Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 7
Efficacy and safety of ustekinumab in adolescents
Authors Kellen R, Silverberg N ![]() , Lebwohl M
, Lebwohl M
Received 15 October 2015
Accepted for publication 28 January 2016
Published 19 September 2016 Volume 2016:7 Pages 109—120
DOI https://doi.org/10.2147/PHMT.S75836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Laurens Holmes, Jr
Roselyn Kellen,1 Nanette B Silverberg,2,3 Mark Lebwohl1
1Department of Dermatology, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 2Department of Dermatology, Mount Sinai St Luke’s-Roosevelt Hospital, New York, NY, USA; 3Beth Israel Medical Centers, New York, NY, USA
Abstract: The biologic agent ustekinumab is a human monoclonal antibody that binds to the p40 subunit shared by interleukins (ILs) 12 and 23. The antibody is able to prevent binding of cytokines to the IL-12Rβ1 cell surface receptor and therefore may prevent IL-23 driven activation of the IL-23/Th 17 axis of inflammation. The anti-inflammatory activity has been beneficial in adult psoriasis. Ustekinumab has been approved in the United States for the treatment of adults with psoriasis and psoriatic arthritis. Approval in children and adolescents has not been granted by the US Food and Drug Administration. Subcutaneous injections of ustekinumab are administered at baseline, week 4 and every 12 weeks thereafter, a regimen that is particularly appealing to young patients who do not like more frequent injections at home. The product is attractive because, although it works through an immune system mechanism, the selective activity is such that the drug has not been associated with many of the side effects attributed to other immunosuppressive medications. Case reports of ustekinumab for pediatric psoriasis have shown promising results, and the recent Phase III CADMUS trial tested the agent in adolescents aged 12–17 years with psoriasis, using standard dose 0.75 mg/kg (≤60 kg), 45 mg (>60–≤100 kg), and 90 mg (>100 kg) or half-standard dosing 0.375 mg/kg (≤60 kg), 22.5 mg (>60–≤100 kg), and 45 mg (>100 kg) with a loading dosage at week 0 and week 4. Psoriasis area and severity index-75 was achieved in more than three-quarters of patients in full and half dosing by 12 weeks, and psoriasis area and severity index-90 in 54.1% and 61.1% of half and full dosage by 12 weeks, respectively. Ustekinumab was generally well tolerated in adolescents, with some patients developing antibodies, and nasopharyngitis being the major adverse event. Ustekinumab is a promising agent in adolescent psoriasis that appears to be well tolerated. The best monitoring plan and usage in younger patients still remain to be defined.
Keywords: pediatric psoriasis, ustekinumab, IL-12, IL-23, TNF agent
Introduction
Biologic agents are being used more frequently for the treatment of chronic childhood diseases. They require less-frequent monitoring and offer a more convenient dosing schedule – two considerations that become even more important when dealing with a pediatric population. In addition, since these agents target specific features of the inflammatory pathways, they are likely not as toxic as other systemic agents, which is important for the management of chronic diseases.1,2 Here we will review the efficacy and safety of ustekinumab for chronic childhood diseases with a focus on pediatric psoriasis, for which we have the most data. We will incorporate data from clinical trials in adult patients and the usage of ustekinumab for other chronic childhood diseases.
Psoriasis: epidemiology and clinical presentation
Psoriasis vulgaris is a chronic skin disease with a worldwide prevalence ranging from 1% to 3%.3 Raychaudhuri and Gross4 sent questionnaires to 707 patients with psoriasis and found that 31.5% reported disease onset in childhood, which their study defined as onset of psoriasis on or before the age of 16. The mean age at diagnosis varies among studies; in addition, children and adolescents are sometimes divided up into separate groups.5 Nonetheless, females and those with a family history appear to be diagnosed at a younger age.5 There is data arguing that the annual incidence of pediatric psoriasis has more than doubled from 1970 (29.6 cases per 100,000) to 2000 (62.7 cases per 100,000), and further, that it increases with age.6 The incidence of each type of psoriasis varies between studies. In 2012, Kwon et al7 analyzed the records of 358 pediatric patients with psoriasis and found that plaque psoriasis was the most common phenotype, affecting 67.3% of their cases. The next most common types were guttate psoriasis (13.5%–27.6%) and generalized pustular psoriasis (4.8%–11.6%).7 Unlike adult plaque psoriasis, the plaques in children are thinner, smaller, and tend to have less scales.5,8 The most commonly affected areas in children are the extensor surfaces of the knees and elbows, scalp, face, trunk, and posterior auricular regions.5 A diaper rash is the most common presentation in infants and toddlers below the age of 2.5
There are several aspects of psoriasis that, although not unique to the pediatric population, are of special concern. Psoriasis can be very disfiguring, especially because the affected areas are often exposed, causing children to suffer from significant psychological and emotional distress. Those who suffer from psoriatic arthritis can also experience debilitating disease that impairs daily activities. It is imperative to quickly gain control of flare-ups and establish a reliable maintenance regimen. This requires that patients have regular contact with their dermatologist/pediatric dermatologist, which can pose both financial and logistical challenges for many families. Several of the treatment options for severe disease require frequent doctor visits, resulting in missed school days and parents needing to take time off from work.
Psoriasis: pathogenesis
The cause of psoriasis is multifactorial. Histological examination of psoriatic cells points to the involvement of both the innate and adaptive immune systems.9 The dermis and epidermis exhibit an inflammatory infiltrate of T-lymphocytes, macrophages, neutrophils, and mast cells.9 The end result is epidermal acanthosis, hyperkeratosis, parakeratosis, as well as exaggeration of the rete ridges.9
Two of the key mediators involved in the excessive proliferation of the epidermis appear to be T-helper (Th)1 cells and T-cells that express interleukin-17 (IL-17), so called Th17 cells.10 Th1 cells release cytokines such as interferon-γ (IFN-γ), tumor necrosis factor-α (TNF-α), IL-2, and IL-12.10 Dendritic cells and macrophages produce IL-23, which activates Th17 cells.10 Th17 cells produce IL-17, which leads to the production of other inflammatory cytokines by endothelial cells and macrophages, and the production of interleukins by keratinocytes.10 It is thought that IFN-γ from the Th1 cells stimulates macrophages to release IL-23, which acts in combination with IL-1 to support the population of T-cells that express IL-17 and IL-22.10,11
There is substantial evidence that psoriasis also has a genetic component. The strongest link to date is the region psoriasis susceptibility 1 on chromosome 6p21, located within the major histocompatibility complex, a region that contains various genes involved in the immune response.11 Genome-wide association studies have analyzed this region and identified associations with various genes including human leukocyte antigen (HLA-C), three genes involved in IL-23 signaling (IL-23A, IL-23R, and IL-12B), two genes involved in TNF-α signaling (TNF-α-induced protein 3: TNAIP3 and TNFAIP3 interacting protein 1: TNIP1), and two genes involved in the Th2 pathway (IL-4 and IL-13).11,12 Lastly, twin studies also show higher concordance in monozygotic twins compared to dizygotic twins.13
Various environmental triggers have been associated with psoriasis, including streptococcal infections (particularly for the guttate form of psoriasis), stress, HIV infection, humidity, drugs, trauma, smoking, and obesity.14 Obesity (as manifested with high body mass index [BMI] and waist circumference) in particular deserves special mention in association with pediatric psoriasis. Children, like adults with psoriasis, appear to be at an increased risk of developing obesity and other components of the metabolic syndrome.15 In addition, several large studies have shown an association between increasing BMI and the severity of psoriasis.16 Paller et al17 studied 409 children with psoriasis and found that the odds ratio of obesity (defined by BMI ≥95%) was 4.29 for children with psoriasis compared with controls. The odds ratio for having a waist circumference above the 90th percentile was 2.52 for children with psoriasis compared with controls.17
The association between obesity and inflammation is well established. Adipose tissue is very active in secreting adipocyte-derived cytokines and other inflammatory mediators.15,16 For example, leptin promotes production of TNF-α and IL-6, favors Th1 cell differentiation, and stimulates proliferation of keratinocytes.18 Furthermore, there is increasing evidence that psoriasis is associated with a state of systemic inflammation that is, unfortunately, not limited to the skin.15 Such a state might contribute to insulin resistance and endothelial cell dysfunction, which in the long term could contribute to atherosclerosis.15
Psoriasis: the role of biologic agents
Kim et al19 compared the efficacies of commonly used biologics in adult patients – infliximab, ustekinumab, adalimumab, etanercept, and alefacept – and found psoriasis area and severity index (PASI)-75 to be 78.6%, 72.1%, 70.5%, 48.1%, and 21%, respectively after 12 weeks. Fortunately, most children with psoriasis have mild disease that can be managed with topical therapies. However, those with moderate-to-severe disease may require systemic treatments, of which none are approved by the US Food and Drug Administration (FDA) for use in pediatric psoriatic patients. Thus far, the biologic agents that have been used to treat pediatric psoriasis include the TNF-α antagonists infliximab, etanercept, and adalimumab and the IL-12/IL-23 antagonist ustekinumab.2 Three of these agents – etanercept, adalimumab, and more recently ustekinumab – have been studied in randomized controlled trials with adolescent patients.20–22 Two biologic agents, etanercept and adalimumab, have been approved for the therapy of pediatric psoriasis in the European Union.
The role of TNF blockers in other chronic childhood diseases
Crohn’s disease, characterized by chronic inflammation of the gastrointestinal tract, not only impairs quality of life but also causes growth failure in many children.23 In the “bottom–up” treatment approach, children are started on “conventional therapies” such as 5-aminosalicylates, corticosteroids, and immunomodulators; infliximab and adalimumab are reserved for those with recalcitrant disease.23 There is debate in the literature about adopting a “top–down” approach in which the anti-TNF agents would be introduced sooner after diagnosis to prevent disease progression.23 Although the anti-TNF agents have had remarkable success, not every patient has a robust response, which calls into question the possible use of other biologic agents.23–25
Juvenile idiopathic arthritis (JIA) is the most common rheumatologic disease in children and often persists into adulthood.26 Treatment options include nonsteroidal anti- inflammatory drugs in combination with long-acting drugs such as sulfasalazine, methotrexate, and corticosteroids.26 Patients who do not show adequate response within 3–6 months are considered for the biological agents.26 The following biologics are approved by the FDA to treat JIA: TNF antagonists (etanercept and adalimumab), IL-1 antagonists (anakinra, canakinumab, and rilonacept), and the IL-6 antagonists (tocilizumab, abatacept, and rituximab).26 Anterior uveitis occurs in 10%–20% of patients with JIA and can be managed with topical and oral steroids, immunosuppressive drugs such as methotrexate, and antimetabolites.27 Despite the fact that no biologics are approved for the treatment of JIA-associated uveitis, the TNF antagonists have been employed to treat patients with refractory disease.27
Behçet’s disease (BD) is characterized by systemic inflammation and vasculitis, with a variable presentation and clinical course that can present in childhood.28 Because the etiology is unknown, therapeutic treatments have been guided by basic science research trying to divulge the pathogenesis of this disease.29 Similar to other inflammatory diseases, BD is thought to involve inflammatory mediators such as TNF-α, IL-1β, and IL-6.29 Genome wide association studies suggest an association between pediatric-onset BD and HLA-B51, and possibly also IL-17 and IL-23.30 As with Crohn’s disease, anti-TNF agents are effective, but not every patient shows an adequate response.29 The use of other biologic agents has been studied for this disease, including ustekinumab, though only in adult patients.29
Ustekinumab: indications and dosing recommendations
The FDA approved ustekinumab in 2009 for the treatment of moderate-to-severe plaque psoriasis in adults >18 years of age who are candidates for phototherapy or systemic therapy, and for psoriatic arthritis either as monotherapy or in combination with methotrexate.31 There is currently no approval for the use of ustekinumab in pediatric patients for any conditions in the United States or European Union. For psoriasis in adults, ustekinumab is administered as a subcutaneous injection at weeks 0, 4, and subsequently every 12 weeks with either 45 or 90 mg dosages based on weight ≤ or >100 kg, respectively.31 For the treatment of psoriatic arthritis in adults, the 45 mg dosage is used, with the same dosing frequency, unless the adult patient has coexisting moderate-to-severe plaque psoriasis.31
Ustekinumab: pretreatment screening and monitoring
Suggested screening before the use of ustekinumab in pediatric patients includes tuberculosis (TB) testing with either a purified protein derivative test or Quantiferon Gold, followed by annual TB testing and periodic full body skin examinations.2 Complete blood count and liver function testing is ideally screened and documented normal prior to drug initiation and can be repeated periodically thereafter to identify rare liver function test alterations or signs of infection. Dosages can be held for active fevers and/or infections. Patients must be closely monitored for signs of active TB or other serious infections. Patients should not receive live viral or bacterial vaccinations while taking ustekinumab.32
Ustekinumab: mechanism of action
As described earlier, IL-12 and IL-23 are two cytokines that play a role in the differentiation of Th1 and Th17 cells. IL-12 is an inflammatory cytokine involved in both the innate and adaptive immune responses.33 IL-12 is made up of two subunits connected by disulfide bonds, p35 and p40, encoded by IL12A and IL12B, respectively.34 IL-12Rβ1 and IL-12Rβ2 together form the heterodimer receptor for IL-12.35 IL-23 contains a p40 subunit that it shares with IL-12, as well as a unique p19 subunit.36 Ustekinumab is a human monoclonal antibody that binds to the p40 protein subunit shared by these two cytokines.31 Preclinical testing showed that ustekinumab interfered with the ability of these cytokines to bind their common cell surface receptor IL-12Rβ1.31
Ustekinumab: pharmacodynamics
Skin biopsies taken before and up to 2 weeks after treatment with ustekinumab in adult patients with psoriasis showed decreased expression levels of messenger RNA of both IL-12 and IL-23.31
Ustekinumab: pharmacokinetics
In patients with psoriasis, it takes 13.5 and 7 days, respectively, for the drug to reach maximum concentration in the serum after one injection of the 45 or 90 mg dosage.31 Steady-state concentrations are achieved by week 28.31 There were no changes in clearance or distribution noted when the drug was studied in patients older than 65 years of age.31 In addition, pharmacokinetic properties did not seem to be affected by simultaneous use of methotrexate, nonsteroidal anti-inflammatory drugs, oral corticosteroids, or prior use of anti-TNF-α agents in patients with psoriatic arthritis.31
Ustekinumab: efficacy
Psoriasis
Table 1 summarizes the current literature on the use of ustekinumab for psoriasis in adults and children. There is extensive data on the use of ustekinumab for the treatment of plaque psoriasis in adults.
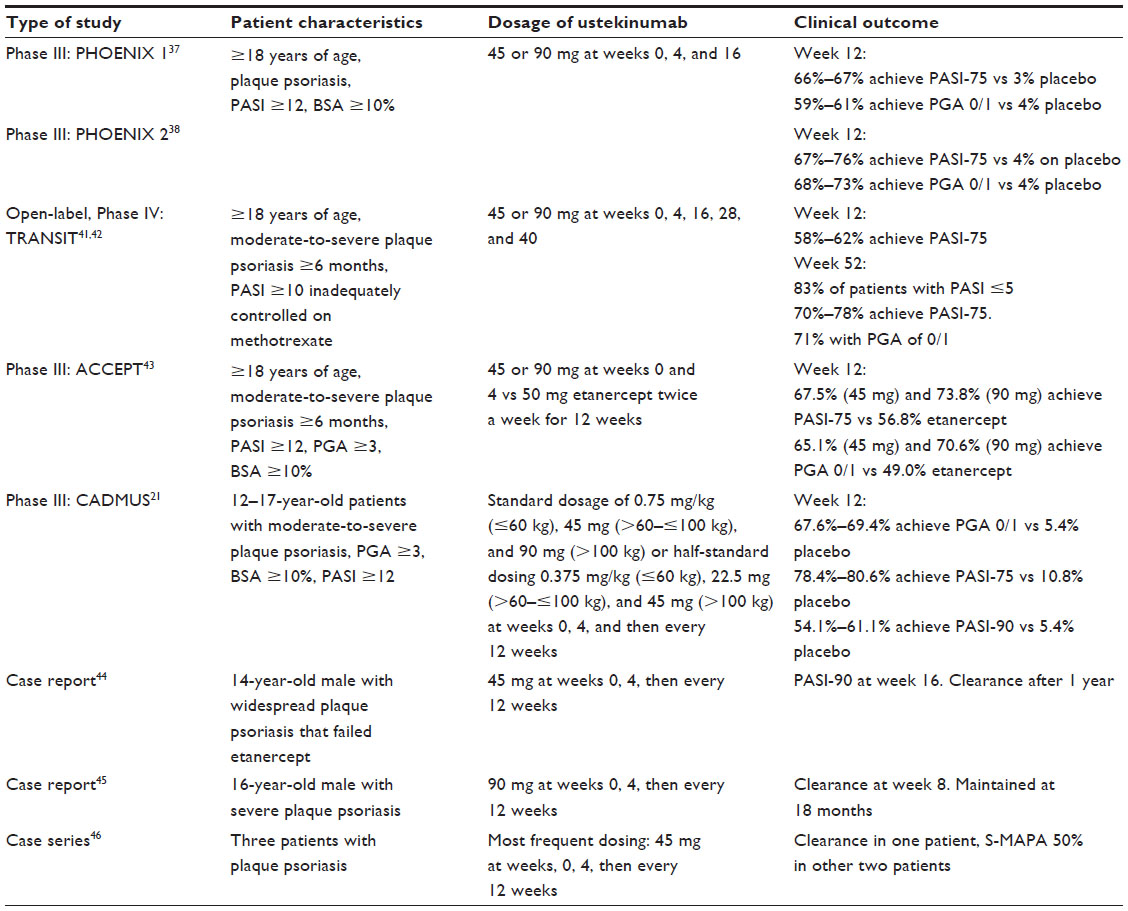 | Table 1 Ustekinumab for adult and adolescent patients with psoriasis |
Adult trials
Two multicenter, randomized, double-blind, placebo-controlled studies (PHOENIX 1 and PHOENIX 2) together enlisted 1,996 patients ≥18 years of age with plaque psoriasis, PASI ≥12, body surface area (BSA) ≥10%, and who were candidates for phototherapy or systemic therapy. Patients received either placebo or the 45 or 90 mg dosage at weeks 0, 4, and 12.37 By week 12 of PHOENIX 1, a higher percentage of patients on ustekinumab (66.4% on the 90 mg dosage and 67.1% on the 45 mg dosage) achieved PASI-75 compared to placebo (3.1%).37,38 At week 28, PASI-75 was maintained by 71.2% and 78.6% of patients on the 45 and 90 mg doses, respectively.37 By week 12 of PHOENIX 2, a higher percentage of patients on ustekinumab (75.7% on the 90 mg dosage and 66.7% on the 45 mg dosage) had achieved PASI-75 compared to placebo (3.7%).38 At week 28, PASI-75 was maintained by 69.5% and 78.5% of patients on the 45 and 90 mg doses, respectively.38
Extensive follow-up studies were conducted on the original patients enrolled in PHOENIX 1 and 2 to examine long-term efficacy as well as adverse effects (AEs). By week 244, follow-up data of PHOENIX 1 demonstrated PASI-75 of 63.4% and 72.0%, PASI-90 of 39.7% and 49.0%, and PASI-100 of 21.6% and 26.4% for patients receiving either the 45 or 90 mg doses, respectively.39 The follow-up studies on PHOENIX 2 confirmed the long-lasting efficacy of ustekinumab: 76.5% and 78.6% of patients with PASI-75, 50.0% and 55.5% with PASI-90 based on continuing the 45 or 90 mg dosage, respectively.40
Reich et al41 analyzed the TRANSIT study, a 52-week, multicenter, open-label, parallel-group, Phase IV randomized clinical trial that enlisted adults with moderate-to-severe psoriasis ≥6 months and PASI ≥10, who were inadequately controlled on methotrexate 10–25 mg weekly for at least 8 consecutive weeks. Patients were administered ustekinumab 45 or 90 mg based on weight ≤100 or >100 kg, and methotrexate was either discontinued immediately (arm 1) or gradually (arm 2).41 By week 12, the mean PASI score had decreased from a baseline of 15.2 (arm 1) and 15.4 (arm 2) to 2.9 (arm 1) and 2.8 (arm 2), respectively.42 PASI-75 was achieved by 58% of patients in arm 1 and 62% of patients in arm 2, and physician global assessment (PGA) 0/1 was achieved by 65% of patients in arm 1 and 69% of patients in arm 2.42 By week 52, 83% of patients had PASI ≤5 and 70%–78% achieved PASI-75 on the 90 and 45 mg doses, respectively.41
The ACCEPT trial enrolled 903 adult patients with moderate-to-severe plaque psoriasis to receive either 45 or 90 mg subcutaneous ustekinumab at weeks 0 and 4, or 50 mg etanercept twice a week for 12 weeks.43 At week 12, PASI-75 was achieved by 67.5% of patients receiving ustekinumab 45 mg and 73.8% of patients receiving ustekinumab 90 mg, compared to 56.8% of patients receiving etanercept (P<0.05 for both comparisons).43 At week 12, PASI-90 was achieved by more patients receiving ustekinumab 45 or 90 mg (36.4% and 44.7%, respectively) compared to those receiving etanercept (23.1%), (P<0.05 for both comparisons).43 In addition, a higher number of patents on ustekinumab 45 mg (65.1%) and ustekinumab 90 mg (70.6%) had PGA 0/1 compared to those on etanercept (49.0%), (P<0.001 for both comparisons).43
Adolescent trials
Until recently, clinical data on the use of ustekinumab for pediatric psoriasis was sparse; there were only five cases of usage reported in the literature.44–46 Three patients with plaque psoriasis were on a mean dose of 45 mg, with one patient attaining complete clearance. The other two achieved S-MAPA of 50%: the Simple-Measure for Assessing Psoriasis Activity (S-MAPA) correlates with PASI.46,47 A 16-year-old male with severe plaque psoriasis on the 90 mg dose achieved clearance at week 8, which was maintained after 18 months.45 A 14-year-old male with widespread plaque psoriasis who had failed etanercept therapy achieved PASI-90 by week 16 and clearance by 1 year on the 45 mg dose administered with standard regimen.44
A recently completed multicenter Phase III randomized, double-blind, placebo-controlled trial (CADMUS) evaluated the safety and efficacy of ustekinumab in adolescents.21 The trial enrolled 110 patients 12–17 years of age with moderate-to-severe plaque psoriasis ≥6 months, with PGA ≥3, BSA ≥10% and PASI ≥12, and who were either inadequately controlled on topical therapy or candidates for phototherapy or systemic therapy. They were administered ustekinumab at weeks 0, 4, and subsequently every 12 weeks until 40 weeks. Patients received either standard dose (SD) 0.75 mg/kg (≤60 kg), 45 mg (>60–≤100 kg), and 90 mg (>100 kg), or half-standard dosing (HSD) 0.375 mg/kg (≤60 kg), 22.5 mg (>60–≤100 kg), and 45 mg (>100 kg). The mean ages were 15.6, 15.1, and 14.8 in the placebo, HSD, and SD groups, respectively. The primary end point was PGA 0/1 by week 12. By week 12, the percentage of patients with PGA 0/1 was higher in patients treated with ustekinumab (67.6% in HSD and 69.4% in SD) compared to placebo (5.4%).21 Furthermore, one-third of the patients receiving ustekinumab reached PGA 0/1 by week 4.21 The two secondary end points were PASI-75 and PASI-90 by week 12. By week 12, a higher percentage of patients on ustekinumab achieved PASI-75 (78.4% in HSD and 80.6% in SD, compared to 10.8% in the placebo group) and PASI-90 (54.1% in HSD and 61.1% in SD, compared to 5.4% in the placebo group).21
Although objective outcomes such as PASI, PGA, and BSA are important when it comes to determining efficacy, we must also pay attention to patient-reported outcomes. The CADMUS trial tracked improvements in health-related quality of life (HRQoL) using the Children’s Dermatology Life Quality Index (CDLQI).48 At baseline, the mean CDLQI was 9.1 in the placebo group, 9.4 in the HSD group, and 10.3 in the SD group, with an overall mean of 9.6 indicating moderate-to-severe disease. At week 12, the mean reductions in severity from baseline were significantly greater in the group receiving HSD (−5.6) and SD (−6.7) compared to those receiving placebo (−1.5, P=0.03 and P<0.001, respectively). This response was still maintained by week 52, in which the mean changes were −4.9 in the HSD group and −7.6 in the SD group.
The role of ustekinumab in other chronic childhood diseases
A randomized controlled trial highlighted the benefits of intravenous ustekinumab in adult patients with moderate-to-severe Crohn’s disease refractory to TNF antagonists.49 However, Rinawi et al50 has thus far described the first and only successful use of ustekinumab for pediatric Crohn’s disease in a 7-year-old male who failed both adalimumab and infliximab. He received three subcutaneous doses of 22.5 mg ustekinumab (1.3 mg/kg) at weeks 0, 4, and 12.50 Within 8 weeks of treatment, his diarrhea and arthritis both resolved, and his Pediatric Crohn’s Disease Activity Index decreased to zero.50 One year later, he remained in remission on azathioprine, showed improvements in height and weight, and had normalization of his erythrocyte sedimentation rate and C-reactive protein.50 No AEs were reported.
To date, there is no report of the use of ustekinumab for pediatric JIA, uveitis, or BD. Of note, there is one case report of the successful use of ustekinumab for the treatment of BD in a 39-year-old woman with concurrent psoriasis and hidradenitis suppurativa.51 After a flare-up of psoriasis, she was prescribed 45 mg of subcutaneous ustekinumab at weeks 0, 4, and 12, and achieved PASI-50 in 4 weeks and PASI-75 by 3 months.51 During this time, her symptoms of hidradenitis suppurativa and BD both resolved and she remained in remission for at least 3 years.51 As stated earlier, with the possible association of IL-17 and IL-23 with pediatric-onset BD, it is possible that ustekinumab, and other biologic agents, may in the future play a role in the treatment of this poorly characterized disease.
Ustekinumab: safety
Through week 12 of the PHOENIX 1 trial in adults with psoriasis, the most common AEs from ustekinumab were nasopharyngitis (8.2%–10.2%), upper respiratory tract infection (6.3%–7.1%), and headache (5.1%–5.5%).37 Serious AEs (SAEs) occurred in two patients on the 45 mg dose, four patients on the 90 mg dose, and two patients in the placebo group.37 There were three serious infections, one cardiovascular event, and no cutaneous or noncutaneous cancers.37 By week 76, 5.1% of patients had developed antibodies to ustekinumab.37
Through week 12 of PHOENIX 2, the most common AEs from ustekinumab in adults with psoriasis were nasopharyngitis (6.8%–7.3%), headache (4.6%), and upper respiratory tract infection (2.9%–4.4%).38 SAEs occurred in eight patients in the 45 mg dose group, five patients in the 90 mg dose group, and eight patients in the placebo group.38 There were three serious infections, two cutaneous cancers, one noncutaneous cancer, and one cardiovascular event.38 By week 52, 5.4% of patients had antibodies to ustekinumab.38
Although the clinical trials highlighted the efficacy of ustekinumab, one of the major concerns was the long-term safety, especially with regards to malignancies. Here, we will briefly review the 1- to 5-year follow-up data in adults with psoriasis treated with ustekinumab.
Pooled safety data from Phase II and III clinical trials showed that during the placebo-controlled periods (12–20 weeks), there were comparable rates of AEs between patients on the 45 mg dose (57.6%), 90 mg dose (51.6%), and placebo (50.4%).52 The rates of overall infections and malignancies were also similar between patients on the 45 mg dose, 90 mg dose, and placebo.53 There were no reports of TB or demyelinating conditions.52,53 Apart from nonmelanoma skin cancers, the rates of malignancies were similar to those observed in the general US population.53 Importantly, by the third year, the rates of overall infections, AE, SAE, and malignancies remained stable over time.52,53
Five-year follow-up studies in adult patients with psoriasis enrolled in the PHOENIX 1 and 2 trials individually demonstrated favorable safety profiles. In the PHOENIX 1 study, the data revealed comparable rates of AEs, SAEs, infections, malignancies, and major adverse cardiovascular events among those in the 45 and 90 mg dose groups.39 There was one case of disseminated cutaneous herpes zoster but no reports of active TB, atypical mycobacterial, systemic fungal or salmonella infections, anaphylaxis, or serum-sickness-like reactions.39 Only 5.2% of patients developed antibodies and none reported injection-site reactions.39
Safety monitoring of PHOENIX 2 until week 264 showed that cumulative rates of AEs and SAEs were similar among patients in the 45 mg dose group, 90 mg dose group, and the general population.40 Importantly, there was no increase in the rates of SAEs, serious infections, nonmelanoma skin cancers, other malignancies, or major adverse cardiovascular events.40 The most common serious infections were diverticulitis (seven cases), cellulitis (five cases), and cholecystitis (three cases), with no reports of active TB, atypical mycobacterial, systemic fungal or salmonella infections, anaphylaxis, or serum-sickness-like reactions.40
Pooled safety data from PHOENIX 1 and 2, as well as their 5-year follow-up studies, demonstrated that the rates of overall mortality and malignancies (excluding nonmelanoma skin cancers) were found to be comparable to those in the general US population.54 The event rates for overall AEs, SAEs, serious infections, nonmelanoma skin cancers, other malignancies, and major adverse cardiovascular events were comparable between patients on the 45 and 90 mg doses.54 The rates of AEs were found to be comparable to other biologics used to treat psoriasis, and the study did not show evidence of cumulative toxicity up to 5 years.54
Safety data from the TRANSIT trial was analyzed through week 52.41 The rates of AEs were comparable between patients on the 45 and 90 mg doses and only led to cessation of ustekinumab in 0.4% of these patients.41 There were four serious infections, two of which required cessation of ustekinumab (pneumonia and acute hepatitis B), and four malignancies (keratoacanthoma, cervical carcinoma in situ, breast cancer in situ, and metastatic prostate cancer).41 There were three major adverse cardiovascular events: one cerebrovascular accident, one myocardial infarction, and one death from cardiorespiratory arrest.41 The overall rates of serious infections, malignancies, and major adverse cardiovascular events were 0.85, 0.85, and 0.64, respectively, per 100 patient-years of treatment.41
During the first 12 weeks of the ACCEPT trial comparing ustekinumab with etanercept for adult psoriasis patients, 66.0% of patients on ustekinumab and 70.0% of patients on etanercept reported at least one AE.43 In this time period, the most common adverse events were nasopharyngitis (8.6% of those on etanercept, 10.0% of those on 45 mg ustekinumab, and 9.8% of those on 90 mg ustekinumab), upper respiratory tract infection (5.8%, 6.2%, and 6.3%, respectively), headache (11.0%, 14.8%, and 12.1%, respectively), back pain (2.0%, 6.7%, and 4.3%, respectively), and injection-site reaction (24.8%, 4.3%, and 3.7%, respectively).43 The rate of infections as well as proportions of patients who stopped treatment due to adverse events were similar between the three treatment arms.43 Two patients receiving 45 mg ustekinumab and one patient receiving 90 mg ustekinumab were found to have nonmelanoma skin cancers.43
Safety data was also reported through week 64 of the ACCEPT trial.43 Patients on 45 and 90 mg doses of ustekinumab had similar rates and types of common adverse events, with the exception of injection-site reactions.43 One patient in each treatment arm died (motor vehicle accident, gunshot wound, and multisystem organ failure and sepsis, the latter in a patient who received 90 mg ustekinumab).43 Serious infections occurred in four patients who received etanercept, two patients who received 45 mg ustekinumab, and ten patients who received 90 mg ustekinumab (P=0.23 when comparing the low- and high-dose ustekinumab groups).43 There were nine reports of nonmelanoma skin cancers, and five patients who received ustekinumab had other malignant conditions.43 Three patients experienced major adverse cardiovascular events (one patient in the 45 mg ustekinumab group, one patient in the 90 mg ustekinumab group, and one patient who had crossed over to ustekinumab after etanercept).43 Although 3.8% of patients developed antibodies to ustekinumab, it was not associated with injection-site reactions.43
With regard to the use of ustekinumab in children, we have the pooled data of the five case reports and the CADMUS trial. Among the five previously described case reports, there was one report of elevated liver function tests and one report of intolerance necessitating treatment cessation. The addition of the CADMUS trial greatly expanded available safety data in adolescents; patients were monitored for adverse events though week 60.21 By week 12, the percentage of patients who had reported more than one AE was 44.4% in the SD, 51.4% in the HSD, and 56.8% in the placebo groups – no dose effect was noted.21 The most common AEs were nasopharyngitis (2.8% in SD, 13.5% in HSD, and 27% in placebo) and headache (8.3% SD, 10.8% HSD, and 5.4% placebo).21 One SAE (worsening of psoriasis) was reported in the HSD group.21
By week 40, after the placebo group had crossed over and received ustekinumab, the most common side effects were nasopharyngitis (34.5%), upper respiratory tract infections (12.7%), and pharyngitis (8.2%).21 By week 60, an additional five SAEs were also reported – one transient incident of leukopenia, pyelonephritis, ear infection, allergic contact dermatitis from hair dye, and one death from a motor vehicle accident, as well as one injection-site reaction.21 Although nine patients had developed antibodies to the drug – six in the HSD group and three in the SD group – six reached PGA 0/1 and only one reported an injection-site reaction, which was mild.21 Importantly, through week 60, there were no reports of malignancies, opportunistic infections, active TB, anaphylaxis, or serum-sickness-like reaction.21
The long-term safety of ustekinumab is also supported by data from PSOLAR – the Psoriasis Longitudinal Assessment and Registry that prospectively follows patients with plaque psoriasis being treated with biologic agents including ustekinumab.55 In 2014, Papp et al55 analyzed data accumulated from 12,093 patients: the unadjusted rates of serious infection were lower for ustekinumab (0.93 per 100 patient-years) as compared with infliximab (2.91 per 100 patient-years) and other biologic agents (1.91 per 100 patient-years).55 Importantly, no increased risk of malignancies, mortality, serious infections, or major adverse cardiovascular events were observed with the use of ustekinumab.55 Additional safety data accumulated from PSOLAR indicates a lower rate of serious infections with ustekinumab (0.83 per 100 patient-years) compared to etanercept (1.47 per 100 patient-years), adalimumab (1.97 per 100 patient-years), and infliximab (2.49 per 100 patient-years).56
Discussion
The biologic agents have revolutionized the treatment of several chronic childhood diseases including psoriasis, Crohn’s disease, JIA, and JIA-associated uveitis.2 Before these drugs were available, children were placed on long-term immunosuppressive agents, often without adequate disease management. The use of biologic agents can have a remarkable impact on quality of life, which is especially important for pediatric diseases that cause significant psychological and emotional distress. The major advantage of ustekinumab is the dosing schedule: after two initial loading doses, children only require four doses a year. Ustekinumab also spares children the toxic systemic effects of many other immunosuppressants. This makes it an ideal candidate for chronic childhood disorders that often entail life-long therapy.
Thus far, etanercept and adalimumab have been approved by the EU for the treatment of pediatric psoriasis; we will briefly review the efficacy and safety data from their use in pediatric patients.20,57
In 2008, the results of a 48-week randomized, double-blind trial evaluating etanercept for pediatric psoriasis were published.20 The trial enrolled 211 patients aged 4–17 years with moderate-to-severe plaque psoriasis and PASI ≥12. Dosing was 0.8 mg/kg with a maximum dose of 50 mg. At week 12, a higher percentage of patients on etanercept achieved PASI-75 (57%) and PASI-90 (27%) compared to those on placebo (11% and 7%, respectively) (P<0.001). A significant difference was noted even by week 4. A higher percentage of patients on etanercept also achieved PGA 0/1 (53%) compared to those on placebo (13%). At weeks 24 and 36, 57% and 53% of the patients who had initially received etanercept had PGA of 0/1, compared to 13% and 53%, respectively, of the original placebo group. The mean percentage improvement in PASI relative to baseline PASI was greater in patients receiving etanercept (22%) compared to those receiving placebo (5%) (P<0.001). By weeks 24 and 36, the mean percentage PASI improvement was 77% and 77%, respectively, in the group receiving etanercept compared to 71% and 76%, respectively, in the group receiving placebo. No SAEs occurred during the initial placebo-controlled phase. All subsequent serious noninfectious and infectious AEs resolved. Importantly, no deaths, cancers, opportunistic infections, TB, or demyelination events were reported from this trial.
In June 2015, the results of a four-part, Phase III study comparing adalimumab and methotrexate for pediatric patients with plaque psoriasis were reported.22,58 The trial included 114 children and adolescents ≥4 and <18 years of age with severe chronic plaque psoriasis who had either failed or were inappropriate candidates for topical therapy and phototherapy. Subjects received either 0.4 or 0.8 mg/kg subcutaneous adalimumab, or 0.1–0.4 mg/kg methotrexate, every other week.22 At 16 weeks, a significantly higher proportion of patients treated with adalimumab 0.8 mg/kg achieved PASI-75 (57.9%) compared to those who received methotrexate (32.4%).22 A higher number of patients treated with adalimumab 0.8 mg/kg achieved PGA 0/1 (60.5%) compared to those who received methotrexate (40.5%), although this number was not statistically significant.22
During the 16-week double-blind period, AEs were reported in 68% of patients receiving adalimumab and 76% of patients receiving methotrexate.22 There were no SAEs, no AEs requiring treatment cessation, or deaths reported.22 Approximately 47.4% of patients who received adalimumab 0.8 mg/kg reported an infection, compared to 54.1% who received methotrexate.22
Safety data was also reported from the 16-week re-treatment period (in which patients who did not have adequate disease control during treatment withdrawal were treated with adalimumab): 65.8% of patients on adalimumab reported treatment-emergent AEs.58 Approximately 10.5% experienced severe AEs including viral upper respiratory tract infection and urticaria in two patients who received methotrexate, and tonsillitis, upper respiratory tract infection, urinary tract infection, and bronchospasm in two patients who received adalimumab.58 One patient who received methotrexate followed by adalimumab developed urticaria and was withdrawn from the study.58 Infections were reported in 42.1% of those receiving adalimumab 0.8 mg/kg compared to 50.0% of those receiving methotrexate.58 No serious infections were reported in patients who received methotrexate or 0.8 mg/kg adalimumab; however, one patient who received 0.4 mg/kg adalimumab developed a serious gastrointestinal infection.22,58 Importantly, no malignancies were reported.22,58
One major concern relating to the use of biologic agents in children is that of malignancy. Notably, the TNF antagonists carry a black box warning for the increased risk of lymphoma and overall cancer risk. As with adults, there have been reports of malignancies in children taking TNF blockers including etanercept and adalimumab.59–64 However, none of the reported lymphoma cases were pediatric psoriatics, and the majority of children who develop lymphoma are children who are on more than one immunosuppressive medication. Diak et al59 analyzed the FDA’s Adverse Event Reporting System and found 48 reports of malignancies in children exposed to infliximab, etanercept, and adalimumab, of which half were lymphomas. However, in 88% of these cases, the patient was on another immunosuppressive agent. It can be challenging to link the use of TNF blockers to malignancies given that there might be an association with the underlying primary disease, and patients are often on other immunosuppressive agents.65
Hooper et al66 conducted a review on malignancies in children and young adults exposed to etanercept using the Amgen clinical trial database and postmarketing global safety database. For the 0- to 17-year age group, the reported rate appeared higher than incidence rates from a general pediatric population of similar ages and was primarily due to an increase in Hodgkin lymphoma.66 However, no increased rate was observed in the young-adult age group (18–30 years of age).66 In a different study, the estimated reporting rate of lymphomas in etanercept-exposed patients 4–17 years of age was 0.01 per 100 patient-years and was found to be higher than that of nonexposed children.65
With regard to the malignancies in ustekinumab-exposed patients, our long-term safety data comes from studies in adults. Pooled 5-year safety data from four studies of ustekinumab for psoriasis showed that the rates of malignancies (excluding nonmelanoma skin cancers) were comparable between patients on the 45 and 90 mg doses as well as comparable to rates in the general US popluation.54 Through week 60 of the CADMUS trial, there were no reports of malignancies.21 Longer-term safety data from this trial is still necessary to monitor occurrences of AEs, with a particular emphasis on malignancies. These rates could then be compared to those of other TNF blockers that are frequently used for childhood diseases.
In addition to the abundant safety data garnered from clinical trials, we have the advantage of mice knockout models and patients with unique genetic mutations in the IL-12/IL-23 circuit that have come to be known as the Mendelian susceptibility to mycobacterial disease syndrome.67
Production of IL-12 is triggered by bacterial and parasitic infections, mainly from phagocytic cells but also B-lymphocytes.33 Among other effects, IL-12 leads to the production of IFN-λ from natural killer and T-cells and encourages Th1 differentiation.33 Wu et al68 showed that mice deficient in IL-12Rβ1 were not able to produce IFN-λ even when provided with high concentrations of IL-12. Several years later, studies showed that mice deficient in IL-12Rβ2 also had abnormal IL-12 signaling and were unable to produce IFN-λ.35 Cooper et al69 analyzed the susceptibility of mice with defects in IL-12 to infection by Mycobacterium tuberculosis. Mice lacking either the p35 or p40 subunit were not able to adequately control infection by M. tuberculosis; however, those lacking the p40 subunit had higher rates of bacterial growth and less production of IFN-λ.69
The importance of Th1 cells in combating intracellular infections – whether viral, bacterial, fungal, or parasitic – would suggest that corresponding deficiencies in humans would be devastating. Interestingly, from the data we have on patients with genetic mutations in the IL-12/IL-23 pathway, this does not seem to be the case. One study reported a series of 41 patients from 17 countries, all with IL-12Rβ1 deficiency, and discovered that the only two opportunistic infections observed in 34 of these patients were Salmonella and Mycobacteria, the latter caused by Bacille Calmette-Guerin (BCG) vaccination or exposure to nontuberculous environmental Mycobacteria.67 Although salmonellosis was not fatal, three patients died from environmental Mycobacteria and two from BCG.67 These five deaths occurred in childhood, all before the age of eight.67 Similarly, Filipe-Santos et al34 noted that patients with IL-12p40 deficiency had a predilection to develop vaccination-induced BCG disease, environmental Mycobacteria infections, as well as Salmonella-associated diseases.
Fieschi and Casanova70 reviewed the frequency and types of infections in 73 patients with IL-12p40 or IL-12Rβ1 deficiencies. As with the previous study, their data confirmed that these patients were only susceptible to weakly virulent Mycobacteria (14 cases of environmental mycobacteriosis and 42 cases of BCG disease) and nontyphoid Salmonella (30 cases).70 There were four cases of TB and 15 deaths due to weakly virulent Mycobacteria.70 Interestingly, patients who recovered from and survived BCG disease did not develop recurrences of BCG or environmental mycobacteriosis, suggesting that they are able to mount a defense against secondary mycobacterial infections.70 The same was not true of Salmonella – disease often recurred, even with different species.70 Incredibly, the usual gamut of viral infections that plague immunocompromised patients – such as herpes simplex, varicella zoster, Epstein–Barr, and cytomegalovirus – did not cause severe disease in these patients.70 The same was true of fungal infections including Pneumocystis, Aspergillus, and Cryptococcus, as well as Gram-positive and Gram-negative bacteria including intracellular bacteria.70 Furthermore, the fact that not everyone developed BCG disease after vaccination or environmental mycobacteriosis suggested low penetrance.70
IL-12 appears to have a “redundant” role in fighting intracellular infections other than Mycobacteria and Salmonella, and perhaps even for Mycobacteria and Salmonella in some people.70 Most importantly, there does not seem to be an increased rate of malignancies. Overall, these individuals appear to have a favorable prognosis.
Apart from expanding the armamentarium of treatment options for childhood diseases, the increased use of biologic agents is evidence of a growing trend toward developing and using more targeted therapies. Recently, Quiniou et al36 designed a small peptide that acts solely as an IL-23R antagonist. IL-23 plays a central role not only in the pathogenesis of psoriasis, but also in other chronic inflammatory diseases such as multiple sclerosis, inflammatory bowel disease, and rheumatoid arthritis.36 Not only should targeted therapies improve the safety profile of future medications, but hopefully also their therapeutic efficacy. In order to develop such targeted therapies, we need to expand our knowledge vis-à-vis the molecular mechanisms that contribute to the pathogenesis of psoriasis and other chronic diseases, of which there is likely substantial overlap.
Conclusion
Ustekinumab requires fewer injections compared to other biologic agents, which greatly improves compliance and quality of life for any patient, but especially for pediatric patients. While the CADMUS trial and case reports described in this paper support the use of ustekinumab in adolescent patients, additional studies are required to ensure its clinical efficacy and safety. Long-term registries are not yet available in pediatric patients but will be of the utmost importance going forward. For now, we are relying on data from adult studies with the understanding that we cannot simply apply the same conclusions to a pediatric population. Yet, we also have the benefit of studying a population of patients with defects in the IL-12/IL-23 pathways. These patients appear to have a favorable prognosis and, most importantly, do not appear to have an increased risk of malignancies.
Perhaps in the future, the use of ustekinumab can be extended to other chronic childhood diseases such as Crohn’s disease, JIA, JIA-associated uveitis, and BD. Not all patients show adequate response to conventional therapies, and we need to expand our array of treatment options.
Disclosure
Mark Lebwohl is an employee of the Mount Sinai Medical Center which receives research funds from Amgen, Anacor, Boehringer Ingleheim, Celgene, Lilly, Janssen Biotech, Kadmon, LEO Pharmaceuticals, Medimmune, Novartis, Pfizer, Sun Pharmaceuticals, and Valeant. Nanette B Silverberg has been an advisor for Anacor, Galderma and Johnson and Johnson CPC, and an investigator and/or consultant for Astellas and Novartis. The authors report no other conflicts of interest in this work.
References
Luu M, Cordoro KM. The evolving role of biologics in the treatment of pediatric psoriasis. Skin Therapy Lett. 2013;18(2):1–4. | |
Bellodi Schmidt F, Shah KN. Biologic response modifiers and pediatric psoriasis. Pediatr Dermatol. 2015;32(3):303–320. | |
Lebwohl MG, Bachelez H, Barker J, et al. Patient perspectives in the management of psoriasis: results from the population-based Multinational Assessment of Psoriasis and Psoriatic Arthritis Survey. J Am Acad Dermatol. 2014;70(5):871–881. e1–e30. | |
Raychaudhuri SP, Gross J. A comparative study of pediatric onset psoriasis with adult onset psoriasis. Pediatr Dermatol. 2000;17(3):174–178. | |
Pepper AN, Pothiawala S, Silverberg NB. In: Weinberg JM, Lebwohl M, editors. Advances in Psoriasis: A Multisystemic Guide. London, UK: Springer-Verlag London; 2014. | |
Tollefson MM, Crowson CS, McEvoy MT, Maradit Kremers H. Incidence of psoriasis in children: a population-based study. J Am Acad Dermatol. 2010;62(6):979–987. | |
Kwon HH, Na SJ, Jo SJ, Youn JI. Epidemiology and clinical features of pediatric psoriasis in tertiary referral psoriasis clinic. J Dermatol. 2012;39(3):260–264. | |
Fotiadou C, Lazaridou E, Ioannides D. Management of psoriasis in adolescence. Adolesc Health Med Ther. 2014;5:25–34. | |
Boehncke WH, Schon MP. Psoriasis. Lancet. 2015;386(9997):983–994. | |
Coimbra S, Figueiredo A, Castro E, Rocha-Pereira P, Santos-Silva A. The roles of cells and cytokines in the pathogenesis of psoriasis. Int J Dermatol. 2012;51(4):389–395; quiz 395–398. | |
Elder JT. Genome-wide association scan yields new insights into the immunopathogenesis of psoriasis. Genes Immun. 2009;10(3):201–209. | |
Nair RP, Duffin KC, Helms C, et al. Genome-wide scan reveals association of psoriasis with IL-23 and NF-κB pathways. Nat Genet. 2009;41(2):199–204. | |
Lonnberg AS, Skov L, Skytthe A, Kyvik KO, Pedersen OB, Thomsen SF. Heritability of psoriasis in a large twin sample. Br J Dermatol. 2013;169(2):412–416. | |
Chandran V, Raychaudhuri SP. Geoepidemiology and environmental factors of psoriasis and psoriatic arthritis. J Autoimmun. 2010;34(3):J314–J321. | |
Gutmark-Little I, Shah KN. Obesity and the metabolic syndrome in pediatric psoriasis. Clin Dermatol. 2015;33(3):305–315. | |
Fleming P, Kraft J, Gulliver WP, Lynde C. The relationship of obesity with the severity of psoriasis: a systematic review. J Cutan Med Surg. 2015;19(5):450–456. | |
Paller AS, Mercy K, Kwasny MJ, et al. Association of pediatric psoriasis severity with excess and central adiposity: an international cross-sectional study. JAMA Dermatol. 2013;149(2):166–176. | |
Davidovici BB, Sattar N, Prinz J, et al. Psoriasis and systemic inflammatory diseases: potential mechanistic links between skin disease and co-morbid conditions. J Invest Dermatol. 2010;130(7):1785–1796. | |
Kim IH, West CE, Kwatra SG, Feldman SR, O’Neill JL. Comparative efficacy of biologics in psoriasis: a review. Am J Clin Dermatol. 2012;13(6):365–374. | |
Paller AS, Siegfried EC, Langley RG, et al. Etanercept treatment for children and adolescents with plaque psoriasis. N Engl J Med. 2008;358(3):241–251. | |
Landells I, Marano C, Hsu MC, et al. Ustekinumab in adolescent patients age 12 to 17 years with moderate-to-severe plaque psoriasis: Results of the randomized phase 3 CADMUS study. J Am Acad Dermatol. 2015;73(4):594–603. | |
Efficacy and safety of adalimumab versus methotrexate treatment in pediatric patients with severe chronic plaque psoriasis: results from the 16-week randomized, double-blind period of a phase 3 study. Poster presented at: The 23rd World Congress of Dermatology, June 8–13, 2015, Vancouver, Canada. | |
Hyams JS. Biologics in pediatric Crohn’s disease: is it time to move to an earlier therapeutic approach? Expert Rev Clin Immunol. 2014;10(11):1423–1426. | |
Mandel MD, Miheller P, Mullner K, Golovics PA, Lakatos PL. Have biologics changed the natural history of Crohn’s disease? Dig Dis. 2014;32(4):351–359. | |
Assa A, Hartman C, Weiss B, et al. Long-term outcome of tumor necrosis factor alpha antagonist’s treatment in pediatric Crohn’s disease. J Crohns Colitis. 2013;7(5):369–376. | |
Kasapcopur O, Barut K. Treatment in juvenile rheumatoid arthritis and new treatment options. Turk Pediatri Ars. 2015;50(1):1–10. | |
Wells JM, Smith JR. Uveitis in juvenile idiopathic arthritis: recent therapeutic advances. Ophthalmic Res. 2015;54(3):124–127. | |
Piram M, Koné-Paut I. Maladie de Behçet de l’enfant [Pediatric Behcet’s disease]. Rev Med Interne. 2014;35(2):121–125. French. | |
Caso F, Costa L, Rigante D, et al. Biological treatments in Behcet’s disease: beyond anti-TNF therapy. Mediators Inflamm. 2014;2014:107421. | |
Ozen S, Eroglu FK. Pediatric-onset Behcet disease. Curr Opin Rheumatol. 2013;25(5):636–642. | |
Stelara® (ustekinumab) [package insert]. Horsham, PA: Janssen Inc; 2014. | |
Janssen Research and Development, LLC. A study of the safety and efficacy of ustekinumab in adolescent patients with psoriasis (CADMUS). NLM identifier: NCT01090427. Available from: https://clinicaltrials.gov/ct2/show/results/NCT01090427?sect=X01256. Accessed September 10, 2015. | |
Trinchieri G. Interleukin-12: a proinflammatory cytokine with immunoregulatory functions that bridge innate resistance and antigen-specific adaptive immunity. Annu Rev Immunol. 1995;13:251–276. | |
Filipe-Santos O, Bustamante J, Chapgier A, et al. Inborn errors of IL-12/23- and IFN-γ-mediated immunity: molecular, cellular, and clinical features. Semin Immunol. 2006;18(6):347–361. | |
Wu C, Wang X, Gadina M, O’Shea JJ, Presky DH, Magram J. IL-12 receptor β2 (IL-12Rβ2)-deficient mice are defective in IL-12-mediated signaling despite the presence of high affinity IL-12 binding sites. J Immunol. 2000;165(11):6221–6228. | |
Quiniou C, Dominguez-Punaro M, Cloutier F, et al. Specific targeting of the IL-23 receptor, using a novel small peptide noncompetitive antagonist, decreases the inflammatory response. Am J Physiol Regul Integr Comp Physiol. 2014;307(10):R1216–R1230. | |
Leonardi CL, Kimball AB, Papp KA, et al. Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 76-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 1). Lancet. 2008;371(9625):1665–1674. | |
Papp KA, Langley RG, Lebwohl M, et al. Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 52-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 2). Lancet. 2008;371(9625):1675–1684. | |
Kimball AB, Papp KA, Wasfi Y, et al. Long-term efficacy of ustekinumab in patients with moderate-to-severe psoriasis treated for up to 5 years in the PHOENIX 1 study. J Eur Acad Dermatol Venereol. 2013;27(12):1535–1545. | |
Langley RG, Lebwohl M, Krueger GG, et al. Long-term efficacy and safety of ustekinumab, with and without dosing adjustment, in patients with moderate-to-severe psoriasis: results from the PHOENIX 2 study through 5 years of follow-up. Br J Dermatol. 2015;172(5):1371–1383. | |
Reich K, Puig L, Paul C, et al. One-year safety and efficacy of ustekinumab and results of dose adjustment after switching from inadequate methotrexate treatment: the TRANSIT randomized trial in moderate-to-severe plaque psoriasis. Br J Dermatol. 2014;170(2):435–444. | |
Paul C, Puig L, Kragballe K, et al. Transition to ustekinumab in patients with moderate-to-severe psoriasis and inadequate response to methotrexate: a randomized clinical trial (TRANSIT). Br J Dermatol. 2014;170(2):425–434. | |
Griffiths CE, Strober BE, van de Kerkhof P, et al. Comparison of ustekinumab and etanercept for moderate-to-severe psoriasis. N Engl J Med. 2010;362(2):118–128. | |
Fotiadou C, Lazaridou E, Giannopoulou C, Ioannides D. Ustekinumab for the treatment of an adolescent patient with recalcitrant plaque psoriasis. Eur J Dermatol. 2011;21(1):117–118. | |
Dixit S, Shumack S, Fischer G. Ustekinumab in the treatment of severe paediatric psoriasis. Australas J Dermatol. 2013;54(2):147. | |
Garber C, Creighton-Smith M, Sorensen EP, Dumont N, Gottlieb AB. Systemic treatment of recalcitrant pediatric psoriasis: a case series and literature review. J Drugs Dermatol. 2015;14(8):881–886. | |
Walsh JA, McFadden M, Woodcock J, et al. Product of the Physician Global Assessment and body surface area: a simple static measure of psoriasis severity in a longitudinal cohort. J Am Acad Dermatol. 2013;69(6):931–937. | |
Lewis-Jones MS, Finlay AY. The Children’s Dermatology Life Quality Index (CDLQI): initial validation and practical use. Br J Dermatol. 1995;132(6):942–949. | |
Sandborn WJ, Gasink C, Gao LL, et al. Ustekinumab induction and maintenance therapy in refractory Crohn’s disease. N Engl J Med. 2012;367(16):1519–1528. | |
Rinawi F, Rosenbach Y, Assa A, Shamir R. Ustekinumab for resistant pediatric Crohn’s disease. J Pediatr Gastroenterol Nutr. Epub July 11, 2014. | |
Baerveldt EM, Kappen JH, Thio HB, van Laar JA, van Hagen PM, Prens EP. Successful long-term triple disease control by ustekinumab in a patient with Behcet’s disease, psoriasis and hidradenitis suppurativa. Ann Rheum Dis. 2013;72(4):626–627. | |
Lebwohl M, Leonardi C, Griffiths CE, et al. Long-term safety experience of ustekinumab in patients with moderate-to-severe psoriasis (part I of II): results from analyses of general safety parameters from pooled phase 2 and 3 clinical trials. J Am Acad Dermatol. 2012;66(5):731–741. | |
Gordon KB, Papp KA, Langley RG, et al. Long-term safety experience of ustekinumab in patients with moderate to severe psoriasis (part II of II): results from analyses of infections and malignancy from pooled phase II and III clinical trials. J Am Acad Dermatol. 2012;66(5):742–751. | |
Papp KA, Griffiths CE, Gordon K, et al. Long-term safety of ustekinumab in patients with moderate-to-severe psoriasis: final results from 5 years of follow-up. Br J Dermatol. 2013;168(4):844–854. | |
Papp K, Gottlieb AB, Naldi L, et al. Safety surveillance for ustekinumab and other psoriasis treatments from the Psoriasis Longitudinal Assessment and Registry (PSOLAR). J Drugs Dermatol. 2015;14(7):706–714. | |
Kalb RE, Fiorentino DF, Lebwohl MG, et al. Risk of serious infection with biologic and systemic treatment of psoriasis: results from the psoriasis longitudinal assessment and registry (PSOLAR). JAMA Dermatol. 2015;151(9):961–969. | |
AbbVie.com [homepage on the Internet]. North Chicago, IL: AbbVie’s HUMIRA® (Adalimumab) Approved by European Commission to Treat Children and Adolescents with Severe Chronic Plaque Psoriasis; 2014 [updated April 1, 2015]. Available from: http://abbvie.mediaroom.com/2015-04-01-AbbVies-HUMIRA-Adalimumab-Approved-by-European-Commission-to-Treat-Children-and-Adolescents-with-Severe-Chronic-Plaque-Psoriasis. Accessed December 22, 2015. | |
Kim Papp. Efficacy, safety of adalimumab vs methotrexate in pediatric patients with severe chronic plaque psoriasis: results from the treatment withdrawal and double-blind retreatment periods of a phase 3 study. Poster presented at: The 23rd World Congress of Dermatology, June 8–13, 2015, Vancouver, Canada. | |
Diak P, Siegel J, La Grenade L, Choi L, Lemery S, McMahon A. Tumor necrosis factor alpha blockers and malignancy in children: forty-eight cases reported to the Food and Drug Administration. Arthritis Rheum. 2010;62(8):2517–2524. | |
Deepak P, Sifuentes H, Sherid M, Stobaugh D, Sadozai Y, Ehrenpreis ED. T-cell non-Hodgkin’s lymphomas reported to the FDA AERS with tumor necrosis factor-α (TNF-α) inhibitors: results of the REFURBISH study. Am J Gastroenterol. 2013;108(1):99–105. | |
Burmester GR, Panaccione R, Gordon KB, McIlraith MJ, Lacerda AP. Adalimumab: long-term safety in 23,458 patients from global clinical trials in rheumatoid arthritis, juvenile idiopathic arthritis, ankylosing spondylitis, psoriatic arthritis, psoriasis and Crohn’s disease. Ann Rheum Dis. 2013;72(4):517–524. | |
McCluggage LK. Safety of TNF inhibitors in adolescents and children. Adolesc Health Med Ther. 2011;2:1–8. | |
Keystone EC. Does anti-tumor necrosis factor-α therapy affect risk of serious infection and cancer in patients with rheumatoid arthritis? A review of longterm data. J Rheumatol. 2011;38(8):1552–1562. | |
Brown SL, Greene MH, Gershon SK, Edwards ET, Braun MM. Tumor necrosis factor antagonist therapy and lymphoma development: twenty-six cases reported to the Food and Drug Administration. Arthritis Rheum. 2002;46(12):3151–3158. | |
McCroskery P, Wallace CA, Lovell DJ, et al. Summary of worldwide pediatric malignancies reported after exposure to etanercept. Pediatr Rheumatol Online J. 2010;8:18. | |
Hooper M, Wenkert D, Bitman B, Dias VC, Bartley Y. Malignancies in children and young adults on etanercept: summary of cases from clinical trials and post marketing reports. Pediatr Rheumatol Online J. 2013;11(1):35. | |
Fieschi C, Dupuis S, Catherinot E, et al. Low penetrance, broad resistance, and favorable outcome of interleukin 12 receptor β1 deficiency: medical and immunological implications. J Exp Med. 2003;197(4):527–535. | |
Wu C, Ferrante J, Gately MK, Magram J. Characterization of IL-12 receptor β1 chain (IL-12Rβ1)-deficient mice: IL-12Rβ1 is an essential component of the functional mouse IL-12 receptor. J Immunol. 1997;159(4):1658–1665. | |
Cooper AM, Kipnis A, Turner J, Magram J, Ferrante J, Orme IM. Mice lacking bioactive IL-12 can generate protective, antigen-specific cellular responses to mycobacterial infection only if the IL-12 p40 subunit is present. J Immunol. 2002;168(3):1322–1327. | |
Fieschi C, Casanova JL. The role of interleukin-12 in human infectious diseases: only a faint signature. Eur J Immunol. 2003;33(6):1461–1464. | |
Yancoski J, Rocco C, Bernasconi A, et al. A 475 years-old founder effect involving IL12RB1: a highly prevalent mutation conferring Mendelian susceptibility to mycobacterial diseases in European descendants. Infect Genet Evol. 2009;9(4):574–580. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.