Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Efficacy of Transcutaneous Electrical Acupoint Stimulation Applied During the Post-Anesthesia Recovery Period in Improving Postoperative Recovery Quality After Gynecological Laparoscopic Surgery: A Randomized Controlled Trial
Authors Zhou Z ![]() , Yang X, Shi M
, Yang X, Shi M ![]() , Huang L, Wu D, Yang H, Zhang X
, Huang L, Wu D, Yang H, Zhang X ![]()
Received 2 December 2024
Accepted for publication 20 July 2025
Published 24 July 2025 Volume 2025:21 Pages 1175—1186
DOI https://doi.org/10.2147/TCRM.S507856
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor De Yun Wang
Zhihu Zhou,* Xiang Yang,* Min Shi, Liqiao Huang, Danping Wu, Huailong Yang, Xu Zhang
Department of Anesthesiology, The Second Affiliated Hospital of Guilin Medical University, Guilin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xu Zhang, Department of Anesthesiology, The Second Affiliated Hospital of Guilin Medical University, No. 212, Renmin Road, Lingui District, Guilin, Guangxi, 541199, People’s Republic of China, Tel +86 189 3477 9973, Email [email protected]
Purpose: Transcutaneous electrical acupoint stimulation (TEAS) has emerged as a promising non-pharmacological intervention to enhance postoperative recovery. However, its application during the post-anesthesia recovery period remains underexplored. This study investigated the impact of TEAS during the post-anesthesia recovery period on postoperative recovery quality in patients undergoing laparoscopic gynecological surgery.
Patients and Methods: In this single-center, randomized, double-blinded, sham-controlled trial, 100 patients undergoing elective gynecological laparoscopic surgery were randomly allocated to receive either TEAS or sham stimulation at bilateral Hegu (LI4), Neiguan (PC6), Zusanli (ST36), and Sanyinjiao (SP6) acupoints for 30 minutes during the post-anesthesia recovery period in the post-anesthesia care unit (PACU). The primary outcome was the Quality of Recovery-15 (QoR-15) score assessed on postoperative days (POD) 1, 2, and 3. Secondary outcomes included pain, postoperative nausea and vomiting (PONV), recovery times, and adverse events.
Results: Ninety-seven patients completed the study, with 48 in the TEAS group and 49 in the Sham group. The TEAS group exhibited significantly higher QoR-15 scores on POD 1 compared to the Sham group, with improvements in emotional state, physical comfort, and pain dimensions. On POD 2, the TEAS group had significantly higher pain dimension scores. The TEAS group also reported lower resting VAS scores on POD 1 and lower exercise VAS scores on POD 1 and 2. The incidence of PONV was lower on POD 1, with fewer patients requiring rescue antiemetics. Additionally, the TEAS group experienced shorter times to first flatus and ambulation. Adverse events were comparable between the groups, with no local skin irritation noted in the TEAS group.
Conclusion: TEAS applied during the post-anesthesia recovery period significantly improves early postoperative recovery quality, reduces pain and PONV, and accelerates functional recovery in patients undergoing gynecological laparoscopic surgery.
Keywords: TEAS, post-anesthesia recovery period, gynecological laparoscopic surgery, postoperative recovery quality, QoR-15
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Huang has been published for this article.
Introduction
In recent decades, gynecological laparoscopic surgery has revolutionized the management of various benign and malignant conditions of the female reproductive system, providing numerous benefits over traditional open surgery. These minimally invasive procedures are linked to smaller incisions, decreased blood loss, fewer postoperative complications and accelerated recovery times.1,2 However, despite these advantages, patients undergoing gynecological laparoscopic surgery often experience significant postoperative discomfort, pain, and functional limitations. Studies show that 60–80% of patients report moderate to severe pain within the first 24 hours, with complete functional recovery typically requiring 3–7 days.3,4 Additionally, 30–50% suffer from postoperative nausea and vomiting,5 which can negatively impact their recovery and overall well-being.6,7 Therefore, identifying effective strategies to optimize postoperative recovery in this patient population remains a critical challenge.
To address these issues, interest in non-pharmacological interventions for enhancing postoperative recovery quality has grown.8–10 Transcutaneous Electrical Acupoint Stimulation (TEAS), based on traditional Chinese medicine (TCM) principles, has shown promise as an adjunct therapy.11 TEAS involves applying low-frequency electrical stimulation to specific acupuncture points on the body’s surface. This non-invasive modality has been demonstrated to exert various therapeutic effects, including pain relief,12 anti-inflammatory action,13 and modulation of autonomic nervous system function.14 The underlying mechanisms may involve the activation of peripheral nerves and the subsequent release of neurotransmitters and endogenous opioids, contributing to the regulation of nociception and the stress response.15,16
Numerous studies have investigated the efficacy of TEAS in various surgical settings, demonstrating its potential to reduce postoperative pain,17 PONV,18 and accelerate gastrointestinal function recovery.19 However, the application of TEAS specifically during the post-anesthesia recovery period and its impact on recovery quality in gynecological laparoscopic surgery patients remains insufficiently studied. The post-anesthesia recovery period, encompassing time in the PACU, represents a critical phase marking the transition from unconsciousness to consciousness and the onset of recovery.20 Interventions administered during this period have the potential to influence the course of recovery and patient outcomes. Therefore, exploring the application of TEAS during this specific phase is of great significance for improving postoperative recovery quality.
To comprehensively evaluate the quality of postoperative recovery, the present study employs the Quality of Recovery-15 (QoR-15) questionnaire, a well-validated and widely utilized patient-reported outcome measure designed to assess multiple aspects of recovery, including emotional state, physical comfort, psychological support, physical independence, and pain.21–23 By adopting this multidimensional approach, this study aims to investigate the efficacy of TEAS applied during the post-anesthesia recovery period on the overall quality of recovery in gynecological laparoscopic surgery patients. Our hypothesis posits that TEAS administration will result in improved QoR-15 scores, indicating enhanced postoperative recovery across multiple domains. This study’s findings may inform clinical practice, guide the development of enhanced recovery protocols, and potentially improve patient outcomes and satisfaction following gynecological laparoscopic surgery.
Methods
Study Design
This study was conducted at the Second Affiliated Hospital of Guilin Medical University in accordance with the Declaration of Helsinki. Patient recruitment took place from February 1, 2022 to June 20, 2022. The Ethics Committee of the Second Affiliated Hospital of Guilin Medical University approved the study protocol (NO. ZYYJ_2021001) and the study was prospectively registered in the Chinese Clinical Trial Registry (ChiCTR2200055338) on January 7, 2022. The manuscript adheres to the CONSORT reporting guidelines.
Participants
Eligibility screening was conducted for patients scheduled to undergo elective gynecological laparoscopic surgery under general anesthesia. Inclusion criteria were as follows: (1) Age range: 18–65 years; (2) American Society of Anesthesiologists (ASA) physical status I–III; (3) Capacity to provide written informed consent. Patients were excluded if they: (1) participation in other clinical trials within 4 weeks prior to surgery; (2) severe cardiovascular, respiratory, hepatic, or renal dysfunction; (3) history of neurological or psychiatric disorders or long-term use of sedative medications; (4) severe cognitive, visual, or hearing impairment, or severe motor disorders that could hinder cooperation with the study; or (5) skin infection, damage, or scarring at the acupoint sites. Eligible patients were approached by trained research personnel, informed about the study, including details on randomization, procedures, and potential risks and benefits. They were given time to consider their participation. Written informed consent was obtained from all participants, who were advised of their right to withdraw at any time without impacting their clinical care.
Sample Size Calculation
A preliminary study involving 10 patients (5 per group) was conducted to assess the study protocol’s feasibility and inform sample size calculation. The primary outcome, the QoR-15 score one day post-surgery, was significantly higher in the TEAS group (111.1 ± 9.7) compared to the control group (105.3 ± 9.5). Based on these preliminary results, sample size calculation using PASS 15 software (assuming a two-sided α of 0.05, 80% power, 1:1 allocation ratio, and 10% dropout rate) determined that 98 patients (49 per group) were required. To ensure adequate statistical power, the final sample size was set at 50 patients per group, totaling 100 patients.
Randomization and Blinding
Participants underwent randomization into either the TEAS or Sham group at a 1:1 ratio, utilizing a computer-generated randomization sequence. Allocation was concealed using sequentially numbered, sealed, opaque envelopes. An independent research assistant, uninvolved in patient recruitment, intervention, or outcome assessment, opened these envelopes sequentially in the PACU just before the intervention to reveal group assignment. Patients, anesthesiologists, surgeons, and data collectors remained blinded to group allocation. Due to the nature of the intervention, the acupuncturist administering TEAS could not be blinded. To maintain blinding, the acupuncturist adhered to a standardized interaction protocol for both groups. This involved scripted explanations, identical application of electrodes and device operation, and neutral responses to inquiries, avoiding any cues about group allocation. Patients were informed they would receive electrical acupoint stimulation, Sham TEAS was performed using the same protocol as real TEAS, but without electrical current output from the stimulator.
Anesthesia Management
Experienced anesthesiologists administered standard general anesthesia with endotracheal intubation to all patients, adhering to the institutional protocol. Monitoring included electrocardiography, noninvasive blood pressure, pulse oximetry, end-tidal carbon dioxide (PetCO2), and bispectral index (BIS). Anesthesia was induced after sufficient denitrogenation using midazolam (0.05 mg/kg), etomidate (0.2 mg/kg), cisatracurium (0.2 mg/kg), and sufentanil (0.5 μg/kg). Once sufficient muscle relaxation was achieved, endotracheal intubation was performed. Mechanical ventilation was adjusted to maintain PetCO2 between 35–45 mmHg.
Anesthesia was maintained with continuous infusion of propofol (4–10mg/kg/h) and remifentanil (0.1–0.4μg/kg/min), supplemented with intermittent sevoflurane inhalation (1.0–2.0%) to keep BIS values between 40 and 60 and vital signs within 20% of baseline values. Patients received flurbiprofen axetil (50 mg) and sufentanil (0.1 μg/kg) for postoperative pain management, and tropisetron (5 mg) for PONV prophylaxis, 30 minutes prior to the conclusion of surgery. Ropivacaine (0.5%, 10 mL) was infiltrated at the abdominal incision site for local analgesia at the conclusion of the surgery. All patients were transferred to the PACU with endotracheal tubes, maintaining continued monitoring and respiratory support until they met the extubation criteria. Discharge from the PACU occurred after meeting the modified Aldrete criteria. Postoperative pain management included intravenous tramadol (50–100 mg) every 6 hours as needed, at the discretion of the treating gynecologists.
TEAS Intervention
After patients arrived at PACU and their vital signs stabilized, the TEAS intervention was conducted in the PACU by a certified acupuncturist using the SDZ-II acupoint nerve stimulator (Hwato, Suzhou Medical Appliance Factory, China). The intervention involved stimulating four pairs of acupoints—LI4 (Hegu), PC6 (Neiguan), ST36 (Zusanli), and SP6 (Sanyinjiao)—located according to the WHO Standard Acupuncture Point Locations (Figure 1).24 These acupoints were strategically selected for their established therapeutic roles in postoperative recovery: LI4 (Hegu) is primarily used for its potent analgesic effects;25 PC6 (Neiguan) is a key point for preventing nausea and vomiting,26 ST36 (Zusanli) and SP6 (Sanyinjiao) are known to modulate gastrointestinal motility and regulate autonomic function.27,28 A more detailed mechanistic discussion of these effects is provided in the Discussion section. The stimulation parameters were set to an alternating dense-disperse wave mode at 2/10 Hz, with an intensity of 10–15 mA and a duration of 30 minutes. Prior to anesthesia induction, the optimal intensity for each patient was determined by gradually increasing the current until the patient experienced a strong but comfortable “De Qi” sensation, a traditional Chinese medicine indicator of effective stimulation.29 This intensity was then applied during the TEAS intervention in the PACU.
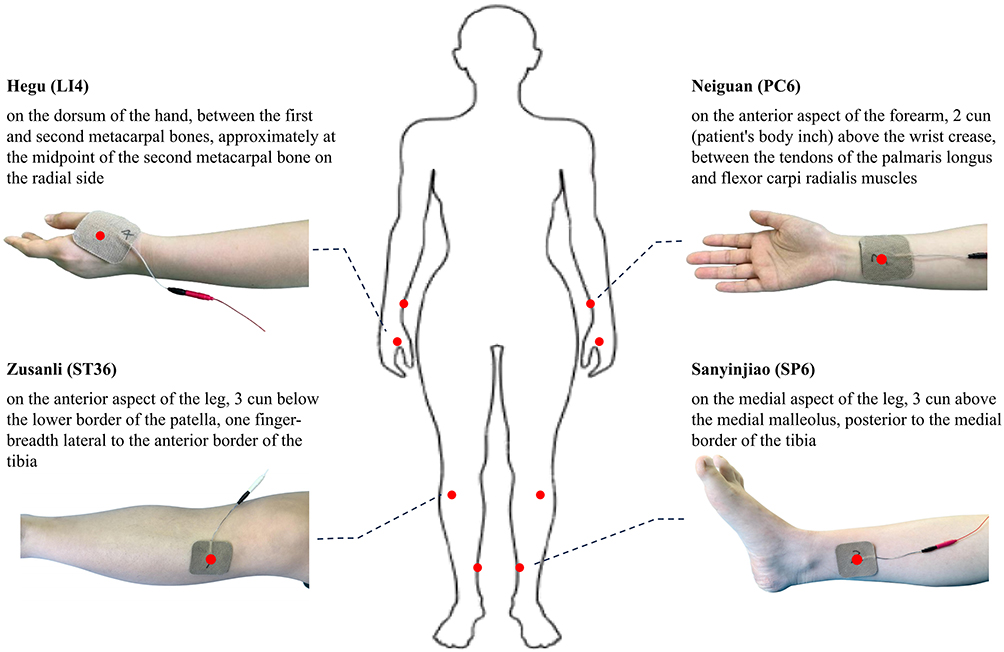 |
Figure 1 Body Surface Location of PC6, LI4, ST36 and SP6. |
Outcome Measurements
The primary outcome was the QoR-15 score, assessed at baseline (one day before surgery) and on POD 1, 2, and 3. The QoR-15 is a validated, patient-reported questionnaire that evaluates five dimensions of recovery: physical comfort, emotional state, physical independence, psychological support, and pain. The total QoR-15 score ranges from 0 to 150, with higher scores indicating better overall recovery quality. In this study, QoR-15 scores were compared between groups at each time point, and the scores for each dimension were analyzed separately.
Secondary outcomes included: (1) Postoperative pain and analgesic consumption: Pain levels were measured using a Visual Analog Scale (VAS) at rest and during exercise (coughing and movement) preoperatively and on POD 1, 2, and 3. Rescue analgesic consumption: Proportion of patients requiring additional analgesics within the first three postoperative days. (2) PONV: PONV was assessed by recording its incidence and the proportion of patients requiring rescue antiemetics within the first three postoperative days. (3) Recovery times: Recovery times included time to awakening (from the end of surgery to eye opening on command), time to extubation (from the end of surgery to extubation), time to first flatus, and time to first ambulation. (4) Adverse events: Adverse events included dizziness, headache, hypertension (SBP> 180 mmHg or DBP> 100 mmHg), hypotension (SBP < 90 mmHg or a decrease of > 30% from the baseline blood pressure), hypoxemia (pulse oxygen saturation < 92%), and local skin irritation at the acupoint sites. The occurrence of these adverse events was recorded during the first three postoperative days.
Statistical Analysis
Data were analyzed using SPSS version 27.0. The normality of data distribution was assessed with the Shapiro–Wilk test. For continuous variables that followed a normal distribution, outcomes were expressed as mean ± standard deviation and compared via independent samples t-tests. In cases where continuous variables did not conform to a normal distribution, they were reported as median with interquartile ranges and evaluated using the Mann–Whitney U-test. Categorical data were presented as frequencies and percentages, and were examined using either the chi-square test or Fisher’s exact test, depending on suitability. Statistical significance was determined at a two-sided P-value of less than 0.05.
Results
Initially, 127 patients were assessed for study eligibility. Out of these, 18 patients did not meet the inclusion criteria and 9 declined participation. Consequently, 100 patients were successfully enrolled and subsequently randomized into two distinct groups: the TEAS group (n=50) and the Sham group (n=50). Each participant received the intervention assigned to their respective group. During the postoperative assessment period, two patients from the TEAS group and one from the Sham group were lost due to their decision to withdraw. Ultimately, 97 patients completed the study, with 48 from the TEAS group and 49 from the Sham group. The data from these participants were incorporated into the final analysis. An overview of the recruitment, allocation, postoperative assessment, and analysis of the trial participants is illustrated in Figure 2.
 |
Figure 2 CONSORT 2010 flow chart of randomized controlled trials. |
Demographic and Intraoperative Characteristics
A comparison of the baseline demographics and intraoperative characteristics of the TEAS and Sham groups is presented in Table 1. Age, height, weight, and ASA physical status did not differ significantly between the two groups (P > 0.05). The distribution of surgical types, including ovarian and tubal surgery, uterine surgery, gynecologic oncologic Surgery, and other surgeries, was also comparable between the TEAS and Sham groups (P > 0.05). Furthermore, the analysis revealed no statistically significant differences in the duration of surgery and anesthesia between the two groups (P > 0.05). Intraoperative fluid input volume, urine volume, and intraoperative bleeding volume were also similar between the groups (P > 0.05).
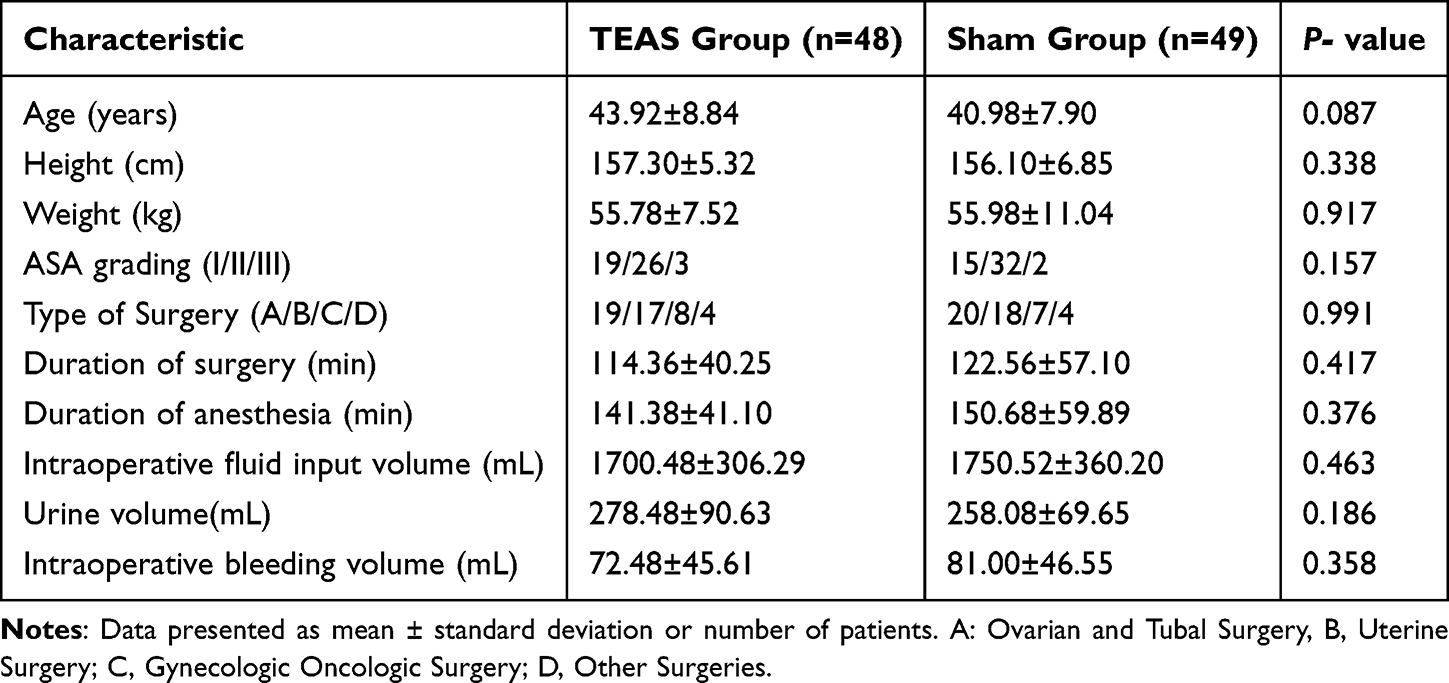 |
Table 1 Demographic and Intraoperative Characteristics |
Primary Outcomes
The QoR-15 total and dimensional scores for the TEAS and Sham groups at various time points are presented in Table 2. Preoperatively, there were no significant differences in the QoR-15 total and dimensional scores between the TEAS and Sham groups (P>0.05). On POD 1, the TEAS group showed a significantly higher global QoR-15 score compared to the Sham group (112.00±10.67 vs 107.62±10.27, P=0.042), with notable improvements in emotional state (30.10±3.07 vs 28.59±3.42, P=0.024), physical comfort (36.83±3.31 vs 35.30±3.52, P=0.030), and pain (14.18±2.91 vs 12.47±2.92, P=0.005) dimensions. On POD 2, despite no significant difference in the global QoR-15 scores between the two groups (P>0.05), the TEAS group exhibited significantly higher scores in the pain dimension (16.54±2.66 vs 15.10±2.97, P = 0.014). On POD 3, no significant differences were found in the QoR-15 total and dimensional scores between the groups (P>0.05).
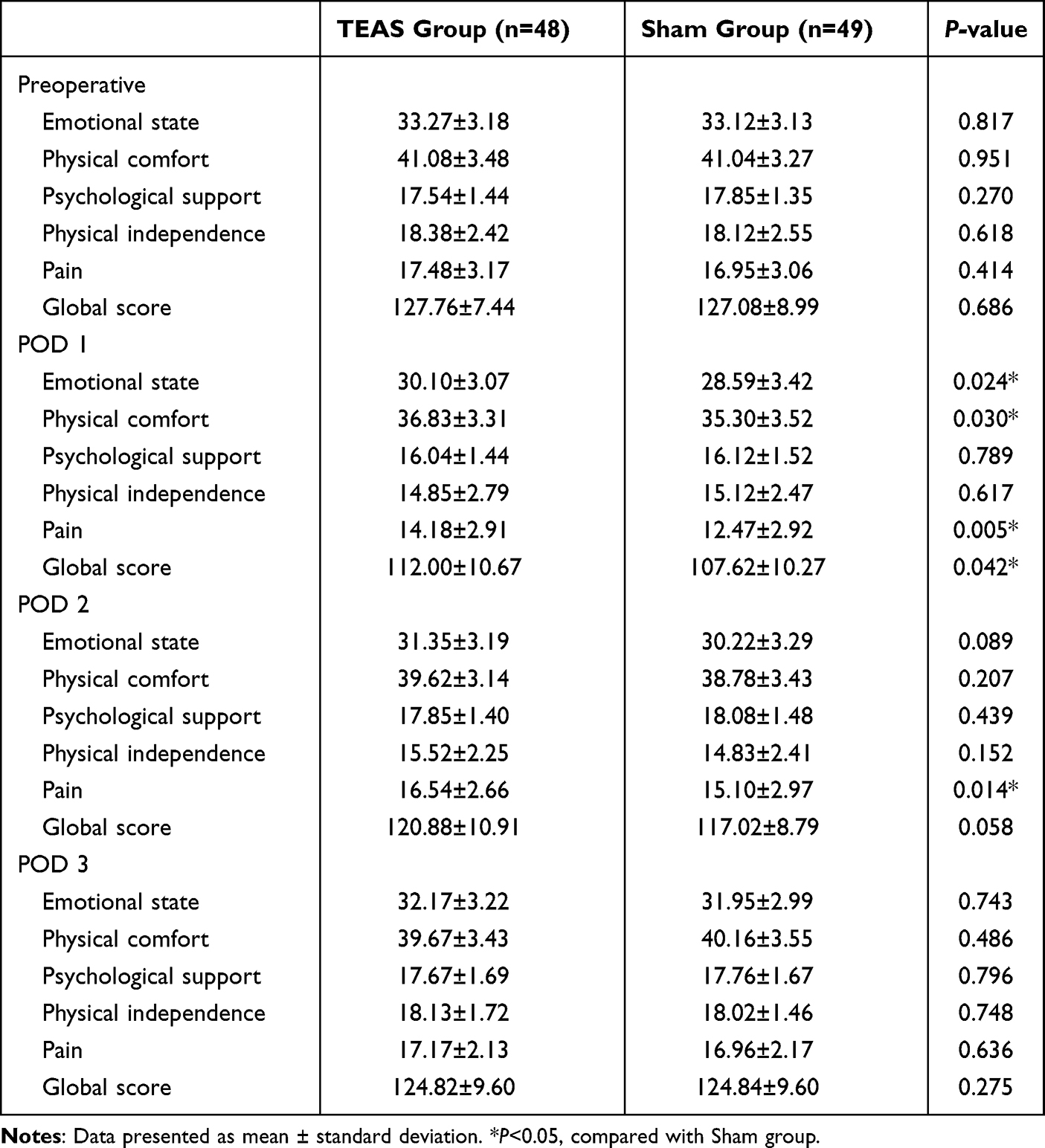 |
Table 2 QoR-15 Total and Dimensional Scores |
Secondary Outcomes
Table 3 presents a comparative analysis of postoperative pain intensity (VAS scores) and analgesic requirements between the TEAS and Sham groups. Preoperative VAS scores, both at rest and during exercise, showed no statistically significant differences between the groups (P>0.05). The TEAS group demonstrated significantly lower VAS scores compared to the Sham group: at rest on POD 1 [3 (3–4) vs 4 (4–5), P<0.001], and during exercise on both POD 1 [4 (4–5) vs 5 (4–6), P=0.008] and POD 2 [2 (2–3) vs 4 (3–4), P=0.036]. The TEAS group exhibited a lower proportion of patients requiring rescue analgesia within the first three postoperative days (12.5% vs 26.5% in the Sham group), although this difference did not reach statistical significance (P=0.124).
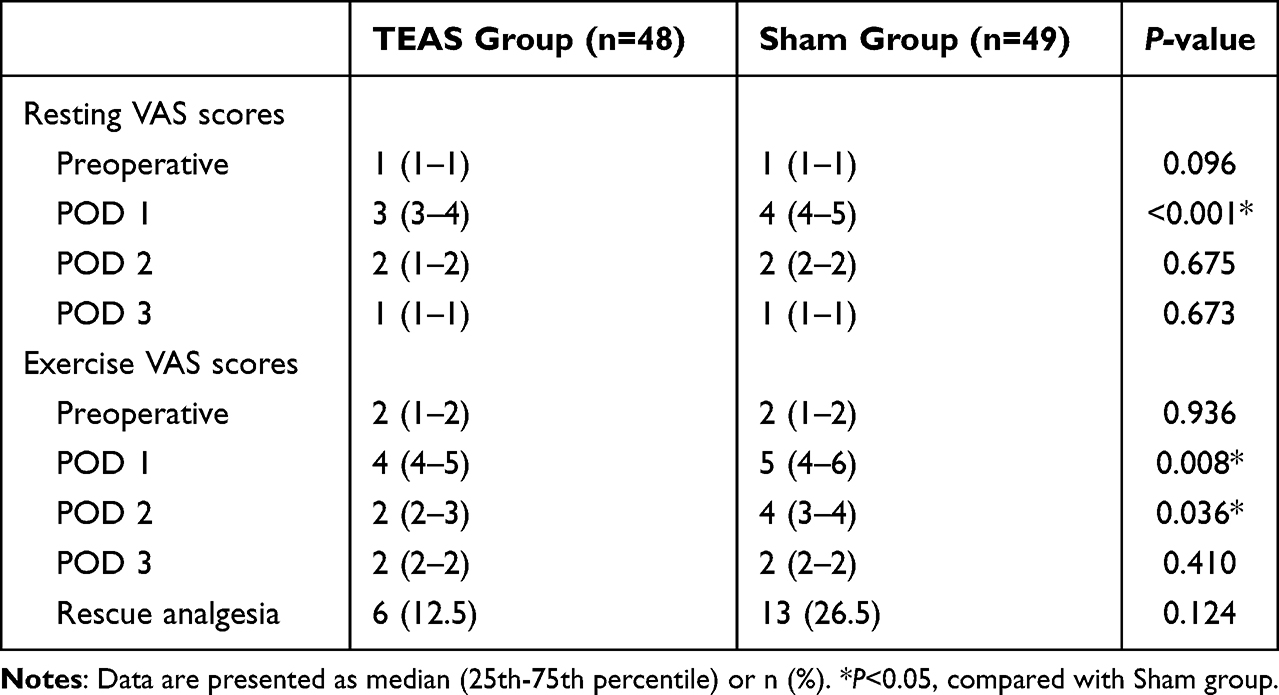 |
Table 3 VAS Scores and Rescue Analgesia |
Table 4 illustrates the prevalence of PONV and the frequency of rescue antiemetic administration. On POD 1, the TEAS group had a significantly lower incidence of PONV compared to the Sham group (20.8% vs 38.7%; P=0.047). No statistically significant intergroup differences in PONV incidence were observed on POD 2 or POD 3 (P>0.05). Within the first three postoperative days, the TEAS group demonstrated a significantly lower requirement for rescue antiemetics compared to the Sham group (20.8% vs 40.8%, P=0.033).
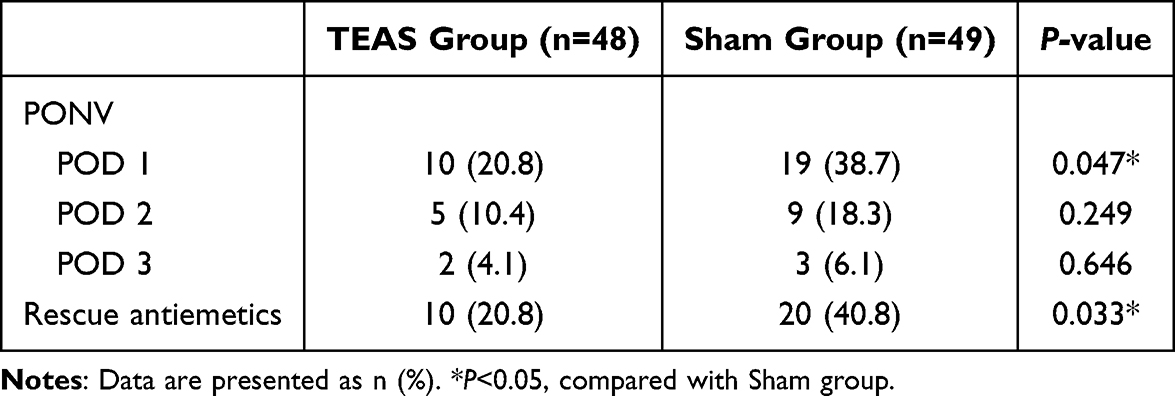 |
Table 4 Incidence of PONV and Rescue Antiemetics |
Table 5 shows no significant differences in time to awakening and extubation between the TEAS and Sham groups (P>0.05). Compared to the Sham group, the TEAS group had significantly shorter times to first flatus (14.10±3.19 vs 15.88±3.78 hours, P = 0.014) and first ambulation (17.50±3.40 vs 19.42±4.03 hours, P = 0.013).
 |
Table 5 Recovery Parameters |
Table 6 presents the occurrence of adverse events in the TEAS and Sham groups. The incidence of adverse events was low in both groups, with no statistically significant intergroup differences observed (P>0.05). No local skin irritation related to acupoint electrical stimulation was observed in the TEAS group.
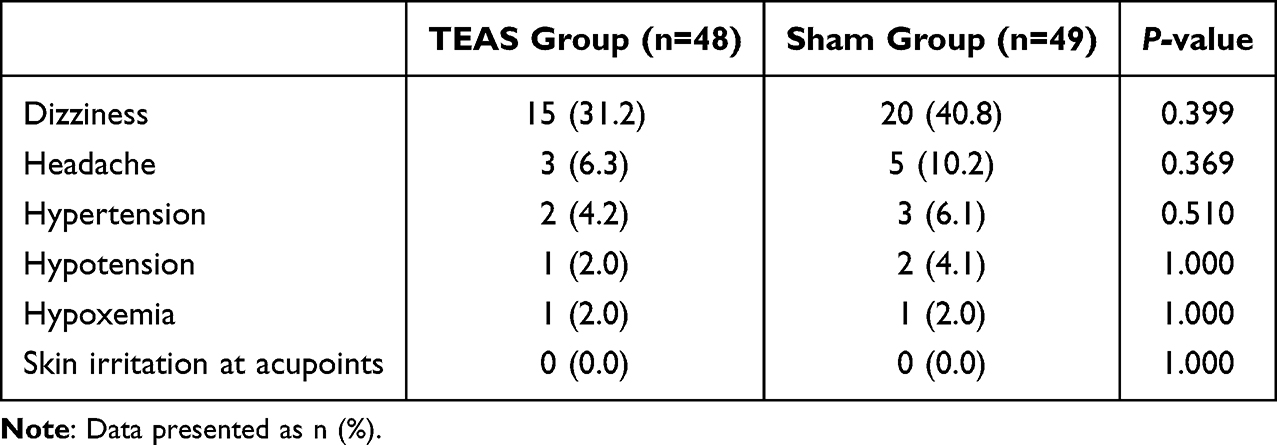 |
Table 6 Adverse Events |
Discussion
This study evaluated the impact of TEAS during post-anesthesia recovery on postoperative recovery quality in patients after gynecological laparoscopic surgery. Our findings indicate that TEAS significantly enhances early postoperative recovery quality, as measured by the QoR-15 scale, with notable improvements in emotional state, physical comfort, and pain dimensions. Additionally, TEAS effectively alleviates postoperative pain, reduces the incidence of PONV, and promotes early recovery of gastrointestinal function and postoperative mobility in these patients.
Post-operative recovery is a complex process involving physiological, psychological, and social aspects, requiring a patient-centred assessment from multiple dimensions. Numerous studies have consistently demonstrated the efficacy of TEAS in enhancing postoperative recovery quality, particularly through improvements in Quality of Recovery-40 (QoR-40) scores across various surgical populations.23,30,31 A recent meta-analysis confirmed these findings, showing improved QoR-40 scores at 24 and 48 hours post-surgery in patients receiving TEAS.32 Our study employed the QoR-15 scale, a shorter yet well-validated measure for evaluating postoperative recovery, chosen for its conciseness, ease of administration, and reduced patient burden.33 In line with our hypothesis, the TEAS group exhibited significantly higher global QoR-15 scores on POD 1 compared to the Sham group, indicating better overall recovery quality. Our analysis revealed significant improvements in emotional state, physical comfort, and pain dimensions in the TEAS group on POD 1, and in the pain dimension on POD 2. These results suggest that TEAS positively influences psychological well-being, reduces postoperative discomforts, and provides effective pain relief, collectively contribute to enhanced recovery quality. The observed benefits of TEAS across different assessment tools underscore its versatility and broad applicability in improving postoperative recovery outcomes.
Our study demonstrated that TEAS effectively alleviated postoperative pain, as evidenced by lower resting VAS scores in the TEAS group on POD1 and lower exercise VAS scores on POD 1 and POD 2. Although VAS score differences between groups were modest (1–2 points), these changes met the minimal clinically important difference (MCID) of 0.99 points established for acute postoperative pain.34 The 20–25% relative reduction in pain scores, achieved alongside standard multimodal analgesia, represented a clinically meaningful improvement.35 This was further supported by associated improvements in functional recovery outcomes (earlier ambulation and flatus) and overall recovery quality (QoR-15 scores). This finding aligns with the results reported by Yao et al and Yu et al who observed significant pain relief in patients undergoing gynecological laparoscopic surgery receiving TEAS.29,31 Several recent meta-analyses have also confirmed the efficacy of TEAS in reducing postoperative pain and decreasing the consumption of postoperative analgesics in patients undergoing various types of surgeries.36–38 The analgesic effects of TEAS are thought to be mediated through the activation of endogenous opioid pathways, leading to increased release of endorphins and enkephalins, which inhibit pain transmission at the spinal and supraspinal levels.39
PONV frequently occurs as a distressing complication after gynecological laparoscopic surgery.5 In our study, the incidence of PONV was significantly lower in the TEAS group on POD 1, and fewer patients in the TEAS group required rescue antiemetics within the first three postoperative days. According to these results, TEAS has antiemetic properties similar to those demonstrated in previous studies.40–42 The antiemetic effects of TEAS may be attributed to its regulatory impact on the autonomic nervous system and gastrointestinal motility, leading to improved gastric emptying and reduced nausea and vomiting.43
Functional recovery outcomes, such as time to first flatus and time to first ambulation, were significantly shorter in the TEAS group compared to the Sham group. These findings suggest that TEAS promotes the early recovery of gastrointestinal function and encourages early mobilization, which are crucial factors in postoperative recovery. These results align with the findings of Yao et al, who reported that TEAS significantly reduced the time to first bowel movement and accelerated overall recovery in patients undergoing gynecological laparoscopic surgery.44 Similarly, several studies have demonstrated the efficacy of TEAS in promoting postoperative gastrointestinal function recovery and early mobilization in patients undergoing various surgical procedures.27,45 The mechanisms underlying these benefits may involve the regulation of gastrointestinal motility, the reduction of postoperative pain and discomfort, and the attenuation of surgical stress and inflammatory responses.46
The application of TEAS during the post-anesthesia recovery period offers several advantages and holds significant clinical value. This critical phase of postoperative recovery presents an opportunity to implement interventions that can shape the recovery trajectory and improve patient outcomes.47 TEAS, being a non-invasive, safe, and easily applicable technique, can be seamlessly integrated into the PACU setting. Its simplicity and minimal risk profile make it an attractive option for enhancing postoperative recovery quality in patients undergoing gynecological laparoscopic surgery. TEAS has been shown to effectively modulate pain and inflammation, support autonomic nervous system balance, and promote both physiological and psychological recovery.48 By targeting this crucial period, TEAS can alleviate immediate postoperative discomfort and set a foundation for improved long-term recovery, highlighting its potential to become a standard component of enhanced recovery protocols.
To optimize these therapeutic benefits, the selection of appropriate acupoints is crucial. This study utilized four classical acupoints: PC6, LI4, ST36, and SP6. PC6, located on the pericardium meridian, is a well-documented point for preventing postoperative nausea and vomiting through its regulatory effects on gastrointestinal function and autonomic nervous system.26 LI4, the source point of the large intestine meridian, has been extensively studied for its analgesic properties and ability to modulate pain perception pathways.49 ST36, a key point on the stomach meridian, has demonstrated effects on gastrointestinal motility and vagal nerve activity, potentially contributing to improved postoperative recovery.50 SP6, an intersection point of the spleen, liver, and kidney meridians, has been shown to influence both digestive and endocrine functions.51 The combination of these specific acupoints was strategically chosen to comprehensively address post-surgical recovery needs in gynecological laparoscopic procedures.44
Nonetheless, our study has notable limitations. The generalizability of our findings may be limited by the single-center design and small sample size. Additionally, the short-term postoperative assessment period of three days does not provide insight into the long-term effects of TEAS on postoperative recovery. Thirdly, we did not assess patients’ beliefs or expectations regarding the TEAS treatment, which could have influenced their reported outcomes, although both groups received identical-appearing devices and attention from the acupuncturist. Future large-scale, multicenter trials with extended postoperative assessment periods are warranted to validate our results and explore the long-term impact of TEAS in this patient population.
Conclusion
In conclusion, TEAS applied during the post-anesthesia recovery period significantly improves early postoperative recovery quality, reduces pain and PONV, and accelerates functional recovery in patients undergoing gynecological laparoscopic surgery. These findings support the integration of TEAS into perioperative care protocols as a non-invasive, safe, and effective adjunct to enhance patient outcomes and satisfaction following gynecological laparoscopic surgery, potentially reducing reliance on pharmacological interventions.
Abbreviations
TEAS, Transcutaneous electrical acupoint stimulation; LI4, Hegu; PC6, Neiguan; ST36, Zusanli; SP6, Sanyinjiao; PACU, post-anesthesia care unit; QoR-15, Quality of Recovery-15; POD, postoperative days; PONV, postoperative nausea and vomiting; TCM, traditional Chinese medicine; VAS, Visual Analog Scale.
Data Sharing Statement
The datasets used during this study are available from corresponding authors on reasonable request.
Author Contributions
Zhihu Zhou and Xiang Yang made equal contributions to this work, serving as co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The present study is supported by the project of the Guangxi Medical and Health Appropriate Technology Development and Promotion Application Project (S2020108); Self-financed scientific research projects of the Administration of Traditional Chinese Medicine of the Guangxi Zhuang Autonomous Region (GXZYZ20210390); Middle-aged Teachers in Colleges and Universities in Guangxi (2020KY12023).
Disclosure
The authors state that they do not have any conflicts of interest.
References
1. Levy L, Tsaltas J. Recent advances in benign gynecological laparoscopic surgery. Faculty Rev. 2021;10:60. doi:10.12703/r/10-60
2. Sweterlitsch KM, Meyer R, Ohayon A, et al. Clinical trial racial and ethnic disparities in minimally invasive gynecologic surgery. J Minim Invasive Gynecol. 2024;31(5):414–422. doi:10.1016/j.jmig.2024.01.019
3. Ding X, Ma Y, Ma Y, et al. Efficacy of nonopioid analgesics and regional techniques for perioperative pain management in laparoscopic gynecological surgery: a systematic review and network meta-analysis. Int J Surg. 2023;109(11):3527–3540. doi:10.1097/JS9.0000000000000630
4. Lee SR, Shim S, Yu T, et al. Sources of pain in laparoendoscopic gynecological surgeons: an analysis of ergonomic factors and proposal of an aid to improve comfort. PLoS One. 2017;12(9):e0184400. doi:10.1371/journal.pone.0184400
5. Luo D, Huang Z, Tang S, et al. Risk analysis of postoperative nausea and vomiting in patients after gynecologic laparoscopic surgery. BMC Anesthesiol. 2024;24(1):345. doi:10.1186/s12871-024-02727-y
6. O’Neill AM, Calpin GG, Norris L, et al. The impact of enhanced recovery after gynaecological surgery: a systematic review and meta-analysis. Gynecologic Oncol. 2023;168:8–16. doi:10.1016/j.ygyno.2022.10.019
7. Kaya AC, Radosa MP, Zimmermann JSM, et al. Intraoperative and postoperative complications of gynecological laparoscopic interventions: incidence and risk factors. Arch Gynecol Obstet. 2021;304(5):1259–1269. doi:10.1007/s00404-021-06192-7
8. Ehinger LMG, Marte MK, Kozachik SL, et al. Nonpharmacologic pain management for patients in ambulatory extended recovery after minimally invasive gynecologic and urologic surgery. Oncol Nursing Forum. 2023;50(1):47–57. doi:10.1188/23.ONF.47-57
9. Zhao L, Guo Y, Zhou X, et al. The research progress of perioperative non-pharmacological interventions on postoperative cognitive dysfunction: a narrative review. Front Neurol. 2024;15:1369821. doi:10.3389/fneur.2024.1369821
10. Komann M, Weinmann C, Schwenkglenks M, et al. Non-pharmacological methods and post-operative pain relief: an observational study. Anesthesiol Pain Med. 2019;9(2):e84674. doi:10.5812/aapm.84674
11. Szmit M, Krajewski R, Rudnicki J, et al. Application and efficacy of transcutaneous electrical acupoint stimulation (TEAS) in clinical practice: a systematic review. Adv Clin Exp Med. 2023;32(9):1063–1074. doi:10.17219/acem/159703
12. Vickers AJ, Linde K. Acupuncture for chronic pain. JAMA. 2014;311(9):955–956. doi:10.1001/jama.2013.285478
13. Tan Z, Dong F, Wu L, et al. Transcutaneous electrical acupoint stimulation attenuated neuroinflammation and oxidative stress by activating SIRT1-induced signaling pathway in MCAO/R rat models. Experimental Neurology. 2024;373:114658. doi:10.1016/j.expneurol.2023.114658
14. Li YW, Li W, Wang ST, et al. The autonomic nervous system: a potential link to the efficacy of acupuncture. Frontiers in Neuroscience. 2022;16:1038945. doi:10.3389/fnins.2022.1038945
15. Chen LZ, Kan Y, Zhang ZY, et al. Neuropeptide initiated mast cell activation by transcutaneous electrical acupoint stimulation of acupoint LI4 in rats. Scientific Reports. 2018;8(1):13921. doi:10.1038/s41598-018-32048-3
16. Chen T, Zhang WW, Chu YX, et al. Acupuncture for pain management: molecular mechanisms of action. American J Chin Med. 2020;48(4):793–811. doi:10.1142/S0192415X20500408
17. Wang D, Shi H, Yang Z, et al. Efficacy and safety of transcutaneous electrical acupoint stimulation for postoperative pain: a meta-analysis of randomized controlled trials. Pain Research & Management. 2022;2022:7570533. doi:10.1155/2022/7570533
18. Wang N, Ding P, Zheng DY, et al. Wearable transcutaneous electrical acupoint stimulation bracelet for prevention of postoperative nausea and vomiting in patients undergoing hysteroscopic surgery: a randomised controlled trial. Br J Anaesth. 2022;129(4):e85–e7. doi:10.1016/j.bja.2022.06.028
19. Li WJ, Gao C, An LX, et al. Perioperative transcutaneous electrical acupoint stimulation for improving postoperative gastrointestinal function: a randomized controlled trial. J Integr Med. 2021;19(3):211–218. doi:10.1016/j.joim.2021.01.005
20. Phoebe S, Rachael C. Recovery and post-anaesthetic care. Anaesth Intensive Care Med. 2009;10(12):576–579. doi:10.1016/j.mpaic.2009.09.003
21. Léger M, Campfort M, Cayla C, et al. Postoperative quality of recovery measurements as endpoints in comparative anaesthesia studies: a systematic review. Br J Anaesth. 2021;126(6):e210–e2. doi:10.1016/j.bja.2021.03.008
22. Deshmukh PP, Chakole V. Post-anesthesia recovery: a comprehensive review of Sampe, Modified Aldrete, and White Scoring Systems. Cureus. 2024;16(10):e70935. doi:10.7759/cureus.70935
23. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
24. Lim S. WHO Standard Acupuncture Point Locations. Evid Based Complement Alternat Med. 2010;7(2):167–168. doi:10.1093/ecam/nep006
25. Lu Z, Wang Q, Sun X, et al. Transcutaneous electrical acupoint stimulation before surgery reduces chronic pain after mastectomy: a randomized clinical trial. J Clin Anesthesia. 2021;74:110453. doi:10.1016/j.jclinane.2021.110453
26. Lee A, Chan SK, Fan LT. Stimulation of the wrist acupuncture point PC6 for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev. 2015;2015(11):Cd003281. doi:10.1002/14651858.CD003281.pub4
27. Jiang T, Li J, Meng L, et al. Effects of transcutaneous electrical acupoint stimulation on gastrointestinal dysfunction after gastrointestinal surgery: a meta-analysis. Complementary Ther Med. 2023;73:102938. doi:10.1016/j.ctim.2023.102938
28. Kao TW, Lin J, Huang CJ, et al. Electroacupuncture of ST36 and PC6 for postoperative gastrointestinal recovery: a systematic review and meta-analysis. J Tradit Complement Med. 2024;14(6):666–674. doi:10.1016/j.jtcme.2024.03.014
29. Yuan HW, Ma LX, Qi DD, et al. The historical development of deqi concept from classics of traditional Chinese medicine to modern research: exploitation of the connotation of Deqi in Chinese medicine. Evid Based Complement Alternat Med. 2013;2013:639302. doi:10.1155/2013/639302
30. Zhang M, Zhang H, Li P, et al. Effect of transcutaneous electrical acupoint stimulation on the quality of postoperative recovery: a meta-analysis. BMC Anesthesiol. 2024;24(1):104. doi:10.1186/s12871-024-02483-z
31. Ge Y, Zheng J. The efficacy of transcutaneous electronic acupoint stimulation for improving postoperative recovery after gynecologic surgery: a systematic review and meta-analysis. Medicine. 2023;102(35):e34834. doi:10.1097/MD.0000000000034834
32. Pan Y, Shao Y, Chi Z, et al. Transcutaneous electrical acupoint stimulation accelerates the recovery of patients undergoing laparoscopic myomectomy: a randomized controlled trial. J Pain Res. 2023;16:809–819. doi:10.2147/JPR.S399249
33. Tan SY, Jiang H, Ma Q, et al. Effects of transcutaneous electrical acupoint stimulation on early postoperative pain and recovery: a comprehensive systematic review and meta-analysis of randomized controlled trials. Front Med. 2024;11:1302057. doi:10.3389/fmed.2024.1302057
34. Myles PS, Myles DB, Galagher W, et al. Measuring acute postoperative pain using the visual analog scale: the minimal clinically important difference and patient acceptable symptom state. Br J Anaesth. 2017;118(3):424–429. doi:10.1093/bja/aew466
35. Farrar JT, Young JP, LaMoreaux L, et al. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. doi:10.1016/S0304-3959(01)00349-9
36. Meng D, Mao Y, Song QM, et al. Efficacy and safety of transcutaneous electrical acupoint stimulation (TEAS) for postoperative pain in laparoscopy: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2022;2022:9922879. doi:10.1155/2022/9922879
37. Qiu L, Cai J, Mei A, et al. Predictors of postoperative nausea and vomiting after same-day surgery: a retrospective study. Clin Ther. 2023;45(3):210–217. doi:10.1016/j.clinthera.2023.01.013
38. Wang Y, Guo J, Cheng Y. A commentary on ‘transcutaneous electrical acupoint stimulation for preventing postoperative nausea and vomiting after general anesthesia: a meta-analysis of randomized controlled trials’. Int J Surg. 2024;110(6):3962–3963. doi:10.1097/JS9.0000000000001251
39. Qin J, Ye X, Ye C, et al. The effect of transcutaneous electrical acupoint stimulation on high-risk patients with PONV undergoing laparoscopic gynecologic surgery: a randomized controlled trial. J Clin Med. 2023;12(3):1192. doi:10.3390/jcm12031192
40. Gao W, Zhang L, Han X, et al. Transcutaneous electrical acupoint stimulation decreases the incidence of postoperative nausea and vomiting after laparoscopic non-gastrointestinal surgery: a multi-center randomized controlled trial. Front Med. 2022;9:766244. doi:10.3389/fmed.2022.766244
41. Tu LD, Li PC, Zhao Y, et al. Transcutaneous electrical acupoint stimulation for postoperative nausea and vomiting in patients undergoing craniotomy: a randomized controlled trial. Complementary Ther Clin Pract. 2024;54:101824. doi:10.1016/j.ctcp.2023.101824
42. Lu L, Xie C, Li X, et al. Efficacy and safety of electrical acupoint stimulation for postoperative nausea and vomiting: a systematic review and meta-analysis. PLoS One. 2023;18(5):e0285943. doi:10.1371/journal.pone.0285943
43. Li JL, Wang XJ, Rong JF. Transcutaneous electrical acupoint stimulation relieves post-operative nausea and vomiting possibly by reducing serum motilin secretion in patients undergoing laparoscopic surgery. Zhen Ci Yan Jiu. 2020;45(11):920–923. doi:10.13702/j.1000-0607.200060
44. Yao Y, Zhao Q, Gong C, et al. Transcutaneous electrical acupoint stimulation improves the postoperative quality of recovery and analgesia after gynecological laparoscopic surgery: a randomized controlled trial. Evid Based Complement Alternat Med. 2015;2015:324360. doi:10.1155/2015/324360
45. Zhang B, Hu Y, Shi X, et al. Integrative effects and vagal mechanisms of transcutaneous electrical acustimulation on gastroesophageal motility in patients with gastroesophageal reflux disease. The American Journal of Gastroenterology. 2021;116(7):1495–1505. doi:10.14309/ajg.0000000000001203
46. Zhang S, Guo W, Jiao Y, et al. Systematic review and meta-analysis of the effect of transcutaneous electrical acupoint stimulation on gastrointestinal function after laparoscopic surgery. Ann Palliative Med. 2021;10(11):11840–11848. doi:10.21037/apm-21-3046
47. Ludbrook G, Lloyd C, Story D, et al. The effect of advanced recovery room care on postoperative outcomes in moderate-risk surgical patients: a multicentre feasibility study. Anaesthesia. 2021;76(4):480–488. doi:10.1111/anae.15260
48. Zhang Q, Zhou M, Huo M, et al. Mechanisms of acupuncture-electroacupuncture on inflammatory pain. Mol Pain. 2023;19:17448069231202882. doi:10.1177/17448069231202882
49. Chavez LM, Huang SS, MacDonald I, et al. Mechanisms of acupuncture therapy in ischemic stroke rehabilitation: a literature review of basic studies. Int J Mol Sci. 2017;18(11):2270. doi:10.3390/ijms18112270
50. Chen KB, Huang Y, Jin XL, et al. Electroacupuncture or transcutaneous electroacupuncture for postoperative ileus after abdominal surgery: a systematic review and meta-analysis. Int J Surg. 2019;70:93–101. doi:10.1016/j.ijsu.2019.08.034
51. Abaraogu UO, Igwe SE, Tabansi-Ochiogu CS. Effectiveness of SP6 (Sanyinjiao) acupressure for relief of primary dysmenorrhea symptoms: a systematic review with meta- and sensitivity analyses. Complementary Ther Clin Pract. 2016;25:92–105. doi:10.1016/j.ctcp.2016.09.003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.