Back to Journals » Drug Design, Development and Therapy » Volume 20
Efficacy and Safety of Everolimus in Advanced Unresectable and Progressive Epithelioid Hemangioendothelioma: A Single-Center Case Series
Authors Tan H, Wang H ![]() , Sun Y, Ying J, Chi Y
, Sun Y, Ying J, Chi Y
Received 12 July 2025
Accepted for publication 15 May 2026
Published 26 May 2026 Volume 2026:20 553262
DOI https://doi.org/10.2147/DDDT.S553262
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Huijing Tan,1,* Huike Wang,1,* Yuting Sun,1 Jianming Ying,2 Yihebali Chi1
1Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, People’s Republic of China; 2Department of Pathology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yihebali Chi, Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, 17 South Panjiayuan Lane, Chaoyang District, Beijing, 100021, People’s Republic of China, Email [email protected]
Background: Epithelioid hemangioendothelioma (EHE) is an ultra-rare vascular sarcoma, with the liver and lungs as the predominant primary sites. To date, no standard systemic therapy has been established for advanced EHE. This study aimed to evaluate the efficacy and safety of everolimus in patients with advanced, unresectable, and progressive EHE.
Methods: This case series retrospectively included 11 patients with advanced, progressive EHE who received systemic therapy with everolimus at our hospital spanning a 3-year period. The clinical outcomes, including time to treatment failure (TTF), overall survival (OS), objective response rate (ORR), disease control rate (DCR), and adverse events (AEs), were analyzed. The median follow-up time was estimated using the reverse Kaplan–Meier method.
Results: At the data cutoff (April 11, 2025), the median follow-up time was 21.9 months. The median TTF was 21.3 months, and median OS was not reached at the time of analysis. All 11 cases achieved stable disease (SD); the ORR was 0% (0/11), and the DCR was 100.0% (11/11). The most common AEs were mucositis accompanied by multiple oral ulcers (54.5%), which was limited to grade 1– 2 severity. One patient (9.1%) experienced grade 3 upper gastrointestinal bleeding. Other AEs included interstitial pneumonia (27.3%), rash (18.2%), and thrombocytopenia (18.2%). No grade 4 or 5 AEs were observed.
Conclusion: Everolimus showed preliminary activity, primarily disease stabilisation, in this small retrospective case series of patients with advanced, unresectable, and progressive EHE. Further studies with larger cohorts are warranted to validate these findings.
Keywords: epithelioid hemangioendothelioma, targeted therapy, mTOR inhibitor, everolimus, adverse events
Introduction
Epithelioid hemangioendothelioma (EHE) is an extremely rare vascular soft tissue sarcoma, with a global annual incidence of 0.038 per 100,000 and a prevalence of less than 1 per 1,000,000.1 The liver and lungs are the two most common primary sites. Approximately 20–30% of patients develop metastatic disease, with a reported median overall survival (OS) of 4.6 years and a 5-year survival rate of 78.8%.2–4 EHE is a tumor of intermediate malignant potential, occupying a position between completely benign hemangiomas and highly aggressive angiosarcomas.5 Notably, tumor markers for EHE are typically within normal ranges, and it is often detected incidentally. Diagnosis primarily relies on histopathological examination and immunohistochemical staining for vascular endothelial and epithelial markers. In over 75% of hepatic EHE cases, patients present with multifocal liver lesions, while those with pulmonary EHE may exhibit lymph node involvement and wedge-shaped infarcts.6 To date, the etiology of EHE remains unclear.7 Some patients may experience symptoms such as abdominal pain, weight loss, or ascites.8 In severe cases, a massive tumor burden can lead to liver failure, spontaneous rupture,9 or metastatic complications such as pleural effusion.10
The development of EHE is associated with recurrent genetic alterations that drive tumorigenesis. The most characteristic alterations include the chromosomal translocations t(1;3)(p36;q25) and t(11;x)(q13;p11), which result in the formation of the WWTR1–CAMTA1 and YAP1–TFE3 fusion proteins, respectively. These fusion proteins function as aberrant transcription factors and are considered key oncogenic drivers in EHE.11 Approximately 90% of EHE cases harbor the WWTR1–CAMTA1 fusion, while all angiosarcomas are negative for this marker, making it useful in differential diagnosis.11 Only a small subset of patients (6–10%) harbor the YAP1-TFE3 fusion gene,12 with occasional reports of other fusion variants. Given the variable clinical course of EHE, ranging from spontaneous regression to indolent progression, an initial active surveillance strategy may be appropriate for selected patients. Treatment options include surgical resection for localized EHE, and in cases of advanced, unresectable, or metastatic disease, various systemic therapies, such as targeted therapies and chemotherapy, may be considered, but no standard systemic therapy has been established for EHE.13,14
Everolimus is an oral mammalian target of rapamycin (mTOR) inhibitor approved as an anti-cancer agent for treating various cancers. It acts by inhibiting the mTOR pathway, which is essential for tumor cell growth, proliferation, and survival.15–17 Although not specifically approved for EHE, its mechanism of action and inhibitory effects on tumor growth and angiogenesis provide a rationale for exploring everolimus as a potential treatment option for this ultra-rare vascular soft tissue sarcoma. In our hospital, everolimus has been used as a systemic treatment for patients with advanced, unresectable, or metastatic EHE. However, these data have not yet been systematically reported.
This study aimed to evaluate the efficacy and safety of everolimus in patients with advanced, progressive EHE, and to provide preliminary evidence to inform future research in this setting.
Materials and Methods
Study Subjects
This single-center case series included patients from the National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College (Beijing, China). All patients met the following eligibility criteria: histopathologically confirmed advanced, unresectable, and progressive EHE with imaging data, treatment initiation with everolimus between July 2021 and July 2024, at least one unidimensionally measurable lesion according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1; Eastern Cooperative Oncology Group (ECOG) performance status ≤2; age≥18 years; and an expected survival time of at least 3 months.
This study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice (GCP) guidelines. All patient data were anonymized to ensure confidentiality. The study protocol was approved by the Institutional Review Board (IRB), and the requirement for written informed consent was waived due to the retrospective nature of the study. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Treatment
Everolimus was initiated at a dose of 10 mg orally once daily. Treatment continued until disease progression or unacceptable toxicity. Dose reduction to 5 mg daily and/or treatment interruptions were implemented in cases of intolerable adverse events (AEs). If further dose adjustment was required, dosing every other day using the lowest available tablet strength could be considered. Each treatment cycle was defined as 28 days.
Efficacy Outcomes
Tumor response was assessed every two treatment cycles according to RECIST version 1.1 and categorized as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). The objective response rate (ORR) was defined as the proportion of patients achieving CR and PR, and the disease control rate (DCR) as the proportion achieving CR, PR, or SD.
Time to treatment failure (TTF) was defined as the time from the initiation of everolimus therapy to the first occurrence of any of the following events: radiological disease progression assessed according to RECIST criteria, all-cause death, or permanent treatment discontinuation due to intolerable treatment-related toxicity. Patients who remained on treatment without experiencing any failure event were censored at the last valid follow-up assessment. No radiological progression was required for patients discontinuing treatment because of toxicity. Overall survival (OS) was defined as the time from treatment initiation to death from any cause. The primary endpoint was TTF, while OS was evaluated as a secondary endpoint.
Changes in tumor size from baseline were visualized using waterfall plots (maximum percentage change per patient) and spider plots (longitudinal percentage change at each assessment time point). Treatment exposure and follow-up duration for individual patients were illustrated using swimmer plots.
Safety Assessment
AEs were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE), version 5.0. Safety was evaluated based on the incidence and severity of AEs.
Statistical Analysis
Continuous variables were summarized as median with interquartile range (IQR), and categorical variables were presented as counts and percentages. Missing data were handled by case-wise deletion, and no imputation was performed. Due to the small sample size, no formal statistical comparisons or hypothesis testing was conducted.
Time to treatment failure (TTF) and overall survival (OS) were estimated using the Kaplan–Meier method. The median follow-up time was calculated using the reverse Kaplan–Meier method, which appropriately accounts for censored observations.
Statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). GraphPad Prism version 10.1.2 and R software (version 4.0.1) were used for data visualization.
Results
Baseline Characteristics
A total of 11 patients with advanced, unresectable, and progressive EHE treated with everolimus were included. Among them, 7 patients received first-line therapy, 3 received second-line therapy, and 1 received third-line therapy. The study cohort comprised 7 males and 4 females, with a median age of 34 years (IQR: 31–58).
The median tumor size was 3.6 cm (IQR: 2.9–8.7). Ki-67 was available for 9 patients, with a median value of 5% (IQR: 5–10%). Primary tumors were predominantly located in the liver (n=9), with 2 patients presenting with pulmonary lesions. Detailed baseline characteristics are summarized in Table 1.
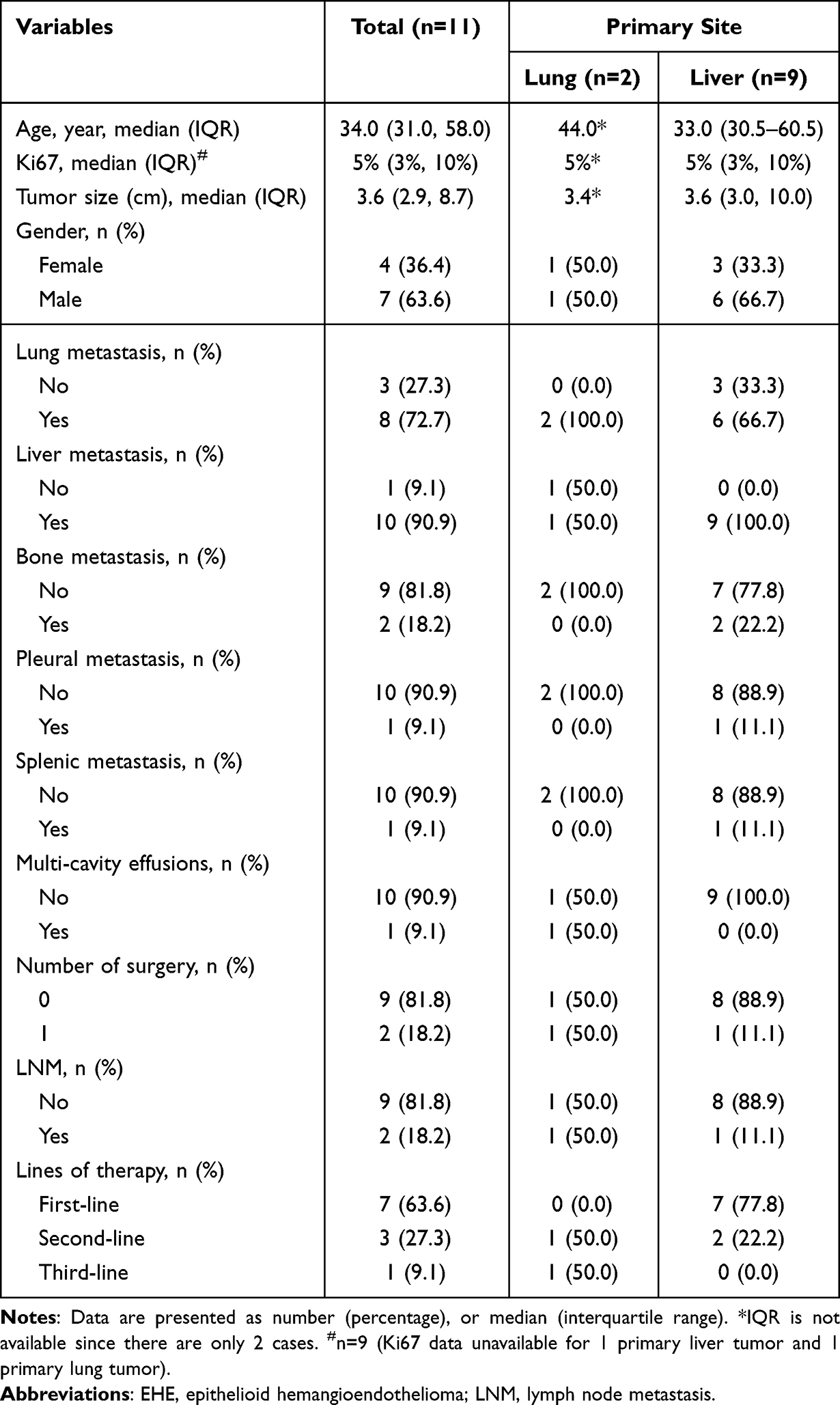 |
Table 1 Characteristics of the Study Patients with Advanced EHE |
Efficacy Outcomes
As of the data cut-off date (April 11, 2025), 4 patients (36.4%) remained on treatment, 4 patients (36.4%) discontinued due to intolerable toxicity and switched to alternative therapies, and 3 (27.3%) initiated next-line treatment following disease progression. All 11 patients achieved SD, resulting in an ORR of 0% (0/11) and a DCR of 100.0% (11/11). Treatment responses are illustrated in Figure 1.
 |
Figure 1 Overview of treatment responses in 11 patients with advanced, unresectable, and progressive EHE. The cut-off date for data analysis was April 11, 2025. Abbreviations: EHE, epithelioid hemangioendothelioma; mo, months; TTF, time to treatment failure. |
The longest observed TTF was 37.0 months in one patient, who discontinued everolimus after experiencing adverse events, including upper gastrointestinal bleeding.
Further short-term efficacy data and long-term prognostic outcomes are presented in Table 2, Figures 2 and 3. The median TTF was 21.3 months (Figure 4), with a total of 7 patients defined as events (3 with radiological disease progression, 4 with permanent treatment discontinuation due to intolerable toxicity), and the remaining 4 patients censored at their last follow-up without any treatment failure event. The median OS was not reached at the time of analysis, with 2 patients died (events), and 9 patients censored at the last follow-up. The median follow-up duration was 21.9 months.
 |
Table 2 Treatment Response and Survival Outcomes by Patient Characteristics |
 |
Figure 2 Changes in tumor size from baseline. (A) Waterfall plot analysis of the maximum percentage of tumor shrinkage from baseline in each patient (n=11). Bars are ordered from left to right according to the magnitude of tumor shrinkage; (B) Spider plot analysis of the percentage change in tumor size compared to baseline at each tumor response assessment. |
 |
Figure 3 Swimmer plot analysis of everolimus treatment duration and follow-up duration for each patient. The horizontal bars represent individual patients, with distinct segments indicating periods of treatment and follow-up. |
 |
Figure 4 Kaplan-Meier curve analysis of TTF in 11 patients. The median TTF was 21.3 months as of the cutoff date (April 11, 2025). Abbreviations: NR, not reached. TTF, time to treatment failure. |
AEs
Among the 11 patients, the most common AE was mucositis (54.5%), followed by interstitial pneumonitis (27.3%), rash (18.2%), and thrombocytopenia (18.2%). Most AEs were grade 1–2 in severity. One patient (9.1%) experienced grade 3 upper gastrointestinal bleeding. No grade 4 or 5 AEs were observed. Treatment discontinuation associated with AEs occurred in 4 patients (36.4%). Detailed safety data are presented in Table 3.
 |
Table 3 Summary of Adverse Events in 11 Patients |
Discussions
This study retrospectively analyzed a small cohort of advanced, unresectable, and progressive EHE patients who received systemic therapy with everolimus at our hospital. Given the rarity of EHE cases, which limits randomized controlled trials and results in inconsistent therapeutic approaches, and a lack of approved standardized treatments for advanced EHE,18 assessing clinical outcomes is critical for enhancing the management of this ultra-rare patient population. As of the cutoff date (April 11, 2025), the median TTF was 21.3 months, and the median OS was not reached.
Management options for EHE include anti-angiogenic agents, radiotherapy, chemoembolization, chemotherapy, surgical resection, and liver transplantation.19,20 A retrospective study of 228 EHE patients found 1-, 3-, and 5- year OS rates of 96.2%, 87.9%, and 84.9%, respectively, with no significant OS differences between surgical and non-surgical treatments.21 Surgical resection does not offer a survival advantage, and the role of liver transplantation in hepatic EHE, particularly in multifocal or infiltrative lesions, requires critical reevaluation, no prospective studies have yet defined its utility. Future research should focus on establishing standardized treatment selection criteria, noting that liver transplantation is generally not recommended for hepatic EHE with extrahepatic disease.21,22
A study found that approximately 25% of EHE patients received no treatment during their disease course; yet, 40% remained alive after a median follow-up of 32 months.23 The presence of metastases did not affect survival rates.23 Among 93 translocation-positive EHE patients, 83 harbored WWTR1-CAMTA1 fusions, and 10 had YAP1-TFE3 fusions. It was of note that 70% of WWTR1-CAMTA1-positive EHE patients presented with distant metastases at diagnosis, with 3- and 5-year OS rates of 70% and 59%, respectively. In contrast, 60% of YAP1-TFE3-positive patients also had distant metastases at diagnosis but achieved higher 3- and 5-year OS rates of 88% and 86%.24 These findings indicated that while EHE patients generally have a high 5-year OS rate, a subset exhibited markedly shortened survival and aggressive clinical progression, underscoring the intrinsic heterogeneity in tumor biology.4 LNM is a significant risk factor for recurrence and progression of EHE, and the primary tumor site also critically influences outcomes, with pulmonary and pleural involvement typically conferring poorer prognosis.25 However, the pulmonary subgroup consisted of only two patients, as did the LNM positive subgroup.
Systemic therapy is critical in treating patients with unresectable, progressive EHE, or significant symptoms. For EHE in deep soft tissues or visceral organs, chemotherapy may be preferred and active agents include platinum compounds, paclitaxel, doxorubicin, vinorelbine, gemcitabine, etoposide, ifosfamide, dacarbazine, cyclophosphamide, vincristine, pemetrexed, and 5-fluorouracil, with platinum-based regimens combined with paclitaxel being the most common.24 Combination regimens with anti-angiogenic therapies like bevacizumab have shown improved clinical outcomes, resulting in partial remission in some patients. Other agents such as thalidomide, lenalidomide, apatinib, and sorafenib have also been utilized, but most evidence comes from case reports or small studies, with a lack of Phase III clinical trial data. A retrospective analysis of 13 metastatic EHE patients treated with first-line pazopanib reported median progression-free survival (PFS) of 35.1 months and median OS of 53.8 months. Notably, patients with serous effusions/systemic symptoms had markedly poorer survival outcomes, suggesting pazopanib as a potential alternative.14 In a Phase II trial of trametinib for metastatic EHE, 40% of patients achieved disease stabilization for at least 6 months, with concurrent pain improvement. Treatment discontinuations were attributed to progression, death, withdrawal, or AEs. Common toxicities included rash, fatigue, nausea/vomiting, diarrhea, alopecia, and edema; grade ≥3 events such as anemia, dyspnea, hypoxia, hypotension, syncope, and dermatitis. Responses were restricted to tumors with CAMTA1-mediated MAPK pathway activation, highlighting the need for driver mutation screening beyond MAPK dependence.26
A recent case series of 18 patients with advanced/progressive EHE treated with the mTOR inhibitor sirolimus showed clinical benefit in 56% of patients, with over 24 months survival.27 This previous study indicated that YAP/TAZ molecular markers associated with oncogenic fusions contributed to activation of the mTOR complex, supporting sirolimus use in EHE.27 In a cohort study, 66% of sirolimus-treated patients maintained therapy for over a year, with 16% continuing treatment beyond five years, indicating meaningful therapeutic efficacy.28 In advanced EHE patients on a continuous daily dose of 5 mg sirolimus, all patients had disease progression prior to sirolimus treatment, and the median PFS was 13.0 months with median OS of 18.8 months.29 A clinical study evaluating the short-term efficacy of sirolimus-interferon combination therapy in 29 hepatic EHE patients reported a median treatment duration of 8.0 months, with tumor volume reduction in 79.3% of cases, ORR of 41.4%, and DCR of 86.2%.30 For advanced EHE patients with high-risk features (eg bulky tumors, rapid progression, severe symptoms, effusions, or prior treatment failure), two combination chemotherapy regimens (nab-paclitaxel plus bevacizumab, and nab-paclitaxel plus sirolimus) were evaluated.31 Results showed a PR in 5 patients (23.8%), DCR of 80.9%, symptomatic improvement in 83.3% of symptomatic patients, and effusion reduction in 6 of 12 patients (50.0%). Survival analysis revealed 1- and 2-year PFS rates of 50.7% and 13.5% respectively, with corresponding OS rates of 70.6% and 51.5%.31
It is worth noting that this study provides real-world everolimus use in clinical practice and highlights the importance of effectively managing AEs. Patient education regarding the recognition and management of treatment-related AEs may be important in clinical practice. Supportive measures, dose reduction, or temporary discontinuation may be applied for AEs management. We recommended that patients be educated on: (1) the risks of oral mucositis/ulceration, emphasizing rigorous oral hygiene, dietary modifications (avoiding spicy/acidic foods), and prompt reporting symptoms, with prophylactic dexamethasone mouthwash potentially reducing stomatitis incidence;32,33 (2) dermatologic toxicities that require proactive skin care and early intervention; and (3) the increased infection risk due to everolimus-induced immunosuppression, necessitating immediate reporting of any infectious symptoms, particularly new or worsening respiratory manifestations like cough, dyspnea or fever, with prompt CT evaluation for suspected interstitial pneumonitis.33 Concurrent lifestyle modifications, including weight reduction, physical activity, dietary adjustments, are essential for metabolic management.33,34 Most AEs can be effectively controlled through supportive measures, dose reduction, or temporary discontinuation. Comprehensive patient education on AE recognition, preventive strategies, and timely reporting is crucial for enhancing treatment compliance, enabling early clinical intervention, maintaining therapeutic continuity, and ultimately preserving long-term treatment benefits and quality of life.
This study has several limitations. First, the very small sample size restricts the statistical power and generalizability of the findings. Second, the instability of subgroup estimates, especially given the highly unbalanced subgroup sizes, hinders reliable comparative or prognostic inferences. Third, the retrospective nature prevents us from disentangling potential confounding factors, making it difficult to establish causal relationships. Fourth, the analyses are mainly descriptive and exploratory, and no definitive conclusions regarding efficacy or safety can be established. Finally, the small number of events limits the precision of survival estimates, and the results should be interpreted with caution. Despite these limitations, this study provides real-world clinical evidence for this ultra-rare disease, where large prospective trials are challenging to conduct. Therefore, further validation through prospective, multi-center studies with larger cohorts is warranted.
Conclusions
In summary, the exploratory analysis in this single-center retrospective study offers preliminary evidence supporting the potential role of everolimus as a therapeutic option for patients with advanced, unresectable, and progressive EHE. The variability in TTF highlight the necessity of selecting patients who may benefit from this treatment. Additionally, AEs management remains an important consideration during treatment. As such, the findings from this study may provide insights into patient selection, requiring prospective, multi-center studies with larger cohorts for validation.
Data Sharing Statement
The datasets generated and analyzed in the present study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board of Peking Union Medical College and adhered to the principles outlined in the Declaration of Helsinki. Written informed consent was waived due to the retrospective nature of the study.
Acknowledgments
We thank Medjaden Inc. for scientific editing of this manuscript.
Author Contributions
Huijing Tan and Huike Wang shared first authorship. All authors made significant contributions to the work reported, whether that is in the conception, study design, execution, data acquisition, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Wu Jieping Medical Foundation of China [grant numbers H011211, H011212, H011215] and the Scientific Research Start-up Foundation for Returned Overseas Scholars [grant number D422].
Disclosure
The authors declare that they have no competing interests.
References
1. Mehrabi A, Kashfi A, Fonouni H, et al. Primary malignant hepatic epithelioid hemangioendothelioma: a comprehensive review of the literature with emphasis on the surgical therapy. Cancer. 2006;107(9):2108–10. doi:10.1002/cncr.22225
2. Weiss SW, Enzinger FM. Epithelioid hemangioendothelioma: a vascular tumor often mistaken for a carcinoma. Cancer. 1982;50(5):970–981. doi:10.1002/1097-0142(19820901)50:5<970::AID-CNCR2820500527>3.0.CO;2-Z
3. Lau K, Massad M, Pollak C, et al. Clinical patterns and outcome in epithelioid hemangioendothelioma with or without pulmonary involvement: insights from an internet registry in the study of a rare cancer. Chest. 2011;140(5):1312–1318. doi:10.1378/chest.11-0039
4. Rosenbaum E, Jadeja B, Xu B, et al. Prognostic stratification of clinical and molecular epithelioid hemangioendothelioma subsets. Mod Pathol. 2020;33(4):591–602. doi:10.1038/s41379-019-0368-8
5. Folpe AL. Vascular tumors of intermediate malignancy: an update. Hum Pathol. 2024;147:114–128. doi:10.1016/j.humpath.2024.01.014
6. Mamone G, Miraglia R. The “Target sign” and the “Lollipop sign” in hepatic epithelioid hemangioendothelioma. Abdom Radiol. 2019;44(4):1617–1620. doi:10.1007/s00261-018-1820-9
7. Gurung S, Fu H, Zhang WW, Gu YH. Hepatic epithelioid hemangioendothelioma metastasized to the peritoneum, omentum and mesentery: a case report. Int J Clin Exp Pathol. 2015;8(5):5883–5889.
8. Zhou L, Cui MY, Xiong J, et al. Spectrum of appearances on CT and MRI of hepatic epithelioid hemangioendothelioma. BMC Gastroenterol. 2015;15(1):69. doi:10.1186/s12876-015-0299-x
9. Yang JW, Li Y, Xie K, Dong W, Cao XT, Xiao WD. Spontaneous rupture of hepatic epithelioid hemangioendothelioma: a case report. World J Gastroenterol. 2017;23(1):185–190. doi:10.3748/wjg.v23.i1.185
10. Afrit M, Nasri M, Labidi S, Mejri N, El Benna H, Boussen H. Aggressive primary hepatic epithelioid hemangioendothelioma: a case report and literature review. Cancer Biol Med. 2017;14(2):187–190. doi:10.20892/j.issn.2095-3941.2016.0105
11. Doyle LA, Fletcher CD, Hornick JL. Nuclear expression of CAMTA1 distinguishes epithelioid hemangioendothelioma from histologic mimics. Am J Surg Pathol. 2016;40(1):94–102. doi:10.1097/PAS.0000000000000511
12. Antonescu CR, Le Loarer F, Mosquera JM, et al. Novel YAP1-TFE3 fusion defines a distinct subset of epithelioid hemangioendothelioma. Genes Chromosomes Cancer. 2013;52(8):775–784. doi:10.1002/gcc.22073
13. Frezza AM, Ravi V, Lo Vullo S, et al. Systemic therapies in advanced epithelioid haemangioendothelioma: a retrospective international case series from the World Sarcoma Network and a review of literature. Cancer Med. 2021;10(8):2645–2659. doi:10.1002/cam4.3807
14. Burkhard-Meier A, Rechenauer VV, Jurinovic V, et al. First-line pazopanib in patients with metastatic epithelioid hemangioendothelioma: a retrospective single-center analysis. J Cancer Res Clin Oncol. 2025;151(4):150. doi:10.1007/s00432-025-06208-8
15. Dancey J. mTOR signaling and drug development in cancer. Nat Rev Clin Oncol. 2010;7(4):209–219. doi:10.1038/nrclinonc.2010.21
16. Polivka J Jr, Janku F. Molecular targets for cancer therapy in the PI3K/AKT/mTOR pathway. Pharmacol Ther. 2014;142(2):164–175. doi:10.1016/j.pharmthera.2013.12.004
17. Stacchiotti S, Tap W, Leonard H, Zaffaroni N, Baldi GG. New Molecular Insights, and the Role of Systemic Therapies and Collaboration for Treatment of Epithelioid Hemangioendothelioma (EHE). Curr Treat Options Oncol. 2023;24(6):667–679. doi:10.1007/s11864-023-01076-1
18. Emamaullee JA, Nowak K, Beach M, Bacani J, Shapiro AMJ. Hepatic epithelioid hemangioendothelioma presenting as an enlarging vascular lesion within the spleen. Case Rep Transplant. 2018;2018:3948784. doi:10.1155/2018/3948784
19. Makhlouf HR, Ishak KG, Goodman ZD. Epithelioid hemangioendothelioma of the liver: a clinicopathologic study of 137 cases. Cancer. 1999;85(3):562–582. doi:10.1002/(SICI)1097-0142(19990201)85:3<562::AID-CNCR7>3.0.CO;2-T
20. Gan LU, Chang R, Jin H, Yang LI. Typical CT and MRI signs of hepatic epithelioid hemangioendothelioma. Oncol Lett. 2016;11(3):1699–1706. doi:10.3892/ol.2016.4149
21. Liu X, Yang P, Liu L, et al. Long-term prognosis and treatment modalities of hepatic epithelioid hemangioendothelioma: a retrospective study of 228 patients. BMC Cancer. 2024;24(1):1285. doi:10.1186/s12885-024-13053-4
22. Jung DH, Hwang S, Hong SM, et al. Clinicopathological features and prognosis of hepatic epithelioid hemangioendothelioma after liver resection and transplantation. Ann Transplant. 2016;21:784–790. doi:10.12659/AOT.901172
23. Llueca A, Piquer D, Maazouzi Y, et al. Hepatic epithelioid hemangioendothelioma: a great mimicker. Int J Surg Case Rep. 2018;53:25–28. doi:10.1016/j.ijscr.2018.10.013
24. Tsuchihashi K, Baba E. Epithelioid hemangioendothelioma-its history, clinical features, molecular biology and current therapy. Jpn J Clin Oncol. 2024;54(7):739–747. doi:10.1093/jjco/hyae037
25. Lai Q, Feys E, Karam V, et al. Hepatic epithelioid hemangioendothelioma and adult liver transplantation: proposal for a prognostic score based on the analysis of the ELTR-ELITA Registry. Transplantation. 2017;101:555–564. doi:10.1097/TP.0000000000001603
26. Schuetze SM, Ballman KV, Heise R, et al. A single-arm Phase 2 trial of trametinib in patients with locally advanced or metastatic epithelioid hemangioendothelioma. Clin Cancer Res. 2024;30(20):4584–4592. doi:10.1158/1078-0432.CCR-23-3817
27. Smrke AM, Huang PH, Jones RL. Sirolimus for patients with progressive epithelioid hemangioendothelioma. Cancer. 2021;127(4):504–506. doi:10.1002/cncr.33246
28. Robinson D, Leonard H, Baldi GG, et al. The patient perspective on sirolimus for epithelioid hemangioendothelioma (EHE): results of a community survey highlighting the importance of equitable access to treatments. Front Oncol. 2024;14:1367237. doi:10.3389/fonc.2024.1367237
29. Stacchiotti S, Simeone N, Lo Vullo S, et al. Activity of sirolimus in patients with progressive epithelioid hemangioendothelioma: a case-series analysis within the Italian Rare Cancer Network. Cancer. 2021;127(4):569–576. doi:10.1002/cncr.33247
30. Liu X, Zhou R, Liu L, et al. Short-term outcomes of combined therapy with sirolimus and interferon-alpha 2b for advanced hepatic epithelioid hemangioendothelioma. Ther Adv Med Oncol. 2024;16:17588359231220509. doi:10.1177/17588359231220509
31. Liu X, Yang P, Liu L, et al. Nab-paclitaxel based chemotherapy in the treatment of advanced epithelioid hemangioendothelioma: a single-institution experience. Cancer Manag Res. 2025;17:373–381. doi:10.2147/CMAR.S508673
32. Pilotte AP, Hohos MB, Polson KM, Huftalen TM, Treister N. Managing stomatitis in patients treated with Mammalian target of rapamycin inhibitors. Clin J Oncol Nurs. 2011;15(5):E83–E89. doi:10.1188/11.CJON.E83-E89
33. Porta C, Osanto S, Ravaud A, et al. Management of adverse events associated with the use of everolimus in patients with advanced renal cell carcinoma. Eur J Cancer. 2011;47(9):1287–1298. doi:10.1016/j.ejca.2011.02.014
34. Eisen T, Sternberg CN, Robert C, et al. Targeted therapies for renal cell carcinoma: review of adverse event management strategies. J Natl Cancer Inst. 2012;104(2):93–113. doi:10.1093/jnci/djr511
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.