Back to Journals » Clinical Ophthalmology » Volume 19
Ellipsoid Zone Hyporeflectivity as an Early Sign of Non-Reversible Hydroxychloroquine Retinopathy: A Case Series
Authors Groothoff JD, Browning DJ ![]()
Received 19 July 2025
Accepted for publication 4 November 2025
Published 11 November 2025 Volume 2025:19 Pages 4177—4191
DOI https://doi.org/10.2147/OPTH.S554892
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yousef Fouad
Jonathan D Groothoff,1 David J Browning1,2
1Wake Forest University School of Medicine, Winston-Salem, NC, USA; 2Department of Ophthalmology, Wake Forest University School of Medicine, Winston-Salem, NC, USA
Correspondence: David J Browning, Department of Ophthalmology, Wake Forest University School of Medicine, 1 Medical Center Boulevard, Winston-Salem, North Carolina, 27157, USA, Tel +1 336-416-1199, Fax +1 336-716-9334, Email [email protected]
Introduction: The purpose of this study was to evaluate the progression of hydroxychloroquine (HCQ) retinopathy following parafoveal loss of the ellipsoid zone (EZ) without retinal pigment epithelium damage (RPE).
Methods: This was a single-center retrospective case series of patients with hydroxychloroquine retinopathy who presented between 2012 and 2023 and in whom the drug was stopped prior to damage of the RPE. Patient imaging from the time of HCQ discontinuation to the most recent follow up appointment was reviewed to assess for retinopathy progression, and spectral domain optical coherence tomography (SD-OCT) images were analyzed using ImageJ2 to quantify ellipsoid zone damage.
Results: Five patients met the criteria for inclusion in this study. All patients were female, with a mean age of 69.5 ± 12.2 years. Patients had been taking HCQ for 18.2 years on average (range: 5– 32 years). 40% of patients were overdosed according to real weight guidelines and 60% by ideal weight guidelines. All patients demonstrated worsening of retinopathy following drug discontinuation. The length of parafoveal zones of EZ hyporeflectivity on SD-OCT increased by an average of 26.8 ± 8.6% in right eyes and 22.5 ± 15.0% in left eyes over an average follow-up period of 31.4 months (range 8– 71 months).
Conclusion: Progression of HCQ retinopathy can occur even when HCQ is discontinued before RPE damage. Ophthalmologists should be aware of the risks associated with HCQ use following damage to the EZ. The acknowledged threshold at which irreversible progression of retinopathy is predicted despite cessation of the drug may need to be reconsidered and shifted earlier than RPE loss.
Plain Language Summary: Parafoveal hyporeflectivity of the ellipsoid zone signals irreversible progression of hydroxychloroquine retinopathy even in the absence of retinal pigment epithelium loss.
Keywords: hydroxychloroquine, hydroxychloroquine retinopathy, ellipsoid zone, retinal pigmented epithelium, spectral domain OCT
Introduction
Hydroxychloroquine (HCQ) is a disease-modifying antirheumatic drug widely used for the treatment of autoimmune diseases such as rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE).1,2 In the United States, RA affects an estimated 1.3 million individuals, while the overall prevalence of SLE is estimated at 72.8 per 100,000, or 204,295 individuals.3,4 Over half of patients with RA and nearly two-thirds of patients with SLE start HCQ within one year of diagnosis.5 HCQ is typically well-tolerated; however, irreversible retinal toxicity is a known adverse effect that affects an estimated 1.5 to 2% of lifetime users.6,7 Prescribed dosages of HCQ have steadily decreased in recent decades due to this risk.8 Nevertheless, HCQ retinopathy remains problematic, as an estimated 30% of patients continue to receive higher than recommended doses.9
Risk of Toxicity
The toxicity of HCQ is believed to be due to the drug’s disruptive effects on lysosomal autophagy. Lysosomes exposed to HCQ may accumulate dysfunctional proteins that prevent breakdown of waste products such as lipofuscin.10–12 The accumulation of these materials prevents lysosomes from binding autophagic vacuoles and disrupts retinal recycling.11
Previous studies have reported numerous risk factors associated with the development of HCQ retinopathy. HCQ is primarily cleared by the kidneys; therefore, patients with renal disease are at a higher risk of HCQ buildup in the plasma.10 Older individuals, female patients, and those with concurrent tamoxifen use are also more likely to develop toxicity.13 Additional risk factors include a daily dose greater than 5.0 mg/kg/day by real body weight (RBW), 6.5 mg/kg/day by ideal body weight (IBW), a cumulative dose greater than 1000 mg, and long term use greater than five years.1,2
Characteristics of Hydroxychloroquine Retinopathy
Advanced HCQ retinopathy manifests as a visible “bull’s eye” maculopathy on fundus photography. However, this is a late finding associated with irreversible and progressive retinal damage and visual loss.14,15 On 10–2 visual fields (10–2 VF), HCQ toxicity presents as a paracentral scotoma.10,16 Spectral domain optical coherence tomography (SD-OCT) typically shows parafoveal thinning of the outer nuclear layer and decreased reflectivity followed by focal loss of the ellipsoid zone (EZ), along with disruption of the retinal pigment epithelium (RPE).2,16,17 Notably, the fovea is resilient against toxicity, evidenced by an intact foveal external limiting membrane (ELM) and photoreceptor layer until the last stages of retinopathy.18
Screening
For patients without major risk factors for HCQ toxicity, current screening guidelines recommend a baseline fundus examination to evaluate for preexisting retinopathy, followed by annual screening beginning after five years of continuous use.1 Preferred screening techniques include 10–2 VF, SD-OCT, fundus autofluorescence (FAF), and multifocal electroretinogram (ERG). Some authors recommend the use of 30–2 visual fields (30–2 VF) in Asian patients due to its greater sensitivity in detecting pericentral retinopathy compared to 10–2 VF.19,20 Of these techniques, SD-OCT is the most reproducible.10,21,22
Purpose
Because HCQ retinopathy can result in irreversible and progressive retinal damage despite drug cessation, early discontinuation of the drug is essential to preventing significant functional deficits. Disagreement exists regarding the threshold at which damage to the retina becomes irreversible. The presence of RPE loss is a well-recognized marker of HCQ toxicity that some identify as the point of no return.23,24 However, other studies suggest that this threshold may be too advanced.18,25 To date, limited research has explored whether damage to more superficial retinal layers portends irreversible retinal damage. The purpose of this study was to evaluate the progression of retinopathy in eyes in which HCQ toxicity was diagnosed and the drug was stopped prior to RPE loss. It was hypothesized that eyes would experience worsening of retinopathy despite the patient no longer taking the drug. Special attention was given to the ellipsoid zone, a layer of the inner segment of photoreceptors composed primarily of mitochondria. This layer is believed to determine photoreceptor integrity and appears as a hyperfluorescent line on SD-OCT.26 It was hypothesized that damage to the EZ in the absence of RPE loss would still result in irreversible progression of HCQ toxicity.
Methods
This was a retrospective case series of all eyes diagnosed with HCQ retinopathy between 2012 and 2023 at a large academic medical center in North Carolina, United States. Institutional Review Board (IRB) approval was obtained prior to data collection (protocol number 00115910), and the research process was conducted in accordance with the tenets put forward in the Declaration of Helsinki.
Patient Recruitment
Patients with HCQ retinopathy were identified through an I2B2 query of ICD-9 and ICD-10 codes. Eyes were included once HCQ toxicity was confirmed through a manual review of patient charts and ancillary testing, including 10–2 VF, SD-OCT, and FAF. Inclusion in this study required HCQ discontinuation, SD-OCT, VF, and FAF imaging available at the time of drug cessation and follow up imaging available from a minimum of two visits after drug cessation. Importantly, an intact RPE at the time HCQ was stopped was necessary for inclusion. Eyes were excluded if they possessed a prior diagnosis of retinopathy, exhibited evidence of RPE damage before HCQ cessation, lacked baseline imaging, or were lost to follow up.
Data Collection
Demographic and treatment characteristics were collected from patient charts within the electronic medical record. Baseline patient data included age, self-reported race, sex, height, RBW, IBW, kidney disease, liver disease, tamoxifen use, date of HCQ initiation, date of HCQ cessation, and daily HCQ dose. IBW was calculated using the National Heart, Lung, and Blood Institute (NHLBI) table and its equivalent algorithm.27 Patient dosing was compared with the 2016 American Academy of Ophthalmology (AAO) guidelines, which recommend a daily dose less than 5.0 mg/kg/day based on RBW.1
Image Analysis
Patient images were reviewed from the time of HCQ cessation until the most recent follow up appointment. Visual field testing was recorded using a Zeiss Humphrey Field Analyzer (Zeiss Meditec, Dublin, California). Four patients received 10–2 VF while one patient received 30–2 and 24–2 VF. Early retinopathy was defined as fragments of a ring scotoma while advanced retinopathy was defined as a complete ring scotoma.
FAF imaging was obtained with an Optos widefield scanning microscope (Optos, Dunfermline, United Kingdom). Early HCQ retinopathy was defined as parafoveal hyperfluorescence without parafoveal hypofluorescence, while advanced retinopathy was defined as both parafoveal hyperfluorescence and focal hypofluorescence, indicating RPE loss.28,29 Identification of the characteristic “bull’s eye maculopathy” was also considered to be indicative of severe progression. Progression was assessed through qualitative comparison of images over time, with judgments made only on tests in which the same FAF imaging camera was used.29
SD-OCT images were collected with Zeiss (Zeiss Meditec, Dublin, California) or Heidelberg (Heidelberg Engineering, Heidelberg, Germany) instruments. Early retinopathy on SD-OCT was defined as an intact RPE with decreased reflectivity of the parafoveal ELM, EZ, or interdigitation zone, or an intact RPE with a normal ELM, EZ, and interdigitation zone but three to five paracentral Early Treatment Diabetic Retinopathy Study (ETDRS) sectors falling outside 99% of norms.29 Advanced retinopathy was defined as parafoveal ELM, EZ, and interdigitation zone discontinuity and parafoveal RPE loss, indicated by choroidal transmission of the illuminating beam.29 HCQ discontinuation in the setting of RPE damage has already been associated with disease progression.2,23 In contrast, this study identified eyes in which the drug was stopped earlier than this point.
Retinopathy progression on SD-OCT was quantified using ImageJ2.30,31 The Java-based software has good inter-rater reliability when analyzing OCT images and has been employed previously to evaluate OCTs of human patients and mouse models.25,32,33 Using this tool, progression of HCQ toxicity was quantified by the relative increase in length of EZ hyporeflectivity; a greater percent change indicated worsening of disease. As an intact RPE was a prerequisite for inclusion in this study, evidence of choroidal transmission on SD-OCT also signaled disease progression.
Results
An initial I2B2 query yielded 59 patients with ocular toxicity due to HCQ. After manual review, 54 patients were excluded due to insufficient imaging (n = 33), lack of follow up (n = 2), other comorbid retinopathy at baseline (n = 6), or pre-existing RPE damage at the time of HCQ discontinuation (n = 13). This left 5 patients who met the criteria for inclusion.
Patient Demographics
Table 1 displays the characteristics of patients included in this study. All patients were female, with a mean age of 69.5 ± 12.2 years (range: 50–84 years). Four patients were White, and one patient was Black. SLE was the most common reason for HCQ prescription (n = 3). On average, patients had taken HCQ for 18.2 ± 14.1 years (range: 5–32 years). Four patients took 400 mg/day and one patient took 200 mg/day. Mean daily dose by RBW was 5.0 ± 1.0 mg/kg/day (range: 3.8–6.1 mg/kg/day). Two patients were overdosed according to the revised 2016 AAO guidelines, which use RBW dosing. If adjusted for IBW, the mean daily dose was 5.8 ± 1.5 mg/kg/day (range: 3.1–6.7 mg/kg/day), with three patients overdosed by IBW guidelines and receiving a daily dose greater than 6.5 mg/kg/day.34 Three patients were diagnosed with kidney disease while taking HCQ; no patients had liver disease and no patients were taking tamoxifen. Mean follow up after HCQ cessation was 31.4 months (range: 8–72 months) Table 1.
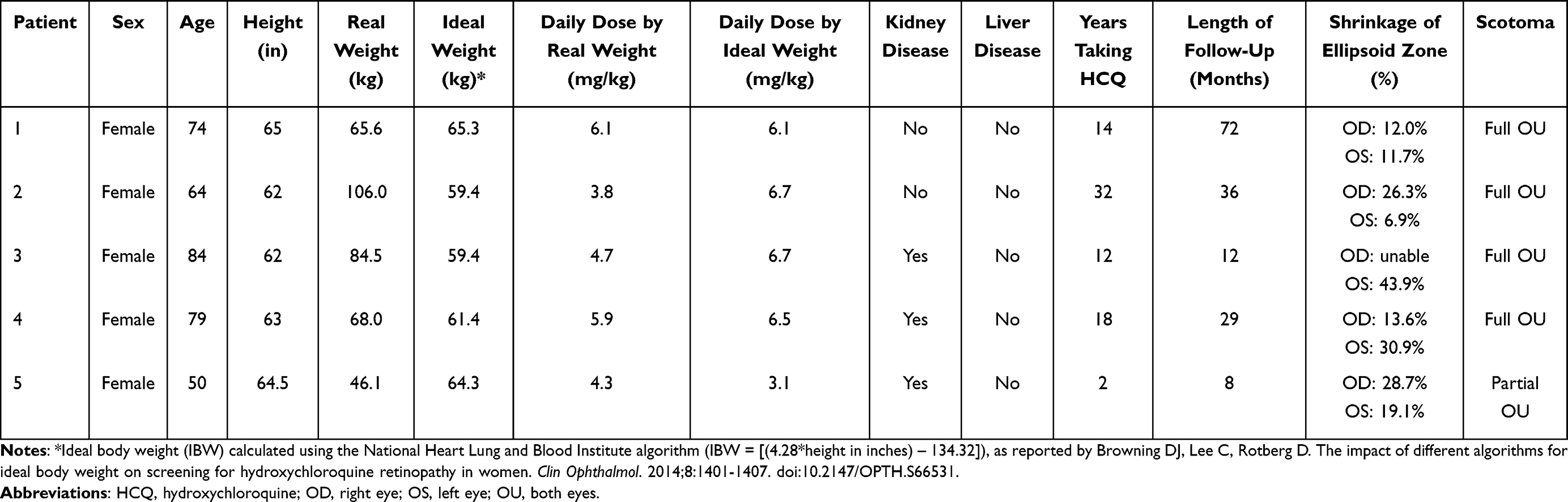 |
Table 1 Patient Demographic and Treatment Characteristics |
Patient Imaging
All patients underwent visual fields, SD-OCT, and FAF imaging. All patients had visual fields and SD-OCT abnormalities characteristic of HCQ retinopathy. Three of five patients had FAF imaging abnormalities consistent with HCQ retinopathy at the time of drug cessation. Visual fields revealed scotoma progression in all eyes, with eight eyes developing full scotomas and two eyes developing partial scotomas. During the follow up period, SD-OCT showed mean increases in EZ hyporeflectivity of 20.2 ± 8.6% in the right eye and 22.5 ± 15.0% in the left eye. HCQ retinopathy progression on FAF was unable to be assessed in all patients due to insufficient imaging.
Case Reports
Case 1
Patient 1 was a 74-year-old female who had been taking HCQ for 18 years to manage SLE and RA. She was 65 inches tall and weighed 65.6 kg. Her daily HCQ dose and daily dose based on RBW were 400 mg/day and 6.1 mg/kg/day, respectively. Daily dose based on IBW was also 6.1 mg/kg/day. She had no history of kidney or liver disease.
The patient’s baseline visual acuity after correction was 20/30 in the right eye and 20/20 in the left eye. Figure 1 displays ancillary testing at the time HCQ was stopped. HCQ retinopathy was identified by the presence of a full ring scotoma in both eyes on 10–2 VF and a bull’s eye pattern with a hyperfluorescent ring on FAF. SD-OCT revealed EZ loss without choroidal transmission of the illuminating light, indicating an intact RPE.
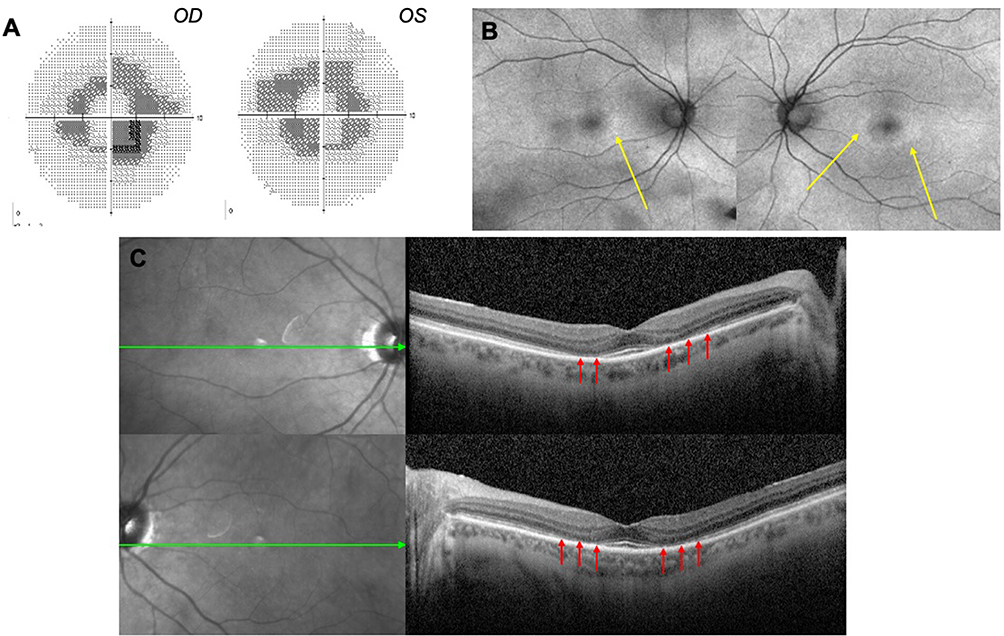 |
Figure 1 Ancillary testing for Case 1 at the time of HCQ discontinuation. (A) Bilateral complete ring scotomas consistent with advanced retinopathy were present on 10–2 visual fields, worse in the right eye. (B) Annular hyperfluorescent lesions (yellow arrows) were visible in both eyes, left worse than right, on widefield fundus autofluorescence imaging. (C) Parafoveal hyporeflectivity of the EZ (red arrows) with outer nuclear layer thinning was present in both eyes on spectral domain optical coherence tomography, with faint parafoveal hypofluorescent changes on near infrared reflectance imaging. The green arrows on the near infrared reflectance images indicate the position of the associated optical coherence tomography scans. |
Early signs of RPE damage were observed 12 months after HCQ cessation. Figure 2 illustrates the progression of RPE damage in the left eye on SD-OCT and focal loss on near infrared reflectance (NIR) imaging. The right eye similarly showed signs of HCQ retinopathy progression during the follow up period (Figure 3).
 |
Figure 2 Spectral domain optical coherence tomography of the left eye at 1, 2, and 5 years after HCQ discontinuation for Case 1. Parafoveal hyporeflectivity of the EZ (red arrows) increased in length over the follow up period, signifying further damage to the outer retina. Increased choroidal light beam transmission (light blue arrows) – indicative of retinal pigment epithelium damage – appeared 1 year after HCQ was discontinued. Subsequent progression of RPE damage was evident at 3 and 5 years after HCQ cessation. Near infrared reflectance imaging also demonstrated focal loss (purple arrows) that progressed after the drug was discontinued. |
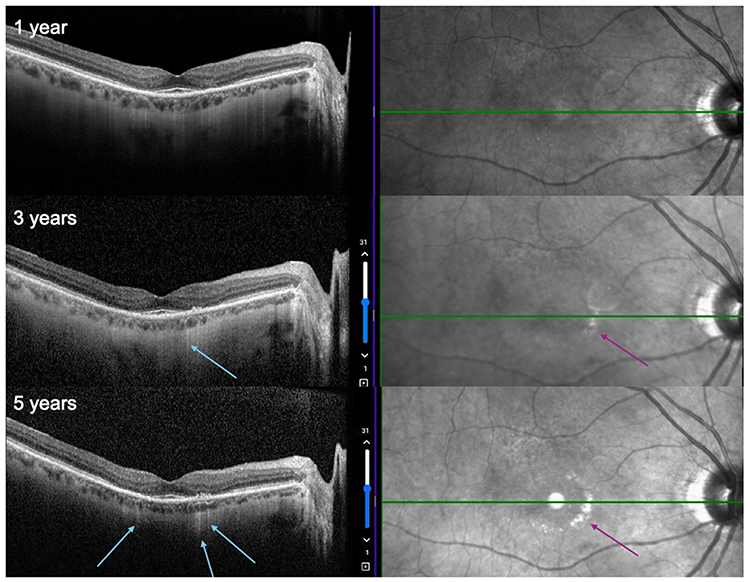 |
Figure 3 Spectral domain optical coherence tomography of the right eye at 1, 3, and 5 years after HCQ discontinuation for Case 1. Like the left eye (Figure 2), spectral domain optical coherence tomography showed lengthening of parafoveal ellipsoid zone hyporeflectivity with increased transmission of the illuminating light beam into the choroid (light blue arrows), indicating progressive damage to the outer retina. Despite HCQ cessation, near infrared reflectance imaging demonstrated further progression of focal loss (purple arrows), worse nasally. |
Final ancillary testing is displayed in Figure 4. Over 72 months, the length of EZ hyporeflectivity increased by 12.0% in the right eye and 11.7% in the left eye. Focal loss of the RPE was present in addition to loss of the outer nuclear layer, in contrast to baseline SD-OCT that showed an intact RPE. NIR imaging displayed significant hyperfluorescent changes in both eyes. Visual fields testing also showed more advanced retinopathy bilaterally. FAF of both eyes revealed annular hyperfluorescent lesions and new hypofluorescent lesions. At the patient’s most recent appointment, visual acuity after correction was 20/25 and 20/25 in the right and left eyes, respectively.
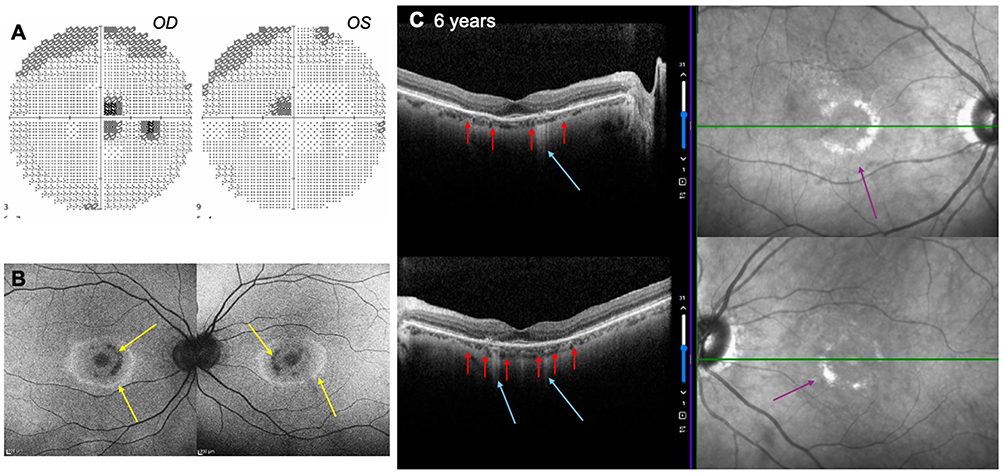 |
Figure 4 Ancillary testing for Case 1 6 years after HCQ was discontinued. These images should be compared to those in Figure 1. (A) 30–2 visual fields demonstrated bilateral advanced retinopathy worse than that seen on 10–2 visual fields 6 years prior. (B) Fundus autofluorescence showed extensive annular hyperfluorescent lesions with new hypoautofluorescent lesions (yellow arrows) in both eyes. (C) Spectral domain optical coherence tomography (SD-OCT) and near infrared reflectance (NIR) imaging showed more severe SD-OCT damage with focal loss of retinal pigment epithelium, signified by transmission of the illuminating beam into the choroid (blue arrows) and focal collapse of the outer nuclear layer and ellipsoid zone loss (red arrows). NIR displayed significant bilateral parafoveal hyperfluorescent changes (purple arrows) worse nasally that were more apparent than at the time of HCQ cessation. |
Case 2
Patient 2 was a 64-year-old female who had been taking HCQ for 32 years for management of SLE. She was 62 inches tall and weighed 106 kg, with a daily HCQ dose of 400 mg/day, corresponding to a 3.8 mg/kg/day dose based on RBW. Daily dose based on IBW was 6.7 mg/kg/day. She had no history of kidney or liver disease.
The patient’s visual acuity after correction was 20/25 in the right eye and 20/45 in the left eye. Early signs of HCQ toxicity were present three years before HCQ cessation, evidenced by a total scotoma bilaterally on 10–2 VF, despite normal retinal imaging (Figure 5A). However, the 10–2 VF was misinterpreted as normal at that time, and by drug cessation severe parafoveal deficits were visible in both eyes (Figure 5B). During the three years leading up to HCQ discontinuation, NIR imaging demonstrated increased hyperreflectivity, suggestive of retinopathy progression (Figure 6). Thinning of the parafoveal outer nuclear layer and decreased reflectivity of the EZ with an intact RPE were observed on SD-OCT three years after the first signs of toxicity appeared on 10–2 VF (Figure 7), prompting HCQ discontinuation. 10–2 VF at this time showed more severe parafoveal deficits in both eyes (Figure 5B).
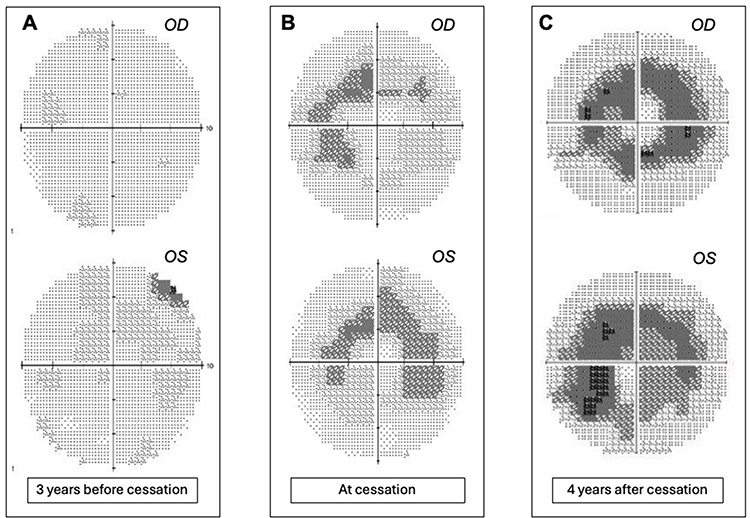 |
Figure 5 Progression of visual field changes in Case 2. (A) Four quadrant, unconnected paracentral scotomata were present on 10–2 visual fields (10–2 VF) in both eyes 3 years prior to drug cessation, but the testing was mistakenly classified as normal. (B) At the time of HCQ cessation, 10–2 VF demonstrated worse bilateral paracentral scotomata compared to panel A. (C) At last follow up, the central scotomas demonstrated further progression, despite the drug having been discontinued 4 years prior. |
 |
Figure 6 Near infrared reflectance (NIR) imaging for Case 2 before HCQ cessation. NIR demonstrated increased hyperreflectivity (purple arrows) in the 3 years leading up to HCQ discontinuation. |
 |
Figure 7 Spectral domain optical coherence tomography at the time HCQ was discontinued in Case 2. Parafoveal hyporeflectivity of the ellipsoid zone can be observed in both eyes (red arrows). There is no evidence of choroidal transmission of the illuminating beam in either eye, indicating that the RPE was intact at the time of HCQ cessation. The green arrows on the near infrared reflectance images indicate the position of the associated optical coherence tomography scans. |
The patient was monitored for 36 months after stopping HCQ. During this period, the length of the zone of parafoveal EZ hyporeflectivity increased by 26.3% in the right eye and 6.9% in the left eye. Final SD-OCT images are displayed in Figure 8. No choroidal transmission of light rays was observed, suggesting that the RPE remained intact in both eyes, despite ongoing damage to the EZ. Additionally, final 10–2 VF revealed worsening total and pattern deviations in both eyes compared to when HCQ was discontinued (Figure 5C). At the end of the follow up period, the patient’s visual acuity after correction was 20/40 in the right eye and 20/30 in the left eye.
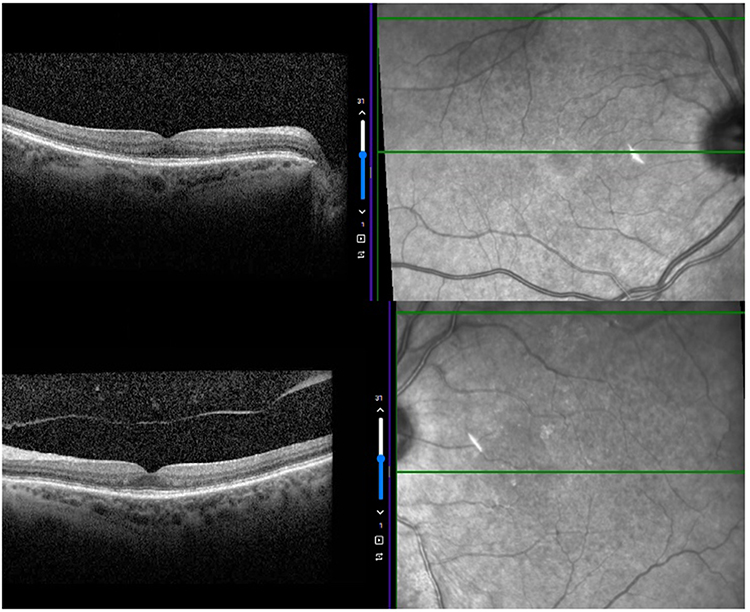 |
Figure 8 Final spectral domain optical coherence tomography images for Case 2. The length of parafoveal ellipsoid zone hyporeflectivity increased in both eyes compared to the state at drug cessation. At the patient’s most recent appointment, no choroidal transmission of light rays was observed, indicating an intact retinal pigment epithelium. |
Case 3
Patient 3 was an 84-year-old female with a 12-year history of daily HCQ use for management of RA. She was 62 inches tall, weighed 84.5 kg, and had been dosed at 400 mg/day (4.7 mg/kg/day based on RBW, 6.7 mg/kg/day based on IBW). She possessed a history of renal cell carcinoma and nephrectomy and developed stage III chronic kidney disease during the time she was on HCQ. Her creatinine was 2.01 at the time HCQ was discontinued.
10–2 VF four years prior to HCQ cessation indicated no major pattern deviations or visual deficits. Her visual acuity after correction was 20/20 bilaterally. However, 12 months before HCQ discontinuation, a full central scotoma was apparent on the 10–2 VF pattern deviation plot of the right eye. This 10–2 VF was misinterpreted as normal. Full scotomas were then subsequently noted on bilateral pattern deviation plots and the right eye’s grayscale display, at which point HCQ was discontinued. Both Zeiss Cirrus and Heidelberg SD-OCT showed bilateral parafoveal EZ hyporeflectivity, left worse than right, at the time of HCQ cessation.
Progression of retinopathy occurred quickly, with the length of the zone of EZ hyporeflectivity increasing by 43.9% in the left eye within 12 months of HCQ discontinuation. No choroidal transmission was present, suggesting that the RPE remained intact. In the right eye, no change was measurable by ImageJ2 on Heidelberg SD-OCT. However, Zeiss Cirrus imaging performed 22 months after HCQ cessation demonstrated bilateral progression of retinopathy, evidenced by additional paracentral ETDRS sectors falling less than 99% of population norms. Heidelberg SD-OCT images at HCQ cessation and after 12 months of follow up are displayed in Figure 9, and Zeiss Cirrus images at HCQ cessation and after 22 months of follow up are displayed in Figures 10 and 11. 10–2 VF showed further worsening pattern deviation. Final visual acuity after correction was 20/20 and 20/25 in the right and left eyes, respectively.
 |
Figure 9 Spectral domain optical coherence tomography images for Case 3. At the time of HCQ cessation, parafoveal hyporeflectivity of the ellipsoid zone (EZ) was observed in both eyes, left worse than right. Parafoveal ellipsoid zone (EZ) hyporeflectivity increased in length and continuity in the left eye over 12 months of follow up (red arrows). We were unable to quantify a change in EZ hyporeflectivity in the right eye using ImageJ2. In both eyes, no choroidal transmission of light rays was observed, indicating an intact retinal pigment epithelium despite progression of retinopathy. |
 |
Figure 10 Zeiss optical coherence tomography of both eyes at the time HCQ was discontinued. In the right eye, 5 parafoveal EDTRS sectors are less than 99% of population norms, indicating early retinopathy. In the left eye, 6 parafoveal EDTRS sectors are less than 99% of population norms, indicating advanced retinopathy. |
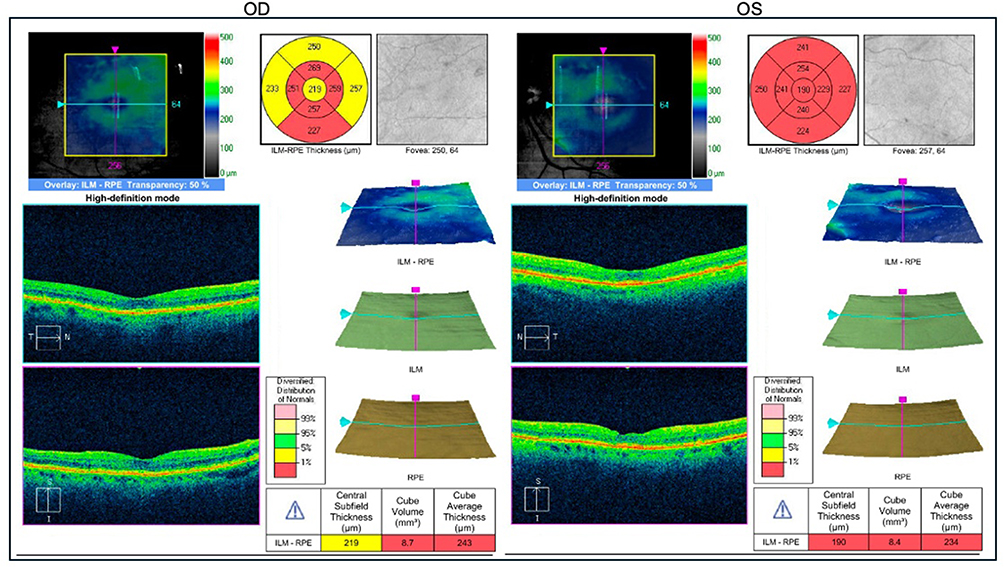 |
Figure 11 Zeiss optical coherence tomography 22 months after HCQ cessation. These results should be compared to Figure 10. In the right eye, 5 parafoveal EDTRS zones are less than 99% of population norms and 4 are less than 95% of population norms, indicating worsening since HCQ cessation. In the left eye, all 8 parafoveal EDTRS zones are less than 99% of population norms, indicating advanced retinopathy worse than 22 months prior. |
Case 4
Patient 4 was a 79-year-old female with SLE and RA who had been taking HCQ for 18 years. She was 63 inches tall and weighed 68.0 kg. Her daily dose was 400 mg/day for the entire treatment period or 5.9 mg/kg/day when adjusted for RBW and 6.5 mg/kg/day by the IBW method. She had a history of stage III CKD diagnosed 2 years prior to stopping HCQ, but her dosage was not adjusted at that time. She had no history of liver disease.
The patient’s vision was complicated by steroid-induced glaucoma with advanced vision loss at baseline. The right eye displayed a superior arcuate defect worst in the superonasal quadrant, consistent with mid-stage glaucoma. The left eye displayed significant nasal step deficits with intact peripheral vision in the lateral visual fields. Visual acuity after correction was 20/30 in the right eye and 20/30 in the left eye.
Decreased parafoveal reflectivity of the EZ in the left eye and bilateral NIR asymmetry was observable three years prior to HCQ discontinuation. Subsequent SD-OCT and 24–2 VF exhibited bilateral parafoveal EZ loss and marked progression of VF loss, at which point HCQ was stopped. At the time of drug discontinuation, 24–2 VF showed near complete VF loss in the left eye and a severe superior arcuate defect in the right eye that had worsened from previous imaging. Bilateral damage was apparent on FAF. However, the RPE remained intact, with no choroidal transmission.
After 29 months of follow up, the length of the zone of EZ loss had increased by 13.6% in the right eye and 30.9% in the left eye. Final 10–2 VF displayed continued worsening of the visual fields. There was diffuse superior and inferotemporal damage in the right eye and near complete visual field loss in the left eye. Final visual acuity after correction was 20/30 in the right eye and 20/40 in the left eye.
Case 5
Patient 5 was a 50-year-old female who took HCQ for 2 years to treat juvenile idiopathic arthritis. She was 64.5 inches tall and 46.1 kg. She had end stage kidney disease on peritoneal dialysis, and no liver disease at the time treatment was initiated. As a result, she was dosed at 200 mg/day or 4.3 mg/kg/day and 3.1 mg/kg/day when adjusted for RBW and IBW, respectively. The daily dose of 200 mg was consistent with current recommendations regarding HCQ dose in patients receiving dialysis treatments.35
Visual acuity without correction was 20/20 in the right eye and 20/30 in the left eye. Baseline 10–2 VFs were unreliable, though 10–2 VF collected 12 months after HCQ was initiated showed partial scotomas bilaterally. HCQ was stopped after 24 months due to abnormal FAF showing hypofluorescence, despite a normal color fundus photograph. Imaging at this time was also significant for bilaterally decreased reflectivity of the parafoveal EZ on SD-OCT, with the right eye worse than the left eye.
She was followed for 8 months after HCQ was stopped, after which the patient was lost to follow up. Final FAF showed increased parafoveal hyperfluorescence and SD-OCT exhibited 28.7% and 19.1% increases in the length of the zone of EZ hyporeflectivity. Though increasingly hyporeflective, the EZ remained present in this patient, in contrast to Patient 1 and Patient 4 whose SD-OCT imaging showed complete EZ loss.
Discussion
All patients in this study were female, consistent with the demographics of other studies.10,13 This is unsurprising, as the prevalence of SLE and RA – two primary indications for HCQ therapy – is greater among female patients.36–38 The mean follow-up length of 31.4 months for the patients studied was also similar to that of previous studies examining patients after cessation of HCQ.2,18,24,25,29,39,40
Previous research indicates that HCQ remains in pigmented tissues for years and can lead to retinal toxicity even after drug cessation.10,41,42 Clinically significant recovery of damaged structures has not been proven.18,43 Retinal regeneration is thought to occur secondary to phagocytosis of damaged cells; however, HCQ exerts its toxicity by interfering with retinal lysosomes, hindering the clearance of retinal debris and production of new cells in outer segments. Thus, detection of HCQ retinopathy, regardless of stage, usually necessitates discontinuation of the drug. In this study, no patients displayed visible regeneration on SD-OCT or meaningful improvements on visual fields or FAF, consistent with previous studies that suggest regeneration of retinal structures is unlikely.
The risk of disease progression appears to be related to the time of HCQ discontinuation, with early cessation corresponding to a lower probability of progression.10,18,23 Previous research describing the progression of HCQ retinopathy has focused on the RPE, a layer of the retina deep to the EZ that is damaged only once the EZ is compromised.23,24,39 Marmor et al23 reported that RPE damage was linked to worsening toxicity on OCT for up to 3 years after HCQ discontinuation, whereas stopping HCQ before RPE damage occurred was associated with significantly less progression and potential stabilization. In contrast, the results of this study indicate that HCQ retinopathy will continue to progress once damage to the parafoveal EZ occurs even if the RPE is intact. All patients experienced expansion of EZ hyporeflectivity during subsequent follow-up appointments despite drug cessation prior to RPE loss, and one patient experienced worsening of retinopathy to the point of RPE loss with choroidal transmission. These anatomic changes corresponded with worsening visual deficits in all patients, as measured by visual fields testing, and have relevance in the discussion regarding whether progression is uncommon or common once focal EZ loss occurs.44,45
The results of this study support previous research that suggests that the threshold of progression occurs prior to RPE damage. A review of 19 eyes by Scarinci et al25 suggested that using RPE damage as a cut-point was too late. They reported that a majority of eyes with damage to the external limiting membrane (ELM) developed worsening of retinopathy, while eyes with an intact ELM remained stable. Mititelu et al18 similarly reported that partial regeneration was only observed in areas of the retina in which the ELM was preserved. Earlier work from our group suggested that studies in which the RPE was chosen as the threshold did not follow cases long enough to observe progression when evaluating earlier thresholds.29
Furthermore, research utilizing machine-learning algorithms in the quantitative analysis of SD-OCT biomarkers report that partial hyporeflectivity of the EZ is a sensitive and specific biomarker for drug toxicity. Prediction models that incorporated EZ integrity into their learning algorithms had high levels of accuracy when predicting progression of HCQ retinopathy.46,47
Proper dosage of HCQ has been debated in the past. Widespread agreement exists that retinopathy is related to daily dose and length of treatment.1,13 Initial guidelines based dosing on IBW and recommended a daily dose less than 6.5 mg/kg/day.8,43 However, in 2013, Browning48 reported that thin patients were more likely to develop toxicity when dosed according to IBW rather than real body weight. Melles et al49 later reported similar findings in a larger sample. In light of these findings, the 2016 AAO guidelines were revised, with a recommended dose less than 5.0 mg/kg/day based on RBW.1 The limitation of this recommendation is that it leads to overdosage of obese patients.50 For example, Cases 2 and 3 received appropriate dosing according to RBW guidelines, but were overdosed based on IBW guidelines. An improved recommendation would be to dose based on the lesser of real and ideal body weight.51
Unfortunately, proper dosage, even based on the lesser of RBW and IBW, does not eliminate the risk of HCQ retinopathy. In this study, Case 5 was appropriately dosed based on both RBW and IBW guidelines yet still developed retinopathy in the setting of concomitant end-stage renal disease. Modifications of dosing in the presence of renal disease are based on theory, though these modifications have not yet been tested experimentally.52 Because HCQ is primarily cleared by the kidneys, expert consensus recommends reducing its dose in patients in whom renal clearance is diminished. The widely accepted guideline is to decrease the daily dose of a patient with normal renal function by 50% in a patient with a GFR less than 30 mL/min.53,54 Unfortunately, the reality is that despite all efforts toward safe dosing, some patients will develop retinopathy, making early detection based on ancillary testing necessary.
This case series illustrates that in practice, clinicians often miss early signs of retinopathy. In Cases 2, 3, and 4 early visual field changes were missed. Another early sign of retinopathy on SD-OCT is decreased parafoveal reflectivity of the EZ. We emphasize this sign because cessation of HCQ at the time of EZ loss but before RPE loss is associated with progression of retinopathy and increasing paracentral scotomas.29
This study has several limitations. To meet the inclusion criteria, patients were required to have an intact RPE at the time of HCQ discontinuation, resulting in a small sample size that limited statistical power. However, previous studies on this topic share this limitation due to the relatively low incidence of HCQ toxicity.18,23–25 Patients were followed at varying intervals, and a variety of tests were used, making it difficult to evaluate the rate of disease progression per unit of time. Additionally, some patients in this study developed kidney disease while taking HCQ. Renal dysfunction is a known risk factor for HCQ toxicity, and it is possible that kidney disease may have influenced disease progression in these patients. However, the likelihood of this association remains unexplored.
In conclusion, definitive markers of HCQ progression are an area of ongoing investigation. The results of this study suggest that focal EZ loss can portend irreversible functional and anatomic progression of HCQ toxicity in patients before RPE loss occurs. Current screening guidelines would benefit from acknowledging an earlier threshold predictive of irreversible damage and use of lesser RBW and IBW in assessing whether a patient’s daily dosing is safe.55 Shifting the threshold and adding the nuance of body weight choice would not eliminate all cases of HCQ retinopathy; however, such changes would improve the sensitivity of screening modalities, prevent avoidable occurrence of potentially reversible toxicity, and reduce the incidence of retinopathy. Ophthalmologists and other providers will benefit from these findings when considering follow-up schedules, dosing strategies, and ancillary testing. Future studies would benefit from prospective designs that incorporate larger sample sizes and standardized multimodal imaging at regular intervals.
Data Sharing Statement
Data is available from David J. Browning at the corresponding author’s address upon request.
Consent to Participate
IRB approval was obtained from the Wake Forest University Institutional Review Board. As a retrospective study, all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties. The risk of harm or discomfort that might occur because of taking part in this research study is not more than in daily life. The rights of subjects were protected through measures to maintain the confidentiality of study information, including password-protected data storage and limited access to study data.
Funding
No funding was received.
Disclosure
J.D.G. has no financial disclosures. D.J.B. receives royalties from Springer Inc. for books written and owns stock in Zeiss-Meditec Inc. totaling between $20,000 and $30,000. The authors report no other conflicts of interest in this work.
References
1. Marmor MF, Kellner U, Lai TY, Melles RB, Mieler WF, American Academy of O. Recommendations on screening for chloroquine and hydroxychloroquine retinopathy (2016 Revision). Ophthalmology. 2016;123(6):1386–1394. doi:10.1016/j.ophtha.2016.01.058
2. Lally DR, Heier JS, Baumal C, et al. Expanded spectral domain-OCT findings in the early detection of hydroxychloroquine retinopathy and changes following drug cessation. Int J Retina Vitreous. 2016;2(1). doi:10.1186/s40942-016-0042-y
3. Xu Y, Wu Q. Prevalence trend and disparities in rheumatoid arthritis among US adults, 2005–2018. J Clin Med. 2021;10(15):3289. doi:10.3390/jcm10153289
4. Izmirly PM, Parton H, Wang L, et al. Prevalence of systemic Lupus erythematosus in the United States: estimates from a meta‐analysis of the centers for disease control and prevention national lupus registries. Arthritis Rheumatol. 2021;73(6):991–996. doi:10.1002/art.41632
5. Yates M, Malaiya R, Stack J, Galloway JB. Hydroxychloroquine use: the potential impact of new ocular screening guidelines. Eye. 2018;32(1):161–162. doi:10.1038/eye.2017.166
6. Wolfe F, Marmor MF. Rates and predictors of hydroxychloroquine retinal toxicity in patients with rheumatoid arthritis and systemic lupus erythematosus. Arthritis Care Res. 2010;62(6):775–784. doi:10.1002/acr.20133
7. Marshall E, Robertson M, Kam S, Penwarden A, Riga P, Davies N. Prevalence of hydroxychloroquine retinopathy using 2018 Royal College of Ophthalmologists diagnostic criteria. Eye. 2021;35(1):343–348. doi:10.1038/s41433-020-1038-2
8. Lee JE, Nam DR, Sung YK, Kim YJ, Jung SY. Nationwide patterns of hydroxychloroquine dosing and monitoring of retinal toxicity in patients with systemic lupus erythematosus. Sci Rep. 2023;13(1):7270. doi:10.1038/s41598-023-34022-0
9. Gianfrancesco MA, Schmajuk G, Haserodt S, et al. Hydroxychloroquine dosing in immune-mediated diseases: implications for patient safety. Rheumatol Int. 2017;37(10):1611–1618. doi:10.1007/s00296-017-3782-6
10. Browning DJ. Hydroxychloroquine and Chloroquine Retinopathy.
11. Yoon YH, Cho KS, Hwang JJ, Lee S-J, Choi JA, Koh J-Y. Induction of lysosomal dilatation, arrested autophagy, and cell death by chloroquine in cultured ARPE-19 cells. Investigat Opthalmol Vis Sci. 2010;51(11):6030. doi:10.1167/iovs.10-5278
12. Toler SM. Oxidative stress plays an important role in the pathogenesis of drug-induced retinopathy. Exp Biol Med. 2004;229(7):607–615. doi:10.1177/153537020422900704
13. Jorge AM, Melles RB, Marmor MF, Zhou B, Zhang Y, Choi HK. Risk factors for hydroxychloroquine retinopathy and its subtypes. JAMA Network Open. 2024;7(5):e2410677. doi:10.1001/jamanetworkopen.2024.10677
14. Wong KL, Pautler SE, Browning DJ. Near-infrared reflectance bull’s eye maculopathy as an early indication of hydroxychloroquine toxicity. Clin Ophthalmol. 2015;9:521–525. doi:10.2147/OPTH.S76963
15. Pandya HK, Robinson M, Mandal N, Shah VA. Hydroxychloroquine retinopathy: a review of imaging. Indian J Ophthalmol. 2015;63(7):570–574. doi:10.4103/0301-4738.167120
16. Chen E, Brown B, MS Benz, et al. Spectral domain optical coherence tomography as an effective screening test for hydroxychloroquine retinopathy (the flying saucer sign). Clin Ophthalmol. 2010:1151. doi:10.2147/opth.s14257.
17. Rodriguez-Padilla JA. High-speed ultra–high-resolution optical coherence tomography findings in hydroxychloroquine retinopathy. Arch Ophthalmol. 2007;125(6):775. doi:10.1001/archopht.125.6.775
18. Mititelu M, Wong BJ, Brenner M, Bryar PJ, Jampol LM, Fawzi AA. Progression of hydroxychloroquine toxic effects after drug therapy cessation: new evidence from multimodal imaging. JAMA Ophthalmol. 2013;131(9):1187–1197. doi:10.1001/jamaophthalmol.2013.4244
19. Melles RB, Marmor MF. Pericentral retinopathy and racial differences in hydroxychloroquine toxicity. Ophthalmology. 2015;122(1):110–116. doi:10.1016/j.ophtha.2014.07.018
20. Kim KE, Ryu SJ, Kim YH, Seo Y, Ahn SJ. Visual field examinations using different strategies in Asian patients taking hydroxychloroquine. Sci Rep. 2022;12(1):14778. doi:10.1038/s41598-022-19048-0
21. Browning DJ, Lee C. Relative sensitivity and specificity of 10-2 visual fields, multifocal electroretinography, and spectral domain optical coherence tomography in detecting hydroxychloroquine and chloroquine retinopathy. Clin Ophthalmol. 2014;8:1389–1399. doi:10.2147/OPTH.S66527
22. Pandey S, Kumar P, Moulick PS, Vats S. Spectral domain optical coherence tomography-based prevalence of hydroxychloroquine maculopathy in Indian patients on hydroxychloroquine therapy: a utopia of underdiagnosis. Med J Armed Forces India. 2020;76(4):395–401. doi:10.1016/j.mjafi.2020.04.012
23. Marmor MF, Hu J. Effect of disease stage on progression of hydroxychloroquine retinopathy. JAMA Ophthalmol. 2014;132(9):1105–1112. doi:10.1001/jamaophthalmol.2014.1099
24. Pham BH, Marmor MF. Sequential changes in hydroxychloroquine retinopathy up to 20 years after stopping the drug: implications for mild versus severe toxicity. Retina. 2019;39(3):492–501. doi:10.1097/IAE.0000000000002408
25. Scarinci F, Shaarawy A, Narala R, Jampol LM, Fawzi AA. Loss of external limiting membrane integrity predicts progression of hydroxychloroquine retinal toxicity after drug discontinuation. Retina. 2016;36(10):1951–1957. doi:10.1097/IAE.0000000000001217
26. Saxena S, Akduman L, Meyer CH. External limiting membrane: retinal structural barrier in diabetic macular edema. Int J Retina Vitreous. 2021;7(1). doi:10.1186/s40942-021-00284-x
27. Browning D, Lee C, Rotberg D. The impact of different algorithms for ideal body weight on screening for hydroxychloroquine retinopathy in women. Clin Ophthalmol. 2014;1401. doi:10.2147/opth.s66531
28. Kellner U, Renner AB, Tillack H. Fundus autofluorescence and mfERG for early detection of retinal alterations in patients using chloroquine/hydroxychloroquine. Investigat Opthalmol Vis Sci. 2006;47(8):3531. doi:10.1167/iovs.05-1290
29. Browning DJ, Koonce DR, Mentreddy A, Punjabi O. The relationship of hydroxychloroquine retinopathy progression to stage at cessation of therapy. Am J Ophthalmol. 2025;277:335–348. doi:10.1016/j.ajo.2025.05.030
30. Rueden CT, Schindelin J, Hiner MC, et al. ImageJ2: ImageJ for the next generation of scientific image data. BMC Bioinf. 2017;18(1). doi:10.1186/s12859-017-1934-z
31. Kirwin AB, J D. Atrophy Advisor: a Clinical Tool for Dry Macular Degeneration with Geographic Atrophy. Available from: https://atrophyadvisor.com/.
32. Lin AN, Mohammed ISK, Munir WM, Munir SZ, Alexander JL. Inter-rater reliability and repeatability of manual anterior segment optical coherence tomography image grading in keratoconus. Eye Contact Lens. 2021;47(9):494–499. doi:10.1097/ICL.0000000000000818
33. Knott EJ, Sheets KG, Zhou Y, Gordon WC, Bazan NG. Spatial correlation of mouse photoreceptor-RPE thickness between SD-OCT and histology. Exp Eye Res. 2011;92(2):155–160. doi:10.1016/j.exer.2010.10.009
34. Marmor MF, Kellner U, Lai TY, Lyons JS, Mieler WF, American Academy of O. Revised recommendations on screening for chloroquine and hydroxychloroquine retinopathy. Ophthalmology. 2011;118(2):415–422. doi:10.1016/j.ophtha.2010.11.017
35. Durcan L, Clarke WA, Magder LS, Petri M. Hydroxychloroquine blood levels in systemic lupus erythematosus: clarifying dosing controversies and improving adherence. J Rheumatol. 2015;42(11):2092–2097. doi:10.3899/jrheum.150379
36. Van Vollenhoven RF. Sex differences in rheumatoid arthritis: more than meets the eye. BMC Med. 2009;7(1):12. doi:10.1186/1741-7015-7-12
37. Kvien TK, Uhlig T, Odegard S, Heiberg MS. Epidemiological aspects of rheumatoid arthritis: the sex ratio. Ann N Y Acad Sci. 2006;1069:212–222. doi:10.1196/annals.1351.019
38. Trentin F, Signorini V, Manca ML, et al. Gender differences in SLE: report from a cohort of 417 Caucasian patients. Lupus Sci Med. 2023;10(1):e000880. doi:10.1136/lupus-2022-000880
39. Allahdina AM, Chen KG, Alvarez JA, Wong WT, Chew EY, Cukras CA. Longitudinal changes in eyes with hydroxychloroquine retinal toxicity. Retina. 2019;39(3):473–484. doi:10.1097/IAE.0000000000002437
40. Sharma A, Maiz AM, Tucker WR, Cukras C. Accelerated onset of retinal toxicity from hydroxychloroquine use with concomitant breast cancer therapy. Retin Cases Brief Rep. 2019;13(2):98–102. doi:10.1097/ICB.0000000000000742
41. Salu P, Uvijls A, Van Den Brande P, Leroy BP. Normalization of generalized retinal function and progression of maculopathy after cessation of therapy in a case of severe hydroxychloroquine retinopathy with 19 years follow-up. Documenta Ophthalmol. 2010;120(3):251–264. doi:10.1007/s10633-010-9220-7
42. Brinkley JR Jr, Dubois EL, Ryan SJ. Long-term course of chloroquine retinopathy after cessation of medication. Am J Ophthalmol. 1979;88(1):1–11. doi:10.1016/0002-9394(79)90743-8
43. Michaelides M, Stover NB, Francis PJ, Weleber RG. Retinal toxicity associated with hydroxychloroquine and chloroquine: risk factors, screening, and progression despite cessation of therapy. Arch Ophthalmol. 2011;129(1):30–39. doi:10.1001/archophthalmol.2010.321
44. Marmor MF. Comment on: the relationship of hydroxychloroquine retinopathy progression to stage at cessation of therapy. Am J Ophthalmol. 2025. doi:10.1016/j.ajo.2025.08.056
45. Browning DJ, Koonce DR, Mentreddy A, Punjabi O. Reply to correspondence on the relationship of hydroxychloroquine retinopathy progression to stage at cessation of therapy. Am J Ophthalmol. 2025. doi:10.1016/j.ajo.2025.09.023
46. Kalra G, Talcott KE, Kaiser S, et al. Machine learning-based automated detection of hydroxychloroquine toxicity and prediction of future toxicity using higher-order OCT biomarkers. Ophthalmol Retina. 2022;6(12):1241–1252. doi:10.1016/j.oret.2022.05.031
47. Talcott KE, Kalra G, Cetin H, et al. Automated evaluation of ellipsoid zone at-risk burden for detection of hydroxychloroquine retinopathy. J Pers Med. 2024;14(5). doi:10.3390/jpm14050448
48. Browning DJ. Impact of the revised American academy of ophthalmology guidelines regarding hydroxychloroquine screening on actual practice. Am J Ophthalmol. 2013;155(3):418–428e1. doi:10.1016/j.ajo.2012.09.025
49. Melles RB, Marmor MF. The risk of toxic retinopathy in patients on long-term hydroxychloroquine therapy. JAMA Ophthalmol. 2014;132(12):1453–1460. doi:10.1001/jamaophthalmol.2014.3459
50. Browning DJ, Easterbrook M, Lee C. The 2016 American Academy of Ophthalmology hydroxychloroquine dosing guidelines for short, obese patients. Ophthalmol Retina. 2019;3(10):809–813. doi:10.1016/j.oret.2019.05.005
51. Browning DJ, Lee C. Somatotype, the risk of hydroxychloroquine retinopathy, and safe daily dosing guidelines. Clin Ophthalmol. 2018;12:811–818. doi:10.2147/opth.s163451
52. Rao IR, Kolakemar A, Shenoy SV, et al. Hydroxychloroquine in nephrology: current status and future directions. J Nephrol. 2023;36(8):2191–2208. doi:10.1007/s40620-023-01733-6
53. Wu C-Y, Tan M, Huang J-Y, Chiou J-Y, Wei J-C-C. Hydroxychloroquine is neutral in risk of chronic kidney disease in patients with systemic lupus erythematosus. Ann Rheumatic Dis. 2022;81(5):e75–e75. doi:10.1136/annrheumdis-2020-217728
54. Fanouriakis A, Kostopoulou M, Cheema K, et al. 2019 update of the joint European League Against Rheumatism and European Renal Association–European Dialysis and Transplant Association (EULAR/ERA–EDTA) recommendations for the management of lupus nephritis. Ann Rheumatic Dis. 2020;79(6):713–723. doi:10.1136/annrheumdis-2020-216924
55. Browning DJ, Yokogawa N, Greenberg PB, Perlman E. Rethinking the hydroxychloroquine dosing and retinopathy screening guidelines. Am J Ophthalmol. 2020;219:101–106. doi:10.1016/j.ajo.2020.06.030
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.