Back to Journals » Clinical and Experimental Gastroenterology » Volume 8
Efficacy of a pH-dependent controlled-release mesalazine based on clinical and endoscopic assessment for ulcerative colitis: a retrospective cohort study
Authors Matsumoto S ![]() , Yoshida Y
, Yoshida Y
Received 13 April 2015
Accepted for publication 9 June 2015
Published 31 July 2015 Volume 2015:8 Pages 225—230
DOI https://doi.org/10.2147/CEG.S86528
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Andreas M. Kaiser
Satohiro Matsumoto, Yukio Yoshida
Department of Gastroenterology, Saitama Medical Center, Jichi Medical University, Saitama, Japan
Background: We conducted a retrospective cohort study to clinically and endoscopically assess the efficacy of delayed-release mesalazine for ulcerative colitis.
Methods: The study included 104 ulcerative colitis patients (52 men, 52 women) initiated on treatment with delayed-release mesalazine between 2009 and 2012. The clinical symptoms at months 0, 1, and 12 were scored using the clinical activity index. An endoscopic index was also used to determine disease activity in 72 patients who underwent total colonoscopy before and after mesalazine treatment.
Results: The clinical activity index at months 0, 1, and 12 were 4.6±2.8, 3.4±1.8, and 2.8±1.4, respectively, decreasing with time after the start of mesalazine treatment (P<0.001). The endoscopic index decreased significantly from 4.5±3.2 before to 3.1±2.8 after the start of delayed-release mesalazine treatment in the mean follow-up period of 1.0±0.4 years (P<0.001).
Conclusion: Delayed-release mesalazine was confirmed to be effective both clinically and endoscopically.
Keywords: ulcerative colitis, pH-dependent controlled-release mesalazine, clinical activity index, endoscopic index
Introduction
The pH-dependent 5-aminosalicylic acid (5-ASA) releasing preparation, widely used as a standard drug for remission induction and maintenance therapies in patients with inflammatory bowel disease, was approved for coverage by the national health insurance in Japan in December 2009. At present, three types of 5-ASA releasing preparations are available in Japan: the time-dependent 5-ASA releasing preparation (Pentasa®), the pH-dependent 5-ASA releasing preparation (Asacol®), and salazosulfapyridine (SASP).
The presumed mechanisms of action of 5-ASA, which exerts local anti-inflammatory effects in the colonic mucosa in cases of inflammatory bowel disease, include inhibition of inflammatory cytokines and elimination of free radicals.1 However, after 5-ASA is absorbed from the gastrointestinal tract into the systemic circulation, it is immediately inactivated. Thus, various pharmaceutical modifications of 5-ASA have been attempted. A time-dependent 5-ASA releasing preparation releases 5-ASA into the entire small intestine and the large intestine in a time-dependent manner because of the methylcellulose coating. Meanwhile, a pH-dependent 5-ASA releasing preparation (delayed-release mesalazine) releases 5-ASA from the distal ileum downwards, where the pH is 7 or above. As compared to conventional preparations (Pentasa®) that release 5-ASA from the small intestine downwards, delayed-release mesalazine (Asacol®) is considered to deliver a larger amount of 5-ASA into the large intestine at similar doses via a drug delivery system that releases 5-ASA into the large intestine from the distal ileum downwards.2,3
Since the launch of delayed-release mesalazine (Asacol®) in the market in Japan, the prescription of the drug for the treatment of ulcerative colitis (UC) has increased dramatically at our center. While there have been a number of reports on the therapeutic efficacy of delayed-release mesalazine (Asacol®), there are still few studies focusing on the therapeutic effects of the drug based on endoscopic assessment. The present study was designed to perform clinical and endoscopic assessment of the efficacy of delayed-release mesalazine (Asacol®) in patients with UC.
Materials and methods
Subjects
A total of 186 UC patients who were started on treatment with delayed-release mesalazine (Asacol®) and underwent periodic follow-up on an outpatient basis at the Saitama Medical Center between 2009 and 2012 were retrospectively identified from medical records and enrolled in this study. The inclusion criteria were as follows: 1) patients who were 16 years of age and older at the time of registration and 2) patients who were under periodic follow-up on an outpatient basis for at least 1 year. The exclusion criteria were as follows: 1) patients who discontinued the treatment with delayed-release mesalazine due to the development of adverse reactions and 2) patients who were observed on an outpatient basis for less than 1 year. Finally, the data of 104 of these patients (52 men, 52 women; mean age at onset of UC, 33±14 years; mean age at entry of the study, 43±15 years; mean disease duration, 11.0±8.8 years) were analyzed and all were followed-up through December 2013. All data of the study were collected exclusively by reviewing preexisting medical records. The mean follow-up period was 2.4±0.6 years (range: 1.2–4.0 years). Adverse reactions to delayed-release mesalazine were observed in six patients, consisting of two with rash, one with pancreatitis, one with elevated serum level of pancreatic amylase, one with nausea, and one with abdominal bloating. None of these adverse reactions were serious.
Efficacy evaluation
The efficacy of delayed-release mesalazine was evaluated using the following indices.
- Clinical activity index (CAI): patients were assessed at months 0, 1, and 12. The CAI described by Lichtiger et al4 was used for the assessment of disease severity and efficacy. The components of the CAI include the following: bowel movement frequency (score 0–4), nocturnal diarrhea (score 0–1), blood in stool (score 0–3), fecal incontinence (score 0–1), use of antidiarrheal drugs (score 0–1), abdominal pain (score 0–3), general well-being (score 0–5), and abdominal tenderness (score 0–3). The sum of the score for each variable ranges from 0 to 21.4
- Endoscopic index (EI): in the 72 patients who underwent total colonoscopy before and after the start of delayed-release mesalazine treatment, the endoscopic findings were scored by the EI described by Rachmilewitz,5 for endoscopic assessment of the treatment efficacy. The first colonoscopy was performed 3 months to 2 years after the start of delayed-release mesalazine treatment. The interval between the start of delayed-release mesalazine treatment and undergoing follow-up colonoscopy was 1.0±0.4 years (0.3–1.9 years).
The four Rachmilewitz score items were included: granulation scattering reflected light (score 0–2), vascular pattern (score 0–2), vulnerability of mucosa (score 0–4), and mucosal damage (mucus, fibrin, exudates, erosions, and ulcers, score 0–4). The sum of the score for each endoscopic variable ranges from 0 to 12.5 The scores for each patient were determined by assessment of the areas showing the most severe inflammation.
UC was diagnosed based on the characteristic endoscopic and biopsy findings, after excluding other inflammatory bowel disorders. Steroid dependence was defined as recurrence developing during tapering or within a short time after discontinuation of the steroid dose, and steroid resistance was defined as no response to prednisolone administered at the dose of 1–1.5 mg/kg/day for 1–2 weeks.
Ethical consideration
This study was approved by The Etiological Study Ethical Review Board of Saitama Medical Center, Jichi Medical University. Because we produced anonymized data and used them, informed consent from all study subjects was not needed.
Statistical analysis
Data are expressed as mean ± standard deviation or percentage. Statistical analysis was performed using the Student’s t-test or one-way analysis of variance (ANOVA) with post hoc Turkey–Kramer tests. All data analyses were performed with the StatView software (version 5.0; SAS Institute Inc., Cary, NC, USA). Differences at P-values of less than 0.05 were regarded as significant.
Results
Table 1 shows the characteristics of patients. In the 104 patients, the distribution of the age at onset of UC showed a peak in their 20s, consistent with the tendency observed in a survey carried out in Japan. During the follow-up period, UC aggravation occurred in 23.1% (24/104) of patients and 10.6% (11/104) were hospitalized due to aggravation of UC. One patient developed colorectal cancer and two patients underwent colectomy (Table 1).
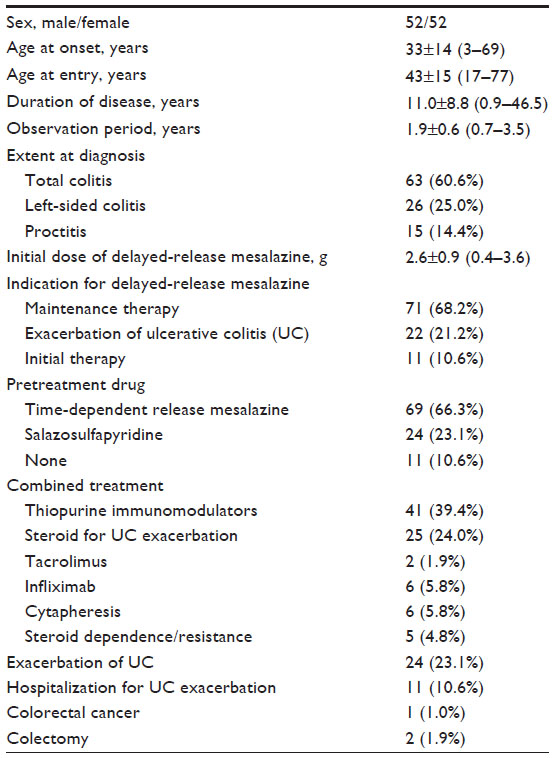 | Table 1 Clinical characteristics and outcomes |
The CAI at months 0, 1, and 12 were 4.6±2.8 (range: 1–12), 3.4±1.8 (2–13), and 2.8±1.4 (1–10), respectively, decreasing significantly with time (P<0.001). The EI decreased significantly from 4.5±3.2 (range: 0–10) before the start of delayed-release mesalazine treatment to 3.1±2.8 (0–10) after the start of treatment with the drug (P<0.001) (Figure 1A). Further analysis was performed after excluding patients who had undergone some additional treatment for UC after the start of delayed-release mesalazine treatment. Under this condition, 69 patients were eligible for assessment of the CAI. Their CAI at months 0, 1, and 12 was 4.1±2.5 (range: 1–12), 3.0±1.3 (2–7) and 2.6±0.9 (1–6), respectively, decreasing significantly with time (P<0.001). The EI was assessed in 49 patients and showed a significant decrease from 4.4±3.6 (range: 0–10) before the start to 2.5±2.5 (0–8) after the start of treatment with the drug (P<0.001) (Figure 1B).
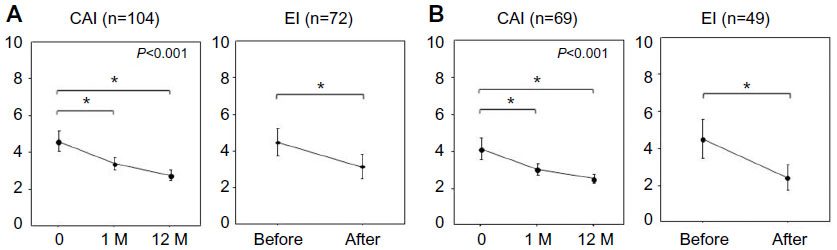 | Figure 1 Transitional change of CAI and EI. |
Stratified analyses were performed to assess the clinical effects of delayed-release mesalazine based on the CAI. The analysis by the lesion extent revealed significant decrease of the CAI after the start of delayed-release mesalazine treatment in patients with all the disease types; especially in patients with left-sided colitis and proctitis, the effects of delayed-release mesalazine were observed within 1 month. The analysis by the indications for delayed-release mesalazine treatment revealed significant decrease of the CAI after the start of delayed-release mesalazine treatment in patients who received delayed-release mesalazine for maintenance therapy, aggravation of UC, and initial therapy, and the analysis by the previously used drug for treatment also revealed significant decreases in the CAI after the start of delayed-release mesalazine treatment in both patients who had received time-dependent release mesalazine and those who had had received SASP (Figure 2). In regard to the blood test findings, the white blood cell counts and platelet counts decreased significantly after the start of delayed-release mesalazine treatment (Figure 3).
 | Figure 2 Transitional change of CAI: clinical efficacy of delayed-release mesalazine with stratified analysis. |
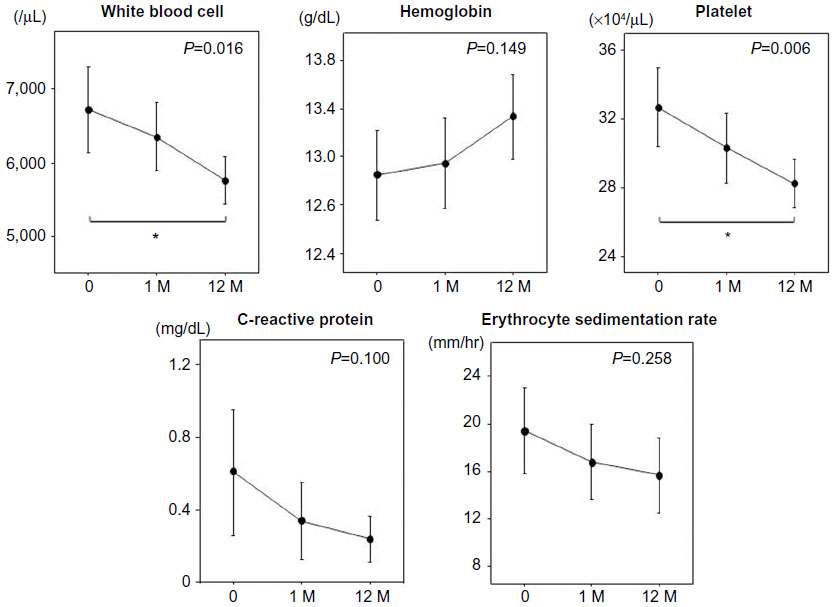 | Figure 3 Transitional change of hematological examinations. |
Discussion
According to a report by D’Inca et al, when a pH-dependent releasing preparation (2.4 g/day) or time-dependent releasing preparation (3 g/day) was administered to patients with inflammatory bowel disease, the concentration of mesalazine in the sigmoid colonic mucosa was higher in the patients receiving the pH-dependent releasing preparation.2 The efficacy of delayed-release mesalazine has been demonstrated for all disease types in clinical studies conducted in Japan, in which the decrease of the Ulcerative Colitis-Disease Activity Index score at the last assessment was more pronounced in the patients with the total colitis type of UC. The European Crohn’s and Colitis Organization does not recommend oral mesalazine alone but topical mesalazine for proctitis.6 A double-blind study on active UC comparing delayed-release mesalazine (2.4 g/day and 3.6 g/day), time-dependent release mesalazine (2.25 g/day), and placebo has also been conducted in Japan. An analysis in patients with proctitis-type UC revealed that delayed-release mesalazine administration at either dose significantly decreased the Ulcerative Colitis-Disease Activity Index as compared to placebo, whereas no significant difference was observed between patients treated with time-dependent release mesalazine and placebo.7 In the present study, delayed-release mesalazine was found to be effective for all the disease types of UC. Because its effects were observed within a month, especially in patients with left-sided colitis and proctitis, delayed-release mesalazine is assumed to be potent especially against distal-type UC. Moreover, the effects of delayed-release mesalazine were also confirmed in patients who were switched from not only time-dependent release mesalazine, but also SASP. Furthermore, the analysis performed after excluding patients who had undergone some additional treatment for UC after the start of delayed-release mesalazine treatment also revealed significant decreases of both the CAI and EI. This result may indicate the therapeutic effects of delayed-release mesalazine alone.
In this study, even after the start of treatment with delayed-release mesalazine or treatment switch from other drugs to delayed-release mesalazine, aggravation of UC and the need for the use of steroids were observed in approximately 20% of all patients. Furthermore, maintenance treatment needed to be augmented by immunomodulatory drugs and infliximab in 7% of all patients. When remission cannot be achieved by oral administration of a sufficient dose of 5-ASA, concomitant transanal administration of 5-ASA may be useful for improving the remission rate.8,9 Administration of 5-ASA preparations in the remission maintenance phase is important for preventing not only relapse, but also preventing cancer caused by UC.10,11 For long-term remission maintenance, once-daily administration is preferable.12 Furthermore, the effect of 5-ASA on inducing remission is dependent on the intramucosal concentrations of 5-ASA, and the effects of oral 5-ASA preparations are dose-dependent.3,13 Thus, it seems to be preferable to start administration of 5-ASA at high doses.
In this study, although adverse reactions to delayed-release mesalazine were observed in 5.5% (6/110) of patients, neither serious adverse events nor allergic reactions to 5-ASA were observed. Because allergic reactions to 5-ASA include diarrhea and fever which are often difficult to distinguish from the symptoms of UC, it is not uncommon for allergic reactions to be diagnosed as refractory UC. After oral administration of 5-ASA, the allergic reactions to the drug are temporarily relieved, and approximately 2 weeks later, often manifest as fever and increased stool frequency accompanied by increased serum levels of C-reactive protein (CRP). Because the therapeutic strategy for the allergic reactions differs greatly from that for UC, sufficient attention should be paid to the occurrence of allergic reactions.
This study had several limitations. First, it was a single-center retrospective cohort study; thus, we could not control all confounding factors in the analysis. Second, the time of colonoscopy before and after the start of delayed-release mesalazine treatment varied among the patients.
In conclusion, delayed-release mesalazine is effective for all types of UC and can be positioned as a key drug for the treatment of UC. However, maintenance therapy with 5-ASA alone is limited in efficacy. It is necessary to identify patients unresponsive to the drug in the early stages of treatment and to augment the maintenance therapy.
Disclosure
The authors declare that they have no conflicts of interest to disclose.
References
Bantel H, Berg C, Vieth M, Stolte M, Kruis W, Schulze-Osthoff K. Mesalazine inhibits activation of transcription factor NF-kappaB in inflamed mucosa of patients with ulcerative colitis. Am J Gastroenterol. 2000;95(12):3452–3457. | |
D’Incà R, Paccagne M, Cardin R, et al. 5-ASA colonic mucosal concentrations resulting from different pharmaceutical formulations in ulcerative colitis. World J Gastroenterol. 2013;19(34):5665–5670. | |
De Vos M, Verdievel H, Schoonjans R, Praet M, Bogaert M, Barbier F. Concentrations of 5-ASA and Ac-5-ASA in human ileocolonic biopsy homogenates after oral 5-ASA preparations. Gut. 1992; 33(10):1338–1342. | |
Lichtiger S, Present DH, Kornbluth A, et al. Cyclosporine in severe ulcerative colitis refractory to steroid therapy. N Engl J Med. 1994; 330(26):1841–1845. | |
Rachmilewitz D. Coated mesalazine (5-aminosalicylic acid) versus sulphasalazine in the treatment of active ulcerative colitis: a randomised trial. BMJ. 1989;298(6666):82–86. | |
Dignass A, Lindsay JO, Sturm A, et al. Second European evidence-based consensus on the diagnosis and managementof ulcerative colitis part 2: current management. J Crohns Colitis. 2012;6(10):991–1030. | |
Ito H, Iida M, Matsumoto T, et al. Direct comparison of two different mesalamine formulations for the induction of remission in patients with ulcerative colitis: a double-blind, randomized study. Inflamm Bowel Dis. 2010;16(9):1567–1574. | |
Ford AC, Khan KJ, Achkar JP, Moayyedi P. Efficacy of oral vs topical, or combined oral and topical 5-aminosalicylates, in ulcerative colitis: systematic review and meta-analysis. Am J Gastroenterol. 2012;107(2):167–176. | |
Meucci G, Fasoli R, Saibeni S, et al. Prognostic significance of endoscopic remission in patients with active ulcerative colitis treated with oral and topical mesalazine: a prospective, multicenter study. Inflamm Bowel Dis. 2012;18(6):1006–1010. | |
Velayos FS, Terdiman JP, Walsh JM. Effect of 5-aminosalicylate use on colorectal cancer and dysplasia risk: a systematic review and metaanalysis of observational studies. Am J Gastroenterol. 2005;100(6):1345–1353. | |
Bernstein CN, Nugent Z, Blanchard JF. 5-aminosalicylate is not chemoprophylactic for colorectal cancer in IBD: a population based study. Am J Gastroenterol. 2011;106(4):731–736. | |
Ford AC, Khan KJ, Sandborn WJ, Kane SV, Moayyedi P. Once-daily dosing vs conventional dosing schedule of mesalamine and relapse of quiescent ulcerative colitis: systematic review and meta-analysis. Am J Gastroenterol. 2011;106(12):2070–2077. | |
Naganuma M, Iwao Y, Ogata H, et al. Measurement of colonic mucosal concentrations of 5-aminosalicylic acid is useful for estimating its therapeutic efficacy in distal ulcerative colitis: comparison of orally administered mesalamine and sulfasalazine. Inflamm Bowel Dis. 2001;7(3):221–225. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.