Back to Journals » Clinical Ophthalmology » Volume 19
Efficiency Comparison Between Two Different Lasers and Cataract Surgery Workflows: A Prospective and Retrospective Analysis
Authors Chapman Jr JM ![]()
Received 19 June 2025
Accepted for publication 17 September 2025
Published 2 October 2025 Volume 2025:19 Pages 3603—3608
DOI https://doi.org/10.2147/OPTH.S548211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jack M Chapman Jr
Clinical Ophthalmology, North Georgia Eye Associates, Gainesville, GA, USA
Correspondence: Jack M Chapman Jr, Clinical Ophthalmology, North Georgia Eye Associates, 2061 Beverly Road, Gainesville, GA, 30501, USA, Tel +1 404 234 5433, Email [email protected]
Purpose: To compare time efficiencies between a traditional femtosecond laser platform and workflow and a single-room model with a robotic laser in patients undergoing cataract surgery.
Patients and Methods: Single site, prospective, non-masked study of 23 patients (n = 23 eyes) who underwent the femtosecond laser portion of their cataract surgery with the LenSx Femtosecond Laser System (Alcon, Ft. Worth, Texas) in one room and were subsequently moved to a second room for the remainder of their surgery compared to 23 patients who underwent surgery with a dual-modality, robotic laser (ALLY, Lensar, Orlando, FL) and remained in the same room for the rest of the surgery. Time parameters evaluated were laser set up, docking, suction, total laser time, docking attempts, surgeon total case time, patient total case time, transition to phacoemulsification start time, and transition preparation and draping. Third party observers tracked all time and motion parameters by using a stopwatch and documented activities with a time stamp.
Results: There were statistical differences in numerous parameters (all outcomes were measured in minutes): mean suction time [ALLY, 1:16 vs LenSx, 2:26, (P < 0.001)], laser completion to phacoemulsification initiation [ALLY, 0:57 vs LenSx, 4:39, (P < 0.001)], laser set up start to docking start [ALLY, 10:05 vs LenSx, 19:31, (P = 0.034)], total laser time for the surgeon [ALLY, 3:17 vs LenSx, 4:53; (P = < 0.001)]; total case time for the surgeon [ALLY, 14:27 vs LenSx,19:40; (P < 0.001)], and total patient time spent in the OR [ALLY, 25:25 vs LenSx 33:22; (P = 0.021)]. There were no statistically significant differences in total phaco procedure time.
Conclusion: Using a robotic laser for cataract surgery can save about 5 minutes of surgeon time per case and 8 minutes of patient’s time in the OR when compared to a traditional femtosecond laser platform set up.
Keywords: phacoemulsification, femtosecond laser, robotic laser, cost-benefit analysis, robotic surgical procedures
Introduction
Cataract is a leading cause of vision impairment,1–5 with the World Health Organization (WHO) estimating between 62 and 94 million people worldwide are affected.3,4,6 Prevent Blindness has predicted the number of cataract cases in the US will increase from 25.7 million cases in 2014 to 38.5 million in 2032 and to 45.6 million in 2050.5
In 2020, there were 7 million cataract surgical procedures performed in Europe, 3.7 million in the US, and 20 million worldwide.7,8 In the US, procedural volume continues to grow at a compound annual rate of 3.1%.9
Ultrashort laser pulses to in-vivo ablation of cataractous lens tissue was first proposed in 1992 (US patent 5,246,435, issued Sept 1993),10 and in 1993, an accidental laser injury to the eye of a graduate student at the University of Michigan showed potential use of femtosecond lasers in ocular surgery.11,12 Femtosecond lasers emit light pulses that cause photodisruption of the tissue with minimal collateral damage.12 In refractive surgery, this meant surgeons could replace the mechanical microkeratome with a more precise option for LASIK flap creation.13 Shortly before the US patent expired, several laser companies introduced femtosecond laser-assisted cataract surgery (also known as FLACS).10 In cataract surgery, the focal photodisruption of the tissue uses a laser beam, typically generated at a wavelength of 1053 nm.12
When femtosecond lasers were introduced for cataract surgery, it was suggested they could improve visual outcomes when compared to conventional phacoemulsification techniques, particularly in complex cases,1,9,14–17 but many surgeons do not believe these lasers achieved those goals. As their technology has advanced, some have suggested these lasers provide another step toward robot-assisted surgery.7 Artificial intelligence (AI) research in ophthalmology is also progressing,9 and has been implemented in some second-generation femtosecond lasers. Kecik et al summarized the move towards robotics:
Robotization of the steps of lens aspiration is in its infancy in cataract surgery,18,19 but this technology could be integrated with [femtosecond laser-assisted cataract surgery] to create fully automated cataract extraction platforms in the future.7
In other specialties, robotic surgery has proven to improve efficiency and productivity and shorten hospital stays.20 Maynou et al showed an increase in total production at the hospital level between 21% and 26%, coupled with a 29% improvement in labor productivity in treating prostate cancer.21 Okamura et al found that telerobotic systems can reduce surgical recovery times and produce more reliable outcomes.22
This study was designed to evaluate the efficiency of two different workflow scenarios for laser-assisted cataract surgery: 1) a dual-room approach with a single laser used to support two operating rooms (OR), which entails moving the patient into the OR after the non-sterile laser portion of the procedure is complete, and 2) a single room approach with a robotic laser in the operating suite (the laser portion of the procedure is performed under sterile technique, in the same room as the remaining portion of the cataract surgery). The hypothesis was if patients did not have to be moved between OR rooms when undergoing cataract extraction with the robotic laser, were there additional time savings with other components of surgery that were not as obvious?
Materials and Methods
This was a single site, prospective, non-masked study of 46 patients who were consecutively enrolled and assigned to one of two cataract surgery workflows: 1) a dual-room approach where patients underwent the non-sterile laser portion of their cataract surgery with the LenSx Femtosecond Laser System (Alcon, Ft. Worth, Texas) in one room and were subsequently moved to a second room for the remainder of their surgery or 2) a single-room approach where patients underwent the femtosecond portion of the surgery under sterile technique, with a robotic laser (ALLY, Lensar, Orlando, FL) and remained in the same room to undergo the remainder of the surgery. Inclusion and exclusion criteria included patients at least 21 years of age with an operable cataract that would be eligible for laser treatment and phacoemulsification; any ocular pathology that would be contraindicated for laser and/or standard of care for routine cataract surgery were exclusionary criteria.
A total of 46 eyes (46 patients) were enrolled: 23 in the ALLY laser group and 23 in the LenSx laser group. Time parameters evaluated were laser set up, docking, suction, total laser time, docking attempts, surgeon total case time, patient total case time, transition to phacoemulsification start time, and transition preparation and draping. All surgeries were performed by the same surgeon (JMC). Third party observers tracked all time and motion parameters by using a stopwatch and documented activities with a time stamp.
All patients provided informed consent, and this study adhered to the Declaration of Helsinki and received institutional review board exemption from Salus Institutional Review Board (Austin, Texas, USA). The retrospective portion of the study was registered on clinicaltrials.gov (ID# NCT07038395).
Lasers Used
There were two laser workflow scenarios evaluated in this study with two different lasers: The LenSx and the ALLY.
The LenSx is a 50 kHz femtosecond infrared laser that has a pulse width of 600–800 fs, a central laser wavelength of 1030 nm, and maximum pulse energy of 15 μJ.23 It is considered a high-pulse energy device.24 The laser combines a three-dimensional spectral-domain optical coherence tomography system designed to provide visualization of the entire anterior segment during the surgical procedure and a liquid-free curved patient interface.23 Patients assigned to the LenSx laser underwent that portion of the cataract surgery in one non-sterile room and were then moved into the OR for the phacoemulsification portion of the surgery.
The ALLY Robotic Cataract Laser System (Lensar, Orlando, FL) is a dual-modality laser that uses a pulse width of 1500 femtoseconds (fs) to fragment the lens and 320 fs to cut the cornea. The reduced imaging time when compared to other femtosecond lasers is attributed to the 6 fixed Scheimpflug cameras (data on file, Lensar). The robotic laser uses artificial intelligence-based analysis (data on file, Lensar); by combining the laser and the imaging components into one system, the patient may undergo the entire cataract procedure under sterile technique in the OR.
Statistical Analysis
A non-participant in the time and motion components oversaw data collection; data analysis was performed using IBM SPSS software version 27.0 (IBM, Armonk, NY). At the time of the study design and protocol preparation, sample size calculations aimed to achieve a power of at least 80% for the primary outcome. Data were analyzed as received (N = 23 for each group). Similar to the a priori sample size calculations, post hoc power calculations would apply to the primary outcome measures. Two variables (surgeon case time and total patient time) were deemed the most important of the time variables evaluated, and a post hoc analysis was performed on these.
Results
A total of 46 eyes of 46 patients were enrolled: the 23 patients in the LenSx group were enrolled in 2023, and the 23 patients in the ALLY group were enrolled in 2024, one year after the laser platform was first introduced in the clinic. Baseline characteristics were not statistically significantly different between the two groups nor between the laser assignments in each group. The LenSx group comprised 10 females (43.5%); average age of 71.9 years while the ALLY group comprised 10 female patients (43.5%); average age 72.8 years. Both groups presented with a mean cataract grade of 2.
There were statistical differences in all but two parameters (see Figure 1). For the laser component, these significant differences included suction time for the ALLY (mean 1:16±0:21 minutes) and the LenSx (mean 2:26±0:30 minutes; P < 0.001, independent t test). Similarly, there were statistically significant differences between laser completion to phacoemulsification initiation (docking release to first touch of the eye by the surgeon) for the ALLY (mean 0:57±0:19 minutes) and the LenSx (mean 4:39±1:01 minutes; P < 0.001, Mann–Whitney). For the workflow components, there were statistically significant differences in laser set up start to docking start with the ALLY (10:05±7:20) and the LenSx (19:31±14:27; P = 0.034, Mann–Whitney), total femto time for the surgeon with the ALLY (mean 3:17±1:14 minutes) and the LenSx (mean 4:53±2:44 minutes; P = <0.001, Mann–Whitney); total case time for the surgeon with the ALLY (mean 14:27±3:29 minutes) and the LenSx (mean 19:40±4:22 minutes; P < 0.001, Mann–Whitney), and between total patient time spent in the OR with the ALLY (25:25±6:36 minutes) and the LenSx (33:22±14:40; P = 0.021, Mann–Whitney). There were no statistically significant differences in docking attempt time with the ALLY (1) and the LenSx (1.13; P = 0.083, Mann–Whitney) or total phaco procedure time between the ALLY (10:15±3:00 minutes) and the LenSx (9:03±3:22; P = 0.07, Mann–Whitney).
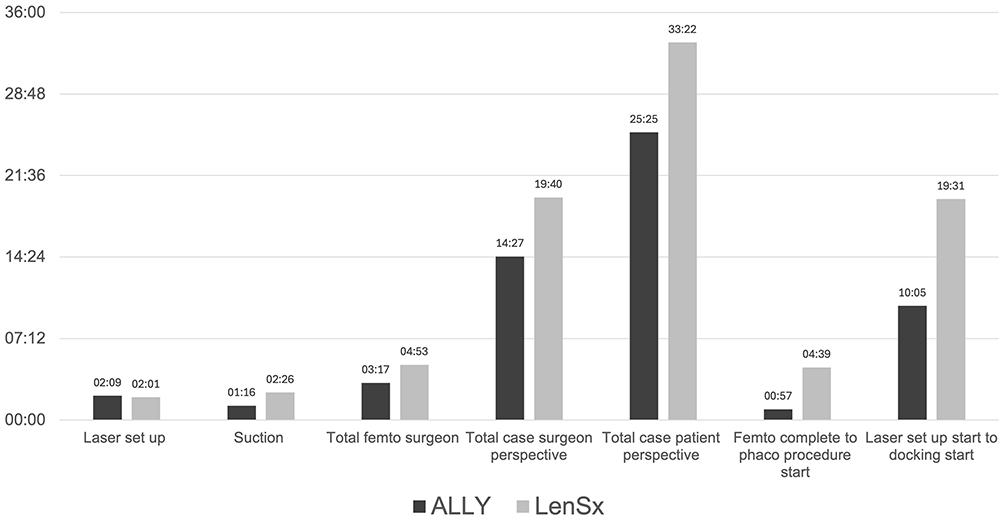 |
Figure 1 Mean Laser Times (in Minutes). |
Discussion
In this study comparing a robotic cataract surgery laser to a more traditional femtosecond laser and workflow, use of the robotic device resulted in statistically significantly time savings in almost every parameter: docking, total case time, laser completion to phacoemulsification initiation, and both surgeon and patient time in the OR. Of interest, these statistically significant differences were shown after only 1 year’s experience with the ALLY compared to 10 years of experience with the LenSx.
The use of laser cataract surgery remains somewhat controversial, with the majority of published studies concentrating on visual outcomes as a measure of cost-effectiveness.1,7,15,16,24–30 The FEMCAT study (N = 870) found femtosecond laser surgery not as cost-effective as conventional phacoemulsification,1 whereas the FACT trial found femtosecond laser not inferior to traditional phaco, but not more cost-effective.25 A recent Cochrane review suggested little difference between femtosecond and traditional phacoemulsification outcomes.27 While the European Registry of Quality Outcomes for Cataract and Refractive Surgery (N = 3379) found femtosecond laser surgery to have favorable outcomes when compared to phaco and a low rate of complications,26 a National Health Service study found femtosecond laser-assisted cataract surgery could be more cost effective than traditional phacoemulsification if efficiency increased substantially or if the cost of the patient interface was reduced substantially.31
Bartlett and Miller recommended financial analyses be performed to assess costs (including those that can be passed onto patients) and to help practices determine if those costs are justified.30 George et al found only 13 femtosecond cases per month in a rural setting were required to have a femtosecond laser cost break even in 5 years’ time (their practice averaged more than 100 cases per month).29 That group further reported that when both facility and physician fees were considered as revenue, only eight cases per month were necessary.
However, fewer studies have evaluated time and motion as variable costs when adding a laser to a facility. Fewer still evaluate robotic laser cataract surgery. In this study, robotic laser cataract surgery reduced the amount of time the surgeon (and ancillary staff) spent in the OR. That time saving allows for additional cases daily or reduced staff costs by allocating staff to other responsibilities. In our clinic, use of the robotic laser allowed us to save about 5 minutes of surgeon time per case and about 8 minutes of the patient’s time in the OR when using the ALLY compared to the LenSx. These results add to the literature on OR/clinic time savings when implementing an advanced technology laser for cataract surgery.
Khodabakhsh and Hofbauer reported no significant differences between the LenSx and CATALYS (Johnson & Johnson Vision) systems in patient interface preparation time, phacoemulsification time, total imaging time, nucleus removal time, phacoemulsification power, and number of docking attempts; however, the LenSx system had significantly shorter suction times (108.5 seconds) compared with the CATALYS system (123.2 seconds) (P < 0.05)32 Heit et al compared LenSx to CATALYS, and found LenSx took significantly less time for patient positioning, imaging, laser treatment, and undocking/transition.33
An earlier study evaluating the LenSx and CATALYS devices concluded increased efficiency associated with CATALYS procedures, with a time saving of 94 seconds for patient interface preparation and 61 seconds for suction.23 George et al reported 5.35 additional minutes were needed for the LenSx part of the procedure, at an incremental cost of $57 per surgery in the first 12 months.29
Weinstock et al found ALLY dual-pulse laser completed the entire laser procedure (including imaging) in 1:05 minutes; traditional phaco procedure time was 7:16 minutes, with a total time per case of less than 12 minutes, and the total time spent by the patient in the OR was under 30 minutes.34 Our results are similar: the laser procedure time was 1:05 minutes; traditional phaco procedure time was about 10 minutes, with a total time per case of about 14 minutes, and the total time spent by the patient in the OR was around 25 minutes.
This study is not without its limitations, however, among them that this was a single-center, non-masked study. Additionally, the study design itself may potentially introduce selection bias, and a larger sample size would allow for a more robust statistical analysis. Our results underscore the necessity of conducting additional assessments of robotic cataract laser systems in randomized clinical environments that are larger in scale. However, we believe the limitations of this study are more than offset by the findings of increased time savings when using a next-generation robotic laser platform. Additionally, third-party independent statisticians and blinded observers were used to minimize further biases.
Conclusion
Using a robotic cataract surgery laser can save a significant amount of time in the OR when compared to a traditional femtosecond laser platform.
Data Sharing Statement
Study data is available upon request from either the author ([email protected]) or the study sponsor (www.lensar.com; Lensar, 2800 Discovery Dr, Orlando, FL 32826 USA).
Acknowledgments
Medical writing was provided by Michelle Dalton, ELS, of Dalton & Associates (USA), which was funded by Lensar, Inc., in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3). Statistical analyses were provided by IrisARC – Analytics, Research, and Consulting (Chandigarh, India); this was funded by Lensar. This study has been presented in part at the American Society of Cataract & Refractive Surgery in 2024 and 2025.
Funding
Lensar funded this study.
Disclosure
JMC Jr is a consultant for Lensar. The author reports no other conflicts of interest in this work.
References
1. Benard A, Sitta R, Brezin AP, et al. Cost utility and value of information analysis of femtosecond laser-assisted cataract surgery. JAMA Ophthalmol. 2023;141(7):625–629. doi:10.1001/jamaophthalmol.2023.1716
2. Hashemi H, Pakzad R, Yekta A, et al. Global and regional prevalence of age-related cataract: a comprehensive systematic review and meta-analysis. Eye. 2020;34(8):1357–1370. doi:10.1038/s41433-020-0806-3
3. World Health Organization. World report on vision. 2019. Available from: https://www.who.int/publications/i/item/9789241516570.
4. Blindness and vision impairment. World Health Organization; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment.
5. Prevent Blindness. The future of vision. 2014. Available from: https://preventblindness.org/the-future-of-vision/.
6. Global Burden of Disease Blindness and Vision Impairment Collaborators, Vision Loss Expert Group of the Global Burden of Disease Study. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study. Lancet Glob Health. 2021;9(2):e144–e160. doi:10.1016/S2214-109X(20)30489-7
7. Kecik M, Schweitzer C. Femtosecond laser-assisted cataract surgery: update and perspectives. Front Med. 2023;10:1131314. doi:10.3389/fmed.2023.1131314
8. Rossi T, Romano MR, Iannetta D, et al. Cataract surgery practice patterns worldwide: a survey. BMJ Open Ophthalmol. 2021;6(1):e000464. doi:10.1136/bmjophth-2020-000464
9. Chen X, Xu J, Chen X, Yao K. Cataract: advances in surgery and whether surgery remains the only treatment in future. Adv Ophthalmol Pract Res. 2021;1(1):100008. doi:10.1016/j.aopr.2021.100008
10. Sun H, Fritz A, Droge G, Neuhann T, Bille JF. Femtosecond-Laser-Assisted Cataract Surgery (FLACS). In: Bille JF, editor. High Resolution Imaging in Microscopy and Ophthalmology: New Frontiers in Biomedical Optics. Springer; 2019:chap14.
11. Wright K. Laser-accident-turned-surgery-breakthrough wins golden goose. Physics. 2022;15:141. doi:10.1103/Physics.15.141
12. Aristeidou A, Taniguchi EV, Tsatsos M, et al. The evolution of corneal and refractive surgery with the femtosecond laser. Eye Vis. 2015;2:12. doi:10.1186/s40662-015-0022-6
13. Salomao MQ, Wilson SE. Femtosecond laser in laser in situ keratomileusis. J Cataract Refract Surg. 2010;36(6):1024–1032. doi:10.1016/j.jcrs.2010.03.025
14. Chen DZ, Chee SP. Femtosecond laser-assisted cataract surgery for complex cataracts - A review. Indian J Ophthalmol. 2024;72(5):629–636. doi:10.4103/IJO.IJO_2996_23
15. Salgado R, Torres P, Marinho AAP. Update on femtosecond laser-assisted cataract surgery: a review. Clin Ophthalmol. 2024;18:459–472. doi:10.2147/OPTH.S453040
16. Zhao L, Tan M, Zhang J, et al. Comparative study of FLACS vs conventional phacoemulsification for cataract patients with high myopia. J Cataract Refract Surg. 2024;50(6):624–630. doi:10.1097/j.jcrs.0000000000001425
17. Lee YW, Cho KS, Hyon JY, Han SB. Application of femtosecond laser in challenging cataract cases. Asia Pac J Ophthalmol. 2023;12(5):477–485. doi:10.1097/APO.0000000000000627
18. Chen CW, Lee YH, Gerber MJ, et al. Intraocular robotic interventional surgical system (IRISS): semi-automated OCT-guided cataract removal. Int J Med Robot. 2018;14(6):e1949. doi:10.1002/rcs.1949
19. Gerber MJ, Hubschman JP, Tsao TC. Robotic posterior capsule polishing by optical coherence tomography image guidance. Int J Med Robot. 2021;17(3):e2248. doi:10.1002/rcs.2248
20. Reddy K, Gharde P, Tayade H, Patil M, Reddy LS, Surya D. Advancements in robotic surgery: a comprehensive overview of current utilizations and upcoming frontiers. Cureus. 2023;15(12):e50415. doi:10.7759/cureus.50415
21. Maynou L, McGuire A, Serra-Sastre V. Efficiency and productivity gains of robotic surgery: the case of the English National Health Service. Health Econ. 2024;33(8):1831–1856. doi:10.1002/hec.4838
22. Okamura A, Mataric M, Christensen H. Medical and health-care robotics. IEEE Robot Autom Mag. 2010;17(3):26–37. doi:10.1109/mra.2010.937861
23. Rivera RP, Hoopes PC, Linn SH, Hoopes PC. Comparative analysis of the performance of two different platforms for femtosecond laser-assisted cataract surgery. Clin Ophthalmol. 2016;10:2069–2078. doi:10.2147/OPTH.S115483
24. Lin HY, Chuang YJ, Lin PJ. Surgical outcomes with high and low pulse energy femtosecond laser systems for cataract surgery. Sci Rep. 2021;11(1):9525. doi:10.1038/s41598-021-89046-1
25. Day AC, Burr JM, Bennett K, et al. Femtosecond laser-assisted cataract surgery versus phacoemulsification cataract surgery (FACT): a randomized noninferiority trial. Ophthalmology. 2020;127(8):1012–1019. doi:10.1016/j.ophtha.2020.02.028
26. Lundstrom M, Dickman M, Henry Y, et al. Femtosecond laser-assisted cataract surgeries reported to the European Registry of Quality Outcomes for Cataract and Refractive Surgery: baseline characteristics, surgical procedure, and outcomes. J Cataract Refract Surg. 2017;43(12):1549–1556. doi:10.1016/j.jcrs.2017.09.029
27. Narayan A, Evans JR, O’Brart D, Bunce C, Gore DM, Day AC. Laser-assisted cataract surgery versus standard ultrasound phacoemulsification cataract surgery. Cochrane Database Syst Rev. 2023;6(6):CD010735. doi:10.1002/14651858.CD010735.pub3
28. Schein OD. Femtosecond laser-assisted cataract surgery-conclusive evidence of lack of incremental value. JAMA Ophthalmol. 2023;141(7):629–630. doi:10.1001/jamaophthalmol.2023.1828
29. George DS, Ainslie-Garcia MH, Ferko NC, Cheng H. Successful implementation of femtosecond laser-assisted cataract surgery: a real-world economic analysis. Clin Ophthalmol. 2021;15:923–929. doi:10.2147/OPTH.S293111
30. Bartlett JD, Miller KM. The economics of femtosecond laser-assisted cataract surgery. Curr Opin Ophthalmol. 2016;27(1):76–81. doi:10.1097/ICU.0000000000000219
31. Roberts HW, Ni MZ, O’Brart DP. Financial modelling of femtosecond laser-assisted cataract surgery within the National Health Service using a ‘hub and spoke’ model for the delivery of high-volume cataract surgery. BMJ Open. 2017;7(3):e013616. doi:10.1136/bmjopen-2016-013616
32. Khodabakhsh AJ, Hofbauer J. Contralateral eye comparison of the phacoemulsification metrics, patient experience and clinical outcomes in patients undergoing bilateral cataract surgery with two commonly used femtosecond laser systems. Clin Ophthalmol. 2018;12:1391–1398. doi:10.2147/OPTH.S164513
33. Heit L, Datar M, Kyriakakos M, et al. Comparing the time efficiency of two lasers used in FLACS: real-world observational study. J Cataract Refract Surg. 2024;50(2):116–121. doi:10.1097/j.jcrs.0000000000001321
34. Weinstock R. Safety, efficacy, and complication rates utilizing a second generation femtosecond laser for FLACS compared to manual phaco.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.