Back to Journals » International Journal of Women's Health » Volume 17
Efficacy of a King’s Goal Attainment Theory-Based Support Model on Breastfeeding Outcomes in Women with Gestational Diabetes Mellitus: A Quasi-Experimental Study
Received 28 July 2025
Accepted for publication 26 September 2025
Published 8 November 2025 Volume 2025:17 Pages 4323—4330
DOI https://doi.org/10.2147/IJWH.S556749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Yuexia Liu,1 Yin Ying,2 Xianling Zou1
1Integrated Obstetrics District 3, Hangzhou Women’s Hospital (Hangzhou Maternity and Child Health Care Hospital), Hangzhou, Zhejiang, 310000, People’s Republic of China; 2Nursing Department, Hangzhou Women’s Hospital (Hangzhou Maternity and Child Health Care Hospital), Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Xianling Zou, Email [email protected]
Objective: To evaluate the effectiveness of a breastfeeding support model based on King’s Goal Attainment Theory in improving breastfeeding outcomes and metabolic health among women with gestational diabetes mellitus (GDM).
Methods: A retrospective cohort study was conducted involving 120 women with GDM who delivered at a tertiary hospital between March 2022 and March 2024. Participants were divided into two groups based on the type of care received: the study group (n = 60) received a structured, theory-based breastfeeding support intervention involving goal negotiation, dynamic assessment, and interactive feedback delivered by a multidisciplinary team; the control group (n = 60) received routine breastfeeding support. Primary outcome was continued breastfeeding rate at 6 weeks, 3 months, and 6 months postpartum. Secondary outcomes included breastfeeding self-efficacy (BSES-SF), glycemic control (FPG and HbA1c), and incidence of neonatal hypoglycemia. Statistical analyses included t-tests, χ²-tests, and generalized estimating equations (GEE).
Results: The study group showed significantly higher continued breastfeeding rates at all time points: 80.0% vs 58.3% at 6 weeks (p = 0.010), 73.3% vs 46.7% at 3 months (p = 0.003), and 65.0% vs 36.7% at 6 months (p = 0.002). At 6 weeks postpartum, the study group also had higher breastfeeding self-efficacy scores (62.50 ± 5.31 vs 53.11 ± 6.82, p < 0.001) and better glycemic control, with higher proportions achieving target FPG (75.0% vs 51.7%, p = 0.008) and HbA1c (80.0% vs 60.0%, p = 0.017). The incidence of neonatal hypoglycemia was significantly lower in the study group (8.33% vs 21.67%, p = 0.041).
Conclusion: The breastfeeding support model based on King’s Goal Attainment Theory was associated with significantly improved breastfeeding rates, self-efficacy, glycemic control, and neonatal outcomes in women with GDM. This theory-driven, multidisciplinary approach shows promise for enhancing perinatal care in this high-risk population.
Keywords: goal attainment theory, gestational diabetes mellitus, breastfeeding, self-efficacy, intervention study
Introduction
Gestational diabetes mellitus (GDM) is a common metabolic disorder during pregnancy, with a globally increasing prevalence that poses significant health risks to both mothers and offspring.1 Women with GDM have a markedly elevated risk of developing type 2 diabetes and are more likely to experience adverse perinatal outcomes.2 Breastfeeding has been recognized as an effective strategy to improve metabolic health in this population, associated with reduced maternal glucose intolerance and improved infant nutrition.3 However, women with GDM consistently demonstrate lower breastfeeding rates and earlier cessation compared to those without GDM, underscoring a critical gap in postnatal support.4
The challenges to breastfeeding in women with GDM are multifactorial, involving physiological barriers such as delayed lactogenesis, psychological factors including reduced self-efficacy and higher rates of postpartum depression, and structural limitations in healthcare support.5–7 Conventional educational interventions often fail to facilitate sustained behavior change, as they predominantly focus on knowledge dissemination rather than addressing individualized barriers and promoting actionable goals.8,9 There is a growing consensus on the need for theory-driven, personalized approaches to support breastfeeding in this vulnerable group.
King’s Goal Attainment Theory provides a structured framework for fostering collaborative goal-setting and sustained behavioral change through dynamic nurse-patient interactions.10 Central to this theory is the process of mutual negotiation, where patients and providers jointly establish meaningful and achievable health goals. The theory has demonstrated efficacy in improving self-management in chronic conditions such as type 2 diabetes,11 yet its application within perinatal contexts—particularly for breastfeeding promotion in GDM—remains limited. This represents a significant research gap, given the potential for theory-based interventions to address the complex interplay of metabolic and behavioral factors in GDM.12
In this study, we developed a tailored breastfeeding support model based on King’s Goal Attainment Theory, designed to enhance self-efficacy and sustain breastfeeding behavior among women with GDM. The intervention emphasizes shared decision-making, continuous assessment, and adaptive feedback mechanisms. We hypothesized that this theory-informed approach would improve breastfeeding outcomes, glycemic control, and psychosocial well-being in women with GDM compared to standard care.
Materials and Methods
Participants
This retrospective cohort study analyzed the medical records of women with GDM who delivered at a tertiary care hospital between March 2022 and March 2024. Based on the type of breastfeeding support intervention they received during their hospitalization, participants admitted from March 2022 to March 2023 were assigned to the study group (n = 60), which received a breastfeeding support model constructed based on King’s Goal Attainment Theory. Those admitted between April 2023 and March 2024 were assigned to the control group (n = 60), which received routine breastfeeding support.
A post-hoc power analysis was conducted to estimate the statistical power. Based on the 6-month exclusive breastfeeding rate of 46.7% reported in a meta-analysis by Finkelstein et al13 and using the observed rate of 65% in the study group as the expected effect size, a power analysis was performed with α = 0.05 (two-sided) and β = 0.20 (power = 80%) using G*Power 3.1. The calculation indicated that a minimum of 58 participants per group was required to detect such a difference. The final sample size of 120 participants (60 per group) in this study was sufficient to meet this requirement and enhance statistical power.
Inclusion and Exclusion Criteria
Inclusion Criteria
- Singleton pregnancy diagnosed with GDM according to IADPSG criteria;
- Enrolled between 28 and 34 gestational weeks;
- Planned to deliver at the study hospital and complete postpartum follow-up.
Exclusion Criteria
- Comorbid thyroid dysfunction or polycystic ovary syndrome;
- Use of lactation-affecting medications (eg, dopamine receptor agonists);
- Neonatal admission to the NICU >72 hours.
Study Design
Control Group
Participants in the control group received routine obstetric breastfeeding support. At 28 weeks gestation, they were given the 2021 edition of the Breastfeeding Guide for Women with GDM and attended a one-time group health education session (45 minutes) covering breastfeeding techniques and lactation physiology. During hospitalization, bedside breastfeeding instruction was provided daily by a staff nurse. Upon discharge, a 24-hour breastfeeding support hotline was made available.
Study Group
The study group received a structured support program involving a multidisciplinary team (one endocrinologist, two International Board Certified Lactation Consultants [IBCLCs], and one dietitian). The intervention followed a three-phase model:
Phase 1: Goal Negotiation (Postpartum 0–24 Hours)
Participants and clinicians collaboratively set metabolic goals (fasting blood glucose ≤5.3 mmol/L by 72 hours postpartum) and behavioral goals (≥5 effective breastfeeding sessions/day within the first 48 hours, each lasting >10 minutes) using the Goal-Setting Decision Board. A co-management agreement was signed.
Phase 2: Dynamic Assessment (Postpartum Days 2–7)
Daily fingertip blood glucose monitoring, single-breast milk output measurement (Medela Symphony breast pump), and breastfeeding quality assessment (LATCH scoring system) were performed. A predefined alert system triggered IBCLC intervention when fasting glucose exceeded 5.6 mmol/L or milk output fell below 10 mL/session.
Phase 3: Interactive Feedback (Day 8 to 6 Months Postpartum)
Customized content was delivered weekly via WeChat, with a real-time “Goal Progress Dashboard”. Follow-ups occurred via phone at 14 days, 6 weeks, and 3 months. Standardized questionnaires assessed weekly breastfeeding frequency goals and barriers. Monthly online focus groups (ORID method) refined the intervention.
Outcomes and Evaluation Criteria
Primary Outcome: Continued Breastfeeding Rate
Defined per WHO 2021 criteria as exclusive (breast milk + essential supplements) or nearly exclusive (breast milk + occasional water/juice <30 mL/day) breastfeeding at 6 weeks, 3 months, and 6 months. Data collection used dual verification: 1) Photo-logged breastfeeding diaries: Participants uploaded ≥1 daily video showing complete feeding (visible clock, infant latch); 2) 48-hour recall interviews: Standardized interviews recording all infant intake.
Inter-rater reliability was confirmed (20% video samples reviewed by two IBCLCs; κ > 0.75). Outliers (>24 feeds/day) were resolved via logic-checking.
Secondary Outcomes
Breastfeeding Self-Efficacy: Assessed using the validated Chinese BSES-SF (14 items; 5-point Likert scale; 14–70 scores; α = 0.89; Liu et al, 2020). Evaluated on postpartum day 3 (inpatient) and 6 weeks (outpatient) via the “Questionnaire Star” platform (IP logging to prevent duplication).
Glycemic Control Rate at 6 weeks: Fasting plasma glucose (FPG; target <5.3 mmol/L) and HbA1c (target <6.0%) measured via venous blood (Roche Cobas c702, Bio-Rad D-10; ISO 15189-certified labs).
Neonatal Metabolic Outcome: Hypoglycemia (≥2 heel-stick readings <2.6 mmol/L within 24 hours). Blood collected via single-use lancets (lateral heel); Abbott FreeStyle Libre meter used (calibrated per manufacturer).
Statistical Analysis
Data were analyzed using SPSS 23.0. Continuous normally distributed variables were compared using t-tests; categorical variables with χ²-tests. Generalized Estimating Equations (GEE) were used to model repeated measures of breastfeeding rates and self-efficacy scores over time, controlling for baseline differences. Adjusted odds ratios (ORs) were calculated including covariates found to be imbalanced at baseline (eg, education, parity). Both intention-to-treat (ITT) and per-protocol (PP) analyses were performed. A two-sided P-value <0.05 indicated statistical significance.
Ethical Considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Hangzhou Women’s Hospital (Approval No: 2021–02607). Informed consent was waived for this retrospective analysis. All data were anonymized and de-identified prior to analysis to ensure patient confidentiality.
Results
Baseline Characteristics
Baseline demographic and clinical characteristics were comparable between the two groups. There were no statistically significant differences in age, pre-pregnancy BMI, fasting plasma glucose at diagnosis, primiparity rate, or mode of delivery (all P > 0.05), indicating successful matching of the groups at baseline (Table 1).
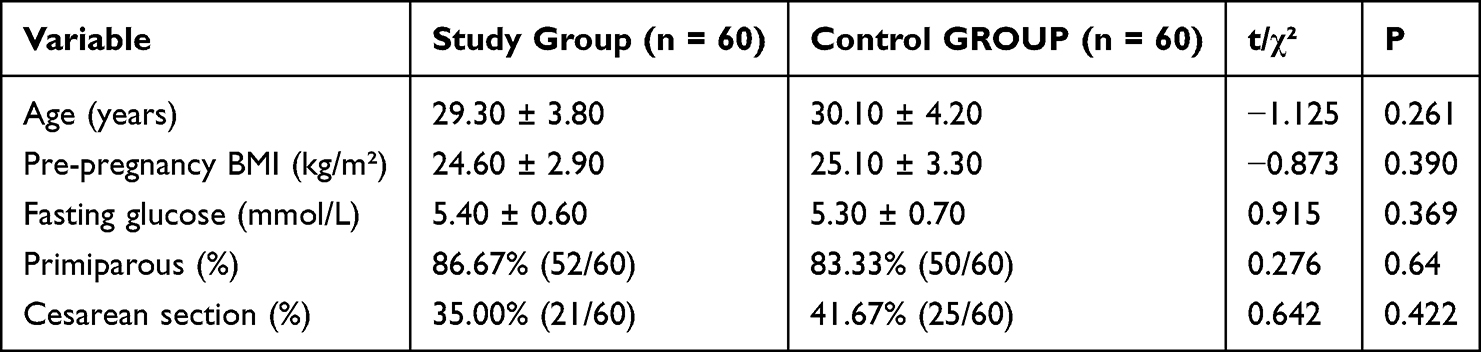 |
Table 1 Baseline Characteristics of the Study Participants |
Sustained Breastfeeding Rates
The study group demonstrated significantly higher continued breastfeeding rates at all assessed postpartum time points (Figure 1). At 6 weeks postpartum, the rate was 48 (80.0%) in the study group compared with 35 (58.3%) in the control group (χ² = 6.604, p = 0.010). This difference remained significant at 3 months (44 [73.3%] vs 28 [46.7%], χ² = 8.889, p = 0.003) and at 6 months (39 [65.0%] vs 22 [36.7%], χ² = 9.636, p = 0.002).
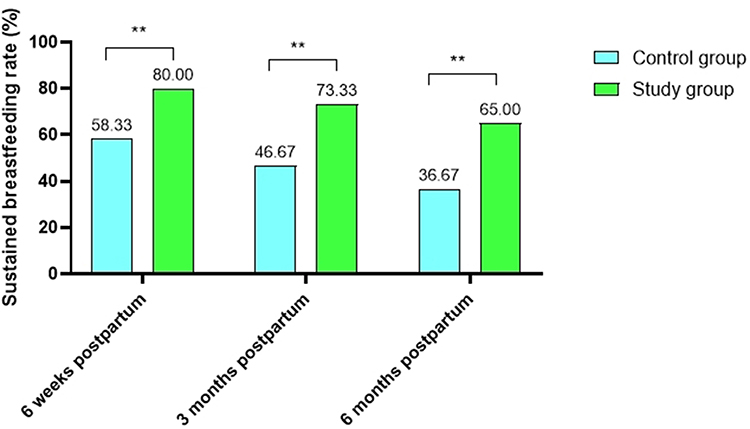 |
Figure 1 Sustained breastfeeding rates at different postpartum time points. **P < 0.05. |
Secondary Outcomes
Breastfeeding Self-Efficacy
No significant between-group difference was observed in BSES-SF scores at 3 days postpartum (48.24 ± 7.17 vs 47.86 ± 6.97, P = 0.625). However, by 6 weeks postpartum, the study group reported markedly higher self-efficacy scores compared to the control group (62.50 ± 5.31 vs 53.11 ± 6.82, P < 0.001). See Figure 2.
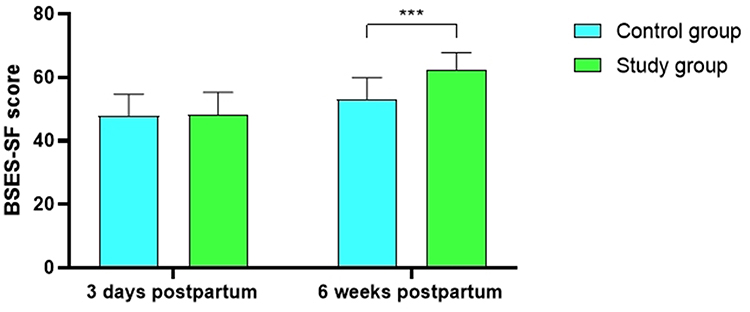 |
Figure 2 Breastfeeding self-efficacy scores at different time points. ***P < 0.001. |
Maternal Glycemic Control
At the 6-week follow-up, a significantly higher proportion of women in the study group achieved target glycemic control compared with the control group (Table 2). For fasting plasma glucose <5.3 mmol/L, the rates were 45/60 (75.00%) in the study group and 31/60 (51.67%) in the control group (p = 0.008). For HbA1c <6.0%, the corresponding rates were 48/60 (80.00%) and 36/60 (60.00%), respectively (p = 0.017).
 |
Table 2 Glycemic Control at 6 Weeks Postpartum |
Neonatal Outcomes
The incidence of neonatal hypoglycemia was significantly lower in the study group compared with the control group (5/60 [8.33%] vs 13/60 [21.67%], χ² = 4.183, p = 0.041), as shown in Table 3.
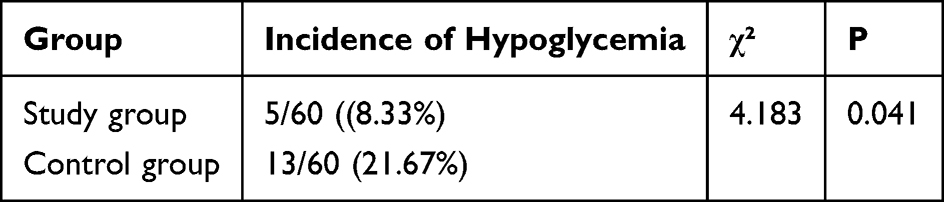 |
Table 3 Incidence of Neonatal Hypoglycemia |
Discussion
This study demonstrates that a breastfeeding support model structured around King’s Goal Attainment Theory was significantly associated with improved maternal and neonatal outcomes among women with GDM. The sustained breastfeeding rates in the intervention group were markedly higher than those in the control group at 6 weeks, 3 months, and 6 months postpartum. This improvement may be attributed to the theory-based, multilevel intervention, which integrated structured health education, ongoing psychological support, and personalized lactation guidance. The critical 6-week postpartum period was supported through dynamic assessment and timely management of breastfeeding barriers—such as latch correction and milk supply concerns—which likely contributed to the reduced early discontinuation observed.14 The notable increase in BSES-SF scores further reflects enhanced maternal confidence and self-efficacy, underscoring the importance of combining practical skills with psychological reinforcement to promote long-term breastfeeding behavior.15
A key novel aspect of this study is the application of King’s Goal Attainment Theory—a nursing theory emphasizing mutual goal-setting and iterative feedback—to the context of breastfeeding support in women with GDM, an area with limited prior evidence. The significantly higher rates of glycemic control (FPG and HbA1c) achieved in the intervention group highlight the metabolic benefits of integrating breastfeeding support with glucose management. These improvements are likely attributable to personalized dietary advice, physical activity planning, and glucose monitoring integrated within the model. The highest compliance rates at 6 weeks suggest sustained self-management behaviors initiated during the intervention period.11 These findings corroborate earlier reports indicating that breastfeeding is associated with a reduced risk of postpartum dysglycemia.16 However, unlike previous studies that focused primarily on long-term outcomes, the present model employed a multidisciplinary team (endocrinologists, IBCLCs, dietitians) to enhance short-term glycemic stability through coordinated care.17
For example, individualized meal planning and exercise guidance during the initial intervention phase helped improve fasting glucose levels. Subsequent real-time monitoring with predefined alert thresholds—such as triggering IBCLC support when milk output fell below 10 mL—may have reduced glycemic fluctuations more effectively than standard care.18 Emerging metabolomic evidence10 suggests that frequent breastfeeding modulates lipid metabolism, particularly triacylglycerol (TAG) and diacylglycerol (DAG) pathways. In this study, the protocol encouraging frequent breastfeeding (≥5 sessions daily within 48 hours postpartum) and continuous lactation monitoring may have potentiated insulin sensitivity, thereby supporting glycemic regulation.19
The significantly lower incidence of neonatal hypoglycemia in the intervention group further supports the clinical utility of this model. This is consistent with previous studies20 in which structured glucose surveillance and supplemental feeding protocols shortened recovery time from neonatal hypoglycemia. In our intervention, daily glucose monitoring combined with milk volume assessment during the first postpartum week—coupled with timely initiation of breastfeeding—likely promoted metabolic stability in neonates.21 Although the study did not directly address gestational weight management, the comprehensive metabolic approach may have indirectly optimized neonatal outcomes by improving intrauterine and postpartum metabolic milieu.22
Practical and Policy Implications
The findings offer several important implications for clinical practice and public health. The theory-based, digitally-assisted model presented here is scalable and can be integrated into existing maternal care programs, including Baby-Friendly Hospital Initiative (BFHI) guidelines and postpartum glycemic management protocols. The use of mobile health platforms for dynamic feedback and monitoring improves accessibility and allows for individualized support even in low-resource settings. However, sustainability may require training for multidisciplinary providers and securing institutional support for role expansion among nurses and lactation consultants. Future implementation should emphasize cultural adaptability and consider hybrid models combining digital tools with in-person consultations to broaden reach across diverse socioeconomic contexts.
Limitations
Several limitations must be considered when interpreting the findings of this study. First, as a retrospective analysis of medical records, the study is subject to inherent biases related to non-randomized data collection, and unmeasured confounders—such as socioeconomic status, social support, and lifestyle factors—may have influenced the outcomes. Second, all participants were recruited from a single center, which may limit the generalizability of the results to other populations or healthcare settings. Third, the 6-month follow-up period did not allow for the assessment of long-term metabolic outcomes, such as the incidence of type 2 diabetes. Finally, although breastfeeding outcomes were verified using a combination of maternal logs and recall interviews, the possibility of reporting bias cannot be entirely excluded. Future research should prioritize prospective, multicenter designs with longer follow-up durations, incorporate objective biomarkers, and evaluate the cost-effectiveness of the intervention to support broader implementation.
Conclusion
This retrospective study suggests that a breastfeeding support model structured around King’s Goal Attainment Theory—incorporating collaborative goal-setting, dynamic assessment, and iterative feedback—was associated with improved breastfeeding rates, maternal glycemic control, and neonatal hypoglycemia outcomes in women with GDM. Despite the limitations inherent in the retrospective design, this patient-centered approach shows promise as a scalable framework for supporting high-risk perinatal populations. Further randomized controlled trials are necessary to establish causal relationships and assess the long-term efficacy and generalizability of the model across diverse clinical settings.
Funding
This study was supported by Zhejiang Provincial Medical and Health Science and Technology Plan Project, No.2025KY1180.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Arabiat D, Al Jabery M, Jenkins M, Kemp V, Whitehead L, Adams G. Language abilities in children born to mothers diagnosed with diabetes: a systematic review and meta-analysis. Early Human Dev. 2021;159:105420. doi:10.1016/j.earlhumdev.2021.105420
2. Stavrou E, Andriopoulou M, Charos D, Vivilaki V. Pregnancy and multiple sclerosis: a review. J Mod Nurs Pract Res. 2025;5(1):3. doi:10.53964/jmnpr.2025003
3. Shah NS, Wang MC, Freaney PM, et al. Trends in gestational diabetes at first live birth by race and ethnicity in the US, 2011-2019. JAMA. 2021;326(7):660–669. doi:10.1001/jama.2021.7217
4. Finkelstein SA, Keely EJ, Feig D, Tu X, Walker MJ. Breastfeeding in women with diabetes: lower rates despite greater rewards. Population-Based Study. 2012;36:S73.
5. Hebeisen I, Rodriguez EG, Arhab A, et al. Prospective associations between breast feeding, metabolic health, inflammation and bone density in women with prior gestational diabetes mellitus. BMJ Open Diabetes Res Care. 2024;12(3):e004117. doi:10.1136/bmjdrc-2024-004117
6. Bernier E, Plante A-S, Lemieux P, et al. Promoting healthy eating in early pregnancy in individuals at risk of gestational diabetes mellitus: does it improve glucose homeostasis? A study protocol for a randomized control trial. Front Nutrition. 2024;10:1336509. doi:10.3389/fnut.2023.1336509
7. Minschart C, De Weerdt K, Elegeert A, et al. Metabolism, Antenatal depression and risk of gestational diabetes, adverse pregnancy outcomes, and postpartum quality of life. J Clin Endocrinol Metabolism. 2021;106(8):e3110–e3124. doi:10.1210/clinem/dgab156
8. Wang H, Li N, Chivese T, et al. IDF diabetes atlas: estimation of global and regional gestational diabetes mellitus prevalence for 2021 by international association of diabetes in pregnancy study group’s criteria. Diabetes Res Clin Pract. 2022;183:109050. doi:10.1016/j.diabres.2021.109050
9. Moore LE, Voaklander B, Savu A, et al. Complications, association between the antepartum oral glucose tolerance test and the risk of future diabetes mellitus among women with gestational diabetes: a systematic review and meta-analysis. J Diabetes Complications. 2021;35(4):107804. doi:10.1016/j.jdiacomp.2020.107804
10. Colandro A. Does tight glucose control reduce maternal and neonatal complications in women with gestational diabetes mellitus. 2023.
11. Lin C, Lin H, Xu Y, Guan Q, Su B, Ge L. Applying king’s theory of goal attainment combined with FMEA-PDCA quality management tool in gestational diabetes mellitus health education: a randomized controlled trial. 2024.
12. Noroozi F, Dehghan A, Bijani M, Nikrouz LJ. Effects of nurse-led intervention programs based on King’s theory of goal attainment on health-promoting behaviors and life satisfaction in patients with type 2 diabetes: a randomized controlled clinical trial. BMC Nursing. 2024;23:684.
13. Behnam S, Timmesfeld N, Arabin BJ. Lifestyle interventions to improve pregnancy outcomes: a systematic review and specified meta-analyses. Geburtshilfe und Frauenheilkunde. 2022;82:1249–1264.
14. Regan MJ, Zvenyach T, Zhu S. Proportional contribution of the women, infant and children’s special supplemental nutrition program on pregnant women’s diet quality. J Mod Nurs Pract Res. 2024;4(4):19. doi:10.53964/jmnpr.2024019
15. Veness SJ. An exploration of western Australian women’s experience of receiving a diagnosis of polycystic ovary syndrome. Curtin University; 2024.
16. Asriadi A, Yetti K, Novieastari E, Gayatri DJF. Development of an educational model with a management approach to improve the competency of diabetes educator nurses; utilizing King’s conceptual framework and goal attainment theory. F1000Research. 2024;13:1018.
17. Yang H, Luo W, Du X, Guan Y, Peng WJM. The implementation and effect evaluation of AIDET standard communication health education mode under the King theory of goal attainment: a randomized control study. Medicine. 2023;102(48):e36083. doi:10.1097/MD.0000000000036083
18. Hashmi IA, Yazidi BA, Al Omari OJ. Translation and psychometric validation of the Arabic gestational diabetes management self-efficacy scale (GDMSES). J Healthcare Quality Res. 2022;37:231–238.
19. Karavasileiadou S, Almegewly W, Alanazi A, Alyami H, Chatzimichailidou SJ. Self-management and self-efficacy of women with gestational diabetes mellitus: a systematic review. Global Health Action. 2022;15(1):2087298. doi:10.1080/16549716.2022.2087298
20. El-Nagar AE, Ahmed MH, Abo-Freikha A, El Welely MZ. Effect of implementation of health educational guidelines on maternal and neonatal outcomes among women with gestational diabetes mellitus. Tanta Scientific Nursing J. 2019;17:148–182.
21. Icard J. Increasing patient compliance with the recommended plan of care for pregnant women with gestational or type 2 diabetes. 2022.
22. Al Hashmi IH. The effectiveness of a health education intervention on self-efficacy for adherence to healthy behaviors among women with gestational diabetes. University of California Los Angeles Los Angeles, CA, USA; 2017.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Breastfeeding Self-Efficacy in Hangzhou Community-Dwelling Mothers During the First 6 Months Postpartum: A Life Course Exploration of Influences
Shen Y, Li Y, Qiu R, Chen Y, Chen X
International Journal of Women's Health 2025, 17:4359-4367
Published Date: 11 November 2025