Back to Journals » International Medical Case Reports Journal » Volume 18
Efficacy of Intravenous Tenecteplase Bridge Thrombectomy for Recurrent Ischemic Stroke Within 3 Months: A Case Report
Authors Liu C, Liu J, Ren H, Xu Y, Liu W ![]()
Received 5 October 2024
Accepted for publication 22 January 2025
Published 10 February 2025 Volume 2025:18 Pages 235—239
DOI https://doi.org/10.2147/IMCRJ.S497458
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rakesh Kumar
Cuicui Liu, Junyan Liu, Huiling Ren, Yuzhu Xu, Wanhu Liu
Department of Neurology, The Third Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China
Correspondence: Wanhu Liu, Department of Neurology, The Third Hospital of Hebei Medical University, 139 Ziqiang Road, Shijiazhuang, 050000, People’s Republic of China, Email [email protected]
Abstract: In the previous guideline recommendations, patients who have had a stroke within 3 months are excluded from intravenous thrombolysis (IVT) regimens. Some studies have suggested that IVT with alteplase (rt-PA) may be effective and safe in such patients, but evidence supporting the use of tenecteplase (TNK) is not sufficient. This paper includes an 80-year-old male patient readmitted for recurrence of ischaemic stroke (IS) after 48 days, who received TNK IVT as a bridging therapy prior to thrombectomy, with favourable results at 8-week follow-up. This case highlights that TNK alone or IVT as a bridging therapy prior to thrombectomy can also benefit patients with recurrent stroke within 3 months.
Keywords: intravenous thrombolysis, recurrent ischemic stroke, tenecteplase
Introduction
Although secondary prevention measures are initiated immediately after stroke, recurrent ischemic stroke (RIS) cannot be completely avoided, especially in patients with large artery atherosclerosis and cardioembolic stroke.1 An RIS in the vertebrobasilar territory is usually associated with poor outcomes and a high mortality rate.2 Nevertheless, considering the increased risk of intracerebral hemorrhage, patients who had a history of previous ischemic stroke within 3 months with severe residual clinical or large infarct lesions were excluded from intravenous thrombolysis (IVT) with alteplase (rt-PA).3 Currently, populations who will benefit from IVT with tenecteplase (TNK) are being screened. The TRACE II study4 confirmed that TNK was noninferior to rt-PA in patients with acute ischemic stroke (IS) within 4.5 h of onset. Based on these results, guidelines indicate that TNK can be considered an alternative to rt-PA when IS onset occurs within 4.5 h. However, the efficacy and safety of TNK intravenous thrombolysis as a bridging treatment prior to mechanical thrombectomy in recurrent stroke within three months has not been previously reported. This case can provide confidence in intravenous tenecteplase bridge thrombectomy for recurrent ischemic stroke within 3 month.
Case Presentation
An 80-year-old right-handed male who was admitted for acute IS presented with consciousness and vomiting for 2 hours; he had experienced IS in the vertebrobasilar territory forty-eight days prior (Figure 1a), accompanied by a decrease in the distal branches of the right posterior cerebral artery (Figure 1b). He had mild cognitive impairment as a residual condition after the previous stroke, but daily life independence was mildly affected (2 points on the modified Rankin scale). The patient was administered 100 mg of aspirin and 75 mg of clopidogrel daily for 21 days, and then administered 100 mg of aspirin along with atorvastatin as a secondary prevention strategy. Additionally, he had a medical history of diabetes and coronary heart disease. On examination, his positive signs included lethargy, dysarthria, sustained right gaze deviation, right-sided central facial paralysis, reduced muscle strength but the ability to withdraw upon painful stimulation, slightly elevated muscle tone, and positive Babinski’s sign bilaterally; his National Institutes of Health Stroke Scale (NIHSS) score was 10 points.
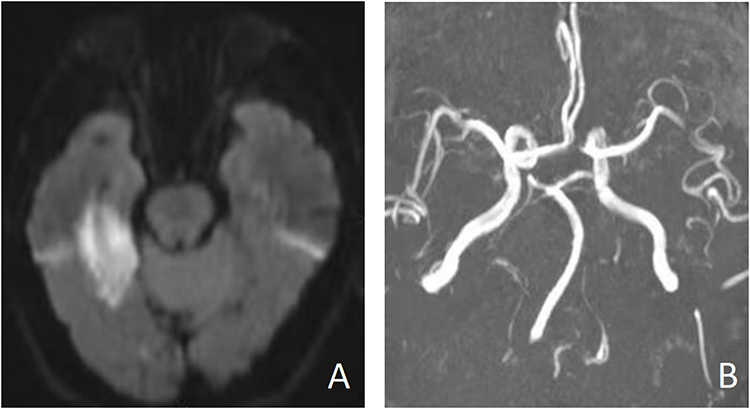 |
Figure 1 First IS occured. (A) DWI revealed an acute infarct lesion in the right temporal lobe. (B) MRA showed a decrease in the distal branches of the right posterior cerebral artery and no development of the left vertebral artery. |
A CT scan ruled out cerebral hemorrhage, while MRA and DWI revealed occlusion of the left vertebral artery and the distal basilar artery (Figure 2c), along with infarction in the right thalamus, bilateral cerebellar hemispheres, and vermis (Figure 2a and b). Notably, there was no evidence of brainstem involvement on DWI. Considering the high risk of neurological deterioration in our patient, which indicated a poor outcome, despite his history of previous IS within 3 months, IVT with TNK 16 mg (0.25 mg/kg, weight = 64 kilograms) was administered (door-to-needle time [DNT] was 22 min). Thrombectomy was delayed because of concerns about the cost of the procedure. There was no notable improvement within 2 hours after intravenous thrombolysis. Ninety-seven minutes after IVT with TNK, we performed digital subtraction angiography (DSA)-guided recanalization of the distal basilar artery and the left vertebral artery, and only the right posterior cerebral artery was occluded (Figure 2d). Subsequently, a thrombectomy was performed on the right posterior cerebral artery, and reperfusion in the posterior circulation was achieved successfully (Figure 2e). A repeat CT scan after 24 hours confirmed the absence of hemorrhagic complications. Postoperative DSA showed no significant posterior circulation vessel stenosis, no thrombosis in subsequent cardiac ultrasound, and paroxysmal array atrial fibrillation was found at 24 h Hoter, so the patient was ultimately considered as cardioembolization.
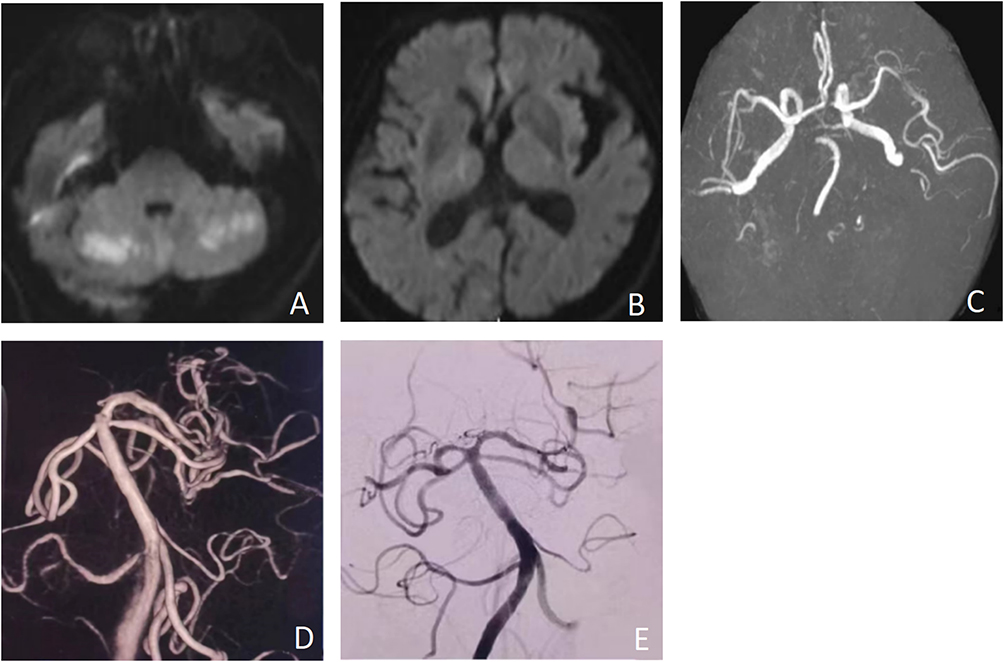 |
Figure 2 Second admission due to RIS. (A and B) RIS onset before using TNK, presented with DWI, confirmed infarction in the right thalamus, bilateral cerebellar hemispheres, and vermis.(C) MRA showed occlusion on a left vertebral artery and the distal basilar artery. (D) 97 minutes later after IVT with TNK, DSA showed recanalization in the bilateral superior cerebellar artery, left posterior cerebral artery and left vertebral artery. (E) After thrombectomy,DSA showed recanalization in the right posterior cerebral artery. |
The 90 days follow-up showed that our patient had recovered to the pre-recurrent-stroke state, without residual ataxia or swallowing disorders, and at the time of publication, there was no significant effect on the patient’s daily life independence, his NIHSS score and mRS was 2 points.
Discussion
Currently, there was no recommendation for IVT with TNK in patients with RIS within 3 months. In patients with RIS < 4.5 h in duration with a small infarct, stroke occurring more than one month earlier, or good clinical recovery, thrombolysis with rt-PA was reasonable based on the expert consensus statement,3 but no large randomized controlled clinical trials have confirmed this recommendation. A previous study demonstrated that there were no significant differences in 90-day functional outcomes, symptomatic intracranial hemorrhage, or mortality between patients diagnosed with RIS within 3 months and those diagnosed with first-ever stroke by using rt-PA. A registry-based analysis of data from Stroke–Eastern Europe suggested that for patients treated with rt-PA, a history of stroke ≤3 months was associated with good outcomes at 3 months (odds ratio [OR] 0.81, 95% CI: 0.61–1.09).5 Even repeated intravenous thrombolysis in the RIS within 3 months seems to be effective. A study by Wen et al showed that patients with RIS within 3 months of either anterior or posterior circulation who achieved a good outcome after previous IVT or a low baseline NIHSS score seemed to benefit from repeated intravenous thrombolysis.6,7 However, this is not the case for those with a short interval between thrombolysis, a high baseline NIHSS score, or cardiogenic embolism, owing to a greater risk of symptomatic intracranial hemorrhage (sICH).6
In terms of safety, studies on the feasibility and safety of IVT with rt-PA in patients with RISs within 3 months have been conducted, but the results differ among a small subset of studies. A recent meta-analysis by Ignacio et al showed that intravenous rt-PA for RIS within 3 months was not associated with an increased incidence of sICH (OR 1.39, 95% CI 0.75–2.58) or mortality (OR 1.36, 95% CI 0.60–3.09).8 A meta analysis by Tsivgoulis et al also showed that IVT administration in patients with RIS within 3 months was not increased the risk of sICH or mortality.9 In addition, Merkler et al suggested that there was no significant difference in the incidence of sICH between the group with RIS or without RIS, but it was associated with a greater risk of death (OR, 1.5; 95% CI, 1.2–1.9; =0.001) and unfavorable discharge disposition (OR, 1.3; 95% CI, 1.0–1.7; =0.04).10 Heldner et al showed that intravenous rt-PA in patients with RISs within 3 months seemed to be associated with higher sICH and mortality rates.11 Malignant event did not occur in our case, which also suggests that intravenous thrombolysis may be safe for early recurrent stroke in the posterior circulation.
Compared with rt-PA, several randomized clinical trials have demonstrated that IVT with TNK is not inferior in terms of good outcomes in patients with IS within 4.5 hours. Patients with acute IS within 4.5 hours of onset were included in the TRACE-2 study4 and were randomly assigned to the TNK or rt-PA treatment group. The results showed that the excellent clinical outcome in the TNK group was not inferior to that in the rt-PA group, similar to the conclusion in ACT research.12 There were indeed no significant differences between TNK and rt-PA in terms of sICH rates, providing evidence supporting the safety of IVT with TNK. Additionally, there are lower odds of sICH after IVT with TNK than after rt-PA in the real world.13,14 A study by Warach et al12 further highlighted its safety in clinical applications. This may be attributed to the greater fibrin specificity of TNK.15
Currently, data on the efficacy and safety of TNK in patients with RIS within 3 months are insufficient. Our patient who had suffered a previous stroke forty-eight days before being treated with TNK had excellent outcomes and no adverse events, indicating that IVT with TNK may be an effective and safe strategy for preventing the progression of stroke.
Stroke in the vertebrobasilar territory is usually associated with a worse prognosis. Dorňák et al16 reported that only 30% of patients achieved good clinical outcomes after stroke. The combination of TNK bridging therapy with thrombectomy was recommended for patients with large vessel occlusion acute ischemic stroke within 4.5 hours to address these problems.17 According to the guidelines, our patient underwent mechanical thrombectomy after IVT with TNK and achieved excellent outcomes at the 90-day follow-up. However, the outcome cannot be credited to mechanical thrombectomy. Notably, DSA conducted two hours after IVT with TNK revealed significant recanalization of most posterior circulation vessels. Hence, the remarkable thrombolytic effect achieved in this patient should not be overshadowed by the subsequent mechanical thrombectomy procedure. The good outcome in our patient also attributed to the short DNT time. In our country, relying on the National Stroke Center Construction Projects, we are working on shorten DNT time for more patients to benefit from intravenous thrombolysis.18
Conclusion
In conclusion, patients with recurrent stroke within 3 months may also benefit from IVT combined with TNK alone or as a bridging therapy before thrombectomy. There is insufficient evidence to substantiate exclusion of this group from IVT with TNK treatment alone or as a bridging therapy before thrombectomy. Despite the positive results of TNK thrombolysis bridging before thrombectomy in our patient, limitations related to the presentation of the one isolated case must be considered. Further large-scale evidence-based clinical trials are needed to re-examine the potential use of TNK in RIS treatment.
Data Sharing Statement
Data are available from the corresponding authors upon reasonable request.
Ethical Statement
This study was approved by the Research Ethics Committee of Hebei Medical University Third Hospital. The patient is informed and consented to the publication of the case and authorizes his next of kin to sign the informed consent on his or her behalf.
Acknowledgment
This paper has been uploaded to Research Square as a preprint: https://www.researchsquare.com/article/rs-4231963/v1.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, they took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grant from the 2024 Medical Science Research Project of Hebei (Grant NO. 20242292).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kolmos M, Christoffersen L, Kruuse C. Recurrent ischemic stroke–a systematic review and meta-analysis. J Stroke Cerebrovasc Dis. 2021;30(8):105935. doi:10.1016/j.jstrokecerebrovasdis.2021.105935
2. Sparaco M, Ciolli L, Zini A. Posterior circulation ischaemic stroke-a review part I: anatomy, aetiology and clinical presentations. Neurol Sci. 2019;40(10):1995–2006. doi:10.1007/s10072-019-03977-2
3. Berge E, Whiteley W, Audebert H, et al. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur Stroke J. 2021;6(1):I–LXII. doi:10.1177/2396987321989865
4. Wang Y, Li S, Pan Y, et al. Tenecteplase versus alteplase in acute ischaemic cerebrovascular events (TRACE-2): a Phase 3, multicentre, open-label, randomised controlled, non-inferiority trial. Lancet. 2023;401(10377):645–654. doi:10.1016/S0140-6736(22)02600-9
5. Karlinski M, Kobayashi A, Czlonkowska A, et al. Intravenous thrombolysis for stroke recurring within 3 months from the previous event. Stroke. 2015;46(11):3184–3189. doi:10.1161/STROKEAHA.115.010420
6. Wen S, Chen F, Chen X, et al. Repeated intravenous thrombolysis in recurrent ischemic stroke within 3 months: a systematic review. BMC Neurol. 2023;23(1):422. doi:10.1186/s12883-023-03472-4
7. Černík D, Ospalík D, Šaňák D, et al. Repeated intravenous thrombolysis in patients with recurrent ischemic stroke in the vertebrobasilar territory. Case Rep Neurol. 2021;13(2):510–514. doi:10.1159/000518193
8. Ignacio KHD, Diestro JDB, Espiritu AI, et al. Re-examining the exclusion criterion of early recurrent ischemic Stroke in intravenous thrombolysis: a meta-analysis. J Neurol Sci. 2020;15(412):116709. doi:10.1016/j.jns.2020.116709
9. Tsivgoulis G, Katsanos AH, Schellinger PD, et al. Intravenous thrombolysis in patients with acute ischaemic stroke with history of prior ischaemic stroke within 3 months. J Neurol Neurosurg Psychiatry. 2019;90(12):1383–1385. doi:10.1136/jnnp-2019-320422
10. Merkler AE, Salehi Omran S, Gialdini G, et al. Safety outcomes after thrombolysis for acute ischemic stroke in patients with recent stroke. Stroke. 2017;48(8):2282–2284. doi:10.1161/STROKEAHA.117.018119
11. Heldner MR, Mattle HP, Jung S, et al. Thrombolysis in patients with prior stroke within the last 3 months. Eur J Neurol. 2014;21(12):1493–1499. doi:10.1111/ene.12519
12. Menon BK, Buck BH, Singh N, et al. Intravenous tenecteplase compared with alteplase for acute ischaemic stroke in Canada (AcT): a pragmatic, multicentre, open-label, registry-linked, randomised, controlled, non-inferiority trial. Lancet. 2022;400(10347):161–169. doi:10.1016/S0140-6736(22)01054-6
13. Warach SJ, Ranta A, Kim J, et al. Symptomatic intracranial hemorrhage with tenecteplase vs alteplase in patients with acute ischemic stroke: the Comparative Effectiveness of Routine Tenecteplase vs Alteplase in Acute Ischemic Stroke (CERTAIN) Collaboration. JAMA Neurol. 2023;80(7):732–738. doi:10.1001/jamaneurol.2023.1449
14. Rose D, Cavalier A, Kam W, et al. Complications of intravenous tenecteplase versus alteplase for the treatment of acute ischemic stroke: a systematic review and meta-analysis. Stroke. 2023;54(5):1192–1204. doi:10.1161/STROKEAHA.122.042335
15. Thiebaut AM, Gauberti M, Ali C, et al. The role of plasminogen activators in stroke treatment: fibrinolysis and beyond. Lancet Neurol. 2018;17(12):
16. Dorňák T, Herzig R, Školoudík D, et al. Outcome predictors in acute basilar artery occlusion. Can J NeurolSci. 2014;41:368–374. doi:10.1017/s0317167100017327
17. Alamowitch S, Turc G, Palaiodimou L, et al. European Stroke Organisation (ESO) expedited recommendation on tenecteplase for acute ischaemic stroke. Eur Stroke J. 2023;8(1):8–54. doi:10.1177/23969873221150022
18. Cheng W, Mofatteh M, Baizabal-Carvallo JF, et al. Impact of thrombolysis time metrics when participating in national stroke center construction project. J Multidiscip Healthc. 2023;16:3333–3338. doi:10.2147/JMDH.S432458
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.