Back to Journals » International Journal of Women's Health » Volume 18
Efficacy of Normobaric High-Flow Oxygen Therapy Combined with Low Molecular Weight Heparin in the Management of Fetal Growth Restriction: A Prospective Cohort Study
Authors He M, Zhao K ![]() , Wei Q, He M, Yuan C, Jian W, Huang J
, Wei Q, He M, Yuan C, Jian W, Huang J
Received 15 October 2025
Accepted for publication 4 March 2026
Published 15 April 2026 Volume 2026:18 574440
DOI https://doi.org/10.2147/IJWH.S574440
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
MeiRong He,* KaiSun Zhao,* QingFang Wei, MeiPing He, ChunLan Yuan, WenQian Jian, JianChun Huang
Department of Obstetrics, The Third Affiliated Hospital of Guangxi Medical University, The Second Nanning People’s Hospital, Nanning, Guangxi Zhuang Autonomous Region, People’s Republic of China
*These authors contributed equally to this work
Correspondence: JianChun Huang, Department of Obstetrics, The Third Affiliated Hospital of Guangxi Medical University, The Second Nanning People’s Hospital, No. 13, Dancun Road, Jiangnan District, Nanning, Guangxi Zhuang Autonomous Region, 530031, People’s Republic of China, Tel +860771-4808241, Email [email protected]
Objective: This study investigated the clinical efficacy of adding normobaric high-flow oxygen therapy (NHFOT) to low molecular weight heparin (LMWH) and standard supportive care for the management of the present FGR cohort, idiopathic fetal growth restriction (FGR).
Methods: This prospective cohort study enrolled 117 women with idiopathic FGR, representing a spectrum of gestational ages at diagnosis, at a single center between July 2022 and June 2025. All participants received standard supportive care including low-flow nasal oxygen (2– 5 L/min, 30– 40% O2) and intravenous nutritional support (vitamin C 4 vials/8 mL in 500 mL 5% dextrose plus 200 mL compound amino acids daily for 7 days). Participants were assigned to three groups based on shared decision-making: Group 1 (n=32) received standard care only; Group 2 (n=37) received standard care plus subcutaneous LMWH (4000 IU daily); Group 3 (n=48) received standard care plus LMWH and NHFOT (8– 10 L/min, 95% O2, 45 min/day).
Results: Compared with Group 1, Group 3 showed a modest but statistically significant prolongation of gestational age at delivery (+2.5 days; 267.5 vs 265.0 days; P=0.002), higher median birth weight (+240 g; 2600 vs 2360 g; P< 0.001), higher FGR cure rate (45.83% vs 18.75%; P=0.042), and lower low birth weight rate (33.33% vs 65.63%; P=0.013). However, no significant differences in FGR cure rate were observed between Group 3 and Group 2 (45.83% vs 32.43%; P=0.213). No significant differences were found in preterm birth rates or umbilical cord blood gas parameters among groups.
Conclusion: Our findings indicate that in a cohort of idiopathic FGR encompassing a range of gestational ages, combining NHFOT with LMWH may improve fetal weight and reduce LBW risk compared to standard care alone. However, no conclusive additional benefit over LMWH alone was observed for the primary cure outcome.
Clinical Trial Number: MR-45-22-008098.
Keywords: fetal growth restriction, low molecular weight heparin, normobaric high-flow oxygen therapy, pregnancy outcome
Introduction
Fetal growth restriction (FGR) refers to a condition in which the fetus fails to achieve its genetically predetermined growth potential due to pathological influences from maternal, fetal, or placental factors. It is typically characterized by an estimated fetal weight or abdominal circumference below the 10th percentile for the corresponding gestational age, as assessed by ultrasound.1–4 As the second leading cause of perinatal mortality,4 the incidence of FGR in China is approximately 8.77%, with a significantly higher prevalence among preterm infants (16.43%) compared to term infants (7.87%).5 The etiology of FGR is multifactorial and not yet fully elucidated; it primarily involves maternal, fetal, placental, and umbilical cord factors. Research indicates that the majority of cases result from impaired placental perfusion, which compromises intrauterine fetal nutrition and oxygen supply, ultimately restricting fetal growth.6 Studies have shown that fetuses with FGR have a 2–3 times higher risk of fetal distress compared to normal fetuses. This increased risk is largely attributable to placental insufficiency, which reduces oxygen and nutrient transfer, thereby predisposing the fetus to hypoxia and acidemia during labor, potentially leading to adverse outcomes such as fetal demise and stillbirth.7 Preterm birth is a major adverse outcome associated with FGR.8 When placental dysfunction causes deterioration of the intrauterine environment, the mother may opt for early delivery to prevent further fetal compromise. However, preterm birth itself introduces additional health risks, including neonatal respiratory distress syndrome, intraventricular hemorrhage, necrotizing enterocolitis, and other severe complications. Long-term consequences encompass metabolic syndrome (obesity, diabetes, insulin resistance), cardiovascular diseases, and neurodevelopmental impairments, which may persist throughout the child’s lifetime.9–14 Given the profound impact of FGR on pregnancy outcomes and the lack of conclusive evidence supporting effective interventions such as low-flow nasal oxygen therapy, enhanced nutritional supplementation, or multivitamins, it is imperative to explore more efficacious therapeutic approaches. Some literature suggests that interventions aimed at improving placental microcirculation or modulating inflammatory responses may indirectly influence FGR outcomes.15 This study focuses on the clinical efficacy of NHFOT combined with low-molecular-weight heparin in the management of fetal growth restriction, aiming to provide novel insights and strategies for clinical practice.
Patients and Methods
General Information
This study was conducted in accordance with the Declaration of Helsinki and was approved by the the Ethics Committee of the Second Nanning People’s Hospital (Approval No.: Y2022021). The study was registered with the Chinese National Medical Research Registration Information System (Registration No.: MR-45-22-008098). As this was a non-randomized prospective cohort study with treatment assignments determined through patient-clinician shared decision-making prior to formal analysis, written informed consent was obtained from all participants. This prospective, single-cent er cohort study enrolled 117 pregnant women diagnosed with FGR admitted to our hospital between July 2022 and June 2025. Participants were allocated into three groups based on their treatment preferences using a non-randomized controlled design:
Group 1 (n=32): Received low-flow nasal oxygen therapy combined with intravenous nutritional support.
Group 2 (n=37): Received the interventions of Group 1 plus subcutaneous low molecular weight heparin (LMWH) at 4000 IU.
Group 3 (n=48): Received the interventions of Group 2 plus NHFOT.
Given the exploratory nature of this novel combined therapy (NHFOT plus LMWH), preliminary data for sample size calculation were not available We adopted a total population sampling approach, consecutively enrolling all eligible cases during the study period to maximize clinical relevance. The sample size of 117 is within the range of previous FGR studies, which reported sizes from 30 to 164 cases.16–19 Treatment strategies were determined through shared decision-making between clinicians and patients, with all participants providing written informed consent.
Inclusion Criteria
- Gestational age confirmed by prenatal ultrasound;
- Singleton viable pregnancy;
- Complete prenatal records with regular check-ups;
- Gestational age between 28 and 37 weeks;
- Idiopathic FGR without other comorbidities;
- Voluntary participation with signed informed consent.
Exclusion Criteria
- Known allergy to study medications;
- Severe cardiac, hepatic, or renal dysfunction;
- Fetal chromosomal abnormalities or malformations;
- Cognitive impairment or psychiatric disorders;
- Coexisting conditions such as diabetes mellitus or hypertensive disorders of pregnancy.
Diagnostic Criteria
- Preterm birth: Delivery occurring between 28 and 36+6 weeks.20,21
- Low birth weight: Neonates born with a weight less than 2500 g.20,21
- FGR was classified as the present FGR cohort based on gestational age at diagnosis (between 32 and 37 weeks) in this study, consistent with common clinical classifications in the literature.22 The severity was further characterized by the proportion of cases with an estimated fetal weight below the 3rd percentile.
Cohort Characteristics: All FGR cases were diagnosed between 28 and 37 weeks of gestation. Based on the standard 32-week cutoff, the cohort included 52 cases of early-onset FGR (diagnosis <32 weeks) and 65 cases of the present FGR cohort FGR (diagnosis ≥32 weeks).
Research Methods and Observational Metrics
Treatment Protocols
After admission, all pregnant women in the three groups received close monitoring, including regular fetal heart rate surveillance and ultrasound assessments. They were positioned in the left lateral decubitus position to optimize uteroplacental perfusion. Clinical management was tailored to prevent intrauterine fetal death, which included prompt evaluation and, if indicated, expedited delivery in cases of non-reassuring fetal status.
Intervention Group 1 (Group 1): Received low-flow nasal oxygen therapy combined with intravenous nutritional support. Low-flow oxygen was delivered via nasal cannula at 2–5 L/min with 30–40% O2 concentration, consistent with conventional management for maternal hypoxia. Oxygen was administered twice daily for 30 minutes per session for 7 days. Intravenous administration included vitamin C (4 vials, 8 mL, Manufacturer: Ruiyang Pharmaceutical Co., Ltd. Approval Number: H41023393) mixed into 500 mL of 5% glucose solution (Manufacturer: Anhui Shuanghe Pharmaceutical Co., Ltd. Approval Number: National Medicine Approval Number H51020634)., and 200 mL of compound amino acids (Manufacturer: Fuzhou Haiwangfu Pharmaceutical Co., Ltd. Approval Number: National Medicine Approval Number H20083703)., administered via infusion once daily for 7 days. This nutritional support regimen, providing antioxidants and basic nutritional substrates, was adopted as part of our institutional standard supportive care for FGR, based on general principles of supporting maternal and fetal nutrition in the context of presumed placental insufficiency.
Intervention Group 2 (Group 2): Received all treatments of Group 1 plus subcutaneous injection of LMWH at a dose of 4000 IU (0.4 mL, Manufacturer: Aventis Pharmaceuticals Co., Ltd. (France), Approval Number: National Drug Approval Number H20030429).
Intervention Group 3 (Group 3): Received all treatments of Group 2 plus NHFOT. Oxygen was delivered via a sealed high-pressure oxygen mask (Manufacturer: Changzhou Wujin Xinhua Medical Devices Co., Ltd. Model: XQ-02) outside the hyperbaric oxygen chamber, with a high-concentration, high-flow oxygen supply at 8–10 L/min, 95% oxygen concentration, for 45 minutes per session, once daily.
Observation Indicators
The following parameters were observed and compared among the three groups:
Maternal age, parity, pre-pregnancy BMI, pre-delivery weight, gestational age at diagnosis; Ultrasound indices: resistance index (RI), pulsatility index (PI), and systolic/diastolic (S/D) ratio; Fetal estimated weight below the 3rd percentile (3%) threshold, a threshold often indicative of more severe growth restriction; Gestational age at delivery post-intervention; Neonatal birth weight; FGR cure rate; Incidence of Low Birth Weight (LBW); Incidence of Preterm Birth (PTB); Umbilical artery blood gas analysis of the neonates.
Due to measurement timing variability, post-treatment umbilical blood flow parameters were not analyzed.
Safety Monitoring
Patients were monitored for any adverse effects related to the treatments. Specifically, for LMWH, signs of bleeding or injection site reactions were noted. For oxygen therapies, patient tolerance and any signs of discomfort were recorded.
Statistical Analysis
Data were analyzed using SPSS version 29.0. Categorical variables were expressed as percentages (%) and compared using the Chi-square (χ2) test; when expected counts were less than 5, Fisher’s exact test was applied. A p-value < 0.05 was considered statistically significant. For continuous variables with normal or near-normal distribution, data were presented as mean ± standard deviation ( ), and comparisons among multiple groups were performed using one-way ANOVA. Non-normally distributed data were expressed as medians with interquartile ranges, and comparisons among groups were conducted using the Kruskal–Wallis H-test. Pairwise comparisons were adjusted with the Bonferroni correction, with p < 0.05 indicating statistical significance.
), and comparisons among multiple groups were performed using one-way ANOVA. Non-normally distributed data were expressed as medians with interquartile ranges, and comparisons among groups were conducted using the Kruskal–Wallis H-test. Pairwise comparisons were adjusted with the Bonferroni correction, with p < 0.05 indicating statistical significance.
Results
Comparison of Baseline Characteristics
Baseline characteristics among the three groups showed no statistically significant differences in age, gravidity, parity, pre-pregnancy BMI, or pre-delivery weight (P > 0.05), Table 1.
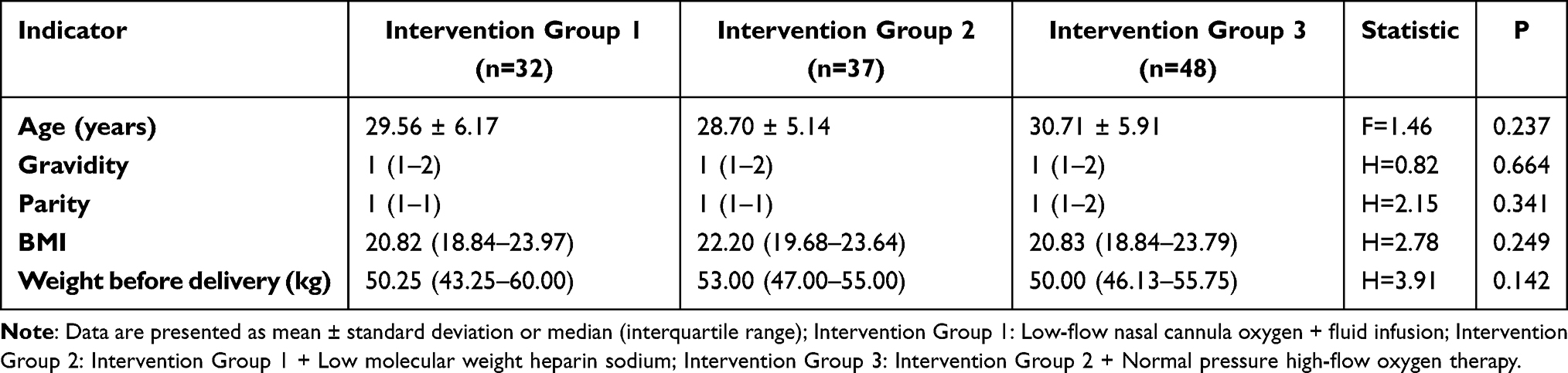 |
Table 1 Comparison of Baseline Characteristics of Pregnant Women in Three Groups |
Comparison of Indicators at Diagnosis of FGR
The three groups demonstrated comparable baseline fetal profiles, with no significant differences in umbilical artery Doppler parameters (RI, PI, S/D), gestational age at FGR diagnosis, or proportion of estimated fetal weight below the 3rd percentile (P > 0.05), Table 2.
 |
Table 2 Comparison of Indicators at Diagnosis of FGR in Three Groups |
Comparison of Neonatal Outcomes
Following the interventions, gestational age at delivery differed significantly among the three groups: Group 3 (267.5 days) was significantly longer than Group 1 (265.0 days) and Group 2 (264.0 days) (overall P = 0.002). There was no statistically significant difference between Group 1 and Group 2 (P > 0.05). Birth weight: Group 3 (2600 g) > Group 2 (2442 g) > Group 1 (2360 g), with significant differences among groups (overall P < 0.001). The weight in Group 3 was significantly higher than in Group 1, with a statistically significant difference between these two groups (P < 0.05). There was no significant difference between Group 2 and the other two groups (P > 0.05). Cure rate: The cure rate was significantly higher in Group 3 than in Group 1 (45.83% vs 18.75%; OR 3.67, 95% CI 1.21–11.15; P = 0.042). The cure rate in Group 2 (32.43%) did not differ significantly from either of the other two groups. Incidence of LBW: The incidence of low birth weight was significantly lower in Group 3 than in Group 1 (33.33% vs 65.63%; OR 0.26, 95% CI 0.09–0.74; P = 0.013). There was no significant difference between Group 2 and the other two groups (P > 0.05). Rates of preterm birth and umbilical artery blood gases (PH, Lac) showed no statistically significant differences among the three groups (P > 0.05), Table 3.
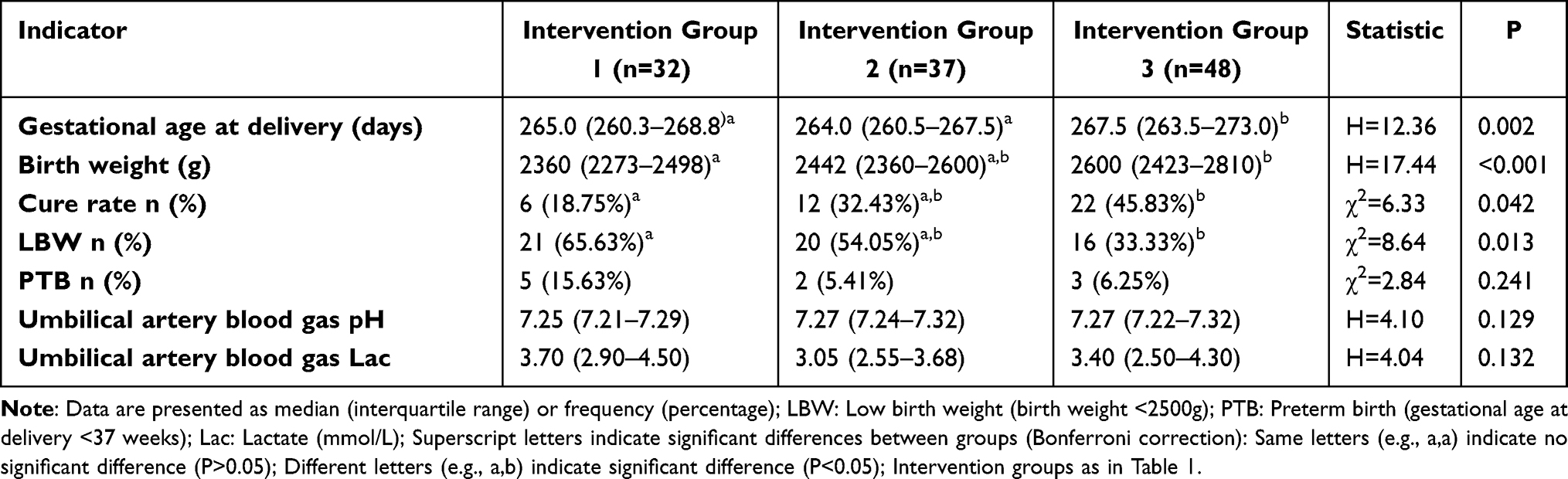 |
Table 3 Comparison of Neonatal Outcomes in Three Groups |
Discussion
Fetal Growth Restriction as a Common Obstetric Complication
FGR is a prevalent obstetric complication, with a global incidence of approximately 5% to 10%,22 posing significant clinical challenges. Current management strategies primarily aim to improve placental blood flow and enhance fetal monitoring. However, traditional conservative treatments often show limited efficacy. Although combined therapies, such as dextran and Salvia miltiorrhiza (a traditional Chinese medicinal herb used for its proposed circulatory benefits) injections, have shown modest benefits, their overall effectiveness remains insufficient.
Emerging Therapeutic Approaches
In recent years, LMWH has garnered attention for its potential to improve placental blood supply.15,23 Nevertheless, robust clinical evidence supporting its widespread use is still lacking.
Study Design and Key Findings
This prospective cohort study systematically compared the effects of three interventions on FGR treatment: Intervention 1: Low-flow nasal oxygen therapy combined with parenteral nutrition. Intervention 2: Intervention 1 plus LMWH. Intervention 3: Intervention 2 plus routine NHFOT therapy. Results indicated that Intervention 3 (NHFOT combined with LMWH) outperformed the group receiving only parenteral nutrition support in several key aspects: Prolongation of gestational age at delivery: 267.5 days versus 265.0 days (P=0.002). Increase in neonatal birth weight: 2600 g versus 2360 g (P<0.001). Higher FGR cure rate: 45.83% versus 18.75% (P=0.042). Reduced incidence of LBW: 33.33% versus 65.63% (P=0.013). While Group 3 demonstrated superior outcomes compared with Group 1 (standard care), the incremental benefit of adding NHFOT to LMWH (ie., Group 3 vs Group 2) did not reach statistical significance for most endpoints—including FGR cure rate (45.83% vs 32.43%, P = 0.213)—though numerical trends favored Group 3. This suggests that the combination of LMWH and NHFOT may yield additive rather than synergistic effects within this sample size, and larger studies are needed to detect smaller but clinically meaningful differences between these two active interventions.
Conclusions and Clinical Implications
These findings suggest that combining NHFOT with LMWH may improve clinical outcomes in FGR by extending gestation, increasing fetal weight, and reducing LBW risk. This integrated approach offers a promising direction for future clinical practice and warrants further investigation.
Non-randomized grouping may introduce selection bias; however, the comparability of baseline characteristics (Table 2) and the patient’s autonomous decision-making mechanism effectively mitigate this risk. According to the study results, at the time of FGR diagnosis with different interventions, no statistically significant differences (P > 0.05) were observed among the three groups in fetal umbilical artery blood flow parameters—including Resistance Index (RI), Systolic/Diastolic ratio (S/D)—gestational age at diagnosis, or the proportion of estimated fetal weight below the 3rd percentile. This indicates that the baseline characteristics among the groups are comparable. Post-treatment umbilical blood flow parameters were not analyzed due to inconsistent follow-up times; future studies should monitor these parameters at fixed time points.
Recent studies have demonstrated that hyperbaric oxygen therapy (HBOT) can improve uterine and placental blood circulation, enhance placental oxygenation and function, and promote fetal growth and development.24 Other research has shown that HBOT significantly reduces fetal RI, S/D values, and whole blood viscosity, substantially improving placental microcirculation, alleviating fetal distress, promoting fetal growth, and improving perinatal outcomes.25,26 Our study suggests that combining NHFOT with LMWH may have a synergistic effect in improving clinical outcomes in FGR.
Key Outcome Comparisons
Gestational Age at Delivery: The median gestational age in Intervention Group 3 was 267.5 days, significantly longer than 264.0 days in Group 2 and 265.0 days in Group 1 (P < 0.05). No significant difference was observed between Groups 1 and 2 (P > 0.05).
Neonatal Birth Weight
The median birth weight in Group 3 was 2600 g, higher than 2442 g in Group 2 and 2360 g in Group 1 (P < 0.05). No significant difference was found between Group 2 and either of the other two groups (P > 0.05).
FGR Cure Rate
The cure rate (birth weight ≥ 10th percentile for gestational age) was 45.83% in Group 3, significantly higher than 18.75% in Group 1 (P < 0.05). No significant difference was observed between Group 2 and the other groups (P > 0.05).
LBW Rate
The LBW rate in Group 3 was 33.33%, significantly lower than 65.63% in Group 1 (P < 0.05). The LBW rate in Group 2 was 54.05%, with no significant difference compared to either of the other groups (P > 0.05).
Preterm Birth Rate & Umbilical Artery Blood Gas
There were no statistically significant differences among the three groups regarding preterm birth rates (P > 0.05) or umbilical artery blood gas parameters (pH, lactate) (P > 0.05). This suggests that NHFOT during pregnancy has limited impact on neonatal umbilical artery blood gas analysis.
Potential Mechanisms of HBOT
Hyperbaric oxygen therapy may improve uteroplacental circulation through multiple mechanisms. Specifically, HBOT can significantly increase blood oxygen partial pressure (by 10–15 times) and extend oxygen diffusion distance (by 3–4 times), effectively alleviating placental hypoxia.27 These effects may be related to: Reversing Hypoxic Vasoconstriction: HBOT increases tissue oxygen reserves, reversing hypoxic vasoconstriction in the intervillous space of the placenta. Reducing Oxidative Stress Damage: It inhibits oxidative stress reactions, reducing free radical damage to placental vascular endothelial cells.26,27 Promoting Vascular Remodeling: It modulates the expression of placental angiogenic factors (such as VEGF, PlGF), promoting placental vascular remodeling.28
However, it is important to note that HBOT still faces significant limitations in obstetric applications. Multiple studies have reported potential complications, including barotrauma-related middle ear damage (incidence approximately 17%), oxygen toxicity (around 2%), and a theoretical increased risk of miscarriage, especially during early pregnancy.29 These safety concerns substantially restrict the clinical use of HBOT during pregnancy.30 In contrast, conventional low-concentration oxygen therapy, which only elevates oxygen partial pressure by about 20–30%, has limited efficacy in improving FGR.26 Based on our findings, NHFOT may serve as an alternative approach that balances efficacy and safety. Theoretically, NHFOT combines the oxygenation advantages of hyperbaric oxygen with the safety profile of normobaric oxygen.26,30 However, this hypothesis requires validation through rigorous controlled studies, particularly to clarify the dose-response relationship between different oxygen therapy modalities and their effects on placental hemodynamics, as well as long-term fetal outcomes.
NHFOT involves the administration of high-concentration, high-flow oxygen via mask or nasal cannula under normobaric conditions. The oxygen flow rate typically ranges from 8 to 10 L/min, with oxygen concentrations reaching up to 95%. Existing studies have demonstrated that normobaric oxygen therapy can directly increase the partial pressure and oxygen content in the maternal blood, placenta, and fetus, thereby enhancing tissue oxygen reserves. It also elevates blood oxygen tension, accelerates blood flow velocity, increases the diffusion radius of oxygen in capillaries, reduces the accumulation of acidic metabolic waste, and improves uterine blood supply and blood flow stagnation. These effects collectively enhance oxygen supply and placental function, increasing fetal oxygen and energy supply.31 In recent years, normobaric oxygen therapy has gradually been applied in clinical obstetric treatments for conditions such as fetal distress, fetal arrhythmia, and placental insufficiency, achieving certain therapeutic effects.32 However, its efficacy and safety in treating other common obstetric conditions—such as FGR, pregnancy-induced hypertension, and oligohydramnios—remain to be further investigated. LMWH also plays an important role during pregnancy. As an anticoagulant, it primarily inhibits coagulation factors, reduces blood viscosity, and improves placental microcirculation. This reduces placental thrombosis and increases placental perfusion, facilitating greater nutrient transfer to the fetus. Animal studies have shown32 that treatment of FGR with normobaric high-concentration oxygen therapy yields comparable significant efficacy to hyperbaric oxygen therapy, suggesting that normobaric high-flow oxygen could serve as a novel therapeutic approach for FGR. Additionally, some studies33 indicate that both standalone NHFOT and LMWH can effectively reduce umbilical artery resistance and improve fetal distress and FGR.
Conclusions
This prospective cohort study suggests that in the present FGR cohort, idiopathic FGR, combining normobaric high-flow oxygen therapy with low molecular weight heparin may offer incremental benefits over standard supportive care alone, primarily in increasing fetal birth weight and reducing the incidence of low birth weight. However, the clinical significance of these modest improvements remains to be determined, and the combination therapy did not conclusively demonstrate superior efficacy to LMWH alone for the primary cure outcome. Given the non-randomized design, sample size constraints, and inherent heterogeneity of FGR, these findings should be considered preliminary. Future large-scale, randomized trials are warranted to validate the efficacy of this combined regimen and to identify which subgroups of FGR patients might benefit most.
Limitations of the Study
This study has limitations that should be considered when interpreting the findings. The non-randomized, patient-preference design, while reflecting real-world decision-making, is inherently susceptible to residual confounding. Although baseline characteristics were comparable, unmeasured or unadjusted variables—such as detailed nutritional intake, patterns of gestational weight gain, maternal anemia, hypoalbuminemia, and subclinical antenatal infections—could influence fetal growth independently of the interventions and may not have been evenly distributed between groups. The single-center setting and relatively modest sample size limit statistical power to detect smaller effects and precluded the use of multivariate models to adjust for these potential confounders. Furthermore, the clinical heterogeneity of the cohort must be acknowledged. Although all cases were diagnosed within the 28- to 37-week window, this range inherently includes both early-onset and late-onset FGR subtypes, which are associated with differing severity and placental pathophysiology. This variability may influence treatment response and suggests that our results should be interpreted as an average effect across this spectrum; generalizability to specific subtypes, particularly more severe early-onset forms, may be limited. The clinical significance of the observed improvements, such as the modest increase in birth weight, requires careful interpretation, as their long-term implications for child health were not assessed—a crucial area for future investigation. Methodologically, umbilical artery Doppler indices were compared as raw values rather than as proportions exceeding gestational age-specific thresholds, and post-treatment Doppler parameters were not analyzed due to inconsistent follow-up timing. Future larger-scale, randomized controlled trials with comprehensive phenotyping and long-term follow-up are needed to confirm the efficacy of this combined regimen and to identify the patient subgroups most likely to benefit.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study received approval from the Ethics Committee of the Second Nanning People’s Hospital [Y2022021].
Acknowledgments
We acknowledge the clinical support provided by the obstetric team at The Second Nanning People’s Hospital during data collection. All researchers maintained independence in study design, data analysis, and interpretation. We would like to thank the funding which gave us financial support: The Self-funded Research Project of the Health Commission of Guangxi Zhuang Autonomous Region.
Author Contributions
MeiRong He and KaiSun Zhao have contributed equally to this work and are both first authors.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by The Self-funded Research Project of the Health Commission of Guangxi Zhuang Autonomous Region [grant number Z-A20221158].
Disclosure
The authors have no conflict of interests to declare.
References
1. Salmeri N, Carbone IF, Cavoretto PI, Farina A, Morano D. Epigenetics beyond fetal growth restriction: a comprehensive overview. Mol Diagn Ther. 2022;26(6):607–10. doi:10.1007/s40291-022-00611-4.
2. Fernandez A, Liauw J, Mayer C, Albert A, Hutcheon JA. Predictive ability of fetal growth charts in identifying kindergarten-age developmental challenges: a cohort study. Ame J Obstetr Gynecol MFM. 2024;6(1):101220. doi:10.1016/j.ajogmf.2023.101220.
3. Sypiańska M, Stupak A. Introduction to the proteomic analysis of placentas with fetal growth restriction and impaired lipid metabolism. Metabolites. 2024;14(11):632. doi:10.3390/metabo14110632.
4. Juan J, Yang HX. Impact of fetal growth restriction on perinatal outcomes and long-term health. Chin J Prac Gynecol Obstet. 2020;36(8):710–713. doi:10.19538/j.fk2020080111
5. Liu J, Wang XF, Wang Y, et al. The incidence rate,high- risk factors, and short- and long- term adverse outcomes of fetal growth restriction:a report from Mainland China. Medicine. 2014;93(27):e210. doi:10.1097/MD.0000000000000210
6. Wang ML, Li Y, Luo D, et al. Pregnancy outcomes of expectant management for early-onset severe preeclampsia complicated with fetal growth restriction. Maternal Child Health Care China. 2016;31(14):2810–2812. doi:10.7620/zgfybj.j.issn.1001-4411.2016.14.16
7. Buffat C, Mondon F, Rigourd V, et al. A hierarchical analysis of transcriptome alterations in intrauterine growth restriction (IUGR) reveals common pathophysiological pathways in mammals. Pathol. 2007;213(3):337–346. doi:10.1002/path.2233
8. Su EJ. Scaling the EVERREST of severe, early-onset fetal growth restriction. J Clin Invest. 2023;133(18):e173563. doi:10.1172/JCI173563.
9. Longo S, Bollani L, Decembrino L, et al. Short-term and longterm sequelae in intrauterine growth retardation (IUGR). Matern Fetal Neonatal Med. 2013;26(3):222–225. doi:10.3109/14767058.2012.715006
10. Godfrey KM, Inskip HM, Hanson MA, et al. The long-term effects of prenatal development on growth and metabolism. Semin Reprod Med. 2011;29(3):257–265. doi:10.1055/s-0031-1275518
11. Fan ZT, Yang HX. The long-term effects of malnutrition during pregnancy on offspring. Chin J Perinat Med. 2005;8(4):278–281. doi:10.3760/cma.j.issn.1007-9408.2005.04.020
12. Thorn SR, Rozance PJ, Brown LD, et al. The intrauterine growth restriction phenotype:fetal adaptations and potential implications for later life insulin resistance and diabetes. Semin Reprod Med. 2011;29(3):225–236. doi:10.1055/s-0031-1275516
13. Kesavan K, Devaskar SU. Intrauterine growth restriction:postnatal monitoring and outcomes. Pediatr Clin North Am. 2019;66(2):403–423. doi:10.1016/j.pcl.2018.12.009
14. Jaddoe VW, de Jonge LL, Hofman A, et al. First trimester fetal growth restriction and cardiovascular risk factors in school age children:population based cohort study. BMJ. 2014;348:g14. doi:10.1136/bmj.g14
15. Singh KK, Gupta A, Forstner D, et al. LMWH prevents thromboinflammation in the placenta via HBEGF-AKT signaling. Blood Adv. 2024;8(18):4756–4766. doi:10.1182/bloodadvances.2023011895.
16. Oluklu D, Menekse Beser D, Uyan Hendem D, et al. Assessment of fetal cardiac morphology and functional changes in early-onset and late-onset fetal growth restriction. Int J Gynaecol Obstet. 2023;161(1):241–249. doi:10.1002/ijgo.14602.
17. Chen Y, Lv X, Yang L, Hu D, Ren M. Evaluation of fetal heart size, morphology and function with fetal growth restriction using fetal HQ. BMC Pregnancy Childbirth. 2024;24(1):751. doi:10.1186/s12884-024-06966-2.
18. Yehuda B, Rabinowich A, Zilberman A, et al. Reduced gyrification in fetal growth restriction with prenatal magnetic resonance images. Cereb Cortex. 2024;34(6):bhae250. doi:10.1093/cercor/bhae250.
19. Ge T, Kong J. Clinical value of serum SIRT1 combined with uterine hemodynamics in predicting disease severity and fetal growth restriction in preeclampsia. J Med Biochem. 2024;43(4):350–362. doi:10.5937/jomb0-37645.
20. Odongkara B, Nankabirwa V, Ndeezi G, et al. Incidence and risk factors for low birthweight and preterm birth in post-conflict Northern Uganda: a community-based cohort study. Int J Environ Res Public Health. 2022;19(19):12072. doi:10.3390/ijerph191912072.
21. Hewish A, Dibley MJ, Raihana S, et al. The neonatal mortality risk of vulnerable newborns in rural Bangladesh: a prospective cohort study within the Shonjibon trial. Trop Med Int Health. 2025;30(4):283–291. doi:10.1111/tmi.14092.
22. Hao W, Hongbo Q. Global guidelines for fetal growth restriction: seeking consensus while acknowledging differences. Chin J Perinatal Med. 2024;27(9):710–721. doi:10.3760/cma.j.cn113903-20240709-00507
23. Wang P, Shan TF. Clinical efficacy and feasibility of low molecular weight heparin combined with magnesium sulfate in the treatment of fetal growth restriction. Maternal Child Health Care China. 2017;32(17):4171–4173. doi:10.7620/zgfybj.j.issn.1001-4411.2017.17.52
24. Liu LH, Yang H, Zhao YZ. Efficacy of magnesium sulfate combined with hyperbaric oxygen therapy in the treatment of fetal growth restriction and its effects on nitric oxide and prostaglandin levels in maternal peripheral blood. Chin J Family Planning Gynecotokol. 2019;11(3):49–52. doi:10.3969/j.issn.1674-4020.2019.03.13
25. Hongjian L, Xiaohua W, Jinbao S, et al. Efficacy analysis of hyperbaric oxygen comprehensive therapy for patients with severe preeclampsia complicated by fetal growth restriction. Chin J Prac Gynecol Obstet. 2007;23(2):113–116.
26. Olex-Zarychta D. Effects of hyperbaric oxygen therapy on human psychomotor performance: a review. J Integr Med. 2023;21(5):430–440. doi:10.1016/j.joim.2023.08.006.
27. Tu P, Halili X, Zhang S, Yang J, Xiao Y. The effectiveness of hyperbaric oxygen therapy in children and adolescents and with autism spectrum disorders: a systematic review and meta-analysis. Prog Neuropsychopharmacol Biol Psychiatry. 2025;137:111257. doi:10.1016/j.pnpbp.2025.111257
28. Zhou H, Zhao C, Wang P, Yang W, Zhu H, Zhang S. Regulators involved in trophoblast syncytialization in the placenta of intrauterine growth restriction. Front Endocrinol. 2023;14:1107182. doi:10.3389/fendo.2023.1107182
29. Zhang Y, Zhou Y, Jia Y, Wang T, Meng D. Adverse effects of hyperbaric oxygen therapy: a systematic review and meta-analysis. Front Med Lausanne. 2023;10:1160774. doi:10.3389/fmed.2023.1160774
30. Kulseng CPS, Sommerfelt S, Flo K, et al. Corrigendum to “Placental size at gestational week 27 and 37: the associations with pulsatility index in the uterine and the fetal-placental arteries” [Placenta 145C (2024) 45-50]. Placenta. 2025;164:49. doi:10.1016/j.placenta.2025.03.011
31. Ren GP, Wang BL, Yuan SX, et al. Efficacy analysis of comprehensive management with normobaric high-concentration oxygen therapy for fetal growth restriction. Chinese J Mod Drug App. 2016;10(19):5–7. doi:10.14164/j.cnki.cn11-5581/r.2016.19.003
32. Wan T, Pan SL, YL A, et al. Efficacy of hyperbaric oxygen and normobaric high-concentration oxygen therapy in experimental fetal growth restricted rats. Med J Chin PLA. 2011;36(10):1057–1061.
33. Li J, Huang CL. Liang XX. Application effect of high-flow oxygen therapy outside the oxygen chamber in pregnant women with increased umbilical artery resistance. Guangxi Med J. 2018;40(18):2141–2143. doi:10.11675/j.issn.0253-4304.2018.18.02
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.