Back to Journals » Drug Design, Development and Therapy » Volume 20
Efficacy and Safety of Finerenone Combined with Dapagliflozin in the Treatment of Non-Diabetic Chronic Kidney Disease: A Single-Center Retrospective Study
Authors Ma J, Su Q, Wang H, Xu J, Yuan C, Fan G ![]() , Ying J, Bian X
, Ying J, Bian X
Received 3 September 2025
Accepted for publication 20 January 2026
Published 24 January 2026 Volume 2026:20 564942
DOI https://doi.org/10.2147/DDDT.S564942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Solomon Tadesse Zeleke
Jianwei Ma,1,2,* Qin Su,1,* Hanlu Wang,1 Jiayan Xu,1,3 Chenyi Yuan,1 Guicai Fan,1,3 Jiapei Ying,1 Xueyan Bian1
1Department of Nephrology, The First Affiliated Hospital of Ningbo University, Ningbo, 315010, People’s Republic of China; 2Department of Clinical Medicine, Tongji University School of Medicine, Shanghai, 200092, People’s Republic of China; 3Health Science Center, Ningbo University, Ningbo, 315211, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xueyan Bian, Department of Nephrology, The First Affiliated Hospital of Ningbo University, 59 Liuting Street, Haishu District, Ningbo, 315010, People’s Republic of China, Email [email protected]
Background: The combination of non-steroidal mineralocorticoid receptor antagonists (nsMRAs) and sodium-glucose cotransporter-2 (SGLT2) inhibitors has shown renoprotective benefits in diabetic kidney disease; however, their synergistic effects in non-diabetic chronic kidney disease (CKD) remain underexplored. This study evaluated the efficacy and safety of finerenone combined with dapagliflozin versus dapagliflozin monotherapy in patients with non-diabetic CKD.
Methods: A single-center, retrospective cohort study was conducted on 121 patients with biopsy- or clinically confirmed non-diabetic CKD treated with either dapagliflozin alone (n = 77) or in combination with finerenone (n = 44) for ≥ 6 months. Propensity score matching (PSM) yielded 33 well-balanced pairs. The primary outcomes were changes in the urinary albumin-to-creatinine ratio (UACR) and estimated glomerular filtration rate (eGFR) over 6 months. Secondary outcomes included Blood Pressure, biochemical parameters, and treatment-related adverse events. Repeated-measures ANOVA and mediation analyses were used to assess longitudinal changes and mechanistic relationships.
Results: Finerenone Combined with Dapagliflozin therapy significantly enhanced UACR reduction at 3 months (median 63.4% vs 47.8%, P = 0.007) and 6 months (66.9% vs 40.8%, P = 0.002), compared with dapagliflozin alone, with a higher proportion of patients achieving ≥ 50% reduction (84.9% vs 45.5%, P < 0.001). The eGFR was preserved or improved with combination therapy (+2.06% vs – 5.08%, P < 0.001), whereas dapagliflozin alone therapy was associated with a decline. Mediation analysis indicated that early UACR reduction explained only 1.45% of the treatment effect on eGFR changes, suggesting albuminuria-independent mechanisms. The incidence of adverse events, including hyperkalemia, did not differ significantly between the groups, and all events were mild and manageable.
Conclusion: Finerenone combined with dapagliflozin yielded superior proteinuria reduction and better preservation of renal function compared with dapagliflozin alone in patients with non-diabetic CKD, without compromising safety. These findings provide real-world evidence for the potential additive renoprotective effects of dual therapy and underscore the need for prospective trials to validate its efficacy in non-diabetic populations.
Keywords: finerenone, dapagliflozin, non-diabetic chronic kidney disease, albuminuria, estimated glomerular filtration rate
Introduction
Chronic kidney disease (CKD) is a major global health burden that affects 15–20% of adults globally.1,2 CKD is characterized by a progressive decline in kidney function, often leading to end-stage renal disease (ESRD), in which patients require dialysis or kidney transplantation to survive.3–5 Fibrosis driven by the excessive accumulation and deposition extracellular matrix is the final common manifestation and pathways of almost all types of chronic repetitive damage in renal tissue and is recognized as a hallmark of CKD.2,6–8 The management of CKD primarily focuses on controlling risk factors, such as proteinuria, hypertension, and diabetes, decelerating kidney damage, and preventing cardiovascular complications.9–11 For decades, the cornerstone of CKD treatment has been the blockade of the renin-angiotensin system (RAS) using angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs).12 These therapies have been shown to reduce proteinuria, a key biomarker of kidney injury, and improve renal outcomes.13,14 However, the efficacy of RAS blockade is often limited, particularly in patients with high albuminuria who do not require hormonal or immunosuppressive therapy. Furthermore, there remains a high risk of progression to end-stages of CKD, even in patients undergoing RAS blockade.15,16
Novel therapeutic approaches have emerged to address these limitations. Recent evidence suggests that a multifaceted treatment regimen combining RAS blockers with newer agents, such as sodium-glucose co-transporter 2 inhibitors (SGLT2i) and non-steroidal mineralocorticoid receptor antagonists (MRAs), may offer enhanced proteinuria control and superior cardiorenal protection in patients with CKD.17–20 SGLT2i have demonstrated significant renoprotective effects in diabetic kidney disease (DKD), reducing albuminuria and decelerating the progression of nephropathy.21,22 These benefits appear to extend beyond glycemic control, as SGLT2i have also shown efficacy in non-diabetic patients.17,23 Similarly, nonsteroidal MRAs, such as finerenone, have shown promise in reducing renal composite endpoints in patients with DKD.24 FIDELITY analysis revealed that finerenone consistently reduced albuminuria and slowed eGFR decline in patients with type 2 diabetes and CKD.25 Additionally, finerenone showed benefits on kidney outcomes, even in patients already receiving SGLT-2 inhibitors.24 Interestingly, the combination of MRAs and SGLT2i is associated with greater reductions in albuminuria than either therapy alone in patients with type 2 diabetes.26 Building on these findings, the recently published CONFIDENCE trial provided the first prospective randomized evidence that combining finerenone with empagliflozin led to greater reductions in albuminuria than either agent alone in patients with type 2 diabetes and CKD.27
While both therapeutic classes have independently demonstrated significant benefits, preliminary evidence suggests potential synergistic effects in diabetic populations, and their combined efficacy and safety in non-diabetic CKD patients remain insufficiently studied. Therefore, this study aimed to systematically evaluate the therapeutic potential of combining finerenone with dapagliflozin compared with dapagliflozin monotherapy in the management of non-diabetic CKD. This single-center retrospective study focused on changes in albuminuria, kidney function, and the incidence of adverse events, thereby contributing to the advancement of CKD treatment strategies.
Materials and Methods
Study Design and Setting
This retrospective study was conducted at a single-center institution to evaluate the efficacy and safety of finerenone in combination with dapagliflozin compared with dapagliflozin monotherapy in the treatment of non-diabetic CKD. With reference to FIGALO-DKD and FIDELIO-DKD, prospective participants had to be without any modifications to dosage, drug choice, or other interventions associated with antihypertensive therapy.
All procedures involving human participants adhered to the ethical standards of the National Research Committee and the 1964 Declaration of Helsinki, along with its subsequent amendments or comparable ethical standards. The study was approved by the Medical and Research Ethics Committee of the First Affiliated Hospital of Ningbo University (approval number: 2024–182RS-02), and all patient data were anonymized to ensure confidentiality. Given the retrospective nature of this study, the requirement for written informed consent was waived in line with the Declaration of Helsinki.
Population
This study included adult patients diagnosed with non-diabetic CKD, as confirmed by clinical and laboratory assessments, who were treated at our institution between August 2023 and December 2024. The inclusion criteria were as follows: 1) Age ≥18 years. 2) Diagnosis of non-diabetic CKD confirmed by biopsy, clinical presentation, or laboratory evidence of kidney dysfunction without a prior diagnosis of diabetes mellitus (Among the enrolled patients, 52.89% had biopsy-proven diagnoses of non-diabetic CKD).28,29 3) Urinary albumin-to-creatinine ratio (UACR) >200 mg/g and <3000 mg/g. 4) Treatment with ACEIs or ARBs for a minimum of 3 months. 5) Dapagliflozin alone or in combination with finerenone was prescribed for more than 6 months. The exclusion criteria were as follows: 1) a history of type 1 or type 2 diabetes mellitus and 2) active malignancies. 3) Severe liver disease or contraindications for finerenone or dapagliflozin. 4) Hyperkalemia prior to medication use (K>5.0mmol/L). 5) Use of glucocorticoids, immunosuppressants, or spironolactone within the preceding three months. 6) eGFR <20 mL/min/1.73 m2. The UACR was calculated by dividing the concentration of albumin by the concentration of creatinine in a spot urine sample, which is typically expressed in mg/g or μg/mg of creatinine.30 The eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.31,32
Data Collection
This retrospective study utilized data from the electronic medical records of the First Affiliated Hospital of Ningbo University and detailed baseline demographic and clinical information, including age, sex, BMI, blood pressure, medical history, comorbidities, hemoglobin levels, UACR, and comprehensive biochemical parameters, such as serum albumin, blood urea nitrogen, serum creatinine, eGFR, uric acid, serum potassium, serum sodium, and fasting blood glucose. Patients were divided into two treatment groups: the finerenone Combined with Dapagliflozin Group and the dapagliflozin alone group. Both groups received dapagliflozin at a fixed dose of 10 mg once daily. In the combination group, finerenone was initiated at a fixed dose of 10 mg once daily and was not titrated during the study period. All enrolled patients met the inclusion criterion of receiving stable ACEI or ARB therapy for at least 3 months prior to group allocation. To reflect real-world practice and maximize renal protection, doses were titrated to the maximum tolerated level based on individual clinical parameters (eg, blood pressure, eGFR, serum potassium), unless contraindicated. Treatment assignment was determined by attending nephrologists based on clinical response and renal function rather than randomization. Key laboratory and clinical parameters were assessed at baseline and 3 and 6 months after treatment initiation. The primary outcomes were changes in UACR and eGFR over six months, which serve as indicators of renal function and proteinuria, respectively. Secondary outcomes included changes in serum albumin, uric acid, potassium, sodium, and fasting blood glucose levels and the incidence of treatment-related adverse events.
Statistical Analysis
All statistical analyses were performed using R software (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria). Continuous variables are reported as mean ± standard deviation (SD) or median [interquartile range (IQR)], based on normality assessed using the Shapiro–Wilk test. Categorical variables were expressed as frequency and percentage. Between-group comparisons were conducted using the independent-samples t-test for normally distributed variables, the Mann–Whitney U-test for non-normally distributed variables, and the chi-square test for categorical variables. Statistical significance was defined as a two-tailed P < 0.05.
Propensity score matching (PSM) was conducted using the MatchIt package to reduce confounding and achieve baseline covariate balance. Propensity scores were estimated using logistic regression, including covariates with standardized mean differences (SMDs) > 0.1. A 1:1 nearest-neighbor matching algorithm without replacement was applied with a caliper width of 0.2 standard deviations of the logit of the propensity score.
Longitudinal changes in UACR, eGFR, SBP, DBP, Serum Albumin, Glucose, Uric Acid, Electrolytes, and Hemoglobin at baseline, 3 months, and 6 months were analyzed using repeated-measures ANOVA, with Time as the within-subject factor, group (combination vs monotherapy) as the between-subject factor, and their interaction. Mauchly’s test was performed to assess the sphericity assumption, and when violated, the Greenhouse–Geisser correction was applied. Bonferroni-adjusted post hoc comparisons were applied where necessary.
Mediation analysis was performed using the mediation package to determine whether early albuminuria reduction—defined as the percentage change in UACR from baseline to 3 months—mediated the treatment effect on renal function, measured as the percentage change in eGFR from 3 to 6 months relative to the 3-month value. Unadjusted linear regression models were used to estimate path coefficients (a: treatment → UACR change; b: UACR change → eGFR change; c′: direct treatment effect), with covariate balance ensured through PSM. Indirect effects (a × b) were calculated using 5,000 bootstrap simulations to generate 95% confidence intervals (CIs).
All statistical plots were generated using the ggplot2 package in R, and the final figure composition and labeling were performed using GraphPad Prism version 9.5.1 (GraphPad Software, Boston, MA, USA).
Results
Baseline Characteristics Before and After PSM
From August 2023 to December 2024, 827 adults withnon-diabetic CKD treated with finerenone and/or dapagliflozin were screened. Of these, 121 met the prespecified eligibility criteria and comprised the full analysis set: 77 received dapagliflozin alone and 44 received finerenone–dapagliflozin combination therapy (Figure 1). Significant pre-matching imbalances in blood glucose, UACR, and eGFR necessitated rigorous adjustment via 1:1 nearest-neighbor PSM (caliper = 0.2 × SD). Matching covariates were selected based on their established relevance to non-diabetic CKD progression and included Age, Sex, BMI, Hypertension, Hyperuricemia, MAP, Albumin, Blood glucose, Scr, Uric acid, potassium, hemoglobin, UACR, and eGFR.
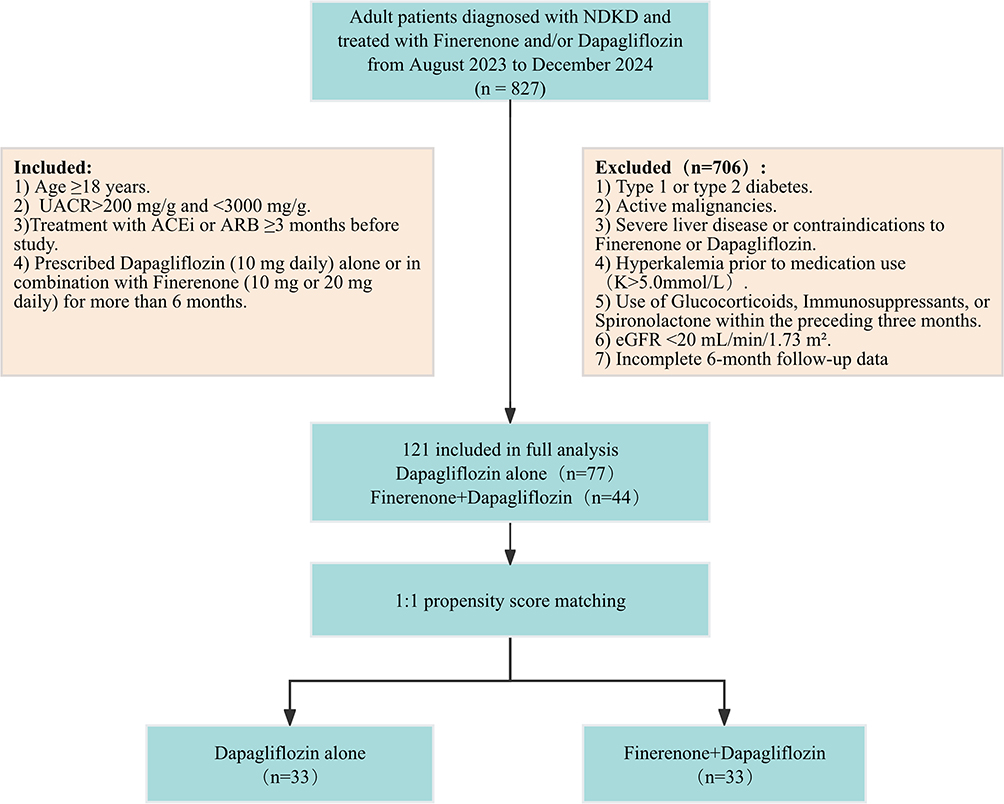 |
Figure 1 Flow diagram of patient selection and grouping. |
After 1:1 nearest-neighbor matching, 33 patients remained in each group (Figure 1). Post-PSM, no significant differences were observed across the baseline variables (all P > 0.05), indicating effective covariate balancing. Fasting glucose [5.43 (5.06–5.90) vs 5.41 (5.13–5.88) mmol/L; P = 0.857], UACR [436 (241–841) vs 500 (372–862) mg/g; P = 0.365], and eGFR [65.0 (49.0–98.0) vs 81.0 (55.0–95.0) mL/min/1.73 m2; P = 0.547] were comparable between groups (Table 1).
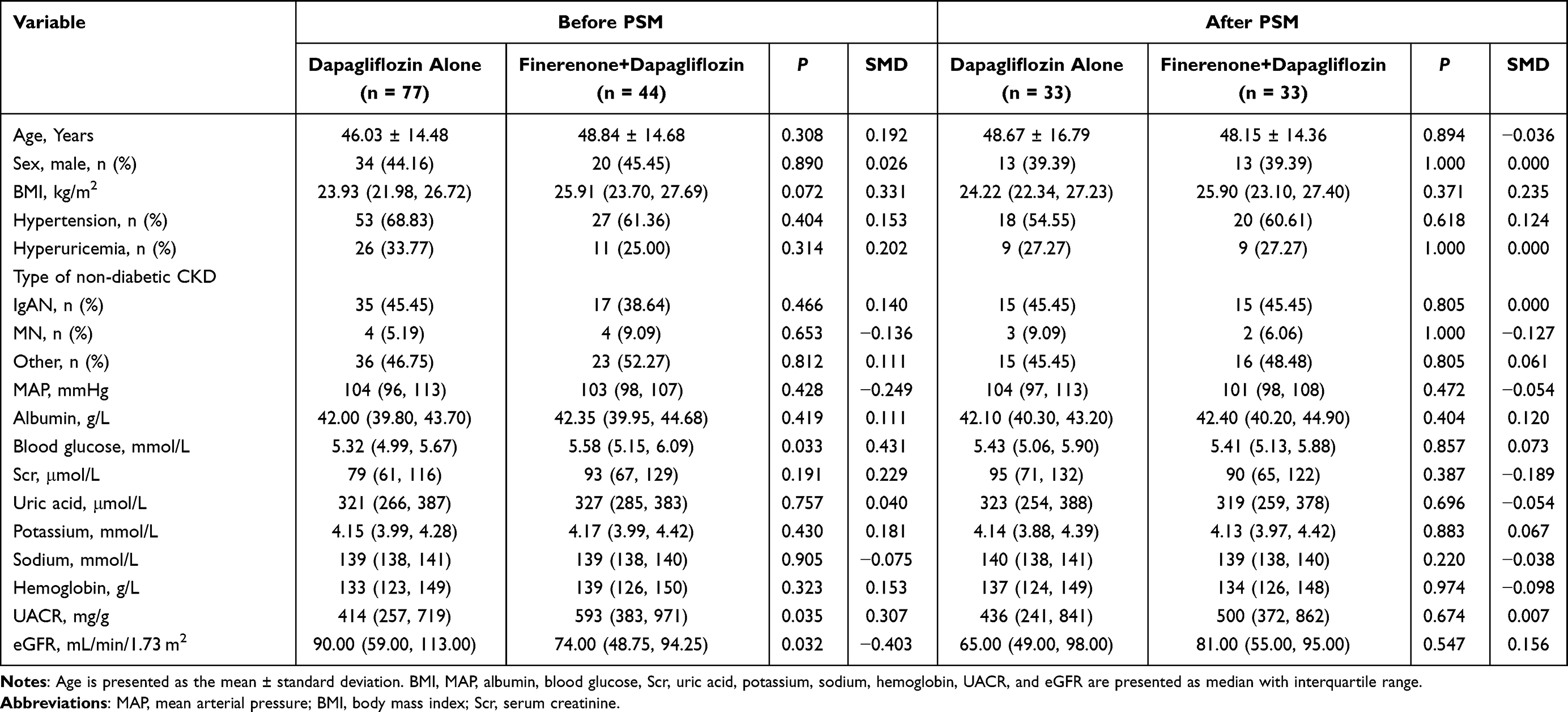 |
Table 1 Baseline Characteristics Before and After PSM |
Primary Outcomes
Longitudinal Changes in Albuminuria and eGFR
Repeated-measures- ANOVA demonstrated significant temporal effects on UACR (F1 = 36.302, P < 0.001) and group × time interaction (F3 = 4.430, P = 0.039), indicating accelerated albuminuria reduction in the finerenone–dapagliflozin combination group. The nonsignificant group effect (F2 = 0.101, P = 0.752) suggests that the differential trajectories were treatment-associated rather than baseline-derived. For eGFR, a significant group × time interaction (F3 = 14.131, P < 0.001) contrasted with nonsignificant time (F1 = 0.268, P = 0.607) and group (F2 = 1.091, P = 0.300) effects (Table 2). These interaction effects necessitated post hoc analyses to delineate the treatment response dynamics.
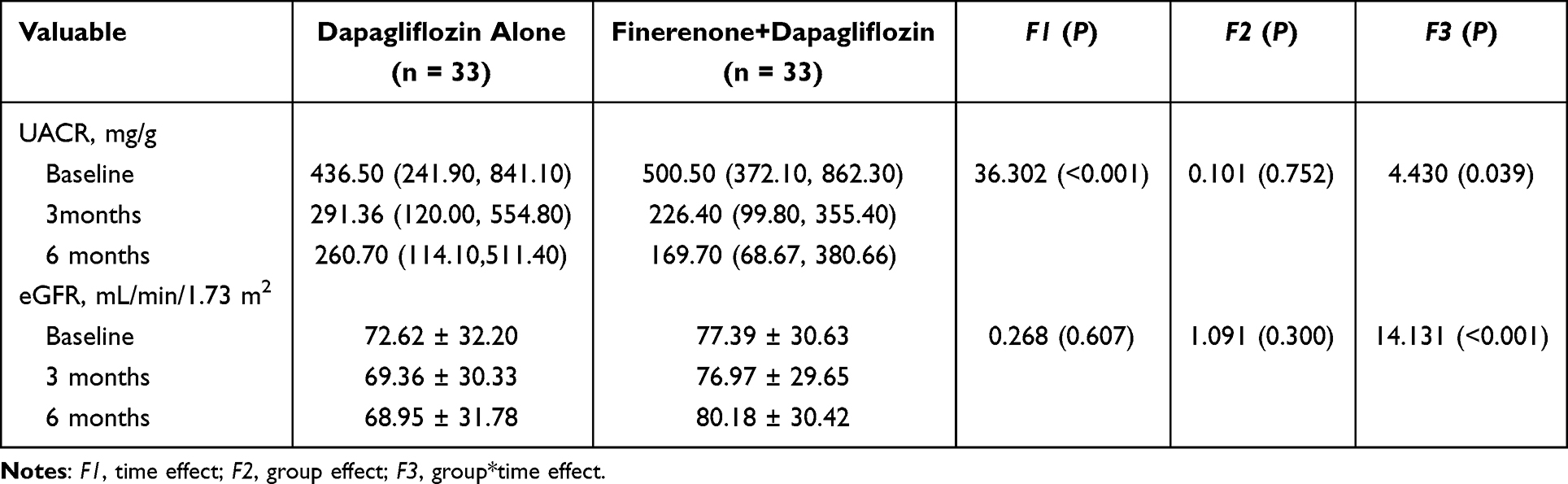 |
Table 2 Longitudinal Changes in UACR and eGFR During Follow-Up in the Two Groups |
Magnitude of UACR Reduction
Post-hoc analysis confirmed more pronounced reductions in albuminuria with combination therapy. At 3 months, the finerenone combined with dapagliflozin group had a median UACR decline of 302.80 mg/g (IQR 145.70–465.48) compared to 158.60 mg/g (IQR 35.40–436.30) in the dapagliflozin alone group (P = 0.023); at 6 months, the reductions were 323.70 vs 194.20 mg/g (P = 0.028) (Figure 2a). Percentage reductions were also greater in the combination therapy group at 3 months (63.43% vs 47.84%; P = 0.007) and 6 months (66.89% vs 40.81%; P = 0.002) (Figure 2b).
 |
Figure 2 Changes in UACR from baseline between the two groups after propensity score matching. (a) Absolute reduction in UACR (mg/g) after 3 and 6 months of treatment. (b) Percentage reduction in UACR (%) after 3 and 6 months of treatment. *P<0.05; **P<0.01. |
Clinically Significant UACR Response
At 3 months, a ≥30% reduction in UACR was observed in 28 of 33 patients (84.85%, 95% CI 69.08–93.35) in the combination group and 19 of 33 (57.58%, 95% CI 40.81–72.76) in the monotherapy group (P = 0.014). The proportion of patients achieving a ≥50% reduction was 20 of 33 (60.61%, 95% CI 43.68–75.32) vs 16 of 33 (48.48%, 95% CI 32.50–64.78) (P = 0.323) (Figure 3a). At 6 months, ≥30% reduction was observed in 31 of 33 (93.94%, 95% CI 80.39–98.32) vs 23 of 33 (69.70%, 95% CI 52.66–82.62) (P = 0.011), while ≥50% reduction was achieved in 28 of 33 (84.85%, 95% CI 69.08–93.35) in the combination group versus 15 of 33 (45.45%, 95% CI 29.84–62.01) in the monotherapy group (P < 0.001) (Figure 3b). These results support the superior and sustained albuminuria-lowering efficacy of combination therapy, which aligns with the KDIGO-recommended thresholds for improved renal outcomes.
 |
Figure 3 Proportion of patients achieving ≥30% or ≥50% reduction in UACR from baseline between the two groups after propensity score matching. (a) At 3 months of treatment. (b) At 6 months of treatment. *P<0.05; ***P<0.001. Abbreviation: ns, not significant. |
Renal Function Trajectories (eGFR)
Combination therapy significantly attenuated eGFR decline compared with monotherapy, with a progressively widening divergence over time. At 3 months, the median absolute change in eGFR was +0.50 mL/min/1.73 m2 (IQR, –2.00 to 4.00) in the combination group versus –2.00 (–5.00 to 1.00) in the monotherapy group (P = 0.007) (Figure 4a); the corresponding percentage changes were +0.63% (–2.65 to 5.41) versus –2.73% (–6.41 to 1.31) (P = 0.013). By 6 months, the between-group difference increased further: +2.00 (–2.00 to 6.00) versus –3.00 (–6.00 to –1.00) mL/min/1.73 m2 (P < 0.001), and +2.06% (–3.82 to 7.14) versus –5.08% (–8.67 to –1.11) (P < 0.001) (Figure 4b).
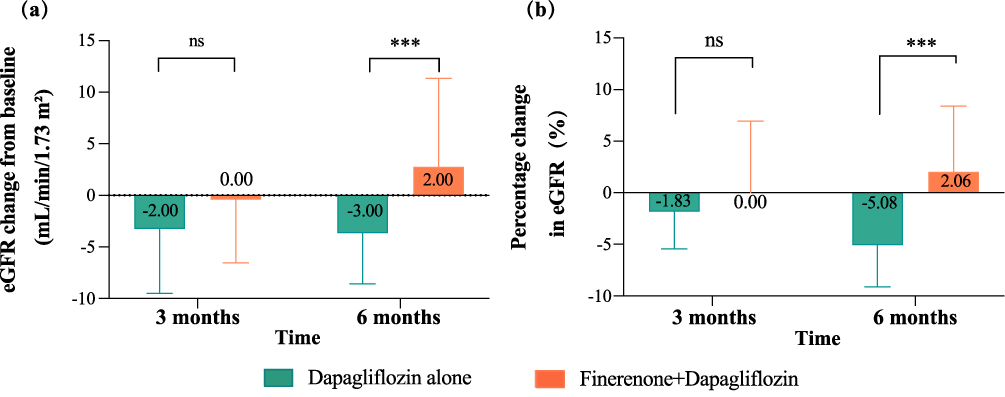 |
Figure 4 Changes in eGFR from baseline between the two groups after propensity score matching. (a) Absolute change in eGFR (mL/min/1.73 m2) at 3 and 6 months of treatment. (b) Percentage change in eGFR (%) at 3 and 6 months of treatment. ***P<0.001. Abbreviation: ns, not significant. |
Mediation Results
To assess whether early albuminuria reduction mediated the renoprotective effects of finerenone-dapagliflozin combination therapy, we performed mediation analysis using the percentage reduction in UACR at 3 months (vs baseline) as the mediator variable and the percentage change in eGFR from 3 to 6 months (vs 3-month value) as the dependent variable.
At 3 months, the combination therapy group demonstrated a significantly greater reduction in UACR than the monotherapy group (β = 37.12; 95% CI: 7.90–66.33; P = 0.015). This was associated with a significant total effect of treatment on the eGFR percentage change between 3 and 6 months (β = 6.10; 95% CI: 0.64–10.50; P = 0.040). However, after adjusting for UACR reduction, the direct effect remained only marginally significant (β = 5.88; 95% CI: –0.50 to 10.74; P = 0.080), and the path from UACR reduction to eGFR change was not significant (β = 0.00; 95% CI: –0.04 to 0.04; P = 0.871). The non-significant indirect effect accounted for only 1.45% of the total effect. This indicates that the renal protection of finerenone-dapagliflozin operates predominantly through albuminuria-independent mechanisms (Table 3 and Figure 5).
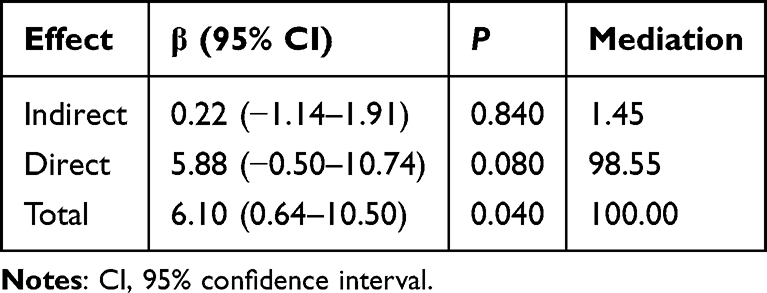 |
Table 3 Mediation Analysis: Relationship Between Early UACR Reduction and eGFR Change in the Finerenone Combined with Dapagliflozin Group |
 |
Figure 5 Mediation analysis showing the main results. Standardized regression coefficients and corresponding P values are presented, together with the relative contributions of the direct and indirect effects to the total effect. |
Secondary Outcomes
Blood Pressure Changes
Over the 6-month follow-up, both Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP)showed a modest downward trend in both treatment groups. In the monotherapy group, SBP decreased from 129.18 ± 15.55 mmHg at baseline to 125.39 ± 12.71 mmHg at 6 months. Similarly, in the combination therapy group, SBP declined from 129.88 ± 11.75 mmHg to 124.18 ± 8.94 mmHg. For DBP, the values decreased from 81.39 ± 10.24 mmHg to 79.15 ± 6.82 mmHg in the monotherapy group, and from 78.76 ± 7.09 mmHg to 75.58 ± 6.46 mmHg in the combination group. A significant time effect was observed for both SBP (F = 28.145, P < 0.001) and DBP (F = 16.733, P < 0.001), while no significant group effect or group-by-time interaction was found (Table 4).
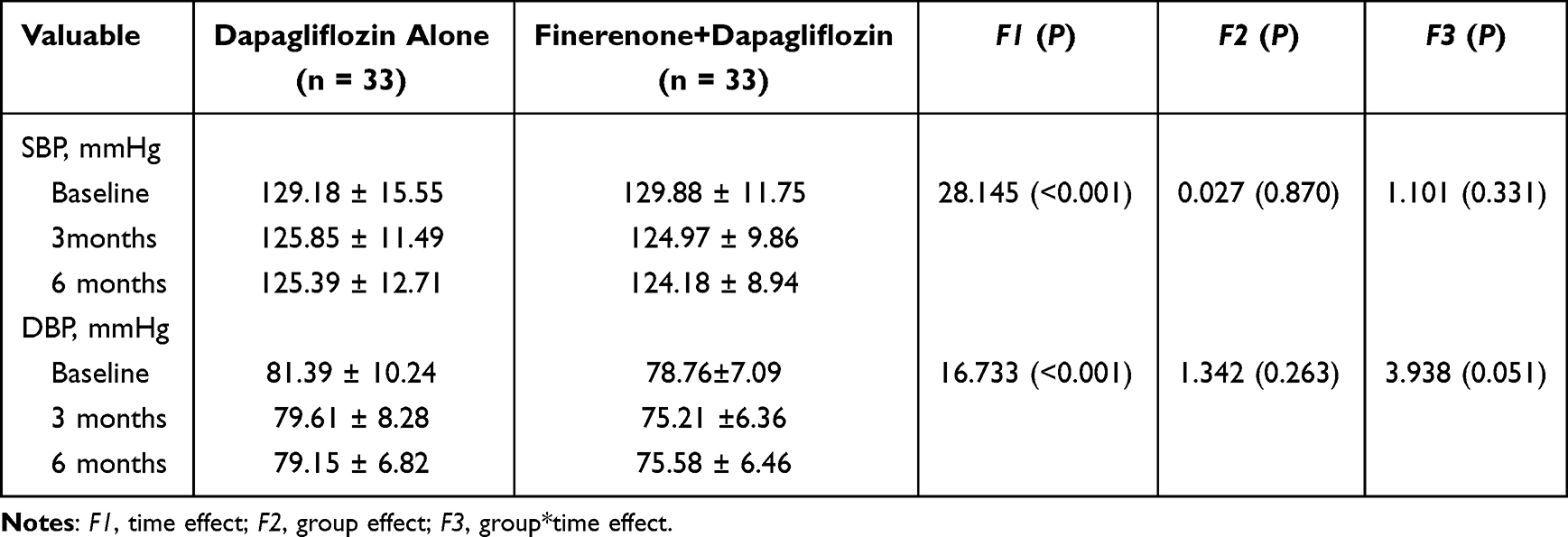 |
Table 4 Longitudinal Changes in SBP and DBP During Follow-Up in the Two Groups |
Serum Albumin, Uric Acid, Sodium, or Hemoglobin
Repeated-measures ANOVA showed no significant longitudinal changes in serum albumin, uric acid, sodium, or hemoglobin. Albumin showed no time effect (F1 = 1.205, P = 0.277), group difference (F2 = 0.000, P = 0.996), or interaction (F3 = 0.519, P = 0.474). Uric acid remained stable (time: F1 = 0.173, P = 0.679; group: F2 = 2.329, P = 0.132; interaction: F3 = 0.858, P = 0.358). Sodium and hemoglobin also showed no significant changes (sodium: F1 = 1.184, P = 0.281; F2 = 0.030, P = 0.864; F3 = 0.098, P = 0.755; hemoglobin: F1 = 1.551, P = 0.217; F2 = 0.101, P = 0.752; F3 = 0.246, P = 0.622).
Blood glucose levels declined significantly over time (F1 = 6.537, P = 0.013), with median reductions from 5.43 to 5.26 mmol/L in the monotherapy group and from 5.41 to 5.32 mmol/L in the combination group. Group (F2 = 1.008, P = 0.319) and interaction (F3 = 3.642, P = 0.061) effects were not significant. Serum potassium exhibited an upward trend over time (F1 = 12.125, P < 0.001), increasing from 4.14 (4.04–4.39) to 4.19 (4.04–4.41) mmol/L in the dapagliflozin group and from 4.13 (3.97–4.42) to 4.34 (4.07–4.64) mmol/L in the combination group. The absolute changes, however, were minimal, with no significant between-group differences (F2 = 0.122, P = 0.728) or time × group interaction effects (F3 = 1.459, P = 0.231) (Table 5).
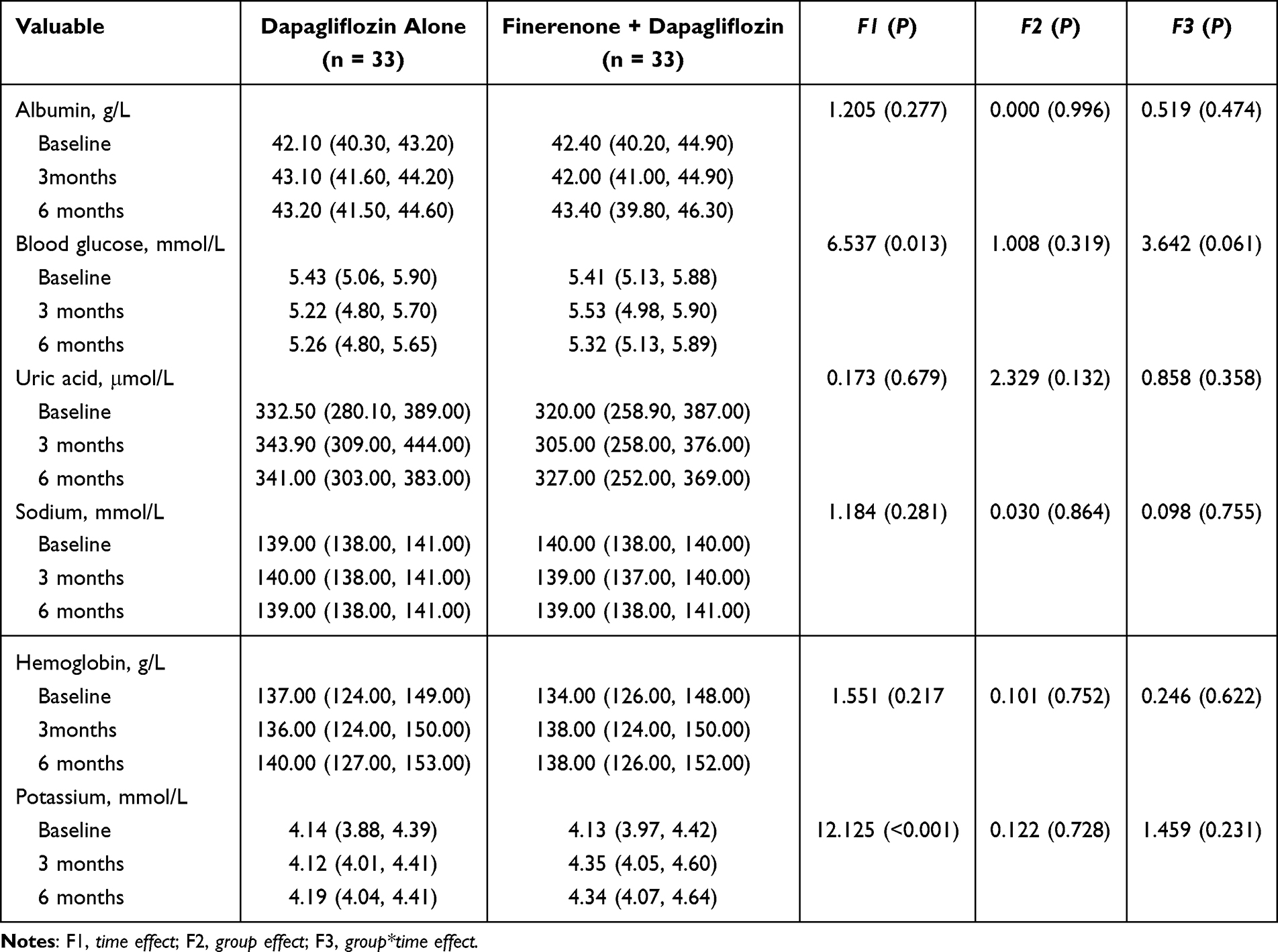 |
Table 5 Longitudinal Changes in Serum Albumin, Glucose, Uric Acid, Electrolytes, and Hemoglobin in Two Treatment Groups |
Safety and Adverse Events
Adverse events occurred in eight patients (24.2%) receiving dapagliflozin alone and 11 patients (33.3%) receiving finerenone —dapagliflozin combination therapy (P = 0.587). Urinary tract infection was the most frequent event in the monotherapy group (12.1% [4/33] vs 6.1% [2/33] with combination therapy; P = 0.672). Hyperkalemia demonstrated a numerically higher incidence with combination therapy (15.2% [5/33] vs 6.1% [2/33]; P = 0.427), with all cases managed per protocol using potassium-binding agents without treatment discontinuation. Other events (3.0% [1/33]) included hypotension, hyponatremia, and genital fungal infection in both groups, with additional upper-limb venous thrombosis in the combination group. The thrombosis event was adjudicated as treatment-unrelated and resolved with rivaroxaban. All adverse events were mild to moderate (CTCAE v5.0 grade 1–2), resolved through standard interventions, and no treatment-related serious adverse events, discontinuations, or deaths occurred (Table 6).
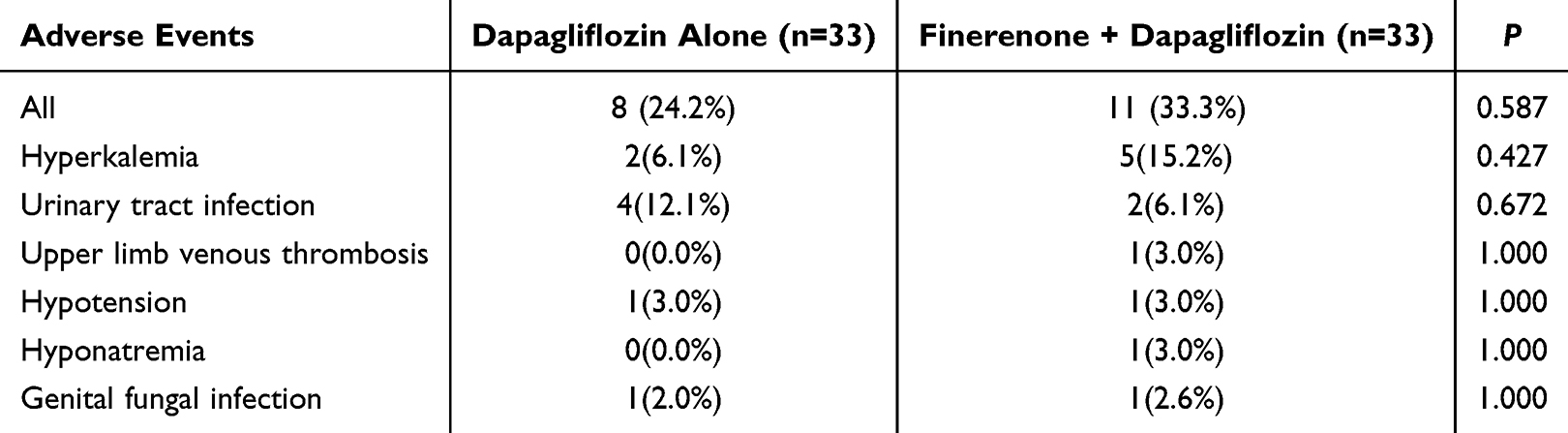 |
Table 6 Adverse Events |
Discussion
Progressive CKD is common determined at a late stage by sustaining eGFR decline and/or obvious albuminuria symptoms.33–35 In CKD, functional impairment is associated with renal fibrosis characterized by inflammatory cell infiltration, tubular atrophy, rarefaction of peritubular capillaries and excessive accumulation of extracellular matrix.36–41 ACEIs and ARBs are recommended as a first-line therapy and as a rescue therapy in CKD patients with cardiovascular disease and in those with diabetes-related and diabetes-independent CKD.42–44 However, chronic ACEI or ARB administration leads to increasing the levels of angiotensin II and aldosterone, which is known as angiotensin II and aldosterone escape.
This single-center, real-world, retrospective cohort study provides compelling evidence supporting the potential additive effects between finerenone, a non-steroidal mineralocorticoid receptor antagonist (nsMRA), and dapagliflozin, a SGLT2i, in patients with non-diabetic CKD. Over a 6-month observation period, the combination therapy group achieved a 67% reduction in UACR, which was substantially greater than the 51% reduction observed with dapagliflozin monotherapy. Furthermore, while the monotherapy group experienced a modest decline in eGFR (−2 mL/min/1.73 m2), the combination group showed eGFR stabilization or mild improvement (+1 mL/min/1.73 m2).
Although the combination group exhibited a slight increase in serum potassium levels, the incidence of clinically significant hyperkalemia or other adverse effects, such as liver dysfunction or genitourinary infections, was not significantly different between the groups. These findings suggest that dual-agent therapy is not only efficacious but also well tolerated, supporting its potential integration into routine clinical management for patients with non-diabetic CKD and persistent albuminuria despite optimized RAS blockade.
Although combination therapy with finerenone and dapagliflozin significantly reduced proteinuria at 3 months and improved the short-term eGFR trajectory from 3 to 6 months, mediation analysis revealed that its renoprotective effect was not significantly mediated by the early reduction in proteinuria. These findings suggest that the renal benefits observed in patients with non-diabetic CKD may not be solely attributable to antiproteinuric effects but rather involve the interplay of multiple underlying mechanisms.45
The potentially additive effects between finerenone and SGLT2i in non-diabetic CKD likely arises from their complementary mechanisms. Finerenone selectively blocks MR signaling, suppressing profibrotic and proinflammatory mediators such as transforming growth factor beta 1 (TGF-β1), Tumor necrosis factor-α, and interleukin-6, thereby reducing glomerulosclerosis and tubulointerstitial injury.46,47 SGLT2i improve glomerular hemodynamics and exert additional anti-inflammatory, antioxidant, and antifibrotic effects, including inhibition of complement activation, TGF-β1/MAPK signaling, and oxidative stress.21,48,49
Preclinical data from Col4a3−/− mice (Alport model) further support these potentially additive effects. Triple therapy (finerenone, SGLT2i, and RAS blockade) resulted in superior preservation of glomerular and tubulointerstitial structures compared to dual therapy. Transcriptomic analyses confirmed broader downregulation of injury- and fibrosis-related gene pathways, while histological findings showed enhanced integrity of the filtration barrier. Notably, finerenone mitigated residual tubulointerstitial damage often unaddressed by SGLT2i/RAS blockade alone, and improved key renal biomarkers, including BUN, serum creatinine, and UACR.50 These findings support MR antagonism as a critical third pillar in CKD treatment, enabling a multi-pathway, multi-compartment therapeutic strategy.50
The renoprotective efficacy of nsMRAs and SGLT2i has been well established in DKD. Large randomized trials, including FIDELIO-DKD and FIGARO-DKD, have demonstrated that finerenone significantly reduces renal and cardiovascular endpoints in patients with type 2 diabetes and CKD.51–53 Similarly, the DAPA-CKD trial confirmed that dapagliflozin slows CKD progression in both diabetic and non-diabetic populations.54,55 A recent meta-analysis demonstrated that SGLT2i significantly delayed eGFR decline (MD = 1.35 mL/min/1.73 m2) and reduced UACR (MD = −24.47%) in patients with non-diabetic CKD without increasing adverse events.56 These findings have solidified SGLT2i as the first-line therapy for CKD management in current guidelines.57 Building on this evidence, the CONFIDENCE trial evaluated the efficacy of combining finerenone with an SGLT2i. At 6 months, the dual therapy led to a 52% reduction in UACR, with 29% and 32% greater reductions compared to finerenone and empagliflozin monotherapy, respectively—demonstrating a favorable additive effect and safety profile.27
Notably, our study observed an even greater reduction in UACR compared to the CONFIDENCE trial, which may be explained by several factors. First, our cohort exclusively included non-diabetic CKD patients, a population more likely to exhibit inflammation- and fibrosis-driven pathophysiology. These underlying mechanisms may enhance sensitivity to the complementary anti-inflammatory and antifibrotic effects of dual therapy. Second, our patients had lower baseline ACR levels, indicating earlier disease stages and potentially a larger therapeutic window for intervention. Third, the fixed 6-month follow-up likely captured the initial phase of response, during which albuminuria reductions are typically more pronounced. Finally, as an observational study, the possibility of selection bias cannot be excluded, since treatment decisions may have been influenced by unmeasured clinical variables.
Despite the robust evidence supporting SGLT2i, data regarding the use of finerenone in non-diabetic CKD—particularly in combination with SGLT2i—remain limited. Most available real-world studies focus predominantly on diabetic populations. For instance, a TriNetX cohort study reported that the combined use of Finerenone and SGLT2i reduced the risk of major adverse kidney events (MAKE), ESRD, and all-cause mortality compared to monotherapy.58 However, over 85% of the included patients had diabetes, limiting the relevance of non-diabetic CKD. Similarly, Hanouneh et al observed a 96% rate of >50% UACR reduction with dual therapy compared to 50% and 59% for SGLT2i or Finerenone alone, respectively; however, 92% of the cohort had diabetes.59
Emerging evidence from small studies suggests potential benefits of finerenone in non-diabetic CKD subtypes. In patients with IgAN, Tang et al reported a significant reduction in 24-hour urinary protein, from 1.07 to 0.49 g/day, after 3 months of finerenone treatment, with stable renal function.60 Similarly, Gao et al noted a 42% median reduction in UACR in a cohort of 49 patients with IgAN over a treatment period of 3–6 months.61 However, both studies were limited by small sample sizes, short durations, and the absence of control arms. More recently, Wang et al conducted a multicenter observational study with a larger IgAN cohort, which demonstrated that 6 months of finerenone therapy was associated with a clinically meaningful reduction in proteinuria without major safety concerns.62
Evidence for combination therapy in non-diabetic CKD remains sparse. One small open-label study of 20 patients reported a 36% reduction in UACR after 8 weeks of dapagliflozin plus finerenone, but also noted a significant decline in eGFR and limited follow-up duration.63 In this context, our study contributes real-world evidence from a broader and more representative non-diabetic CKD cohort with a longer follow-up period. Despite the inherent limitations of its retrospective design, we observed sustained albuminuria reduction and renal function preservation without increased rates of hyperkalemia or AKI, thus addressing key safety concerns previously raised in short-term studies. These findings support the hypothesis that finerenone and SGLT2i may offer additive effects in non-diabetic CKD. However, confirmation through large-scale prospective trials remains essential. The ongoing FIND-CKD study (N=1,584) will provide valuable long-term data on finerenone monotherapy in non-diabetic CKD; notably, 16.9% of the enrolled participants were already on SGLT2i at baseline, offering an opportunity to evaluate the combined effects within a unified framework.29
Hyperkalemia remains a significant safety concern with MRAs in patients with CKD, particularly when combined with RAAS inhibitors, such as ACEIs or ARBs.64,65 Meta-analyses have shown that finerenone increases the risk of hyperkalemia (RR ~2.2), often leading to treatment discontinuation.66 Nevertheless, current guidelines recommend against empiric dose reduction or premature withdrawal of RAASi or MRA therapy, highlighting the need for careful monitoring and individualized management.
In our study, all patients were maintained on background RAAS inhibition. Although the combination group exhibited elevated serum potassium levels, the incidence of clinically significant hyperkalemia or related adverse effects was comparable between the groups. This finding aligns with the FIDELIO-DKD study, in which finerenone resulted in increased potassium levels; however, severe incidents were infrequent with appropriate monitoring.51,67
Recent meta-analyses suggest that the addition of SGLT2i to RAASi + MRA therapy can reduce the risk of hyperkalemia. One network meta-analysis showed a significant decrease in hyperkalemia events, and another large meta-analysis involving over 11,000 patients reported a 39% relative risk reduction compared to MRA monotherapy.68,69 The proposed mechanism involves SGLT2i-induced natriuresis, enhanced distal sodium delivery, and subsequent stimulation of potassium excretion via sodium–potassium exchange.70,71
These effects support the continued use of dual therapy while minimizing electrolyte-related complications.72 For high-risk patients, potassium binders may offer additional protection by helping to maintain normokalemia. Integrating such agents into long-term treatment plans could expand the feasibility and safety of RAASi + MRA-based regimens in nephrology.73,74
Limitations
This study had several limitations that should be acknowledged. First, as a single-center retrospective cohort analysis, it was inherently subject to selection bias and does not permit causal inference; all observed associations should therefore be interpreted as exploratory and hypothesis-generating. Although we adjusted for key confounders using multivariable models and applied propensity score–based adjustment to balance measured baseline covariates, residual confounding may have persisted. Second, the follow-up period was relatively short, precluding a robust evaluation of long-term renal and cardiovascular outcomes. Third, the study did not include comparator groups receiving finerenone or ACEIs/ARBs monotherapy, which limited our ability to isolate the additive benefits of each agent. Additionally, treatment allocation was not randomized, and baseline characteristics, although comparable, may reflect residual confounding. Fifth, the sample size was modest, which may have reduced the statistical power to detect less-frequent adverse events or subgroup effects. Taken together, these limitations underscore the need for validation through prospective, multicenter randomized controlled trials with longer follow-up durations and more diverse populations.
Conclusion
In conclusion, this real-world, retrospective cohort study provides preliminary evidence that the combination of finerenone and SGLT2i may be associated with greater renoprotective effects in patients with non-diabetic CKD. The observed greater reduction in albuminuria and attenuation of short-term eGFR decline, along with an acceptable safety profile, suggest that dual-agent therapy could be a potential strategy for patients with persistent proteinuria despite optimized RAAS inhibition. However, these findings are preliminary and derived from a real-world, retrospective cohort. Future large-scale randomized controlled trials are essential to validate these observations, determine long-term clinical outcomes, and define the optimal therapeutic role of finerenone–SGLT2i combination therapy in the management of non-diabetic CKD.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work has been supported by Zhejiang Province Medicine and Health Technology Plan Project (2025KY1343), the Nature Science Foundation of Ningbo (2023J160), and the Key Research and Development Program of Ningbo (2023Z177).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
References
1. Matsushita K, Ballew SH, Wang AY, Kalyesubula R, Schaeffner E, Agarwal R. Epidemiology and risk of cardiovascular disease in populations with chronic kidney disease. Nat Rev Nephrol. 2022;18(11):696–16. doi:10.1038/s41581-022-00616-6
2. Li XJ, Shan QY, Wu X, Miao H, Zhao YY. Gut microbiota regulates oxidative stress and inflammation: a double-edged sword in renal fibrosis. CMLS. 2024;81(1):480. doi:10.1007/s00018-024-05532-5
3. McIntyre CW, Jain A. Dialysis and cognitive impairment. Nat Rev Nephrol. 2025. doi:10.1038/s41581-025-00960-3
4. Fang L, Li Q, Mu S, Wang X. Peritoneal dialysis complicated by severe acute pancreatitis: a case report. Integrative Medi Nephrol Androl. 2023;10(4):e00002. doi:10.1097/imna-d-23-00002
5. Shdaifat EA, Abu-Sneineh FT, Ibrahim AM. Quality of life and psychological distress in end-stage renal disease patients undergoing hemodialysis and transplantation. World J Nephrol. 2024;13(3):95739. doi:10.5527/wjn.v13.i3.95739
6. Youhua L. Kidney fibrosis: fundamental questions, challenges, and perspectives. Integrative Medi Nephrol Androl. 2024;11(4):e24–00027. doi:10.1097/imna-d-24-00027
7. Huang R, Fu P, Ma L. Kidney fibrosis: from mechanisms to therapeutic medicines. Signal Transduct Target Ther. 2023;8(1):129. doi:10.1038/s41392-023-01379-7
8. Hall AM. Protein handling in kidney tubules. Nat Rev Nephrol. 2025;21(4):241–252. doi:10.1038/s41581-024-00914-1
9. Blum MF, Neuen BL, Grams ME. Risk-directed management of chronic kidney disease. Nat Rev Nephrol. 2025;21(5):287–298. doi:10.1038/s41581-025-00931-8
10. Deodhare KG, Pathak N. Hypertension and associated complications in pregnant women with chronic kidney disease. World J Nephrol. 2024;13(4):100680. doi:10.5527/wjn.v13.i4.100680
11. Yang X, Bayliss G, Zhuang S. Obesity-related glomerulopathy: epidemiology, pathogenesis, and current treatments. Integrative Medi Nephrol Androl. 2024;11(3):e24–00011. doi:10.1097/imna-d-24-00011
12. Raikou VD. Renoprotective strategies. World J Nephrol. 2024;13(1):89637. doi:10.5527/wjn.v13.i1.89637
13. Loutradis C, Ferro CJ, Sarafidis P, Price A. Renin-angiotensin system blockade in patients with chronic kidney disease: benefits, problems in everyday clinical use, and open questions for advanced renal dysfunction. J Human Hypertens. 2021;35(6):499–509. doi:10.1038/s41371-021-00504-9
14. Sarafidis P, Pella E, Kanbay M, Papagianni A. SGLT-2 Inhibitors and Nephroprotection in Patients with Diabetic and Non-diabetic Chronic Kidney Disease. Curr Med Chem. 2023;30(18):2039–2060. doi:10.2174/0929867329666220825121304
15. Sarafidis P, Alexandrou M-E, Ferro C, et al. Mineralocorticoid receptor antagonist use in chronic kidney disease with type 2 diabetes: a clinical practice document by the European Renal Best Practice (ERBP) board of the European Renal Association (ERA). Clin Kidney J. 2023;16(11):1885–1907. doi:10.1093/ckj/sfad139
16. Forbes A, Gallagher H. Chronic kidney disease in adults: assessment and management. Clin Med. 2020;20(2):128–132. doi:10.7861/clinmed.cg.20.2
17. DeFronzo RA, Reeves WB, Awad AS. Pathophysiology of diabetic kidney disease: impact of SGLT2 inhibitors. Nat Rev Nephrol. 2021;17(5):319–334. doi:10.1038/s41581-021-00393-8
18. Zhao BR, Hu XR, Wang WD, Zhou Y. Cardiorenal syndrome: clinical diagnosis, molecular mechanisms and therapeutic strategies. Acta Pharmacol Sin. 2025;46(6):1539–1555. doi:10.1038/s41401-025-01476-z
19. Hoda F, Negi H, Saini D, et al. Navigating the therapeutic landscape of SGLT2 inhibitors in diabetes management: exploring efficacy and emerging concerns. Explor Med. 2024;5(6):774–796. doi:10.37349/emed.2024.00255
20. Taheri S. Heterogeneity in cardiorenal protection by sodium glucose cotransporter 2 inhibitors in heart failure across the ejection fraction strata: systematic review and meta-analysis. World J Nephrol. 2023;12(5):182–200. doi:10.5527/wjn.v12.i5.182
21. Dharia A, Sridhar VS, Cherney DZI, Khan A. SGLT2 Inhibitors: the Sweet Success for Kidneys. Ann Rev Med. 2023;74(1):369–384. doi:10.1146/annurev-med-042921-102135
22. Mima A. A Narrative Review of Diabetic Kidney Disease: previous and Current Evidence-Based Therapeutic Approaches. Adv Ther. 2022;39(8):3488–3500. doi:10.1007/s12325-022-02223-0
23. Herrington WG, Haynes R. Diabetic Kidney Disease — semaglutide Flows into the Mainstream. N Engl J Med. 2024;391(2):178–179. doi:10.1056/nejme2406408
24. Rossing P, Filippatos G, Agarwal R, et al. Finerenone in Predominantly Advanced CKD and Type 2 Diabetes With or Without Sodium-Glucose Cotransporter-2 Inhibitor Therapy. Kidney Int Rep. 2021;7(1):36–45. doi:10.1016/j.ekir.2021.10.008
25. Bakris GL, Ruilope LM, Anker SD, et al. A prespecified exploratory analysis from FIDELITY examined finerenone use and kidney outcomes in patients with chronic kidney disease and type 2 diabetes. Kidney Int. 2022;103(1):196–206. doi:10.1016/j.kint.2022.08.040
26. Morita R, Tsukamoto S, Obata S, et al. Effects of sodium-glucose cotransporter 2 inhibitors, mineralocorticoid receptor antagonists, and their combination on albuminuria in diabetic patients. Diabetes Obes Metab. 2023;25(5):1271–1279. doi:10.1111/dom.14976
27. Agarwal R, Green JB, Heerspink HJL, et al. Finerenone with Empagliflozin in Chronic Kidney Disease and Type 2 Diabetes. N Engl J Med. 2025. doi:10.1056/NEJMoa2410659
28. Levey AS, Eckardt KU, Tsukamoto Y, et al. Definition and classification of chronic kidney disease: a position statement from Kidney Disease: improving Global Outcomes (KDIGO). Kidney Int. 2005;67(6):2089–2100. doi:10.1111/j.1523-1755.2005.00365.x
29. Heerspink HJL, Agarwal R, Bakris GL, et al. Design and baseline characteristics of the Finerenone, in addition to standard of care, on the progression of kidney disease in patients with Non-Diabetic Chronic Kidney Disease (FIND-CKD) randomized trial. Nephrol Dial Transplant. 2025;40(2):308–319. doi:10.1093/ndt/gfae132
30. Chapman D, Judge PK, Sardell RJ, et al. Interference of urinary albumin-to-creatinine ratio measurement by glycosuria: clinical implications when using SGLT-2 inhibitors. Kidney Int. 2023;103(4):787–790. doi:10.1016/j.kint.2022.12.027
31. Stevens PE, Levin A. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013;158(11):825–830. doi:10.7326/0003-4819-158-11-201306040-00007
32. Schold JD, Navaneethan SD, Jolly SE, et al. Implications of the CKD-EPI GFR estimation equation in clinical practice. Clin J Am Soc Nephrol. 2011;6(3):497–504. doi:10.2215/cjn.04240510
33. Glastras SJ, Pollock CA. Targeted identification of risk and treatment of diabetic kidney disease. Nat Rev Nephrol. 2024;20(2):75–76. doi:10.1038/s41581-023-00796-9
34. Tran TTT, Ha TK, Phan NM, Le MV, Nguyen TH. Detection of decline in estimated glomerular filtration rate in patients with type 2 diabetes by cystatin C-based equations. World J Nephrol. 2024;13(4):95761. doi:10.5527/wjn.v13.i4.95761
35. Liu D, Chen X, He W, et al. Update on the pathogenesis, diagnosis, and treatment of diabetic tubulopathy. Integrative Medi Nephrol Androl. 2024;11(4):e23–00029.
36. De Gregorio V, Barua M, Lennon R. Collagen formation, function and role in kidney disease. Nat Rev Nephrol. 2025;21(3):200–215. doi:10.1038/s41581-024-00902-5
37. Chung JY-F, Zhang -Y-Y, ZZ-Y J, et al. Immunodynamics of macrophages in renal fibrosis. Integrative Medi Nephrol Androl. 2023;10(3):e00001. doi:10.1097/imna-d-23-00001
38. Ren LL, Miao H, Wang YN, Liu F, Li P, Zhao YY. TGF-β as a master regulator of aging-associated tissue fibrosis. Aging and Disease. 2023;14(5):1633–1650. doi:10.14336/ad.2023.0222
39. Balakumar P. Unleashing the pathological role of epithelial-to-mesenchymal transition in diabetic nephropathy: the intricate connection with multifaceted mechanism. World J Nephrol. 2024;13(2):95410. doi:10.5527/wjn.v13.i2.95410
40. Ma FY, Tesch GH, Grynberg K, Ozols E, Mulley WR, Nikolic-Paterson DJ. A model of ischaemia-induced renal interstitial fibrosis in mice with established diabetes. Integrative Medi Nephrol Androl. 2023;10(2):e00032.
41. Cao G, Miao H, Wang YN, et al. Intrarenal 1-methoxypyrene, an aryl hydrocarbon receptor agonist, mediates progressive tubulointerstitial fibrosis in mice. Acta Pharmacol Sin. 2022;43(11):2929–2945. doi:10.1038/s41401-022-00914-6
42. Abbad L, Esteve E, Chatziantoniou C. Advances and challenges in kidney fibrosis therapeutics. Nat Rev Nephrol. 2025;21(5):314–329. doi:10.1038/s41581-025-00934-5
43. Chinnadurai R, HHL W, Abuomar J, et al. Antihypertensive prescribing patterns in non-dialysis dependent chronic kidney disease: findings from the Salford Kidney Study. World J Nephrol. 2023;12(5):168–181. doi:10.5527/wjn.v12.i5.168
44. Correa-Rotter R, Maple-Brown LJ, Sahay R, Tuttle KR, Ulasi II. New and emerging therapies for diabetic kidney disease. Nat Rev Nephrol. 2024;20(3):156–160. doi:10.1038/s41581-023-00782-1
45. Agarwal R, Bakris GL, Pitt B, et al. Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: the FIDELITY pooled analysis. Eur Heart J. 2021;43(6):474–484. doi:10.1093/eurheartj/ehab777
46. Shah M, Awad A, Abdel-Rahman E. Nonsteroidal Mineralocorticoid Receptor Antagonist (Finerenone) in Cardiorenal Disease. J Clin Med. 2023;12(19):6285. doi:10.3390/jcm12196285
47. Barrera-Chimal J, Bakris GL, Jaisser F, Lima-Posada I. Mineralocorticoid receptor antagonists in diabetic kidney disease - mechanistic and therapeutic effects. Nat Rev Nephrol. 2021;18(1):56–70. doi:10.1038/s41581-021-00490-8
48. Salvatore T, Lettieri M, Marfella R, et al. An Overview of the Cardiorenal Protective Mechanisms of SGLT2 Inhibitors. Int J Mol Sci. 2022;23(7):3651. doi:10.3390/ijms23073651
49. Ala M. SGLT2 Inhibition for Cardiovascular Diseases, Chronic Kidney Disease, and NAFLD. Endocrinology. 2021;162(12):157. doi:10.1210/endocr/bqab157
50. Zhu Z, Gross O, Romagnani P, et al. Finerenone Added to RAS/SGLT2 Blockade for CKD in Alport Syndrome. Results of a Randomized Controlled Trial with Col4a3-/- Mice. JASN. 2023;34(9):1513–1520. doi:10.1681/asn.0000000000000186
51. Bakris GL, Agarwal R, Anker SD, et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N Engl J Med. 2020;383(23):2219–2229. doi:10.1056/NEJMoa2025845
52. Agarwal R, Anker SD, Filippatos G, et al. Effects of canagliflozin versus finerenone on cardiorenal outcomes: exploratory post hoc analyses from FIDELIO-DKD compared to reported CREDENCE results. Nephrol Dial Transplant. 2022;37(7):1261–1269. doi:10.1093/ndt/gfab336
53. Ruilope LM, Pitt B, Anker SD, et al. Kidney outcomes with finerenone: an analysis from the FIGARO-DKD study. Nephrol Dial Transplant. 2023;38(2):372–383. doi:10.1093/ndt/gfac157
54. Wheeler DC, Toto RD, Stefánsson BV, et al. A pre-specified analysis of the DAPA-CKD trial demonstrates the effects of dapagliflozin on major adverse kidney events in patients with IgA nephropathy. Kidney Int. 2021;100(1):215–224. doi:10.1016/j.kint.2021.03.033
55. Wheeler DC, Stefánsson BV, Jongs N, et al. Effects of dapagliflozin on major adverse kidney and cardiovascular events in patients with diabetic and non-diabetic chronic kidney disease: a prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021;9(1):22–31. doi:10.1016/s2213-8587(20)30369-7
56. Cleveland KH, Schnellmann RG. Pharmacological Targeting of Mitochondria in Diabetic Kidney Disease. Review Pharmacol Rev. 2023;75(2):250–262. doi:10.1124/pharmrev.122.000560
57. Iordan L, Gaita L, Timar R, Avram V, Sturza A, Timar B. The Renoprotective Mechanisms of Sodium-Glucose Cotransporter-2 Inhibitors (SGLT2i)-A Narrative Review. Int J Mol Sci. 2024;25(13):7057. doi:10.3390/ijms25137057
58. Chuang MH, Wang HY, Kan WC, et al. Cardio-Kidney Outcomes for Combined versus Monotherapy with Finerenone or SGLT2 Inhibitors in Patients with CKD. Nephrol Dial Transplant. 2025. doi:10.1093/ndt/gfaf064
59. Hanouneh M, Le D, Jaar BG, Tamargo C, Cervantes CE. Real-Life Experience on the Effect of SGLT2 Inhibitors vs. Finerenone vs. Combination Albuminuria in Chronic Kidney Disease Diagnostics. 2024;14(13):1357. doi:10.3390/diagnostics14131357
60. Tang C, Si FL, Chen P, et al. Effectiveness and safety of finerenone in non-diabetic patients with IgA nephropathy. J Nephrol. 2025. doi:10.1007/s40620-025-02240-6
61. Gao Q, Lin H, Zhao Z, et al. Effectiveness and safety of finerenone in the treatment of IgA Nephrology patients: a retrospective, real-world study. Int Urol Nephrol. 2025. doi:10.1007/s11255-025-04512-3
62. Wang QR, Wu L, Huang J, et al. Efficacy and safety of finerenone in IgA nephropathy: an observational multicentre study. Clin Kidney J. 2025;18(5):sfaf125. doi:10.1093/ckj/sfaf125
63. Mårup FH, Thomsen MB, Birn H. Additive effects of dapagliflozin and finerenone on albuminuria in non-diabetic CKD: an open-label randomized clinical trial. Clin Kidney J. 2024;17(1):sfad249. doi:10.1093/ckj/sfad249
64. Morales J, Palmer BF. Non-steroidal mineralocorticoid antagonists and hyperkalemia monitoring in chronic kidney disease patients associated with type II diabetes: a narrative review. Postgrad Med. 2024;136(2):111–119. doi:10.1080/00325481.2024.2316572
65. Yang S, Zhao L, Mi Y, He W. Effects of sodium-glucose cotransporter-2 inhibitors and aldosterone antagonists, in addition to renin-angiotensin system antagonists, on major adverse kidney outcomes in patients with type 2 diabetes and chronic kidney disease: a systematic review and network meta-analysis. Diabetes Obes Metab. 2022;24(11):2159–2168. doi:10.1111/dom.14801
66. Fnu J, Kamran M, Tirath P, et al. A Systematic Review and Meta-Analysis on the Efficacy and Safety of Fi nerenone Therapy in Patients with Cardiovascular and Chronic Kidney Di seases in Type 2 Diabetes Mellitus. Cureus. 2023;2023:41746. doi:10.7759/cureus.41746
67. Agarwal R, Pitt B, Kolkhof P, et al. Investigating new treatment opportunities for patients with chronic kidney disease in type 2 diabetes: the role of finerenone. Nephrology Diialysis Transplantation. 2020;37(6):1014–1023. doi:10.1093/ndt/gfaa294
68. Yuan Y, Chen C, Lin Y, et al. Incidence of hyperkalemia RAASi and SGLT-2i treatment in individuals with diabetic kidney disease: a systematic review and network meta-analysis. Front Pharmacol. 2024;15:1462965. doi:10.3389/fphar.2024.1462965
69. Cordovez RAB, Rivera KA, Denila RW, Patricio MD. Effects of sodium glucose cotransporter 2 inhibitors on the risk of hyperkalemia in patients on mineralocorticoid receptor antagonist: a systematic review and meta-analysis. Eur Heart J. 2023;44(Supplement_1):
70. Packer M, Wilcox CS, Testani JM. Critical Analysis of the Effects of SGLT2 Inhibitors on Renal Tubular Sodium, Water and Chloride Homeostasis and Their Role in Influencing Heart Failure Outcomes. Circulation. 2023;148(4):354–372. doi:10.1161/circulationaha.123.064346
71. Ravindran S, Munusamy S. Renoprotective mechanisms of sodium-glucose co-transporter 2 (SGLT2) inhibitors against the progression of diabetic kidney disease. J Cell Physiol. 2021;237(2):1182–1205. doi:10.1002/jcp.30621
72. Costa D, Zicarelli M, Coppolino G, et al. Hyperkalemia in CKD: an overview of available therapeutic strategies. Front Med. 2023;10:1178140. doi:10.3389/fmed.2023.1178140
73. Silva-Cardoso J, Frazão JM, Bettencourt P, et al. Management of RAASi-associated hyperkalemia in patients with cardiovascular disease. Heart Failure Rev. 2021;26(4):891–896. doi:10.1007/s10741-020-10069-3
74. Paolillo S, Basile C, Dell’Aversana S, et al. Novel potassium binders to optimize RAASi therapy in heart failure: a systematic review and meta-analysis. Eur J Internal Med. 2023;119:109–117. doi:10.1016/j.ejim.2023.08.022
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.