Back to Journals » Infection and Drug Resistance » Volume 13
Emergence of an NDM-5-Producing Escherichia coli Sequence Type 410 Clone in Infants in a Children’s Hospital in China
Authors Li J, Yu T, Tao XY, Hu YM, Wang HC, Liu JL, Zhou HJ, Zou MX
Received 6 January 2020
Accepted for publication 15 February 2020
Published 28 February 2020 Volume 2020:13 Pages 703—710
DOI https://doi.org/10.2147/IDR.S244874
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sahil Khanna
Jun Li, 1 Ting Yu, 1 Xiao-Yan Tao, 1 Yong-Mei Hu, 1 Hai-Chen Wang, 1 Jian-Long Liu, 2 Hai-Jian Zhou, 3 Ming-Xiang Zou 1
1Department of Clinical Laboratory, Xiangya Hospital, Central South University, Changsha, Hunan 410008, People’s Republic of China; 2Department of Clinical Laboratory, Hunan Children’s Hospital, Changsha, Hunan 410007, People’s Republic of China; 3State Key Laboratory for Infectious Disease Prevention and Control, National Institute for Communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 102206, People’s Republic of China
Correspondence: Ming-Xiang Zou
Department of Clinical Laboratory, Xiangya Hospital, Central South University, Changsha, Hunan 410008, People’s Republic of China
Tel +86 13907496278
Email [email protected]
Purpose: Outbreaks of infection due to carbapenem-resistant Enterobacterales (CRE), including New Delhi metallo-β-lactamase (NDM)-producing Escherichia coli, have been increasingly reported worldwide, primarily in adults and rarely in children. The goal of this study was to characterize an outbreak of infection caused by NDM-5-producing E. coli in a children’s hospital in China.
Methods: A total of 86 CRE isolates were collected from 85 hospitalized children between June 2017 and May 2018. These isolates were subjected to multiple phenotypic and molecular tests, including in vitro antimicrobial susceptibility testing, PCR, pulsed-field gel electrophoresis (PFGE), multilocus sequence typing (MLST), and whole-genome sequencing (WGS).
Results: Among the 86 CRE isolates, we identified 9 NDM-5-producing E. coli isolates, with 5 of them sharing the same PFGE pattern, same MLST type (ST410), same plasmid replicon type (IncFII), and nearly the same set of additional resistance genes. All 9 isolates were resistant to most antimicrobial agents, including carbapenems, cephalosporins, and levofloxacin, while being sensitive to trimethoprim/sulfamethoxazole, amikacin, tigecycline, and colistin. According to the clinical background, all 9 isolates were collected in a period of < 3 months from infants among whom there was overlap in the time of hospitalization. None of them had a travel history.
Conclusion: Our analysis suggests an outbreak of clonal dissemination, presumably due to nosocomial transmission. This study represents the first documented outbreak of NDM-5-producing E. coli mediated by IncFII in infants. Close monitoring is urgently needed to prevent and control the spread of this difficult-to-treat superbug.
Keywords: Enterobacterales, carbapenem resistance, blaNDM-5, IncFII
Introduction
Carbapenem-resistant Enterobacterales (CRE) have emerged as one of the major multidrug-resistant bacterial pathogens responsible for a variety of healthcare-associated infections.1–3 CRE are very difficult to treat and have been referred as superbugs and nightmare bacteria, because they do not respond to commonly used antibiotics and are associated with high mortality. While there have been numerous reports of CRE infections including nosocomial outbreaks in adult patients worldwide, there are few reports of such infections in children.4,5 A nationwide study in the USA reported that the frequency of CRE isolates in children (age range 1–17 years) increased from 0% in 1999–2000 to 0.47% in 2010–2011.6 Despite this increasing threat to children, little is known about the epidemiology, treatment, and prognosis of these infections in this population.
Among the heterogeneous forms of carbapenemases, New Delhi metallo-β-lactamase (NDM) is one of the most important enzymes accounting for carbapenem-resistance. Since the first NDM reported in 2009 from Klebsiella pneumoniae, a total of 24 variants of the NDM enzyme have been identified globally, and they are referred to as NDM-1 to NDM-24.7 Among these variants, NDM-5, first identified in an Escherichia coli strain in the UK in 2011, has attracted extensive attention due to its increased resistance phenotype and rapid dissemination.8 This enzyme is encoded by the blaNDM-5 gene, which can be carried and transferred among different incompatibility types of plasmids, such as IncX3 and IncFII.9–11 These properties enable wide dissemination of blaNDM-5 through horizontal gene transfer among the members of Enterobacterales. Indeed, NDM-5-producing isolates have been identified worldwide,8,9,12–17 not only from humans but also from animals such as dog and cow,18,19 as well as hospital environments’ sewage water.20 Like all other CRE isolates, the vast majority of the human NDM-5 isolates have been identified in the adult population with only a few cases reported in children.21,22 Reports of outbreaks of NDM-5-producing in neonates are rarer still.23 There has been only one report of clonal dissemination involving NDM-5-producing E. coli (ST410) in 4 adults in a university hospital in China.24 However, there has been no report of an outbreak of NDM-5-producing E. coli (ST410) in children.
In this report, we describe the first outbreak of NDM-5-producing E. coli isolates representing the sequence type 410 isolated from infants in a children’s hospital in China.
Materials and Methods
Ethics Statement and Study Subjects
This retrospective study was carried out in accordance with the recommendations of the Ethics Committee of Hunan Children’s Hospital (Changsha, Hunan Province, China) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The protocol was approved by the Ethics Committee of Hunan Children’s Hospital (Changsha, Hunan Province, China). Written informed consent was obtained from the patients’ guardians prior to the study.
Bacterial Strains
A total of 86 CRE isolates confirmed by a VITEK-2 automated microbiology analyzer (bioMérieux, Marcyl’Etoile, France) were collected between June 2017 and May 2018 from 85 infants (aged from 0 to 36 months) at the Hunan Children’s Hospital in China. A single isolate was obtained from each patient except for one patient from whom 2 sequential isolates were available. All isolates were further identified by Matrix Assisted Laser Desorption/Ionization Time of Flight Mass Spectrometry (MALDI-TOF-MS; Bruker Daltonics GmbH, Germany). E. coli ATCC 25922 was obtained from the National Center for Clinical Laboratories, China, and used as a quality control strain.
Identification of the blaNDM-5 Gene
Genomic DNA in clinical isolates was extracted from overnight cultured strains using a boiling method.25 To detect the blaNDM-5 gene in these DNA samples, PCR was performed using blaNDM-5-specific primers as previously described.8 Positive PCR products were subjected to direct Sanger sequencing. All blaNDM-5-containing isolates were further characterized as described below.
Antimicrobial Susceptibility Testing and Detection of Metallo-Lactamases Phenotypes
Minimal inhibitory concentrations (MICs) of the following antibiotics against blaNDM-5-positive isolates were determined using the broth microdilution method: piperacillin/tazobactam (TZP), ertapenem (ETP), imipenem (IPM), meropenem (MEM), aztreonam (ATM), ceftazidime (CAZ), ceftriaxone (CRO), levofloxacin (LEV), amikacin (AMK), colistin (CST), and trimethoprim/sulfamethoxazole (TMP-SMZ). The susceptibility breakpoints were defined according to the Clinical and Laboratory Standards Institute (CLSI) standards.26 The MIC of tigecycline (TGC) was determined by E-test (bioMérieux, France) and interpreted in accordance with the US Food and Drug Administration (FDA) breakpoint (resistant breakpoint, 2 μg/mL). In all MIC tests, E. coli ATCC 25922 was used as a quality control strain.
The EDTA-modified carbapenem inactivation method (eCIM) combined with the modified carbapenem inactivation method (mCIM) was used to identify metallo-lactamases according to the standard procedures of CLSI.26
Determination of Genetic Relatedness
Genetic relatedness among blaNDM-5-positive isolates was determined by pulsed-field gel electrophoresis (PFGE). In brief, bacterial cells harvested from stationary-phase culture were embedded in agarose gel plugs (Lonza Rockland, ME, USA) and lysed by proteinase K, followed by restriction digestion with XbaI (Promega, USA) for 18 h at 37°C. Electrophoresis was performed at 14°C for 19 h using the Bio-Rad CHEF III system (120° angle, 6 V/cm, with switch times of 6 s and 36 s). Gels were stained with GelRed (Biotium Inc.) and digitally captured under UV light. Cluster analysis was performed with BioNumerics software Version 5.1 (Applied Maths, Kortrijk, Belgium) using the Dice Similarity Coefficient. Isolates with >85% pattern similarities were considered to be from the same PFGE cluster.27,28
A subset of isolates representing different PFGE clusters were further analyzed by multilocus sequence typing (MLST) based on 7 housekeeping genes of E. coli (adk, fumC, gyrB, icd, mdh, purA, and recA) following the Institut Pasteur scheme.29
WGS-Based Deduction of Resistance Genes and Plasmids
WGS was performed to detect resistant genes and identify resistant plasmids in NDM-5-producing strains. Briefly, genomic DNA was extracted using the DNeasy UltraClean Microbial Kit (QIAGEN, GmbH, Germany) following the manufacturer’s recommendations. Approximately 10 μg of DNA for each strain was used to construct 2 Illumina paired-end libraries with average insertion lengths of 500 bp and 2000 bp. Libraries were sequenced using an Illumina GA IIx sequencer (Illumina Inc., San Diego, CA, USA). Raw data were processed by removing the following: 1) reads with 5 bp of ambiguous bases, 2) reads with 20 bp of low-quality (≤ Q20) bases, 3) adapter contamination, and 4) duplicated reads. The final cleaned reads had an about 100 × genome coverage for each strain. Genome assembly was performed using SOAPdenovo v1.05.30 The resistant genes and typing of plasmids of all NDM-5-producing isolates were analyzed using Resfinder and PlasmidFinder tool, respectively, which were provided by the Centre for Genomic Epidemiology.31
Results
Clinical Characteristics of blaNDM-5-Positive Isolates
Based on MALDI-TOF-MS analyses, the 86 CRE isolates confirmed by VITEK-2 were categorized into 5 species, including K. pneumoniae (56 isolates), E. coli (16 isolates), Enterobacter aerogenes (9 isolates), Enterobacter cloacae (3 isolates), and Serratia marcescens (2 isolates). Further analysis by PCR using blaNDM-5-specific primers revealed that 9 of them were blaNDM-5-carrying E. coli, which accounted for 10.5% of all isolates tested. These 9 E. coli isolates were collected within 3 months from 8 infants aged from 13 days to 15 months in the same hospital (Table 1). One infant had 2 isolates collected 2 days apart from blood and ascites, separately, while each of the other 7 infants had only one isolate collected from sputum (n = 5) or blood (n = 2). The diagnosed diseases for these infants included pneumonia (n = 4), sepsis (n = 2), megacolon (n = 1, the infant with 2 isolates available), and duodenal atresia (n = 1). None of them had a travel history to other cities. All 8 infants received antibiotic treatment. Only one patient showed no response and died, and the 7 others recovered as evidenced by the resolution of symptoms along with a normal infection index (Table 1).
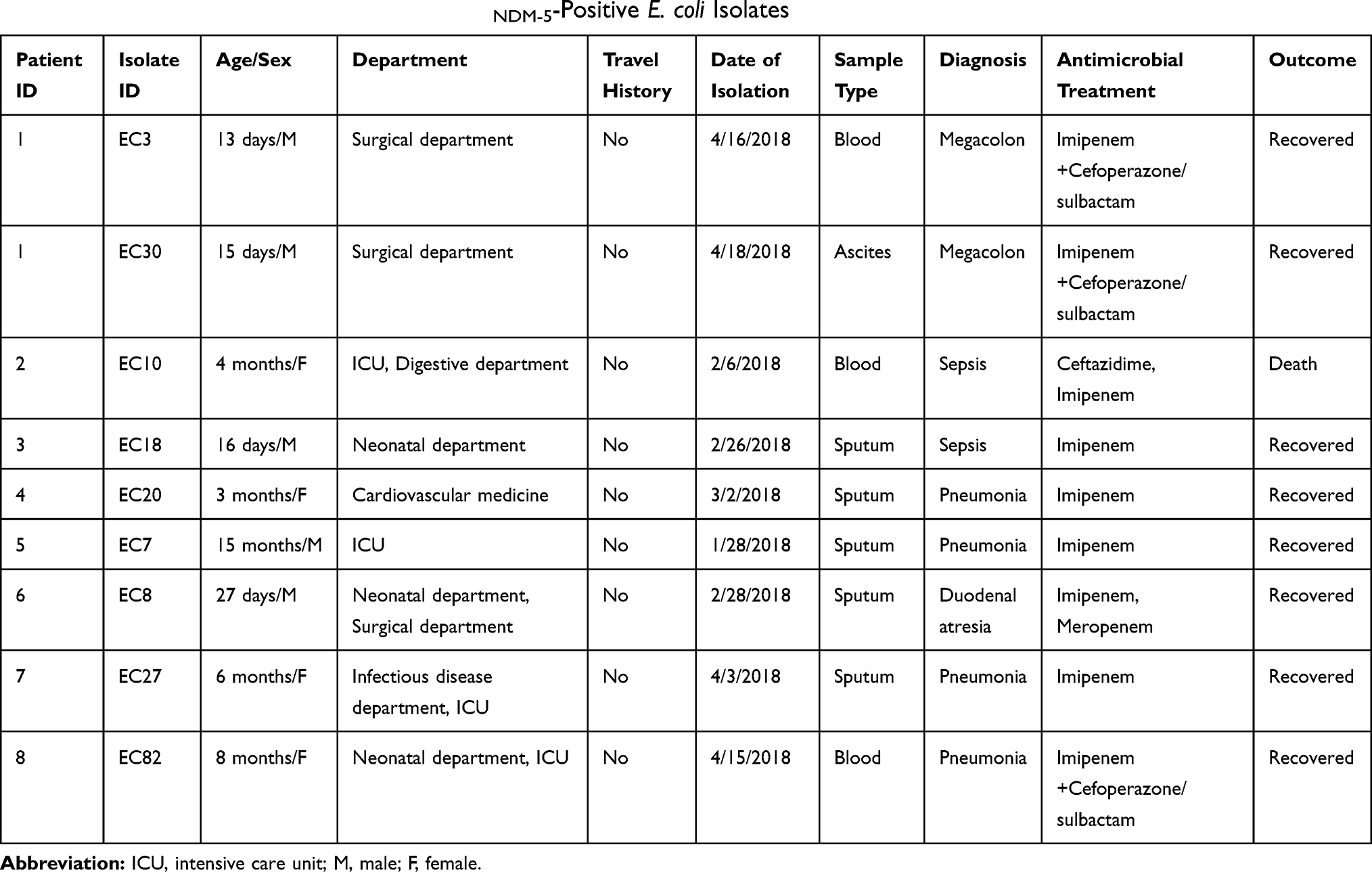 |
Table 1 Clinical Background Information of blaNDM-5-Positive E. coli Isolates |
The timeline of patient admission and sample collection is shown in Figure 1. The first 2 blaNDM-5-carrying E. coli isolates were collected from patients in the intensive care unit (ICU) about 1 week apart, and then 7 isolates were collected one after another from 4 other departments over a period of approximately 2 months. There was overlap in the time of hospitalization among the patients.
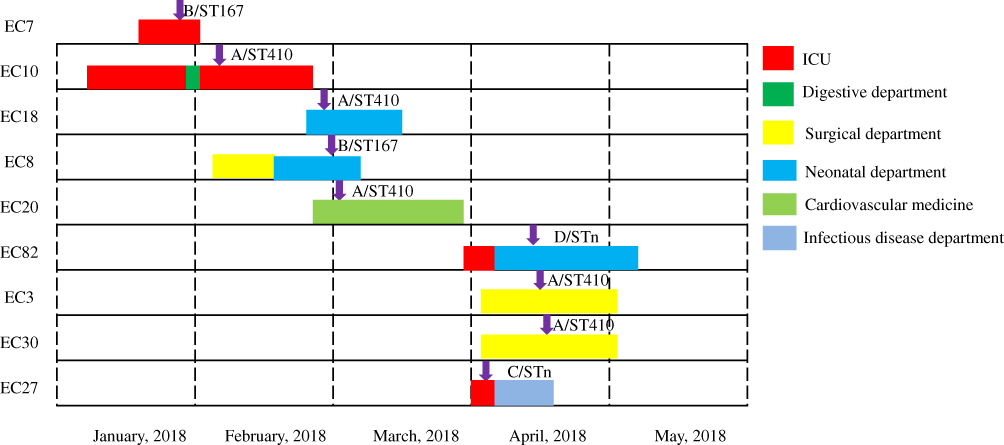 |
Figure 1 Timeline of outbreak of NDM-5-producing E. coli in 8 infants in a Children’s hospital. Labels at the left side represent E. coli isolate IDs, including 2 (EC3 and EC30) obtained from the same patient. The different colors of the bars represent the different departments in which the patients were hospitalized (as shown at the top right), with the length of the bars representing the period of hospitalization. Four patients (for isolates EC10, EC8, EC27, and EC82) were hospitalized in 2 or more departments. The purple arrows indicate the dates of sampling. |
Antimicrobial Susceptibility and Carbapenems Phenotypes
Based on MIC tests, all 9 blaNDM-5-carrying E. coli isolates were resistant to a broad spectrum of antimicrobial agents, including carbapenems, cephalosporins, and levofloxacin. Nevertheless, they were all sensitive to trimethoprim/sulfamethoxazole, amikacin, tigecycline, and colistin (Table 2).
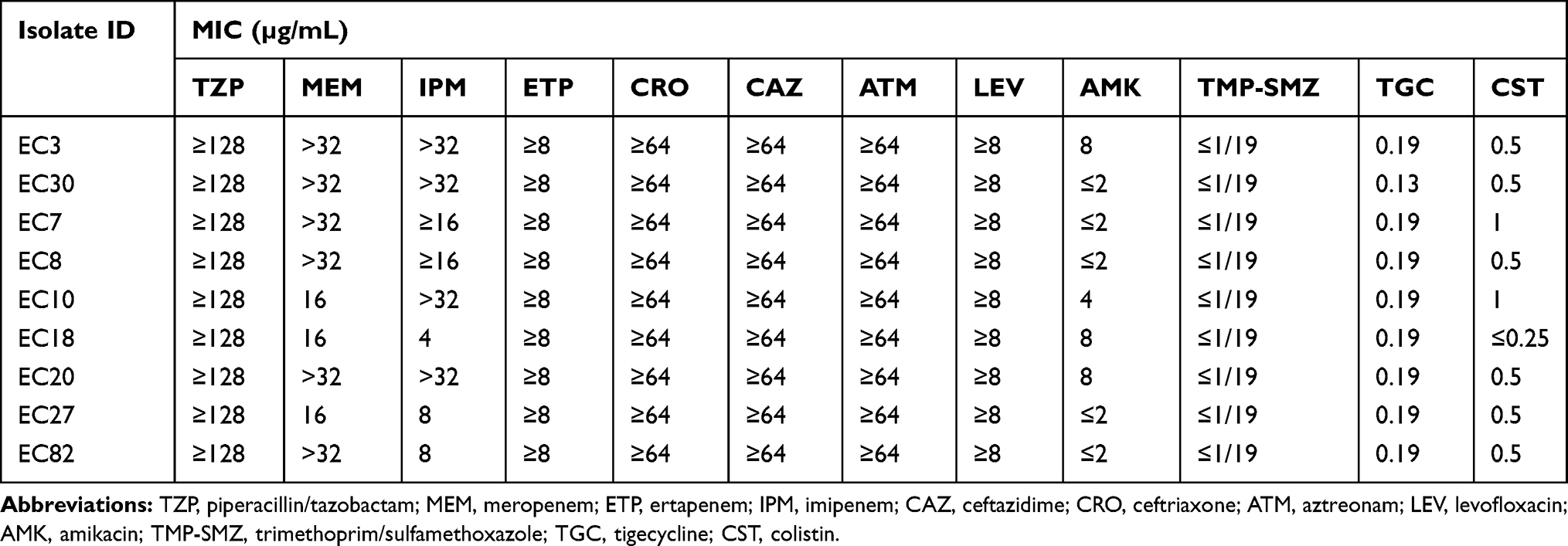 |
Table 2 Antimicrobial Susceptibility of 9 NDM-5-Producing E. coli Isolates |
Based on the eCIM–mCIM combination test, all the 9 isolates were positive for MBL production.
PFGE and Genetic Relatedness Analysis
According to PFGE patterns, 9 blaNDM-5-positive E. coli isolates were divided into 4 distinct types: type A (n = 5), type B (n = 2), type C (n = 1), and type D (n = 1). Based on MLST, these 9 isolates belonged to 3 distinct sequence types (STs), including ST410 (6-4-12-1-20-18-7), ST167 (10-11-4-8-8-13-2), and STn (a new ST). Comparison of the results between PFGE and MLST revealed that PFGE types A and B corresponded to ST410 and ST167, respectively, while both types C and type D of PFGE corresponded to STn. Five blaNDM-5-positive E. coli isolates sharing the same PFGE pattern (type A) and the same MLST type (ST410).
Characterization of Plasmid Replicon Types and Resistance Genes Based on WGS Data
When contigs assembled using Illumina reads from all 9 blaNDM-5-carrying isolates were analyzed by PlasmidFinder, 3 different types of plasmids were detected, including IncFII (n = 5), IncX3 (n = 3), and IncN (n = 1). Correlations of these plasmid types with PFGE and MLST types are illustrated in Figure 2. Of note, all 5 isolates with the same PFGE and MLST types also showed the same plasmid type (IncFII).
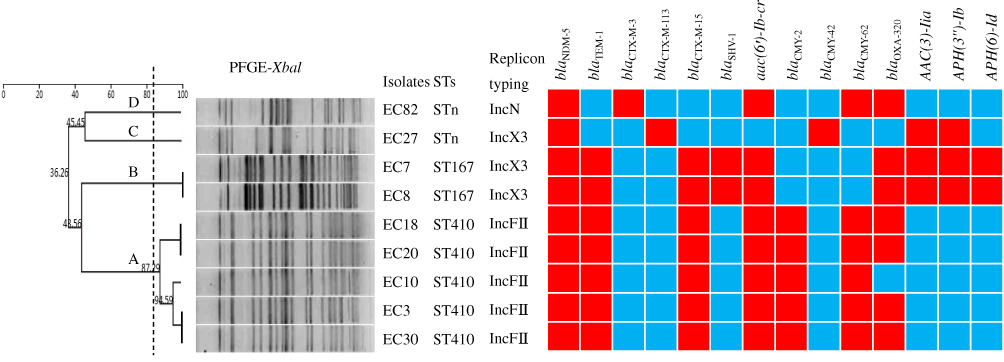 |
Figure 2 Dendrogram of 9 NDM-5-producing E. coli isolates based on pulsed-field gel electrophoresis (PFGE) patterns (indicated as A to D above the branches in the left) and their correlations with multilocus sequence typing (STs), replicon typing, and distribution of resistance genes. The dashed line in the left dendrogram represents 85% pattern similarity; isolates with >85% similarity were considered to have the same homogeneity. The red and blue squares indicate the presence and absence of the resistance genes indicated at the top, respectively. |
Analysis of contigs also confirmed the presence of the blaNDM-5 gene in all nine isolates. In addition, other β-lactamase genes were detected, including blaTEM-1, blaCTX-M-15, blaOXA-320, blaCMY-2, and blaCMY-62, each of which was detected in at least 5 isolates. Plasmid-mediated aac(6′)-Ib-cr was detected in 8 isolates. The remaining genes were infrequent, with each detected in no more than 3 isolates (Figure 2). Of note, all 5 isolates with the same PFGE, MLST and plasmid types also contained the same set of resistance genes except for one (EC10), which did not carry blaOXA-320.
Discussion
In this study, we performed VITEK-2 and MALDI-TOF-MS analyses on a panel of 86 Enterobacterales isolates collected from children between June 2017 and May 2018 in a single Children’s hospital in China. Further PCR analysis revealed 9 of these 86 isolates to be blaNDM-5-carrying E. coli. These 9 E. coli isolates were collected within 3 months from 8 infants aged from 13 days to 15 months (Table 1). Subsequent molecular and phenotypic characterization suggests an outbreak due to clonal dissemination.
The possibility of clonal dissemination was supported by the following observations. First, based on DNA analysis by multiple approaches (Figure 2), all 9 E. coli isolates carried blaNDM-5, with 5 of them (isolates EC3, EC10, EC18, EC20, and EC30) sharing the same PFGE pattern (type A), the same MLST type (ST410), the same plasmid replicon type (IncFII), and nearly the same set of resistance genes (including blaTEM-1, blaCTX-M-15, aac(6′)-Ib-cr, blaCMY-2, blaCMY-62, and blaOXA-320). Two other isolates (EC7 and EC8) also showed the same molecular profile. In addition, eCIM–mCIM confirmed the production of metallo-lactamase in all 9 isolates. These results suggest that these isolates, especially the 5 isolates with the same molecular profile, originated from the same clone.
Second, in vitro MIC tests revealed that all 9 isolates were resistant to a broad spectrum of antimicrobial agents, including carbapenems, third-generation cephalosporins, β-lactam enzyme-inhibitor, and levofloxacin, while they were all sensitive to trimethoprim/sulfamethoxazole, amikacin, tigecycline, and colistin (Table 2).
Third, according to the clinical background and epidemiological information, all 9 isolates were collected over a period of less than 3 months from patients in the same hospital, and there was overlap in the time of hospitalization among these patients (Figure 1). None of these patients had a travel history, although that of their parents is unknown. These findings support the possibility of a nosocomial transmission. Based on the outbreak timeline, it seems that the outbreak started in the ICU and then was transmitted to other departments, although we were unable to identify the original bacterial source or how it was transmitted from one patient to another.
Infections due to NDM-5-producing E. coli ST410 have been mainly reported in adults in Asia, as summarized in Table 3. Recently, Sun et al reported an outbreak involving 4 NDM-5-producing E. coli ST410 isolates in adults in a university hospital in China.24 Our present study is the first to document an outbreak of NDM-5-producing E. coli ST410 in infants. The dominance of the ST410 isolate in our study appears to be different from the previous reports in China showing a dominance of ST167,11,24,32–34 though this difference may be insignificant due to the small sample sizes in all of these studies. While only 2 ST167 isolates were identified in our study, this type of NDM-5-producing E. coli is widely disseminated over the world16,35–37 and has been found to be the predominant type in China.11,24,32–34
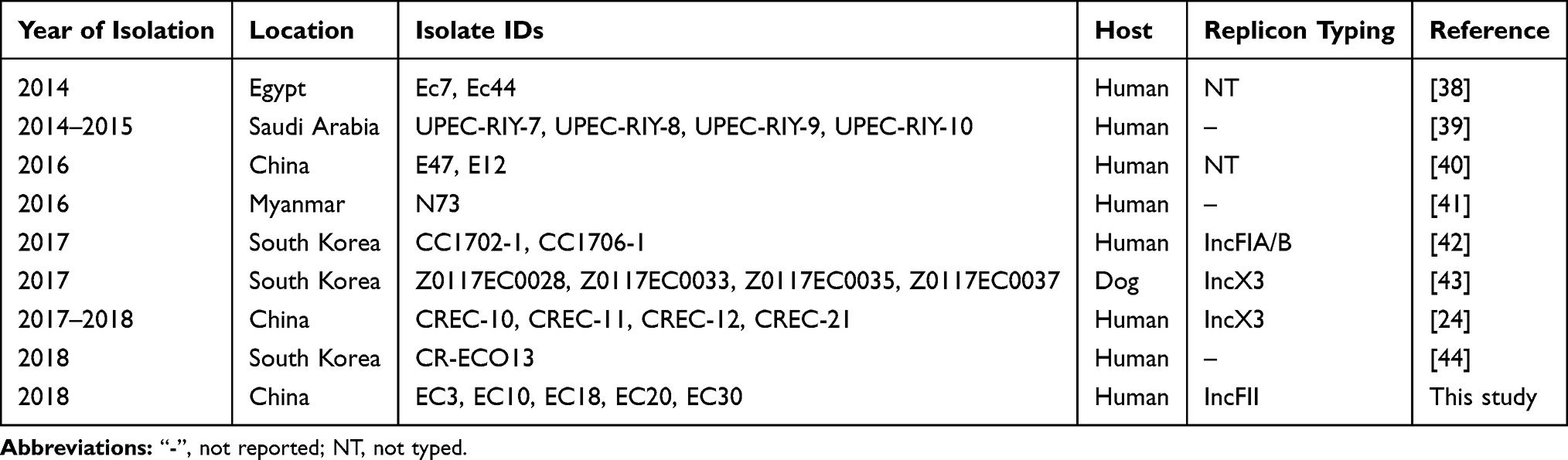 |
Table 3 Previously Reported E. coli Isolates Carrying NDM-5 and ST410 |
As in many bacterial species, mobile elements play a major role in the transmission of blaNDM in a variety of Enterobacterales species. In this study, 5 out of 9 E. coli isolates carried IncFII plasmids, which may account for the clonal spread of blaNDM-5 gene in infants, as has been reported previously for outbreaks in adult patients.45,46 Our study is the first to show a clonal spread of NDM-5-producing E. coli isolates carrying IncFII plasmids in infants. We also detected IncX3 plasmids in 3 NDM-5-producing E. coli isolates. This type of plasmid has been also previously reported in China24,32,47 and other countries.17,38,42,48
Outbreaks of CRE can have a potentially devastating impact on children, especially infants. The outbreak described in this report highlights the need to develop better strategies for determining susceptibility to CRE so that appropriate treatment can be initiated once diagnosed. This outbreak also highlights the importance of improving our knowledge of epidemiological factors that might enhance CRE transmission to susceptible children. Such knowledge is essential for the development of effective control and prevention measures.
Acknowledgments
We are thankful to Jian-Long Liu, a teacher in the Department of Clinical Laboratory, Hunan Children’s Hospital in China, for her help with the isolates collection. We would also like to thank Hai-Jian Zhou, a teacher at the Chinese Center for Disease Control and Prevention, for her help with the PFGE experiments.
Funding
This study was supported by the Natural Science Foundation of Hunan Province (2017JJ3478 and 2018JJ6058), the National Natural Science Foundation of China (81702068), and the Graduate Free Exploration Foundation (502211911) of Central South University.
Disclosure
The authors declare no conflicts of interest.
References
1. Lutgring JD. Carbapenem-resistant Enterobacteriaceae: an emerging bacterial threat. Semin Diagn Pathol. 2019;36(3):182–186. doi:10.1053/j.semdp.2019.04.011
2. Zhang Y, Wang Q, Yin Y, et al. Epidemiology of carbapenem-resistant Enterobacteriaceae infections: report from the China CRE network. Antimicrob Agents Chemother. 2018;62(2):e01882–17. doi:10.1128/AAC.01882-17
3. Li J, Zou MX, Wang HC, et al. An outbreak of infections caused by a Klebsiella pneumoniae ST11 clone coproducing Klebsiella pneumoniae carbapenemase-2 and RmtB in a Chinese teaching hospital. Chin Med J (Engl). 2016;129(17):2033–2039. doi:10.4103/0366-6999.189049
4. Chiotos K, Tamma PD, Flett KB, et al. Increased 30-day mortality associated with carbapenem-resistant Enterobacteriaceae in children. Open Forum Infect Dis. 2018;5(10):ofy222. doi:10.1093/ofid/ofy222
5. Logan LK. Carbapenem-resistant Enterobacteriaceae: an emerging problem in children. Clin Infect Dis. 2012;55(6):852–859. doi:10.1093/cid/cis543
6. Logan LK, Renschler JP, Gandra S, et al. Carbapenem-resistant Enterobacteriaceae in children, United States, 1999–2012. Emerg Infect Dis. 2015;21(11):2014–2021. doi:10.3201/eid2111.150548
7. Wu W, Feng Y, Tang G, et al. NDM metallo-β-lactamases and their bacterial producers in health care settings. Clin Microbiol Rev. 2019;32(2):e00115–18. doi:10.1128/CMR.00115-18
8. Hornsey M, Phee L, Wareham DW. A novel variant, NDM-5, of the New Delhi metallo-beta-lactamase in a multidrug-resistant Escherichia coli ST648 isolate recovered from a patient in the United Kingdom. Antimicrob Agents Chemother. 2011;55(12):5952–5954. doi:10.1128/AAC.05108-11
9. Wailan AM, Paterson DL, Caffery M, et al. Draft genome sequence of NDM-5-producing Escherichia coli sequence type 648 and genetic context of blaNDM-5 in Australia. Genome Announc. 2015;3(2):e00194-15. doi:10.1128/genomeA.00194-15
10. Rojas LJ, Hujer AM, Rudin SD, et al. NDM-5 and OXA-181 beta-lactamases, a significant threat continues to spread in the Americas. Antimicrob Agents Chemother. 2017;61(7):e00454-17. doi:10.1128/AAC.00454-17
11. Xu L, Wang P, Cheng J, et al. Characterization of a novel blaNDM-5-harboring IncFII plasmid and an mcr-1-bearing IncI2 plasmid in a single Escherichia coli ST167 clinical isolate. Infect Drug Resist. 2019;12:511–519. doi:10.2147/IDR.S192998
12. Nakano R, Nakano A, Hikosaka K, et al. First report of metallo-beta-lactamase NDM-5-producing Escherichia coli in Japan. Antimicrob Agents Chemother. 2014;58(12):7611–7612. doi:10.1128/AAC.04265-14
13. Sassi A, Loucif L, Gupta SK, et al. NDM-5 carbapenemase-encoding gene in multidrug-resistant clinical isolates of Escherichia coli from Algeria. Antimicrob Agents Chemother. 2014;58(9):5606–5608. doi:10.1128/AAC.02818-13
14. Valentin T, Feierl G, Masoud-Landgraf L, et al. Proteus mirabilis harboring carbapenemase NDM-5 and ESBL VEB-6 detected in Austria. Diagn Microbiol Infect Dis. 2018;91(3):284–286. doi:10.1016/j.diagmicrobio.2018.02.009
15. Giufre M, Errico G, Accogli M, et al. Emergence of NDM-5-producing Escherichia coli sequence type 167 clone in Italy. Int J Antimicrob Agents. 2018;52(1):76–81. doi:10.1016/j.ijantimicag.2018.02.020
16. Zhu YQ, Zhao JY, Xu C, et al. Identification of an NDM-5-producing Escherichia coli sequence type 167 in a neonatal patient in China. Sci Rep. 2016;6:29934. doi:10.1038/srep29934
17. Paul D, Babenko D, Toleman MA. Human carriage of cefotaxime-resistant Escherichia coli in North-East India: an analysis of STs and associated resistance mechanisms. J Antimicrob Chemother. 2020;75(1):72-76. doi:10.1093/jac/dkz416
18. Yousfi M, Mairi A, Bakour S, et al. First report of NDM-5-producing Escherichia coli ST1284 isolated from dog in Bejaia, Algeria. New Microbes New Infect. 2015;8:17–18. doi:10.1016/j.nmni.2015.09.002
19. He T, Wei R, Zhang L, et al. Characterization of NDM-5-positive extensively resistant Escherichia coli isolates from dairy cows. Vet Microbiol. 2017;207:153–158. doi:10.1016/j.vetmic.2017.06.010
20. Parvez S, Khan AU. Hospital sewage water: a reservoir for variants of New Delhi metallo-beta-lactamase (NDM)- and extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae. Int J Antimicrob Agents. 2018;51(1):82–88. doi:10.1016/j.ijantimicag.2017.08.032
21. Khalifa HO, Soliman AM, Ahmed AM, et al. NDM-4- and NDM-5-producing Klebsiella pneumoniae coinfection in a 6-month-old infant. Antimicrob Agents Chemother. 2016;60(7):4416–4417. doi:10.1128/AAC.00479-16
22. Ahmad N, Khalid S, Ali SM, et al. Occurrence of blaNDM variants among Enterobacteriaceae from a neonatal intensive care unit in a northern India hospital. Front Microbiol. 2018;9:407. doi:10.3389/fmicb.2018.00407
23. Brinkac LM, White R, D’Souza R, et al. Emergence of New Delhi metallo-beta-lactamase (NDM-5) in Klebsiella quasipneumoniae from neonates in a Nigerian hospital. mSphere. 2019;4(2):e00685-18. doi:10.1128/mSphere.00685-18
24. Sun P, Xia W, Liu G, et al. Characterization of blaNDM-5-positive Escherichia coli prevalent in a university hospital in eastern China. Infect Drug Resist. 2019;12:3029–3038. doi:10.2147/IDR.S225546
25. Li J, Zou M, Dou Q, et al. Characterization of clinical extensively drug-resistant Pseudomonas aeruginosa in the Hunan province of China. Ann Clin Microbiol Antimicrob. 2016;15(1):35. doi:10.1186/s12941-016-0148-y
26. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. 29th ed. Document M100-S29 Wayne, PA: Clinical and Laboratory Standards Institute; 2019.
27. Tenover FC, Arbeit RD, Goering RV, et al. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: criteria for bacterial strain typing. J Clin Microbiol. 1995;33(9):2233–2239. doi:10.1128/JCM.33.9.2233-2239.1995
28. Li J, Huang ZY, Yu T, et al. Isolation and characterization of a sequence type 25 carbapenem-resistant hypervirulent Klebsiella pneumoniae from the mid-south region of China. BMC Microbiol. 2019;19(1):219. doi:10.1186/s12866-019-1593-5
29. Pan F, Tian D, Wang B, et al. Fecal carriage and molecular epidemiology of carbapenem-resistant Enterobacteriaceae from outpatient children in Shanghai. BMC Infect Dis. 2019;19(1):678. doi:10.1186/s12879-019-4298-3
30. Sui W, Zhou H, Du P, et al. Whole genome sequence revealed the fine transmission map of carbapenem-resistant Klebsiella pneumonia isolates within a nosocomial outbreak. Antimicrob Resist Infect Control. 2018;7:70. doi:10.1186/s13756-018-0363-8
31. Carattoli A, Zankari E, Garcia-Fernandez A, et al. In silico detection and typing of plasmids using plasmidfinder and plasmid multilocus sequence typing. Antimicrob Agents Chemother. 2014;58(7):3895–3903. doi:10.1128/AAC.02412-14
32. Yang P, Xie Y, Feng P, et al. BlaNDM-5 carried by an IncX3 plasmid in Escherichia coli sequence type 167. Antimicrob Agents Chemother. 2014;58(12):7548–7552. doi:10.1128/AAC.03911-14
33. Zhang LP, Xue WC, Meng DY. First report of New Delhi metallo-beta-lactamase 5 (NDM-5)-producing Escherichia coli from blood cultures of three leukemia patients. Int J Infect Dis. 2016;42:45–46. doi:10.1016/j.ijid.2015.10.006
34. Sun L, Xu J, He F. Draft genome sequence of an NDM-5, CTX-M-15 and OXA-1 co-producing Escherichia coli ST167 clinical strain isolated from a urine sample. J Glob Antimicrob Resist. 2018;14:284–286. doi:10.1016/j.jgar.2018.08.005
35. Gronthal T, Osterblad M, Eklund M, et al. Sharing more than friendship - transmission of NDM-5 ST167 and CTX-M-9 ST69 Escherichia coli between dogs and humans in a family, Finland, 2015. Euro Surveill. 2018;23(27):1700497. doi:10.2807/1560-7917.ES.2018.23.27.1700497
36. Peterhans S, Stevens MJA, Nuesch-Inderbinen M, et al. First report of a blaNDM-5-harbouring Escherichia coli ST167 isolated from a wound infection in a dog in Switzerland. J Glob Antimicrob Resist. 2018;15:226–227. doi:10.1016/j.jgar.2018.10.013
37. Nukui Y, Ayibieke A, Taniguchi M, et al. Whole-genome analysis of EC129, an NDM-5-, CTX-M-14-, OXA-10- and MCR-1-co-producing Escherichia coli ST167 strain isolated from Japan. J Glob Antimicrob Resist.2019;18:148–150. doi:10.1016/j.jgar.2019.07.001
38. Soliman AM, Zarad HO, Nariya H, et al. Genetic analysis of carbapenemase-producing Gram-negative bacteria isolated from a university teaching hospital in Egypt. Infect Genet Evol. 2020;77:104065. doi:10.1016/j.meegid.2019.104065
39. Abd El Ghany M, Sharaf H, Al-Agamy MH, et al. Genomic characterization of NDM-1 and 5, and OXA-181 carbapenemases in uropathogenic Escherichia coli isolates from Riyadh, Saudi Arabia. PLoS One. 2018;13(8):e0201613. doi:10.1371/journal.pone.0201613
40. Bi R, Kong Z, Qian H, et al. High Prevalence of blaNDM variants among carbapenem-resistant Escherichia coli in northern Jiangsu province, China. Front Microbiol. 2018;9:2704. doi:10.3389/fmicb.2018.02704
41. Aung MS, San N, Maw WW, et al. Prevalence of extended-spectrum beta-lactamase and carbapenemase genes in clinical isolates of Escherichia coli in Myanmar: dominance of blaNDM-5 and emergence of blaOXA-181. Microb Drug Resist. 2018;24(9):1333–1344. doi:10.1089/mdr.2017.0387
42. Baek JY, Cho SY, Kim SH, et al. Plasmid analysis of Escherichia coli isolates from south Korea co-producing NDM-5 and OXA-181 carbapenemases. Plasmid. 2019;104:102417. doi:10.1016/j.plasmid.2019.102417
43. Hong JS, Song W, Park HM, et al. First Detection of New Delhi Metallo-β-Lactamase-5-Producing Escherichia coli from Companion Animals in Korea. Microb Drug Resist. 2019;25(3):344–349. doi: 10.1089/mdr.2018.0237
44. Park Y, Choi Q, Kwon GC, et al. Emergence and transmission of New Delhi metallo-beta-lactamase-5-producing Escherichia coli Sequence Type 361 in a Tertiary Hospital in South Korea. J Clin Lab Anal. 2020;34(2):e23041. doi:10.1002/jcla.23041
45. Pitart C, Sole M, Roca I, et al. Molecular characterization of blaNDM-5 carried on an IncFII plasmid in an Escherichia coli isolate from a nontraveler patient in Spain. Antimicrob Agents Chemother. 2015;59(1):659–662. doi:10.1128/AAC.04040-14
46. Sugawara Y, Akeda Y, Hagiya H, et al. Spreading patterns of NDM-producing Enterobacteriaceae in clinical and environmental settings in Yangon, Myanmar. Antimicrob Agents Chemother. 2019;63(3):e01924-18. doi:10.1128/AAC.01924-18
47. Zhang F, Xie L, Wang X, et al. Further spread of blaNDM-5 in Enterobacteriaceae via IncX3 plasmids in Shanghai, China. Front Microbiol. 2016;7:424. doi:10.3389/fmicb.2016.00424
48. Ouchar Mahamat O, Lounnas M, Hide M, et al. Spread of NDM-5 and OXA-181 carbapenemase-producing Escherichia coli in Chad. Antimicrob Agents Chemother. 2019;63(11):e00646-19. doi:10.1128/AAC.00646-19
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.