Back to Journals » International Medical Case Reports Journal » Volume 18
Eltrombopag for Refractory Immune Thrombocytopenia in a Patient with Chronic Lymphocytic Leukemia: A Case Report
Authors Alsalman M ![]()
Received 20 July 2025
Accepted for publication 7 October 2025
Published 9 October 2025 Volume 2025:18 Pages 1291—1294
DOI https://doi.org/10.2147/IMCRJ.S555045
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Mortadah Alsalman
Department of Medicine, College of Medicine, King Faisal University, Alahsa, Saudi Arabia
Correspondence: Mortadah Alsalman, Department of Medicine, College of Medicine, King Faisal University, Po Box Alandalus 4842, Alahasa, 36341, Saudi Arabia, Tel +966506914993, Email [email protected]
Introduction: We report a case of chronic lymphocytic leukemia associated immune thrombocytopenia (CLL-associated ITP) with suboptimal response to steroid responding to second line agent.
Case Presentation: A 68-year-old female patient known to have diabetes mellitus and chronic lymphocytic leukemia (CLL) presented with spontaneous bruising on her body and around her right eye. Initial laboratory investigations reveal hemoglobin level of 10.6 g/dL, platelet count of 11 × 109/L, white blood cell count of 50.0 × 109/L with negative direct and indirect Coombs tests were negative. The patient has a suboptimal response and rapid platelet declines once prednisone is tapered off. Consequently, Eltrombopag was introduced at a daily dosage of 50 mg, resulting in a rapid and sustained response over two years, reaching a platelet count of 282 × 109/L without requiring rescue treatment. Notably, steroids were tapered within the first three weeks of Eltrombopag administration, and aspirin was resumed once the platelet count reached 50 × 109/L.
Conclusion: Eltrombopag represents an effective and safe treatment alternative for patients with CLL-associated ITP, particularly those diagnosed with diabetes mellitus. However, the potential risks of iron deficiency and Eltrombopag’s food interactions prior to initiating therapy, during dose escalations, or when transitioning to alternative treatments are important considerations. Future studies with large number sample size along with identification of cytogenetic and molecular abnormalities are required to identify patient populations that may respond favorably to Eltrombopag without necessitating rescue therapies, chemotherapy, immunotherapy or CLL directed therapy.
Keywords: chronic lymphocytic leukemia, immune thrombocytopenia, Eltrombopag
Introduction
Chronic lymphocytic leukemia (CLL) is a slowly progressive hematologic malignancy characterized by the accumulation of CD5+ mature B cells in the peripheral blood, bone marrow, and lymphoid organs. The clinical presentations of CLL exhibit considerable heterogeneity, ranging from an indolent course, in which many patients remain asymptomatic with a normal life expectancy, to aggressive forms of the disease that may lead to progressive cytopenia or B symptoms, including unintentional weight loss, severe night sweats, and fever.1,2 A notable characteristic of CLL is the presence of immune disturbances, which set it apart from other chronic lymphoproliferative disorders. Among the various manifestations, autoimmune cytopenias represent a significant proportion of the clinical presentations, with autoimmune hemolytic anemia being the most prevalent, followed by immune thrombocytopenia (ITP) with an incident rate of 7% and 5%, respectively.3,4 This report outlines a case of steroid-refractory immune thrombocytopenia occurring in the context of chronic lymphocytic leukemia, highlighting the complexities associated with managing this condition.
Case Presentations
A 68-year-old female patient, with a medical history of type II diabetes mellitus for around ten years on Lingliptin complicated by advanced retinopathy and blindness. She was diagnosed with chronic lymphocytic leukemia approximately four years before this presentation. She had been managed through a watchful waiting approach. The patient presented to the emergency department with spontaneous bruising on her body and around her right eye, without any bleeding from other orifices or evidence of neurological symptoms, such as headaches, limb weakness, or paresthesia. Physical examination revealed bruising localized to the right eye and body, with no signs of lymphadenopathy or organomegaly.
Initial laboratory investigations indicated the following results: hemoglobin level of 10.6 g/dL, platelet count of 11 × 109/L, white blood cell count of 50.0 × 109/L, neutrophil percentage of 13%, lymphocyte percentage of 81%, mean corpuscular volume (MCV) of 77 fL, creatinine of 0.68 mg/dL, total bilirubin of 0.55 mg/dL, LDH 281 U/L, ALT 15 U/L, AST 17 U/L, ferritin of 13 µg/L, HbA1C 5.8%, Beta 2 microglobulin 11.2 ng/mL, CRP 0.5 mg/L and both direct and indirect Coombs tests were negative. An echocardiogram demonstrated a reduced ejection fraction of 45%. The patient was initiated on prednisone at a dosage of 1 mg/kg, and aspirin was temporarily discontinued pending platelet recovery. Although her platelet count improved partially to 55 × 109/L within two weeks, it subsequently declined during the tapering of steroids. Consequently, thrombopoietin receptor agonist Eltrombopag was introduced at a daily dosage of 50 mg, resulting in a rapid and sustained response over two years without requiring rescue treatment and both liver and kidney functions remain unchanged (Figure 1). Notably, steroids were tapered within the first three weeks of Eltrombopag administration, and aspirin was resumed once the platelet count reached 50 × 109/L. It is worth noting that her platelet count dropped once, but she recovered gradually, and this decline was attributed to Eltrombopag interaction with calcium-containing foods. Furthermore, during her treatment course, the patient experienced a small lacunar infarct; however, Eltrombopag was not discontinued, as it was determined that the stroke was attributable to her multiple underlying risk factors rather than the use of the thrombopoietin receptor agonist. Additionally, the patient was commenced on oral iron replacement after excluding autoimmune hemolytic anemia; however, she expressed reluctance to proceed with bidirectional endoscopy to investigate iron deficiency anemia.
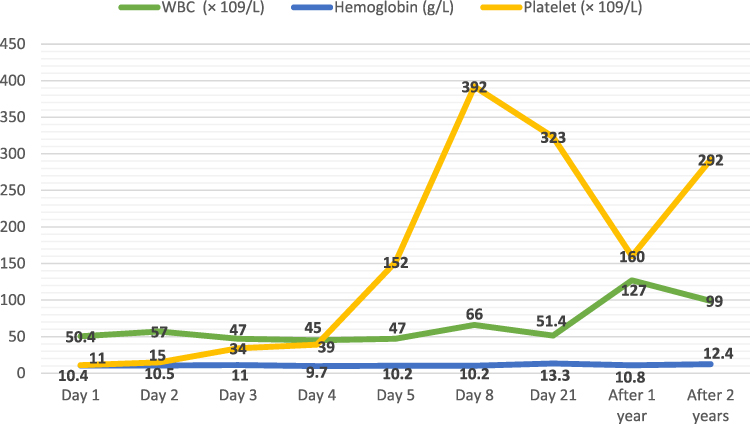 |
Figure 1 Trends of Platelet Count Post-Eltrombopag. |
Discussion
Platelets exhibit diverse interactions with their surrounding environment and play essential roles in the hemostatic system. In addition to these primary functions, they are also significantly involved in angiogenesis, inflammation, and immune responses.5,6 Immune thrombocytopenia affects approximately 5% of patients with chronic lymphocytic leukemia (CLL) and has been linked to poorer survival outcomes and diminished responses to steroid compared to those with adult immune thrombocytopenic purpura (ITP). Historically, steroid is the a main stay of treatment of CLL associated ITP with a 50% response rate.7 However, refractoriness to steroid or relapse after tapering off in the context of CLL as in our report represents a notable clinical challenge and may indicate disease progression, thereby necessitating the initiation of chemotherapy or immunotherapy.6,8
Eltrombopag is an orally administered, non-peptide thrombopoietin receptor agonist that initiates thrombopoietin signaling and stimulates the production of normally functioning platelets. It is approved as a second-line treatment for refractory or relapsed immune thrombocytopenic purpura (ITP); however, its role in the context of chronic lymphocytic leukemia (CLL) remains a topic of debate.9,10 Previous studies have shown that individuals with steroid-refractory CLL-associated ITP may also exhibit refractoriness to thrombopoietin receptor agonists. Consequently, splenectomy should be considered before the initiation of chemotherapy or immunotherapy.11,12 Both splenectomy and Rituximab are considered effective treatment in steroid refractory ITP with an estimated response rate of 80%, however both could increase patient risk of infection in the context of old age and diabetes mellitus in addition to CLL comorbidity.7,13 On the other hand, several reports indicate that CLL-associated ITP may respond similarly to Eltrombopag as primary thrombocytopenia, with a median dose of 50 mg/day and a median duration of treatment eighteen weeks.9,14 Of note, previous report indicated that 5% of the patients receiving Eltrombopag developed thromboembolic events with more predilection toward venous thromboembolism as compared to arterial ones.13 In the study presented herein, we observed significant improvement and normalization of platelet counts following the administration of Eltrombopag with the same dose. Notably, this response was sustained for over two years without requiring rescue treatment, chemotherapy, or immunotherapy unlike previous reports.
This report underscores that refractory or relapsed immune thrombocytopenic purpura in the context of chronic lymphocytic leukemia does not necessarily signify disease progression, nor does it automatically necessitate a transition to chemotherapy or immunotherapy for the management of CLL. Furthermore, Eltrombopag emerges as an effective and safe second-line treatment option for this patient population. In instances of worsening thrombocytopenia or diminished response while using Eltrombopag, it is imperative to evaluate potential drug-drug and food interactions before considering dose escalation or determining treatment failure. Similarly, development of anemia during treatment with Eltrombopag may not unequivocally indicate bone marrow failure or the presence of autoimmune hemolytic anemia; instead, it may be attributable to iron deficiency, as Eltrombopag acts as a potent iron chelator that mobilizes iron and ferritin. Conversely, Eltrombopag has the potential to restore insulin production to clinically significant levels, rendering it a viable alternative for patients with diabetes mellitus experiencing CLL-associated ITP, as opposed to conventional steroid therapy. Additionally, this report highlights the importance of sparing patient from steroid side effect particularly increase risk of infections and worsening blood glucose.15,16 Nevertheless, this report is limited by the absence of cytogenetic and molecular data, which is typically should be assessed upon initiation of the primary treatment for CLL. Such information may prove valuable in CLL-associated ITP, as it could assist in identifying individuals with a higher likelihood of responding favorably to thrombopoietin receptor agonists.
In conclusion, Eltrombopag represents an effective and safe treatment alternative for CLL-associated ITP, particularly in those diagnosed with diabetes mellitus. This medication aids in restoring insulin production, thereby minimizing the requirement for steroid treatment. However, it is crucial to educate patients regarding the potential risks of iron deficiency, as well as food interactions, before initiating therapy, during dose escalations, or when transitioning to alternative treatments. Future studies with large number sample size along with identification of cytogenetic and molecular abnormalities are required to identify patient populations that may respond favorably to Eltrombopag without necessitating rescue therapies, chemotherapy, or immunotherapy.
Ethical Approval
Institutional approval is not required for publication so informed written consent for using patient information and case report publication was obtained from the patient as long as identifying data are anonymous.
Funding
This case report received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The author declares no conflicts of interest in this work.
References
1. Borges FC, Ramos A, Lourenço A, da Silva MG, Miranda A. Detailing the epidemiological and clinical characteristics of chronic lymphocytic leukaemia in Portugal—results from a population-based cancer registry cohort study. PLoS One. 2021;16(10):1–14.
2. Eichhorst B, Robak T, Montserrat E, et al. Chronic lymphocytic leukaemia: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2021;32(1):23–33. doi:10.1016/j.annonc.2020.09.019
3. De Back TR, Kater AP, Tonino SH. Autoimmune cytopenias in chronic lymphocytic leukemia: a concise review and treatment recommendations. Expert Rev Hematol. 2018;11(8):613–624. doi:10.1080/17474086.2018.1489720
4. Hodgson K, Ferrer G, Montserrat E, Moreno C. Chronic lymphocytic leukemia and autoimmunity: a systematic review. Haematologica. 2011;96(5):752–761. doi:10.3324/haematol.2010.036152
5. Sonmez O, Sonmez M. Role of platelets in immune system and inflammation. Porto Biomed J. 2017;2(6):311–314. doi:10.1016/j.pbj.2017.05.005
6. Visco C, Ruggeri M, Evangelista ML, et al. Impact of immune thrombocytopenia on the clinical course of chronic lymphocytic leukemia. Blood. 2008;111(3):1110–1116. doi:10.1182/blood-2007-09-111492
7. Fattizzo B, Barcellini W, Gisondi P, Bellinato F, Girolomoni G. Autoimmune cytopenias in chronic lymphocytic leukemia: focus on molecular aspects. Front Oncol. 2020;9:1–14. doi:10.3389/fonc.2019.01435
8. Woo T, Carter M, Follows G, Patten PEM. Case report: successful treatment of refractory immune thrombocytopenia in chronic lymphocytic leukaemia with venetoclax monotherapy. Front Oncol. 2023;13:1–5. doi:10.3389/fonc.2023.1260003
9. Visco C, Rodeghiero F, Romano A, et al. Eltrombopag for immune thrombocytopenia secondary to chronic lymphoproliferative disorders: a Phase 2 multicenter study. Blood. 2019;134(20):1708–1711. doi:10.1182/blood.2019001617
10. Wong RSM, Saleh MN, Khelif A, et al. Safety and efficacy of long-term treatment of chronic/persistent ITP with eltrombopag: final results of the EXTEND study. Blood. 2017;130(23):2527–2536. doi:10.1182/blood-2017-04-748707
11. Jolliffe E, Romeril K. Eltrombopag for resistant immune thrombocytopenia secondary to chronic lymphocytic leukaemia. Intern Med J. 2014;44(7):697–699. doi:10.1111/imj.12468
12. Koehrer S, Keating MJ, Wierda WG. Eltrombopag, a second-generation thrombopoietin receptor agonist, for chronic lymphocytic leukemia-associated ITP. Leukemia. 2010;24(5):1096–1098. doi:10.1038/leu.2010.45
13. Ghumman GM, Fatima H, Singh G, Khalid T, Ayoubi M. Risk of thromboembolism with eltrombopag: a case report of deep vein thrombosis and bilateral pulmonary embolism. Cureus. 2023;15(1):12–15.
14. Paul S, Jain N, Ferrajoli A, et al. A Phase II trial of eltrombopag for patients with chronic lymphocytic leukaemia (CLL) and thrombocytopenia. Br J Haematol. 2019;185(3):606–608. doi:10.1111/bjh.15581
15. Vlachodimitropoulou E, Chen YL, Garbowski M, et al. Eltrombopag: a powerful chelator of cellular or extracellular iron(III) alone or combined with a second chelator. Blood. 2017;130(17):1923–1933. doi:10.1182/blood-2016-10-740241
16. Lambert MP, Witmer CM, Kwiatkowski JL. Therapy induced iron deficiency in children treated with eltrombopag for immune thrombocytopenia. Am J Hematol. 2017;92. doi:10.1002/ajh.24705
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.