Back to Journals » Patient Preference and Adherence » Volume 13
Efficient development and usability testing of decision support interventions for older women with breast cancer
Authors Lifford KJ ![]() , Edwards A
, Edwards A ![]() , Burton M
, Burton M ![]() , Harder H
, Harder H ![]() , Armitage F, Morgan JL, Caldon L, Balachandran K, Ring A, Collins K, Reed M, Wyld L, Brain K
, Armitage F, Morgan JL, Caldon L, Balachandran K, Ring A, Collins K, Reed M, Wyld L, Brain K
Received 26 June 2018
Accepted for publication 7 September 2018
Published 14 January 2019 Volume 2019:13 Pages 131—143
DOI https://doi.org/10.2147/PPA.S178347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Kate J Lifford,1 Adrian Edwards,1 Maria Burton,2 Helena Harder,3 Fiona Armitage,4 Jenna L Morgan,4 Lisa Caldon,5 Kirsty Balachandran,6 Alistair Ring,7 Karen Collins,2 Malcolm Reed,8 Lynda Wyld,4 Kate Brain1
1Division of Population Medicine, Cardiff University, Cardiff, UK; 2Faculty of Health and Wellbeing, Sheffield Hallam University, Sheffield, UK; 3Sussex Health Outcomes Research and Education in Cancer, Brighton and Sussex Medical School, University of Sussex, Brighton, UK; 4Department of Oncology and Metabolism, University of Sheffield, Sheffield, UK; 5Department of General Surgery, The Rotherham NHS Foundation Trust, Rotherham, UK; 6Department of Medical Oncology, Imperial College London, London, UK; 7Breast Unit, Royal Marsden Hospital NHS Foundation Trust, Sutton, UK; 8Brighton and Sussex Medical School, Brighton, UK
Background: Around one-third of breast cancers diagnosed every year in the UK are in women aged ≥70 years. However, there are currently no decision support interventions (DESIs) for older women who have a choice between primary endocrine therapy and surgery followed by adjuvant endocrine therapy (surgery+endocrine therapy), or who can choose whether or not to have chemotherapy following surgery. There is also little evidence-based guidance specifically on the management of these older patients. A large UK cohort study is currently underway to address this lack of evidence and to develop two DESIs to facilitate shared decision-making with older women about breast cancer treatments. Here, we present the development and initial testing of these two DESIs.
Methods: An initial prototype DESI was developed for the choice of primary endocrine therapy or surgery+endocrine therapy. Semi-structured interviews with healthy volunteers and patients explored DESI acceptability, usability, and utility. A framework approach was used for analysis. A second DESI for the choice of having chemotherapy or not was subsequently developed based on more focused development and testing.
Results: Participants (n=22, aged 75–94 years, 64% healthy volunteers, 36% patients) found the primary endocrine therapy / surgery+endocrine therapy DESI acceptable, and contributed to improved wording and illustrations to address misunderstandings. The chemotherapy DESI (tested with 14 participants, aged 70–87 years, 57% healthy volunteers, 43% patients) was mostly understandable, however, suggestions for rewording sections were made. Most participants considered the DESIs helpful, but highlighted the importance of complementary discussions with clinicians.
Conclusion: It was possible to use a template DESI to efficiently create a second prototype for a different treatment option (chemotherapy). Both DESIs were acceptable and considered helpful to support/augment consultations. Development of acceptable additional DESIs for similar target populations using simplified methods may be an efficient way to develop future DESIs. Further research is needed to test the effectiveness of the DESIs.
Keywords: patient decision aids, decision support, shared decision-making, breast cancer, older patients
Introduction
Every year about one-third of all new invasive breast cancer diagnoses in the UK are in women aged ≥70 years.1 Several patient decision aids exist to support women with breast cancer when making treatment decisions.2 However, to date, none has been developed for older women with estrogen receptor positive breast cancer who have a choice between primary endocrine therapy and surgery followed by adjuvant endocrine therapy (surgery+endocrine therapy), or for older women with high recurrence risk breast cancers (eg, HER2 positive, estrogen receptor negative, node positive) who can choose whether or not to have chemotherapy following surgery. The current absence of decision support may, in part, reflect heterogeneous research and practice in managing breast cancer in older women.3–6
Research is needed to guide clinicians (this term is used to include all healthcare professionals) and patients about appropriate treatment for older women with estrogen receptor positive breast cancer and for older women with breast cancer with high recurrence risk. Surgery is the recommended treatment for breast cancer for those who are fit enough, that is, unless precluded due to comorbidities.7,8 However, the benefits of surgery vary in older women because life expectancy varies; there are some women for whom primary endocrine therapy may be as effective as surgery if they have a reduced life expectancy.9 For older women (70+), randomized trials have shown that while overall survival is not significantly different, primary endocrine therapy is less effective for local control9 and survival outcomes may be inferior on long-term follow-up.10 The decision for older women is therefore preference sensitive. There is evidence for benefit of chemotherapy following surgery for older women with high-risk breast cancer.7,11 However, the trial evidence to underpin this is weak relative to other age groups, side effects are more common in older women,12 and the benefits of chemotherapy are less marked than in younger women. Consequently, rates of adjuvant chemotherapy use are highly variable across the UK in this older population.13
The Bridging the Age Gap in Breast Cancer program (National Institute for Health Research Programme Grants for Applied Research programme RP-PG-1209–10071, ISRCTN46099296)14 aims to provide guidance to clinicians about management and to provide decision support for patients. As part of this program of work, decision support interventions (DESIs) for two treatment choices (primary endocrine therapy or surgery+endocrine therapy and adjuvant chemotherapy or no chemotherapy) were developed. DESIs are tools that aim to support shared decision-making between clinicians and patients. The DESIs developed as part of this study each included a brief decision aid to be used within a consultation (a table of frequently asked questions with the answers for each treatment option), along with a booklet for patients which provided detailed information and a values clarification exercise (see “Methods” for more details) for use at home, with family or friends if desired. Guidelines from the International Patient Decision Aid Standards (IPDAS)15 were consulted for advice on areas such as how to best present probabilities. An online algorithm to predict individual survival outcomes under each treatment option has also been developed (similar to Adjuvant! Online16 and PREDICT17)for clinicians to use alongside the DESIs in clinical practice, which permits some tailoring of outcomes for the different options according to disease stage and type, age, and fitness. Development and usability testing of the brief decision aids and booklets are the focus of the present study.
Although it has been assumed that older cancer patients have stronger preferences for taking passive roles (doctor-centered or paternalistic decision-making) in the decision-making process than younger patients,18–20 recent evidence suggests that many older cancer patients do want to be involved in treatment decisions,20 including women with breast cancer.21–24 Preferences for decision-making style vary amongst older women with breast cancer treatment decisions.22,23 In a questionnaire survey of women aged ≥75 years who had previously had a choice of primary endocrine therapy or surgery+endocrine therapy, preferences for patient-centered or doctor-centered decision-making were fairly even (39% and 38%, respectively) with slightly fewer preferring shared decision-making (24%).22 Most women discussing chemotherapy were found to prefer to be involved in decision-making.23 DESIs improve knowledge, accuracy of risk perception, and participation in decision-making as well as decreasing aspects of decisional conflict in decision-making in older samples.25 They may therefore be particularly useful for clinicians and older women.
When developing DESIs it is important to use a transparent and systematic approach.15 This includes an initial needs assessment and collating and summarizing the clinical evidence.15 Another integral part of DESI development is usability testing, before finalizing it for effectiveness testing and implementation.26 This consists not only of checking the DESI for clarity and understanding but also for its perceived usefulness by the target population and potential implementation barriers and facilitators. Field testing with patients facing the decision and their clinicians involved in shared decision-making about the decision has been included as a criterion of decision aid quality in the IPDAS instrument (IPDASi).26,27 The aims of the present study were to 1) develop two DESIs (primary endocrine therapy / surgery+endocrine therapy and chemotherapy) for older women with breast cancer treatment choices, with a more focused development and testing stage for the second DESI and 2) test the DESIs for usability, acceptability, and utility amongst older participants.
Methods
Prototype development
Approval for healthy volunteer involvement in the study was obtained from Cardiff University School of Medicine Research Ethics Committee (reference 13/72) and Brighton and Sussex Medical School Research Governance and Ethics Committee (reference 15/111/HAR). Approval of the study protocol for patient involvement was obtained from the National Research Ethics Service London – Surrey Borders committee (reference 12/LO/1722) and the appropriate National Health Service Trust Research and Development Departments.
Primary endocrine therapy / surgery+endocrine therapy DESI
A schematic representation of DESI development is shown in Figure 1. The prototype DESI (brief decision aid plus booklet) was initially based on literature reviews and analyses of previous patient interviews conducted by members of the group9,10,18,21,24 and was developed using an iterative process. Literature reviews of the clinical evidence and patient informational needs and preferences were conducted. Existing breast cancer treatment decision aids were also reviewed. Data from patient interviews21,24 and a focus group with healthy female volunteers in a similar age group (not reported here) were collected and a summary of all the collated evidence was produced. The Coping in Deliberation (CODE) framework28 was the theoretical basis for the DESI.24 The CODE framework highlights that cognitions, emotions, and coping are important in healthcare decisions throughout the deliberation process.28 The DESI therefore addressed cognitive and emotional processes throughout deliberation as well as coping resources. The CODE framework was previously adapted for the decision about primary endocrine therapy or surgery+endocrine therapy in older women,24 and this was included within the overall evidence summary which guided the content of the DESI. An expert reference group consisting of 15 experts in the field (plus a chair from the study management group) reviewed the clinical evidence summary in detail (they also had the opportunity to comment on a draft prototype and the overall evidence summary). The overall summary was used as a basis for the DESI content. Guidelines from the Plain English Campaign29 were followed and editorial suggestions to improve the readability of the DESI were received from the Plain English Campaign29 before testing with patients (the final brief decision aid and booklet had “Crystal Marks” for clarity from the Plain English Campaign29). Feedback from healthcare professionals (n=3) who used the DESI during testing with patients was used to improve the DESI (not reported here). An outline of the DESI content is shown in Figure 2.
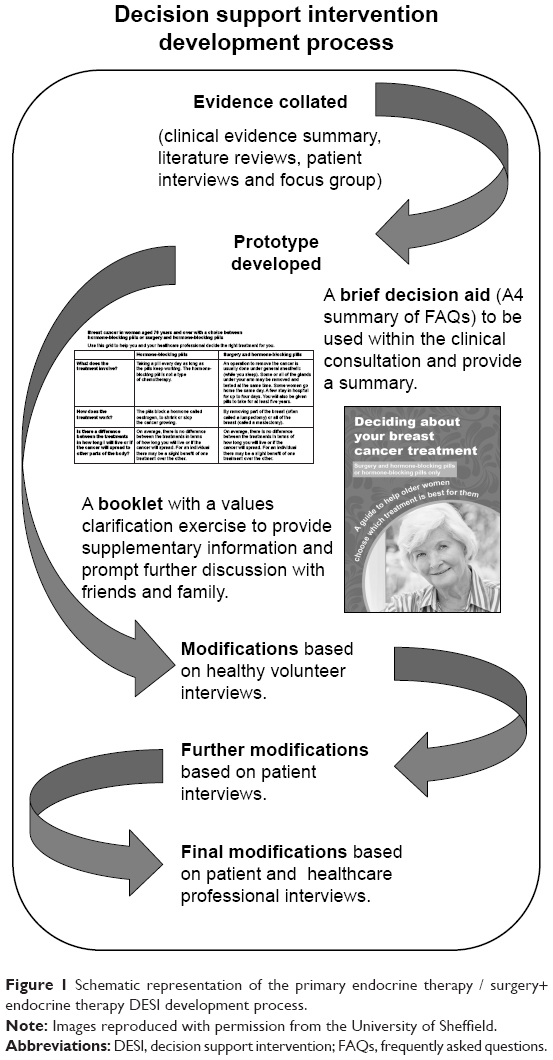 | Figure 1 Schematic representation of the primary endocrine therapy / surgery+endocrine therapy DESI development process. |
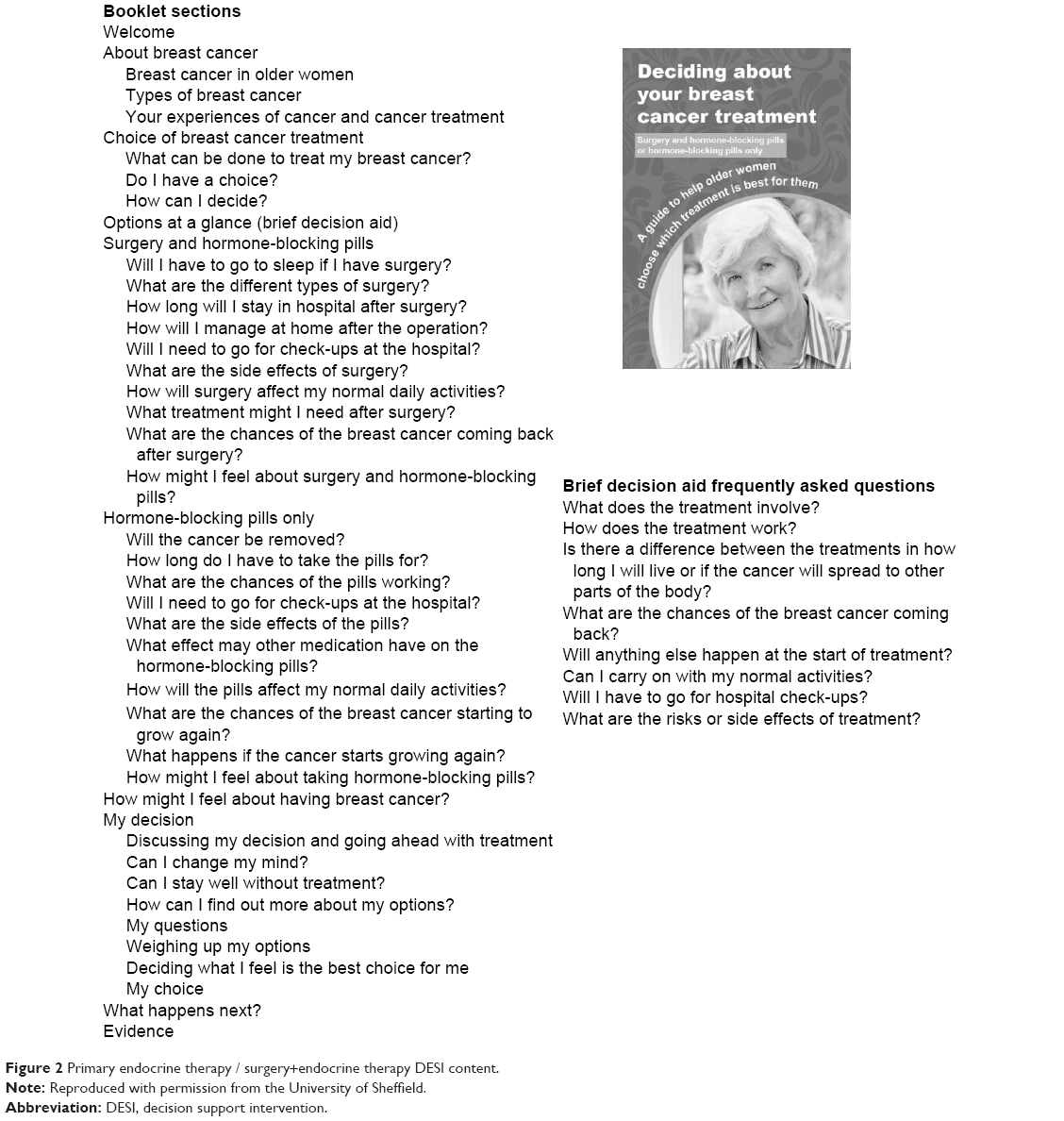 | Figure 2 Primary endocrine therapy / surgery+endocrine therapy DESI content. |
Chemotherapy DESI
A similar but more focused method was used to develop the prototype chemotherapy DESI. Content was based on analysis of patient interviews23 and a review of the published clinical evidence about chemotherapy use in older women by a small group of experts. The format and style (and some of the wording/headings/questions where appropriate) of this DESI were based on the primary endocrine therapy / surgery+endocrine therapy DESI due to similarity between the patient populations. An outline of the chemotherapy DESI content is shown in Figure 3.
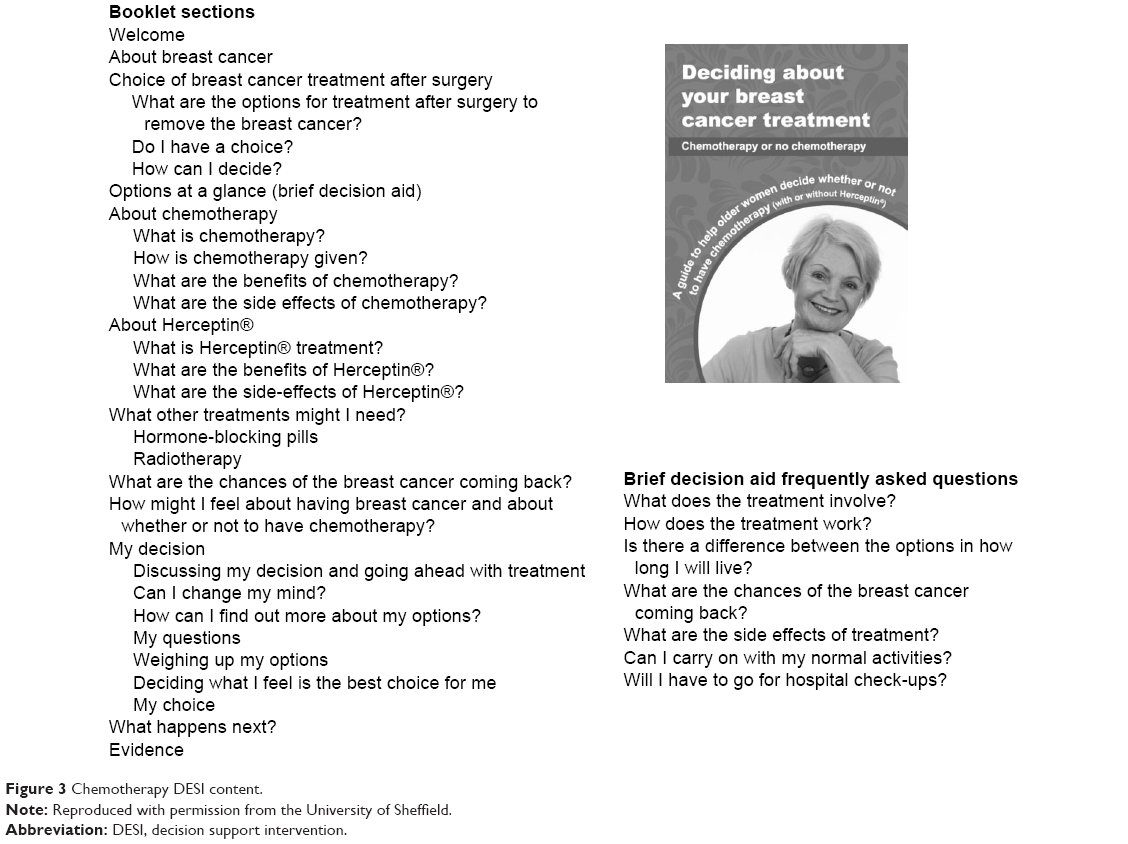 | Figure 3 Chemotherapy DESI content. |
Usability testing
Following initial development, both prototype DESIs (both brief decision aid and booklet for each decision) were tested for usability, acceptability, and utility using semi-structured interviews (Supplementary material). To minimize burden among women diagnosed with breast cancer, preliminary testing was first conducted among healthy volunteers aged ≥70 years (≥75 years for the primary endocrine therapy / surgery+endocrine therapy DESI). This was followed by testing with patients who had made a breast cancer treatment decision in the last 12 months, before finally testing the DESI (primary endocrine therapy / surgery+endocrine therapy DESI only) with those currently facing the treatment decision. Modifications to the DESIs were made between the two phases based on the results and further changes to the primary endocrine therapy / surgery+endocrine therapy DESI were made following patient feedback.
Sample recruitment
Volunteers
Female volunteers were recruited from a number of sources including breast cancer charities and local community groups (eg, older persons’ groups in churches and community centers). Emails and phone calls were made to various organizations and in some cases the researchers visited groups and either gave a presentation or had an informal discussion about the study. A snowball sampling method was used. Invitation packs (including invitation letter, information sheet, consent form, and prepaid envelope) were given to anyone interested.
Patients
Patients were recruited via four UK breast units: Cardiff, Doncaster, Sheffield, and Southampton. They were identified from other strands of the Bridging the Age Gap in Breast Cancer programme (having completed a form to register their interest) or from clinic records and multidisciplinary team meetings. Some patients who had already registered interest in the study were sent an invitation pack directly. Others were invited by a research nurse and/or their clinician.
Procedure
Completed consent forms were returned to the researcher, who then contacted the participants to answer any further questions about the study and arrange an interview. Participants were sent the relevant DESI along with a letter confirming their interview appointment. Semi-structured interviews were conducted at a place convenient to the participant (most in their home, one in a church, and six by telephone), and were audio-recorded if participants consented to this. Participants who used the DESI when they faced the decision of primary endocrine therapy or surgery+endocrine therapy and chose surgery were interviewed before surgery. The interview guide included the following topics: understanding of the content, layout, usefulness, and potential improvements of the DESI (Supplementary material).
Data analysis
Sections relevant to data analysis were transcribed. A framework30 approach was used to analyze the data. This included the following stages 1) familiarization of the data (both listening to the recordings and reading transcripts), 2) coding of the data (Table 1), 3) charting the data by each code, and 4) reviewing and summarizing each of the charted codes for the groups of participants. Data were initially coded by KL and 20% was double coded by HH or MB. Following discussions about discrepancies, all transcripts were recoded (KL). NVivo qualitative data analysis Software31 version 11 was used to manage the data.
 | Table 1 Interview transcript coding framework |
Results
Sample characteristics
Primary endocrine therapy / surgery+endocrine therapy DESI
Interviews were completed with 22 women: 14 were healthy volunteers, four were patients who had faced the decision in the last 12 months, and four were currently facing the decision when they first received the DESI. Women were aged between 75 and 94 years (median 82.5 years). Volunteers were from South Wales (n=9) and South West England (n=5). Patients were from South Wales (n=3), Wessex (n=3), and Yorkshire and the Humber (n=2). Of the eight patients, four were having primary endocrine therapy and four were due to have (currently facing the decision) or had undergone (previously faced the decision) surgery. Transcripts from 21 participants were analyzed. One participant chose not to be recorded, therefore, interviewer’s notes were analyzed.
Chemotherapy DESI
Interviews were completed with 14 women: eight were healthy volunteers and six were patients who had faced the decision in the last 12 months. Participants’ ages ranged from 70 to 87 years (median 74 years). Healthy volunteers from South Wales (n=3), South West England (n=1), and South England (n=4) were recruited and interviewed. Of the six patients, all of whom were from Yorkshire and the Humber, five had had chemotherapy and one had not.
DESI feedback
Results from the main analyses are presented in three sections below: primary endocrine therapy / surgery+endocrine therapy DESI content, chemotherapy DESI content, and DESI use/implementation (covering both DESIs). Sample quotes to demonstrate the findings are presented in Table 2 and referred to in the text in parentheses. Each quote is followed by a description of the participant characteristics as follows: DESI viewed, which element they are referring to, and which part of the testing they were involved with (see Table 1 footnote for details).
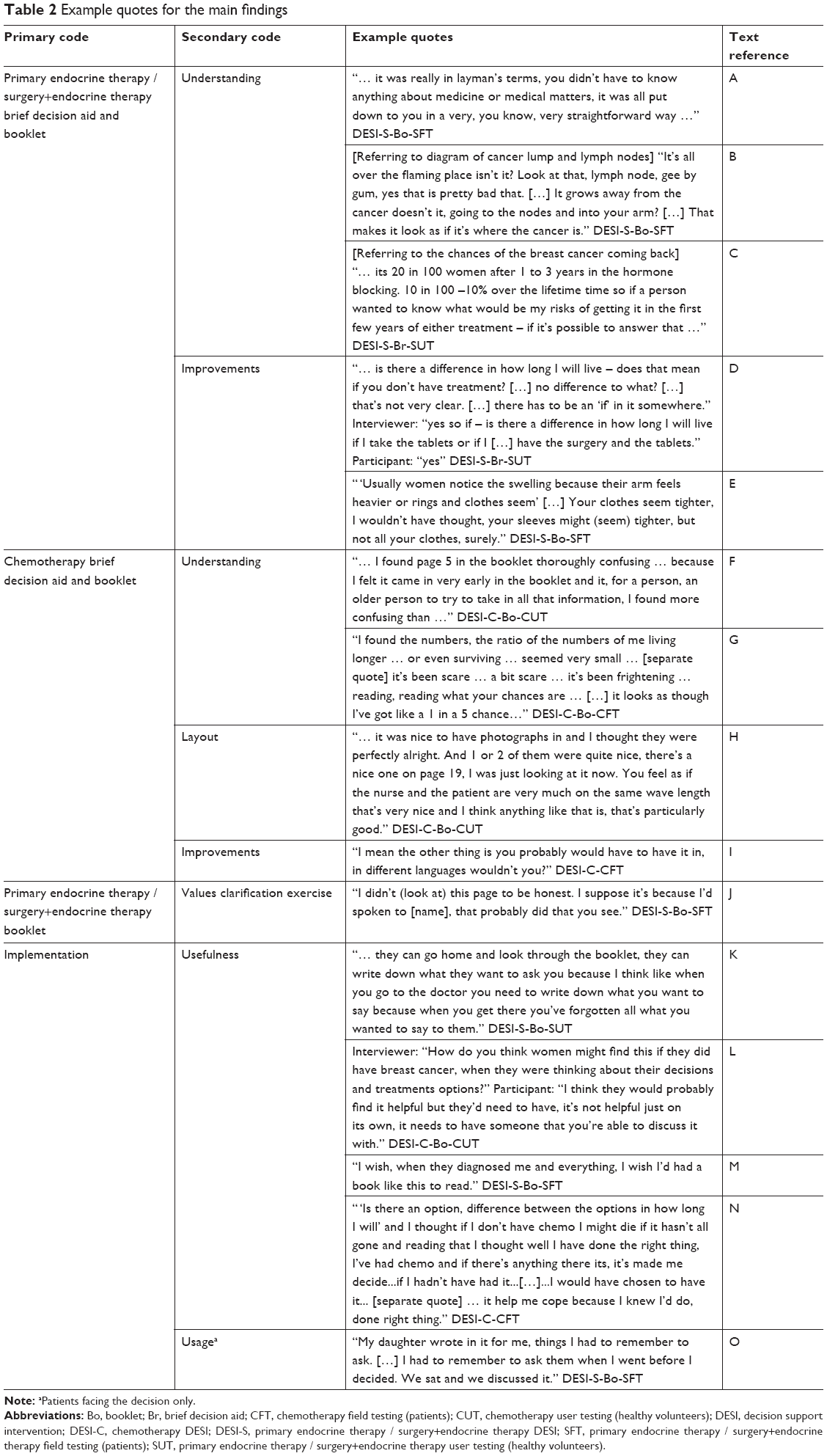 | Table 2 Example quotes for the main findings |
Primary endocrine therapy / surgery+endocrine therapy DESI content
Generally, the feedback was positive about the primary endocrine therapy / surgery+endocrine therapy DESI. Both the brief decision aid and booklet were understood and mostly clear (A). The brief decision aid was described as the “headlines” and the booklet containing more detailed backup information. Women thought that the DESI covered the information patients would want and most women thought the amount of information was appropriate. Some of the healthy volunteers felt that the booklet was quite long, but none said the amount should be reduced; rather, it was comprehensive. A mixture of views was given by volunteers about the size of the booklet, some liking the A4 size (user testing paper version) and others liking the idea of an A5 booklet. The graphic design version of the booklet received generally positive feedback from patients in terms of color, size (A5 was standard and a large print A4 version was also available), and layout. The diagrams and pictures had mixed reviews in terms of both understanding and helpfulness (some thought redundant). A diagram showing lymph nodes was misinterpreted as cancer by one patient (who had previously faced the decision) and was thought quite frightening by two other patients, so was changed during field testing (before testing with patients currently facing the decision) (B). This new version of the diagram was understood. Natural frequencies in the text were understood by most volunteers, although two found them confusing. Pictograms were added in the field testing versions of the booklet and most, but not all, patients were positive about these.
Some information lacked clarity and/or caused confusion to the volunteers. Examples include the information on recurrence not being comparable and for some the values clarification exercise – which included a table with each treatment option listed at the top of each column where participants could enter their preferences for that treatment (see Figure 4 for final version) – needed more explanation (C). These were reviewed by the development team and changes were made to the DESI as appropriate before field testing. Similarly, volunteers suggested improvements such as rewording sentences, emphasizing particular pieces of information and adding details which were amended as seen appropriate (D). A number of questions were raised. Some questions raised by volunteers could be addressed within the DESI, others would be asked of a clinician. Patients asked general questions as well as requested clarifications and made suggestions for improvements (E).
 | Figure 4 Values clarification exercise in primary endocrine therapy / surgery+endocrine therapy booklet. |
Chemotherapy DESI content
The feedback on the chemotherapy DESI was also positive overall. Most women thought that it was understandable and included the things that patients would want to know. However, some healthy volunteers acknowledged that some people might need help going through it and one woman found the page about secondary breast cancer and what increases the risk of the cancer spreading (page 5) particularly confusing (F). Despite changes, a few things were not understood by patients, with one not understanding about having trastuzumab and another struggling to understand the increased benefit of trastuzumab (but another woman felt that it clarified some people have trastuzumab alongside chemotherapy). One woman did not seem to understand the increase in benefit that chemotherapy offers; she interpreted the increase as the chance of survival (G).
Most liked the layout, describing it as well set out and they liked the photographs (H). However, one woman commented that there were no women from ethnic minorities. The lack of ethnic minority photographs was deliberate because there are currently very few ethnic minority women in the ≥70 years age group in the UK,32 although this will change in the future as cohorts age. Some women felt the booklet was a bit repetitive but others felt that the repetition was appropriate and that all the information needed to be included, hence no changes were made. Patients thought the amount of information was about right. Some improvements were suggested by healthy volunteers (eg, emphasizing that not everyone will experience the side effects) and patients (eg, supplying the information in different languages); however, few patients thought that any improvements were needed (I).
DESI use/implementation
The DESIs were generally thought to be helpful. Women mentioned it being a good basis for questions (eg, as a prompt or reminder) and primary endocrine therapy / surgery+endocrine therapy patients talked about reading the information multiple times and finding it useful to be able to do this (K). Many healthy volunteers thought that it would be useful to take the DESI home to read, refer back to, and discuss with friends/family with a further discussion with clinicians afterward. Some mentioned that the information would be too much to take in at the diagnostic consultation or when initially hearing about treatments. They highlighted the importance of discussions with and advice from clinicians and expressed the view that some patients might need additional help with processing the information (L).
Many patients (previously facing the decision) thought that it could be helpful for others (including family members) (M). One found it very useful to confirm her chemotherapy decision, another felt she had learned more from the primary endocrine therapy / surgery+endocrine therapy brief decision aid than she had at diagnosis and another found receiving the information as part of the study useful (N). Two patients, however, felt the chemotherapy DESI was not for them (one preferring discussions with clinicians). Two patients found some of the information about treatment benefits and survival changes in the chemotherapy DESI upsetting and frightening (for one, possibly due to some misunderstanding of what the natural frequencies were) (G). Two patients who were currently facing the primary endocrine therapy / surgery+endocrine therapy decision thought the DESI had helped to reinforce their initial decision leaning or to make the decision. Only one patient currently facing the decision (primary endocrine therapy / surgery+endocrine therapy) wrote in the values clarification exercise or “My questions” sections (O). The others felt no need to use it as they had already made their decision or spoken with their clinician (J).
Discussion
Two DESIs for older women with breast cancer treatment choices were developed based on the best available published evidence and feedback from healthy volunteers and patients. A detailed and iterative process was used to develop the primary endocrine therapy / surgery+endocrine therapy DESI, both in terms of the initial prototype development (reviews of literature, theory based, new data collected, and Plain English Campaign29 involvement) and usability testing (with healthy volunteers and patients). It was possible to use the primary endocrine therapy / surgery+endocrine therapy DESI as a template upon which to base the chemotherapy DESI, hence a more efficient development and testing process was used for this second DESI. General feedback about language, colors, format, and size of the DESIs was transferable from one to the other. Feedback from participants about the DESIs included many positive comments, but areas of confusion were noted and possible changes were suggested. Potential amendments to the DESIs were discussed among the development team and changes were made where appropriate (eg, in the case where a diagram had been misinterpreted). While the DESIs were thought to be useful (for self or others), some patients preferred not to use the values clarification exercise as they had already spoken with their clinicians or made their decision. However, this section was retained in the DESIs, as helping patients consider and discuss their values and preferences about the options is a key element of decision support.15 Furthermore, the importance of discussions with clinicians was highlighted by women, and was reflected by the inclusion of signposting to this in the DESIs.
To our knowledge, no DESIs currently exist for older women making these two breast cancer treatment choices. The DESIs are currently being trialed within the Bridging the Age Gap in Breast Cancer study as part of an intervention (which includes the booklets, brief decision aids, and an online algorithm to predict survival under different treatment options) to primarily assess their effects on quality of life.14 Other measures of decision support are also being evaluated in the trial (eg, shared decision-making, decision regret, and knowledge).14 Another strength of this study is the detailed and systematic process used to develop the initial DESI, following IPDAS15 guidelines, and use of the first DESI as a template to develop the second DESI. The advantages of being able to develop a DESI more efficiently are important. Using a more efficient development method could save resources, both in terms of burden to participants (which may be particularly relevant in this older and sometimes frailer population) and in terms of developers’ time and funds. That a sample of older women was recruited to the present study, including some much older people (four participants were ≥90 years), is a further strength. Previously, difficulties in recruiting older women have been described, though these were within the context of clinical trials (and due to protocol restrictions and clinician reservation about treatments) rather than studies in general.33
We recognize the limitations of our development study. Firstly, the two groups of women likely to be eligible for the respective treatment options are different; those with a choice of primary endocrine therapy or surgery+endocrine therapy are likely to be frailer and older than those with a choice about chemotherapy. Older women may have different preferences for information style. Burton et al22 found an inverse association between preference for written information and age even within a sample of older breast cancer patients (≥75 years) offered a choice of primary endocrine therapy or surgery+endocrine therapy. Preferences elicited for the first DESI (which were based on women aged ≥75 years) may therefore not be completely transferable to the chemotherapy DESI. Secondly, due to time constraints of the program of work, patients currently facing the decision about chemotherapy were not included in the sample. Lastly, while the DESIs are based on the best clinical evidence available at the time, new survival outcome data for this older population are being collected as part of the Bridging the Age Gap in Breast Cancer study (ISRCTN46099296).14 Not only will the DESIs therefore need updating when this is available, they will also need updating if new treatment options become available in the future.
Participants highlighted the need for interaction with clinicians, and the importance of clinicians’ shared decision-making skills and attitudes has recently been highlighted.34 Skills development for shared decision-making along with guidance on using the DESIs remains crucial for successful implementation in clinical practice.
Further research is needed in a larger sample to test the effectiveness of the DESIs in improving shared decision-making for older women with breast cancer treatment choices (currently being done in the Bridging the Age Gap in Breast Cancer study, ISRCTN 4609929614). If they are effective, this will show that where patient populations are similar, DESIs for different treatment decisions can be developed based on the template of another DESI and on information already obtained from the patient population, and then implemented. Resources saved (both time and funds) during the initial prototype and testing phases of development could then be directed toward supporting shared decision-making skills for clinicians and updating DESIs with new clinical evidence.
Conclusion
Two DESIs for older women with breast cancer have been successfully developed for two different treatment choices (primary endocrine therapy / surgery+endocrine therapy and chemotherapy / no chemotherapy). Using an iterative process of feedback and improvements, the DESIs were found to be acceptable and usable by patients. Having developed one DESI using a detailed and systematic process, it was possible to develop the second DESI for a different treatment choice more efficiently using information already captured for the initial DESI. Before developing the DESIs, there were none (to our knowledge) available for this group of older women having to make these particular treatment choices. With policy makers keen to promote shared decision-making and enhance patient-centered care, development of DESIs which inform patients about treatments and enable them to be involved in treatment decisions is vital. An efficient process to develop these is therefore beneficial.
Data sharing statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and informed consent
Approval for healthy volunteer involvement in the study was obtained from Cardiff University School of Medicine Research Ethics Committee (reference 13/72) and Brighton and Sussex Medical School Research Governance and Ethics Committee (reference 15/111/HAR). Sheffield Hallam University provided approval based on Cardiff University approval and the University of Sheffield Research Ethics Committee deemed that duplicate ethical approval from them was not required. Approval of the study protocol for patient involvement was obtained from the National Research Ethics Service London – Surrey Borders committee (reference 12/LO/1722) and the appropriate National Health Service Trust Research and Development Departments. All participants completed a consent form for their participation in the study.
Participants gave consent for words said during the interviews to be used anonymously, in the presentation of the research. All personal identifiers have been removed or disguised so the person(s) described are not identifiable and cannot be identified through the details of the story.
Acknowledgments
We are very grateful for the help of the principal investigators (PI) and their teams at each of the sites recruiting patients: University Hospital Llandough, Cardiff (PI Prof Helen Sweetland); Doncaster Royal Infirmary, Doncaster (PI Miss Clare Rogers); Royal Hallamshire Hospital, Sheffield (PIs Prof Malcolm Reed [now at Brighton and Sussex Medical School] and Dr Matthew Winter); and Southampton General Hospital, Southampton (PI Dr Ramsey Cutress). We would also like to thank all the participants for their time and generosity in sharing their ideas and experiences. We would like to thank the other members of the Bridging the Age Gap in Breast Cancer study management group and the experts who reviewed the clinical information for both DESIs. The Plain English Campaign gave editorial suggestions on the primary endocrine therapy / surgery+endocrine therapy DESI and Australian Welsh Design and Print completed the graphic design work on the booklets for both DESIs. This paper presents independent research funded by the National Institute for Health Research (NIHR) under the Programme Grants for Applied Research programme (RP-PG-1209–10071). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health. Dr Kate J Lifford reports grants from NIHR, during the conduct of the study. Professor Adrian Edwards reports grants from UK National Institute for Health Research, during the conduct of the study. Dr Lisa Caldon reports grants from National Institute of Health Research, during the conduct of the study.
Author contributions
Design of the study, acquisition, analysis and interpretation of data, drafting the article: KJL; conception and design of the study, acquisition, analysis and interpretation of data, drafting the article: AE and KBr; design of the study, acquisition, analysis and interpretation of data: MB; acquisition, analysis and interpretation of data: HH; acquisition of data: FA; conception and design of the study: JLM, LC, KBa, AR, KC, MR, and LW. All authors contributed towards critically revising the article, gave final approval of the article, and agree to be accountable for all aspect of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Cancer Research UK [webpage on the Internet]. Breast cancer incidence (invasive) statistics. Available from: http://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/breast-cancer/incidence-invasive#heading-One. Accessed June 20, 2017. | ||
Ottawa Inventory of Patient Decision Aids [webpage on the Internet]. Available from: https://decisionaid.ohri.ca/AZinvent.php. Accessed December 17, 2014. | ||
Bayer A, Tadd W. Unjustified exclusion of elderly people from studies submitted to research ethics committee for approval: descriptive study. BMJ. 2000;321(7267):992–993. | ||
Wyld L, Reed MW. The need for targeted research into breast cancer in the elderly. Br J Surg. 2003;90(4):388–399. | ||
Audisio RA, Wyld L. No standard is set for older women with breast cancer. Eur J Surg Oncol. 2015;41(5):607–609. | ||
Morgan J, Richards P, Ward S, et al. Case-mix analysis and variation in rates of non-surgical treatment of older women with operable breast cancer. Br J Surg. 2015;102(9):1056–1063. | ||
Biganzoli L, Wildiers H, Oakman C, et al. Management of elderly patients with breast cancer: updated recommendations of the International Society of Geriatric Oncology (SIOG) and European Society of Breast Cancer Specialists (EUSOMA). Lancet Oncol. 2012;13(4):e148–e160. | ||
National Institute for Health and Care Excellence [webpage on the Internet]. Early and locally advanced breast cancer: diagnosis and management. Available from: https://www.nice.org.uk/guidance/ng101/chapter/Recommendations. Accessed July 31, 2018. | ||
Morgan J, Wyld L, Collins KA, Reed MW. Surgery versus primary endocrine therapy for operable primary breast cancer in elderly women (70 years plus). Cochrane Database Syst Rev. 2014;37(Suppl 5)Art. No.: CD004272. | ||
Morgan JL, Reed MW, Wyld L. Primary endocrine therapy as a treatment for older women with operable breast cancer – a comparison of randomised controlled trial and cohort study findings. Eur J Surg Oncol. 2014;40(6):676–684. | ||
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), Peto R, Davies C, et al. Comparisons between different polychemotherapy regimens for early breast cancer: meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet. 2012;379(9814):432–444. | ||
Adjogatse D, Thanopoulou E, Okines A, et al. Febrile neutropaenia and chemotherapy discontinuation in women aged 70 years or older receiving adjuvant chemotherapy for early breast cancer. Clin Oncol (R Coll Radiol). 2014;26(11):692–696. | ||
Ring A, Harder H, Langridge C, Ballinger RS, Fallowfield LJ. Adjuvant chemotherapy in elderly women with breast cancer (AChEW): an observational study identifying MDT perceptions and barriers to decision making. Ann Oncol. 2013;24(5):1211–1219. | ||
Collins K, Reed M, Lifford K, et al. Bridging the age gap in breast cancer: evaluation of decision support interventions for older women with operable breast cancer: protocol for a cluster randomised controlled trial. BMJ Open. 2017;7(7):e015133. | ||
International Patient Decision Aid Standards [homepage on the Internet]. Available from: http://ipdas.ohri.ca/. Accessed May 22, 2017. | ||
Olivotto IA, Bajdik CD, Ravdin PM, et al. Population-based validation of the prognostic model ADJUVANT! for early breast cancer. J Clin Oncol. 2005;23(12):2716–2725. | ||
PREDICT [homepage on the Internet]. Available from: http://www.predict.nhs.uk/. Accessed June 21, 2017. | ||
Burton M, Collins K, Caldon LJM, Wyld L, Reed MWR. Information needs of older women faced with a choice of primary endocrine therapy or surgery for early-stage breast cancer: a literature review. Curr Breast Cancer Rep. 2014;6(3):235–244. | ||
Cox A, Jenkins V, Catt S, Langridge C, Fallowfield L. Information needs and experiences: an audit of UK cancer patients. Eur J Oncol Nurs. 2006;10(4):263–272. | ||
Pinquart M, Duberstein PR. Information needs and decision-making processes in older cancer patients. Crit Rev Oncol Hematol. 2004;51(1):69–80. | ||
Burton M, Collins KA, Lifford KJ, et al. The information and decision support needs of older women (>75 yrs) facing treatment choices for breast cancer: a qualitative study. Psychooncology. 2015;24(8):878–884. | ||
Burton M, Kilner K, Wyld L, et al. Information needs and decision-making preferences of older women offered a choice between surgery and primary endocrine therapy for early breast cancer. Psychooncology. 2017;26(12):2094–2100. | ||
Harder H, Ballinger R, Langridge C, Ring A, Fallowfield LJ. Adjuvant chemotherapy in elderly women with breast cancer: patients’ perspectives on information giving and decision making. Psychooncology. 2013;22(12):2729–2735. | ||
Lifford KJ, Witt J, Burton M, et al. Understanding older women’s decision making and coping in the context of breast cancer treatment. BMC Med Inform Decis Mak. 2015;15:45. | ||
van Weert JC, van Munster BC, Sanders R, Spijker R, Hooft L, Jansen J. Decision aids to help older people make health decisions: a systematic review and meta-analysis. BMC Med Inform Decis Mak. 2016;16:45. | ||
Elwyn G, O’Connor AM, Bennett C, et al. Assessing the quality of decision support technologies using the International Patient Decision Aid Standards instrument (IPDASi). PLoS One. 2009;4(3):e4705. | ||
Joseph-Williams N, Newcombe R, Politi M, et al. Toward minimum standards for certifying patient decision aids: a modified Delphi consensus process. Med Decis Making. 2014;34(6):699–710. | ||
Witt J, Elwyn G, Wood F, Brain K. Decision making and coping in healthcare: the Coping in Deliberation (CODE) framework. Patient Educ Couns. 2012;88(2):256–261. | ||
Plain English Campaign [homepage on the Internet]. Available from: http://www.plainenglish.co.uk/. Accessed May 22, 2017. | ||
Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Huberman AM, Miles MB, editors. The Qualitative Researcher’s Companion. London: Sage Publications; 2002:305–329. | ||
NVivo qualitative data analysis Software (Version 11); Melbourne: QSR International Pty Ltd; 2015. | ||
Office for National Statistics [webpage on the Internet]. Available from: https://www.nomisweb.co.uk/census/2011/dc2101ew. Accessed June 21, 2017. | ||
Reed MWR, Wyld L, Ellis P, Bliss J, Leonard R on behalf of the ACTION and ESTEeM Trial Management Groups. Breast cancer in older women: trials and tribulations. Clin Oncol (R Coll Radiol). 2009;21(2):99–102. | ||
Joseph-Williams N, Lloyd A, Edwards A, et al. Implementing shared decision making in the NHS: lessons from the MAGIC programme. BMJ. 2017;357: j1744. |
Supplementary material
Interview guide
- What do you think about the brief decision aid/booklet?
- Is the brief decision aid/booklet easy to use and understand?
- What do you think about the questions listed on the left (brief decision aid only)?
- What do you think about the different sections of the booklet (booklet only)?
- Are there areas in the brief decision aid/booklet that need changing?
- Healthy volunteers: How useful do you think it could be for women who have a decision to make about treatment? Patients: How useful do you think it was/could have been when making your decision about treatment?
- Do you have any suggestions for improvement?
- Any other comments?
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.