Back to Journals » Local and Regional Anesthesia » Volume 14
Effects of Ultrasound-Guided Bilateral Cervical Plexus Block Combined with General Anesthesia in Patients Undergoing Total Parathyroidectomy and Partial Gland Autotransplantation Surgery
Authors Gong J ![]() , Yao Y, Wang Y
, Yao Y, Wang Y
Received 7 January 2021
Accepted for publication 17 March 2021
Published 23 April 2021 Volume 2021:14 Pages 75—83
DOI https://doi.org/10.2147/LRA.S299312
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Stefan Wirz
Jing Gong,1 Youxiu Yao,2 Yanbiao Wang3
1Department of Anesthesiology, The 960th Hospital of the People’s Liberation Army Joint Logistical Support Force, Jinan, Shandong, People’s Republic of China; 2Department of Anesthesiology, Peking University Third Hospital, Beijing, People’s Republic of China; 3Department of Orthopaedics, The 960th Hospital of the People’s Liberation Army Joint Logistical Support Force, Jinan, Shandong, People’s Republic of China
Correspondence: Youxiu Yao
Department of Anesthesiology, Peking University Third Hospital, Beijing, People’s Republic of China
Tel +8618810488772
Email [email protected]
Background: The aim of this study is to evaluate the effect of ultrasound-guided bilateral cervical plexus block on general anesthesia, postoperative analgesia, and surgical outcomes in patients undergoing total parathyroidectomy with autotransplantation.
Patients and Methods: Forty-eight ASA III–IV patients with hyperparathyroidism secondary to renal failure were included: 24 patients received ultrasound-guided bilateral superficial and deep cervical plexus block combined with general anesthesia (group A), and 24 patients received general anesthesia alone (group B). Postoperative patient-controlled intravenous analgesia was provided with sufentanil 2 μg/kg. The primary outcome is the postoperative pain scores. Secondary outcomes include intraoperative remifentanil dosage, changes in hemodynamics, extubation time, and sufentanil consumption. Surgical outcomes regarding calcium, phosphorus and parathormone values were also noted.
Results: The patients in group A required less remifentanil than group B (2.56± 0.92mg vs 3.38± 0.84mg, P=0.002) and lower VAS scores at 1, 3, 10, 24, and 48h postoperatively (P < 0.001). While the systolic blood pressure in group A patients was significantly greater than that in group B at T3 (immediately after extubation, [138.33± 11.36 vs 129.08± 17.06 mmHg; P=0.032]), heart rates in group A were lower than in group B at 1 min before induction (T1 [89.46 ± 9.14 vs 96.71± 14.19, P=0.042]) and 1 min after intubation (T2 [70.08 ± 5.35 vs 79.25 ± 11.81, P=0.002]). The extubation time in group A was shorter than that in group B (P < 0.001). There was no difference in calcium, phosphorus and parathormone values, nor in sufentanil consumption between the groups.
Conclusion: Ultrasound-guided bilateral superficial and deep cervical plexus block combined with general anesthesia for TPTA is an effective strategy to improve anesthesia management and achieve better postoperative analgesia, and has no impact on surgical outcomes.
Keywords: ultrasound guidance, cervical plexus block, hyperparathyroidism, renal failure
Introduction
Secondary hyperparathyroidism (SHPT) is one of the common complications in hemodialysis patients in the final stages of uremia. Patients with hyperparathyroidism secondary to renal failure are characterized by elevated levels of parathyroid hormone, and high calcium and phosphate concentrations. Related symptoms include itching, bone pain, and inattention,1 which seriously affect the quality of life and survival period of patients. Pain levels are extremely high, with 50% of patients unresponsive to drugs and requiring surgical treatment.2
Total parathyroidectomy with autotransplantation (TPTA) is the most commonly performed operation for this kind of patient.3 General anesthesia is necessary to reduce discomfort, as intraoperative neuroelectrophysiological monitoring (IONM), used globally at a rate of 20–40% in thyroid surgery,4 is introduced to avoid nerve injury during the operation. Significant risks are involved in placing SHPT patients under general anesthesia due to their poor physical condition: accompanying conditions include secondary hypertension, hyperkalemia, arrhythmia, water and sodium exchange dysregulation, bone deformity, and osteoporosis; some patients may even suffer heart failure and mild liver function damage. It has been reported that ultrasound-guided bilateral cervical plexus block (CPB) is a better method with higher patient satisfaction that can provide good analgesia in neck surgery,5 but its application alone cannot fully meet the needs of TPTA surgery. To sum up, the aim of this study is to explore a combined anesthesia method for this category of patients and to provide reference for clinical anesthesia more generally.
Patients and Methods
Study Design and Participants
This is an observational study discussed and approved by the ethics committee of the 960th Hospital of the People’s Liberation Army Joint Logistical Support Force. The participants provided signed informed consent; written informed consent for publication of clinical images was also obtained from the patients. This study was conducted in accordance with the Declaration of Helsinki.
During the pre-operative visit, the purpose, risks and benefits of the procedure were introduced to patients by trained researchers. All personal information will remain strictly confidential and will be used for research purposes only.
From December 2017 to March 2019, SHPT patients scheduled to undergo TPTA in the Department of Thyroid and Breast in our hospital were recruited. Inclusion criteria: age 24–68 years, gender unlimited, American Society of Anesthesiologists (ASA) III–IV. Exclusion criteria included primary hyperparathyroidism, hyperparathyroidism concomitant with thyroid diseases, peripheral or central nervous system diseases, severe cardiopulmonary dysfunction, refusal of nerve monitoring endotracheal intubation, drug abuse or long-term use of analgesic drugs that would affect the outcome of the trial.
Study Protocol
The study consisted of two groups (n=24). Group A: bilateral cervical plexus block combined with general anesthesia under the monitoring of Narcotrend (observation group); group B: general anesthesia alone (control group). All anesthesia and operations were performed by the same team. Once the patient entered the operating theatre, an intravenous drip infusion of sodium lactate Ringer’s solution was administered after securing the lower extremity vein access, with fluid input strictly controlled. Routine monitoring included pulse oxygen saturation, ECG, and invasive arterial blood pressure (ABP) obtained by puncturing the dorsalis pedis artery.
The patients in group B received general anesthesia alone. After preoxygenation, anesthesia was induced via intravenous injection of midazolam 0.04 mg/kg, sufentanil 0.4 μg/kg, etomidate emulsion 0.3 mg/kg, and cisatracurium 0.2 mg/kg according to the patient’s weight. After rapid induction, the nerve monitoring tracheal tube was intubated and fixed securely, and then intermittent positive pressure ventilation was performed at a tidal volume of 8–10 mL/kg, a respiratory frequency of 12–14 times/min, and an inspiratory-to-expiratory ratio of 1:2 to maintain expiratory carbon dioxide between 35–40 mmHg. 2–12 mg/kg/h propofol, 0.1–0.2 mg/kg/h cisatracurium, and 0.02–0.04 mg/kg/h remifentanil were infused to maintain depth of anesthesia. During the operation, the Narcotrend index was maintained at D1 (50–55). A mean arterial pressure (MAP) of less than 60 mmHg was considered as hypotension, in which case 1 mg dopamine was infused intravenously. All infused anesthesia drugs were stopped 10 minutes before the completion of surgery. The tracheal tube was removed after spontaneous respiration, muscle strength and tidal volume returned to normal; the Narcotrend index was greater than 95 at the end of each surgery. All patients left the operating theatre and returned to the postoperative ward with a Steward score > 5.
In group A, the patients were supine with the head tilted to the opposite side. A high frequency linear array probe was used and a short bevel needle was inserted into the plane using in-plane technique (Figure 1). Under the guidance of ultrasound, the deep cervical plexus block was performed using the method of one point transverse process of the fourth cervical vertebrae, and 5mL of local anesthetic mixture (2% lidocaine 5mL + 0.75% ropicaine 5mL + normal saline 5mL) was infused (Figure 2A). The puncture needle was withdrawn beneath the middle layer of the cervical fascia (Figure 2B) and 7mL of the above local anesthetic mixture was injected. When no abnormality was observed after 10 to 15 minutes, the deep and superficial cervical plexus blocks on the opposite side were performed using the same blocking process. After observing for 10min, the operation then proceeded to the next step. The induction and maintenance of general anesthesia were the same for group B. Patient controlled intravenous analgesia (PCIA) pumps were used in both groups after surgery. The volume of PCIA was 100 mL, containing 2 μg/kg sufentanil. The background infusion rate was maintained at 2 mL/h, and the patient controlled bolus volume was 2 mL, with a lockout interval of 15 min.
 |
Figure 1 Position of the ultrasound probe and the needle during the procedure of cervical plexus blocks. |
 |
Figure 2 Ultrasound-guided deep and superficial cervical plexus block. (A) Ultrasound-guided transverse process block of the fourth cervical vertebrae. (B) Ultrasound-guided superficial cervical plexus block. Position of the needle and local anesthetic distribution was showed under the guidance of ultrasound during the procedure. Abbreviations: SCM, sternocleidomastoid muscle; IJV, internal jugular vein; CB, carotid bifurcation; C4, transverse process of the fourth cervical vertebrae. |
Data Collection and Outcome Measures
The primary outcome measure in this study was the postoperative visual analogue scale (VAS) scores at 10 minutes after extubation (T4), and at 1h, 3h, 10h, 24h and 48h after surgery. Secondary aims were to investigate the dosage of remifentanil during the operation, the systolic blood pressure, diastolic blood pressure and heart rate of patients at the following time points: after entering the room (T0), 1 minute before induction of general anesthesia (T1), 1 minute after intubation (T2), immediately after extubation (T3), and 10 minutes after extubation (T4); and the medication during the maintenance period of intravenous anesthesia in the two groups, including the dosages of propofol and cisatracurium, and cases of dopamine use. The time of operation, maintenance of intravenous anesthesia and extubation were all recorded. Adverse reactions of dyspnea, pharyngeal pain, nausea and vomiting, and sufentanil consumption in the postoperative period were also noted. Surgical outcome data regarding calcium, phosphorus and parathormone values were collected.
Statistical Analysis
SPSS 21.0 software was used for statistical analysis. The quantitative data of normal distribution was expressed as mean ± standard deviation, and the comparison between the two groups was performed by independent sample t-test; the data between multiple time points was analyzed by repeated measures ANOVA, with Bonferroni’s post hoc test if necessary. Categorical variables are summarized as counts (percentages); Chi square test or Fisher’s exact test methods are used for counting data. P < 0.05 is considered to be statistically significant. Graph displays were performed using GraphPad Prism software version 6.0.
Results
Results were similar in terms of gender, weight, age, ASA grade, and comorbidities between the two groups (P > 0.05) (Table 1). The VAS scores in group A were significantly lower than those of group B at 1h, 3h, 10h, 24h and 48h postoperatively (P < 0.05), whereas there was no difference between scores at T4 (10 min after extubation) (Figure 3). The pain scores in both groups were within tolerance levels for all patients.
 |
Table 1 Patient Demography and Comorbidities Data |
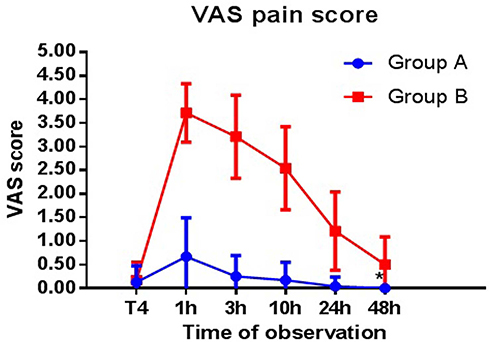 |
Figure 3 Postoperative 48-hour pain trends (mean±SD). *P< 0.001, ANOVA with repeated measures. T4 indicates 10 min after extubation. |
Patients in group A reported less remifentanil use than group B (2.56±0.92 mg vs 3.38±0.84 mg, P=0.002). Anesthetics (propofol) and cisatracurium consumption were also significantly lower in group A patients than in group B after anesthesia induction (P < 0.05). There was no difference in dopamine use between the two groups (P > 0.05) (Table 2). The extubation time of group A was less than that of group B (P = 0.000), whereas no statistical difference was observed between the two groups in terms of anesthesia maintenance time and operation time (P > 0.05).
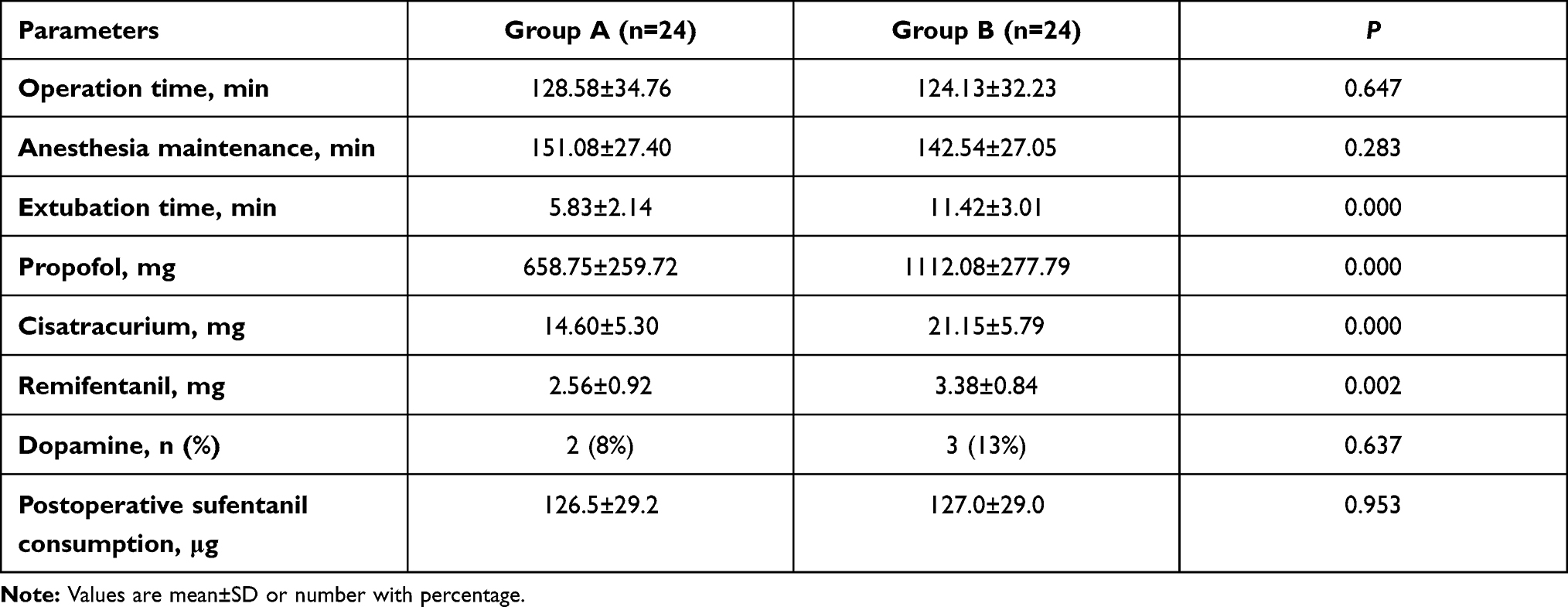 |
Table 2 Comparison of Anesthesia and Operation Time, and Drug Usage During the Perioperative Period |
There were no significant differences at T0 and T4 in invasive systolic blood pressure, diastolic blood pressure, and heart rate (HR) between the two groups (P > 0.05). However, significant differences were observed over time (T1, T2 and T3). The HRs at T1 and T2 in group A were significantly lower than those in group B (89.46 ± 9.14 vs 96.71 ± 14.19, P =0.042; 70.08 ± 5.35 vs 79.25 ± 11.81, P=0.002; respectively), whereas the invasive blood pressures at the two timepoints were similar (P > 0.05). At T3 the invasive systolic blood pressure in group A (138.33 ± 11.36 mmHg) was significantly higher than in group B (129.08 ± 17.06 mmHg) (P =0.032), whereas differences in invasive diastolic blood pressure and HR did not reach statistical significance (78.21±7.62 vs 73.71±8.06, P=0.053; 76.13±6.58 vs 74.71±11.94, P=0.614; respectively) (Table 3).
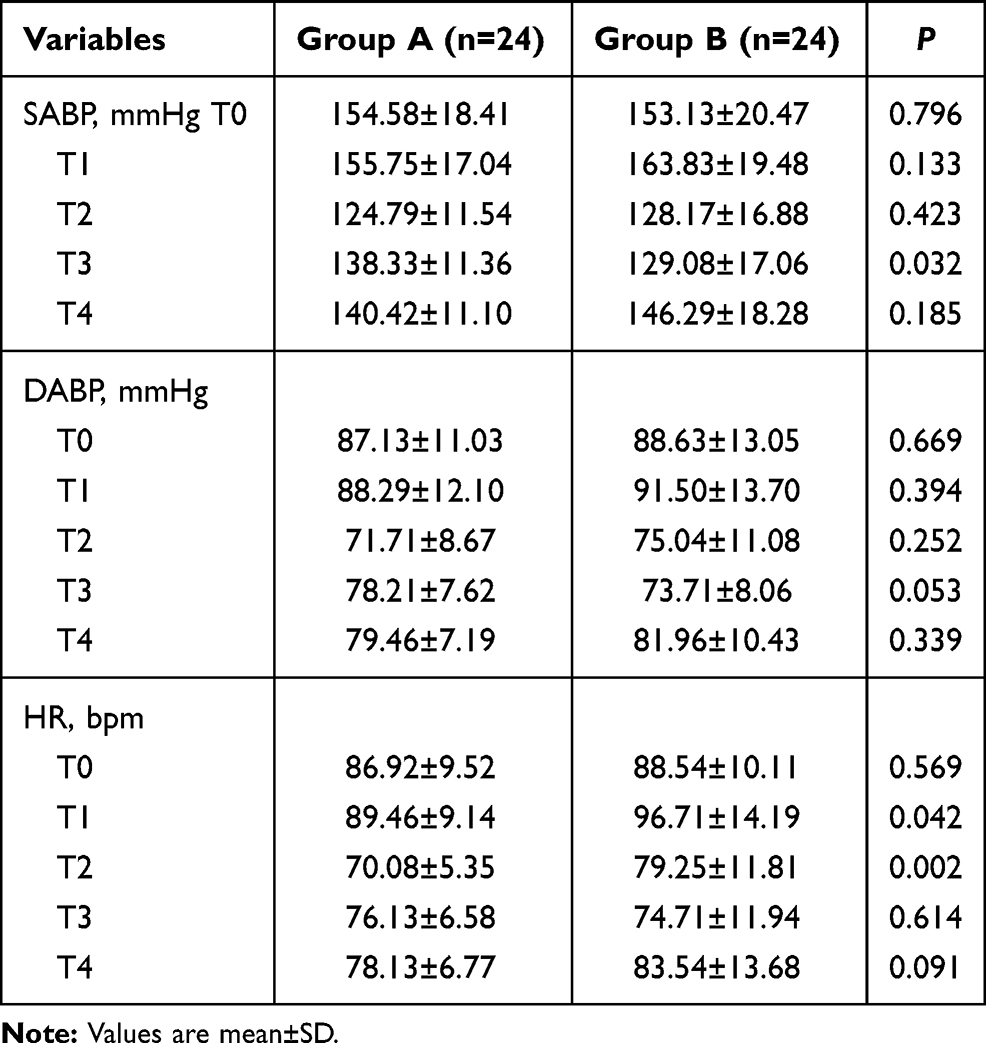 |
Table 3 Hemodynamics in the Operating Room (Invasive Systolic Arterial Blood Pressure [SABP], Diastolic Arterial Blood Pressure [DABP], and Heart Rate [HR]) |
In a 48h follow-up, there were no cases of dyspnea in either group. The incidence of pharyngeal pain in group B (8 patients) was significantly higher than in group A (0 patients) (P < 0.05). No significant difference was observed in terms of PONV between the two groups (P > 0.05) (Table 4). Calcium, phosphorus and parathormone values decreased after surgery, but there was no significant difference between the groups (Table 5, Figure 4). Details of localization of parathyroid adenomas with double-phase 99mTc-sestamibi (99mTc-MIBI) imaging techniques for this study are provided (Figure 5).
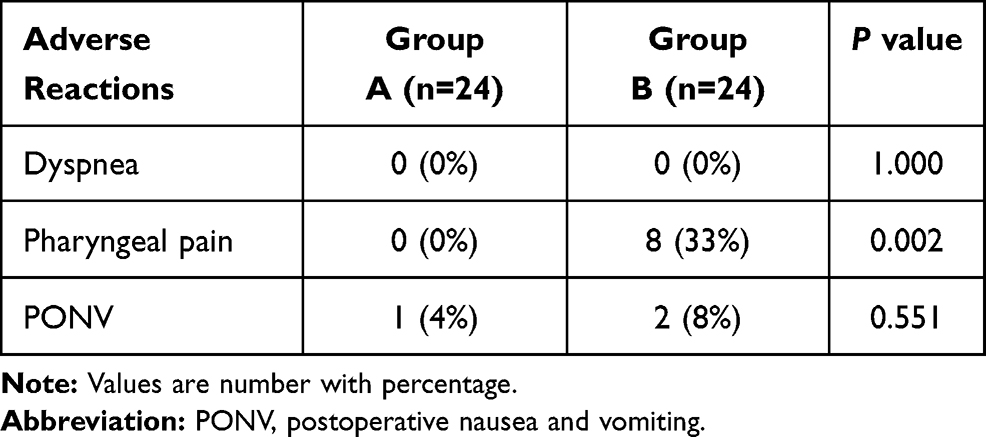 |
Table 4 Statistics of Adverse Reactions |
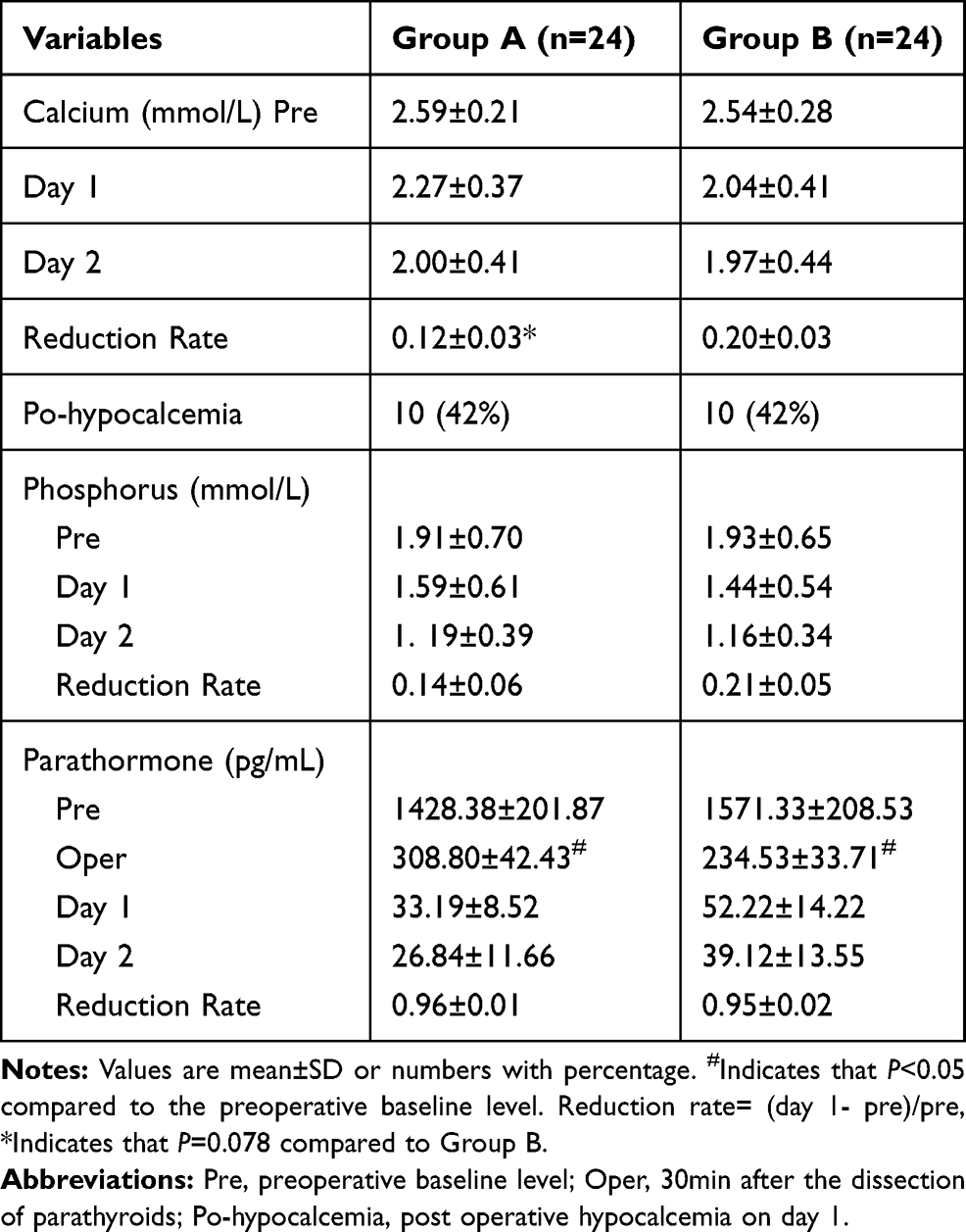 |
Table 5 Changes of Calcium, Phosphorus and Parathormone During the Perioperative Period |
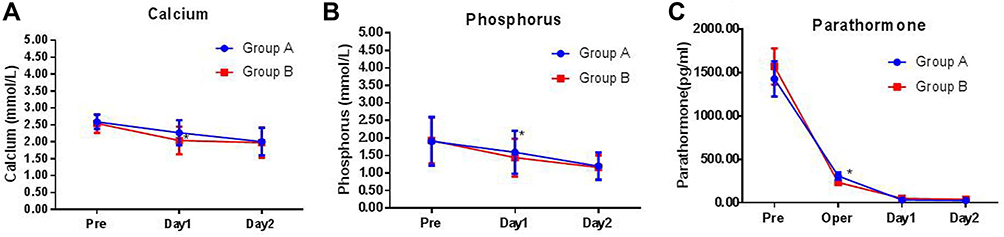 |
Figure 4 Calcium (A), phosphorus (B) and parathormone (C) values decreased after the surgery. *Indicates that there was no significant difference between the groups (P> 0.05). |
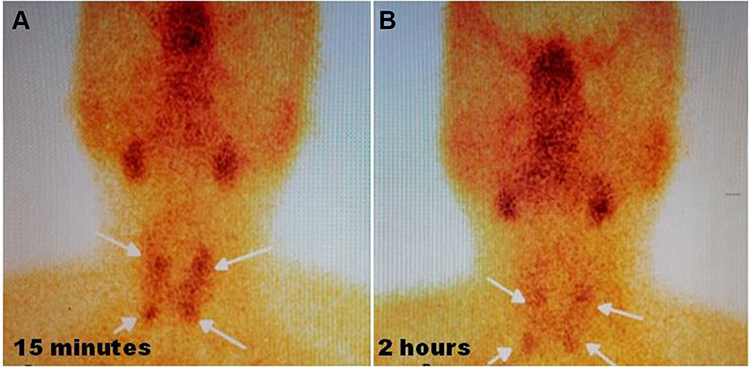 |
Figure 5 Localized nodules with increased uptake of radionuclides in the parathyroid region of bilateral thyroid lobes were considered as parathyroid hyperplasia or adenomas. 99mTc-MIBI was injected intravenously, and anterior imaging of the neck was performed 15 minutes after injection. Bilateral lobes of the thyroid gland were normal, and the radioactivity was evenly distributed. Radioactivity was aggregated in the parathyroid area of the upper and lower poles of the thyroid gland (A). After 2 hours delay, the distribution of thyroid radioactivity was lower than before, and there was still a slight localized radioactive accumulation in the parathyroid region of the upper and lower poles of the thyroid gland (B). |
Discussion
The majority of SHPT patients require surgical treatment, and the safety of parathyroidectomy with anesthesia methods including local anesthesia and cervical plexus block have been described.6 TPTA is used in our hospital to ensure postoperative outcomes, and is one of the most effective options available at present.7 There are more comorbidities and greater anesthesia risks in these patients, which is less reported.8 Although the safety of bilateral superficial plus deep cervical plexus block combined with general anesthesia in thyroid surgery have been reported, along with the improved postoperative analgesic effects compared to the traditional method,9,10 in previous studies it has always been a landmark technique performed in low risk (ASA I–II) patients. The innovation of our study is that ultrasound-guided bilateral deep plus superficial cervical block anesthesia was performed in high-risk ASA III/IV patients with secondary hyperparathyroidism undergoing TPTA surgery, which achieved a hemodynamic stability in anesthesia induction and maintenance, and reduced the dosage of anesthetics. No hoarseness, phrenic nerve block or other complications were observed either before induction or after extubation. The safety of bilateral cervical plexus block is further improved, since the cervical plexus block is combined with general anesthesia and performed under the guidance of ultrasound, providing an accurate location of the puncture sites and a dynamically observed needle path. In addition, the combination with general anesthesia in this study eliminates concerns about the lagging effect of bilateral cervical plexus, which can lead to respiratory depression and other complications. We do not advocate bilateral deep plus superficial cervical plexus block in patients without general anesthesia.
The extubation time of group A was significantly shorter than that of group B, which was considered to be associated with reduced dosages of remifentanil, propofol and atracurium during the anesthesia maintenance period. Bilateral cervical plexus block (including deep plus superficial plexus block) combined with general anesthesia is feasible and safe. In general, in this study, patients undergoing cervical plexus anesthesia combined with general anesthesia under ultrasound guidance were more stable than those under general anesthesia alone. These patients also woke up more quickly, with a shorter extubation time, hence reducing retention time in the operating room. The total dosage of anesthetics was reduced, which may lessen the impact of drug metabolism on side effects in patients with secondary hyperparathyroidism, and anesthesia related complications such as hypotension. The whole anesthesia process and early postoperative recovery of patients was relatively comfortable.
The evaluation of postoperative analgesia is affected by surgical approaches and patients’ individual differences. In this study, all patients were sent to the general ward after extubation. Based on the VAS scores, the overall postoperative analgesia effect in group A was better than that in group B. It has also been reported that ultrasound-guided cervical plexus anesthesia can meet the requirements of parathyroidectomy,11,12 and provide better postoperative analgesia than general anesthesia and reduce the incidence of postoperative vomiting and nausea;13 nevertheless, 10.6% of such patients will need to change to general anesthesia,14 whereas ultrasound-guided cervical plexus anesthesia combined with general anesthesia will not present this awkward situation.
In this study, the patients undergoing general anesthesia combined with nerve block still used postoperative intravenous analgesia, which was very convenient and reduced the usage of opioid analgesics post-surgery. In addition, the analgesic effectiveness of this combined anesthesia method was greater than that of intravenous analgesia alone, and there is no gap period, a fact which is accepted by the majority of anesthesiologists. Overall, this study has achieved a relatively satisfactory postoperative analgesic effect.
According to the data, both groups showed very low incidence of postoperative complications such as dyspnea, nausea and vomiting, and hoarseness; however, the incidence of pharyngeal pain in group B was higher than in group A, which is considered to be related to the use of nerve monitoring tracheal tubes and requires further study. In order to ensure the effectiveness of TPTA and reduce surgical complications, general anesthesia with nerve monitoring endotracheal intubation is needed to better expose the recurrent laryngeal nerve, which can provide greater comfort and a shortened operation time. With the introduction of IONM technology, injury to the recurrent laryngeal nerve can be effectively avoided.15 Only when the recurrent laryngeal nerve is completely exposed can injury be effectively reduced,16 and a variety of comparative results support the effectiveness of IONM.17
In view of the comorbidities, poor physical condition, and high risk of anesthesia in patients with secondary hyperparathyroidism, the use of a nerve monitoring tracheal tube is preferred during the operation, which can shorten operation times and avoid injury to the laryngeal nerve. Of course, the application of intraoperative recurrent laryngeal nerve monitoring technology is not absolutely safe. Although improvements in surgical technology and equipment have reduced the incidence of recurrent laryngeal nerve injuries,18,19 some injuries still occur to the non-recurrent laryngeal nerve, or in cases of serious adhesion in the surgical field. Such patients should not undergo rushed extubation, and the recovery of breath should be closely monitored to avoid anesthesia accidents. Suspension of arytenoid and cricoid cartilage, or tracheotomy may be performed in severe cases of recurrent laryngeal nerve injury.
In this study, cervical plexus block under the guidance of ultrasound was more accurate, and no obvious complications were observed. It is a superior anesthesia scheme with the following advantages: (1) the intubation response is relatively mild with a smaller change in heart rate, which is possibly because the effect of the bilateral cervical plexus block may spread and affect the laryngeal nerve to reduce intubation stress, though further research is needed to confirm this; (2) hemodynamics during the whole procedure are more stable, since the dosage of anesthetics is reduced, which can permit an early extubation benefiting an enhanced recovery; (3) the scheme has a better postoperative analgesic effect with reduced use of opioids.
The present study also has some limitations. We acknowledge that this work is a small sample sized observational study. First, although the number of cervical blocks was adequate to pursue the primary outcome, the relatively small sample was likely insufficient to detect differences in the secondary outcomes of complications between the groups. Second, the design of an observational study means that there is no real intervention in the treatment of patients. There was no placebo control group because the ethics committee could not allow puncture only infusing normal saline; it is consequently difficult to form a strict sense of control. In addition, in this study, we could only decide which patients received cervical plexus block or not according to the patients’ choices, which is not a rigorous randomization method.
Conclusions
Ultrasound-guided bilateral deep and superficial CPB combined with general anesthesia can not only promote better anesthesia management, but also reduce the incidence of postoperative pain and pharyngeal discomfort. It provides a better anesthesia scheme and can be safely used in TPTA for patients with hyperparathyroidism secondary to renal failure.
Abbreviations
TPTA, total parathyroidectomy with autotransplantation; SHPT, Secondary hyperparathyroidism; IONM, intraoperative neuroelectrophysiological monitoring; CPB, cervical plexus block; VAS, visual analogue scale; 99mTc-MIBI, 99mTc-sestamibi.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study was approved by the ethics committee of the 960th Hospital of the People’s Liberation Army Joint Logistical Support Force. The participants provided signed informed consent.
Consent for Publication
Written informed consent for publication of the clinical details and clinical images was obtained from the patients.
Acknowledgments
This work was supported in part by the National Natural Science Foundation of China (81500178). The funding body had no role in the design of the study, the collection, analysis, and interpretation of data, or the writing of the manuscript. Thanks to Richard Lester from Peking University Health Sciences Center for help in editing and polishing the language of this paper. Dr. Yanbiao Wang is now affiliated with The Third Affiliated Hospital of Shandong First Medical University, Jinan, Shandong, People's Republic of China.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. van der Plas WY, Noltes ME, van Ginhoven TM, Kruijff S. Secondary and tertiary hyperparathyroidism: a narrative review. Scand J Surg. 2019;1457496919866015. doi:10.1177/1457496919866015
2. Jing Y, Zhao H, Ge Y, et al. Application of total parathyroidectomy with auto-transplantation for uremia secondary hyperparathyroidism treatment. Int J Clin Exp Med. 2015;8(7):11188–11194.
3. Hou J, Shan H, Zhang Y, et al. Network meta-analysis of surgical treatment for secondary hyperparathyroidism. Am J Otolaryngol. 2019;41(2):102370. doi:10.1016/j.amjoto.2019.102370
4. Horne SK, Gal TJ, Brennan JA. Prevalence and patterns of intraoperative nerve monitoring for thyroidectomy. Otolaryngol Head Neck Surg. 2007;136(6):952–956. doi:10.1016/j.otohns.2007.02.011
5. Sait Kavakli A, Kavrut Ozturk N, Umut Ayoglu R, et al. Comparison of combined (Deep and Superficial) and intermediate cervical plexus block by use of ultrasound guidance for carotid endarterectomy. J Cardiothorac Vasc Anesth. 2016;30(2):317–322. doi:10.1053/j.jvca.2015.07.032
6. Rajeev P, Stechman MJ, Kirk H, Gleeson FV, Mihai R, Sadler GP. Safety and efficacy of minimally-invasive parathyroidectomy (MIP) under local anaesthesia without intra-operative PTH measurement. Int J Surg. 2013;11(3):275–277. doi:10.1016/j.ijsu.2013.02.002
7. Polistena A, Sanguinetti A, Lucchini R, et al. Surgical treatment of secondary hyperparathyroidism in elderly patients: an institutional experience. Aging Clin Exp Res. 2017;29(Suppl 1):23–28. doi:10.1007/s40520-016-0669-4
8. Gunst MA, Drop LJ. Chronic hypercalcaemia secondary to hyperparathyroidism: a risk factor during anaesthesia? Br J Anaesth. 1980;52(5):507–511. doi:10.1093/bja/52.5.507
9. Aunac S, Carlier M, Singelyn F, De Kock M. The analgesic efficacy of bilateral combined superficial and deep cervical plexus block administered before thyroid surgery under general anesthesia. Anesth Analg. 2002;95(3):746–50, table of contents. doi:10.1097/00000539-200209000-00039
10. Senapathi TGA, Widnyana IMG, Aribawa I, et al. Ultrasound-guided bilateral superficial cervical plexus block is more effective than landmark technique for reducing pain from thyroidectomy. J Pain Res. 2017;10:1619–1622. doi:10.2147/JPR.S138222
11. Pintaric TS, Hocevar M, Jereb S, Casati A, Novak Jankovic V. A prospective, randomized comparison between combined (deep and superficial) and superficial cervical plexus block with levobupivacaine for minimally invasive parathyroidectomy. Anesth Analg. 2007;105(4):1160–3, table of contents. doi:10.1213/01.ane.0000280443.03867.12
12. Lee KH, Jeon SY. Parathyroidectomy under superficial cervical plexus block in a patient with severe kyphoscoliosis. Indian J Anaesth. 2014;58(3):355–356. doi:10.4103/0019-5049.135091
13. Black MJ, Ruscher AE, Lederman J, Chen H. Local/cervical block anesthesia versus general anesthesia for minimally invasive parathyroidectomy: what are the advantages? Ann Surg Oncol. 2007;14(2):744–749. doi:10.1245/s10434-006-9261-z
14. Carling T, Donovan P, Rinder C, Udelsman R. Minimally invasive parathyroidectomy using cervical block: reasons for conversion to general anesthesia. Arch Surg. 2006;141(4):
15. Perie S, Ait-Mansour A, Devos M, Sonji G, Baujat B, St Guily JL. Value of recurrent laryngeal nerve monitoring in the operative strategy during total thyroidectomy and parathyroidectomy. Eur Ann Otorhinolaryngol Head Neck Dis. 2013;130(3):131–136. doi:10.1016/j.anorl.2012.09.007
16. Dralle H, Sekulla C, Lorenz K, Brauckhoff M, Machens A, German ISG. Intraoperative monitoring of the recurrent laryngeal nerve in thyroid surgery. World J Surg. 2008;32(7):1358–1366. doi:10.1007/s00268-008-9483-2
17. Randolph GW, Kamani D. Intraoperative electrophysiologic monitoring of the recurrent laryngeal nerve during thyroid and parathyroid surgery: experience with 1381 nerves at risk. Laryngoscope. 2017;127(1):280–286. doi:10.1002/lary.26166
18. Farizon B, Gavid M, Karkas A, Dumollard JM, Peoc’h M, Prades JM. Intraoperative monitoring of the recurrent laryngeal nerve by vagal nerve stimulation in thyroid surgery. Eur Arch Otorhinolaryngol. 2017;274(1):421–426. doi:10.1007/s00405-016-4191-2
19. Lynch J, Parameswaran R. Management of unilateral recurrent laryngeal nerve injury after thyroid surgery: a review. Head Neck. 2017;39(7):1470–1478. doi:10.1002/hed.24772
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.