was waived due to the retrospective nature of the study. All identifiers on patient charts such as medical record numbers, names, phone numbers and addresses were not disclosed to ensure full confidentiality of patient data.
Acknowledgments
The authors would like to acknowledge the cooperation of staff members of both SPHMMC and TASH in the process of data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
St. Paul’s Hospital Millennium Medical College (SPHMMC) funded the research project.
Disclosure
All authors declared that they had no competing interests.
References
1. Efesoy O, Saylam B, Bozlu M, Çayan S, Akbay E. The results of ultrasound-guided percutaneous nephrostomy tube placement for obstructive uropathy: a single-centre 10-year experience. Turk J Urol. 2018;44(4):329. doi:10.5152/tud.2018.25205
2. Kirstan K. Pathophysiology of urinary tract obstruction. In: Wein AJ, Kavoussi LR, Partin AW, Peters CA, editors. Campbell-Walsh Urology.
3. Allen DJ, Longhorn SE, Philp T, Smith RD, Choong S. Percutaneous urinary drainage and ureteric stenting in malignant disease. Clin Oncol. 2010;22(9):733–739. doi:10.1016/j.clon.2010.07.004
4. Çırakoğlu A, Benli E. Easy method for percutaneous nephrostomy placement with transrectal ultrasonography probe. J Laparoendosc Adv Surg Tech. 2019;29(12):1565–1570. doi:10.1089/lap.2018.0810
5. Rana AM, Zaidi Z, El-Khalid S. Single-center review of fluoroscopy-guided percutaneous nephrostomy performed by urologic surgeons. J Endourol. 2007;21(7):688–691. doi:10.1089/end.2006.0281
6. Hwang JY, Shin JH, Lee YJ, Yoon HM, Cho YA, Kim KS. Percutaneous nephrostomy placement in infants and young children. Diagn Interv Imaging. 2018;99(3):157–162. doi:10.1016/j.diii.2017.07.002
7. Egilmez H, Oztoprak I, Atalar M, et al. The place of computed tomography as a guidance modality in percutaneous nephrostomy: analysis of a 10-year single-center experience. Acta Radiol. 2007;48(7):806–813. doi:10.1080/02841850701416528
8. Sood G, Sood A, Jindal A, Verma DK, Dhiman DS. Ultrasound guided percutaneous nephrostomy for obstructive uropathy in benign and malignant diseases. Int Braz J Urol. 2006;32:281–286. doi:10.1590/S1677-55382006000300004
9. Daniel K, Kenneth K, Evonne T. Are All Urgent Nephrostomies That Urgent? Melbourne, VIC, Australia: Springer; 2018. doi:10.1007/s10140-018-1598-7
10. Karim R, Sengupta S, Samanta S, Aich RK, Das U, Deb P. Percutaneous nephrostomy by direct puncture technique: an observational study. Indian J Nephrol. 2010;20(2):84. doi:10.4103/0971-4065.65301
11. Ahmed M, Lawal AT, Bello A, et al. Ultrasound guided percutaneous nephrostomy: experience at ahmadu bello university teaching hospital, Zaria. Niger J Clin Pract. 2017;20(12):1622–1625. doi:10.4103/njcp.njcp_138_17
12. Radecka E, Magnusson A. Complications associated with percutaneous nephrostomies. A Retrospective Study Acta Radiologica. 2004;45(2):184–188. doi:10.1080/02841850410003671
13. Ali SM, Mehmood K, Faiq SM, Ali B, Naqvi SA, Rizvi AU. Frequency of complications in image guided percutaneous nephrostomy. J Pak Med Assoc. 2013;63(7):816–820.
14. Wah TM, Weston MJ, Irving HC. Percutaneous nephrostomy insertion: outcome data from a prospective multi-operator study at a UK training centre. Clin Radiol. 2004;59(3):255–261. doi:10.1016/j.crad.2003.10.021
15. Liu BX, Huang GL, Xie XH, Zhuang BW, Xie XY, Lu MD. Contrast-enhanced US-assisted percutaneous nephrostomy: a technique to increase success rate for patients with nondilated renal collecting system. Radiology. 2017;285(1):293–301. doi:10.1148/radiol.2017161604
16. Brandt MP, Lehnert T, Czilwik T, et al. CT-guided nephrostomy–an expedient tool for complex clinical scenarios. Eur J Radiol. 2019;110:142–147. doi:10.1016/j.ejrad.2018.11.028
17. Speed JM, Wang Y, Leow JJ, et al. The effect of physician specialty obtaining access for percutaneous nephrolithotomy on perioperative costs and outcomes. J Endourol. 2017;31(11):1152–1156. doi:10.1089/end.2017.0441
18. Cui XW, Ignee A, Maros T, Straub B, Wen JG, Dietrich CF. Feasibility and usefulness of intra-cavitary contrast-enhanced ultrasound in percutaneous nephrostomy. Ultrasound Med Biol. 2016;42(9):2180–2188. doi:10.1016/j.ultrasmedbio.2016.04.015
19. Abdelazim H, Amer A, Tarig H. Audit of percutaneous nephrostomy in rabat urological centre. Sud J Med Sc. 2010;5:9–11.
20. Turo R, Horsu S, Broome J, et al. Complications of percutaneous nephrostomy in a district general hospital. Turk J Urol. 2018;44(6):478. doi:10.5152/tud.2018.37336
21. Bhatt S, Verma P, Grover RK, Sharma P, Rajaram S. Success, effectiveness and safety of combined sonographic and fluoroscopic guided percutaneous nephrostomy in malignant ureteral obstruction. Int J Radiol Radiat Ther. 2017;3(1):00048. doi:10.15406/ijrrt.2017.03.00048
22. Skolarikos A, Alivizatos G, Papatsoris A, Constantinides K, Zerbas A, Deliveliotis C. Ultrasound-guided percutaneous nephrostomy performed by urologists: 10-year experience. Urology. 2006;68(3):495–499. doi:10.1016/j.urology.2006.03.072
23. Camunez F, Echenagusia A, Prieto ML, Salom P, Herranz F, Hernandez C. Percutaneous nephrostomy in pyonephrosis. Urol Radiol. 1989;11(1):77–81. doi:10.1007/BF02926481
24. Pabon-Ramos WM, Dariushnia SR, Walker TG, d’Othée BJ, Ganguli S, Midia M. Quality improvement guidelines for percutaneous nephrostomy. J Vasc Interv Radiol. 2016;27(3):410–414. doi:10.1016/j.jvir.2015.11.045
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.