Back to Journals » Patient Preference and Adherence » Volume 20
Efficacy of Nurse-Led WIKAP Intervention on Hypoglycemia Coping Confidence and Outcomes in Adolescents with Type 1 Diabetes Mellitus: A Quasi-Experimental Study in Zhijiang, China
Authors Xiao W, Zheng D ![]() , Guo Q, Peng X
, Guo Q, Peng X
Received 15 January 2026
Accepted for publication 21 May 2026
Published 4 June 2026 Volume 2026:20 596598
DOI https://doi.org/10.2147/PPA.S596598
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Wei Xiao,1,* Dandan Zheng,2,* Qiaozhen Guo,3 Xiaoyan Peng1
1Department of Gastroenterology, Zhijiang People’s Hospital, Zhijiang, Hubei, People’s Republic of China; 2Xianning Medical College, Hubei University of Science and Technology, Xianning, Hubei, People’s Republic of China; 3Department of Gastroenterology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoyan Peng, Department of Gastroenterology, Zhijiang People’s Hospital, Zhijiang, Hubei, People’s Republic of China, Email [email protected]
Background: Hypoglycemia is a frequent and burdensome complication in adolescents with type 1 diabetes mellitus (T1DM). Despite its high prevalence, structured interventions targeting hypoglycemia coping confidence remain scarce, especially in China. This study evaluated the effectiveness of the nurse’s web-based Information-Knowledge-Attitude-Practice (WIKAP) model in improving coping confidence, reducing hypoglycemia events, and enhancing caregiver satisfaction.
Methods: This quasi-experimental, non-randomized controlled trial was conducted in the Endocrinology Department of a tertiary hospital in Zhijiang, China. A total of 110 adolescents with type 1 diabetes mellitus (T1DM) were assigned to either the WIKAP intervention group (n = 55) or routine care control group (n = 55) based on sequential enrollment period. The 8-week WIKAP intervention combined web-based and offline approaches targeting knowledge, attitude, and practice. Primary outcomes included hypoglycemia coping confidence measured by the Hypoglycemia Avoidance Behavior Scale (HABS; anxiety, avoidance, and confidence subscales), HbA1c levels, hypoglycemia incidence, and primary caregiver satisfaction. Descriptive statistics summarized baseline characteristics. Mixed-design ANOVA and MANOVA were used to analyze continuous outcomes over time, while chi-square tests compared categorical variables. Analyses were performed using SPSS 27.0 and R software.
Results: Doubly multivariate MANOVA revealed a significant Group × Time interaction (Pillai’s Trace = 0.855, p < 0.001). Compared with routine care, the 8-week WIKAP intervention significantly improved hypoglycemia coping confidence (reduced anxiety and enhanced confidence and total scores, all p < 0.001), lowered hypoglycemia incidence (p = 0.015), and increased caregiver satisfaction (p = 0.002), with no significant effect on HbA1c (p = 0.851).
Conclusion: The WIKAP model effectively improved hypoglycemia coping confidence, reduced hypoglycemia incidence, and enhanced caregiver satisfaction in adolescents with T1DM, without significant effect on HbAlc. These results support its integration into clinical diabetes care, with future multi-center studies needed to confirm long-term benefits.
Trial Registration: ChiCTR2500104670 (registered at Chinese Clinical Trial Registry).
Keywords: adolescents, type 1 diabetes mellitus, KAP model, hypoglycemia coping
Introduction
Type 1 diabetes mellitus (T1DM) is a chronic autoimmune disorder characterized by the destruction of pancreatic beta cells, leading to absolute insulin deficiency and lifelong dependence on exogenous insulin. The global incidence of T1DM among children and adolescents has been steadily increasing.1 In 2021, approximately 1.5 million individuals under the age of 20 worldwide were diagnosed with T1D.2 In China, this trend is particularly pronounced; the “Chinese Diabetes Prevention and Control Guidelines (2024 Edition)” reports a near fourfold increase in T1DM incidence among individuals under 15 years over the past two decades, positioning China as the fourth highest globally in terms of affected children and adolescents.3 Recent epidemiological data from China report approximately 68,816 cases of T1DM in children in 2021, with 10,559 new diagnoses.4 This growth trend is expected to continue over the next 15 years.5
Adolescents with T1DM face a heightened risk of hypoglycemia, a common and potentially life-threatening complication arising from insulin therapy mismatches with glucose levels.6 Mild (grade 1) hypoglycemic episodes occur frequently,7 often multiple times per week, while severe events contribute significantly to morbidity and mortality.8 Studies estimate that hypoglycemia accounts for 4–10% of deaths in children and adolescents with T1DM, with rates as high as 6.9 deaths per 1,000 person-years in affected individuals.9 Adolescents with T1DM encounter unique challenges in disease management, including developmental behaviors such as insulin restriction for weight control, fluctuating family dynamics, perceived social pressures, and negative coping strategies that foster pessimistic attitudes toward their condition.10 These barriers often exacerbate fear of hypoglycemia and impair hypoglycemic confidence (HC),11 defined as an individual’s perceived ability to safely manage and avoid hypoglycemia,12 which is essential for mitigating adverse outcomes and improving quality of life.13 However, existing interventions for hypoglycemia management in adolescents with T1DM often focus primarily on glycemic control and education, with limited emphasis on improving hypoglycemic confidence and related behavioral and psychological factors.
The web-based Information-Knowledge-Attitude-Practice (WIKAP) model serves as a structured health education framework that promotes personalized interventions by healthcare professionals to address patients’ specific needs, encouraging active participation in self-management and enhancing coping confidence.14 Importantly, the WIKAP framework aligns closely with the multidimensional nature of hypoglycemic confidence, as it targets not only knowledge acquisition but also cognitive and behavioral components, including risk perception, emotional responses, and self-management skills. By systematically improving patients’ understanding (Information/Knowledge), reshaping attitudes toward hypoglycemia (Attitude), and reinforcing appropriate self-care behaviors (Practice), WIKAP may provide a comprehensive approach to addressing the psychological and behavioral barriers underlying low hypoglycemic confidence. This relational nursing approach has demonstrated efficacy in managing various chronic diseases, including systemic lupus erythematosus, chronic obstructive pulmonary disease, cerebrovascular disease, Alzheimer’s disease, and gastric cancer, by improving health literacy, attitudes, and behaviors.15–18 Despite its success in these contexts, the WIKAP model has not been applied to hypoglycemia management in adolescent T1DM. Therefore, its application in this context is theoretically justified but remains empirically underexplored, highlighting the need for targeted investigation. Additionally, the WIKAP model provides a structured and patient-centered framework for nursing practice, enabling nurses to deliver more targeted, continuous, and individualized education and support, thereby enhancing the quality and effectiveness of diabetes care.
In pediatric T1DM management, primary caregivers play a critical role in daily glycemic control, including insulin administration, dietary regulation, and monitoring for hypoglycemic events. Adolescents often rely on caregivers for support in recognizing and managing hypoglycemia, particularly in complex or emergency situations. Caregivers’ knowledge, confidence, and psychological responses can directly influence adolescents’ self-management behaviors and health outcomes. Moreover, caregiver satisfaction and engagement are increasingly recognized as important indicators of intervention effectiveness, as they are closely associated with adherence, continuity of care, and overall treatment success. Despite this, many interventions primarily focus on patients while overlooking the integral role of caregivers. Therefore, incorporating caregiver-related outcomes is essential to provide a more comprehensive evaluation of diabetes management strategies.
With the rapid advancement of internet technology, web-based interventions have become increasingly feasible for continuous patient-provider communication, offering scalable tools to support diabetes self-management.19–21 However, evidence on WIKAP models specifically targeting HC in adolescent T1DM remains limited. Therefore, this study investigates the impact of a nurse-led WIKAP on hypoglycemic confidence among adolescents with T1DM, while also considering caregiver-related outcomes, aiming to provide empirical evidence for enhancing diabetes care through technology-integrated behavioral strategies.
Materials and Methods
Study Design
This prospective, non-concurrent controlled trial was conducted in the endocrinology department of a tertiary hospital in Zhijiang City, China. The department serves approximately 400 pediatric and adolescent patients with T1DM annually. It is staffed by 8 senior endocrinologists, 6 certified diabetes educators, and a specialized nursing team. Services provided include continuous glucose monitoring (CGM) training, insulin pump therapy, and comprehensive diabetes self-management education (DSME).
A quasi-experimental, non-randomized design was adopted to prioritize contamination control in a single-center clinical setting, where individual randomization would likely lead to treatment imitation among participants. Participants were purposively recruited from June to December 2025 to ensure a representative sample reflecting the clinical heterogeneity of adolescents with T1DM. To reduce group contamination, those enrolled from June to September 2025 formed the control group (n=55), receiving routine care, while those enrolled from October to December 2025 formed the intervention group (n=55), receiving the WIKAP model alongside routine care. Allocation was determined strictly by the period of enrollment (sequential allocation), and no randomization was applied after selection. The non-concurrent design was employed to allow sequential enrollment and control for temporal biases in outcomes.22 The trial lasted 8 weeks per participant, with assessments at baseline and follow-up. Ethical approval was granted by the Institutional Review Board of Zhijiang People’s Hospital (Approval No. ZJ2025-41). The study was conducted in accordance with the Declaration of Helsinki, and written informed consent was obtained from all participants or their legal guardians. This clinical trial was registered with the Chinese Clinical Trial Registry (registration number: ChiCTR2500104670).
Participants and Sample Size
Adolescents with T1DM were eligible if they met the following strict and objective inclusion criteria: (1) aged 10–24 years with a clinical diagnosis of T1DM; (2) history of hypoglycemic symptoms as per the American Diabetes Association (ADA) classification, defined as blood glucose <70 mg/dL (<3.9 mmol/L) for level 1 hypoglycemia; (3) adequate reading, comprehension, and communication skills; (4) awareness of their condition and willingness to provide informed consent; (5) access to an effective communication device (eg., smartphone) with parental oversight; and (6) regular use of bicycles or motor vehicles, which increases the risk of hypoglycemia during physical exertion. Exclusion criteria included: (1) cognitive impairment or psychiatric disorders; (2) severe comorbidities or T1DM complications (eg., advanced retinopathy or nephropathy); (3) withdrawal due to medical or personal reasons; (4) participation in other concurrent studies; and (5) repeated hospitalizations during the trial period. During screening, two independent researchers evaluated eligibility to minimize selection bias, with all screened individuals documented to ensure transparency.
Sample size was calculated based on prior studies of behavioral interventions in T1DM,23 targeting a medium effect size (Cohen’s d=0.5) on hypoglycemic confidence, with 80% power and α=0.05, resulting in approximately 50 participants per group, adjusted to 58 to account for 15% attrition. Baseline imbalances between groups will be adjusted as covariates in the final analysis to ensure internal validity.
Interventions
Control Group
Participants received standard care, including health education on T1DM management (diet, medication, and hypoglycemia prevention) and psychological support with referrals if needed. Follow-up occurred weekly during hospitalization and biweekly post-discharge via WeChat.
Intervention Group (WIKAP Model)
The WIKAP intervention, adapted from the KAP framework,24,25 utilized web-based tools for continuous nurse-led support. It consisted of three stages. Preparation Stage: A multidisciplinary team (chief nurse, two endocrinology nurses, psychological counselor, and head nurse) was formed. Baseline assessments using the Scale and a general questionnaire established personalized participant profiles. Implementation Stage: An 8-week tailored plan was developed based on WIKAP literature,26,27 delivered hybridly (in-person during hospitalization and web-based post-discharge). The intervention details are outlined in Table 1. Final Stage: All materials (scales, images, and records) were archived by a graduate student. A dedicated WeChat group was maintained for the intervention group, with files organized chronologically for easy access.
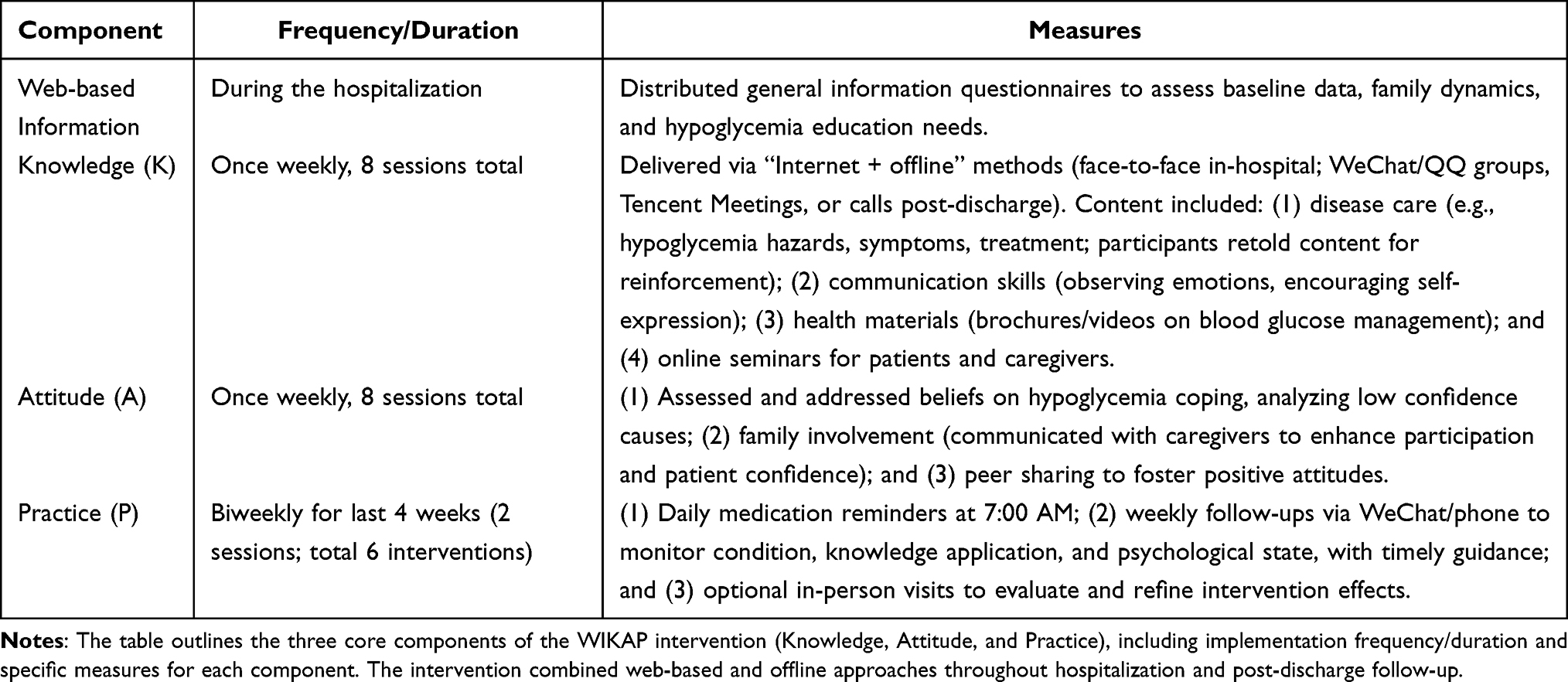 |
Table 1 WIKAP Model Intervention Plan for Hoglycemia Confidence in Adolescents T1DM |
Outcome Measures
Primary Outcome: Hypoglycemic Confidence
The Chinese version of the Hypoglycemia Attitudes and Behavior Scale (HABS) was used to assess anxiety, avoidance, and coping confidence related to hypoglycemia. Originally developed by Polonsky et al in 2015,28 the HABS consists of 14 items-5 items measuring anxiety, 4 items measuring avoidance, and 5 items measuring coping confidence. The scale is designed to assess the level of hypoglycemia fear and concern in diabetic patients.29 The Chinese version was adapted by Song in 2021,30 maintaining the same structure and scoring system. The scale uses a 5-point Likert scale, with responses ranging from “Never” (1) to “Always” (5). Total scores range from 14 to 70, with higher scores indicating greater concern about hypoglycemia. The Chinese adaptation demonstrated good reliability, with a Cronbach’s α coefficient of 0.893 and a split-half reliability of 0.816, making it a valid tool for assessing hypoglycemic attitudes and behaviors in Chinese patients with T1DM.
Secondary Outcomes
Glycated Hemoglobin (HbA1c)
HbA1c levels were measured as an indicator of long-term glycemic control. Venous blood samples were collected at baseline and at the 8-week follow-up, analyzed using high-performance liquid chromatography (HPLC) in a certified central laboratory. Results were expressed as percentages, with target values aligned to age-appropriate guidelines for adolescents with T1DM (typically <7.0–7.5%).31,32
Hypoglycemia Incidence
Hypoglycemia incidence was assessed as the frequency of events over the 8-week study period, self-reported via standardized participant diaries. Events were classified according to American Diabetes Association (ADA) guidelines: level 1 (blood glucose <70 mg/dL [<3.9 mmol/L] and ≥54 mg/dL [≥3.0 mmol/L]), level 2 (<54 mg/dL [<3.0 mmol/L]), and level 3 (severe events requiring assistance, regardless of glucose level).33 Participants were trained to record symptoms, confirmatory blood glucose readings (via glucometer), and any interventions. Incidence rates were calculated as events per participant-week, with separate reporting for total, nocturnal, and severe episodes to capture intervention impacts on hypoglycemia burden in adolescents.
Caregiver Satisfaction
A holistic nursing satisfaction survey evaluated caregivers’ perceptions of health education format, nursing competence, and hypoglycemia prevention confidence. Responses were categorized as very satisfied, satisfied, mostly satisfied, or Unsatisfied. The survey was administered anonymously at the 8-week follow-up to primary caregivers.
Data Collection
Two specialist nurses from the gastroenterology department (independent of the intervention team) administered baseline assessments (general data, HABS, HbA1c, and initial hypoglycemia diary instructions). Follow-up evaluations (HABS, HbA1c, hypoglycemia diaries, and satisfaction survey) occurred at 8 weeks via WeChat or phone appointments, supervised by a postgraduate student during discharge transitions. All data were double entered to ensure accuracy.
Statistical Analysis
Data were analyzed using SPSS version 27.034 and R software (version 4.2.0). Normality of continuous variables was assessed via the Shapiro–Wilk test or visual inspection of histograms. Normally distributed continuous variables were presented as mean ± standard deviation. To account for the intercorrelations between psychological outcomes, a doubly multivariate repeated-measures MANOVA was first conducted using Pillai’s Trace statistic. Pre- to post-intervention changes were also evaluated through mixed-design analysis of variance (ANOVA) to examine time, group, and interaction effects. Simple effects analysis and post-hoc comparisons were performed using the emmeans package with Bonferroni correction. Ordinal variables were compared using the Mann–Whitney U-test. Categorical variables were expressed as frequencies and percentages, with between-group differences analyzed via chi-square tests or Fisher’s exact tests as appropriate. All p-values were two-sided, with statistical significance set at p < 0.05.
Results
General Characteristics of the Study
Following the 8-week intervention period, in the observation group, one participant withdrew due to changes in their medical condition, and two withdrew for personal reasons, resulting in a final inclusion of 55 cases. In the control group, three participants were lost to follow-up due to inability to establish contact, leading to a final inclusion of 55 cases (Figure 1). The detailed comparison of general data between the two groups is presented in Table 2.
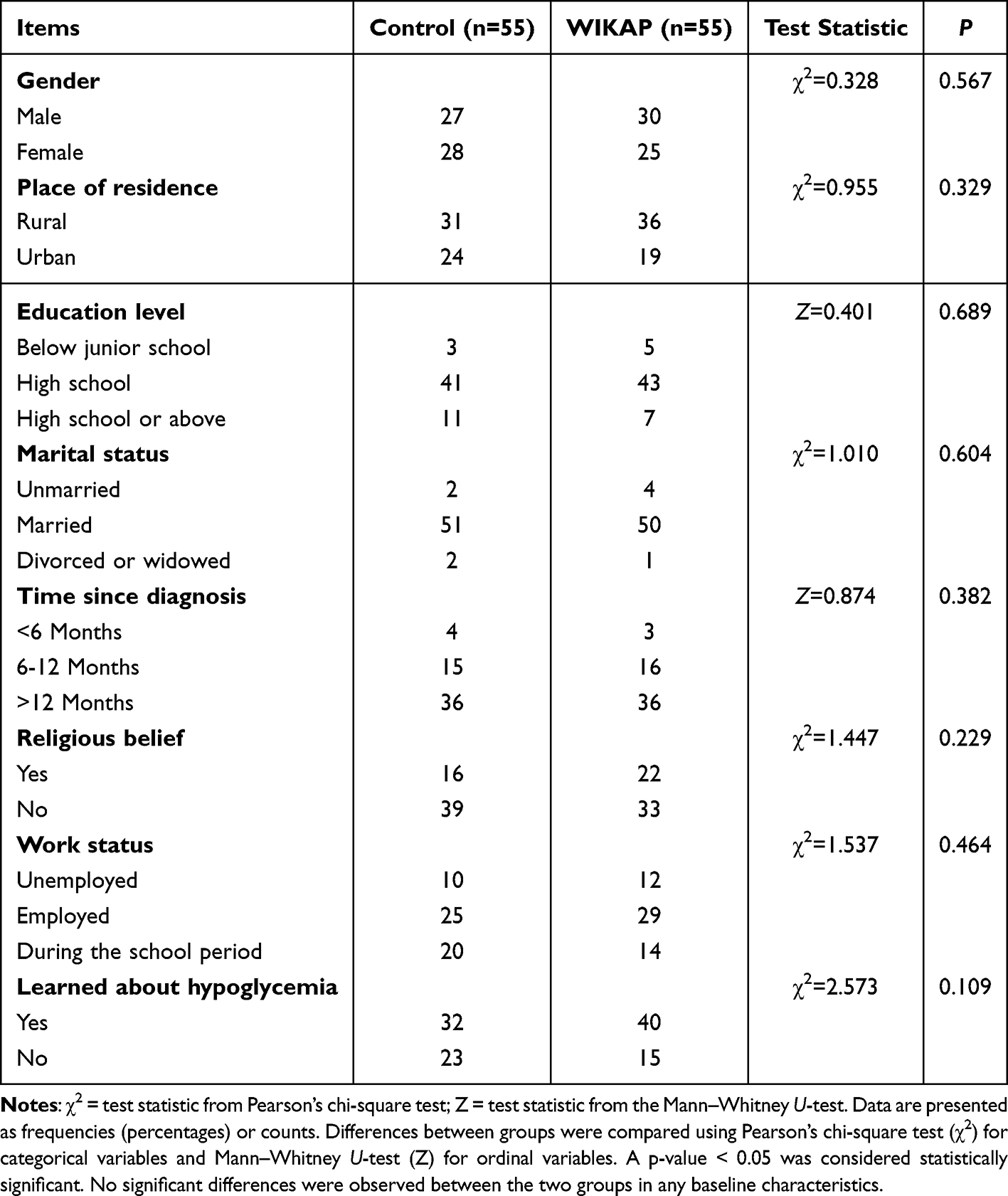 |
Table 2 Comparison of General Data of the Two Groups (N = 110) |
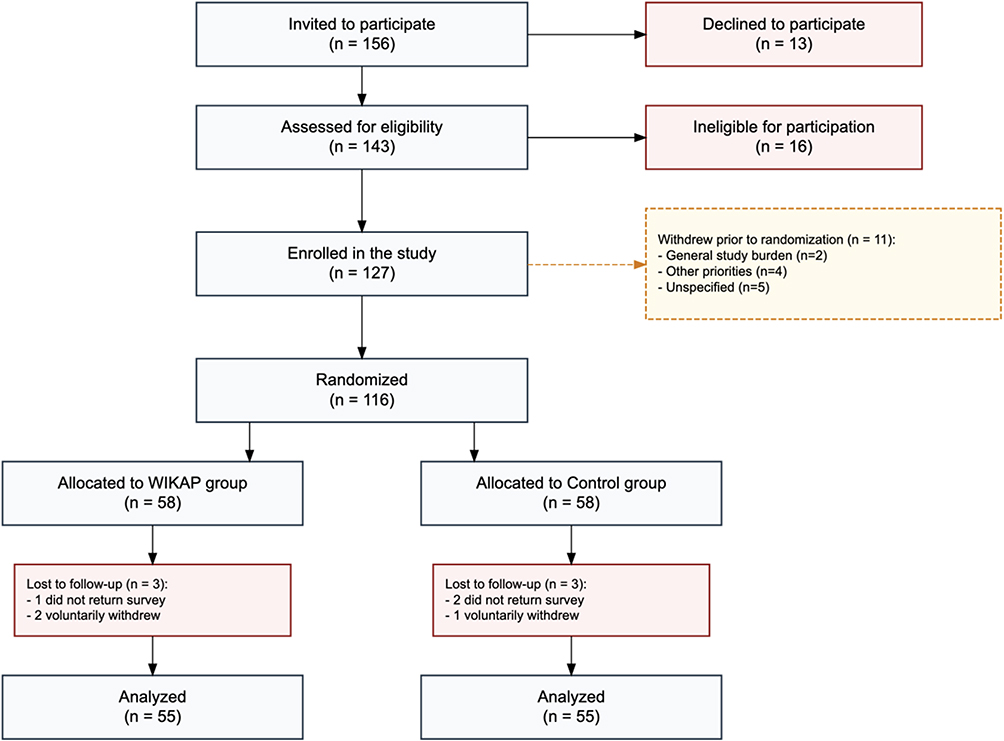 |
Figure 1 Flow diagram of participant recruitment and allocation in the study. A total of 156 individuals were invited to participate. After eligibility screening, 127 participants were enrolled in the study, and 116 were randomized equally into the WIKAP intervention group (n = 58) and the Control group (n = 58). Reasons for declining participation, ineligibility, withdrawal prior to randomization, and loss to follow-up are detailed in the diagram. The final analysis included 55 participants in each group. |
Hypoglycemia Coping Outcomes Between Two Groups
Overall Multivariate Analysis
To account for the inter-correlations between the psychological dimensions (Anxiety, Avoidance, and Confidence), a doubly multivariate repeated-measures MANOVA was conducted. The analysis revealed a highly significant Group x Time interaction effect (Pillai’s Trace = 0.855, F(1, 108) = 635.45, P< 0.001, Partial η2 = 0.635).(Table 3)
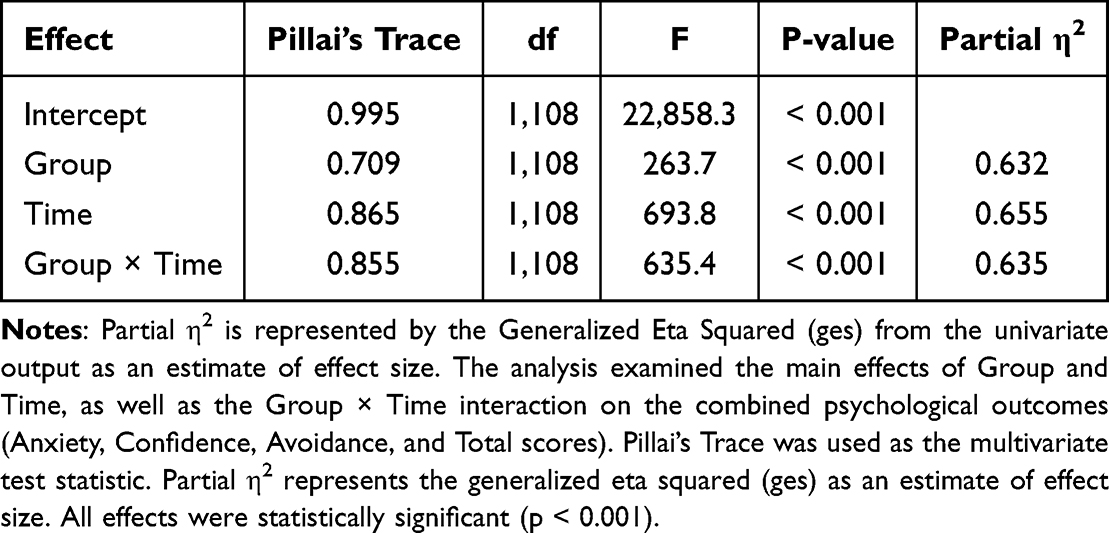 |
Table 3 Doubly Multivariate MANOVA Results for Psychological Outcomes (N = 110) |
Univariate Analysis and Group Comparisons
Following the significant MANOVA, univariate mixed-design ANOVAs were performed for each outcome. As shown in Tables 4 and 5, significant Time × Group interactions were found for all variables (all P < 0.001).(Figure 2)
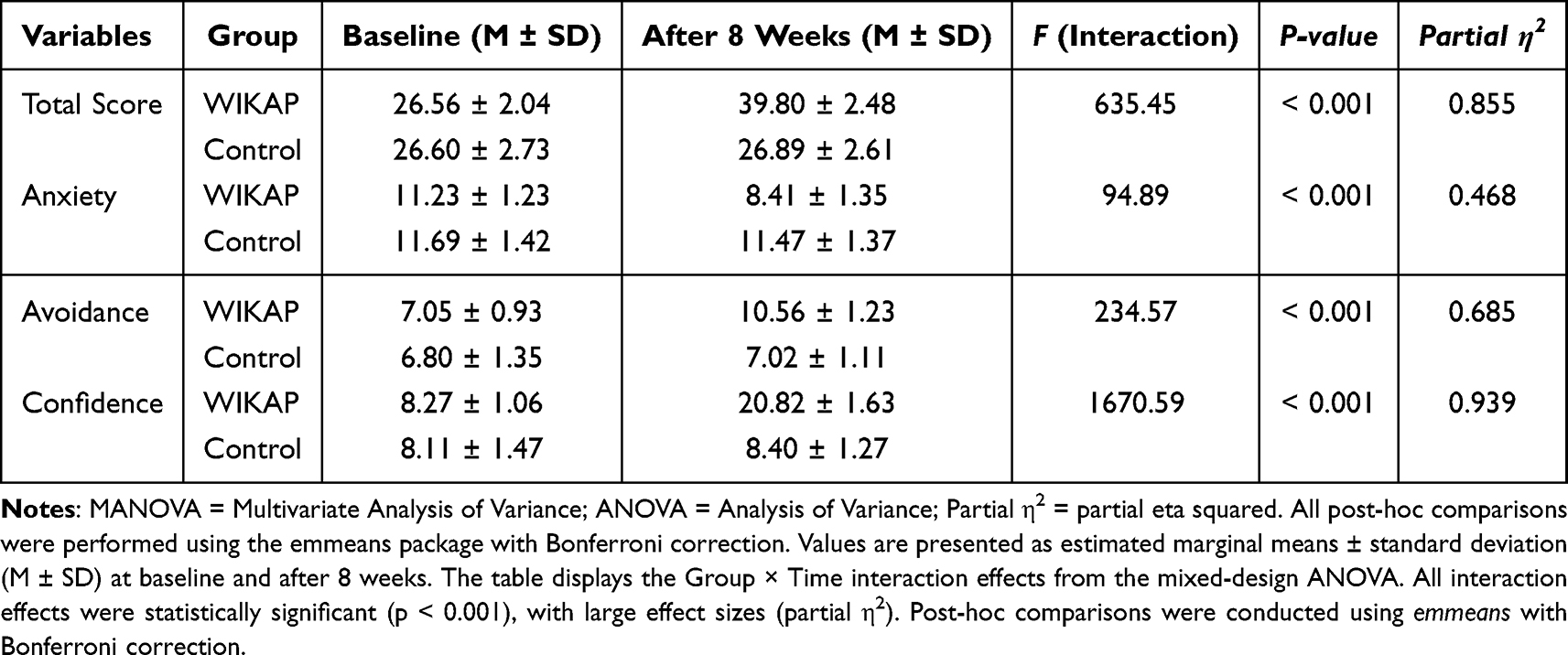 |
Table 4 Psychological Outcomes and Mixed-Design ANOVA Results (N = 110) |
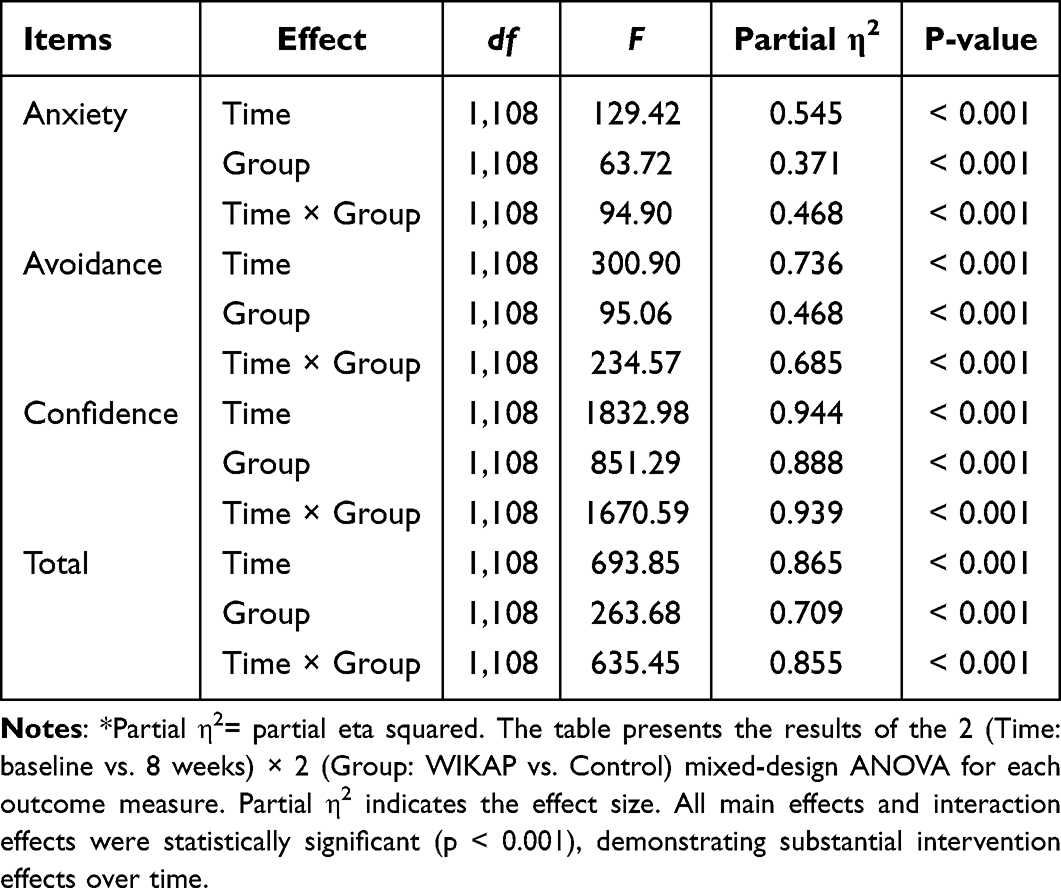 |
Table 5 Mixed-Design ANOVA Results for Study Outcomes (Time × Group) (N = 110) |
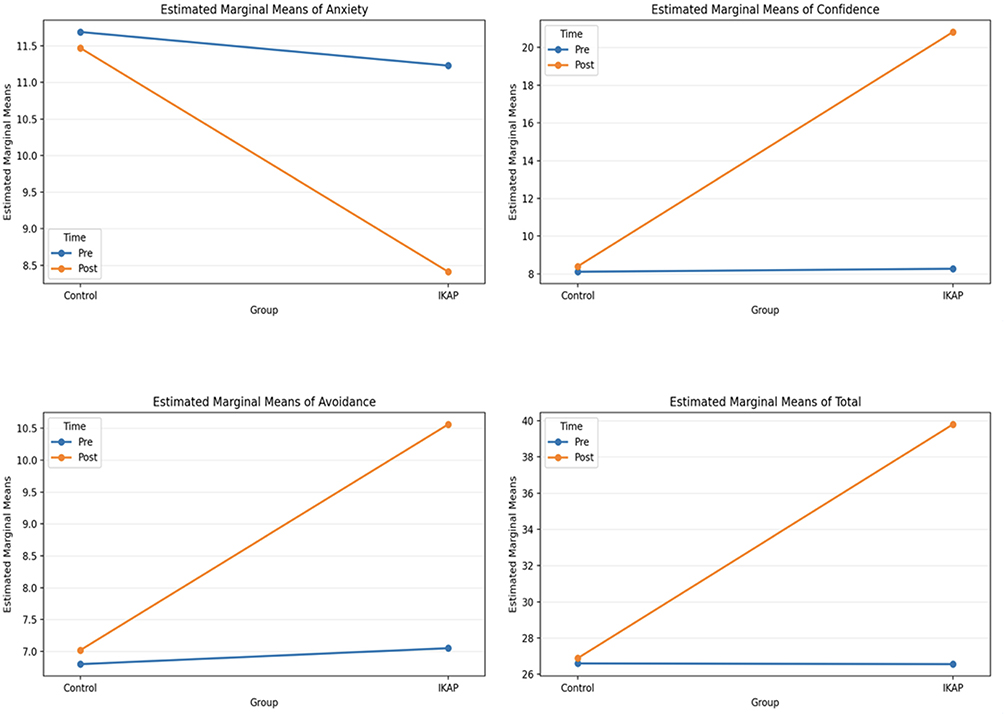 |
Figure 2 Line graph showing changes in confidence in coping strategies. Line graphs showing changes in (A) Anxiety, (B) Confidence in coping strategies, (C) Avoidance, and (D) Total scores from baseline (Pre) to post-intervention (Post) between the Control group and the WIKAP intervention group. Values are estimated marginal means adjusted for the mixed-design ANOVA model. Error bars represent 95% confidence intervals. |
HbA1c Outcomes Between Two Groups
HbA1c decreased from pre to post in the control group and the WIKAP group. Mixed-design ANOVA showed no significant time × group interaction and no significant main effect of group. The main effect of time approached significance. Although the interaction did not reach statistical significance, the clinical trend suggests improved glycemic control in both groups over time. (Tables 6 and 7)
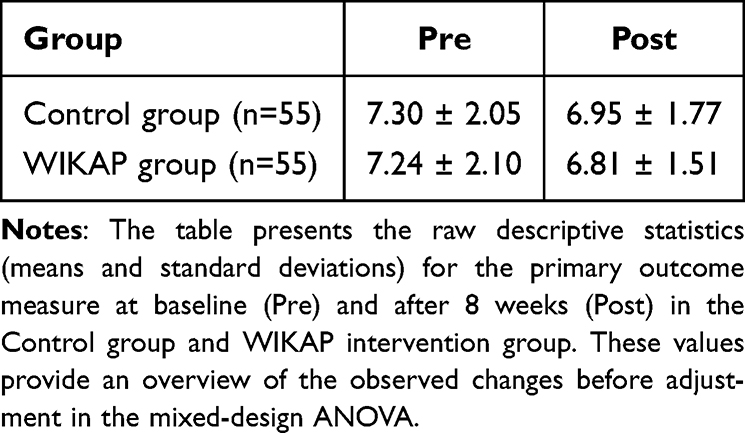 |
Table 6 Means and Standard Deviations of Outcomes by Group and Time (M ± SD) (N = 110) |
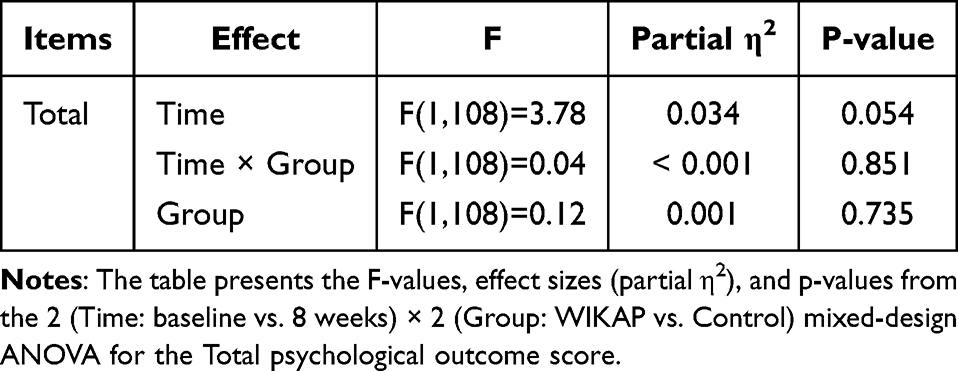 |
Table 7 Mixed-Design ANOVA Results for HbA1c Outcomes (Time × Group) (N = 110) |
Hypoglycemia Incidence Between Two Groups
The incidence of hypoglycemia differed between the control and WIKAP groups (Table 8).
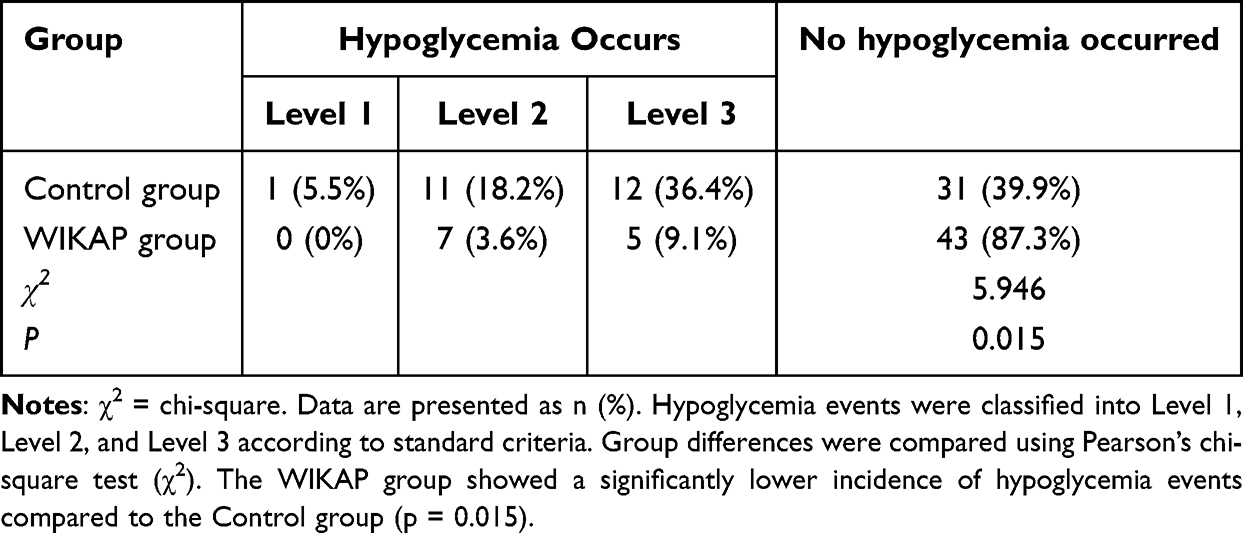 |
Table 8 Comparison of the Incidence of Hypoglycemia Between the Two Groups (N = 110) |
Primary Caregiver Satisfaction
Primary caregiver satisfaction differed significantly between the control and WIKAP groups (Table 9).
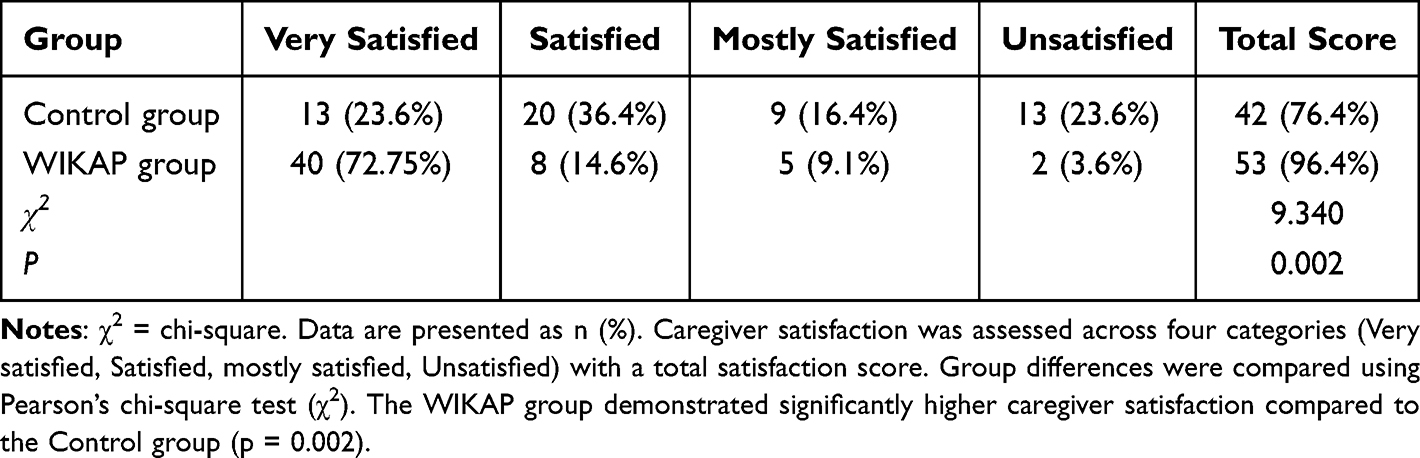 |
Table 9 Comparison of the Nursing Satisfaction of the Main Caregivers of the Two Groups of Patients (N = 110) |
Discussion
WIKAP’ Mechanism of Action
The effectiveness of the WIKAP intervention in this study stems from its foundation in the KAP framework, which integrates information delivery, knowledge acquisition, belief formation, and behavioral practice to convert health-related knowledge into enduring self-care behaviors. Structured education enables patients to heighten disease awareness, build self-management confidence, and enact positive attitudes through practical changes, leading to enhanced glycemic control. This mechanism, rooted in WIKAP theory, promotes tailored knowledge acquisition that strengthens self-care and hypoglycemia management confidence. It facilitates the translation of knowledge into behaviors that resolve rehabilitation issues. Interactive features, including group discussions for experience sharing, boosted coping strategies and alleviated anxiety, as evidenced by a participant’s statement:
I had similar symptoms before. As soon as they occurred, I panicked and didn’t know how to deal with them. Now I have more confidence in handling hypoglycemia and won’t be anxious or scared because of this.
Adolescents with T1DM frequently struggle with disease acceptance, fostering anxiety while juggling academic and daily responsibilities; the WIKAP method counters these emotions via guided support. Limited skill development during brief hospitalizations worsens post-discharge challenges, especially in rural areas with scarce resources. By filling this void, the model reduces anxiety, fortifies disease management, and decreases hypoglycemia incidence. Comparable mechanisms are supported in recent literature. For example, a study of 417 diabetic adolescents in Jordan revealed moderate-to-high knowledge levels but poor attitudes and practices, underscoring the need for targeted education to improve management.35 Additionally, a study on recurrent education for children and adolescents with T1DM demonstrated enhanced hypoglycemia awareness, appropriate self-treatment, and reduced fear through repeated sessions, aligning with KAP principles.36 Furthermore, a review of age-based T1DM challenges in pediatrics highlighted the role of structured DSME in addressing self-management barriers, anxiety, and hypoglycemia risks in adolescents.10
Effectiveness of the WIKAP Intervention in Enhancing Hypoglycemia Coping and Reducing Incidence in Adolescents with T1DM
The study findings indicate that the WIKAP intervention significantly enhanced hypoglycemia coping outcomes in adolescents with T1DM in the observation group relative to controls. To rigorously evaluate these multi-faceted psychological changes, we employed a doubly multivariate MANOVA, which revealed a highly significant interaction effect (p< 0.001). This multivariate approach accounted for the inherent correlations between anxiety, avoidance, and confidence, confirming that the WIKAP model produced a robust, systemic improvement in the overall coping profile rather than mere fragmented changes. Mixed analyses of variance showed notable time effects and time-by-group interactions across dimensions, highlighting the intervention’s distinct influence. Anxiety declined substantially in the WIKAP group but remained consistent in controls, with post-intervention anxiety scores notably lower in the observation group. Comparable reductions in anxiety and fear of hypoglycemia have been reported in recent research, such as a feasibility trial of the cognitive behavioral and technology-aided intervention (FREE), which demonstrated notable fear reductions in young adults with T1D.37 Furthermore, a randomized trial assessing the Bring Blood Glucose Down! Intervention indicated reduced hypoglycemia fear in caregivers of T1DM adolescents.38 The Standards of Care in Diabetes also emphasize preventing diabetes distress in adolescents with T1DM through targeted programs.39
Avoidance behaviors improved markedly in the WIKAP group, with minimal changes in controls. This aligns with educational strategies that promote proactive self-management, as seen in a cross-sectional analysis of pediatric T1DM self-care, which revealed that sufficient parental involvement mitigates severe hypoglycemia risks and supports behavioral adaptations.40 Additionally, a review advocated classroom-based self-care for T1D adolescents to optimize insulin dosing and prevent hypoglycemia through team-led education.41
Confidence and total coping scores exhibited pronounced elevations in the WIKAP group, with post-intervention confidence scores notably higher in the observation group. Similar enhancements in self-efficacy and coping are supported by a prospective study on recurrent education for T1DM youth, which showed improved hypoglycemia awareness, appropriate self-treatment, and reduced fear via repeated sessions.36 The Children and Adolescents Standards of Care in Diabetes highlight psychological interventions for adherence, metabolic control, and coping with stress in this population.42
The intervention also led to decreased hypoglycemia incidence attributable to enhanced knowledge and behavioral adaptations. This outcome is consistent with findings from a study using structural equation modeling, which linked better knowledge and attitudes to improved dietary and activity practices in diabetic patients.43 A randomized trial on educational impacts for type 2 diabetes nutritional adherence showed gains in knowledge, attitudes, practices, and metabolic markers, including reduced glucose levels.44,45 Another study on diabetic weight management identified moderate knowledge levels and positive knowledge-attitude-practice correlations, emphasizing targeted education for self-management.46
The WIKAP Intervention Model’s Impact on Glycemic Control, Hypoglycemia Incidence, and Caregiver Satisfaction in Adolescents with T1DM
HbA1c levels decreased modestly from pre- to post-intervention in both the control group and the WIKAP group, with no significant time-by-group interaction or main effect of group observed in the mixed-design ANOVA. The main effect of time approached statistical significance, suggesting a general trend toward improvement irrespective of the intervention. This finding aligns with a Meta-analysis indicating that educational and psychoeducational self-management interventions yield only small short-term reductions in HbA1c among children and adolescents with type 1 diabetes, with no sustained effects at longer follow-ups and high heterogeneity across studies.47 However, it contrasts with a prospective interventional study demonstrating that tailored diabetes education significantly lowered HbA1c and enhanced glycemic control in pediatric patients transitioning to continuous subcutaneous insulin infusion, highlighting the potential variability in intervention efficacy based on delivery methods and patient contexts.48
The incidence of hypoglycemia was significantly lower in the WIKAP group compared to the control group, as evidenced by chi-square analysis, with fewer occurrences across all severity levels in the intervention participants. This outcome supports the role of structured educational models in mitigating hypoglycemic events through improved self-management. A study on recurrent education for children and adolescents with T1DM reported significant reductions in hypoglycemia duration and incidence, alongside enhanced awareness and appropriate self-treatment, following targeted sessions on monitoring and prevention.36 Similarly, a Meta-analysis of non-pharmacological interventions, including education, noted improvements in overall glycemic control that indirectly contribute to reduced hypoglycemia risks, although direct effects on incidence were not isolated in the analysis.49
Primary caregiver satisfaction was significantly higher in the WIKAP group than in the control group post-intervention, as confirmed by chi-square comparison, reflecting enhanced engagement and support through personalized health education inclusive of caregivers. This result underscores the value of family-oriented approaches in fostering positive caregiving experiences. A mixed-methods feasibility study evaluating a digital caregiving platform for families of children with T1DM found significant improvements in caregiver mood, well-being, and satisfaction, with reductions in depression, anxiety, and stress over a three-month period.50 Additionally, a Meta-analysis of psychological interventions for families of children with T1DM demonstrated reductions in caregiver psychological distress post-intervention, which correlates with increased satisfaction and better family functioning in diabetes management.51
Our study has several limitations. First, the prospective, quasi-experimental design and purposive sampling were adopted to minimize treatment contamination in a single-center clinical setting; however, these approaches may have introduced selection and temporal biases. We addressed these concerns through independent screening and rigorous statistical adjustments. Specifically, we employed ANCOVA to control for baseline imbalances and used MANOVA to account for the inter-correlations between psychological dimensions, thereby providing a more integrated and robust estimation of the intervention’s effects. Despite these constraints, this study provides a robust pragmatic foundation for the model’s efficacy. Future multicenter cluster-randomized trials are warranted to further validate these results across broader populations.
Conclusion
This study demonstrates that the WIKAP intervention effectively enhances hypoglycemia coping confidence and reduces anxiety in adolescents with T1DM, while also decreasing hypoglycemia incidence and improving primary caregiver satisfaction, with statistically significant differences compared to controls. Although HbA1c levels showed a modest decline across groups without intervention-specific effects, these outcomes underscore the model’s utility in fostering self-management and family support, grounded in the KAP framework. Despite these advancements, domestic research on T1DM hypoglycemia coping confidence remains limited. Study constraints include a single-center sample potentially introducing selection bias, reliance solely on the HABS scale’s anxiety dimension without dedicated anxiety assessments, exclusive use of HABS for coping evaluation, and a short 8-week duration lacking long-term psychosocial follow-up. Future investigations should employ multi-center designs with larger cohorts to validate findings, incorporate supplementary tools for anxiety and coping measurement, and conduct extended randomized controlled trials to assess sustained impacts.
Data Sharing Statement
The authors intend to share de-identified individual participant data, including demographic information, primary and secondary outcomes, and adverse events. The study protocol, statistical analysis plan, and informed consent form will also be available. Data may be obtained upon reasonable request to the corresponding author ([email protected]). Data will be available from 6 months after publication and for a period of 5 years thereafter.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Gong B, Yang W, Xing Y, et al. Global, regional, and national burden of type 1 diabetes in adolescents and young adults. Pediatr Res. 2025;97(2):568–14. doi:10.1038/s41390-024-03107-5
2. Gregory GA, Robinson TIG, Linklater SE, et al. Global incidence, prevalence, and mortality of type 1 diabetes in 2021 with projection to 2040: a modelling study. Lancet Diabetes Endocrinol. 2022;10(10):741–760. doi:10.1016/s2213-8587(22)00218-2
3. Jingxia Y, Li Y, Danlan P, et al. Interpretation of the “Guidelines for the prevention and treatment of diabetes in China (2024 Edition)”. J Chongqing Med Univ. 2025;50(05):557–564.
4. Jin F, Xie L, Wang G, et al. Epidemiology and temporal trends of childhood type 1 diabetes in China: an analysis of the GBD 2021. Front Endocrinol. 2025;16(1638187). doi:10.3389/fendo.2025.1638187
5. Li Y, Qian K, Wu D, et al. Incidence of childhood type 1 diabetes in Beijing during 2011–2020 and predicted incidence for 2025–2035: a Multicenter, Hospitalization-Based Study. Diabetes Therapy. 2023;14(3):519–529. doi:10.1007/s13300-023-01367-8
6. Chen S, Lu J, Peng D, et al. Incidence rate and risk factors for hypoglycemia among individuals with type 1 diabetes or type 2 diabetes in China receiving insulin treatment. Diabetes Res Clin Pract. 2023;206(110987). doi:10.1016/j.diabres.2023.110987
7. Moser O, Rafferty J, Eckstein ML, et al. Impact of severe hypoglycaemia requiring hospitalization on mortality in people with type 1 diabetes: a national retrospective observational cohort study. Diabetes Obes Metab. 2023;25(8):2243–2254. doi:10.1111/dom.15102
8. Cryer PE. Severe hypoglycemia predicts mortality in diabetes. Diabetes Care. 2012;35(9):1814–1816. doi:10.2337/dc12-0749
9. Urakami T. Severe hypoglycemia: is it still a threat for children and adolescents with type 1 diabetes? Front Endocrinol. 2020;11(609). doi:10.3389/fendo.2020.00609
10. Lan YY, Kovinthapillai R, Kędzia A, et al. Age-based challenges to type 1 diabetes management in the pediatric population. Front Pediatr. 2024;12(1434276). doi:10.3389/fped.2024.1434276
11. Borus JS, Laffel L. Adherence challenges in the management of type 1 diabetes in adolescents: prevention and intervention. Curr Opin Pediatr. 2010;22(4):405–411. doi:10.1097/MOP.0b013e32833a46a7
12. Azar S, Maroun Abou Jaoude N, Kędzia A, et al. Barriers to type 1 diabetes adherence in adolescents. J Clin Med. 2024;13(19):5669.
13. Menon S, Desalvo D, Erraguntla M, et al. 614-P: Fear of hypoglycemia, hypoglycemia confidence, and time in range in adolescents and young adults with type 1 diabetes (T1D). Diabetes. 2022;71(Supplement_1). doi:10.2337/db22-614-P
14. Zarei F, Dehghani A, Ratansiri A, et al. ChecKAP: a checklist for reporting a knowledge, attitude, and practice (KAP) study. Asian Pac J Cancer Prev. 2024;25(7):2573–2577. doi:10.31557/apjcp.2024.25.7.2573
15. Kang J, Zhu X, Kan Y, et al. Application of the knowledge, attitude, and practice model combined with motivational interviewing for health education in female patients with systemic lupus erythematosus. Medicine. 2023;102(12):e33338. doi:10.1097/md.0000000000033338
16. Sotoodeh Jahromi A, Jokar M, Sharifi N, et al. Systematic review and meta-analysis of knowledge, attitudes, and practices regarding COVID-19 among chronic disease patients: a global perspective. Health Sci Rep. 2024;7(1):e1793. doi:10.1002/hsr2.1793
17. Mahmood MM, Rehman J, Arif B, et al. Knowledge, attitudes and practices of patients with chronic illnesses during the COVID-19 pandemic: a cross-sectional survey from Pakistan. Chronic Illn. 2022;18(3):608–619. doi:10.1177/17423953211023961
18. Lv S, Du Y, Sun Z, et al. IKAP model-based nursing interventions on elderly patients with chronic obstructive pulmonary disease and its impact on self-management ability and quality of life. Afr Health Sci. 2025;25(3):145–153. doi:10.4314/ahs.v25i3.19
19. Marker AM, Monzon AD, Nelson EL, et al. An Intervention to reduce hypoglycemia fear in parents of young kids with type 1 diabetes through video-based telemedicine (REDCHiP): trial design, feasibility, and acceptability. Diabetes Technol Ther. 2020;22(1):25–33. doi:10.1089/dia.2019.0244
20. Rondags SM, de Wit M, Twisk JW, et al. Effectiveness of hypoaware, a brief partly web-based psychoeducational intervention for adults with type 1 and insulin-treated type 2 diabetes and problematic hypoglycemia: a cluster randomized controlled trial. Diabetes Care. 2016;39(12):2190–2196. doi:10.2337/dc16-1614
21. Lin YK, Aikens JE, de Zoysa N, et al. An mHealth text messaging program providing symptom detection training and psychoeducation to improve hypoglycemia self-management: intervention development study. JMIR Form Res. 2023;7:e50374. doi:10.2196/50374
22. Bofill Roig M, Burgwinkel C, Garczarek U, et al. On the use of non-concurrent controls in platform trials: a scoping review. Trials. 2023;24(1):408. doi:10.1186/s13063-023-07398-7
23. Newton KT, Ashley A. Pilot study of a web-based intervention for adolescents with type 1 diabetes. J Telemed Telecare. 2013;19(8):443–449. doi:10.1177/1357633x13512069
24. Holtz B, Mitchell KM, Holmstrom AJ, et al. An mHealth-Based intervention for adolescents with type 1 diabetes and their parents: pilot feasibility and efficacy single-arm study. JMIR Mhealth Uhealth. 2021;9(9):e23916. doi:10.2196/23916
25. Titoria R, Amed S, Tang TS. Peer support interventions on digital platforms for children with type 1 diabetes and their caregivers. Diabetes Spectr. 2022;35(1):26–32. doi:10.2337/ds21-0081
26. Zhu Y, Qian J, Ma W, et al. Evaluating the health promotion effects of the IKAP care model in older adults with periodontitis. Medicine. 2025;104(36):e44034. doi:10.1097/md.0000000000044034
27. Nan W, Zhuo H, Yongni J, et al. A retrospective study examined the impact of the IKAP nursing model on the self-efficacy and quality of life of colorectal cancer patients with permanent stomas. SAGE Open Nurs. 2025;11(23779608251397442). doi:10.1177/23779608251397442
28. Polonsky WH, Fisher L, Hessler D, et al. Identifying the worries and concerns about hypoglycemia in adults with type 2 diabetes. J Diabet Complicat. 2015;29(8):1171–1176. doi:10.1016/j.jdiacomp.2015.08.002
29. Polonsky WH, Fisher L, Hessler D, et al. Worries and concerns about hypoglycemia in adults with type 1 diabetes: an examination of the reliability and validity of the Hypoglycemic Attitudes and Behavior Scale (HABS). J Diabet Complicat. 2020;34(7):107606. doi:10.1016/j.jdiacomp.2020.107606
30. Cailing S, Daling Z, Min H, et al. Chinese localization and reliability and validity testing of the hypoglycemia attitudes and behaviors scale. Nursing Research. 2021;35(15):2666–2669.
31. Committee ADAPP. 14. Children and adolescents: standards of care in diabetes—2025. Diabetes Care. 2024;48(Supplement_1):S283–S305. doi:10.2337/dc25-S014
32. Redondo MJ, Libman I, Maahs DM, et al. The evolution of hemoglobin A(1c) targets for youth with type 1 diabetes: rationale and supporting evidence. Diabetes Care. 2021;44(2):301–312. doi:10.2337/dc20-1978
33. Committee ADAPP. 6. Glycemic goals and hypoglycemia: standards of care in diabetes—2024. Diabetes Care. 2023;47(Supplement_1):S111–S125. doi:10.2337/dc24-S006
34. IBM Corp. IBM SPSS Statistics for Windows. Armonk, NY, USA: IBM Corp; 2020.
35. Elsahoryi NA, Odeh MM, Alsous M, et al. Adolescents with diabetes, exploring knowledge, attitude and practice: a Cross-Sectional Analytical Study. Pharmacy Pract. 2024;22(4):1–12.
36. Güneş Kaya D, Bayramoğlu E, Turan H, et al. Recurrent education: a promising strategy for enhancing diabetes management and reducing hypoglycemia in children with type 1 diabetes. BMC Endocr Disord. 2025;25(1):109. doi:10.1186/s12902-025-01917-0
37. Martyn-Nemeth P, Duffecy J, Quinn L, et al. FREE: a randomized controlled feasibility trial of a cognitive behavioral therapy and technology-assisted intervention to reduce fear of hypoglycemia in young adults with type 1 diabetes. J Psychosom Res. 2024;181(111679). doi:10.1016/j.jpsychores.2024.111679
38. O’Donnell HK, Vigers T, Johnson SB, et al. Bring blood glucose down! An intervention to reduce fear of hypoglycemia in caregivers of adolescents with type 1 diabetes: study design and participant characteristics. Contemp Clin Trials. 2022;118(106792). doi:10.1016/j.cct.2022.106792
39. ElSayed NA, Aleppo G, Aroda VR, et al. 14. Children and adolescents: standards of care in diabetes—2023. Diabetes Care. 2022;46(Supplement_1):S230–S253. doi:10.2337/dc23-S014
40. Smudja M, Milenković T, Minaković I, et al. Self-care activities in pediatric patients with type 1 diabetes mellitus. PLoS One. 2024;19(3):e0300055. doi:10.1371/journal.pone.0300055
41. Virmani A. Classroom as the site for type 1 diabetes self-care activities. Indian Pediatr. 2024;61(5):486–488.
42. American Diabetes Association Professional Practice Committee for Diabetes. 14. Children and adolescents: standards of care in diabetes—2026. Diabetes Care. 2025;49(Supplement_1):S297–S320. doi:10.2337/dc26-S014
43. Zhu W, Liang D, Petersen JD, et al. Relationship between diabetic knowledge, attitudes and practices among patients with diabetes in China: a structural equation model. BMJ Open. 2023;13(11):e076464. doi:10.1136/bmjopen-2023-076464
44. Gortzi O, Dimopoulou M, Androutsos O, et al. Effectiveness of a nutrition education program for patients with type 2 diabetes mellitus. Appl Sci. 2024;14(5):2114.
45. Dehghan T, Mohsenpour MA, Karimi M, et al. Educational intervention based on the extended parallel process model improves adherence to diabetic diet and glycaemic control indices: a randomised, double-blind, controlled, factorial field trial. Br J Nutr. 2024;131(12):2068–2079. doi:10.1017/s0007114524000497
46. Li X, Shi Y, Wei D, et al. Knowledge, attitude, and practice toward weight management among diabetic patients in Qidong City, Jiangsu Province. BMC Public Health. 2024;24(1):922. doi:10.1186/s12889-024-18392-2
47. Cockcroft EJ, Clarke R, Dias RP, et al. Effectiveness of educational and psychoeducational self-management interventions in children and adolescents with type 1 diabetes: a systematic review and meta-analysis. Pediatric Diabet. 2024;2024(1):2921845.
48. Hassan M, ElHelaly M, Badawi N, et al. Impact of tailored diabetes education on adherence and glycemic control in children and adolescents on continuous subcutaneous insulin infusion, prospective interventional study in a tertiary center. BMC Pediatr. 2025;25(1):670. doi:10.1186/s12887-025-06018-4
49. Lee D, Lee H, Shin Y, et al. Effectiveness of non-pharmacological interventions for adolescents with type 1 diabetes in the last five years: a systematic review and meta-analysis. Asian Nurs Res. 2024;18(1):51–59. doi:10.1016/j.anr.2024.01.008
50. de Arriba Muñoz A, Civitani Monzon E, Ferrer MP, et al. Empowering caregiver well-being with the adhera caring digital program for family caregivers of children living with type 1 diabetes: mixed methods feasibility study. JMIR Pediatr Parent. 2025;8:e66914. doi:10.2196/66914
51. Wakelin KE, Read RK, Williams AY, et al. The effectiveness of psychological interventions for families of children with type 1 diabetes on caregiver and child functioning: a systematic review and meta-analysis. J Diabetes. 2025;17(6):e70112. doi:10.1111/1753-0407.70112
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.