Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Efficacy and Best Mode of Delivery for Tranexamic Acid in Post-Inflammatory Hyperpigmentation: A Systematic Review
Authors Alsharif SH, Alghamdi AS ![]() , Alwayel ZA, Alaklabi SN
, Alwayel ZA, Alaklabi SN ![]() , Alyamani NA
, Alyamani NA ![]() , Sabsabee MA
, Sabsabee MA ![]() , Bu izran DAA, Alajlan AM
, Bu izran DAA, Alajlan AM ![]()
Received 26 October 2022
Accepted for publication 16 December 2022
Published 28 December 2022 Volume 2022:15 Pages 2873—2882
DOI https://doi.org/10.2147/CCID.S394889
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Sahar Hasan Alsharif,1 Asail Saeed Alghamdi,2 Zahraa Ali Alwayel,3 Saeed Nasser Alaklabi,4 Nawras Ali Alyamani,5 Mohamad Abdulwahab Sabsabee,6 Dunya Ali Abdulathem Bu izran,3 Abdulmajeed M Alajlan1
1Department of Dermatology, King Saud University, Riyadh, Saudi Arabia; 2Department of Medicine, Albaha University, Albaha, Saudi Arabia; 3Department of Medicine, King Faisal University, Al Ahsaa, Saudi Arabia; 4Department of Medicine, Bisha University, Bisha, Saudi Arabia; 5Department of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 6Department of Medicine, Sulaiman Al Rajhi University, Qassim, Saudi Arabia
Correspondence: Sahar Hasan Alsharif, Department of Dermatology, King Saud University, P.O. Box 24353, Riyadh, 11322, Saudi Arabia, Tel +00966555539141, Email [email protected]
Background: Post-inflammatory hyperpigmentation (PIH) is skin hyperpigmentation that occurs due to any inflammatory condition. Triggering the melanocytes by inflammation leads to melanin overproduction and deposition. Tranexamic acid (TXA) is an antifibrinolytic medication prescribed to treat bleeding. Recently, there are some studies about the use of TXA in the treatment of PIH.
Objective: The aim of this study is to identify the efficacy and the best mode of delivery for tranexamic acid in the treatment of PIH.
Methods: This systematic review is reported in accordance with PRISMA guidance. We included all relevant English-language studies that were published up to September 2022 in the following electronic databases: Cochrane Library, PubMed, Embase, and Google Scholar. The initial search yielded 61 articles, 9 of which were included after applying inclusion and exclusion criteria.
Results: The systematic review included a total of 196 patients who were over the age of 16 years old. Tranexamic acid was delivered orally in 4 studies, topically in 2 studies, and both simultaneously in 1 study. In addition, intradermal injection was used in 2 other studies. Almost all studies advocated the use of all routes for accelerating the clearance of hyperpigmentation with more favor towards topical and intradermal routes due to their mild reported side effects when compared to oral routes.
Conclusion: Intradermal TXA is considered the best route, which exhibits fewer side effects with less cost and excellent outcomes, while oral TXA is found to be less preferable than other routes due to the incidence of undesirable adverse events.
Keywords: tranexamic acid, post-inflammatory hyperpigmentation, TXA, PIH, efficacy
Introduction
Post-inflammatory hyperpigmentation (PIH) is hyperpigmentation of the skin that occurs due to any type of inflammatory condition. Triggering the melanocytes by inflammation leads to melanin overproduction and deposition. In severe cases, it extends to the dermis layer causing blue-gray discoloration, explaining why it is also known as hypermelanosis.1 Darker-skinned people (especially Fitzpatrick skin types III–VI) are more prone to have severe and chronic pigments.2 PIH in the epidermal layer mostly improves within a year, whereas in the dermal layer, it resolves slowly and may be permanent.3 Undesirable psychological problems like distress and low self-esteem can happen as a complication of untreated PIH.4
Men and women both have PIH at the same age, with an equal incidence. According to several international studies, African, Asian, and South American people have been found to have a greater incidence of pigmentary disorders, with PIH being the most prevalent diagnosis.5–7 In a single-center study of 1412 patient visits in the USA, dyschromia (apart from vitiligo) was found to be the second most common diagnosis among Black and Hispanic patients but not among the top ten diagnoses in Caucasian patients.8 Among Arab Americans, those with darker skin tones (originating from Yemen) express concerns about PIH more frequently than those with lighter skin tones such as people from Lebanon and Syria.9 In contrast to Caucasian patients, people with dark skin color are likely to get PIH more frequently, according to numerous epidemiological research.10 The prevalence of PIH was found to be higher in Asians with darker skin in a Singaporean study, demonstrating the significance of the level of constitutive cutaneous pigmentation in PIH development.11 No gender distinction exists in the prevalence of PIH.12 Epidemiological studies show that PIH is the third most common reason for African Americans to visit a dermatologist. When treating such patients, dermatologists should always address the triggering inflammatory disease that initiated the process of hypermelanosis; otherwise, the patient may feel that the treatment is insufficient.13
The most important treatment for PIH is strong ultraviolet (UV) and visible light (VL) blocking photoprotection. The most well-studied options for topical treatment are still hydroquinone-containing combinations like triple combination therapy. However, cysteamine and topical tranexamic acid (TXA) are also good options. Oral TXA could be a systemic treatment for people who do not respond to topical treatments. Chemical peels like glycolic acid and Jessner’s solution could be helpful for some patients as a part of their treatment. Low-fluence Q-switched lasers (LFQSL) could also help people with lesions that do not respond to treatment.14
As tranexamic acid exhibits antiplasmin activity, it is utilized to cure or prevent excessive blood loss. However, it has been demonstrated that tranexamic acid can reverse UV-induced hyperpigmentation. This is because tranexamic acid inhibits the binding of plasminogen to keratinocytes, which in turn reduces the activity of melanocyte tyrosinase, resulting in a decrease in arachidonic acid and prostaglandins. The latter is a well-known inflammatory mediator that leads to melanogenesis, particularly in the face region, which is regarded as a primary contributor to the appearance of aged skin.15
No evidence in the literature identified what route of TXA is better for targeting PIH, so we conducted this research to ascertain the best mode of delivery for optimal efficacy of TXA.
Materials and Methods
The review is reported in accordance with PRISMA guidance.
Literature Search
Systematic literature research was undertaken to identify relevant articles published up to September 2022 in the following electronic databases: Cochrane Library, PubMed, Embase, and Google Scholar.
The following Medical Subject Headings (MeSH) terms and keywords were used alone or in combination: “Tranexamic acid or TXA”, “post-inflammatory hyperpigmentation or post inflammatory melanosis or PIH”, “mode of delivery or method of administration or Administration method”, and ‘Efficacy or Effectiveness’. All titles and abstracts of publications identified in the course of the primary search were reviewed for relevance and eligibility. The reference lists of the selected papers and of the reviewed articles were also searched manually for articles that may have been missed in the initial search.
Study Selection
The inclusion criteria for this systematic review were as follows:
(1) Original studies (Randomized control trials, cohort studies, and case–control studies) on the usage of Tranexamic acid with or without any other medication to treat PIH.
(2) Descriptive studies (Case reports, case series, and cross-sectional studies) that report an apparent effect of TXA on treating PIH.
(3) Studies published in English.
(4) There were no restrictions on the mode of delivery, gender, race, and age.
We excluded:
(1) studies dealing only with melasma.
(2) unrelated topics, comments, and duplicates.
(3) Studies with data that are unreliable for extraction.
Data Extraction and Quality Assessment
Data Extraction
Data from the selected studies were extracted by two reviewers. The following types of data were extracted: study characteristics (first author, publication year, study design, countries/regions, sample size, mean age of participants, study duration, and PIH type), tranexamic acid treatment, delivery mode, dose, duration of follow-up, additional interventions, primary outcomes (melanin index [MI], and erythema index [EI]), and side effects. Disagreements were resolved through discussion.
Quality Assessment
Random clinical trials (RCTs) were assessed by the Cochrane risk-of-bias tool. We implemented the risk-of-bias criteria suggested by Newcastle-Ottawa Scale for cohort studies and JBI critical appraisal tool for case report studies. Two reviewers independently assessed the methodological quality of each study. Disagreements were resolved by consensus.
Results
In this review process, following the above-detailed selection [Figure 1], a total of 9 articles were selected, all meeting the inclusion criteria. All these articles were published in English. From a timing standpoint, out of these 9 selected articles, 3 were published in 2021,16–18 two in 2019,19,20 and only four in the period from 2011 to 2018.21–24 No article was published before 2011.
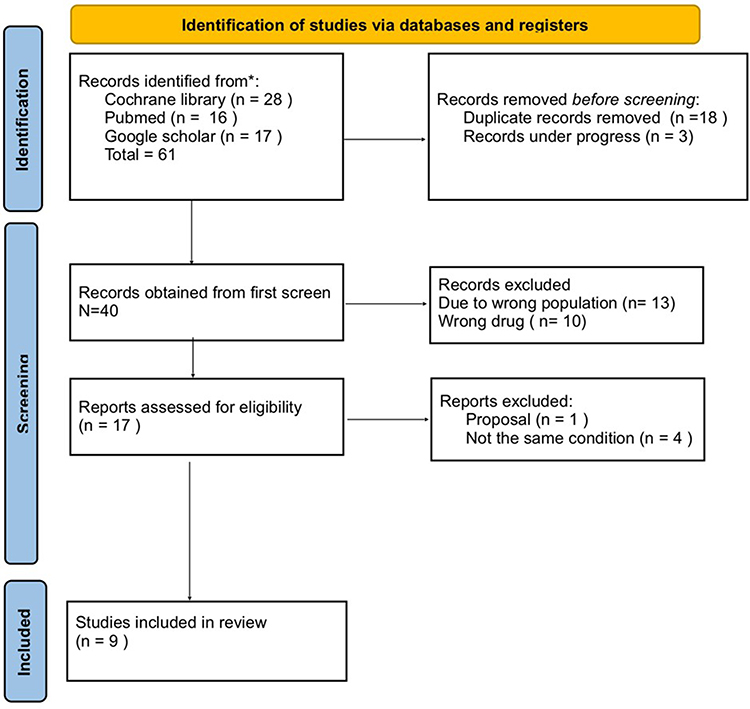 |
Figure 1 Flowchart of literature identification, screening, eligibility, and inclusion process. |
The agreement among the authors for the selection of the title was high (κ = 90%), and the one for the assessment of the full text (κ = 100%) was unanimous.
Study Characteristics
The main characteristics of the included studies are presented in Table 1. The studies were published in the period between 2011 and 2021. A total of 196 participants who were over the age of 16 years old were included.
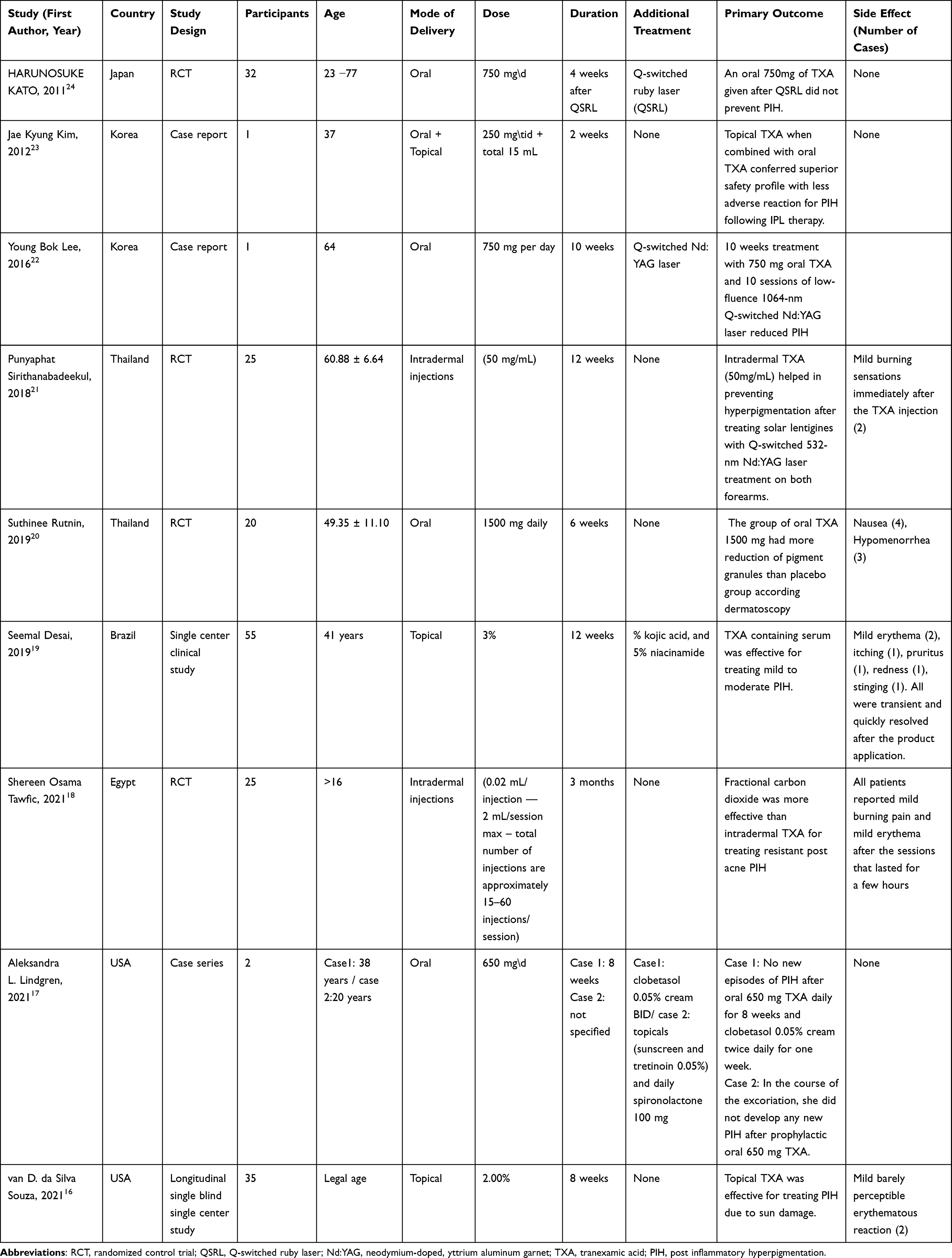 |
Table 1 Study Characteristics |
Among these 9 studies, 2 were conducted in Korea,22,23 2 in Thailand,20,21 2 in the USA,16,17 and 1 from each of the following countries: Japan,24 Brazil,19 and Egypt.18 Of the included studies, 2 were case reports,22,23 4 were RCTs,18,20,21,24 1 was a single-center clinical study,19 1 was a longitudinal single-blind single-center study,16 and 1 was a case series study.17 Tranexamic acid was delivered orally in 4 studies,17,20,22,24 topically in 2 studies,16,19 and both concurrently in 1 study.23 In addition, intradermal injection was used in 2 other studies.18,21
The selected studies included all types of PIH: PIH after Q-switched ruby laser,24 post Intense Pulsed Light (IPL) spots,23 PIH after allergic contact dermatitis to pure henna,22 PIH post Q-switched 532-nm Nd YAG laser,20,21 and post-acne hyperpigmentation.17,18
The additional treatments used were Q-switched ruby laser (QSRL),24 Q-switched Nd:YAG laser,22 spironolactone,17 and various topicals (kojic acid, niacinamide, clobetasol, sunscreen and tretinoin).17,19 However, the dose, duration, and side effects differ among these studies.
Quality Assessment
For an accurate valuation of the research, the quality was assessed using the Cochrane risk-of-bias tool in Figure 2 for RCTs, the modified Newcastle-Ottawa Scale in Table 2 for non-randomized trials, and JBI Critical Appraisal Checklist in Figure 3 for case reports. The study carried out by Kato, 2011, demonstrated concerns for bias in multiple aspects, which in turn could affect the validity of the study results, in contrast to the other included RCT studies that were of high-quality assessment with little to no issue of bias. By omitting the nonexposed cohort and the comparability components, modifications were done based on the Newcastle-Ottawa Scale to be utilized in the non-randomized trials. The total points are 6 lowering the giving cutoff to 5 for good quality and 4 for fair quality. Souza, 2020, was marked to be of fair quality in the cutoff of the scale as a result of the nonrepresentative population in addition to shorter follow-up duration. Even though all case reports suffered from poor definitions of demographics and adverse events, all of them described the used intervention and its efficacy in full detail.
 |
Table 2 Assessment of the Quality of the Included Non-Randomized Trials |
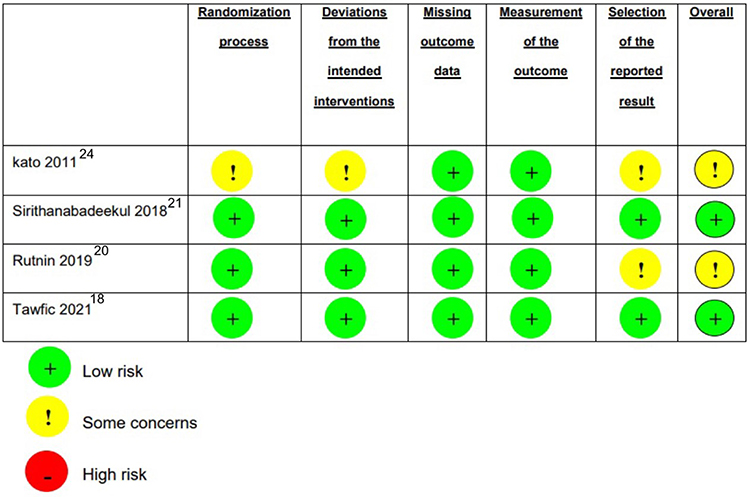 |
Figure 2 Risk of bias summary for included RCTs. |
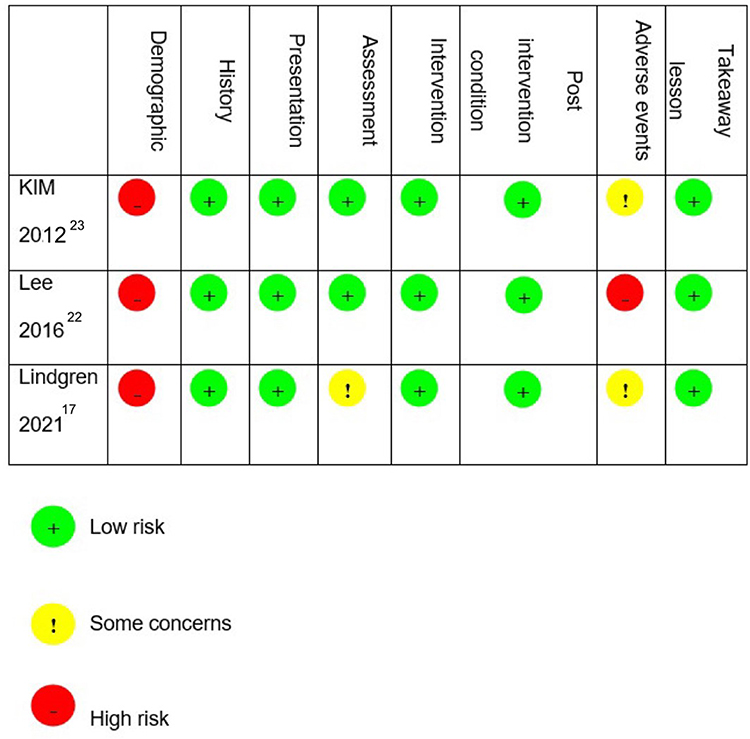 |
Figure 3 Assessment of the quality of the included case reports. |
Despite all study findings that provided support for tranexamic acid efficacy on PIH, Kato et al, 2011, did not support its use. This might be explained by the concerns of bias in multiple aspects of the study results. However, other studies came out with similar outcomes, which can be correlated with similar quality scores.
The Effect of the Intervention on the Outcome
Oral TXA
These studies17,20,22–24 used TXA by the oral route as shown in Table 1. As was found in the first case series with two independent cases published by Aleksandra L. Lindgren in 2021, a 38-year-old woman with Fitzpatrick skin type 3 complained of recurrent severe PIH after application of chemical peel and topical anesthetic cream, respectively. The patient presented with normal-appearing skin without new episodes of PIH at the 16th Week after ingesting oral 650 TXA daily for 8 weeks and applying clobetasol 0.05% cream twice daily for one week. The second case was of a 20-year-old woman with Fitzpatrick skin type 4 who had acne excoriee-induced PIH and was started on 650 mg of oral TXA as a preventative measure for the continuous excoriations and worsening PIH. Even though the excoriation persisted, she did not experience any new PIH throughout the study period.17 In 2019, Suthinee Rutnin divided the patients in his Prospective Randomized Controlled Study into two groups, one of which was assigned to receive oral TXA 1500 mg daily, while the other group received a placebo for 6 weeks, after delivering QS 532‐nm Nd:YAG laser treatment for both. After 4 weeks of evaluation, the inspection of the hyperpigmented lesions with a dermatoscope revealed the presence of tiny gray pigment granules in 18 patients who received oral TXA and in 20 patients who received a placebo (P = 0.487). Pigment granules were discovered in three patients (15%) in the TXA group and ten patients (52.63%) in the placebo group at the 12-week (P = 0.013) which indicated rapid clearance of PIH for who received oral TXA. Four (20%) in the TXA group and three (15%) in placebo group reported nausea as an adverse outcome. Furthermore, hypomenorrhea was reported by Three patients (15%) in the TXA group but not in the placebo group. Vascular thrombosis was absent in both groups.20 A case report of Korean female with allergic contact dermatitis due to p-phenylenediamine dihydrochloride (henna hair dye) followed by PIH which is improved after 10 weeks treatment with 750 mg oral TXA and 10 sessions of low-fluence 1064-nm Q-switched Nd:YAG laser.22 In contrast to these supporting findings, Kato et al established that the use of 750mg oral TXA given after QSRL had no significant influence upon preventing PIH of 32 participants with senile lentigines (SLs).24
Topical TXA
Three studies evaluated the efficacy of topical TXA whether as a monotherapy or an adjunctive treatment for hyperpigmentation. In a 12-week single-center clinical study involving 55 patients in Brazil, Desai S et al found that a novel topical facial serum containing 3% tranexamic acid, 1% kojic acid, and 5% niacinamide was effective for treating mild-to-moderate PIH.19 Similarly, an 8-week longitudinal single-blind center study involving 35 patients in the USA demonstrated that topical TXA (2%) was effective for treating PIH induced by sun damage.16 In both studies, an improvement from baseline was appreciated as early as 2 weeks with a noticeable change in the appearance of PIH, hyperpigmentation, skin texture, and skin tone homogeneity. The results established the safety of topical TXA over traditional regimens for hyperpigmentation with a minimal reported adverse reaction such as mild erythema, pruritus, and stinging which were transient and resolved immediately after application. Furthermore, topical TXA (15 mL, 3 times/week for 20 minutes), when combined with oral TXA (250 mg/TID), conferred a superior safety profile with less adverse reaction as was evident in a case report of 12 weeks duration conducted in Korea on a female subject with PIH following Intense Pulsed Light (IPL) therapy.23
Intradermal TXA
Two studies evaluated the efficacy of intradermal TXA as monotherapy for hyperpigmentation. One study revealed that the use of intradermal TXA (50mg/mL) helped in preventing hyperpigmentation of 25 patients with solar lentigines after Q-switched 532-nm Nd: YAG laser treatment on both forearms. Patients underwent treatment with intradermal TXA injection on one arm and normal saline injection on the other arm. The results showed that intradermal TXA was more effective for preventing PIH compared to the placebo side.21 In contrast, findings were different in a 12-week RCT involving 25 patients that evaluated the efficacy of intradermal TXA (0.02mL/injection) compared to fractional carbon dioxide laser for treating resistant post-acne hyperpigmentation. The study showed that fractional carbon dioxide was more effective than intradermal TXA. However, this study clearly claimed that intradermal TXA is cost-effective and thus can be a good alternative for patients who cannot afford laser treatments.18 The adverse reactions of both studies were minimal, such as mild burning pain, and mild erythema that resolved quickly after application.
Discussion
In this literature analysis, we assessed the results of studies that investigated the efficacy of TXA with all its possible routes; topical, intradermal, and oral, for preventing and treating PIH. For treating PIH, almost all studies advocated the use of all routes for accelerating the clearance of hyperpigmentation with more favor towards topical and intradermal routes due to their mild reported side effects when compared to the oral route. However, intradermal TXA showed to be less effective for treating resistant post-acne PIH when compared to low-dose fractional carbon dioxide laser treatment.18 As for preventing PIH, oral TXA was ineffective in preventing PIH compared with the placebo group, while intradermal TXA was slightly effective in reducing PIH compared with placebo (0.9% normal saline) injection.20,21,24 Based on our systematic study, TXA was well tolerated, with a small proportion of patients experiencing transient adverse effects. Adverse events mentioned in association with oral 1500 mg/day TXA were generally minor, some (eg, oligomenorrhoea) being associated with the hemostatic effects of TXA. Since TXA is an important component in the treatment of PIH as plasmin has known melanogenic properties, our systematic review suggests that topical TXA does indeed significantly reduce PIH while causing few side effects and that it should be considered as a potential treatment for PIH. Overall, while TXA was effective in treating and preventing PIH, its effectiveness could have been undermined by the different follow-up periods, different doses, and different forms of scoring used in each study. With this being the first systematic review exploring the effectiveness of TXA based on the administration routes for PIH, several studies can be dedicated to improving treatment modalities and effective routes of TXA administration for what is suitable for patient’s quality of life.
A couple of limitations are associated with this systematic review. Concerns of bias were observed, particularly in the study by Kato et al, 2011,24 and the risk of bias is created by the low number of participants divided into subgroups, no observation of TXA administration, and subgroups which necessitate more RCTs with larger sample size to get more robust results. Besides these limitations, language restriction might result in the loss of a substantial number of eligible studies. Furthermore, because there were not enough RCTs on the effect of TXA for improving PIH, we included other types of studies, which could result in biased estimates of effect and reduce generalizability.
Conclusion
This is the first systematic review aimed to find out the best mode of delivery of TXA in treating and preventing PIH. TXA has been performed with and without several adjuvants, at various oral dosages, at various topical concentrations, and at varied intradermal time intervals. Intradermal TXA is considered the best route, which exhibits fewer side effects with less cost and excellent outcomes, while oral TXA is found to be less preferable than intradermal and topical due to the incidence of undesirable adverse events. Because the number of studies included was insufficient, we recommend providing further information about the therapeutic differences between various TXA routes of administration as well as treatment duration, dosage, and co-therapy. We thus advise that more future large-scale RCTs focus on investigating the routes of TXA to provide what is best for patients with PIH and to compare it with other existing treatment modalities by outcomes, costs, and side effects; in order to create satisfying practice and basic guideline interventions for such cases.
Acknowledgment
This work was supported by the College of Medicine Research Center, Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia.
Funding
No funding was received.
Disclosure
The authors report no conflict of interest in this work.
References
1. Davis EC, Callender VD. Postinflammatory hyperpigmentation: a review of the epidemiology, clinical features, and treatment options in skin of color. J Clin Aesthet Dermatol. 2010;3(7):20–31.
2. Huerth KA, Hassan S, Callender VD. Therapeutic Insights in Melasma and Hyperpigmentation Management. J Drugs Dermatol. 2019;18(8):718–729.
3. Plensdorf S, Livieratos M, Dada N. Pigmentation disorders: diagnosis and management. Am Fam Physician. 2017;96(12):797–804.
4. Darji K, Varade R, West D, Armbrecht ES, Guo MA. Psychosocial impact of postinflammatory hyperpigmentation in patients with acne vulgaris. J Clin Aesthet Dermatol. 2017;10(5):18–23.
5. El-Essawi D, Musial JL, Hammad A, Lim HW. A survey of skin disease and skin-related issues in Arab Americans. J Am Acad Dermatol. 2007;56(6):933–938. doi:10.1016/j.jaad.2007.01.031
6. Sanchez MR. Cutaneous diseases in Latinos. Dermatol Clin. 2003;21(4):689–697. doi:10.1016/S0733-8635(03)00087-1
7. Dunwell P, Rose A. Study of the skin disease spectrum occurring in an Afro-Caribbean population. Int J Dermatol. 2003;42(4):287–289. doi:10.1046/j.1365-4362.2003.01358.x
8. Alexis AF, Sergay AB, Taylor SC. Common dermatologic disorders in skin of color: a comparative practice survey. Cutis. 2007;80(5):387–394.
9. Kaufman BP, Aman T, Alexis AF. Postinflammatory hyperpigmentation: epidemiology, clinical presentation, pathogenesis and treatment. Am J Clin Dermatol. 2017;19(4):489–503. doi:10.1007/s40257-017-0333-6
10. Davis EC, Callender VD. Postinflammatory hyperpigmentation: a review of the epidemiology, clinical features, and treatment options in skin of color. J Clin Aesthet Dermatol. 2010;3(7):20.
11. Silpa-archa N, Kohli I, Chaowattanapanit S, et al. Postinflammatory hyperpigmentation: a comprehensive overview: epidemiology, pathogenesis, clinical presentation, and noninvasive assessment technique. J Am Acad Dermatol. 2017;77(4):591–605. doi:10.1016/j.jaad.2017.01.035
12. Lotti T, Tanini T, Kovacevic M. Postinflammatory Hyperpigmentation. Hyperpigmentation. 2022;1:88–95.
13. Savory SA, Pandya AG. Post-inflammatory Hyperpigmentation. Dermatol Atlas Skin Color. 2014:21–25.
14. Moolla S, Miller-Monthrope Y. Dermatology: how to manage facial hyperpigmentation in skin of colour. Drugs in Context. 2022;11:1–14. doi:10.7573/dic.2021-11-2
15. Forbat E, Al‐Niaimi F. The emerging importance of tranexamic acid in dermatology. Wiley Online Library. 2020;45(4):445–449.
16. da Silva Souza ID, Lampe L, Winn D. New topical tranexamic acid derivative for the improvement of hyperpigmentation and inflammation in the sun-damaged skin. J Cosmet Dermatol. 2021;20(2):561–565. doi:10.1111/jocd.13545
17. Lindgren A, Austin A, The use of tranexamic acid to prevent and treat post-inflammatory hyperpigmentation; 2021. Available from: https://scholar.archive.org/work/3s2ct37ktbbfpm7vtd7mcxvede/access/wayback/https://jddonline.com/wp-content/themes/jdd-salient-child/download.php?pii=S1545961621P0344X&download=1.
18. Tawfic SO, Abdel Hay R, Salim H, Elmasry MF. Tranexamic acid versus fractional carbon dioxide laser in post-acne hyperpigmentation. Dermatol Ther. 2021;34(6). doi:10.1111/dth.15103
19. Desai S, Ayres E, Bak H, et al. Effect of a tranexamic acid, kojic acid, and niacinamide containing serum on facial dyschromia: a clinical evaluation. J Drugs Dermatol. 2019;18(5):454–459.
20. Rutnin S, Pruettivorawongse D, Prospective Randomized A. Controlled Study of Oral Tranexamic Acid for the Prevention of Postinflammatory Hyperpigmentation After Q-Switched 532-nm Nd: yAGLaser for Solar Lentigines. Lasers Surg Med. 2019;51(10):850–858. doi:10.1002/lsm.23135
21. Sirithanabadeekul P, Srieakpanit R. Intradermal tranexamic acid injections to prevent post-inflammatory hyperpigmentation after solar lentigo removal with a Q-switched 532-nm Nd: yAGlaser. J Cosmetic Laser Therapy. 2018;20(7–8):398–404. doi:10.1080/14764172.2018.1444770
22. Lee YB, Park SM. Combination treatment of low-fluence Q-switched Nd: yAGlaser and oral tranexamic acid for post-inflammatory hyperpigmentation due to allergic contact dermatitis to henna hair dye. J Cosmetic Laser Therapy. 2016;18(2):95–97. doi:10.3109/14764172.2015.1114634
23. Kyung Kim J, Eun Chang S, Won H, et al. Dramatic improvement of long lasting post-inflammatory hyperpigmentation by oral and topical tranexamic acid. File Scirp Org. 2012;2:62–63.
24. Kato H, Araki J, Eto H, et al. A prospective randomized controlled study of oral tranexamic acid for preventing postinflammatory hyperpigmentation after Q-switched ruby laser. Dermatol Surg. 2011;37(5):605–610. doi:10.1111/j.1524-4725.2011.01957.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.