Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Electroacupuncture as a Non-Pharmacological Intervention for Nicotine Dependence: Evidence from a Randomized Clinical Trial
Authors Lai Z, Fan Q, Lee AL, Yao X ![]() , Dai R, Liang Y
, Dai R, Liang Y
Received 5 September 2025
Accepted for publication 19 December 2025
Published 30 December 2025 Volume 2025:21 Pages 1869—1885
DOI https://doi.org/10.2147/TCRM.S565463
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Zhen Lai,1,* Qian Fan,2,* Ai Ling Lee,3 Xujing Yao,3 Ranran Dai,4 Yan Liang2
1TCM Department, Jiading District Central Hospital Affiliated Shanghai University of Medicine & Health Sciences, Shanghai, People’s Republic of China; 2Acupuncture Department, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 3Acupuncture Department, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 4Pneumology Department, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Liang, Acupuncture Department, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China, Email [email protected]
Abstract: Nicotine dependence, a chronic addictive disorder characterized by high relapse rates, represents a significant global public health challenge. This study employed a randomized, single-blind, parallel-group controlled design to systematically evaluate the efficacy and safety of electroacupuncture compared with varenicline in the treatment of nicotine dependence. The results demonstrated that electroacupuncture achieved significantly superior outcomes across multiple key outcome measures relative to varenicline: the electroacupuncture group exhibited a greater mean daily reduction in Fagerström Test for Nicotine Dependence (FTND) scores (− 1.11 points/day vs − 0.33 points/day, P < 0.001) and a higher rate of sustained improvement at the 3-month follow-up (84.4% vs 69.5%). With respect to the Heaviness of Smoking Index (HSI), the electroacupuncture group showed a more rapid and sustained decline (sustained rate: 81.7% vs 63.9%, P = 0.002). Moreover, electroacupuncture demonstrated significant advantages in alleviating nicotine withdrawal symptoms (sustained rate: 75.3% vs 52.8%, P = 0.026) and reducing daily cigarette consumption (79.0% vs 56.2%, P < 0.001). The potential mechanism may involve modulation of the mesolimbic dopamine system. These findings support electroacupuncture as a safe, effective, and sustainable non-pharmacological intervention for smoking cessation, particularly suitable for individuals with high nicotine dependence who are sensitive to adverse drug reactions or exhibit poor medication adherence, and suggest its potential role as a complementary or alternative strategy in clinical smoking cessation programs. Future research should further validate its long-term efficacy and investigate the neurobiological mechanisms underlying its effects on relapse prevention.
Keywords: electroacupuncture, nicotine dependence, smoking cessation, varenicline, withdrawal symptoms, randomized controlled trial
Introduction
Long-term exposure to nicotine, the main addictive component of tobacco, induces feelings of euphoria and pleasure in smokers. When nicotine intake is reduced or discontinued, individuals often experience dependence and withdrawal symptoms, a condition known as nicotine dependence.1 Nicotine dependence typically manifests in two dimensions: physiological and psychological. Physiological dependence may present with withdrawal symptoms such as throat irritation, cough, anxiety, depression, impaired concentration, and insomnia;2 psychological dependence is characterized by a strong subjective craving to smoke.3
According to the World Health Organization (WHO), the tobacco epidemic represents one of the greatest public health threats globally, being a leading cause of mortality, morbidity, and poverty.4 China is currently the world’s largest producer and consumer of tobacco, with more than 300 million smokers. Each year, over one million deaths are attributed to smoking, and an additional one million deaths are caused by exposure to second-hand smoke.5 Extensive research has established smoking as a major risk factor for various cancers, pulmonary diseases, and cardiovascular conditions. Consequently, smoking is not only a critical health issue but also a broader social security concern.6
The 2025 guideline on nicotine replacement therapy (NRT)7 recommends that physicians use the “5R” method to enhance smoking cessation motivation and the “5A” method to support cessation. First-line pharmacological treatments include nicotine patches, nicotine chewing gum, sustained-release bupropion, and varenicline, while second-line agents include clonidine and nortriptyline. Although these medications demonstrate certain therapeutic benefits, they are frequently associated with adverse effects such as headache, dry mouth, and insomnia.8 Furthermore, side effects combined with limited willpower often lead smokers to relapse. Consequently, the WHO has classified nicotine dependence under the International Classification of Diseases (ICD-10, F17.2) as a mental and behavioral disorder. As a chronic condition, nicotine dependence poses a serious threat to public health.9 Therefore, identifying a green, safe, effective intervention that prolongs relapse intervals and minimizes adverse reactions has become a global priority.
Tobacco was introduced to China during the Wanli period of the Ming Dynasty, and historical records regarding its use have become increasingly comprehensive. The application of acupuncture for smoking cessation was first documented in the context of auricular acupuncture therapy. By the 1970s, international research had reported on both auricular acupuncture and combined body-auricular acupuncture approaches for smoking cessation.10 As a core component of Traditional Chinese Medicine, acupuncture exerts preventive and therapeutic effects through the stimulation of specific acupoints, with its theoretical foundation rooted in the Huangdi Neijing.11
Recent studies suggest that acupuncture may alleviate withdrawal symptoms and craving behaviors associated with substance use disorders by modulating the mesolimbic dopamine system.12,13 However, the precise mechanisms and clinical efficacy of acupuncture in the treatment of nicotine dependence remain to be systematically validated. Building upon preliminary investigations conducted by our research group on acupuncture-based interventions for addiction,14 we have identified a set of effective acupoints and incorporated electroacupuncture to enhance stimulation intensity. This study aims to systematically evaluate the effects of electroacupuncture on nicotine withdrawal symptoms.
The present study proposes to test the following hypothesis through a randomized controlled trial: electroacupuncture can effectively reduce withdrawal symptoms and diminish psychological craving intensity in individuals with nicotine dependence. The findings are expected to provide high-quality clinical evidence supporting the use of acupuncture in the management of nicotine dependence and to contribute novel insights into the neural regulatory mechanisms underlying addictive behaviors.
Methods
Study Design
This randomized clinical trial adopted a participant-blinded, parallel-group controlled design, and was conducted from April 2024 to April 2025. The trial design and reporting followed the Consolidated Standards of Reporting Trials (CONSORT)15 and the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA).16 The study complied with the Declaration of Helsinki and was approved by the Ethics Committee of Shanghai Yueyang Hospital of Integrated Traditional Chinese and Western Medicine (Approval No. 2024–042). The trial was registered in the Chinese Clinical Trial Registry (ChiCTR2400087626).
Participants
Patients with nicotine dependence presenting to the Acupuncture Department of Yueyang Hospital, Shanghai University of Traditional Chinese Medicine, were recruited and underwent an initial clinical interview. All interventions were performed at the outpatient acupuncture clinic of Yueyang Hospital.
Diagnostic Criteria
Nicotine dependence was diagnosed according to the diagnostic criteria for substance dependence,17 including:
① Strong craving for smoking;
② Uncontrollable smoking behavior;
③ Withdrawal symptoms after cessation or reduction of smoking;
④ Tolerance to tobacco, requiring increased smoking to achieve the same effect previously obtained with smaller amounts;
⑤ Abandonment or reduction of other activities and preferences due to smoking;
⑥ Persistent smoking despite awareness of harmful consequences.
A diagnosis of nicotine dependence was established if at least three of the above criteria were met within the past year.
Inclusion Criteria
① Voluntary smokers meeting the diagnostic criteria;
② Aged 18–70 years;
③ Smoking history ≥1 year;
④ Daily cigarette consumption ≥10;
⑤ Provided informed consent and voluntarily participated;
⑥ No smoking cessation treatment received within the past two weeks.
Exclusion Criteria
① Severe cardiovascular, pulmonary, cerebrovascular, hematologic disease, or diabetes;
② Psychiatric disorders or illicit drug use;
③ Pregnancy.
Interventions
All acupuncture procedures in this study were performed by licensed attending physicians holding a Master’s degree in Traditional Chinese Medicine and Acupuncture and possessing at least three years of clinical experience. These physicians completed a 48-hour standardized training and assessment program, achieving a Kappa value of ≥0.85, indicating high inter-rater reliability in protocol implementation. During treatment sessions, participants wore opaque eye masks and maintained a standardized prone position, with isolation bed curtains deployed to prevent visual exposure. Physicians strictly adhered to aseptic techniques, including the use of sterile gloves and a three-step disinfection procedure with 75% alcohol, and utilized disposable sterile acupuncture needles to ensure patient safety. The medication group received varenicline tartrate, a first-line pharmacological agent for smoking cessation, serving as a positive control. This design enabled a direct comparison between electroacupuncture—a non-pharmacological physical intervention—and standard drug therapy, with the aim of evaluating its potential as an effective alternative in clinical practice. The study was specifically designed to investigate differential mechanisms of action, namely neuromodulation versus receptor antagonism. Both groups were balanced with respect to non-specific factors, including physician-patient interaction and treatment context, to isolate the specific effects of the interventions. To ensure the integrity of blinding, independent monitors were appointed to conduct regular process audits throughout the trial, thereby minimizing performance and detection biases to the greatest extent possible.
Electroacupuncture Group
Based on our previous clinical studies on acupuncture for substance dependence,14 a series of validated acupoints were selected for the electroacupuncture treatment protocol in this trial. The following bilateral acupoints were used: PC6 (Neiguan), HT7 (Shenmen), ST36 (Zusanli), SP6 (Sanyinjiao), Huatuojiaji (T5), BL23 (Shenshu), and the Sweet Point. Acupoint locations were defined according to the WHO Standard Acupuncture Point Locations in the Western Pacific Region18 (Table 1). Disposable sterile acupuncture needles (0.25 mm × 40 mm; Guizhou Andi Medical Equipment Co., Ltd.) were used. Needle insertion depths were as follows: PC6 (Neiguan): 0.5–1 cun (1–2 cm), perpendicular insertion (90°); HT7 (Shenmen): 0.3–0.5 cun (0.5–1 cm), perpendicular; ST36 (Zusanli): 1–1.5 cun (2–3 cm), perpendicular; SP6 (Sanyinjiao): 0.5–1 cun (1–2 cm), perpendicular; BL23 (Shenshu): 0.5–1 cun (1–2 cm), perpendicular; Huatuojiaji (T5): 0.5–1 cun (1–2 cm), oblique insertion toward the spine at 45°–60°; Sweet Point: 0.1–0.2 cun (1–2 mm), shallow insertion at 15°-30°.
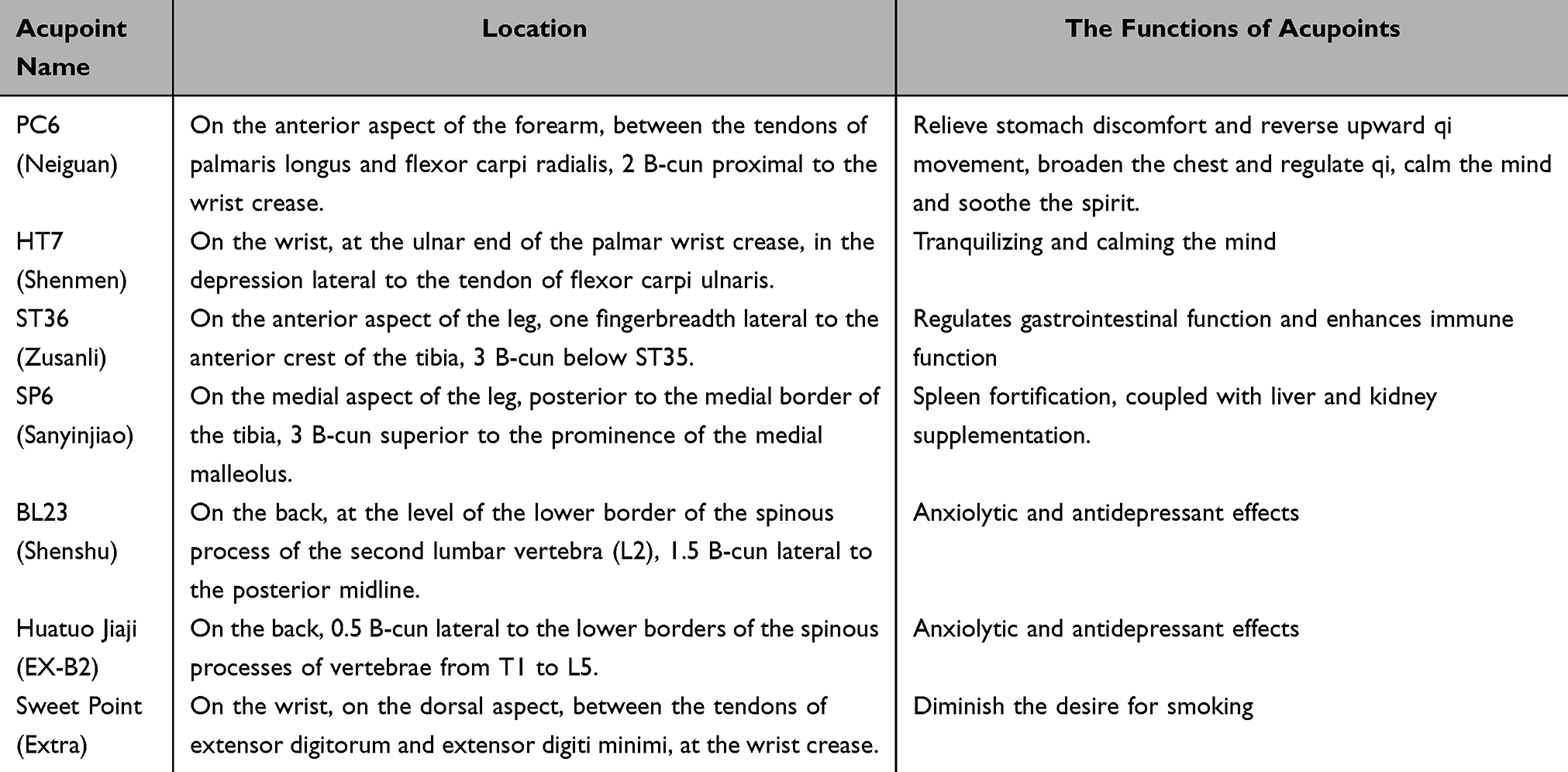 |
Table 1 Locations of Selected Acupoints |
All acupoints were stimulated using a balanced reinforcing–reducing method. After eliciting the deqi sensation, electrodes were connected with the positive pole (+) attached to Huatuojiaji (T5) and the negative pole (–) to BL23 (Shenshu) on the same side. A G6805-II low-frequency electroacupuncture device (Shanghai Medical Electronic Instrument Co., Ltd.) was applied, delivering continuous waves at 2 Hz. The intensity was adjusted to the maximum tolerance level of each participant. Each treatment lasted 20 minutes, administered three times per week for four weeks, constituting one treatment course. Participants were followed up for three months after completion of treatment.
Drug Group
Participants in the drug group received varenicline tartrate tablets (Champix). The dosing regimen was as follows: Days 1–3: 0.5 mg once daily, orally administered 30 minutes after breakfast; Days 4–7: 0.5 mg twice daily, orally administered 30 minutes after breakfast and dinner; Weeks 2–4: 1.0 mg twice daily, orally administered 30 minutes after breakfast and dinner. The treatment course lasted 4 weeks, constituting one full treatment cycle. All participants were followed up for 3 months after completion of therapy.
Outcome Measures
Primary Outcome Measures
Nicotine Dependence Severity (FTND)
The Fagerström Test for Nicotine Dependence (FTND)19 was used to evaluate the degree of nicotine dependence. The scale includes core items such as smoking frequency, time to first cigarette after waking, difficulty refraining from smoking in restricted situations, number of cigarettes smoked per day, and nocturnal smoking. Each item is scored based on behavioral characteristics, with higher total scores indicating greater severity of nicotine dependence, and lower scores reflecting milder dependence.
Heaviness of Smoking Index (HSI)
The Heaviness of Smoking Index (HSI)20 was employed to assess the overall severity of smoking. This index evaluates the impact of smoking behavior on physiological, psychological, and social functioning, including interference with daily life and concerns regarding smoking-related health issues. Scores are graded according to severity, with higher scores reflecting more severe smoking problems and lower scores indicating milder severity.
Nicotine Craving (QSU-Brief)
Nicotine craving was measured using the Brief Questionnaire of Smoking Urges (QSU-Brief).21 This scale focuses on the subjective intensity of craving and the frequency of uncontrollable urges to smoke. Items are scored on a Likert scale (eg, from “none” to “extremely strong”), with higher total scores indicating stronger nicotine craving and lower scores suggesting reduced craving.
Nicotine Withdrawal Symptoms (MNWS)
The Minnesota Nicotine Withdrawal Scale (MNWS)22 was used to assess withdrawal symptoms. The scale covers emotional disturbances (eg, irritability, anxiety) and physiological discomfort (eg, insomnia, difficulty concentrating, changes in appetite). Scores are assigned according to frequency and severity, with higher totals reflecting more severe withdrawal symptoms and lower scores indicating milder withdrawal.
All scales were completed under the guidance of trained assessors. For participants unable to complete the questionnaires independently, trained evaluators recorded responses based on accurate verbal descriptions to ensure objectivity and accuracy of data collection.
Safety Assessment
During treatment, any adverse reactions associated with electroacupuncture or varenicline administration were documented in detail. The causes of such events were analyzed, and preventive as well as management strategies were implemented accordingly. Potential adverse events related to electroacupuncture included device malfunction (eg, electrical leakage), allergic reactions, needle bending, needle stagnation, fainting, hematoma, and local skin infection. Varenicline-related adverse reactions may include nausea, dizziness, and other gastrointestinal or neurological effects.
In addition, participants’ vital signs were closely monitored throughout the trial. If any participant experienced discomfort, treatment was temporarily suspended or the trial was discontinued as appropriate.
Sample Size
The sample size was calculated using the formula for comparing two independent proportions:

Where n1and n2 represent the required sample size for each group, p1 and p2 denote the estimated effective rates of the two groups, and uα and uβ correspond to the critical values for type I error (α) and type II error (β), respectively.
Assuming an expected efficacy rate of 60% in the electroacupuncture group (p1) and 50.6% in the drug group (p2),23 with α = 0.05 and β = 0.20, the calculation yielded n = 26 per group. Considering a 15% dropout rate (≈5 cases), the required sample size was increased to 31 per group. Therefore, the total sample size for this study was set at 62 participants.
Randomization and Blinding
This trial adopted a randomized controlled, partially blinded design, with participants randomly assigned in a 1:1 ratio to either the electroacupuncture group or the drug group. Random numbers between 1 and 62 were generated using SPSS 27.0 software and placed in opaque, sealed envelopes labeled only with sequence numbers. The treating acupuncturists opened the envelopes immediately prior to treatment after verifying the integrity of the seal.
To ensure blinding, outcome assessment and data analysis were conducted independently by investigators who were unaware of group allocation. Given the inherent differences between electroacupuncture and pharmacological treatment, several measures were implemented to minimize bias:
A standardized treatment protocol was used to ensure procedural consistency;
Primary outcome measures were assessed by blinded evaluators;
Treatment adherence and adverse events were monitored throughout the study;
An independent data monitoring committee supervised trial quality.
These measures ensured maximal objectivity of results while acknowledging the unavoidable differences between intervention modalities.
Statistical Analysis
All data were analyzed using SPSS Statistics version 23.0. Continuous variables with normal distribution were expressed as mean ± standard deviation ( ± s) and compared using independent-samples t tests; non-normally distributed data were presented as median (interquartile range) and analyzed using the Mann–Whitney U-test. Categorical variables were expressed as frequency or percentage and compared using the chi-square (χ2) test. Repeated measures analysis of variance (ANOVA) was applied to evaluate changes over time and between groups. A two-sided P value < 0.05 was considered statistically significant.
± s) and compared using independent-samples t tests; non-normally distributed data were presented as median (interquartile range) and analyzed using the Mann–Whitney U-test. Categorical variables were expressed as frequency or percentage and compared using the chi-square (χ2) test. Repeated measures analysis of variance (ANOVA) was applied to evaluate changes over time and between groups. A two-sided P value < 0.05 was considered statistically significant.
Results
Participant Characteristics
This trial was conducted from April 2024 to April 2025. During this period, 96 potential participants underwent eligibility screening. After strict evaluation, 62 individuals met all inclusion criteria and none of the exclusion criteria, and were subsequently enrolled. Participant flow is shown in Figure 1. Two participants withdrew during the trial: one from the drug group due to adverse drug reactions, and one from the electroacupuncture group due to intolerance of needle sensation. Ultimately, follow-up assessments were completed in April 2025, with 60 participants completing the entire protocol (30 in the electroacupuncture group and 30 in the drug group).
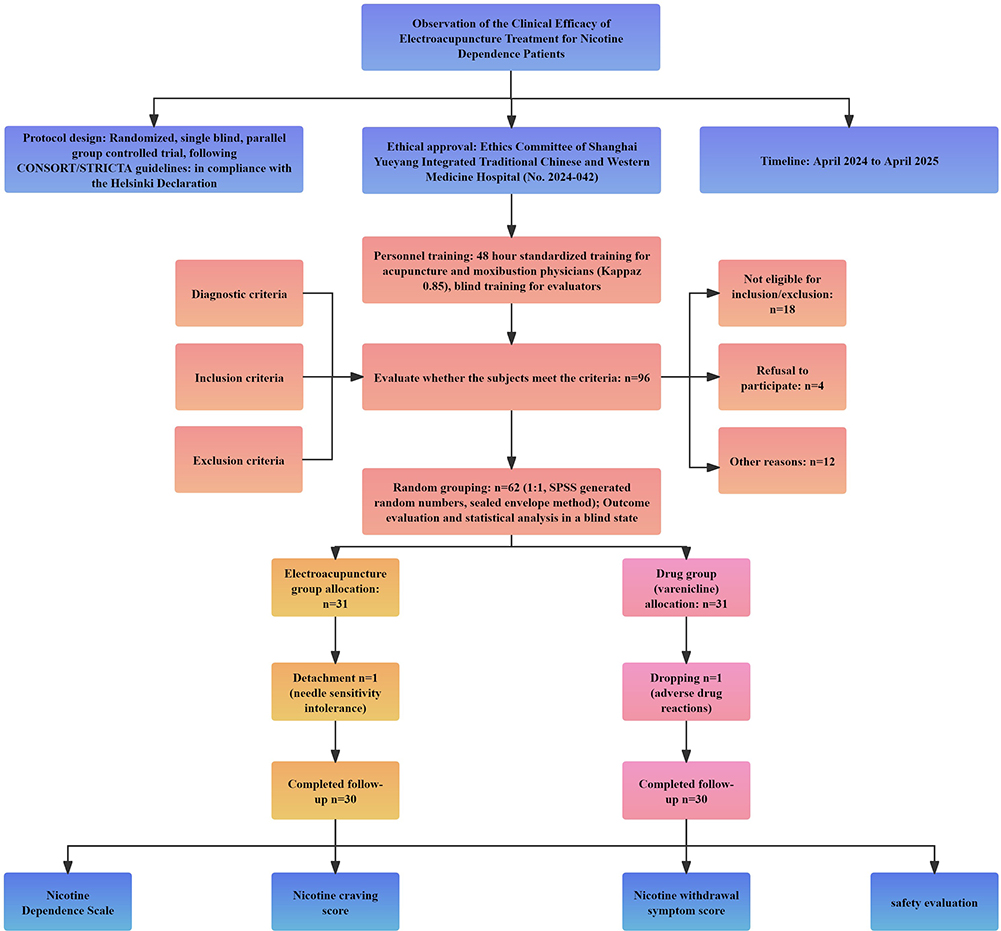 |
Figure 1 Flow diagram of participant enrollment and trial process. |
Baseline characteristics, including age, smoking history, daily cigarette consumption, education level, and marital status, showed no significant differences between groups (P > 0.05), indicating comparability (Table 2).
 |
Table 2 Comparison of Baseline Characteristics Between Groups |
Efficacy
Comparison of FTND Scores Between Groups
At baseline, there was no significant difference in FTND scores between the two groups (P = 0.753), confirming the validity and balance of the randomization process.
Acute phase (0–3 days): The rate of FTND score reduction in the electroacupuncture group was −1.11 points/day (95% CI: −1.18 to −1.04), significantly faster than that of the drug group (−0.33 points/day; Δ = 0.78 points/day, P < 0.001). Within the first three days of treatment, the electroacupuncture group achieved the same level of improvement that required seven days in the drug group (56.1% vs 16.3%). Maintenance phase (1–4 weeks): By the end of week 4, the electroacupuncture group demonstrated a cumulative reduction in FTND scores that was 15.8% greater than that of the drug group (F = 188.1, P < 0.001, η2 = 0.75).
Follow-up phase (3 months): The electroacupuncture group maintained 84.4% of its initial improvement, significantly higher than the 69.5% retention observed in the drug group (Δ = 14.9%, P < 0.001) show in Table 3. Overall, electroacupuncture produced significantly greater reductions in FTND scores across all phases compared with varenicline treatment. In the acute phase (0–3 days), the electroacupuncture group achieved a 56.1% reduction (95% CI: 53.0–59.2), markedly higher than the 16.3% reduction in the drug group (95% CI: 13.2–19.4). At the end of the maintenance phase (week 4), the cumulative reductions were 83.2% (95% CI: 79.9–86.5) in the electroacupuncture group and 67.4% (95% CI: 63.1–71.7) in the drug group. At the 3-month follow-up, the retention of improvement remained significantly higher in the electroacupuncture group (84.4%, 95% CI: 81.1–87.7) compared with the drug group (69.5%, 95% CI: 65.2–73.8), show in Figure 2.
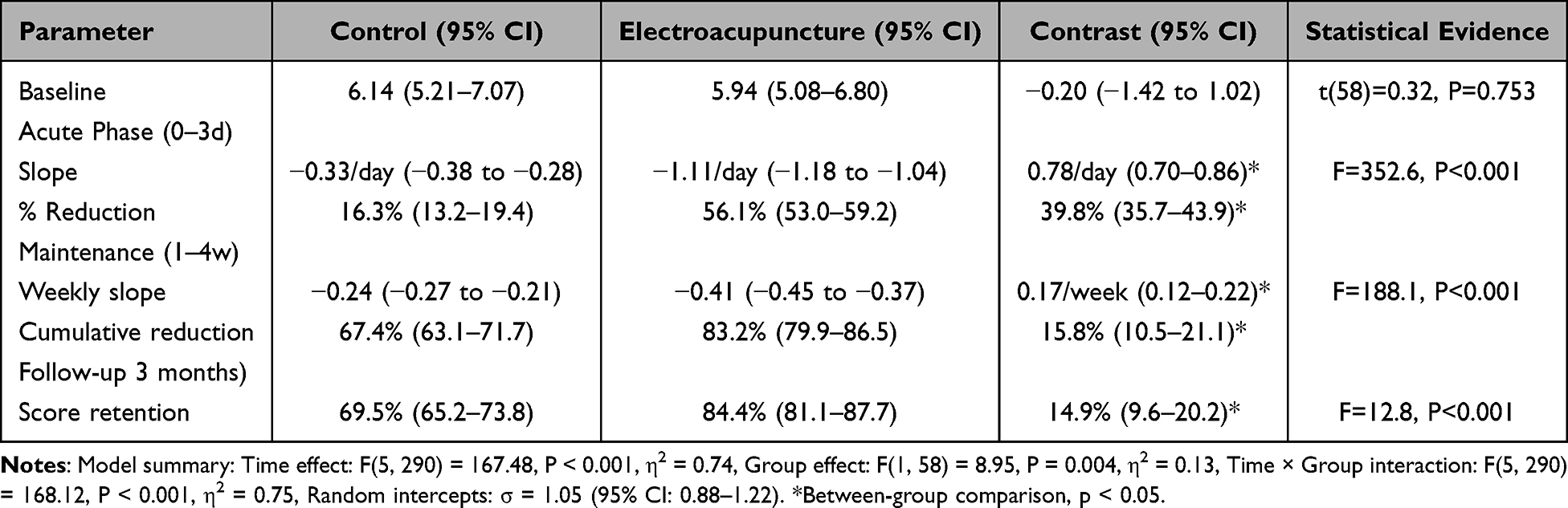 |
Table 3 Comparison of FTND Scores Between Groups |
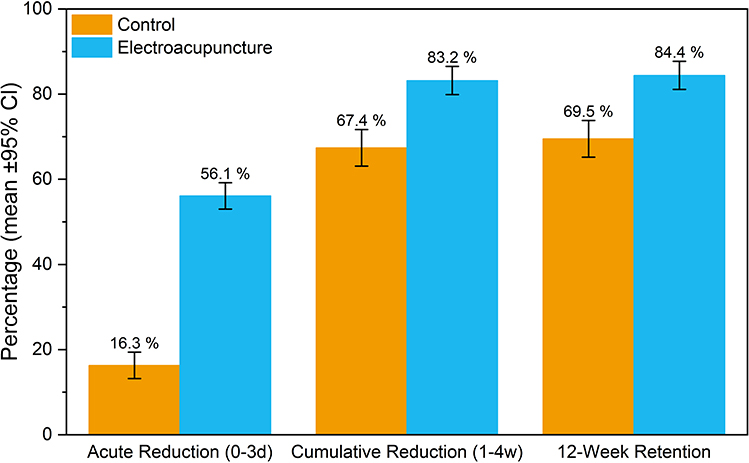 |
Figure 2 Key percentage outcomes of FTND scores: Control vs Electroacupuncture (mean ± 95% CI). |
Heaviness of Smoking Index (HSI) Scores
At baseline, there was no significant difference in HSI scores between groups (P = 0.730), confirming the validity of the randomization process.
Acute phase (0–3 days): The rate of HSI score reduction in the electroacupuncture group was −0.62 points/day (95% CI: −0.68 to −0.56), significantly greater than the drug group’s −0.12 points/day (Δ = 0.50/day, P < 0.001). Notably, electroacupuncture achieved within 3 days the absolute reduction that required 25 days in the drug group (50.9% vs 9.7%).
Maintenance phase (1–4 weeks): The electroacupuncture group demonstrated a cumulative reduction that was 17.8% greater than the drug group (F = 188.9, P < 0.001, η2 = 0.78).
Follow-up phase (3 months): Electroacupuncture maintained 81.7% of the initial improvement, which was significantly higher than the 63.9% retention observed in the drug group (Δ = 17.8%, P = 0.002), show in Table 4.
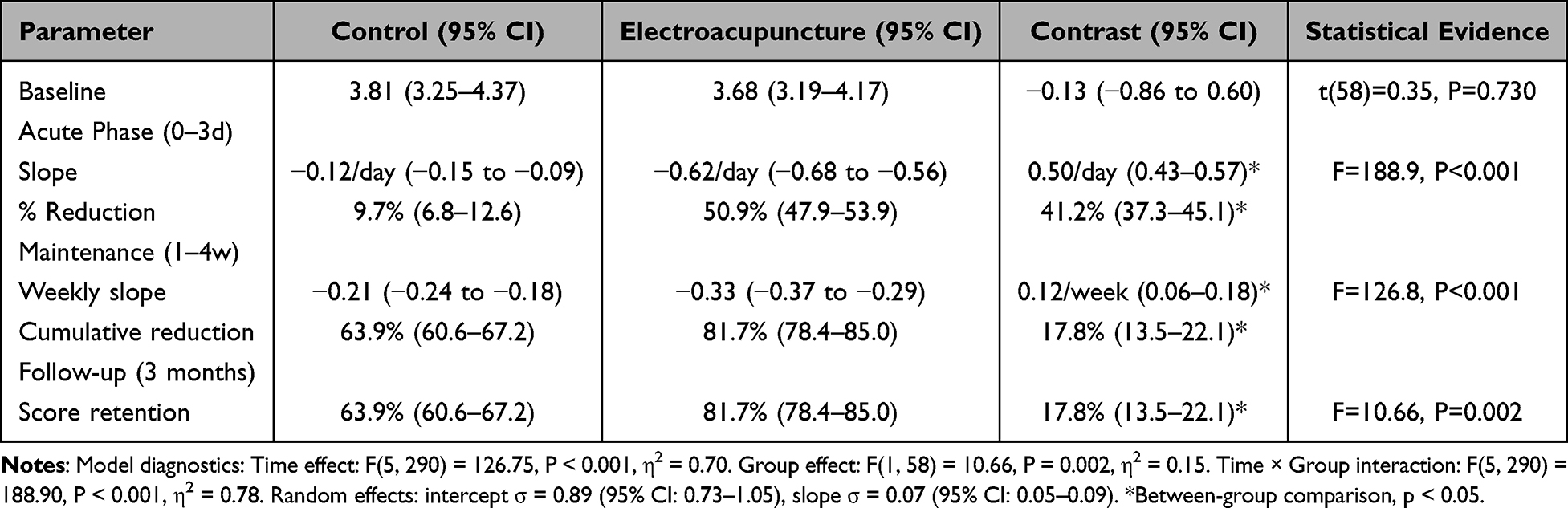 |
Table 4 Comparison of HSI Scores Between Electroacupuncture and Drug Groups |
Overall, electroacupuncture produced consistently greater improvements in HSI scores across all phases compared with drug therapy. In the acute phase, reductions were 50.9% (95% CI: 47.9–53.9) in the electroacupuncture group versus 9.7% (95% CI: 6.8–12.6) in the drug group. By the end of the maintenance phase, cumulative reductions reached 81.7% (95% CI: 78.4–85.0) and 63.9% (95% CI: 60.6–67.2), respectively. At 3 months, retention of improvement remained significantly higher in the electroacupuncture group (81.7% vs 63.9%), show in Figure 3.
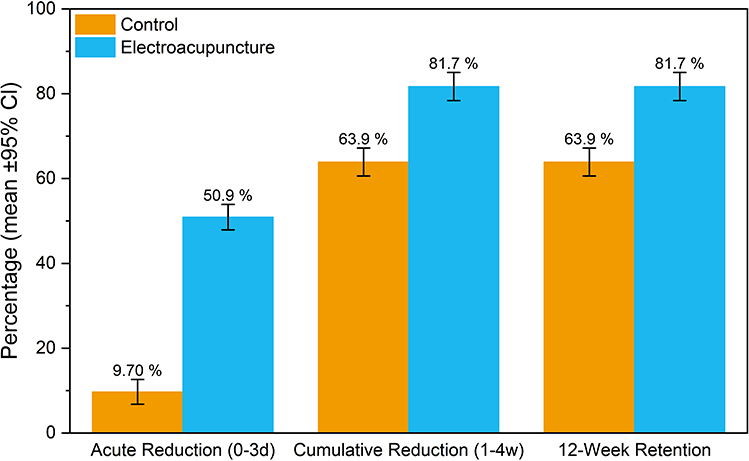 |
Figure 3 Key percentage outcomes of HSI scores: Control vs Electroacupuncture (mean ± 95% CI). |
Effect of Electroacupuncture on Nicotine Craving (QSU-Brief)
At baseline, there was no significant difference in QSU-Brief scores between groups (P = 0.165), confirming the validity of the randomization process.
Acute phase (0–3 days): The reduction rate in the electroacupuncture group was −4.72 points/day (95% CI: −5.02 to −4.42), significantly faster than the drug group’s −1.08 points/day (Δ = 3.64 points/day, P < 0.001). Within 3 days, the electroacupuncture group achieved the same degree of improvement that required 12 days in the drug group (38.6% vs 7.9%).
Maintenance phase (1–4 weeks): During weeks 1–4, the cumulative reduction in QSU-Brief scores did not differ significantly between groups (P = 0.296). The early advantage observed in the electroacupuncture group persisted, with no evidence of catch-up by the drug group. Follow-up phase (3 months): At 3 months, score retention was similar between groups (64.7% in the electroacupuncture group vs 63.4% in the drug group; Δ = 1.3%, P = 0.542), show in Table 5.
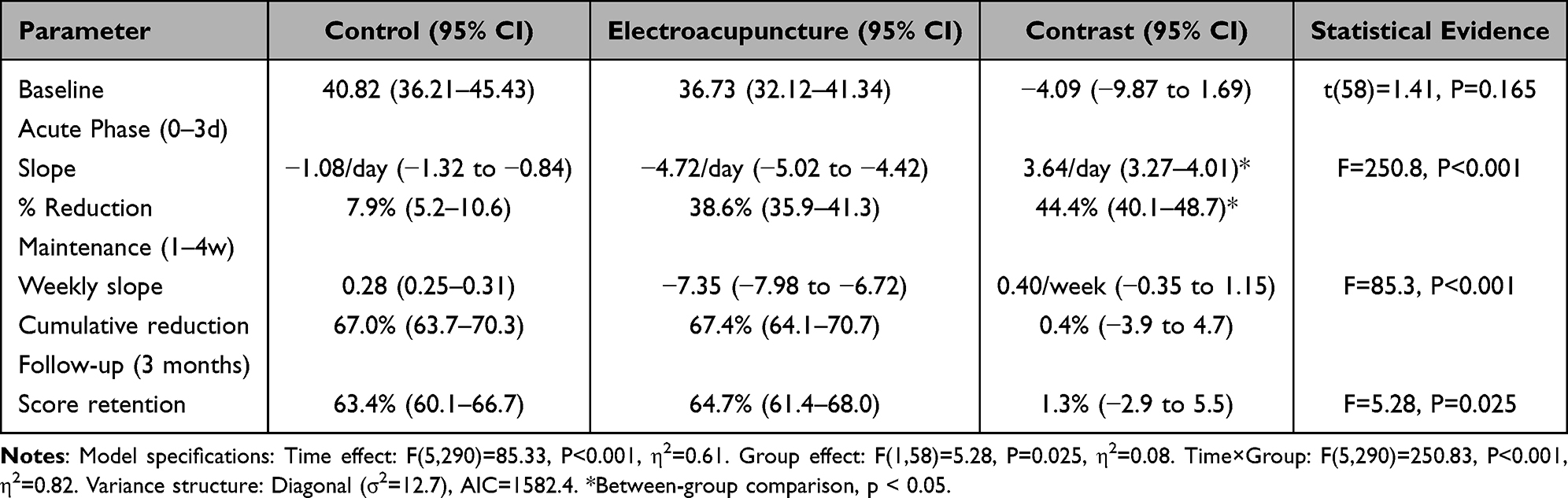 |
Table 5 Comparison of QSU-Brief Scores Between Electroacupuncture and Drug Groups |
Overall, electroacupuncture produced more rapid improvements in nicotine craving during the acute phase, while the long-term outcomes were comparable between groups. In the acute phase, reductions were 38.6% (95% CI: 35.9–41.3) in the electroacupuncture group and 7.9% (95% CI: 5.2–10.6) in the drug group. At the end of the maintenance phase, cumulative reductions were 67.4% (95% CI: 64.1–70.7) vs 67.0% (95% CI: 63.7–70.3). At the 3-month follow-up, retention of improvement remained comparable (64.7% vs 63.4%), show in Figure 4.
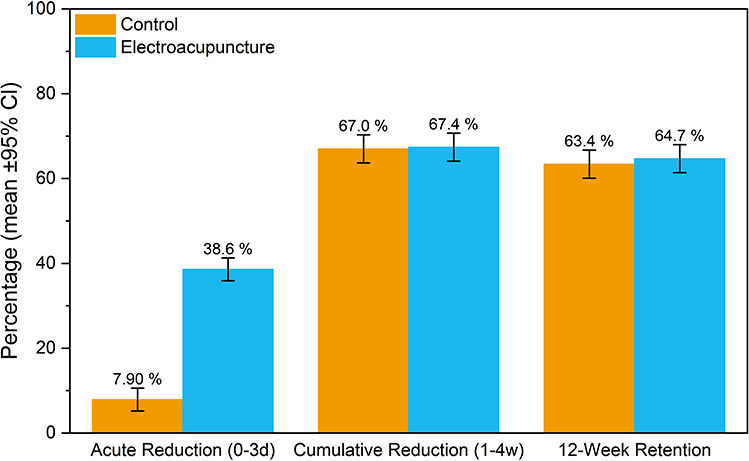 |
Figure 4 Key percentage outcomes of QSU-Brief scores: Control vs Electroacupuncture (mean ± 95% CI). |
Effect of Electroacupuncture on Nicotine Withdrawal Symptoms (MNWS)
At baseline, there was no significant difference in MNWS scores between the two groups (P = 0.409), confirming the validity of randomization.
Acute phase (0–3 days): The rate of MNWS score reduction in the electroacupuncture group was −2.90 points/day (95% CI: −3.13 to −2.67), significantly greater than the drug group’s −0.99 points/day (Δ = 1.91/day, P < 0.001). Within 3 days, the electroacupuncture group achieved a 55.2% reduction in withdrawal symptoms, equivalent to the improvement that required 8 days in the drug group (55.2% vs 20.5%), show in Table 6.
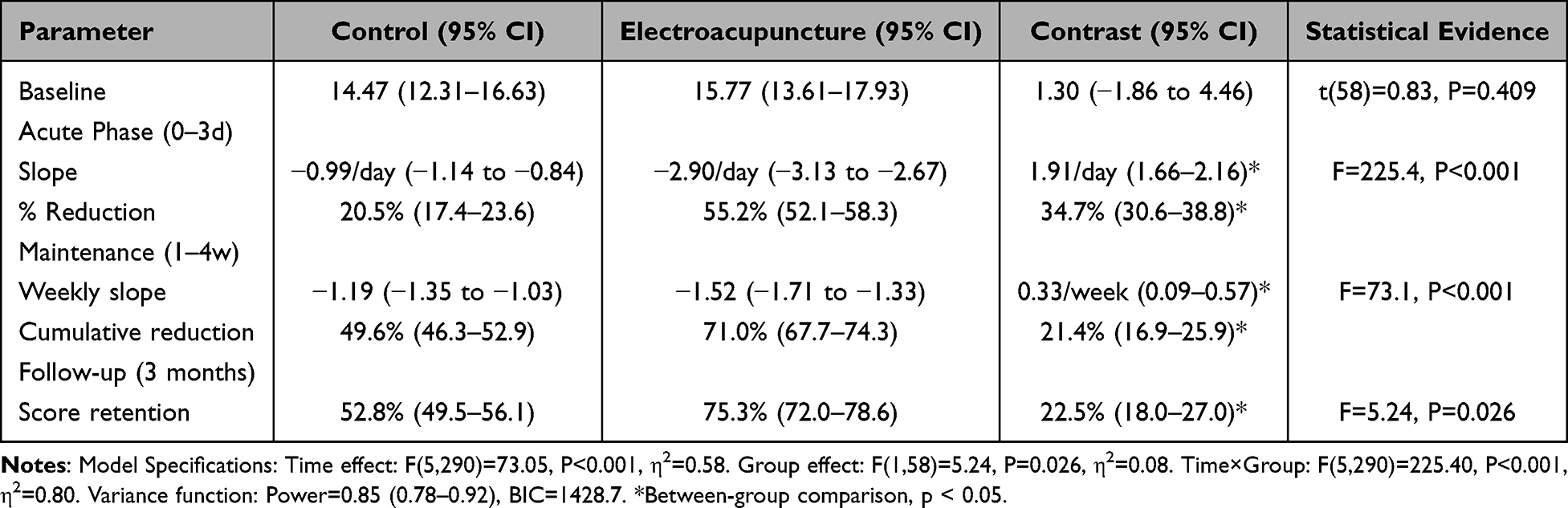 |
Table 6 Comparison of MNWS Scores Between Electroacupuncture and Drug Groups |
Maintenance phase (1–4 weeks): By the end of week 4, the cumulative reduction was 71.0% (95% CI: 67.7–74.3) in the electroacupuncture group, significantly higher than 49.6% (95% CI: 46.3–52.9) in the drug group, with a between-group difference of 21.4% (F = 73.1, P < 0.001, η2 = 0.58).
Follow-up phase (3 months): Electroacupuncture maintained 75.3% of the initial improvement, significantly higher than the 52.8% observed in the drug group (Δ = 22.5%, P = 0.026), show in Figure 5.
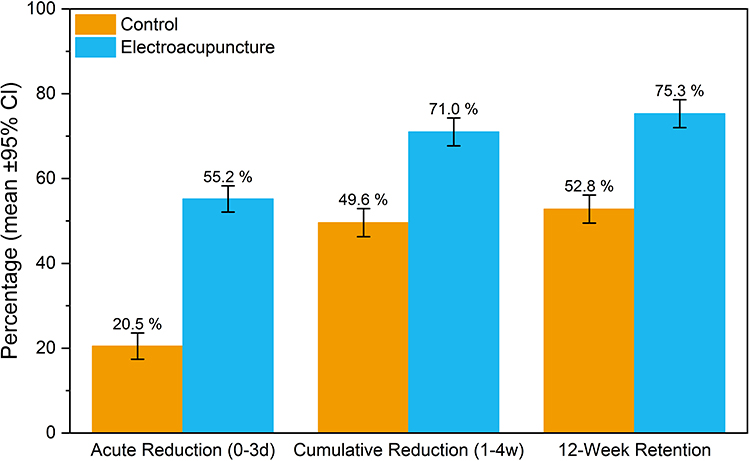 |
Figure 5 Key percentage outcomes of MNWS scores: Control vs Electroacupuncture (mean ± 95% CI). |
Overall, electroacupuncture demonstrated significantly greater improvements in withdrawal symptoms during both the acute and maintenance phases, and these effects were better preserved at follow-up compared with drug therapy.
Comparison of Cigarette Consumption Scores
At baseline, there was no significant difference in cigarette consumption scores between groups (P = 0.899), confirming the validity of randomization.
Acute phase (0–3 days): The rate of reduction in cigarette consumption was −0.27 cigarettes/day (95% CI: −0.30 to −0.24) in the electroacupuncture group, significantly faster than −0.03 cigarettes/day in the drug group (Δ = 0.24/day, P < 0.001). After 3 days, the electroacupuncture group had reduced cigarette consumption by 50.9%, compared with only 6.5% in the drug group.
Maintenance phase (1–4 weeks): At the end of 4 weeks, the cumulative reduction was 76.4% (95% CI: 73.1–79.7) in the electroacupuncture group, significantly greater than 58.8% (95% CI: 54.5–63.1) in the drug group (F = 175.3, P < 0.001, η2 = 0.58), reflecting a between-group difference of 17.6% show in Table 7.
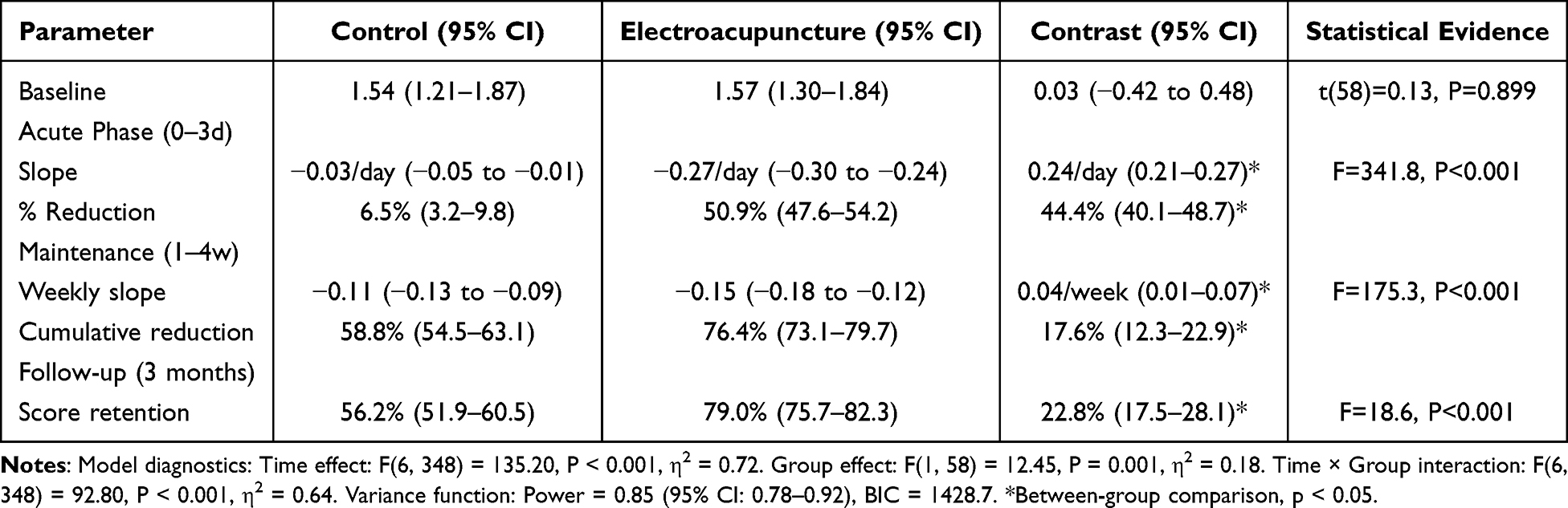 |
Table 7 Comparison of Cigarette Consumption Scores Between Electroacupuncture and Drug Groups |
Follow-up phase (3 months): The electroacupuncture group maintained 79.0% (95% CI: 75.7–82.3) of the initial improvement, significantly higher than 56.2% (95% CI: 51.9–60.5) in the drug group (Δ = 22.8%, P < 0.001), show in Figure 6.
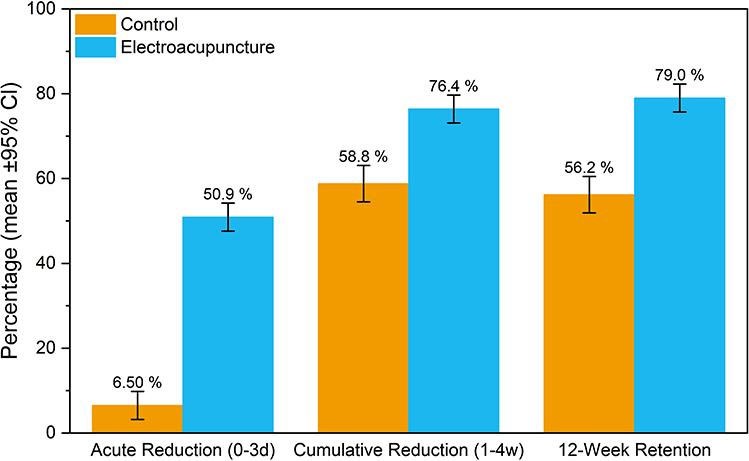 |
Figure 6 Key percentage outcomes of Smoking volume scores in the control and electroacupuncture groups (mean ± 95% CI). |
Overall, electroacupuncture resulted in a significantly faster and more sustained reduction in cigarette consumption compared with varenicline.
In summary, across the five core efficacy indicators—FTND, HSI, QSU-Brief, MNWS, and cigarette consumption—the electroacupuncture group demonstrated significantly greater improvement rates compared to the pharmacotherapy group during the acute phase (0–3 days), as evidenced by a more rapid decline in scores (P < 0.001). During the maintenance phase (1–4 weeks), the electroacupuncture group showed significantly greater cumulative reductions in four of the five indicators (excluding QSU-Brief) relative to the pharmacotherapy group (P < 0.001). At long-term follow-up (3 months), the electroacupuncture group maintained significantly higher rates of improvement retention in FTND, HSI, MNWS, and cigarette consumption compared to the pharmacotherapy group (P < 0.05), whereas both groups exhibited comparable retention rates for QSU-Brief (P = 0.542). Overall, electroacupuncture demonstrated superior efficacy in alleviating nicotine dependence, reducing smoking severity and withdrawal symptoms, and modifying smoking behavior, characterized by a faster onset of action, stronger cumulative effects, and more sustained therapeutic benefits.
Safety Evaluation
During the treatment period, one participant in the drug group (n = 31) and one in the electroacupuncture group (n = 31) withdrew, resulting in a total dropout rate of 2/62.
In the drug group, show in Table 8, mild adverse reactions were observed in 41.94% of participants (13/31) during varenicline treatment, including nausea in 9 cases (29.03%), constipation in 2 cases (6.45%), and insomnia in 2 cases (6.45%). All adverse reactions occurred within 3–14 days of treatment initiation and gradually subsided thereafter. Only one participant discontinued treatment due to drug intolerance.
 |
Table 8 Adverse Events Recorded in the Two Groups |
In the electroacupuncture group, one participant withdrew due to intolerance of needle sensation.
Discussion
This study systematically evaluated the efficacy and safety of electroacupuncture for nicotine dependence using a multimodal assessment strategy. By monitoring changes in nicotine dependence severity, craving, cigarette consumption, and withdrawal symptoms, we found that electroacupuncture produced more significant improvements than varenicline, effectively reducing the likelihood of relapse and increasing cessation success rates. Importantly, electroacupuncture demonstrated a faster onset of action, with therapeutic effects maintained up to three months after treatment. These findings provide high-quality clinical evidence supporting electroacupuncture as a green, effective, non-pharmacological intervention for smoking cessation.
Electroacupuncture significantly reduced nicotine dependence. In the acute phase, the rate of FTND score reduction in the electroacupuncture group was −1.11 points/day, 3.4 times faster than the drug group (−0.33 points/day, P < 0.001). At follow-up, 84.4% of the initial improvement was retained in the electroacupuncture group, significantly higher than the 69.5% in the drug group (P < 0.001).
Electroacupuncture effectively reduced smoking severity as measured by the HSI. In the acute phase, the electroacupuncture group achieved within three days the absolute reduction that required 25 days in the drug group (1.86 vs 0.36 points). At follow-up, the electroacupuncture group retained 81.7% of initial improvement, compared with 63.9% in the drug group (P = 0.002).
Electroacupuncture also alleviated withdrawal symptoms more effectively. On the MNWS, the electroacupuncture group eliminated 55.2% of withdrawal symptoms within three days, compared with only 20.5% in the drug group. At follow-up, retention of improvement remained significantly higher in the electroacupuncture group (75.3% vs 52.8%, P = 0.026).
Electroacupuncture reduced cigarette consumption more rapidly and sustainably. In the acute phase, cigarette consumption declined by 50.9% in the electroacupuncture group versus only 6.5% in the drug group. At three months, the electroacupuncture group retained 79.0% of the initial reduction, significantly higher than 56.2% in the drug group (P < 0.001).
Interestingly, the effect of electroacupuncture on psychological craving was comparable to that of varenicline. According to QSU-Brief scores, no significant differences were observed between groups at week 4 or during follow-up (P > 0.05). Several mechanisms may account for this equivalence: (1) both interventions modulate the dopaminergic reward system, thereby reducing nicotine dependence;24 (2) both alleviate withdrawal-related negative emotions, such as anxiety and depression, with prior evidence showing electroacupuncture is as effective as varenicline in improving mood disturbances;25 (3) electroacupuncture may regulate addiction-related neural pathways, such as NRG3/ErbB4 signaling in the hippocampus, thereby affecting synaptic plasticity and weakening craving-related memory consolidation;26 (4) the use of the “Sweet Point”, widely applied in smoking cessation, may alter taste perception during smoking (eg, inducing bitter, astringent, or metallic sensations), thereby reducing smoking-related pleasure.27 Varenicline similarly diminishes the rewarding effect of nicotine, which may explain the comparable efficacy in psychological craving.
The earliest documented reports on the use of acupoints for the treatment of drug addiction date back to the late Republic of China period, appearing in Dr. Huang Hanru’s “Manual of One-Finger Meditation Massage – Miscellaneous Notes”. Subsequently, medical practitioners evolved the approach from manual acupressure to acupuncture and eventually to electroacupuncture. In modern times, building upon research into the analgesic mechanisms of acupuncture—particularly its influence on endogenous opioid peptides28—electroacupuncture has emerged as a non-pharmacological intervention grounded in the principle of “physiological regulation” and has been widely validated for its efficacy in substance use disorders.29
First, in terms of mechanism of action, electroacupuncture exhibits multi-system regulatory capabilities that extend beyond single-receptor targeting. Varenicline acts selectively on the α4β2 nicotinic acetylcholine receptor,11 whereas electroacupuncture exerts networked neuromodulatory effects. Studies have demonstrated that low-frequency (2 Hz) electroacupuncture not only activates μ and δ opioid receptors,30 promoting the release of endorphins, enkephalins, and endomorphins to alleviate negative affective states and withdrawal-related pain, but also concurrently modulates monoamine neurotransmitters such as norepinephrine and serotonin.31 This dual action contributes to synergistic improvements in anxiety, depression, and other emotional disturbances associated with withdrawal. The capacity to simultaneously engage multiple endogenous neurochemical systems represents a therapeutic advantage that single-target pharmacological agents cannot easily replicate.
Second, regarding depth of intervention, electroacupuncture can directly target core pathological processes in addiction—namely neuroadaptation and addiction memory. Addiction is fundamentally a disorder of maladaptive learning and memory. Evidence indicates that low-frequency electroacupuncture can attenuate the consolidation and reactivation of addiction memories by restoring homeostasis between the cholinergic and dopaminergic systems in the hippocampus.32 This contrasts sharply with varenicline, which primarily blocks acute reward signaling. By intervening at the level of memory formation and retrieval, electroacupuncture offers a more fundamental strategy for preventing relapse.
Finally, at the level of neural system repair, electroacupuncture demonstrates protective and restorative effects on impaired neural circuits. As shown in preliminary data from this study, morphine or heroin dependence induces adaptive changes in receptors within the dopamine projection pathways. Electroacupuncture not only suppresses craving behaviors and withdrawal symptoms but also normalizes the aberrant expression of dopamine receptors, thereby protecting neuronal integrity and facilitating functional recovery of the dopaminergic system.33,34 These findings suggest that the “physiological regulation” achieved through electroacupuncture transcends mere substitution or blockade; rather, it involves active “guidance” and “repair”, promoting the restoration of disrupted neural networks to physiological homeostasis.
In this study, we selected bilateral PC6 (Neiguan), HT7 (Shenmen), ST36 (Zusanli), SP6 (Sanyinjiao), Huatuojiaji (T5), BL23 (Shenshu), and the Sweet Point. Electroacupuncture was delivered to bilateral Huatuojiaji (T5) and BL23, with the positive pole connected to Huatuojiaji (T5) and the negative pole to BL23. Each acupoint has specific therapeutic effects: PC6 is associated with harmonizing the stomach, regulating qi, and calming the mind;35 HT7 calms the spirit;36 ST36 strengthens the body and tonifies qi;37 SP6 harmonizes the spleen, liver, and kidney;38 Huatuojiaji (T5), in combination with PC6, has been shown to alleviate anxiety and depression following withdrawal;39 the Sweet Point modifies taste perception during smoking, thereby reducing craving.40 A 2 Hz stimulation frequency was chosen, consistent with prior evidence that low-frequency electroacupuncture effectively suppresses craving-related behavior.41
This study systematically evaluated the efficacy and safety of electroacupuncture in the treatment of nicotine dependence. The results demonstrated that electroacupuncture significantly outperformed varenicline in reducing nicotine dependence (FTND), smoking severity (HSI), withdrawal symptoms (MNWS), and cigarette consumption, with this therapeutic advantage being sustained throughout the 3-month follow-up period. Regarding psychological craving, as assessed by the QSU-Brief, electroacupuncture exhibited comparable efficacy to pharmacological treatment, suggesting its potential to achieve similar long-term effects in mitigating psychological dependence. These findings indicate that electroacupuncture may serve as a promising non-pharmacological therapeutic option for clinical smoking cessation.
Limitations of this study should be acknowledged.
Because of the inherent differences between interventions, participant-reported outcomes (eg, craving scores) may have been influenced by expectancy effects, with acupuncture’s sensory stimulation potentially enhancing placebo response, and varenicline’s side effects possibly undermining blinding. To minimize bias, we used blinded evaluators, standardized questionnaires, strict operator training (48 h; Kappa ≥ 0.85), fixed acupoint selection, and independent monitoring, with varenicline serving as an active control to address ethical concerns about sham acupuncture.
Future studies may extend the follow-up period to 6 months or 1 year. While the 3-month follow-up in this study effectively captures the mid-term stability and trajectory of withdrawal symptom alleviation and demonstrates sustained advantages of electroacupuncture, it is insufficient for a comprehensive assessment of long-term outcomes—such as abstinence rates and relapse risk—in nicotine dependence. Given the chronic nature of nicotine dependence, long-term outcomes warrant substantial clinical attention. Although the maintenance of efficacy at 3 months provides a promising early indicator of potential long-term success, further research with extended follow-up periods is necessary to definitively establish the durability of electroacupuncture’s therapeutic effects.
The study relied on validated behavioral scales (FTND, HSI, QSU-Brief, MNWS) but did not include biochemical validation (eg, urinary or salivary cotinine). Future research should incorporate biomarkers to improve objectivity.
This study was conducted in a Chinese population, where cultural acceptance of acupuncture is higher than in many Western regions, potentially influencing adherence and expectancy effects. Replication in diverse populations is necessary to enhance external validity and global generalizability.
This study did not include a control group receiving standard behavioral interventions, such as the 5A approach. Although this design is consistent with the primary objective of comparing electroacupuncture with first-line pharmacotherapy, future studies employing a three-arm trial design—incorporating behavioral intervention, pharmacotherapy, and electroacupuncture groups—would allow for a more comprehensive and precise evaluation of electroacupuncture’s distinct contribution and clinical value across the spectrum of smoking cessation strategies.
In conclusion, this study demonstrates that electroacupuncture is a safe and effective non-pharmacological intervention for nicotine dependence. Electroacupuncture significantly reduced dependence severity, craving, withdrawal symptoms, and cigarette consumption, with sustained benefits up to three months. For patients intolerant of pharmacotherapy, with contraindications, or preferring non-drug options, electroacupuncture may represent a valuable alternative or complementary therapy. Integrating electroacupuncture into clinical smoking cessation programs could be especially beneficial for individuals who have failed conventional methods or are reluctant to rely on long-term pharmacological treatment. With its high acceptance, minimal side effects, and sustained efficacy, electroacupuncture offers a novel strategy for tobacco control and public health promotion.
Data Sharing Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethical Statement
This experiment follows the Helsinki Declaration and has been approved by the Ethics Committee of Shanghai Yueyang Integrated Traditional Chinese and Western Medicine Hospital (No. 2024-042). The registration number of China Clinical Trial Registry is ChiCTR2400087626.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was supported by This study was funded by the National Natural Science Foundation of China (81403473); Key Discipline (Specialty) of Integrated Traditional Chinese and Western Medicine and Advantageous Specialty Construction Project of Public Hospital Reform and High Quality Development in Jiading District, Shanghai (JDZXYSZK04); Public Hospital Reform and High-Quality Development Initiative: The “Jiading Medical Elite” Talent Cultivation Plan (JDLCXLQNXZ-17). The Pudong New Area Demonstration Project for Inheritance and Innovation of Traditional Chinese Medicine (YC-2023-0901).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. National Center for Chronic Disease Prevention and Health Promotion (US). Office on smoking and health. the health consequences of smoking—50 years of progress: a report of the surgeon general. Atlanta (GA): Centers for Disease Control and Prevention (US); 2014. PMID: 24455788.
2. Hartmann-Boyce J, Chepkin SC, Ye W, Bullen C, Lancaster T. Nicotine replacement therapy versus control for smoking cessation. Cochrane Database Syst Rev. 2018;5(5):CD000146. PMID: 29852054; PMCID: PMC6353172. doi:10.1002/14651858.CD000146.pub5
3. Benowitz NL. Nicotine addiction. N Engl J Med. 2010;362(24):2295–2303. PMID: 20554984; PMCID: PMC2928221. doi:10.1056/NEJMra0809890
4. GBD 2021 Tobacco Forecasting Collaborators. Forecasting the effects of smoking prevalence scenarios on years of life lost and life expectancy from 2022 to 2050: a systematic analysis for the global burden of disease study 2021. Lancet Public Health. 2024;9(10):e729–e744. PMID: 39366729; PMCID: PMC11447278. doi:10.1016/S2468-2667(24)00166-X
5. Xiao D, Wang C. Tobacco dependence should be recognised as a lethal non-communicable disease. BMJ. 2019;365:l2204. PMID: 31113798. doi:10.1136/bmj.l2204
6. Ezzati M, Lopez AD. Estimates of global mortality attributable to smoking in 2000. Lancet. 2003;362(9387):847–852. PMID: 13678970. doi:10.1016/S0140-6736(03)14338-3
7. National Respiratory Medicine Center, Chinese Medical Association Respiratory Disease Branch Tobacco Disease Study Group. Clinical Application Guidelines for Nicotine Replacement Therapy. Beijing: People’s Medical Publishing House; 2025.
8. Streck JM, Rigotti NA, Livingstone-Banks J, et al. Interventions for smoking cessation in hospitalised patients. Cochrane Database Syst Rev. 2024;5(5):CD001837. PMID: 38770804; PMCID: PMC11106804. doi:10.1002/14651858.CD001837.pub4
9. Samarasekera U. WHO’s ninth report on the global tobacco epidemic. Lancet Oncol. 2023;24(9):957. PMID: 37544312. doi:10.1016/S1470-2045(22)00341-2
10. Qingwen T. Acupuncture for smoking cessation. J Luzhou Med College. 1978;(04):79–80.
11. Li JW. Huangdi Neijing and Huangdi Waijing compiled in the Western Zhou. Zhonghua Yi Shi Za Zhi. 2021;51(1):43–49. PMID: 33794583. Chinese. doi:10.3760/cma.j.cn112155-20200928-00154
12. Zhang RJ, Hou XR, Cai XH, et al. Acupuncture effects on synaptic ultrastructure and synaptic cytoskeletal proteins in heroin relapse rats. Acupunct Res. 2019;44(05):324–328. doi:10.13702/j.1000-0607.180437
13. Gao XY, Liang Y, Huo LL, et al. The effects of warm acupuncture on the delayed withdrawal symptoms of heroin-dependent patients with kidney-yang deficiency. Shanghai J Acupunct Moxibustion. 2021;40(10):1217–1222. doi:10.13460/j.issn.1005-0957.2021.10.1217
14. Xu P, Li Y, Luo JX, et al. Rough Set data analysis of acupuncture treatment for delayed symptoms in heroin addicts after detoxification. Shanghai J Traditional Chin Med. 2007;(04):55–57. doi:10.16305/j.1007-1334.2007.04.027
15. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. J Pharmacol Pharmacother. 2010;1(2):100–107. PMID: 21350618; PMCID: PMC3043330. doi:10.4103/0976-500X.72352
16. STRICTA Revision Group; MacPherson H, Altman DG, Hammerschlag R, et al. Revised STandards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. Acupunct Med. 2010;28(2):83–93. PMID: 20615861; PMCID: PMC3002761. doi:10.1136/aim.2009.001370
17. World Health Organization (WHO). The ICD-10 Classification of Mental and Behavioral Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: World Health Organization; 1992.
18. World Health Organization. WHO Standard Acupuncture Point Locations in the Western Pacific Region. Geneva: World Health Organization; 2008.
19. Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The fagerström test for nicotine dependence: a revision of the fagerström tolerance questionnaire. Br J Addict. 1991;86(9):1119–1127. PMID: 1932883. doi:10.1111/j.1360-0443.1991.tb01879.x
20. Kaplan KA, Plante DT, Cook JD, Harvey AG. Development and validation of the Hypersomnia Severity Index (HSI): a measure to assess hypersomnia severity and impairment in psychiatric disorders. Psychiatry Res. 2019;281:112547. PMID: 31494450; PMCID: PMC6961815. doi:10.1016/j.psychres.2019.112547
21. Toll BA, Katulak NA, McKee SA. Investigating the factor structure of the questionnaire on smoking urges-brief (QSU-Brief). Addict Behav. 2006;31(7):1231–1239. PMID: 16226843; PMCID: PMC2527734. doi:10.1016/j.addbeh.2005.09.008
22. Blebil AQ, S Sulaiman SA, A Hassali M, Dujaili JA, Zin AM. Evaluation of the psychometric properties of the Malay version of the minnesota nicotine withdrawal scale. Value Health Reg Issues. 2014;3:19–23. PMID: 29702926. doi:10.1016/j.vhri.2013.09.001
23. Wang C, Xiao D, Chan KP, Pothirat C, Garza D, Davies S. Varenicline for smoking cessation: a placebo-controlled, randomized study. Respirology. 2009;14(3):384–392. PMID: 19192221. doi:10.1111/j.1440-1843.2008.01476.x
24. Yoon SS, Lee BH, Lee SH, et al. Effects of isoflurane anesthesia on addictive behaviors in rats. Psychopharmacology. 2022;239(11):3621–3632. PMID: 36109391. doi:10.1007/s00213-022-06236-z
25. Wang JH, van Haselen R, Wang M, et al. Acupuncture for smoking cessation: a systematic review and meta-analysis of 24 randomized controlled trials. Tob Induc Dis. 2019;17(June):48. PMID: 31516491; PMCID: PMC6662782. doi:10.18332/tid/109195
26. Zhang WT, Zhu BC, Yang JS, et al. The effect of acupuncture on hippocampal NRG3/ErbB4 pathway in nicotine addiction rats and its influence on withdrawal symptoms. Chin J Integr Med. 2025;40(02):550–556.
27. Chen SM, Liu ZY, Ji J, et al. Auricular acupressure combined with transcutaneous electrical acupoint stimulation for smoking cessation: a randomized controlled trial. Chin Acupunct Moxibustion. 2022;42(11):1235–1239. doi:10.13703/j.0255-2930.20220104-k0001
28. Wang XJ, Zhu WH, Gao YM, et al. Understanding and research on the mechanism of acupuncture for smoking cessation. Shaanxi J Tradit Chin Med. 2011;32(09):1266–1269.
29. Xu Y, Xu MY. Current research status of opioid addiction withdrawal mechanisms and treatments. Harbin Med Univ J. 2005;(02):198–201.
30. Han JS, Chen XH, Sun SL, et al. Effect of low- and high-frequency TENS on Met-enkephalin-Arg-Phe and dynorphin A immunoreactivity in human lumbar CSF. Pain. 1991;47(3):295–298. PMID: 1686080. doi:10.1016/0304-3959(91)90218-M
31. Chen XH, Han JS. Analgesia induced by electroacupuncture of different frequencies is mediated by different types of opioid receptors: another cross-tolerance study. Behav Brain Res. 1992;47(2):143–149. PMID: 1350448. doi:10.1016/s0166-4328(05)80120-2
32. Kutralam-Muniasamy G, Pérez-Guevara F. Evolutionary relationships between the transcriptional repressors of the polyhydroxyalkanoate reserve storage system in prokaryotes: conserved but phylogenetically heterogeneous. Gene. 2020;735:144397. PMID: 31991161. doi:10.1016/j.gene.2020.144397
33. Yan L, Liang Z, Yanjin Z, et al. Effects of electroacupuncture on central dopaminergic neurons in morphine-addicted rats. J Shanghai University Trad Chin Med. 2017;31(06):86–90. doi:10.16306/j.1008-861x.2017.06.020
34. Dongsheng L, Bingxia L, Yajie W, et al. Overview of clinical application research on acupuncture anesthesia. Clin J Trad Chin Med. 2024;36(11):2228–2232. doi:10.16448/j.cjtcm.2024.1141
35. Liang Y, Huang Y, Cheng B, et al. Clinical observation of electroacupuncture at Neiguan (PC6) and Shenmen (HT7) for heroin-dependent patients with delayed withdrawal symptoms. Shanghai J Acupunct Moxibustion. 2011;30(12):804–806.
36. Zhu TT, Hu XQ, Ruan YF. Research progress on acupuncture treatment for senile insomnia. Chin J Clin Res. 2022;14(08):130–134.
37. Li M, Liu NN, Zhang JQ, et al. The effects of pre-acupuncture at Zusanli (ST36) on memory T cells in skin and adjacent lymph nodes in mice. J Chengdu Univ TCM. 2021;44(04):9–14. doi:10.13593/j.cnki.51-1501/r.2021.04.009
38. Du L, Song XJ, Li ZW, et al. The effects of acupuncture at Shenmen (HT7) and Sanyinjiao (SP6) on anxiety and depression in insomnia patients: a randomized controlled study. Chin Acupunct Moxibustion. 2022;42(01):13–17. doi:10.13703/j.0255-2930.20210113-k0002
39. Zheng MF, Xie CP, He FR, et al. Effects of transcutaneous acupoint electrical stimulation on delayed withdrawal syndrome in male synthetic drug dependents. Fujian J Tradit Chin Med. 2018;49(05):8–11. doi:10.13260/j.cnki.jfjtcm.011688
40. Wang LY. Clinical efficacy analysis of acupuncture at the Tianmei point for smoking cessation in 105 cases. Sichuan J Tradit Chin Med. 2001;(05):74–75.
41. Liang Y, Zhang XC, Xu B, et al. Clinical observation of electroacupuncture for methamphetamine-dependent patients with withdrawal symptoms. Shanghai J Acupunct Moxibustion. 2014;33(04):287–290. doi:10.13460/j.issn.1005-0957.2014.04.0287
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.