Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Efficacy and Safety Analysis of Concentrated Growth Factor Combined with Photorejuvenation for Sensitive Skin Patients: A Retrospective Cohort Study
Authors Yang L, Yang W, Zhang X, Wang Y
Received 3 March 2026
Accepted for publication 19 June 2026
Published 15 July 2026 Volume 2026:19 600948
DOI https://doi.org/10.2147/CCID.S600948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Liu Yang,1 Wenjing Yang,2 Xin Zhang,1 Yanli Wang1
1Department of Plastic & Cosmetics Surgery, Zibo Central Hospital, Zibo, Shandong, 255000, People’s Republic of China; 2Department of Cosmetic Surgery, Zibo Yimei Plastic and Aesthetic Hospital, Zibo, Shandong, 255000, People’s Republic of China
Correspondence: Yanli Wang, Department of Plastic & Cosmetics Surgery, Zibo Central Hospital, No. 54 Gong-Qing-Tuan West Road, Zhang-Dian District, Zibo, Shandong, 255000, People’s Republic of China, Email [email protected]
Background: Sensitive skin, characterized by heightened reactivity and discomfort, presents therapeutic challenges. This study aimed to evaluate the efficacy and safety of combined CGF and IPL therapy compared to IPL alone for facial sensitive skin.
Methods: This retrospective cohort study included patients with mild to moderate facial sensitive skin treated at a single hospital between January 2022 and January 2025. Patients were divided into two groups of unequal size: the IPL group, receiving IPL alone (n = 128), and the CGF plus IPL group, receiving CGF and IPL treatments (n = 91). Serum growth factors and inflammatory cytokines were measured at baseline and the 6-month follow-up. Wrinkle condition, skin barrier function, skin gloss, and skin elasticity were assessed at baseline, 1 month, and 6 months. The incidence of adverse reactions was recorded, and the Global Aesthetic Improvement Scale (GAIS) and Dermatology Life Quality Index (DLQI) were used to evaluate improvement and quality of life.
Results: Post-treatment vascular endothelial growth factor and epidermal growth factor levels were significantly higher in the combination group than in the IPL group (all P< 0.001). At 1 and 6 months post-treatment, the CGF plus IPL group exhibited significantly greater improvement in wrinkle count and area, lower interleukin-6 and tumor necrosis factor-alpha levels, reduced transepidermal water loss, increased stratum corneum hydration, elastic modulus, and skin firmness compared to the IPL group (all P < 0.05). At 6 months, skin gloss and GAIS scores were significantly higher in the CGF plus IPL group. The combination group exhibited a significantly lower incidence of burning (P=0.003) and stinging (P=0.045). Post-treatment DLQI scores indicated greater quality-of-life improvement in the combined group (P < 0.05).
Conclusion: The combination of CGF and IPL is a highly effective and safe therapeutic strategy that provides superior and synergistic benefits for patients with facial sensitive skin compared to IPL monotherapy.
Keywords: sensitive skin, intense pulsed light, concentrated growth factor, skin barrier function, inflammatory cytokines, skin elasticity
Introduction
Sensitive skin, a frequently encountered condition in dermatological practice, presents as a constellation of subjective discomforts—such as stinging, burning, tightness, or pruritus—typically in the absence of distinct clinical findings or overt disease.1 This syndrome is increasingly prevalent worldwide, affecting up to 60% of women and 40% of men in certain populations, and often substantially impairs quality of life.2 Despite its high prevalence, the underlying etiology of sensitive skin remains incompletely elucidated.3 The pathogenesis is considered multifactorial, involving perturbations of the epidermal barrier, heightened cutaneous nerve reactivity, aberrant immune responses, and heightened vascular reactivity, all of which contribute to abnormal sensations and increased vulnerability to environmental and chemical triggers.4
The conventional management of sensitive skin primarily involves avoiding irritants, using mild moisturizers to repair the barrier, and supplementing with topical anti-inflammatory agents and physical sunscreens to alleviate symptoms.5 However, due to incomplete symptom control and frequent cosmetic concerns such as erythema, uneven skin tone, and irregular texture, patients are often dissatisfied with standard therapies.6 Intense Pulsed Light (IPL) is a multi-wavelength, non-invasive photorejuvenation technology suitable for various skin issues in patients with sensitive skin.7 It achieves photothermal decomposition of vascular and pigmented lesions through selective absorption by hemoglobin and melanin.8 Simultaneously, IPL provides non-selective stimulation to dermal fibroblasts, promoting new collagen production, enhancing elasticity, and overall skin rejuvenation.9 Compared to traditional ablative lasers, IPL has better safety profiles and fewer side effects, but mild erythema, stinging, or delayed barrier recovery may still occur in sensitive skin, necessitating cautious use under professional guidance.10
There is considerable interest in the therapeutic potential of growth factors in dermatology. Growth factors such as Vascular Endothelial Growth Factor (VEGF) and Epidermal Growth Factor (EGF) are key mediators in wound healing and tissue regeneration.11 VEGF promotes angiogenesis and enhances nutrient delivery, while EGF stimulates keratinocyte proliferation and migration, which are crucial for barrier repair.12,13 The interaction between growth factor signaling pathways and inflammatory cytokines suggests a potential mechanistic link; enhancing growth factor activity may simultaneously inhibit pro-inflammatory pathways, thereby improving skin homeostasis and elasticity.14 Concentrated Growth Factor (CGF) is an autologous platelet-derived concentrate rich in multiple growth factors, with reported regenerative effects in dermatology. However, studies specifically exploring the combination of CGF and IPL for facial sensitive skin remain limited.
This study aims to evaluate the clinical efficacy and safety of combined CGF and IPL treatment for facial sensitive skin compared to IPL alone. The innovation lies in exploring the synergistic effects of this combination on photobiomodulation and tissue regeneration. The goal is to achieve more effective and sustained skin improvement, reduce treatment discomfort, increase patient satisfaction, and provide a promising advanced therapeutic strategy.
Materials and Methods
Research Design and Ethical Statement
This study employed a retrospective cohort design, selecting patients with facial sensitive skin who were treated at our hospital between January 2022 and January 2025. Each patient was followed up for six months. Patients were assigned to the IPL group or the CGF plus IPL group based on their treatment preference and clinical judgment after detailed consultation. Consecutive enrollment was applied to all eligible patients during the study period. The Intense Pulsed Light (IPL) group included 128 patients who received only IPL treatment, administered once every four weeks for a total of five sessions. The IPL treatment was performed using the Lumenis M22 device (M22, Lumenis, Israel). The Concentrated Growth Factor and Intense Pulsed Light Combined (CGF and IPL) group included 91 patients who received both CGF and IPL treatments. In this group, IPL was administered once every four weeks for a total of five sessions, while CGF was administered once every four weeks for a total of three sessions, with a 15-day interval between CGF and IPL treatments.
In this study, we used de-identified patient information to ensure all data were anonymized, thereby having no impact on the patients’ treatment or prognosis. All patient information was managed according to the regulations of the hospital’s ethics committee, and an application for exemption from obtaining informed consent was approved by the ethics committee. We strictly adhered to relevant ethical guidelines to ensure patient privacy was protected and data security and confidentiality were maintained throughout the research process.
Inclusion and Exclusion Criteria
The inclusion criteria for this study were: (1) patients aged over 18 years; (2) mild to moderate facial sensitive skin;15 and (3) completion of the entire treatment and follow-up period with complete data.
The exclusion criteria were: (1) presence of severe cardiovascular diseases, current use or use within 4 weeks prior to enrollment of any hormonal medications or photosensitive drugs, or other acute inflammatory conditions; (2) recent history of laser or phototherapy treatments; (3) pregnant or breastfeeding women; (4) known allergies to any component of the treatment protocol; (5) severe systemic diseases such as hematologic disorders (platelet dysfunction syndrome, thrombocytopenia), infectious diseases (tuberculosis, leukemia), or autoimmune diseases; (6) other severe dermatological conditions (such as acne, rosacea, eczema, psoriasis) that could affect treatment outcomes or increase the risk of adverse reactions; and (7) psychological instability, including severe anxiety or depression, which could impact treatment compliance.
Treatment Methods
All patients in the IPL group received IPL treatment once every four weeks, for a total of five treatments. Treatments were performed using the Lumenis M22 system (Lumenis Ltd., Yokneam, Israel) equipped with a 590 nm cut-off filter. The treatment parameters were standardized as follows: fluence of 13–16 J/cm2, pulse duration of 3.0–4.5 ms, and a single pulse mode. IPL was delivered using a single pulse mode with contact cooling (sapphire cooling plate, set at 12°C). Each treatment session consisted of 40–50 pulses applied over the entire facial region with a single non-overlapping pass.
CGF was prepared from autologous peripheral blood for each patient prior to each administration. For each preparation, 36 mL of venous blood was drawn from the antecubital vein using 9 mL sterile, glass-coated plastic tubes (Vacutainer®, Becton Dickinson, Franklin Lakes, NJ, USA) containing no anticoagulant. The tubes were immediately centrifuged using a Medifuge 200 centrifuge (Silfradent SRL, Santa Sofia, Italy) according to the manufacturer’s standardized protocol: acceleration to 2700 rpm, followed by 2 minutes at 2,400 rpm, 4 minutes at 2,700 rpm, 4 minutes at 2,400 rpm, 3 minutes at 2,700 rpm, and 3 minutes at 3,000 rpm, with controlled deceleration. This centrifugation process separates the blood into three distinct layers: a red blood cell layer at the bottom, a buffy coat layer containing concentrated growth factors and platelets in the middle, and a platelet-poor plasma layer at the top. The CGF fraction, which corresponds to the buffy coat and the immediately adjacent plasma layer, was carefully collected using sterile forceps and scissors to excise the fibrin-rich clot. This CGF preparation is rich in multiple growth factors, including vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), platelet-derived growth factor (PDGF), and transforming growth factor-beta (TGF-β). The collected CGF was then compressed into a thin membrane using a sterile stainless steel compression device (Xpansion® Kit, Silfradent SRL, Santa Sofia, Italy). Each preparation yielded approximately 4–5 mL of CGF in membrane form. Immediately after IPL treatment, the CGF membrane was applied topically to the entire facial area and left in place for approximately 20 minutes until fully absorbed. No exogenous activators (eg., calcium chloride or thrombin) were added. The CGF clot formed spontaneously during centrifugation and was used directly after mechanical compression into a membrane.
Data Collection
Demographic Information
Demographic information, including gender, age, and treatment history, was recorded during the initial consultation and obtained from the medical record system.
Serum Growth Factor
Serum levels of VEGF and EGF were measured using enzyme-linked immunosorbent assay (ELISA) kits. To control for circadian variations, all blood samples were collected between 8:00 and 9:00 AM after an overnight fast, both before treatment and at the 6-month follow-up. The collected blood samples were centrifuged at 3000 rpm for 15 minutes using a Heraeus Multifuge X3R centrifuge (Thermo Fisher Scientific, USA) to obtain serum, which was subsequently stored at −80°C until batch analysis. VEGF concentrations were quantified using the Human VEGF Quantikine ELISA Kit (R&D Systems, USA), while EGF levels were determined using the Human EGF Quantikine ELISA Kit (R&D Systems, USA).
Wrinkles Condition
Wrinkles were assessed using the VISIA 7 system (Canfield Scientific, Inc., USA), which captures high-resolution images of the skin and automatically identifies and quantifies the number, length, and depth of wrinkles through its built-in algorithms. High-resolution digital photographs were taken under controlled lighting conditions to ensure uniform illumination and camera settings. For each participant, images were captured from predefined facial regions, such as the forehead. The VISIA 7 system then processed these images to determine the number and area of wrinkles.
Inflammatory Cytokines
Serum levels of IL-6 and TNF-α were measured using enzyme-linked immunosorbent assay (ELISA) kits. Blood samples were collected between 8:00 and 9:00 AM after an overnight fast, both at baseline and at the 6-month follow-up. The collected blood was centrifuged at 3000 rpm for 15 minutes using a Heraeus Multifuge X3R centrifuge (Thermo Fisher Scientific, USA) to separate the serum, which was then stored at −80°C until analysis. IL-6 was measured using the Human IL-6 Quantikine ELISA Kit (R&D Systems, USA). TNF-α was measured using the Human TNF-alpha Quantikine ELISA Kit (R&D Systems, USA). CRP levels were determined using the Roche Cobas c702 automated clinical chemistry analyzer (Roche Diagnostics, Switzerland).
Detection Methods for Transepidermal Water Loss (TEWL) and Stratum Corneum Hydration (SCH)
TEWL was measured using a VapoMeter (Delfin Technologies, Finland). Prior to measurement, participants were asked to refrain from washing the test area for at least 2 hours and to avoid applying any topical products. Measurements were taken on the cheek area of each participant. The probe was placed gently on the skin surface, ensuring no air gaps, and measurements were recorded after stabilization. The average of three readings was used for analysis.
Stratum corneum hydration was assessed using a Corneometer CM 825 (Courage + Khazaka Electronic GmbH, Germany). The Corneometer uses capacitance to measure the water content of the stratum corneum. Participants were asked to refrain from washing the test area for at least 2 hours before the measurement and to avoid applying any topical products. Measurements were taken on the same cheek area as for TEWL. The average of three readings was used for analysis.
Skin Gloss
Skin gloss was measured using a Cutometer® MPA 580 (with gloss measurement module) (Courage + Khazaka Electronic GmbH, Germany). The Gloss Meter measures the amount of light reflected from the skin surface at a specific angle, providing a quantitative assessment of skin gloss. Prior to measurement, participants were asked to refrain from washing the test area for at least 2 hours and to avoid applying any topical products. Measurements were taken on the cheek area of each participant.
Skin Elasticity
The elastic modulus of the skin was measured using a Cutometer Dual MPA 580 (Courage + Khazaka Electronic GmbH, Germany). The Cutometer applies suction to the skin surface, creating a temporary deformation, and measures the force required to deform the skin and its ability to return to its original state. Measurements were taken on the cheek area of each participant. The probe was placed gently on the skin surface, the average of three readings was used for analysis.
Skin firmness was assessed using a Reviscometer RVM600 (Courage + Khazaka Electronic GmbH, Germany). The Reviscometer measures the mechanical properties of the skin, specifically its viscoelasticity, by applying low-frequency vibrations and analyzing the propagation of these waves through the skin. Measurements were taken on the same cheek area as for the elastic modulus. The average of three readings was used for analysis.
Incidence of Adverse Reactions
The incidence of adverse reactions was recorded during the six-month follow-up period. The following symptoms were monitored and documented: stinging, burning, tightness, itching, general malaise, and flushing. Participants were asked to report any occurrence of these symptoms at each follow-up visit.
Improvement Condition
The Global Aesthetic Improvement Scale (GAIS) was used to assess the overall aesthetic improvement of participants following treatment.16 The GAIS is a 5-point scale ranging from −1 (worse) to +3 (very much improved), with 0 indicating no change. Standard white light images (Figures 1A and D) served as reference points for subsequent GAIS assessments. Additionally, inflammatory vascular maps (Figures 1B and E) were used to visualize dermal hemoglobin distribution, reflecting vascular patterns and subclinical inflammation status, while generating pseudo-color heatmaps (Figures 1C and F) to provide a quantitative representation of inflammatory activity. These photographs served as a reference point for subsequent assessments. Follow-up assessments were conducted at 6 months post-treatment. During this visit, new high-resolution photographs were taken under standardized lighting conditions to ensure consistency. One independent, blinded dermatologist reviewed the baseline and follow-up photographs side by side.
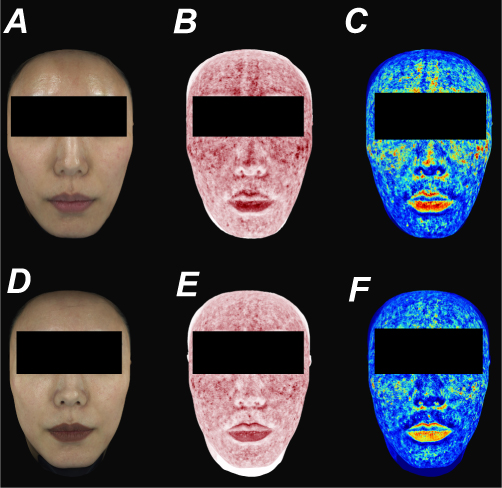 |
Figure 1 Representative multispectral facial skin images of a patient from the CGF plus IPL group before and after treatment. (A) Standard white light image before treatment; (B) red area image before treatment; (C) pseudocolor heatmap of subclinical inflammation before treatment; (D) standard white light image after treatment; (E) red area image after treatment; (F) pseudocolor heatmap of subclinical inflammation after treatment. |
Quality of Life
The Dermatology Life Quality Index (DLQI) was used to assess the impact of skin conditions on participants’ quality of life.17 The DLQI is a validated 10-item questionnaire designed to measure how dermatological conditions affect various aspects of a patient’s life over the past week. Each item is scored on a 4-point scale (0–3), with higher scores indicating greater impairment in quality of life. The total score ranges from 0 to 30, where higher scores indicate a greater impact on quality of life.
Data Analysis
For the statistical analysis, we utilized IBM SPSS Statistics version 29.0 (IBM Corp., Armonk, NY, USA) to process and analyze the gathered data. Categorical variables were summarized using frequencies and percentages [n (%)]. To evaluate categorical data, we applied the chi-square test, represented as χ2. Continuous data that adhered to a normal distribution were presented as means ± standard deviations (M ± SD). For comparing normally distributed continuous data between groups, independent samples t-tests were conducted.
Given the retrospective design, no a priori sample size calculation was performed. A post-hoc power analysis was therefore conducted for the primary outcome measures (serum VEGF, serum EGF, and TEWL at 6 months) using G*Power software (version 3.1.9.7) with α = 0.05 (two-tailed) and effect sizes derived from the observed group differences. The achieved post-hoc power values were 0.99, 0.98, and 0.92, respectively, all exceeding the conventional threshold of 0.80, confirming that the sample sizes (n=128 and n=91) were adequate to detect the observed differences.
Results
Baseline Data
In the present study, baseline characteristics were comparable between the IPL group and the CGF and IPL group (Table 1). There were no significant differences in age, gender distribution, or body mass index. Educational attainment, smoking and alcohol consumption status, allergy history, family dermatological history, skin pH, and skin type were also similar across groups. The mean duration of condition was comparable. Prior treatment modalities, including topical steroids, moisturizers, and antihistamines, showed no significant intergroup differences. These findings indicate well-balanced baseline characteristics between the two cohorts prior to intervention.
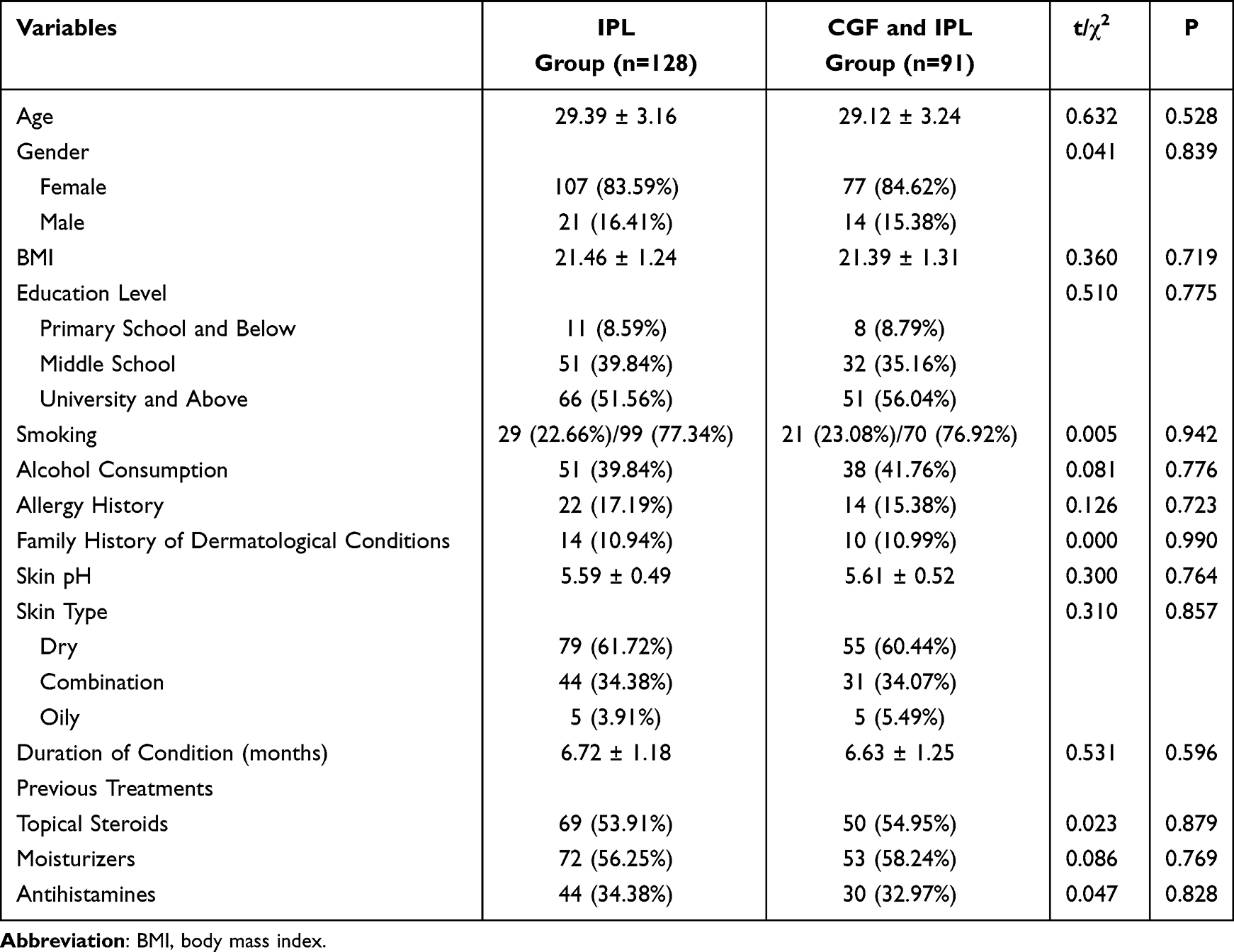 |
Table 1 Baseline Data |
Serum Growth Factor
In the comparison between the IPL group and the CGF and IPL group, there were no significant differences in VEGF and EGF levels before treatment (Table 2). However, after treatment, the CGF and IPL group showed significantly higher VEGF levels compared to the IPL group. Similarly, the CGF and IPL group exhibited significantly higher EGF levels than the IPL group. These results highlight the superior efficacy of the CGF and IPL combination in enhancing both VEGF and EGF levels post-treatment.
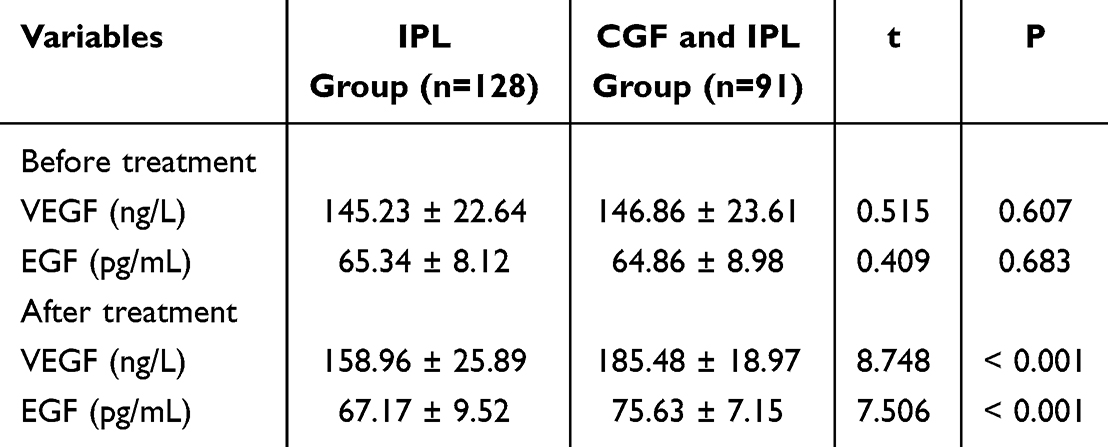 |
Table 2 Serum Growth Factor |
Wrinkle Condition
At baseline, there were no significant differences between the IPL group and the CGF and IPL group in wrinkle count or wrinkle area (Figure 2). However, at both 1 month and 6 months after treatment, the CGF and IPL group demonstrated significantly lower wrinkle counts and smaller wrinkle areas compared with the IPL group, indicating greater improvement in wrinkle condition with combined CGF and IPL therapy.
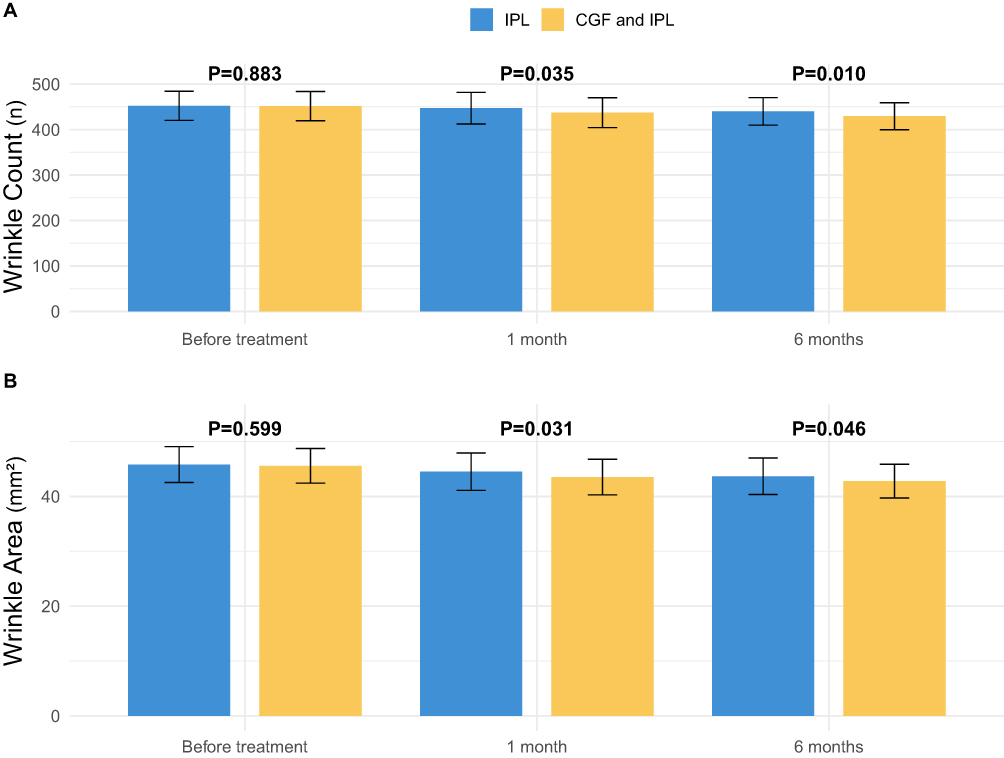 |
Figure 2 Wrinkle Condition. (A) Wrinkle count (n); (B) Wrinkle area (mm2). Data are presented as mean ± SD. Comparisons between the IPL group and the CGF plus IPL group at each time point were performed using independent samples t-test. |
Inflammatory Cytokines
Baseline levels of inflammatory cytokines, including IL-6, TNF-α, and CRP, were comparable between the IPL group and the CGF and IPL group (Figure 3). After treatment, the CGF and IPL group exhibited significantly lower levels of IL-6 and TNF-α compared with the IPL group. Post-treatment CRP levels showed no significant difference between groups. These results suggest that combined CGF and IPL therapy more effectively reduced inflammatory cytokine levels, particularly IL-6 and TNF-α, in patients with sensitive skin.
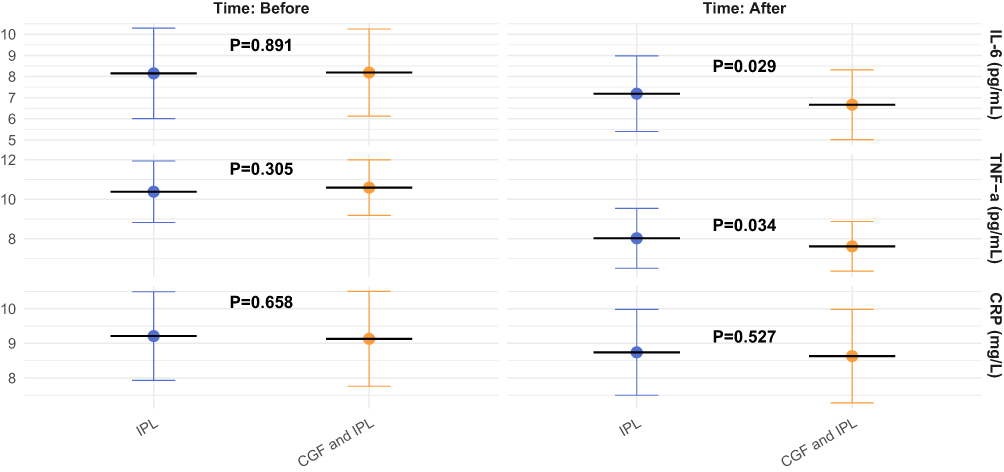 |
Figure 3 Inflammatory Cytokines. Serum levels of IL-6 (pg/mL), TNF-α (pg/mL), and CRP (mg/L) before and after treatment. Data are presented as mean ± SD. Comparisons between the IPL group and the CGF plus IPL group at each time point were performed using independent samples t-test. |
Skin Barrier Function Indicators
Baseline values of skin barrier function indicators, including transepidermal water loss and stratum corneum hydration, were similar between the IPL group and the CGF and IPL group (Figure 4). At both 1 month and 6 months after treatment, the CGF and IPL group demonstrated significantly lower TEWL than the IPL group, as well as significantly higher stratum corneum hydration. These findings indicate that combined CGF and IPL therapy provides greater improvement in skin barrier function compared with IPL alone in patients with sensitive skin.
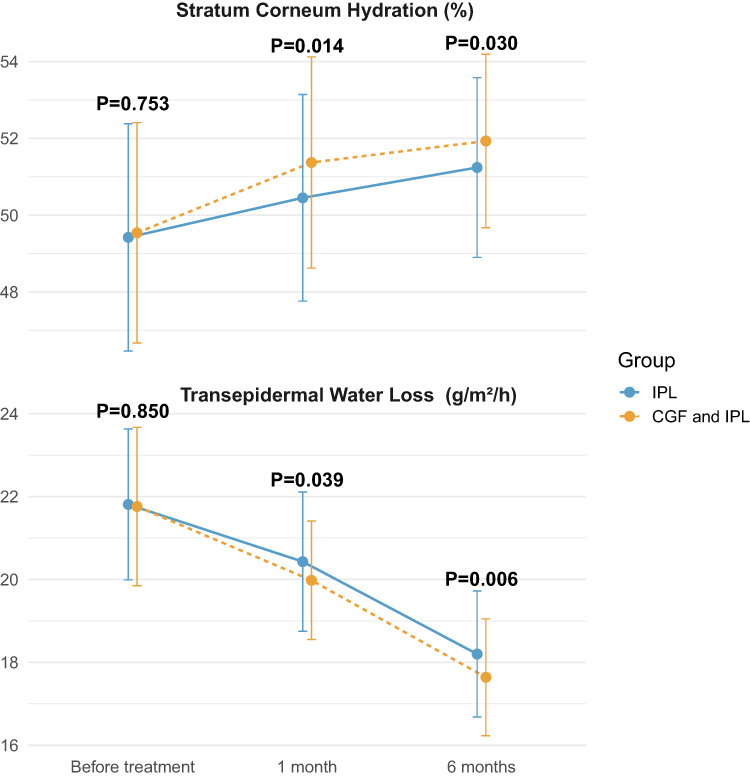 |
Figure 4 Skin Barrier Function Indicators. Transepidermal water loss (TEWL, g/h/m2); stratum corneum hydration. Data are presented as mean ± SD. Comparisons between groups at each time point were performed using independent samples t-test. |
Skin Gloss
At baseline, there was no significant difference in skin gloss between the IPL group and the CGF and IPL group (Figure 5). Skin gloss values at 1 month post-treatment remained similar between groups. However, at 6 months, the CGF and IPL group demonstrated significantly higher skin gloss compared with the IPL group, indicating greater long-term improvement in skin gloss with the combined therapy.
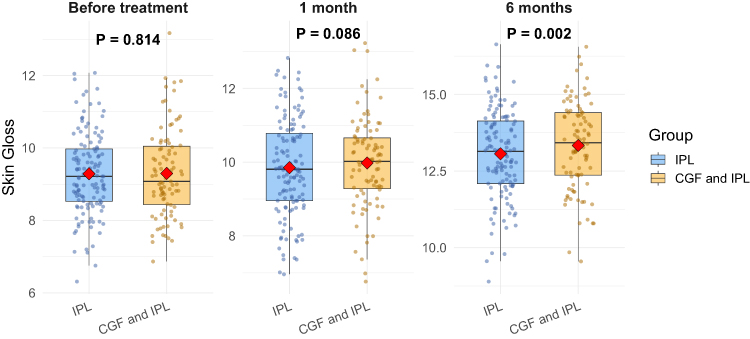 |
Figure 5 Skin Gloss. Skin gloss values measured before treatment, at 1 month, and at 6 months. Boxplots show medians with interquartile ranges. Comparisons between the IPL group and the CGF plus IPL group at each time point were performed using independent samples t-test. |
Skin Elasticity
Baseline elastic modulus and skin firmness were comparable between the two groups (Table 3). After treatment, the CGF and IPL group exhibited significantly higher elastic modulus and greater skin firmness than the IPL group, indicating enhanced skin elasticity and tighter skin structure. These findings demonstrate that the addition of CGF to IPL therapy yields superior biomechanical improvements in patients with sensitive skin.
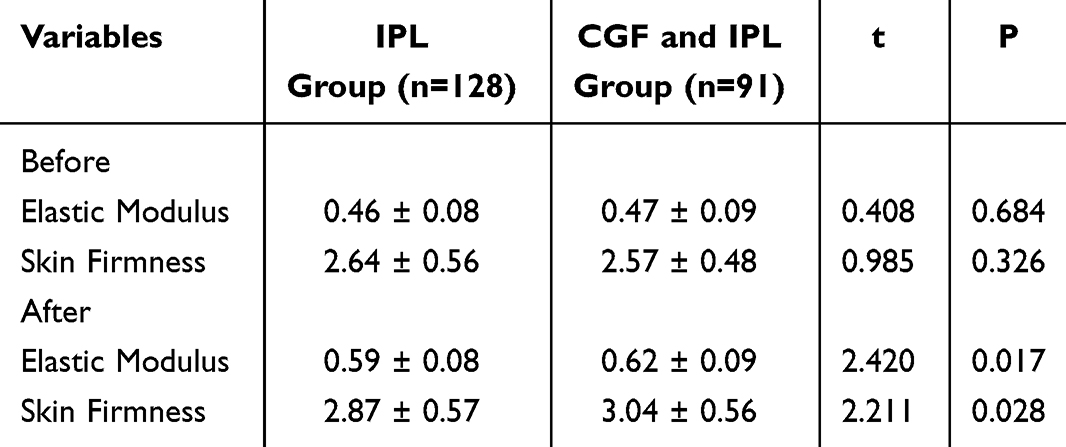 |
Table 3 Skin Elasticity |
Incidence of Adverse Reactions
The overall incidence of adverse reactions was generally comparable between the IPL group and the CGF and IPL group, with no statistically significant differences observed for tightness, itching, general malaise, or flushing and redness (Table 4). However, the incidence of burning and stinging was significantly lower in the CGF and IPL group compared to the IPL group. These findings suggest that combined CGF and IPL therapy may reduce the occurrence of both burning and stinging while maintaining a comparable safety profile to IPL alone in patients with sensitive skin.
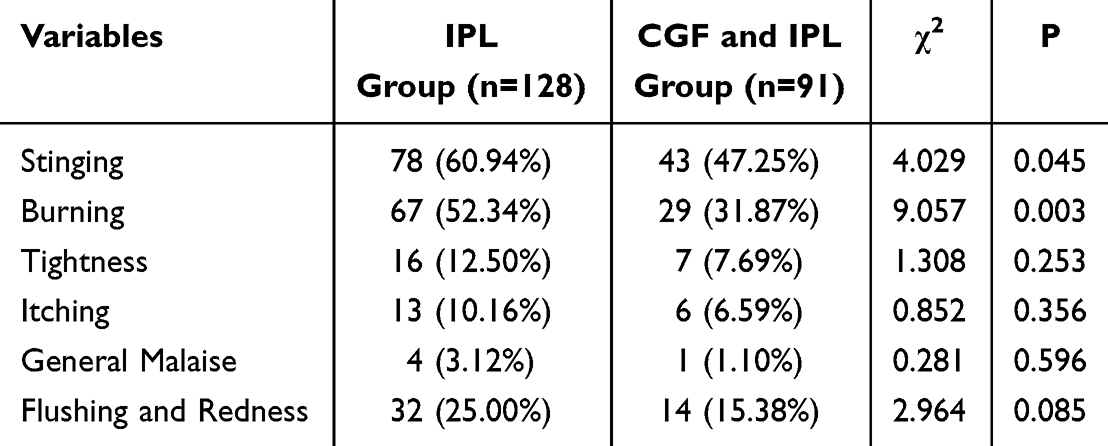 |
Table 4 Incidence of Adverse Reactions |
GAIS Score
The Global Aesthetic Improvement Scale scores indicated that the CGF and IPL group achieved significantly greater improvement than the IPL group alone (Table 5). In the CGF and IPL group, a higher proportion of patients were rated as “much improved” or “very much improved”, while the proportion rated as “improved” was lower, and no patients in the combined group showed “no change” compared with 1.56% in the IPL group. These findings demonstrate superior overall aesthetic improvement with combined CGF and IPL therapy for sensitive skin patients.
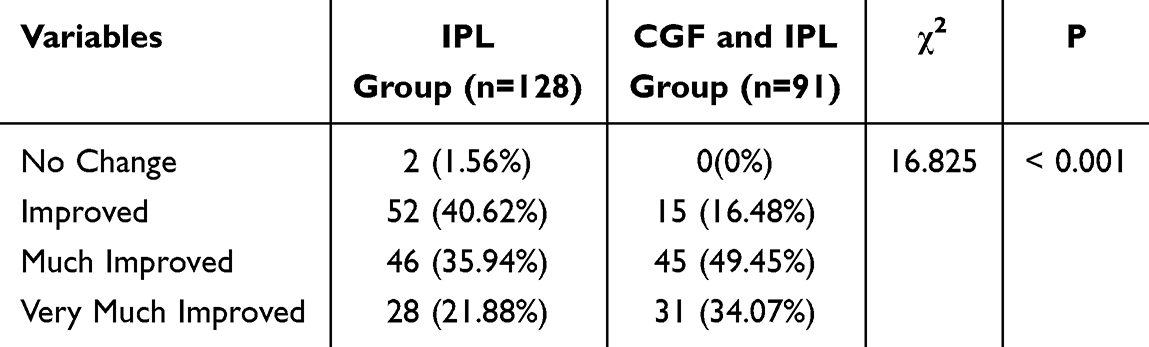 |
Table 5 GAIS Score |
Quality of Life
Baseline DLQI scores were comparable between the two groups. After treatment, both groups showed improvement; however, the CGF and IPL group achieved significantly lower scores than the IPL group (Figure 6), indicating better quality of life as lower DLQI scores reflect less impairment from skin conditions. These results suggest that combined CGF and IPL therapy is associated with superior quality-of-life enhancement in patients with sensitive skin.
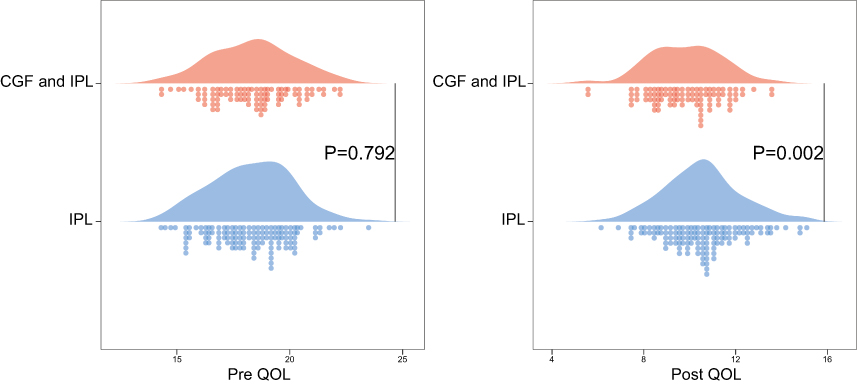 |
Figure 6 Quality of Life Before and after treatment. Data are presented as mean ± SD. Comparisons between the IPL group and the CGF plus IPL group were performed using independent samples t-test. |
Discussion
This retrospective cohort study provides clinical evidence that the combination of CGF and IPL therapy offers a synergistic and superior approach for managing facial sensitive skin compared to IPL monotherapy. The combined regimen not only enhances multiple aspects of skin physiology and appearance but also demonstrates good safety, reducing treatment-related adverse sensations.
Higher serum levels of VEGF and EGF observed in the combined treatment group suggest that systemic bioactivation underpins the clinical improvements. Growth factors are key signaling molecules regulating critical processes in tissue repair and regeneration.18 The surge in these factors post-treatment in the CGF+IPL group indicates that autologous CGF preparations can serve as a sustained biological reservoir, enhancing the regenerative signaling cascades initiated by the photothermal and photobiomodulatory effects of IPL.19 This aligns with the established roles of growth factors in promoting angiogenesis, fibroblast proliferation, and keratinocyte migration, which are central to restoring skin homeostasis.20 Although CGF is locally applied, the improved local barrier function and reduced inflammation may decrease the systemic inflammatory burden, leading to an increase in circulating growth factor levels as tissue repair progresses. The concept that enhanced growth factor activity can simultaneously promote tissue regeneration and modulate inflammation provides a plausible mechanistic basis for the multifaceted benefits observed in our study.
The reduction in the number and area of wrinkles in the combined treatment group suggests enhanced skin remodeling. It is well known that IPL can stimulate new collagen production, but the addition of CGF appears to amplify this process considerably.21 Growth factors, including those present in CGF, are potent stimulators of fibroblast activity and extracellular matrix (ECM) synthesis.22 Improvements in skin elasticity and firmness further confirm this, indicating a more robust recovery of skin structure. This finding is consistent with other studies on platelet concentrates and growth factor serums, which have shown to improve skin texture and elasticity by promoting new collagen formation.23
A key finding of this study is the lower levels of pro-inflammatory cytokines observed after combined treatment. Sensitive skin is often characterized by subclinical inflammation and a state of neurosensory hyperreactivity.24 The reduction in these cytokines suggests that the CGF+IPL combination may effectively alleviate this underlying inflammatory drive. Emerging evidence supports the anti-inflammatory potential of phototherapy; for example, photobiomodulation therapy (PBMT) has been shown to reduce inflammation in human fibroblasts by downregulating genes such as IL-6 and TNF-α.25 CGF and its array of regulatory factors may enhance the anti-inflammatory effects of IPL, leading to a deeper calming of the skin immune response and contributing to fewer adverse reactions.26 These findings are consistent with previous reports, which have shown that platelet concentrates combined with light or laser therapy can increase serum growth factor levels and reduce pro-inflammatory cytokines in patients with inflammatory skin diseases.27
Improvements in skin barrier function in the combined treatment group, as indicated by reduced TEWL and increased stratum corneum hydration, are crucial for managing sensitive skin. A compromised barrier is a cornerstone of the pathophysiology of sensitive skin.28 The synergy between CGF and IPL may accelerate barrier repair through multiple mechanisms. Growth factors like EGF directly promote keratinocyte proliferation and differentiation, which are essential for rebuilding a competent stratum corneum.29 Additionally, the observed anti-inflammatory effects would create a more favorable microenvironment for barrier recovery. This is supported by clinical studies showing that growth factor-based formulations can enhance skin hydration and barrier repair.30
The finding of reduced incidence of stinging and burning in the combined treatment group has direct clinical relevance. These unpleasant sensations are hallmarks of sensitive skin and can be triggered or exacerbated by cosmetic procedures. This reduction could be multifactorial, stemming from a strengthened skin barrier that better protects nerve endings from irritants and a lessened inflammatory environment that lowers peripheral sensitivity of sensory neurons.31,32 This enhanced tolerance makes combined treatment a more comfortable and patient-friendly option. Furthermore, the use of autologous growth factor sources like platelet-rich growth factor (PRGF) has been shown to benefit skin hydration and symptom relief in patients with sensitive skin, while laser and growth factor combination therapies show promise in reducing recurrence rates.33
The superior outcomes in global aesthetic improvement and quality of life serve as the ultimate validation of the clinical value of this treatment. Higher GAIS scores reflect improvements in skin appearance. More importantly, the substantial decrease in DLQI scores in the combined treatment group indicates that these physiological and aesthetic advancements have meaningful positive impacts on patients’ daily lives. Reducing the burden of sensitive skin aligns with broader goals in dermatological care, where patient-reported outcomes are increasingly recognized as important endpoints.34 Our results are consistent with other studies on combination therapies. For example, a regimen containing growth factors and peptides has been shown to improve skin healing, hydration, and patient satisfaction when used in conjunction with various laser procedures.35
Despite promising results, this study has several limitations. The retrospective, non-randomized design, with treatment allocation based on patient preference and clinical judgment, may introduce selection bias and confounding by indication, and the unequal group sizes warrant caution in causal inference. Additionally, multiple secondary outcomes were compared without multiplicity correction, rendering these analyses exploratory. A six-month follow-up period, while sufficient to observe mid-term outcomes, is not long enough to determine the long-term durability of improvements or the optimal frequency for maintenance treatments. The proposed mechanisms, although plausible based on current literature and our biomarker data, would be strengthened by more detailed molecular analyses, such as histological examination of skin biopsies or broader analysis of inflammatory mediators. Prospective, multicenter, randomized controlled trials with longer follow-up periods are needed to confirm these findings. Future studies should also focus on standardizing CGF protocols and elucidating the precise molecular crosstalk between light-based stimulation and growth factor signaling.
In conclusion, the combination of CGF and IPL represents a compelling therapeutic strategy for facial sensitive skin. It synergistically enhances skin barrier function, promotes structural regeneration, inhibits subclinical inflammation, and reduces treatment-related discomfort, ultimately leading to superior aesthetic and quality of life outcomes compared to IPL alone. This integrated approach addresses the multifactorial pathogenesis of sensitive skin and aligns with the trend in dermatology towards comprehensive, mechanism-based treatment regimens.
Data Sharing Statement
The datasets used during the present study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study received approval from the Institutional Review Board and Ethics Committee of the Zibo Central Hospital (Approval No.2026-056), and was conducted in accordance to the tenets of the Declaration of Helsinki. Given the exclusive use of de-identified patient data, which presented no potential harm or impact on patient care, the need for informed consent was waived by the Zibo Central Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The 2024 Zibo Medical and Health Science and Technology Project (No.20240409050).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Borghi A, Guarneri F, Montesi L, Pacetti L, Donelli I, Corazza M. Results from an extended study on the reliability of a questionnaire for the diagnosis of sensitive skin: confirmations and improvements. Int J Cosmet Sci. 2023;45:108–14. doi:10.1111/ics.12817
2. Borghi A, Guarneri F, Pacetti L, et al. Does sensitive skin lie in epidermal barrier impairment or abnormalities? Results from an observational study assessing biophysical parameters. Ital J Dermatol Venerol. 2024;159:349–356. doi:10.23736/S2784-8671.24.07714-4
3. Kircik L, Tan J, Lain ET, et al. One Acne™: a holistic management approach to improve overall skin quality and treatment outcomes in acne with or without sensitive skin. Int J Dermatol. 2025;64:637–646. doi:10.1111/ijd.17546
4. McCormick ET, Desai S, Friedman A. Insight into dermatology providers’ perspectives on approaches to sensitive skin: a pilot survey. J Drugs Dermatol. 2023;22:950–952. doi:10.36849/JDD.7450
5. Goh CL, Wu Y, Welsh B, et al. Challenges and real-world solutions for adoption of holistic skincare routine (cleansing, treatment, moisturization, and photoprotection) in acne, rosacea, atopic dermatitis, and sensitive skin: an expert consensus. J Cosmet Dermatol. 2024;23:2516–2523. doi:10.1111/jocd.16396
6. Jaros-Sajda A, Budzisz E, Erkiert-Polguj A. Ascorbic acid treatments as effective and safe anti-aging therapies for sensitive skin. Antioxidants. 2024;13. doi:10.3390/antiox13020174
7. Whiting C, Azim SA, Friedman A. Pioneers in sensitive skin research: the global sensitive skincare faculty by galderma. J Drugs Dermatol. 2024;23:407636.
8. Shu X, Zhao S, Huo W, et al. Clinical study of a spray containing birch juice for repairing sensitive skin. Arch Dermatol Res. 2023;315:2271–2281. doi:10.1007/s00403-023-02588-4
9. Lu YN, Cheng L, Shi XM. Correlation between the facial skin microbiome and sensitive skin using the 2bRAD-M technique. Int J Cosmet Sci. 2024;46:414–423. doi:10.1111/ics.12941
10. Zhang J, Zhou Y, Zhou F, et al. Development and validation of a prospective questionnaire for assessing oily sensitive skin. Int J Cosmet Sci. 2024;46:657–667. doi:10.1111/ics.12946
11. Zheng SY, Wan XX, Kambey PA, et al. Therapeutic role of growth factors in treating diabetic wound. World J Diabetes. 2023;14:364–395. doi:10.4239/wjd.v14.i4.364
12. Kitano H, Ishikawa T, Masaoka Y, Komiyama K, Takahashi M, Hidai C. The EGF motif with CXDXXXXYXCXC sequence suppresses fibrosis in a mouse skin wound model. Vivo. 2023;37:1486–1497. doi:10.21873/invivo.13233
13. Huang X, Liu Y, Fu H, Rong X, Zhao Y. Silencing IFIT3 suppresses the EGFR/VEGF pathway and modulates SOCS1 to attenuate skin fibrosis in systemic sclerosis. Apoptosis. 2025;30:1852–1874. doi:10.1007/s10495-025-02115-y
14. Hao PC, Burnouf T, Chiang CW, et al. Enhanced diabetic wound healing using platelet-derived extracellular vesicles and reduced graphene oxide in polymer-coordinated hydrogels. J Nanobiotechnology. 2023;21:318. doi:10.1186/s12951-023-02068-x
15. Kim S, Joo KM, Oh M, et al. Improving sensitive skin diagnosis by integrating diagnostic questionnaires, lactic acid sting test, and lipid profiling. J Cosmet Dermatol. 2025;24:e70099. doi:10.1111/jocd.70099
16. Berlin AL, Hussain M, Phelps R, Goldberg DJ. A prospective study of fractional scanned nonsequential carbon dioxide laser resurfacing: a clinical and histopathologic evaluation. Dermatol Surg. 2009;35:222–228. doi:10.1111/j.1524-4725.2008.34413.x
17. Finlay AY, Khan GK. Dermatology life quality index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19:210–216. doi:10.1111/j.1365-2230.1994.tb01167.x
18. Davies C, Miron RJ. Autolougous platelet concentrates in esthetic medicine. Periodontol. 2025;97:363–419. doi:10.1111/prd.12582
19. Lipka-Trawińska A, Deda A, Błońska-Fajfrowska B, et al. Quantitative image analysis of vascular skin response to intense pulsed light therapy. Clin Cosmet Invest Dermatol. 2025;18:2547–2560. doi:10.2147/CCID.S545832
20. Xiao Q, Chu W, Guo J, et al. CGF therapy: bridging androgenetic alopecia observations to psoriasis treatment via IL-17 pathway. Stem Cell Res Ther. 2024;15:353. doi:10.1186/s13287-024-03959-y
21. Dover JS, Liu C, Watchmaker J, et al. The history and advancement of light, lasers, and energy-based devices in dermatologic surgery. Dermatol Surg. 2025;51:113–122. doi:10.1097/DSS.0000000000004542
22. Chen B, Liu Y, Ke C, Xu S. A case of concentrated growth factor gel to fill the defect after large jaw cyst enucleation. Clin Case Rep. 2023;11:e8272. doi:10.1002/ccr3.8272
23. Yang X, Hou Z, Wang K, et al. Efficacy and mechanisms of concentrated growth factor on facial nerve rehabilitation in a rabbit model. Biomater Sci. 2025;13:1059–1074. doi:10.1039/D4BM01454E
24. Kim HO, Um JY, Kim HB, et al. Comprehensive approaches to diagnosis and treatment of sensitive skin. Ann Dermatol. 2025;37:173–182. doi:10.5021/ad.24.157
25. Silva APA, Alexandre da Silva Z, Melo WWP, Lima RR, Souza-Rodrigues RD. Photobiomodulation and dentistry: visualization and analysis of knowledge of the most cited articles. Photobiomodul Photomed Laser Surg. 2025;43:177–189. doi:10.1089/photob.2025.0004
26. Hu X, Liang A, Zhao T, et al. Efficacy and mechanism of high-purity HAMCC combined with CGF in promoting the repair of radiation-induced skin and soft tissue damage. PLoS One. 2025;20:e0330078. doi:10.1371/journal.pone.0330078
27. Bunjaj A, Brandao L, Siracuse K, Soti V. Platelet-Rich plasma for the treatment of plaque psoriasis: a systematic review. Cureus. 2023;15:e50356. doi:10.7759/cureus.50356
28. Seno SI, Shimazu H, Kobayashi H, Kogure E, Watanabe A, Isoyama T. Quantitative evaluation of skin barrier function using water evaporation time related to transepidermal water loss. Skin Res Technol. 2023;29:e13242. doi:10.1111/srt.13242
29. Se AM, Li L, Yu M. Poloxamer-based hydrogel with EGCG and rhEGF for diabetic foot ulcer treatment. J Mater Sci Mater Med. 2025;36:65. doi:10.1007/s10856-025-06917-z
30. Yu G, Lin S, Huang X, et al. Expression of an epidermal growth factor-transdermal peptide fusion protein in Arabidopsis thaliana and its therapeutic effects on skin barrier repair. Front Plant Sci. 2025;16:1573193. doi:10.3389/fpls.2025.1573193
31. Stein M, Böttcher N, Tohidnezhad M, et al. Platelet-Released Growth Factors (PRGFs) activate NRF2-ARE and modulate inflammatory response in an NRF2-Dependent manner in primary human keratinocytes. J Cosmet Dermatol. 2025;24:e70228. doi:10.1111/jocd.70228
32. Castro JBA, Oliveira B, Alves GG, et al. Effects of plasma rich in growth factors on wound healing in patients with venous ulcers. Regen Ther. 2024;25:284–289. doi:10.1016/j.reth.2024.01.002
33. Amiri R, Karimi Maskooni M, Farsinejad A, Karvar M, Khalili M, Aflatoonian M. Combination of plasma rich in growth factors with topical 4% hydroquinone compared with topical 4% hydroquinone alone in the treatment of dermal type of melasma: a single-blinded randomized split-face study. Indian Dermatol Online J. 2024;15:593–598. doi:10.4103/idoj.idoj_551_23
34. Park KY, López Gehrke I. Combined multilevel anti-aging strategies and practical applications of dermocosmetics in aesthetic procedures. J Eur Acad Dermatol Venereol. 2024;38:23–35. doi:10.1111/jdv.19975
35. Zonari A, Brace LE, Buhrer LB, et al. OS-01 Peptide topical formulation improves skin barrier function and reduces systemic inflammation markers: a pilot 12-week clinical trial. J Cosmet Dermatol. 2025;24:e70169. doi:10.1111/jocd.70169
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.